 Ester Marín-Conesa1
Ester Marín-Conesa1 María Dolores Grima-Murcia
María Dolores Grima-Murcia María Luisa Sánchez-Ferrer
María Luisa Sánchez-Ferrer
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
TECHNOLOGY AND CODE article
Front. Surg., 09 June 2021
Sec. Obstetrics and Gynecological Surgery
Volume 8 - 2021 | https://doi.org/10.3389/fsurg.2021.643611
Introduction: Laparoscopic surgery is an increasingly used technique, but it requires a high degree of learning, and communication between the operating room crew is considerably difficult. The use of eye tracking has been proposed as a didactic and evaluation tool in several settings, including in laparoscopy in simulators.
Objectives: This study aimed to evaluate the usefulness of the use of eye tracking systems (Tobii glasses 2) in laparoscopic surgery as a didactic and assessment tool to improve communication in the operating room and improve patients' security.
Methodology: An anonymous survey was sent to the students and medical teachers of a faculty of medicine and practicing doctors and residents. The message contained an explanation about the use of the Tobii glasses, a link to watch the video showing its use in a laparoscopic surgery, and the survey to complete after watching the video.
Results: The survey was answered by 113 participants (51.3% medical students, 27.4% medical teachers, 18.6% practicing doctors, and 2.7% medicine residents). Eighty-three percent agreed with the usefulness of the “Tobii glasses” in the operating room for improving communication between the main surgeon and the assistant, for learning complex surgery techniques, for obtaining didactic videos, and for indicating anatomical structures. The item scored worst was the price of the glasses.
Conclusions: It is possible to record and project expert gaze patterns in the operating room in real time using the Tobii glasses. This device allows improving communication among the surgical crew and the learning of residents and also improving the security of surgical patients.
Laparoscopy is a surgical technique increasingly used due to the advantages it offers, such as the fast recovery of patients. However, it presents as disadvantages the requirement of great technical learning and the acquisition of psychomotor skills that are different from those used in open surgery (1). Besides, during the performance of laparoscopic surgery, as the surgeon cannot point to the monitor due to wearing a sterile suit and gloves and having to handle the laparoscopic instruments, when he gives verbal instructions, uncertainty may arise about the exact point to which he is referring, which hinders learning and may also be difficult for communication among the various members of the surgical team (2). Likewise, in laparoscopic surgery, the main surgeon often operates the surgical instruments while the assistant controls the laparoscopic camera and other secondary instruments. As a result of this, it is important for the surgical team to focus on the same target in order to proceed efficiently (3). As a consequence of this need for fast and quality learning, new training techniques have been proposed based on gaze control (through the use of eye tracking in real time) for learning in laparoscopic surgery.
Eye tracking (eye movements) has been recorded using stationary cameras or cameras fitted to normal glasses. These glasses can record corneal reflection to track the pupils' position in order to map gaze focusing in the video recording in real time. Eye tracking is been used in a wide range of areas, such as market research and advertising testing, the design of web pages, eye control for accessibility (very useful for quadriplegics, for example), psychology and vision research, gaze interaction and car assistant systems and medical research, and in diagnostics and rehabilitation (4). On the other hand, the importance of the strategic behavior of the gaze in the optimization of motor control has been shown (5). Improved learning has been demonstrated when students are shown the exact points on which an expert stops his gaze, which means to follow their gaze pattern, which has been achieved through the use of eye-tracking technology (6, 7). Regarding the health field, we can find its application in many fields, such as in radiology. Dempere-Marco et al. (8) trained novices by showing them the visual search pattern that expert radiologists had carried out during the evaluation of several CTs, improving their accuracy.
O'Meara et al. (9) used eye tracking to train nursing and paramedicine students while facing emergency simulations, obtaining an improvement in student learning.
Many studies (10–13) have analyzed the gaze patterns of experts and novices and showed that there are differences between both gaze patterns and pupillometry data. Studies (11, 13) that use these differences between beginners and experts as a didactic tool to improve the learning of novices and as a method to evaluate them have been carried out. In surgery, Di Stasi et al. (14) concluded that the metrics of the gaze (entropy of the gaze and speed) were a valid and reliable index for evaluating a workload.
In laparoscopy, eye tracking has been proposed as a didactic and evaluation tool (15). Most of these studies were performed in simulated laparoscopic surgery (Supplementary Table 1). Chetwood et al. (2) conducted an interesting research on laparoscopic simulators using the Tobii 1750, 17-in. computer monitor device (Tobii Technology AB, Danderyd, Sweden). The subjects performed the laparoscopic task, receiving instructions from an expert at the same time, which were different according to the group. Three groups were formed with different instructions: (1) verbal queues, (2) a cursor reflecting the supervisor's eye gaze, and (3) both verbal cue and eye gaze. Completion times and the number of errors were significantly reduced when the eye gaze instruction was employed. In addition, the time taken for the subject to correctly focus on the target (latency) was significantly reduced.
We found three studies conducted during real laparoscopy, but the analysis of eye tracking was done after the surgical procedure (16–18). We only found one study during real laparoscopy (12) where the authors published their own experiences with performing eye tracking to improve surgery training. Our objectives were to record a video in a real laparoscopy using Tobii glasses and to evaluate with a Likert-type scale whether this didactic tool could improve the learning of students, residents, and practicing doctors through a survey.
We conducted an observational prospective study in April 2017. This study was approved by the Ethics Research Committee of our university and our clinical university hospital (No. 2015-10-5-HCUVA, approved October 26, 2015). Written informed consent was obtained from all participants. All authors have reviewed this manuscript and approved its submission.
Tobii glasses 2 were tested in a real laparoscopic procedure at a university clinical hospital. The operation consisted of right adnexectomy by laparoscopy for ovarian cyst in a postmenopausal patient. A video of this procedure was recorded (see Supplementary Video 1).
The device used in the video was Tobii glasses 2 (Figure 1). It is a video-based eye-tracking system that uses infrared light. It is integrated in normal glasses (weight, 45 g), with a horizontal visual field of 160 degrees. The total battery time is 120 min, and the software runs on a Windows 8/8.1 or Windows 7 or 8/8.1 tablet. The connection of the glasses with the tablet is through Wi-Fi. It has a data transfer speed of 50 Hz. Through this connection, images and sounds are transmitted to any computer (with the indicated software) with a delay of <1 s. In addition, it allows free movements of the subject that carries it. The system must be calibrated separately for each participant, with the participants having to look at a calibration card for several seconds. After this, it is possible to start recording the subject's vision through the Tobii glasses. The visual field of the subject is recorded by an HD camera located at the front of the Tobii glasses; at the same time, the areas on which the subject fixes his/her gaze are detected (foveal vision is tracked). During the real-time visualization, a red circle is observed, which represents the foveal vision of the subject, on the recording of the visual field. The ocular tracking performed can be seen both in real time and later (as it is recorded).
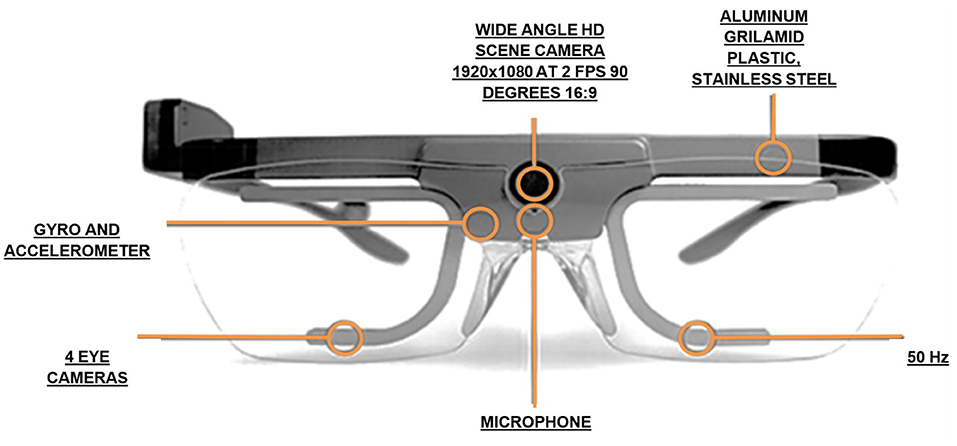
Figure 1. Tobii glasses 2 (technical details).
The participants were students and medical teachers of a faculty of medicine and practicing doctors and residents of a university clinical hospital. All were invited through their university e-mails to complete an anonymous online survey about a laparoscopic procedure video showing the use of eye-tracking technology to objectively measure the usefulness of this instrument.
The survey had two parts. The first one consisted of five general items to collect epidemiological data. The second part contained nine items to value different aspects of the video using the Tobii glasses. In this part, a Likert-type scale was used with five possible answers: “Completely agree,” “Agree,” “Undecided,” “Disagree,” and “Completely disagree” (Table 1).
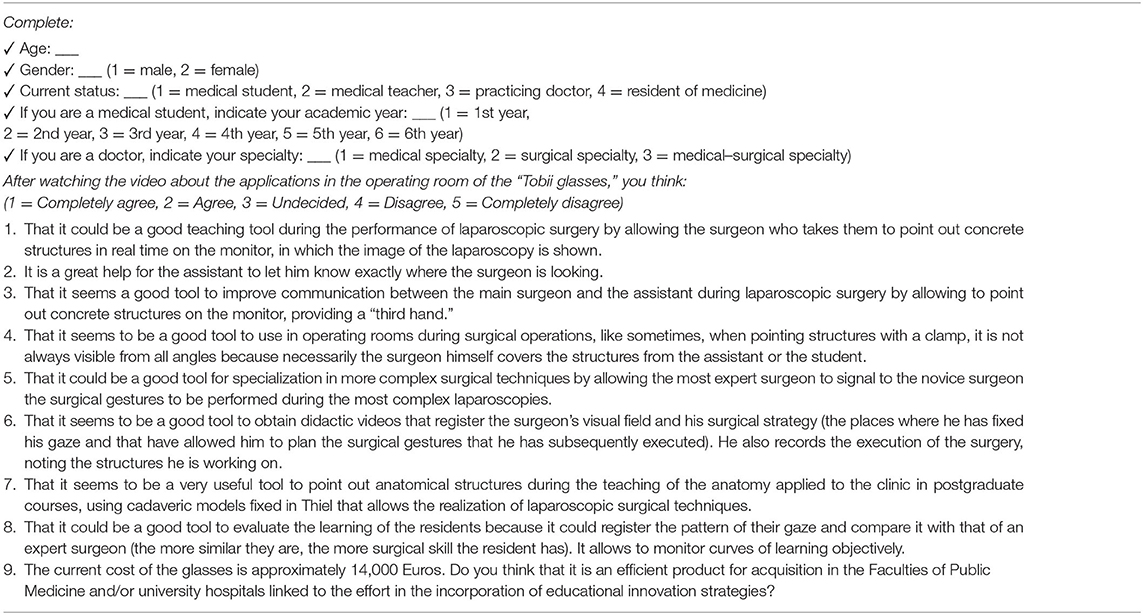
Table 1. Survey on laparoscopic applications of Tobii glasses.
The survey was sent to the participants through the computer application of our university. The survey message contained an explanation about the use of the Tobii glasses, a link to watch the video showing its use in laparoscopic surgery, and the survey to complete after watching the video. This same application was used to analyze the data. Non-parametric range, median, or range-based procedures were used for analyzing these data as distribution-free methods such as tabulations, frequencies, contingency tables, and chi-square statistics. The results were presented as bar charts.
A total of 113 surveys were returned. The participants were 51.3% medical students, 27.4% medical teachers, 18.6% practicing doctors, and 2.7% medical residents. Figure 2 shows a graph in which the responses “Completely agree” and “Agree” have been grouped as positive responses and “Disagree” and “Strongly disagree” as negative responses. The results have been described independently of the status (medical student, teacher, practicing physician, or residents). The positive responses grouped into the different items were 88.5% for item 1, 86.8% for item 2, 90.3% for item 3, 85.8% for item 4, 83.2% for item 5, 83.2% for item 6, 84% for item 7, 71.7% for item 8, and 52.2% for item 9. We can see that the overall results of the survey are very satisfactory.
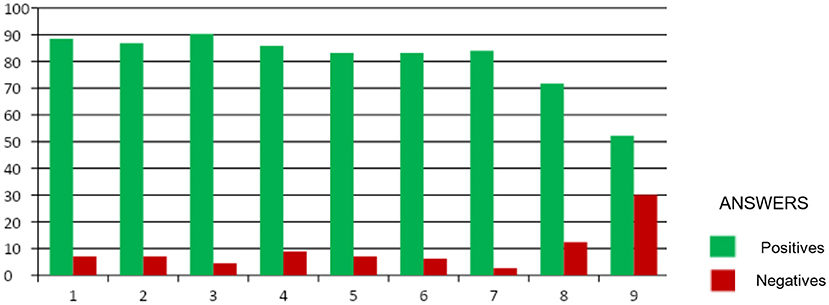
Figure 2. Overall response to the different items of the survey (positive: “Completely agree” and “Agree”; negative: “Disagree” and “Completely disagree”).
The items for questions 1–7 have received satisfactory answers above 83%, being the best rated. It deals with questions regarding the usefulness of the Tobii glasses in the operating room in the teaching of residents, in the improvement of communication between the main surgeon and the assistant, providing a “third hand,” in the learning of techniques for complex surgeries, and in obtaining didactic videos and indicating anatomical structures in real laparoscopy. On the other hand, the item with the worst score was number 9, with 52.2% positive responses, which was in relation to the price of these glasses.
Our group is a pioneer in the use of eye tracking in real time during a real laparoscopy, which allowed the surgeon to use his/her gaze as a pointer, thanks to the option of projecting the foveal fixation of the expert surgeon in real time, thus being able to indicate the exact point to which he/she is referring without endangering the sterility of the surgical field. This sets the possibility of learning based on gaze control in the surgery room at the same time that the surgeon operates, improving the communication among the different members of the surgical team and, consequently, the students' learning in real time, not delayed as previous studies had done. Our study shows that Tobii glasses 2 are considered a good tool for pointing out structures during the surgery, giving more precise “visual” instructions to the students, improving the precision of the novice surgeon and minimizing mistakes, and consequently improving the safety of the surgical patient, avoiding learning of complex surgical techniques. They are also a good didactic tool because they allow carrying out the learning based on gaze control, as much as with videos of the surgery with the gaze patterns of the surgeon registered during the real surgery, like being in the same operating room, thanks to the instant projection of foveal fixation. This possibility of pointing out with higher precision is strongly important to improve precision during surgery. Pucket and Baronia (18) carried out the first study that recorded the eye gaze patterns of an expert and a novice at the same time during live surgery. They described the correlation in the visual attitudes and movements (~85%) between the expert and the novice. Another study (9) described the authors' experiences with performing eye tracking for improving surgery training in the operating room. In our knowledge, no survey about the use of Tobii glasses during real surgery has been reported.
Video libraries have been used as a valid model for learning in laparoscopic surgery and orthopedics. In addition, it has been proposed to record videos from the head of the surgeon in order to capture their visual field. This has been attempted with the “Google Glass.” Adventure sports cameras provide high-quality videos, and their use has also been proposed (19). However, these videos do not have the visual key points during the performance of a surgery printed in their image. With the recent advances in the da Vinci “dual-console” systems and remote collaborative surgery, the demand to accurately represent (20) the point of view on the surgical screen is increasing. This need can be met by a novice's use of gaze-contingent technology and can improve the communication modalities available for surgeons of all grades (2). This is the main advantage of the application of eye-tracking technology in real time. For this reason, studies that explore the didactic potential of eye tracking in surgery have been carried out. In the literature review, we have found several studies (2, 5, 20–22) that analyzed the impact of the use of eye tracking in novices' learning. Three of them were performed in a laparoscopic surgical simulator. These studies (2, 22, 23) show that training based on visual control (watching where the expert surgeon fixes his eyes on) has better results than seeing only the recording from the surgeon's perspective (21) or receiving verbal instructions (2, 24). However, although the results of these studies are relevant, all were limited by the fact that they were performed in a simulator. Wilson et al. (22) reported that observation patterns obtained from the expert surgeon should be recorded during a real operation and then overhead on the registered surgical video, which would provide additional information to beginning surgeons about where the expert surgeon is focusing his/her attention on during every step of the operation. Besides, other studies (3, 10, 12, 17) analyzed the gaze patterns of surgeons and novices in the real operating rooms. Atkins et al. (12) used a “remote” eye tracker—which means a future analysis of the gaze, not in real time during surgery—and observed that there were differences between the gaze patterns of experts and residents.
On the other hand, there are studies that have suggested the use of eye tracking (ocular metrics) to assess an objective evaluation in medical (24, 25) and surgical education (2, 17, 26, 27) and also in high-stakes assessment analogously to other validated objective evaluations, such as the Operative Performance Rating System, the Objective Structured Assessment of Technical Skills (OSATS) (3), or the Global Operative Assessment of Laparoscopic Skills (GOALS) (17). Eye tracking could serve to evaluate skills because this technology allows perceiving not only the pattern of gaze but also the frequency of fixation and the time of permanence, which are used as measures of the importance of the perceived stimulus, as well as pupil dilation, a marker of the effort and concentration of the subject (3, 10, 12). Richstone et al. (15) showed that ocular metrics such as pupil size, blink rate, and fixation rate could be used as objective measures of surgical skill because they were able to classify experts and novices with great precision. The results of the study of Erridge et al. (16) suggested that experts focused on significant stimuli, had increased concentration, and had reduced mental workload. But also because the gaze patterns were different, as we have seen between experts and novices, so students could be assessed by checking that their patterns are more and more similar to those of the experts (17). Dynamic areas of interest reflected that the expert's eye gaze was able to differentiate expertise and the presence of unexpected adverse events (28).
The main limitation of our study is that the evaluation of this tool has been through answers of a survey. The ideal for future research would be to demonstrate this usefulness in terms of ease, speed, and safety through a randomized clinical trial where the usefulness of learning with and without this device is evaluated. Ideally, we would use the Tobii glasses 3 (https://www.tobiipro.com/es/products/tobii-pro-glasses-3/), which is the most modern version, not available when this study was carried out. Another aspect is that the total battery time is 120 min, and it is possible that an operation lasts longer than 120 min. In this case, it is possible to have another battery and change it during the procedure.
The results of the current study, with high scores on the survey, allow us to verify the positive assessment of the usefulness of this eye-tracking device in the field of laparoscopic surgery as an objective learning tool for residents, improving their precision, thanks to the visual instructions, with the foveal vision of the surgeon projected in real time as a “pointer” controlled by sight. This technology minimizes the risk of mistakes, improves communication among members of the operating room, and also improves the learning of complex surgical techniques, resulting in increased patient safety during laparoscopy. It is a good didactic tool because it allows carrying out the learning based on gaze control, as much as with videos of the surgery with the gaze pattern of the surgeon registered during the real surgery, like being in the same operating room, thanks to the instant projection of foveal fixation. Finally, it could be a good tool to evaluate the residents' learning in an objective way, comparing the gaze patterns of experts and novices (the more similar, the better their surgical skill).
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by the Ethics Research Committee of our University and our Clinical University Hospital (No. 2015-10-5-HCUVA approved October 26, 2015). The patients/participants provided their written informed consent to participate in this study.
MS-F performed the laparoscopic procedure, wore the Tobii glasses during surgery, and revised the manuscript. FS-F and MG-M calibrated the device. EM-C wrote the manuscript and conducted the bibliographic research. All authors approved the final version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors acknowledge the Miguel Hernandez University for allowing us to use the Tobii glasses, especially to Eduardo Fernandez, Head of the Bioengineering Institute of the Miguel Hernandez University, Alicante, Spain.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fsurg.2021.643611/full#supplementary-material
Supplementary Table 1. Analysis of studies using eye-tracking systems in laparoscopic surgery.
Supplementary Video 1. Link to the video of laparoscopic surgery in which the foveal fixation of the surgeon is marked by the Tobii glasses: https://youtu.be/9wTrB8Ssoec.
1. Garry J, Casey K, Cole TK, Regensburg A, McElroy C, Schneider E, et al. A pilot study of eye-tracking devices in intensive care. Surgery. (2016) 159:938–44. doi: 10.1016/j.surg.2015.08.012
2. Chetwood ASA, Kwok K-W, Sun L-W, Mylonas GP, Clark J, Darzi A, et al. Collaborative eye tracking: a potential training tool in laparoscopic surgery. Surg Endosc. (2012) 26:2003–9. doi: 10.1007/s00464-011-2143-x
3. Tien T, Pucher PH, Sodergren MH, Sriskandarajah K, Yang G-Z, Darzi A. Eye tracking for skills assessment and training: a systematic review. J Surg Res. (2014) 191:169–78. doi: 10.1016/j.jss.2014.04.032
4. Drewes H. Eye Gaze Tracking for Human Computer Interaction. (2010). Available online at: https://edoc.ub.uni-muenchen.de/11591/
5. Wilson M, McGrath J, Vine S, Brewer J, Defriend D, Masters R. Psychomotor control in a virtual laparoscopic surgery training environment: gaze control parameters differentiate novices from experts. Surg Endosc. (2010) 24:2458–64. doi: 10.1007/s00464-010-0986-1
6. Sadasivan S, Greenstein JS, Gramopadhye AK, Duchowski A. Use of eye movements as feedforward training for a synthetic aircraft inspection task. In: CHI 2005: Technology, Safety, Community: Conference Proceedings - Conference on Human Factors in Computing Systems. (2005). p. 141–9.
7. Vine S. Quiet eye training improves performance and protects against stress in a golf putting task. In: British Association of Sport and Exercise Science Annual Conference Book of Abstracts. (2012). p. 1–8.
8. Dempere-Marco L, Hu X-P, MacDonald SLS, Ellis SM, Hansell DM, Yang G-Z. The use of visual search for knowledge gathering in image decision support. IEEE Trans Med Imaging. (2002) 21:741–54. doi: 10.1109/TMI.2002.801153
9. O'Meara P, Munro G, Williams B, Cooper S, Bogossian F, Ross L, et al. Developing situation awareness amongst nursing and paramedicine students utilizing eye tracking technology and video debriefing techniques: a proof of concept paper. Int Emerg Nurs. (2015) 23:94–9. doi: 10.1016/j.ienj.2014.11.001
10. Zheng B, Jiang X, Atkins MS. Detection of changes in surgical difficulty: evidence from pupil responses. Surg Innov. (2015) 22:629–35. doi: 10.1177/1553350615573582
11. Szulewski A, Roth N, Howes D. The use of task-evoked pupillary response as an objective measure of cognitive load in novices and trained physicians: a new tool for the assessment of expertise. Acad Med. (2015) 90:981–7. doi: 10.1097/ACM.0000000000000677
12. Atkins MS, Tien G, Khan RSA, Meneghetti A, Zheng B. What do surgeons see: capturing and synchronizing eye gaze for surgery applications. Surg Innov. (2013) 20:241–8. doi: 10.1177/1553350612449075
13. Harrison TK, Kim TE, Kou A, Shum C, Mariano ER, Howard SK. Feasibility of eye-tracking technology to quantify expertise in ultrasound-guided regional anesthesia. J Anesth. (2016) 30:530–3. doi: 10.1007/s00540-016-2157-6
14. Di Stasi LL, Diaz-Piedra C, Rieiro H, Sánchez Carrión JM, Martin Berrido M, Olivares G, et al. Gaze entropy reflects surgical task load. Surg Endosc. (2016) 30:5034–43. doi: 10.1007/s00464-016-4851-8
15. Richstone L, Schwartz MJ, Seideman C, Cadeddu J, Marshall S, Kavoussi LR. Eye metrics as an objective assessment of surgical skill. Ann Surg. (2010) 252:177–82. doi: 10.1097/SLA.0b013e3181e464fb
16. Erridge S, Ashraf H, Purkayastha S, Darzi A, Sodergren MH. Comparison of gaze behaviour of trainee and experienced surgeons during laparoscopic gastric bypass. Br J Surg. (2018) 105:287–94. doi: 10.1002/bjs.10672
17. Khan RSA, Tien G, Atkins MS, Zheng B, Panton ONM, Meneghetti AT. Analysis of eye gaze: do novice surgeons look at the same location as expert surgeons during a laparoscopic operation? Surg Endosc. (2012) 26:3536–40. doi: 10.1007/s00464-012-2400-7
18. Puckett Y, Baronia BC. Technical report of successful deployment of tandem visual tracking during live laparoscopic cholecystectomy between novice and expert surgeon. Cureus. (2016) 8:e791. doi: 10.7759/cureus.791
19. Beard HR, Marquez-Lara AJ, Hamid KS. Using wearable video technology to build a point-of-view surgical education library. JAMA Surg. (2016) 151:771–2. doi: 10.1001/jamasurg.2016.0976
20. Atkins MS, Law B, Atkins MS, Kirkpatrick AE, Lomax AJ MC. Eye gaze patterns differentiate novice and experts in a virtual laparoscopic surgery training environment designing radiology workstations for softcopy reading view project human factors in surgery view project eye gaze patterns differentiate novice and E. In: Duchowski AT, Vertegaal R, editors. P of the Eye Tracking Research and Application Symposium, SAT (2004). p. 41–7.
21. Kocak E, Ober J, Berme N, Melvin WS. Eye motion parameters correlate with level of experience in video-assisted surgery: objective testing of three tasks. J Laparoendosc Adv Surg Tech A. (2005) 15:575–80. doi: 10.1089/lap.2005.15.575
22. Wilson MR, Vine SJ, Bright E, Masters RSW, Defriend D, McGrath JS. Gaze training enhances laparoscopic technical skill acquisition and multi-tasking performance: a randomized, controlled study. Surg Endosc. (2011) 25:3731–9. doi: 10.1007/s00464-011-1802-2
23. Vine SJ, Masters RSW, McGrath JS, Bright E, Wilson MR. Cheating experience: guiding novices to adopt the gaze strategies of experts expedites the learning of technical laparoscopic skills. Surgery. (2012) 152:32–40. doi: 10.1016/j.surg.2012.02.002
24. Sánchez-Ferrer ML, Grima-Murcia MD, Sánchez-Ferrer F, Hernández-Peñalver AI, Fernández-Jover E, Sánchez Del Campo F. Use of eye tracking as an innovative instructional method in surgical human anatomy. J Surg Educ. (2017) 74:668–73. doi: 10.1016/j.jsurg.2016.12.012
25. Grima-Murcia MD, Sanchez-Ferrer F, Ramos-Rincón JM, Fernández E. Use of eye-tracking technology by medical students taking the objective structured clinical examination: descriptive study. J Med Internet Res. (2020) 22:e17719. doi: 10.2196/17719
26. Moorthy K, Munz Y, Sarker SK, Darzi A. Objective assessment of technical skills in surgery. BMJ. (2003) 327:1032–7. doi: 10.1136/bmj.327.7422.1032
27. Jiang X, Zheng B, Atkins MS. Video processing to locate the tooltip position in surgical eye-hand coordination tasks. Surg Innov. (2015) 22:285–93. doi: 10.1177/1553350614541859
Keywords: eye tracking systems, laparoscopic surgery, learning tool, real surgery room, Tobii glasses 2, evaluation tool
Citation: Marín-Conesa E, Sánchez-Ferrer F, Grima-Murcia MD and Sánchez-Ferrer ML (2021) The Application of a System of Eye Tracking in Laparoscopic Surgery: A New Didactic Tool to Visual Instructions. Front. Surg. 8:643611. doi: 10.3389/fsurg.2021.643611
Received: 18 December 2020; Accepted: 29 April 2021;
Published: 09 June 2021.
Edited by:
Enkelejda Kasneci, University of Tübingen, GermanyReviewed by:
Ferdinando Antonio Gulino, Garibaldi Hospital, ItalyCopyright © 2021 Marín-Conesa, Sánchez-Ferrer, Grima-Murcia and Sánchez-Ferrer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María Luisa Sánchez-Ferrer, bWFyaXNhc2FuY2hlekB1bS5lcw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.