 Sara Dorri1
Sara Dorri1 Fateme Sari2Seyedeh Nahid Seyedhasani3Alireza Atashi4
Fateme Sari2Seyedeh Nahid Seyedhasani3Alireza Atashi4 Esmatalsadat Hashemi2
Esmatalsadat Hashemi2 Asiie Olfatbakhsh2*
Asiie Olfatbakhsh2*- 1Department of Management and Health Information Technology, School of Management and Medical Information Sciences, Health Information Technology Research Center, Isfahan University of Medical Sciences, Isfahan, Iran
- 2Clinical Research Department, Breast Cancer Research Center, Motamed Cancer Institute, ACECR, Tehran, Iran
- 3Department of Health Information Technology, School of Paramedical Sciences, Torbat Heydariyeh University of Medical Sciences, Torbat Heydariyeh, Iran
- 4E-Health Department, Virtual School, Tehran University of Medical Sciences, Tehran, Iran
Introduction: The new coronavirus (COVID-19) has posed many new challenges to the health care and the timing of surgical care. At the beginning of the pandemic many guidelines recommended postponing elective surgical procedures to reallocate resources. As regards, delay in cancer treatment could be effective on cancer progression. The aim of this systematic review was to outline a guideline for preoperative screening before cancer surgeries and protecting health care workers during the pandemic.
Materials and Methods: This study was conducted through a search in electronic databases up to August 2020. PubMed, EMBASE, Web of Science, Scopus, Science Direct, and Google Scholar databases were searched without time limitation. The keywords were a combination of preoperative, cancer surgery, COVID-19, and their synonyms.
Results: The most commonly used ways to triage preoperatively were telephone pre-assessment for suspicious symptoms and history of contact or travel, 14-day self-isolation, in- hospital queries at admission, temperature monitoring, and isolation in a single room COVID-free ward or physical distancing. Reverse transcription-polymerase chain reaction (RT-PCR) test 24–72 h before operation was recommended commonly, except in inaccessible centers, but non-contrast chest-CT scan is not routinely advised for elective surgeries to salvage medical resources. Recommended personal protective equipment (PPE) for staffs were wearing N95 mask in addition to gown, gloves, eye protection in aerosol-generating procedures (AGPs), and wearing gloves, hats, and disposable surgical masks, practice distancing, and hand hygiene for all staffs. Meanwhile team separation of hospital staffs caring for COVID-19 patients, segregated areas for COVID-19 clean and contact, restriction of visitors and family members, and personal distancing are mostly recommended.
Conclusion: We hope this review would be a guidance for triage, preoperative testing, and summarizing safety principles during COVID-19 pandemic alongside with surgical reintegration.
Introduction
The new coronavirus (COVID-19) was identified in Wuhan, China in 2019. The WHO officially declared the outbreak a pandemic on March 11, 2020 (1). Coronavirus has spread around the world in a short time. Until December 3, 2020, COVID-19 has infected more than 64 million people all over the world, and 1.5 million died from it (2).
This pandemic has posed many new challenges to the health care and social systems, including shortage of resources such as personal protective equipment (PPE), ventilators, intensive care unit (ICU) beds, and blood resources (3). Infection of health care providers was also a major challenge.
In mid-March 2020, recommendations were released by the American College of Surgeons (ACS) (4), the Society of Gynecologic Oncology, and several medical and surgical professional societies to postpone elective surgical interventions (3–6). The document of the Centers for Medicare and Medicaid Services (CMS) provides recommendations to limit those medical services that could be deferred, such as non-emergent, elective treatment, and preventive medical services for patients of all ages (7). The ACS and CMS have categorized most gynecologic cancer cases as semiurgent. However, the ACS further emphasized that if cancer cases are significantly delayed, this could result in significant patient harm (7–9). On the other hand, the association of time interval from cancer diagnosis to definitive cancer surgery with risk of cancer specific outcomes is poorly understood (10).
While some cases could be postponed, the vast majority of the cancer cases have problems. It is important that the decision to cancel or perform a surgical procedure in patients with cancer have medical and legal dilemmas, and the risk of delay and disease progression should be considered. Cancer operation depends on tumor biology, the stage of tumor, and also the waiting list of newly diagnosed patients (11). In some cases, there are some alternative procedures like neoadjuvant systemic therapy. The Department of Surgical Oncology at MD Anderson Cancer Center have traditionally favored neoadjuvant therapy for many solid tumors. After the outbreak of COVID-19, they initiated or continued this treatment sequencing when possible to postpone surgery to beyond the peak of COVID-19 (12). Also there are some reports of hormone neoadjuvant bridging therapy in patients with asymptomatic COVID-19 infection to reduce waiting time during outbreaks and possible cancer progression (13, 14).
Regardless of priority, we know that COVID-19 related infection is most commonly asymptomatic or demonstrated by mild symptoms. Due to the incubation period, the potential of asymptomatic carriers, and the risk of deterioration of COVID-19 intra- and postoperatively, the status of patients should be confirmed before surgery. Preoperative triage during the COVID-19 pandemic is necessary because of the high risk of mortality during the post- or intraoperative period for patients undergoing surgery during the incubation period.
In Iran we had no prior experience to face this challenging situation. In this regards, we conduct a systematic review to outline the preoperative considerations for cancer surgeries during the pandemic of COVID-19 and protocols for protecting health care workers.
Materials and Methods
Search Strategy
First, a basic general search was conducted for a series of studies. The databases PubMed, SCOPUS, Science Direct, and Web of Science were searched until August 10, 2020 by searching on all fields. Citations in-process, which are not indexed with MeSH headings, were also searched. The search query consisted of three subqueries that targeted preoperative, cancer surgery, COVID-19, and their synonyms, all three combined with “AND.” Synonyms within a subquery were combined with “OR.” The search was conducted in English. The search strategy was modified and revised for all databases by two medical informatics specialists. A manual search was also performed for retrieving gray literature and the bibliographies of relevant articles.
Inclusion and Exclusion Criteria
All original papers describing preoperative protocols for cancer surgery in COVID-19 were included and duplicate studies were removed.
Two authors classified the papers by reading their title and abstract (FS, SNSH). In this phase, from all included articles, the studies that are specifically used for preoperative cancer surgery protocols were selected. The results were compared and discussed until a consensus was reached. If needed a paper was read by another reviewer (SD, AO) to reconcile decision on inclusion. References of papers found to be eligible for inclusion were reviewed manually based on their title and abstract (by AA, FS, SNSH). Intended data such as authors name, article title, year of publication, country, journal name, preoperative triage, and PPE were extracted from studies. Studies which were not original or did not mention their protocols were excluded.
Prisma flowchart is shown the Figure 1.
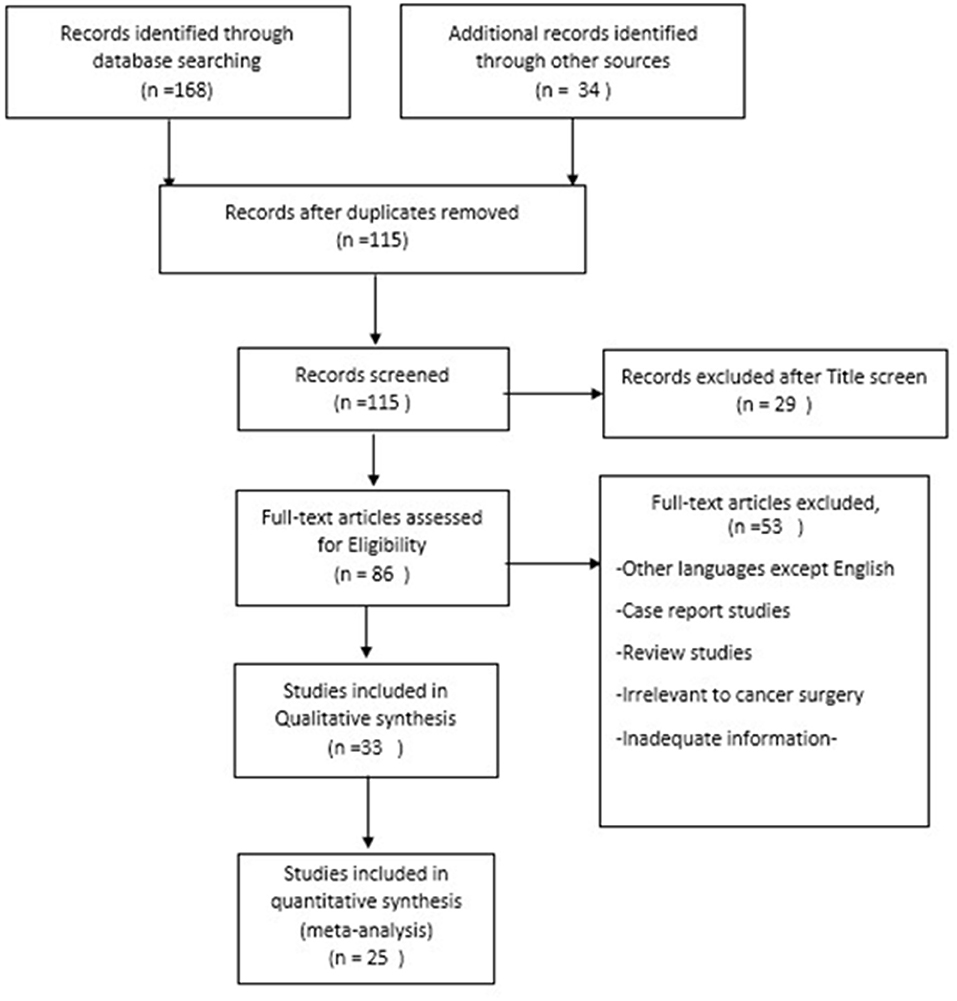
Figure 1. Prisma flowchart of the study.
Results
Until the end of searching, 168 articles were retrieved. By hand searching and finding the citations of some articles, 34 articles were added. After removing duplicates, 115 articles remained for further assessment based on title and abstract screening, among them 29 studies were irrelevant and excluded. After full-text assessments, 53 articles were excluded because of the following: other languages except English, irrelevant review studies, irrelevant to cancer surgery, and inadequate information. Finally, 25 articles remained. All evaluation was performed by two authors. Any conflict was solved by a third specialist (surgeon). All articles had acceptable quality and enough explanation about COVID-19 protocols which they had encountered.
About 70% of the articles were Q1 score quality, 19% were Q2, and 11% were Q3. All articles were written in 2020, right after the pandemic. Most articles were about head and neck, gynecology, esophagus, breast, colorectal, and lung cancer surgery. Most of the articles were written in USA (n = 6), France (n = 4), and China (n = 3). Kind of surgery, preoperative triage, and PPE were extracted from these studies. This information is shown in Table 1 and in summary in Table 2.
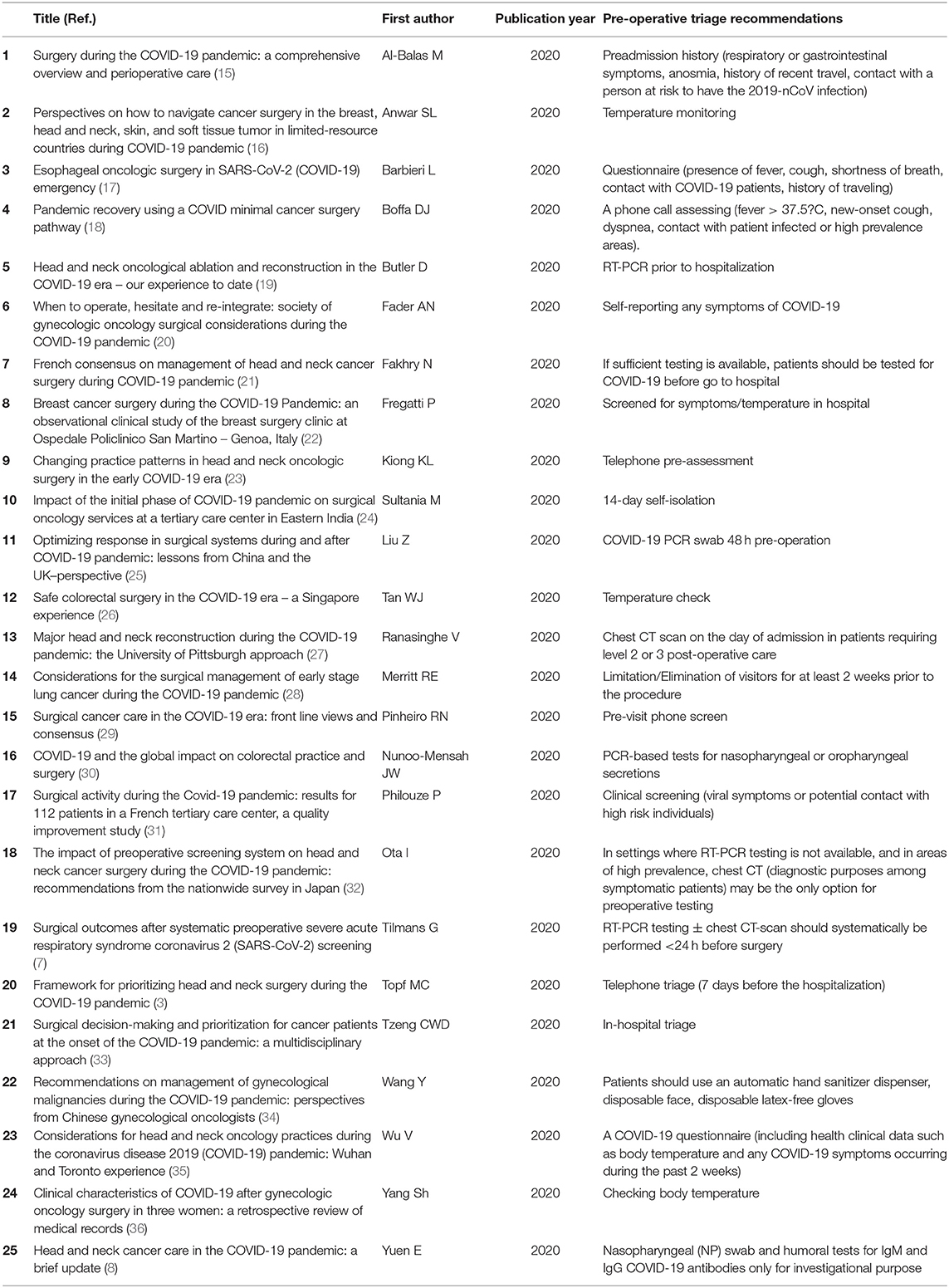
Table 1. The characteristics and the preoperative triage recommendations of the included studies.

Table 2. The type of surgeries and the summary of triage recommendations.
Type of Surgery
The categories of studies included seven cancer surgeries, three gynecologic cancer surgeries, eight head and neck and oral cancer surgeries, four digestive surgeries, two all types of surgeries including cancer, and only one article about breast cancer surgery.
Preadmission Assessment
In 15 articles preadmission process was explained. Six of them had telephone pre-assessment by a breast care nurse who asked them about COVID-19 symptoms and history of contact. Where possible, the preoperative review was completed more than a week ahead of the planned date of surgery and then allowed for 14 days self-isolation (19, 20, 32, 33). Twelve in-hospital assessment included history of contact or travel, and two of them used both (telephone call and in-hospital). Their assessment usually consisted of queries regarding the presence of viral symptoms including fever, cough, myalgia, dyspnea, diarrhea, nausea, and vomiting, and history of contact with high risk individuals, including those in quarantine with active COVID-19. At the time of admission, patients were clinically screened at entry into the institution and any positive screen was evaluated more precisely. Isolation in a single room, COVID-free ward was recommended in four articles (22, 29–31). Temperature monitoring was recommended in five articles and only negative patients were permitted access to the surgery unit (16, 18, 19, 22, 24).
Anesthesiologist consultation to select patients carefully with comorbidities and to discused about the potential COVID-19 related complications during the perioperative period (26). After completing preoperative review, a 14-day self-isolation was recommended in four articles to assist social distancing and to decrease the risk of asymptomatic infection (19, 20, 32, 33).
Preoperative COVID-19 Testing
Access to reliable testing for the presence of active virus has been a major challenge during this pandemic due to limited testing capacity, reagents, and supplies. Twenty-two of all 25 studies recommended routine preoperative COVID-19 test using real-time reverse transcription-polymerase chain reaction (RT-PCR) with nasopharyngeal or oropharyngeal swab between 24 to 72 h before surgery (Table 2). In one study, a repeated nucleic acid test in 24 h was recommended (25). Samples were obtained in-house or in-hospital. Operation was delayed in patients with a positive test until asymptomatic for 14 days, and then the patient was referred to a structure or a team specialized in the management of COVID-19. Some centers also recommended subsequent documentation of negative RT-PCR testing before proceeding to the operating room (20, 21). Patients who tested negative had a confirmatory telephone triage repeated on the day before hospitalization (22). A recent literature review and pooled analysis of previously published studies on RT-PCR performance from nasopharyngeal specimens demonstrated that the false negative rate of COVID-19 ranged from 20 to 100% depending on the test time since exposure to symptom onset (20). COVID-19 RT-PCR tests appear to be 100% specific (20). Humoral tests for IgM and IgG COVID-19 antibodies were performed only for investigational purpose and did not affect the surgical program in one article (22), and the coronavirus-specific IgM antibody was tested positive in another one in combination with chest-CT (25).
Chest CT-Scan or Chest-X ray
A non-contrast chest CT scan on the day or 1 day before admission to evaluate for any features consistent with COVID-19 infection was used in some studies (7, 17, 19–21, 25, 26, 29–32, 34, 36). Due to the limited laboratory testing capabilities, the diagnosis in many studies was not based solely on laboratory testing; therefore, a combination with chest-CT was proven to be effective during the outbreak. The sensitivity of chest-CT for COVID-19 was reported between 60 and 97% (7, 17, 25), and some patients had an initial positive chest-CT even before a positive RT-PCR result. Generally, the incubation period for COVID-19 can last 2 weeks or longer considering that CT scan rather than x-ray of the chest plays an essential role in the diagnosis of COVID-19 (36). However chest CT scans was not routinely practical for the preoperative screening of any elective surgery, especially in low-prevalence and low-income countries. This was because of avoiding wastage of medical resources (19, 20, 30, 32). Chest-X-ray was recommended as the alternative preoperative modality for chest-CT scan only in two articles (26, 36).
Personal Protective Equipment
Personal protective equipment was pointed in 22 of all the articles. The most recommendations were: Wearing mask, usually surgical mask, FFP2 or FFP3. N95 mask was reserved for aerosol-generating procedures (AGPs) like otolaryngology, endoscopy, thoracic surgeries, and for anesthesiologists (20, 21, 26, 29, 33). Also wearing gloves (double-layered in suspicious or unknown cases), gowns, eye protection, face shield, caps, footwear, and meticulous hand hygiene are referred to as standard PPE (3, 15–17, 20–23, 25–30, 32, 34, 35).
Screening symptoms and daily or twice daily temperature monitoring of health-care workers were mentioned in four articles (15, 16, 18, 29). Using minimum number of staff in the operation room (20, 24, 29) and negative pressure or good air exchange in the operating room (8, 20, 26) were also considered. The type of surgery and triage recommendations are summarized in Table 2.
Discussion
Overview
This systematic review provided comprehensive considerations for preoperative cancer triage in COVID-19 pandemic. Results revealed that preoperative triage process should start before patient admission till after surgery. Telephone pre-assessment, if possible, asking for suspicious symptoms, history of contact or travel, and if negative, a 14-day self-isolation is one of the best ways for preoperative triage. On the day of admission, it should be continued by in-hospital queries, temperature monitoring, and isolation in a single room COVID-free ward or physical distancing. Reverse transcription-polymerase chain reaction test 24–72 h before operation was recommended commonly, except in unaccessible centers. Non-contrast chest-CT scan on the day or 1 day before admission was recommended only in conditions like limited laboratory testing, but not routinely for elective surgeries to salvage medical resources. Using PPE for staffs are recommended.
While many surgical communities recommended specific guidelines to triage surgical cases for delaying during COVID-19 pandemic, there is scant guidance on how to resume surgical practice in cancer patients. At the beginning of the pandemic, many national and international scientific societies published recommendations to prioritize cancer management strategies, preserve hospital resources for COVID-19, and reduce the risk of cross-infection. But the association between time interval from cancer diagnosis to definitive cancer surgery with the risk of cancer specific outcomes is a challenging problem and creates anxiety in the patient (10). Vanni et al. evaluated the impact of breast cancer screening suspension and treatment delay during the COVID-19 outbreak. In a multicentric study, they retrospectively analyzed data from four Italian breast units. All patients who underwent breast surgery from March 11, 2020 to May 30, 2020 were compared with patients who underwent breast surgery during the same period of the previous year, defined as the prelockdown group. They reported an increase in lymph nodes involvement, and the most significant factor predictive of major advanced N stage was the waiting time on list before surgery. They predicted that in the coming months, an increase in tumor dimensions might occur, and the importance of maintaining breast cancer screening programs and avoiding oncological treatment delay is recommended (37).
In another study, Turaga et al. utilized the National Cancer Database (NCDB) to measure overall survival of all patients undergoing definitive cancer surgery. In this cohort study, from 2004 to 2016, 4,403,437 cancer patients that underwent definitive cancer surgery were included. Patients with head and neck cancers were specifically excluded due to the increased risk of aerosol transmission in their care, making decision making more complex. They found that most cancer surgeries can be safely delayed beyond current wait time for at least 4 weeks without having a significant impact on patient survival or cancer progression. They concluded that these data can be used to assure patients and their family members, and be utilized to build triage systems during a public health emergency (10).
We know that tumor doubling times are not constant. For example, some studies estimated the mean doubling time of breast tumors between 45 and 260 days. This very inaccurate measuring is unhelpful in determining the effect of screening delays on breast cancer survival. However, it is estimated that in 6 months, upto 50% of cases of breast cancer could exhibit a growth of more than the size of a centimeter (38).
Another issue is that in the case of being a candidate for surgery, COVID-19 infection is most commonly asymptomatic or demonstrated by mild symptoms, and because of the potential of asymptomatic carriers and the risk of deterioration of disease intra- and postoperatively, the status of patients should be confirmed before surgery. Yang et al. described the clinical characteristics and outcomes of the patients who were unintentionally scheduled for elective surgeries during the incubation period of COVID-19 infection. In this retrospective cohort study of 34 operative patients with confirmed COVID-19, 15 patients (44.1%) needed ICU care and the mortality rate was 20.5% (36).
A multicentric study, which was funded by the National Institute for Health Research (NIHR), was conducted in patients who had surgery from 235 hospitals in 24 countries and included all surgical patients who were confirmed to have COVID-19 infection. The primary and secondary outcomes were the 30-day mortality rate after surgery and pneumonia, acute respiratory distress syndrome, or accidental ventilation after surgery. Among 1,128 patients undergoing surgery, 294 patients (26.1%) were confirmed to have COVID-19 infection before surgery, their 30-day mortality rate was 23.8%, and pulmonary complications occurred in 51.2% of patients with perioperative COVID-19 infection. They suggested that the increased risks associated with COVID-19 infection should be balanced against the risks of delaying surgery in individual patients (39).
Another important reason to think about treatment delay in addition to the risk of COVID-19 infection is the enormous pressure on health services which emphasize this evaluation. There is a reality that we will face COVID-19 for months, if not years. So reorganization for cancer treatment should be prioritized to maximize the safety of patients, surgeons, and other healthcare professionals during the COVID-19 pandemic.
The referral pathway through the multidisciplinary team (MDT), an individualized plan according to the hospital and regional resources, and to specially introduce anesthetists in this team could help in safely continuing oncologic surgery as long as careful preservation of health care system is taken care of. Anesthesiologists' intervention could evaluate routine comorbidities, risk stratification, and clear the perioperative risks that threaten a patient (19).
The first step is assessing patients if there is any symptom like fever, cough, dyspnea, any contact with infected patient, or travel to high-prevalence areas. This information could be obtained by telephone call or other virtual technologies before admission, if possible. Today, with improvement of electronic health it could be done by web-based applications or telemedicine systems, which could be connected with electronic health records (40–42). Then in-hospital assessment should be done through queries. The patient's body temperature should be detected on admission and in the ward (22). Isolation in a single room, COVID-free ward, or maintaining the correct interpersonal distance is mandatory (22). Clinicians should counsel patients about the risks of cancer surgical delay versus COVID-19 related complications when acquired during the perioperative period or when the patient had a false negative test before admission through a consent form (19, 20).
Diagnostic testing involving identification of COVID-19 using RT-PCR has been a major challenge during this pandemic due to limited resources (20); however, this test was recommended in most studies. The only reasons for limitation are the issues of false negative rate and limited COVID-19 testing availability. Theoretically RT-PCR assays for COVID-19 should be highly sensitive in detecting the presence of viral RNA. However, the limit of detection differs among the various respiratory tract sources. The false negative rate of RT-PCR was reported from 20 to 100% depending on the test time point (5). Care must be taken in interpreting RT-PCR tests for COVID-19 infection, particularly early in the course of infection, when using these results as a basis for removing precautions. COVID-19 RT-PCR tests appear to be 100% specific (20). A single negative test cannot reliably exclude COVID-19, and N95 masks should be worn, when available during AGPs (20). The coronavirus-specific IgM antibody can be tested positive in 3–5 days post-infection (25); however, the COVID-19 serology test usually does not affect the surgical program and has only an investigational purpose (22, 43). Blood samples for blood cell counts and C-reactive protein measurements are encountered as routine measurement, not specifically for COVID-19 triage. Surgery in patients with confirmed COVID-19 should be postponed until proof of virus clearance is obtained and the patient is asymptomatic (44).
Published reports from China during the viral outbreak reported the role of screening computed tomography (CT). One study demonstrated that the sensitivity of chest CT was greater than that of RT-PCR (98 vs. 71%, respectively). Another study demonstrated the sensitivity of CT scan in identifying COVID-19 of 68.4% and specificity of 88% in the population in whom the CT chest was performed as a screening examination (45). Their results supported the use of chest CT for screening for COVD-19 for patients with clinical and epidemiologic features compatible with COVID-19 infection, particularly when RT-PCR testing is negative (46). However as preoperative assessment tool, generalizability of these results is limited (19). In settings where RT-PCR testing is not available, and in areas of high prevalence, chest CT may be the only option for preoperative testing. The American College of Radiology recommends that it need not be performed as a screening test for COVID-19 and rather be reserved for diagnostic purposes among symptomatic patients (47). It is clearly important that imaging facilities are better to be used where there is clear benefit for patients (45, 48). Additionally, the same day discharge can minimize length of hospital stay. Enhancing immunity with some dietary components such as dietary protein, omega-3 fatty acids, and vitamin A can improve the conditions of cancer patients and enhance immunity (49).
After authorization of some COVID-19 vaccines by FDA, the recommendation of the National Comprehensive Cancer Network (NCCN) COVID-19 Vaccination Advisory Committee about vaccination before major surgeries of solid tumors is that vaccination has to be taken at least a few days before the surgery (50). The MSKCC recommendation for patients undergoing cancer-related surgery is a few days or a week or two may be before cancer-related surgery1. In patients with completed vaccination dose, the risk of unintended infection before and during surgery would be decreased.
Personal Protective Equipment
Healthcare workers are at high risk to be affected by virus transmission during surgery in asymptomatic patients with negative COVID-19 tests or those in the incubation period. The risk of transmission is through aerosol and droplets especially during AGPs including bronchoscopy, endotracheal intubation, tracheostomy procedures, cardiopulmonary resuscitation, and diagnostic sputum induction. Wearing N95 mask in addition to droplet PPE (gown, gloves, eye protection) are regarded as minimum protection for all staff members in surgeries involving exposure of upper aero-digestive tracts. The daily assessment of personnel health status and recording body temperature is considered. Routine COVID-19 test is not useful except for workers who directly treat COVID-19 patients and who perform AGPs. All medical staff should perform their clinical tasks wearing gloves, hats, and disposable surgical masks, practice distancing, and hand hygiene correctly (15, 18). Medical leave for all staffs with respiratory symptoms, team separation of hospital staffs caring for COVID-19 patients, as well as segregated areas within the hospital for COVID-19 clean and contact, triage of all hospital visitors (16), restriction of visitors and family members and personal distancing (22) are mostly recommended.
Intraoperative safety that should be taken for all aerosolizing procedures, but not limited to, are the use of N95 respirators, face shields, or goggles for eye protection, gloves, gowns, disposable medical caps, and shoe covers in the operating room. Also quick and safe induction of anesthesia and reducing the number of individuals inside the operating rooms to the minimum required are advised (35, 51). Surgeons should wear the usual cap, gowns, footwear protection, and double gloves. N95 masks (when available) and eye protection are recommended for AGPs; surgical mask with eye protection can be used for non-AGPs (20). Some operating rooms have an average of 15–40 air exchanges per hour to clean air, and that if available could be strongly helpful (26).
Conclusion
There is a reality that the pandemic will not be short-lived although efforts continue to use widespread effective vaccines to protect health care workers and other people. We know that delay in cancer treatment could be harmful for patients. This review could be an applicable guidance to facilitate setting up services in the managing cancer patients in addition to save clinicians and staff during this challenging time. It can easily be transferred to other surgical specialties to reorganize clinical activities and avoid any impairment of survival of cancer patients.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author Contributions
SD: search—title, abstract, and full text assessment and classify—full text evaluation—manuscript writing. FS and SS: search—title, abstract, and full text assessment and classify. AA: search—evaluation of conflicts. EH: manuscript writing. AO: full text evaluation—major contributor in manuscript writing. All authors read and approved the final manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
COVID, corona virus disease; RT-PCR, reverse transcription-polymerase chain reaction; CT, computed tomography; AGPs, aerosol generating procedures; WHO, World Health Organization; PPE, personal protective equipment; ICU, intensive care unit; ACS, American College of Surgeons; SGO, Society of Gynecologic Oncology; CMS, Centers for Medicare and Medicaid Services; IgG, immunoglobulin G; IgM, immunoglobulin M; MDT, multidisciplinary team; RNA, ribonucleic acid; NCCN, National Comprehensive Cancer Network; MSKCC, Memorial Sloan Kettering Cancer Center.
Footnotes
References
1. World Health Organization. Rolling Updates on Coronavirus Disease (COVID-19). (2020). Available online at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (accessed July 31, 2020).
2. Tracking Coronavirus' Global Spread. (2020). Available online at: https://edition.cnn.com/interactive/2020/health/coronavirus-maps-and-cases/ (accessed December 3, 2020).
3. Topf MC, Shenson JA, Holsinger FC, Wald SH, Cianfichi LJ, Rosenthal EL, et al. Framework for prioritizing head and neck surgery during the COVID-19 pandemic. Head Neck. (2020) 42:1159–67. doi: 10.1002/hed.26184
4. COVID-19: Guidance for Triage of Non-Emergent Surgical Procedures. (2020). Available online at: https://www.facs.org/covid-19/clinical-guidance/triage (accessed March 24, 2020).
5. Kucirka LM, Lauer SA, Laeyendecker O, Boon D, Lessler J. Variation in false-negative rate of reverse transcriptase polymerase chain reaction–based SARS-CoV-2 tests by time since exposure. Ann Intern Med. (2020) 173:262–7. doi: 10.7326/M20-1495
6. Available, online at: https://www.sgo.org/wpcontent/uploads/2020/03/Surgical_Considerations_Communique.v14.pdf (accessed March 2020).
7. Tilmans G, Chenevas-Paule Q, Muller X, Breton A, Mohkam K, Ducerf C, et al. Surgical outcomes after systematic preoperative severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) screening. Surgery. (2020) 168:209–11. doi: 10.1016/j.surg.2020.05.006
8. Yuen E, Fote G, Horwich P, Nguyen SA, Patel R, Davies J, et al. Head and neck cancer care in the COVID-19 pandemic: a brief update. Oral Oncol. (2020) 105:104738. doi: 10.1016/j.oraloncology.2020.104738
9. Non-Emergent Elective Medical Services and Treatment Recommendations. Centers for Medicare and Medicaid Services (CMS) (2020).
10. Turaga KK, Girotra S. Are we harming cancer patients by delaying their cancer surgery during the COVID-19 pandemic? Ann Surg. (2020). doi: 10.1097/SLA.0000000000003967
11. Beltran-Miranda P, Muñoz-Cruzado VD, De la Portilla-de Juan F, Pareja-Ciuro F, Padillo J. Comment on: “The management of surgical patients during the coronavirus disease 2019 (COVID-19) pandemic”. Surgery. (2020) 169:478–9. doi: 10.1016/j.surg.2020.07.011
12. Tzeng C-WD, Teshome M, Katz MH, Weinberg JS, Lai SY, Antonoff MB, et al. Cancer surgery scheduling during and after the COVID-19 first wave: the MD Anderson cancer center experience. Ann Surg. (2020) 272:e106. doi: 10.1097/SLA.0000000000004092
13. Pellicciaro M, Granai AV, Marchese G, Materazzo M, Cotesta M, Santori F, et al. Breast cancer patients with hormone neoadjuvant bridging therapy due to asymptomatic Corona virus infection. Case report, clinical and histopathologic findings. Int J Surg Case Rep. (2020) 76:377–80. doi: 10.1016/j.ijscr.2020.10.020
14. Gasparri ML, Gentilini OD, Lueftner D, Kuehn T, Kaidar-Person O, Poortmans P. Changes in breast cancer management during the corona virus disease 19 pandemic: an international survey of the European Breast Cancer Research Association of Surgical Trialists (EUBREAST). Breast. (2020) 52:110–5. doi: 10.1016/j.breast.2020.05.006
15. Al-Balas M, Al-Balas HI, Al-Balas H. Surgery during the COVID-19 pandemic: a comprehensive overview and perioperative care. Amer J Surg. (2020) 219:903–6. doi: 10.1016/j.amjsurg.2020.04.018
16. Anwar SL, Harahap WA, Aryandono T. Perspectives on how to navigate cancer surgery in the breast, head and neck, skin, and soft tissue tumor in limited-resource countries during COVID-19 pandemic. Int J Surg. (2020) 79:206–12. doi: 10.1016/j.ijsu.2020.05.072
17. Barbieri L, Talavera Urquijo E, Parise P, Nilsson M, Reynolds JV, Rosati R. Esophageal oncologic surgery in SARS-CoV-2 (COVID-19) emergency. Dis Esophagus. (2020). 33:doaa028. doi: 10.1093/dote/doaa028
18. Boffa DJ, Judson BL, Billingsley KG, Galeta D, Fontanez P, Odermatt C, et al. Pandemic recovery using a covid-minimal cancer surgery pathway. Ann Thorac Surg. (2020) 110:718–24. doi: 10.1016/j.athoracsur.2020.05.003
19. Butler D, Davies-Husband C, Dhanda J, Francis I, Gulati A, Kapoor K, et al. Head and neck oncological ablation and reconstruction in the COVID-19 era–our experience to date. Brit J Oral Maxillofac Surg. (2020) 58:1008–13. doi: 10.1016/j.bjoms.2020.06.011
20. Fader AN, Huh WK, Kesterson J, Pothuri B, Wethington S, Wright JD, et al. When to operate, hesitate and reintegrate: society of gynecologic oncology surgical considerations during the COVID-19 pandemic. Gynecol Oncol. (2020) 158:236–43. doi: 10.1016/j.ygyno.2020.06.001
21. Fakhry N, Schultz P, Morinière S, Breuskin I, Bozec A, Vergez S, et al. French consensus on management of head and neck cancer surgery during COVID-19 pandemic. Eur Ann Otorhinolaryngol Head Neck Dis. (2020) 137:159–60. doi: 10.1016/j.anorl.2020.04.008
22. Fregatti P, Gipponi M, Giacchino M, Sparavigna M, Murelli F, Toni ML, et al. Breast cancer surgery during the COVID-19 pandemic: an observational clinical study of the breast surgery clinic at ospedale policlinico San Martino–Genoa, Italy. In Vivo. (2020). 34(3 Suppl):1667–73. doi: 10.21873/invivo.11959
23. Kiong KL, Guo T, Yao CM, Gross ND, Hanasono MM, Ferrarotto R, et al. Changing practice patterns in head and neck oncologic surgery in the early COVID-19 era. Head Neck. (2020) 42:1179–86. doi: 10.1002/hed.26202
24. Sultania M, Muduly DK, Balasubiramaniyan V, Imaduddin M, Ephraim R, Chaudhary I, et al. Impact of the initial phase of COVID-19 pandemic on surgical oncology services at a tertiary care center in Eastern India. J Surg Oncol. (2020) 122:839–43. doi: 10.1002/jso.26140
25. Liu Z, Ding Z, Guan X, Zhang Y, Wang X, Khan JS. Optimizing response in surgical systems during and after COVID-19 pandemic: lessons from China and the UK–perspective. Int J Surg. (2020) 78:156. doi: 10.1016/j.ijsu.2020.04.062
26. Tan WJ, Foo FJ, Sivarajah SS, Li LHM, Koh FH, Chew MH. Safe colorectal surgery in the COVID-19 Era–a Singapore experience. Ann Coloproctol. (2020) 36:65–9. doi: 10.3393/ac.2020.04.21
27. Ranasinghe V, Mady LJ, Kim S, Ferris RL, Duvvuri U, Johnson JT, et al. Major head and neck reconstruction during the COVID-19 pandemic: the University of Pittsburgh approach. Head Neck. (2020) 42:1243–7. doi: 10.1002/hed.26207
28. Merritt RE, Kneuertz PJ. Considerations for the surgical management of early stage lung cancer during the COVID-19 pandemic. Clin Lung Cancer. (2020) 22:150–60. doi: 10.1016/j.cllc.2020.06.024
29. Pinheiro RN, Coimbra FJF, Costa-Jr WLD, Ribeiro HSC, Ribeiro R, Wainstein AJA, et al. Surgical cancer care in the COVID-19 era: front line views and consensus. Rev Col Bras Cir. (2020) 47:e20202601. Portuguese, English. doi: 10.1590/0100-6991e-20202601
30. Nunoo-Mensah JW, Rizk M, Caushaj PF, Giordano P, Fortunato R, Dulskas A, et al. Covid-19 and the global impact on colorectal practice and surgery. Clin Colorectal Cancer. (2020) 19:178.e1–90.e1. doi: 10.1016/j.clcc.2020.07.008
31. Philouze P, Cortet M, Quattrone D, Céruse P, Aubrun F, Dubernard G, et al. Surgical activity during the Covid-19 pandemic: results for 112 patients in a French tertiary care center, a quality improvement study. Int J Surg. (2020) 80:194–201. doi: 10.1016/j.ijsu.2020.07.023
32. Ota I, Asada Y. The impact of preoperative screening system on head and neck cancer surgery during the COVID-19 pandemic: recommendations from the nationwide survey in Japan. Auris Nasus Larynx. (2020) 47:687–91. doi: 10.1016/j.anl.2020.05.006
33. Tzeng C-WD, Cao HST, Roland CL, Teshome M, Bednarski BK, Ikoma N, et al. Surgical decision-making and prioritization for cancer patients at the onset of the COVID-19 pandemic: a multidisciplinary approach. Surg Oncol. (2020) 34:182–5. doi: 10.1016/j.suronc.2020.04.029
34. Wang Y, Zhang S, Wei L, Lin Z, Wang X, Wang J, et al. Recommendations on management of gynecological malignancies during the COVID-19 pandemic: perspectives from Chinese gynecological oncologists. J Gynecol Oncol. (2020). 31:e68. doi: 10.3802/jgo.2020.31.e68
35. Wu V, Noel CW, Forner D, Zhang Z-J, Higgins KM, Enepekides DJ, et al. Considerations for head and neck oncology practices during the coronavirus disease 2019 (COVID-19) pandemic: Wuhan and Toronto experience. Head Neck. (2020) 42:1202–8. doi: 10.1002/hed.26205
36. Yang S, Zhang Y, Cai J, Wang Z. Clinical characteristics of COVID-19 after gynecologic oncology surgery in three women: a retrospective review of medical records. Oncologist. (2020) 25:e982–5. doi: 10.1634/theoncologist.2020-0157
37. Vanni G, Tazzioli G, Pellicciaro M, Materazzo M, Paolo O, Cattadori F, et al. Delay in breast cancer treatments during the first COVID-19 lockdown. A multicentric analysis of 432 patients. Anticancer Res. (2020) 40:7119–25. doi: 10.21873/anticanres.14741
38. Vanni G, Pellicciaro M, Materazzo M, Palombi L, Buonomo OC. Breast cancer diagnosis in coronavirus-era: alert from Italy. Front Oncol. (2020) 10:938. doi: 10.3389/fonc.2020.00938
39. Collaborative CO. Mortality and pulmonary complications in patients undergoing surgery with perioperative SARS-CoV-2 infection: an international cohort study. Lancet. (2020) 396:27–38. doi: 10.1016/S0140-6736(20)31182-X
40. Madhavan S, Bastarache L, Brown JS, Butte AJ, Dorr DA, Embi PJ, et al. Use of electronic health records to support a public health response to the COVID-19 pandemic in the United States: a perspective from 15 academic medical centers. J Amer Med Inform Assoc. (2020) 28:393–401. doi: 10.1093/jamia/ocaa287
41. Pryor R, Atkinson C, Cooper K, Doll M, Godbout E, Stevens MP, et al. The electronic medical record and COVID-19: is it up to the challenge? Am J Infect Control. (2020) 48:966–7. doi: 10.1016/j.ajic.2020.05.002
42. Pan S, Jiang J, Chen Z, Yang L. Management and Thinking on the treatment of cancer patients during the COVID-19. Front Mol Biosci. (2021) 8:673360. doi: 10.3389/fmolb.2021.673360
43. For, AotUoP-o-CIT,. https://www.who.int/news-room/commentaries/detC-,ail/advice-on-the-use-of-point-of-care-immunodiagnostic-tests-forcovid-,19#.XpM1L2aCbKI.email (accessed April 3, 2021).
44. Vinh DB, Zhao X, Kiong KL, Guo T, Jozaghi Y, Yao C, et al. Overview of COVID-19 testing and implications for otolaryngologists. Head Neck. (2020) 42:1629–33. doi: 10.1002/hed.26213
45. Callaway M, Harden S, Ramsden W, Beavon M, Drinkwater K, Vanburen T, et al. A national UK audit for diagnostic accuracy of preoperative CT chest in emergency and elective surgery during COVID-19 pandemic. Clin Radiol. (2020) 75:705–8. doi: 10.1016/j.crad.2020.06.010
46. Fang Y, Zhang H, Xie J, Lin M, Ying L, Pang P, et al. Sensitivity of chest CT for COVID-19: comparison to RT-PCR. Radiology. (2020) 296:E115–7. doi: 10.1148/radiol.2020200432
47. American College of Radiology Arftuocr and computed tomography (CT) for suspected COVID-19 infection hwaoA-a-EA-P-SR- for-Chest-Radiography-and-CT-for-Suspected-COVID19-Infection (2020). AA.
48. Chetan MR, Tsakok MT, Shaw R, Xie C, Watson RA, Wing L, et al. Chest CT screening for COVID-19 in elective and emergency surgical patients: experience from a UK tertiary centre. Clin Radiol. (2020) 75:599–605. doi: 10.1016/j.crad.2020.06.006
49. BourBour F, Mirzaei Dahka S, Gholamalizadeh M, Akbari ME, Shadnoush M, Haghighi M, et al. Nutrients in prevention, treatment, and management of viral infections; special focus on coronavirus. Arch Physiol Biochem. (2020) 2020:1–10. doi: 10.1080/13813455.2020.1791188
50. Available, online at: https://www.nccn.org/docs/default-source/covid-19/2021_covid-19_vaccination_guidance_v4-0.pdf?sfvrsn=b483da2b_70 (accessed September 30, 2021).
Keywords: COVID-19, preoperative, screening, cancer, surgery
Citation: Dorri S, Sari F, Seyedhasani SN, Atashi A, Hashemi E and Olfatbakhsh A (2021) Practical Recommendations for the Preoperative Screening and Protective Protocols in Cancer Surgeries During COVID-19: A Systematic Review. Front. Surg. 8:678700. doi: 10.3389/fsurg.2021.678700
Received: 10 March 2021; Accepted: 18 October 2021;
Published: 23 November 2021.
Edited by:
Gianluca Vanni, University of Rome Tor Vergata, ItalyReviewed by:
Benedetto Ielpo, Parc de Salut Mar, SpainMarco Pellicciaro, University of Rome Tor Vergata, Italy
Copyright © 2021 Dorri, Sari, Seyedhasani, Atashi, Hashemi and Olfatbakhsh. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Asiie Olfatbakhsh, Zm9sZmF0YmFraHNoQHlhaG9vLmNvbQ==