 Chaoliang Shi1
Chaoliang Shi1 Yangyun Wang
Yangyun Wang
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Surg. , 14 July 2021
Sec. Genitourinary Surgery and Interventions
Volume 8 - 2021 | https://doi.org/10.3389/fsurg.2021.670123
This article is part of the Research Topic Advances on Pathogenesis and Treatment of Lower Urinary Tract Symptoms and Pelvic Floor Dysfunction Diseases View all 22 articles
Background: This study aimed to evaluate the clinical efficacy of Yun-type optimized pelvic floor training therapy for middle-aged women with severe overactive bladder (OAB).
Methods: This randomized, observer-blinded, parallel-group controlled clinical trial included 108 middle-age women with severe OAB and assigned them to the intervention group (treated with combination of Yun-type optimized pelvic floor training with solifenacin for 12 weeks) and control group (treated with solifenacin for 6 weeks and, after 2 weeks of elution, received the combination of Yun-type optimized pelvic floor training and solifenacin for 6 weeks). The outcomes associated with OAB, pelvic floor muscle (PFM) function, and sexual function were compared after 6 and 12/14 weeks of treatment.
Results: The primary variables were OAB-associated outcomes, including overactive bladder symptom score (OABSS), urgent urination, urine, nocturia, urge urinary incontinence, patient's perception of bladder condition, urogenital distress inventory-6, incontinence impact questionnaire-7, voiding volume, average flow rate, and maximum flow rate. The secondary variables were indicators related to PFM function and sexual function. These indicators were significantly improved in both groups after interventions. Notably, the improvements in most of these indicators were superior in the intervention group than in the control group after 6 weeks and 12/14 weeks of treatment.
Conclusions: The use of Yun-type optimized pelvic floor training adds to the benefits of solifenacin regarding severe OAB-associated outcomes, PMF function, and sexual function in middle-aged women with severe OAB. Combining Yun-type optimized pelvic floor training with traditional drug therapies may improve clinical outcomes in patients with severe OAB.
Trial Registration: ChiCTR-INR-17012189.
Overactive bladder (OAB) is a chronic condition with a negative impact on quality of life (QoL) (1, 2). It is characterized by urinary urgency with or without urgency urinary incontinence (UUI), usually accompanied by urinary frequency and nocturia (3). The prevalence of OAB in the general population is estimated to be 14–16% (4) and increases with age; ~30% of women over 65 years old are diagnosed with OAB (5). The symptoms of OAB have adverse impacts on sleep, mental health, work productivity, and QoL (6, 7). OAB is also associated with lower sexual desire, sexual arousal, orgasm, and sexual satisfaction, resulting in female sexual dysfunction (SD) (6). Moreover, OAB imposes a significant economic burden surpassing $14 billion with societal costs for older women (8). Therefore, it is important to develop an effective treatment strategy for management of OAB.
In clinical practice, OAB is usually treated with antimuscarinic agents such as solifenacin, tolterodine, fesoterodine, trospium, darifenacin, and propantheline to inhibit detrusor contractions (9, 10). However, these antimuscarinic agents have some side effects such as headache, nausea, dry eyes and mouth, and constipation (11). The International Continence Society (ICS) committee has suggested that the cause of OAB is from the detrusor itself. Stress and urge symptoms may both derive from the same anatomical defect, a lax vagina. This laxity may be caused by defects within the vaginal wall itself, or its supporting structures i.e., ligaments, muscles, and their connective tissue insertions, which may dissipate the muscle contraction, causing stress incontinence, and/or activation of an inappropriate micturition reflex, leading to symptoms of frequency, urgency, nocturia with or without urine loss (12–14). Pelvic floor muscle (PFM) training (PFMT) has been shown to reduce detrusor activity and improve QoL in patients with OAB (15) and has been recommended as first-line therapy for women with stress and other types of urinary incontinence (16). PFMT involves the contraction of the puborectal anal sphincter and external urethral muscles that inhibits the detrusor muscle contraction, justifying its use in OAB treatment (17). However, PFMT is monotonous, leading to poor compliance and lack of improvement of OAB symptoms (18). Despite the developments in behavioral medicine, it is still unclear whether making PFMT fashionable and interesting has a better clinical effect on severe OAB than traditional PFMT.
In this study, we established a new safe and effective groin-pelvic floor functional reconstruction training method called Yun-type optimized pelvic floor training. This method combines PFMT with fashionable and sexy dance moves. We then aimed to assess the efficacy and safety of this method for patients with severe OAB using a randomized, observer-blinded, parallel-group controlled clinical trial. Our results will provide new insights for optimizing the treatment of OAB.
This study was designed as a randomized, observer-blinded, parallel-group controlled clinical trial. Written informed consent was obtained from all participants, and the protocol was reviewed and approved by the Ethics Committee of the Shanghai Fifth People's Hospital Affiliated to Fudan University (No. 2017-041). The clinical trial registration was ChiCTR-INR-17012189.
A total of 108 women with severe OAB were recruited from Shanghai Fifth People's Hospital, Fudan University. The inclusion criteria were listed as follows: (1) married women aged 30–45 years; nullipara or gave birth by cesarean section; (2) urgent urination with or without UUI, able to complete a 3-day urination diary, ≥8 episodes of urgent urination within 24 h over 3 days, and ≥2 episodes of urination at night, with urine volume <200 ml each time; (3) the total score of overactive symptom bladder score (OABSS) ≥ 12 points and urgent urination score ≥ 2 points; (4) the female sexual function index (FSFI) <25 points; (5) stable sexual partners; (6) duration of disease > 3 months; and (7) no drug use during the 3 months before selection. The exclusion criteria were as follows: (1) patients had no sexual experience, were breastfeeding or in menopause, or had pelvic floor organ prolapse, gynecological inflammation, tumor, and other endocrine diseases; (2) patients with stress incontinence or mixed urinary incontinence dominated by stress urinary incontinence; (3) patients had urinary infection or chronic inflammation such as interstitial cystitis, bladder stones, and malignant tumors; (4) patients had a history of transurethral and pelvic surgery; (5) patients had diabetes, glaucoma, myasthenia gravis, ulcerative colitis, severe constipation, and dyspepsia; (6) post-voiding residual (PVR) > 50 ml; (7) patients had used M3 receptor blockers or other drugs to treat OAB; (8) patients were intolerant to the adverse effects of solifenacin; and (9) patients were unable to complete treatment course, or could not complete the Yun-type optimized pelvic floor training, urination diary, blood tests, and urodynamic tests.
The patients were randomly assigned into intervention group and control group. Randomization was performed in a double-blinded manner through a central computerized system by using randomly permuted blocks (size = 6). Specifically, 6 community health service centers in our hospital and the same area were grouped using block randomization, and each group included 18 cases. The case was diagnosed in our hospital and transferred to the corresponding community for treatment. Patients in the intervention group received Yun-type optimized pelvic floor training therapy combined with solifenacin (10 mg/d) for 12 weeks. Patients in the control group were first treated with solifenacin (10 mg/d) for 6 weeks and, after 2 weeks of elution, received a combination of Yun-type optimized pelvic floor training therapy and solifenacin (10 mg/d) for 6 weeks. The details regarding the Yun-type optimized pelvic floor training therapy (19–21) were as follows: each patient wore a 488 bi metal waist chain with a weight of (0.8+0.1) kg at the waist and hip during training. The training included 15 min of crotch base warm-up exercises; 25 min of crotch shaking, crotch twisting, crotch shaking, crotch sending, upper crotch, lower crotch, and sago shaking under the condition of contracting the anus and vagina (the specific time and rhythm of anus contraction and vagina contraction were conducted according to the command of the head coach); and the last 15 min of PFM strengthening and body relaxation exercises with soothing music: in detail, legs flexed and slightly apart, followed by slow frequency (contraction of the anus and vagina lasts for 30 s during inhalation, and relaxation lasts for 10 s during exhalation) and fast frequency (contraction of the anus and vagina for 2 s during inhaling, and relaxation for 2 s during exhalation) courses, 45 times per course. Yun-type optimized pelvic floor training was done at least four times a week.
The primary endpoints were OAB-related outcomes such as OABSS, urgent urination, urine, nocturia, UUI, patient's perception of bladder condition (PPBC), urogenital distress inventory-6 (UDI-6), incontinence impact questionnaire-7 (IIQ-7), voiding volume (VV), average flow rate (Qave), maximum flow rate (Qmax), and postvoid residual urine volume (PVR)]. The secondary endpoints were outcomes related to PFM function such as type I/II muscle strength and PFM tension as well as sexual function-associated outcomes such as FSFI, sexual desire, arousal, damp, orgasm, pain, and satisfaction. The PFM assessment was measured using the Glazer Protocol as previous described (22). These outcomes were measured before treatment and 6 weeks and 12/14 weeks after.
Continuous data were tested for normality. Normally distributed data were expressed as mean ± standard deviation and differences between groups were analyzed with the t-test, whereas data that were not normally distributed were presented as median (interquartile range) and compared using the Mann–Whitney U test. Qualitative data were represented as n (%) and analyzed by chi-square (χ2) test. The repeated measures ANOVA was used to analyze the main effect of study group, the main effect of time and the interaction between group and time on the changes in endpoints, including age as a covariate. The required sample size was calculated to have 90% power to detect a difference of endpoints the intervention group and to have 60% power in the control group using unpaired Mann–Whitney U-test. The cutoff value was set as 0.1, α = 0.05, 1-β = 0.8, and the sample size was 1:1. As result, the sample size should be more 102 cases, 51 cases in each group. Assuming that no more than 3 cases were lost to follow-up, thus, 108 cases were enrolled in total. All statistical data were processed with the Statistical Package for the Social Sciences (SPSS) software version 19.0 (SPSS Inc., Chicago, IL, USA). A two-sided P-value < 0.05 was considered statistically significant.
A total of 108 patients with severe OAB were randomly divided into the intervention group (n = 53) and control group (n = 55). The baseline characteristics of patients are shown in Table 1. There were no significant differences between the two groups regarding age (P = 0.5603), OABSS (P = 0.1831), urgent urination (P = 0.3319), urine (P = 0.1079), nocturia (P = 0.5442), UUI (P = 0.8844), PPBC (P = 0.0864), UDI-6 (P = 0.2872), IIQ-7 (P = 0.6820), PVR (P = 0.5442), type I muscle strength (P = 0.3733), type II muscle strength (P = 0.5787), FSFI (P = 0.6645), sexual desire (P = 0.1972), arousal (P = 0.6450), damp (P = 0.6135), orgasm (P = 0.7858), pain (P = 0.1357), and satisfaction (P = 0.0745). However, significant differences were obtained between the two groups regarding VV (P = 0.7858), Qave (P < 0.0001), Qmax (P = 0.0101), and PFM tension (P = 0.0197).

Table 1. The baseline characteristics of patients.
The primary endpoints were OAB-associated outcomes. The results showed that OABSS, urgent urination, urine, nocturia, UUI, PPBC, UDI-6, and IIQ-7 were significantly decreased after treatment in both groups compared with before treatment, whereas VV, Qave, and Qmax were significantly increased in both groups (Table 2). Notably, the improvements in these indicators in the intervention group were superior to the control group after 6 weeks of treatment. However, apart from OABSS, nocturia, urgent urination, PPBC, VV, Qave, and Qmax, other indicators were not significantly different between groups after 12/14 weeks of treatment (Table 2). There were no significant differences in PVR levels between the two groups after both 6 and 12/14 weeks of treatment (Table 2).

Table 2. Outcomes associated with overactive bladder symptom.
The secondary endpoints were indicators related to PFM function and sexual function. In terms of indicators related to PFM function, we found that type I and type II muscle strengths in both groups were dramatically enhanced after treatment compared to those before treatment, while the PFM tension was significantly weakened (Table 3). Moreover, the improvements in these indicators in the intervention group were all superior to the control group after 6 and 12/14 weeks of treatment (Table 3). In terms of sexual function-associated outcomes, the results revealed that patients in both groups had significant improvements in FSFI, sexual desire, arousal, orgasm, and satisfaction after treatment compared to those before treatment (Table 4). Additionally, the improvement of these indicators was significantly larger in the intervention group than in the control group after 6 weeks of treatment, whereas no significant differences were noted between the groups after 12/14 weeks of treatment (Table 4). However, there was no remarkable difference in vaginal damp and sexual pain after treatment in both groups (Table 4).
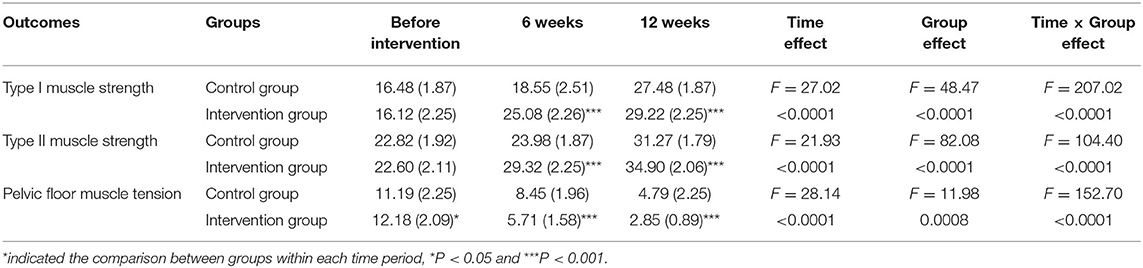
Table 3. Outcomes associated with pelvic floor muscle function.
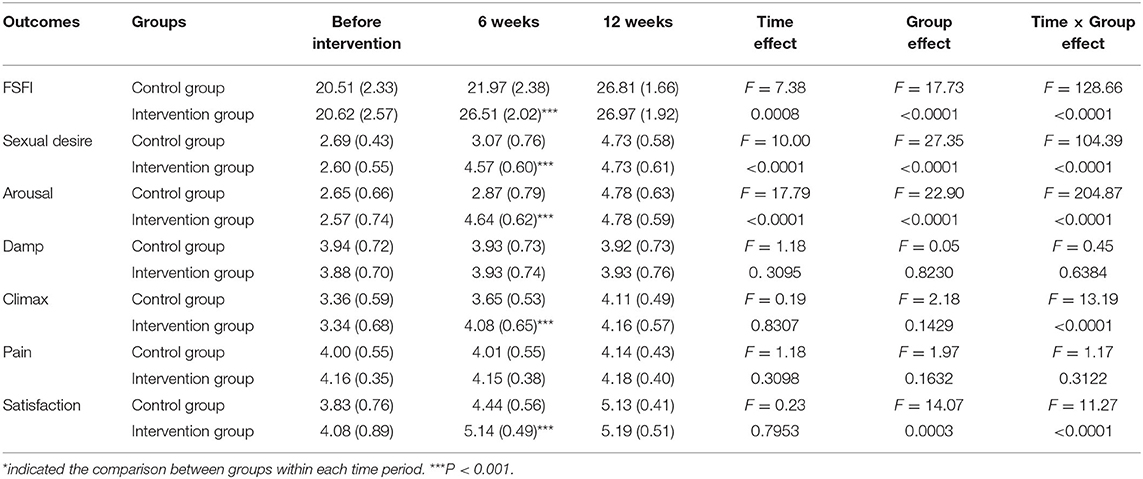
Table 4. Outcomes associated with sexual function.
Bladder training includes lifestyle modification and use of relaxation and distraction techniques to control urinary frequency and urgency (23). It has been revealed that bladder training, including PFMT, is widely used in behavioral and physical therapies for OAB (24). Accumulating evidence has confirmed that PFMT can be combined with other treatment modalities to prevent OAB symptoms (25). However, a recent systematic review shows that the literature regarding the effectiveness of PFMT on improvement of OAB remains inconclusive and heterogeneous (26).
This study aimed to observe the efficacy of Yun-type optimized pelvic floor training therapy on the improvement of OAB and sexual function, to provide guidance for the treatment of severe OAB. By comparing the clinical efficacy of Yun-type optimized pelvic floor training combined with solifenacin vs. solifenacin alone for patients with severe OAB, we found that the OAB-associated outcomes (OABSS, urgent urination, urine, nocturia, UUI, PPBC, UDI-6, IIQ-7, VV, Qave, and Qmax), indicators related to PFM function (type I and type II muscle strength and PFM tension), and sexual function-associated indicators (FSFI, sexual desire, arousal, orgasm, and satisfaction) were significantly improved in both intervention groups. The improvements of these indicators in the intervention group were superior to the control group after 6 weeks of treatment. Moreover, improvements in OAB-associated outcomes (OABSS, nocturia, urgent urination, PPBC, VV, Qave, and Qmax), and PFM function-associated outcomes (type I and type II muscle strength and PFM tension) were also superior in the intervention group than the control group after 12/14 weeks of treatment. Other indicators did not exhibit significant differences between the two groups. These data merit further discussion.
Yun-type optimized pelvic floor training therapy combines professional and scientific PFMT with fashionable and sexy dance. Using this therapy, the groin, pelvic floor, perineum, waist, abdomen, chest, and arms can be exercised. The most prominent characteristic of this therapy is exercises involving the waist, abdomen, hip, and leg. Various groin and leg exercises can produce different weight training effects on PFM groups. In a previous study, dance training was found to significantly improve symptoms in patients with fibromyalgia, including reduced pain and improved functional capacity, QoL, and self-esteem (27). An et al. confirmed that belly dancing can improve the clinical symptoms of middle-aged women with urinary incontinence by increasing the vaginal pressure and strengthening the adductor muscle (28). Moreover, it is reported that an intervention involving pelvic muscle exercise can improve the symptoms of urinary incontinence by increasing the maximum pressure and duration of the PFM contraction (29). Although the efficacy of PFMT in patients with OAB has been studied, inconsistent results have been reported (25, 30). In this study, the following reasons might be responsible for the better clinical efficacy of Yun-type optimized pelvic floor training therapy for the improvement of OAB symptoms: (1) hip training could cause PFM contraction, thereby inhibiting excessive detrusor activity; (2) relaxation of the internal and external urethral sphincters could be inhibited by contraction of the PFM group, thus inhibiting urination; (3) this therapy could improve the associated mental disorders caused by pelvic floor dysfunction; and (4) groin training could increase groin flexibility and vaginal control, as well as further improve the FSFI.
The effectiveness of solifenacin in patients with OAB has already been well-illustrated. It has been reported that solifenacin was efficacious and well-tolerated in patients with OAB, and this treatment could improve QoL in patients (31). Nazir et al. demonstrated that the efficacy of solifenacin was similar to other antimuscarinics for OAB, but it had a lower risk of dry mouth (32). However, drug therapy alone does not completely relieve symptoms in most patients and is often accompanied by adverse effects. Increasing evidence has revealed that patients with OAB may benefit more from a combination of behavioral and drug therapy (33). Burgio et al. revealed that the combination of behavioral and drug therapies showed greater improvements in OAB symptoms than drug therapy alone and that it is reasonable to begin with behavioral therapy alone when using a stepped approach (34). The combination therapy may be more effective in improving frequency, urine output, incontinence and symptom distress (35, 36). In this study, patients in the intervention group experienced additional improvements in the OAB symptoms, PFM function, and sexual function compared to those in the control group. These results suggest that addition of Yun-type optimized pelvic floor training therapy to traditional drug therapies could better benefit women with severe OAB and SD. Moreover, the inclusion of younger women resulted in better compliance to the Yun-type optimized pelvic floor training therapy, which could improve confidence in women and subsequently yield benefits on SD.
Several limitations of this study should be mentioned: Firstly, the age range of patients was narrow, and we did not conduct stratified analyses based on patient characteristics owing to the small number of included patients. Secondly, the number of adverse events was lower than expected, but this was not recorded in this study. Thirdly, the follow-up time was short. Lastly, the analyses in this study were based on short-term interventions. More randomized controlled trials with larger sample sizes and long-term interventions should be performed to explore the clinical application of Yun-type optimized pelvic floor training for middle-aged women with severe OAB.
In conclusion, our findings reveal that the use of Yun-type optimized pelvic floor training may yield additional benefits when combined with solifenacin for severe OAB and sexual function in middle-aged women. A combination of Yun-type optimized pelvic floor training with traditional drug therapies can improve clinical outcomes of severe OAB. This study will be helpful for the treatment of this disease.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Written informed consent was obtained from all participants, and the protocol was reviewed and approved by the Ethics Committee of the Shanghai Fifth People's Hospital Affiliated to Fudan University (No. 2017-041). The clinical trial registration was ChiCTR-INR-17012189.
YW, GS, and CS conceived and designed the research. CS, DZ, and YW participated in the acquisition of data. CS and WY analyzed and interpreted the data. YW, CS, and WY designed the study and performed the statistical analysis. GS participated in obtaining funding. CS, DZ, and WJ drafted the manuscript, conceived the study, and participated in its design and coordination. YW and GS revised the manuscript for important intellectual content. All authors contributed to the article and approved the submitted version.
This work was supported by the Shanghai Key Medical Specialty Program (Program No. ZK2019A03), Subject of Shanghai Municipal Health Committee (Program No. 201940006), and the scientific research project was funded by the Fifth People's Hospital of Shanghai, Fudan University (Program No. 2019WYZT02). The role of the funders is financially supporting this paper.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fsurg.2021.670123/full#supplementary-material
OAB, overactive bladder; QoL, quality of life; UUI, urgency urinary incontinence; SD, sexual dysfunction; PFM, pelvic floor muscle; PFMT, pelvic floor muscle training; OABSS, overactive symptom bladder score; FSFI, female sexual function index; PVR, post-voiding residual; PPBC, patient's perception of bladder condition; UDI-6, urogenital distress inventory-6; IIQ-7, incontinence impact questionnaire-7; VV, voiding volume; Qave, average flow rate; Qmax, maximum flow rate; PVR, postvoid residual urine volume; SPSS, Statistical Package for the Social Sciences.
1. Bo K, Fernandes A, Duarte T, Brito L, Ferreira C. Is pelvic floor muscle training effective for symptoms of overactive bladder in women? A Syst Rev Physiother. (2020) 106:65–76. doi: 10.1016/j.physio.2019.08.011
2. Reisch R. Interventions for overactive bladder: review of pelvic floor muscle training and urgency control strategies. J Women Health Phys Ther. (2020) 44:19–25. doi: 10.1097/JWH.0000000000000148
3. Greenberg DR, Syan R, Young-Lin N, Comiter CV, Enemchukwu E. Outcomes of sacral nerve stimulation for treatment of refractory overactive bladder among octogenarians. Neuro Technol Neural Inter. (2019) 22:738–44. doi: 10.1111/ner.12981
4. Scaldazza CV, Morosetti C, Giampieretti R, Lorenzetti R, Baroni M. Percutaneous tibial nerve stimulation versus electrical stimulation with pelvic floor muscle training for overactive bladder syndrome in women: results of a randomized controlled study. Int Braz J. (2017) 43:121–6. doi: 10.1590/s1677-5538.ibju.2015.0719
5. Stewart W, Van Rooyen J, Cundiff G, Abrams P, Herzog A, Corey R, et al. Prevalence and burden of overactive bladder in the United States. World J Urol. (2003) 20:327–36. doi: 10.1007/s00345-002-0301-4
6. Coyne KS, Sexton CC, Irwin DE, Kopp ZS, Kelleher CJ, Milsom I. The impact of overactive bladder, incontinence and other lower urinary tract symptoms on quality of life, work productivity, sexuality and emotional well-being in men and women: results from the EPIC study. BJU Int. (2008) 101:1388–95. doi: 10.1111/j.1464-410X.2008.07601.x
7. Benner JS, Becker R, Fanning K, Jumadilova Z, Bavendam T, Brubaker L, et al. Bother related to bladder control and health care seeking behavior in adults in the United States. J Urol. (2009) 181:2591–8. doi: 10.1016/j.juro.2009.02.018
8. Ganz ML, Smalarz AM, Krupski TL, Anger JT, Hu JC, Wittrup-Jensen KU, et al. Economic costs of overactive bladder in the United States. Urology. (2010) 75: 526–32. e518. doi: 10.1016/j.urology.2009.06.096
9. Cipullo LM, Cosimato C, Filippelli A, Conti V, Izzo V, Zullo F, et al. Pharmacological approach to overactive bladder and urge urinary incontinence in women: an overview. Eur J Obstetr Gynecol Repr Biol. (2014) 174:27–34. doi: 10.1016/j.ejogrb.2013.12.024
10. Maman K, Aballea S, Nazir J, Desroziers K, Neine M.-E., et al. Comparative efficacy and safety of medical treatments for the management of overactive bladder: a systematic literature review and mixed treatment comparison. Eur Urol. (2014) 65:755–65. doi: 10.1016/j.eururo.2013.11.010
11. Rizvi RM, Chughtai NG, Kapadia N. Effects of bladder training and pelvic floor muscle training in female patients with overactive bladder syndrome: a randomized controlled trial. Urol Int. (2018) 100:420–7. doi: 10.1159/000488769
12. Petros PE, Ulmsten UI. An integral theory of female urinary incontinence. Experimental and clinical considerations. Acta Obstet Gynecol Scand Suppl. (1990) 153:7–31. doi: 10.1111/j.1600-0412.1990.tb08027.x
13. Petros P. A ligamentous explanation for overactive bladder symptoms as defined by international continence society in the female. Cen Eur J Urol. (2018) 71:105–7. doi: 10.5173/ceju.2017.1597
14. Petros P. Understanding the mechanics of closure is key to optimal midurethral sling technique. Int Urogynecol J. (2021) 32:39–45. doi: 10.1007/s00192-020-04533-9
15. Bykoviene L, Kubilius R, Aniuliene R, Bartuseviciene E, Bartusevicius A. Pelvic floor muscle training with or without tibial nerve stimulation and lifestyle changes have comparable effects on the overactive bladder. A randomized clinical trial. Urol J. (2018) 15:186–92. doi: 10.22037/uj.v0i0.4169
16. Dumoulin C, Cacciari LP, Hay-Smith EJC. Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochr Database Syst Rev. (2018) 10:CD005654. doi: 10.1002/14651858.CD005654
17. Fitz F, Sartori M, Girão MJ, Castro R. Pelvic floor muscle training for overactive bladder symptoms–a prospective study. Rev Assoc Méd Bras. (2017) 63:1032–8. doi: 10.1590/1806-9282.63.12.1032
18. Wadie BS. Management of refractory OAB in the non-neurogenic patient. Curr Urol Rep. (2014) 15:438. doi: 10.1007/s11934-014-0438-x
19. Wang Y, Shi C, Wang Y, Wang X, Zhang J, Tu M, et al. Solifenacin combined with optimized pelvic floor training of YUN in treating severe female overactive bladder: a prospective randomized controlled trial. Chin J New Drug Clin Remed. (2017) 36:657–662. doi: 10.14109/j.cnki.xyylc.2017.11.007
20. Xu Y, Zhu L, Wang Y, Shi C. Effect of modified pelvic floor muscle training on patients with stress urinary incontinence. Nurs Prac Res. (2018) 15:88–9. doi: 10.3969/j.issn.1672-9676.2018.22.036
21. Jiao W, Shi C, He J, Wu D, Shi G, Wang Y. Yun's optimized pelvic floor training therapy for idiopathic moderate overactive bladder with sexual dysfunction in young and middle-aged women. Nat J Androl Zhong Nan Xue Zhi. (2019) 25:707–12. doi: 10.13263/j.cnki.nja.2019.08.006
22. Oleksy Ł, Wojciechowska M, Mika A, Antos E, Bylina D, Kielnar R, et al. Normative values for Glazer protocol in the evaluation of pelvic floor muscle bioelectrical activity. Medicine. (2020) 99:e19060. doi: 10.1097/MD.0000000000019060
23. Burgio KL, Locher JL, Goode PS. Combined behavioral and drug therapy for urge incontinence in older women. J Am Geriatr Soc. (2000) 48:370–4. doi: 10.1111/j.1532-5415.2000.tb04692.x
24. Park S-H, Lee JH, Berek JS, Hu MC-T. Auranofin displays anticancer activity against ovarian cancer cells through FOXO3 activation independent of p53. Int J Oncol. (2014) 45:1691–8. doi: 10.3892/ijo.2014.2579
25. Burgio KL. Update on behavioral and physical therapies for incontinence and overactive bladder: the role of pelvic floor muscle training. Curr Urol Rep. (2013) 14:457–64. doi: 10.1007/s11934-013-0358-1
26. Monteiro S, Riccetto C, Araújo A, Galo L, Brito N, Botelho S. Efficacy of pelvic floor muscle training in women with overactive bladder syndrome: a systematic review. Int Urogynecol J. (2018) 29:1565–73. doi: 10.1007/s00192-018-3602-x
27. López-Rodríguez MM, Fernández-Martínez M, Matarán-Peñarrocha GA, Rodríguez-Ferrer ME, Granados Gámez G, Aguilar Ferrándiz E. Efectividad de la biodanza acuática sobre la calidad del sueño, la ansiedad y otros síntomas en pacientes con fibromialgia [Effectiveness of aquatic biodance on sleep quality, anxiety and other symptoms in patients with fibromyalgia]. Med Clin (Barc). (2013) 141:471–8. doi: 10.1016/j.medcli.2012.09.036
28. An S-Y, Kim S-S, Han G. Effect of belly dancing on urinary incontinence-related muscles and vaginal pressure in middle-aged women. J Phys Ther Sci. (2017) 29:384–6. doi: 10.1589/jpts.29.384
29. Radzimińska A, Stra̧czyńska A, Weber-Rajek M, Styczyńska H, Strojek K, Piekorz Z. The impact of pelvic floor muscle training on the quality of life of women with urinary incontinence: a systematic literature review. Clin Interv Aging. (2018) 13:957–65. doi: 10.2147/CIA.S160057
30. Betschart C, Mol SE, Lütolf-Keller B, Fink D, Perucchini D, Scheiner D. Pelvic floor muscle training for urinary incontinence: a comparison of outcomes in premenopausal versus postmenopausal women. Female Pelvic Med Reconstr Surg. (2013) 19:219–24. doi: 10.1097/SPV.0b013e31829950e5
31. Brunton S, Kuritzky L. Recent developments in the management of overactive bladder: focus on the efficacy and tolerability of once daily solifenacin succinate 5 mg. Curr Med Res Opin. (2005) 21:71–80. doi: 10.1185/030079904X20268
32. Nazir J, Kelleher C, Aballea S, Maman K, Hakimi Z, Mankowski C, et al. Comparative efficacy and tolerability of solifenacin 5 mg/day versus other oral antimuscarinic agents in overactive bladder: a systematic literature review and network meta-analysis. Neurourol Urody. (2018) 37:986–96. doi: 10.1002/nau.23413
33. Klutke CG, Burgio KL, Wyman JF, Guan Z, Sun F, Berriman S, et al. Combined effects of behavioral intervention and tolterodine in patients dissatisfied with overactive bladder medication. J Urol. (2009) 181:2599–607. doi: 10.1016/j.juro.2009.02.028
34. Burgio KL, Kraus SR, Johnson TM, Markland AD, Vaughan CP, Li P, et al. Effectiveness of combined behavioral and drug therapy for overactive bladder symptoms in men: a randomized clinical trial. JAMA Int Med. (2020) 180:411–9. doi: 10.1001/jamainternmed.2019.6398
35. Wille S, Sobottka A, Heidenreich A, Hofmann R. Pelvic floor exercises, electrical stimulation and biofeedback after radical prostatectomy: results of a prospective randomized trial. J Urol. (2003) 170:490–3. doi: 10.1097/01.ju.0000076141.33973.75
Keywords: overactive bladder, yun-type pelvic floor optimal training, pelvic floor muscle training, drug therapy, randomized clinical trial
Citation: Shi C, Zhou D, Yu W, Jiao W, Shi G and Wang Y (2021) Efficacy of Yun-Type Optimized Pelvic Floor Training Therapy for Middle-Aged Women With Severe Overactive Bladder: A Randomized Clinical Trial. Front. Surg. 8:670123. doi: 10.3389/fsurg.2021.670123
Received: 25 March 2021; Accepted: 16 June 2021;
Published: 14 July 2021.
Edited by:
Hai-Hong Jiang, First Affiliated Hospital of Wenzhou Medical University, ChinaReviewed by:
Lv Jianwei, Shanghai JiaoTong University, ChinaCopyright © 2021 Shi, Zhou, Yu, Jiao, Shi and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yangyun Wang, d2FuZ3lhbmd5dW4xOTg2QDE2My5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.