 Joshua A. Scheinerman
Joshua A. Scheinerman Jeffrey Jiang
Jeffrey Jiang Stephanie H. Chang
Stephanie H. Chang Travis C. Geraci
Travis C. Geraci Robert J. Cerfolio
Robert J. Cerfolio
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Surg. , 22 February 2021
Sec. Thoracic Surgery
Volume 8 - 2021 | https://doi.org/10.3389/fsurg.2021.597416
This article is part of the Research Topic Cutting Edge Robotic Techniques: From Performance to Teaching to Telemedicine View all 9 articles
While lung cancer remains the most common cause of cancer-related mortality in the United States, surgery for curative intent continues to be a mainstay of therapy. The robotic platform for pulmonary resection for non-small cell lung cancer (NSCLC) has been utilized for more than a decade now. With respect to more localized resections, such as wedge resection or lobectomy, considerable data exist demonstrating shorter length of stay, decreased postoperative pain, improved lymph node dissection, and overall lower complication rate. There are a multitude of technical advantages the robotic approach offers, such as improved optics, natural movement of the operator's hands to control the instruments, and precise identification of tissue planes leading to a more ergonomic and safe dissection. Due to the advantages, the scope of robotic resections is expanding. In this review, we will look at the existing data on extended robotic pulmonary resections, specifically post-induction therapy resection, sleeve lobectomy, and pneumonectomy. Additionally, this review will examine the indications for these more complex resections, as well as review the data and outcomes from other institutions' experience with performing them. Lastly, we will share the strategy and outlook of our own institution with respect to these three types of extended pulmonary resections. Though some controversy remains regarding the use and safety of robotic surgery in these complex pulmonary resections, we hope to shed some light on the existing evidence and evaluate the efficacy and safety for patients with NSCLC.
With nearly a quarter-million lung cancers diagnosed in 2017 in the US, more than 80% of which were non-small cell lung cancer (NSCLC) (1), there is a substantial need for surgical resection for management of disease. In parallel with the growing need for pulmonary resection, there have been significant advances in thoracic minimally invasive surgery (MIS), with nearly 57,000 MIS lobectomies performed from 2002 to 2018, most of which in the latter decade (2). Furthermore, the rate of both video-assisted thoracoscopic surgery (VATS) and robotic thoracic surgery has increased significantly over the last decade. As the field of robotic thoracic surgery continues to develop, the breadth of surgery safely achievable using a robotic platform continues to expand. Complex surgeries with increased adhesions with associated increased risk for bleeding, such as post-induction pulmonary resections, are being performed robotically with more frequency. Other technically complex resections, such as sleeve resection or pneumonectomy, can also be safely completed via a robotic platform. There are numerous tangible advantages to the robotic platform, such as lower overall complication rate, less blood loss, decreased postoperative pain, shorter length of stay, as well as optimized pathologic staging due to a more complete lymph node dissection in comparison to thoracotomy (3). In a large multi-center study with 1,336 robotic lobectomies performed, Cerfolio et al. demonstrates median blood loss of 50 ml, mean operative time of 136 min, and median length of stay of 3 days (4), all of which have improved over the past 2 years (publication pending). Given the benefits of robotic surgery in early-stage NSCLC resection, there is likely a similar benefit of the robotic approach for these extended resections.
The ideal treatment for early-stage NSCLC is complete surgical resection. However, the management increases in complexity for advanced-stage disease. For non-superior sulcus lung cancer with no mediastinal lymph node disease and resectable disease, the standard treatment is surgery, with possible adjuvant systemic therapy and/or radiation depending on the final pathologic stage. Assuming negative pathologic margins, current NCCN guidelines for NSCLC state adjuvant chemo is appropriate for stages IB (high-risk patients), IIA, and IIB. However, for patients with N2 (mediastinal disease), neoadjuvant treatment with chemotherapy or chemoradiation therapy followed by restaging and surgical resection is the standard treatment (5). In 1992, the National Cancer Institute performed a study aimed at evaluating the effect of neoadjuvant chemotherapy on NSCLC. Pass et al. randomized Stage IIIA (N2) disease patients to surgery followed by radiotherapy or neoadjuvant cisplatin/etoposide followed by surgery. Of the 27 patients followed, there was a trend toward improved survival in the neoadjuvant arm, 28.7 months with neoadjuvant vs. 15.6 months. The recurrence rate and disease-free survival also favored the neoadjuvant arm (6). These data are reinforced further by a 2010 Journal of Thoracic Oncology meta-analysis that looked at 13 randomized control trials treating NSCLC patients with neoadjuvant + surgery vs. surgery alone. The data illustrated that neoadjuvant benefited stage III NSCLC patients significantly with respect to comparative survival, with this subgroup analysis of more than 1,500 patients revealing a combined HR = 0.84, p = 0.005 (7) (Table 1).
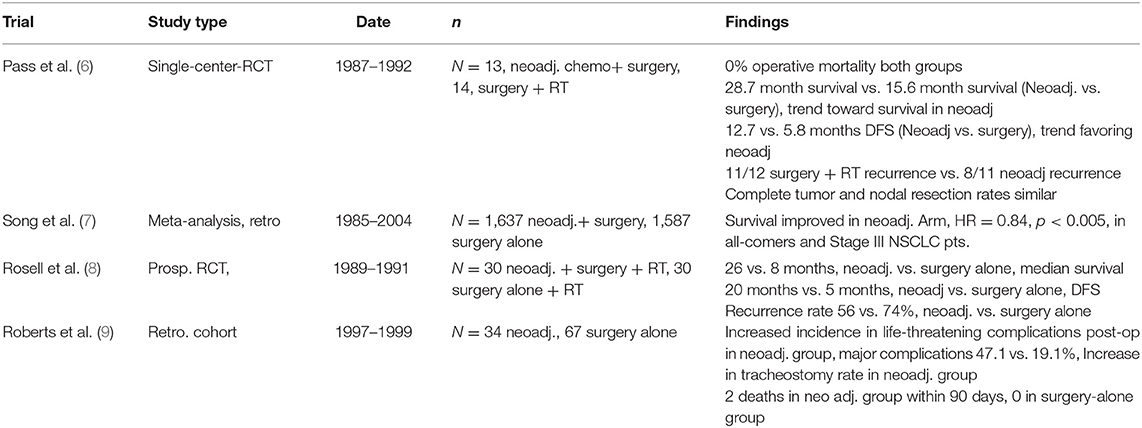
Table 1. Role of neoadjuvant chemotherapy for advanced NSCLC.
Induction therapy for NSCLC poses unique technical challenges for the minimally invasive thoracic surgeon. Dense adhesions and fibrosis in the setting bulky tumors with inflamed lymphadenopathy can create difficult and hazardous dissections. While the initial report in 1994 evaluating the efficacy of induction chemotherapy in stage IIIA disease showed no difference in postoperative mortality between the neoadjuvant vs. upfront surgery arm, there was a high 30-day mortality of 7% in each arm (8). However, there are some data demonstrating increased postoperative 90-day mortality and overall complication rate. Roberts et al. demonstrated increased life-threatening complications (26.5 vs. 6.0%), major complications (47.1 vs. 19.4%), and 90-day mortality (5.9 vs. 0%) in patients who had neoadjuvant treatment vs. upfront surgery, respectively (9).
Some data exist comparing minimally invasive to open resection for NSCLC after induction therapy. Fang et al. demonstrated no significant difference in postoperative morbidity or overall survival in the VATS vs. thoracotomy group, though VATS was associated with decreased postoperative pain with the compromise of decreased number of lymph nodes (10). Park et al. retrospectively reviewed 428 patients with Stage II-IIIA NSCLC after they underwent lobectomy following neoadjuvant chemo/chemoradiotherapy. This group was divided into two cohorts, resection via conventional thoracotomy (N = 397) vs. MIS technique (N = 31, 17 robotic, 14 VATS) (11). Three-year overall and disease-free survival were comparable between two groups, as was the complication rate. Length of stay was shorter for the MIS group. R0 resection rate was similar between both groups, 94% for thoracotomy and 97% for MIS. Conversion to thoracotomy occurred in 8/31 (26%) MIS cases due to extent of disease, severe adhesions, and bleeding (11).
Data looking at MIS resections for neoadjuvant NSCLC have also shown similar metrics regarding a high conversion rate to open resection. Huang et al. evaluated 43 patients with stage IIA-IIIB NSCLC with neoadjuvant treatment who underwent VATS pulmonary resection. Most resections were a lobectomy, though there were nine bronchial sleeve lobectomies, five bi-lobectomies, and four pneumonectomies performed. Survival for the entire cohort at 1, 2, and 3 years were 94, 79, and 65%, respectively. Forty patients received an R0 resection. There was a 2.3% mortality (1/43 patients), and 5 patients had postoperative complications. While no patient was converted to “conventional thoracotomy,” a “hybrid VATS” was performed in 7 (16.7%) of the cases, due to proximity of the tumor to large vessels and/or bronchi, in the setting of mod-severe inflammation and fibrosis due to the neoadjuvant therapy (12). A multi-center retrospective review by Cerfolio et al. evaluated 223 patients with occult or evident N2 disease undergoing robotic-assisted resection. Of these, 15.2% received neoadjuvant therapy, and 8 patients in that group also received pre-operative radiotherapy. Major complications (10.1%) were similar between the neoadjuvant group and surgery-upfront group. R0 resection rate was 98.1%, with a 0% 30 and 90-day mortality in the neoadjuvant group. Of the neoadjuvant resections, 15% converted to thoracotomy. No conversions were for bleeding, but generally for oncologic resection due to discovery of extensive mediastinal lymph node involvement (13) (Table 2).
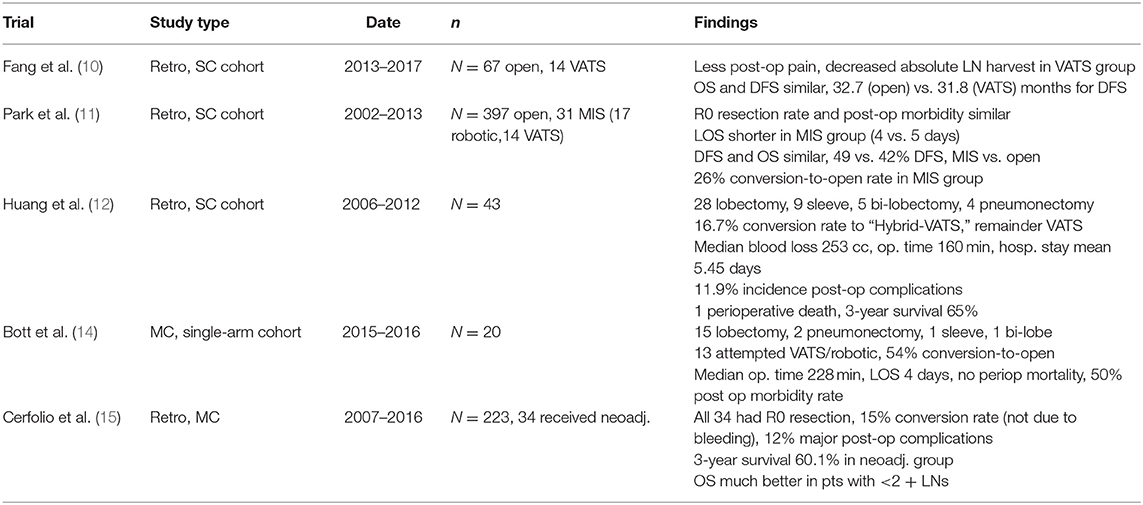
Table 2. Outcomes for minimally invasive vs. open resection after neoadjuvant therapy for NSCLC.
Surgery after induction immunotherapy also poses similar risks. Broderick et al. evaluated outcomes of 20 stage I-IIIA NSCLC patients who received with neoadjuvant Nivolumab followed by pulmonary resection, 13 of which were initially attempted via VATS or robotic. There was 0% perioperative mortality, and 50% morbidity, most commonly atrial fibrillation. Three-quarters of the patients underwent lobectomy, while another 10% received a pneumonectomy. Of the 13 procedures attempted via MIS, seven procedures (54%) converted to thoracotomy. Some of the conversions were due to hemorrhage and/or dense adhesions in the chest. The remainder of conversions were due to severely inflamed mediastinal and hilar nodal stations (14).
Current data demonstrate that induction treatment, with chemotherapy, radiation, or immunotherapy, can lead to increased need to convert from minimally invasive to open resection. However, these studies also demonstrate that minimally invasive pulmonary resection post-induction therapy has similar overall survival compared to open resection. Thus, in the properly chosen patient with locally advanced disease, robotic resection post-induction is safe, effective, and comparable in survival and complications when compared to conventional open resection.
Robotic pulmonary resections at our institution are performed on Da Vinci Xi robot surgical system (Intuitive Surgical Inc., Mountain View, CA). Bronchoscopy is performed to ensure correct placement of the double-lumen tube, and the patient is placed in lateral decubitus position. We employ a standardized set up: a four-arm approach and a 0-degree scope, with congruent port placement in the 8th intercostal space, with one assist port for the bedside assistant that is also utilized as air seal where CO2 is insufflated into the pleural cavity (16). In general, the anterior-most port (a 12-mm port) is placed one rib higher than the other three robotic ports to avoid injury or stunning the nerve to the upper rectus abdominis muscle. A multi-level intercostal nerve block is performed prior to docking.
Dissection usually begins with careful exploration of the chest cavity to ensure there are no pleural metastases or unsuspected free fluid. The inferior pulmonary ligament is divided, with the lung retracted superiorly with the 4th arm, and station 9, and then the eight lymph nodes are harvested. Following this, the subcarinal lymph node packet is entirely removed, as are all of the stations 2–4 if on the right side, or 5–6 if in the left chest. In post-induction resections, we pay close attention to evaluating which aspect of the dissection is going to be most challenging due to adhesions. Location of the mass, lymphadenopathy, and areas of prior positive nodal disease are evaluated with relation to the hilar vessels and bronchus. We prefer to start with a posterior dissection. On the left side, the posterior view allows for identification of the PA, as well as the A2 and A6 PA branches to be identified to help completely open the posterior fissure. On the right side, the posterior approach allows for the right upper lobe bronchus to be encircled and divide prior to any PA branches being ligated. These tricks provide safer PA dissection. Prior to dissection of these area, hilar control can obtained for select cases, with careful dissection around the pulmonary veins using blunt and bipolar energy, as well as dissection of the proximal pulmonary artery. If the tumor is quite proximal, an intra-pericardial technique is used to encircle the pulmonary artery and the pulmonary veins. After this control is obtained, the dissection is done. If significant bleeding is encountered from the pulmonary artery or vein, the operator can effectively clamp the hilum. During dissection around of vascular structures, multiple sponges are in the chest, ready to hold pressure if needed. A thoracotomy tray should be in the room, and blood products should be on hold.
Our group has written about the approach and mindset of the robotic thoracic surgeon before with respect to conversion to open for massive bleeding. The paradigm of preparation, pressure, patience, poise, products, partner, and prolene applies here as well, with the addition of already having had hilar control (15). We find these to be the salient points of performing robotic post-induction pulmonary resection, with the most vital being the potential for massive large vessel hemorrhage and the need for prophylactic hilar control beforehand.
Centrally located NSCLC presents a unique challenge for obtaining an R0 resection. Airway involvement including the proximal lobar bronchus or the main stem airway precludes the ability to perform a lesser anatomic resection and has historically necessitated pneumonectomy. Sleeve resection of the airway was developed as an alternative to pneumonectomy. This was traditionally only offered to frail patients with poor pulmonary reserve for fear of a poor oncologic resection and close margins. Recently, however, sleeve resection has become more accepted as the primary surgical option, even in those who can tolerate pneumonectomy (16). Currently sleeve resection is indicated for any stage I and II centrally located tumors where sleeve reconstruction is technically feasible (17, 18).
The benefits of sleeve resection for early-stage central tumors is highlighted in a large single institution retrospective series conducted in France, which evaluated 1,230 patients with 184 sleeve resections. The authors demonstrate significantly improved 5-year survival (52 vs. 31%) as well as decreased locoregional recurrence (22 vs. 35%) in stage I/II patients of sleeve resection compared to pneumonectomy (19). Okada et al. similarly reported better for 120 matched patients, 60 sleeves vs. 60 pneumonectomies, with a 48 vs. 28% 5-year survival (20). National data from France comparing 941 sleeve lobectomies to 5,318 pneumonectomies resulted in the recommendation for sleeve lobectomy whenever feasible in early-stage cancer based on equitable long-term mortality and possibly better results when propensity matched (18) (Table 3).
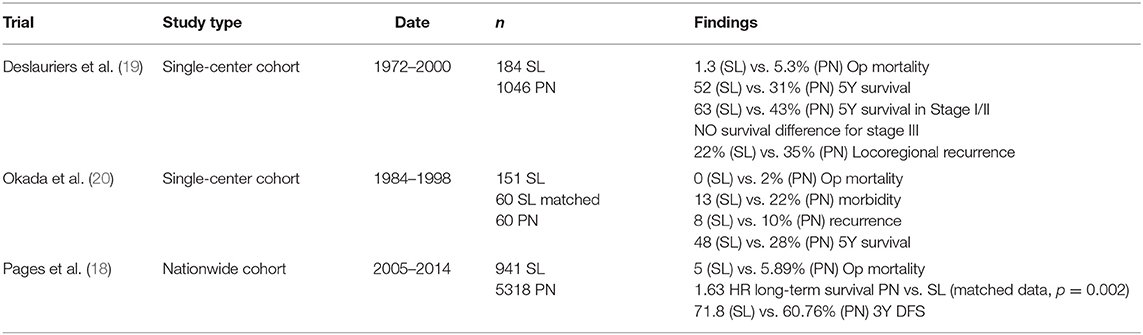
Table 3. Comparison of sleeve lobectomy and pneumonectomy outcomes.
Patients with lesions involving the proximal portion of the pulmonary artery warrant special consideration and have been shown to benefit from pulmonary arterioplasty with or without bronchial sleeve resection. Defects in the artery can vary and reconstruction has been described with patch reconstruction, primary anastomosis, or interposition graft (21). Rendina et al. have reported a 20-year experience with pulmonary arterioplasty during lobectomy in 105 patients. Their series included 47 pulmonary artery sleeves and 65 PA reconstructions associated with bronchial sleeve. Operative mortality was 0.95% and 5-year survival was 44%. Prior concerns of PA thrombosis or hemorrhage were rare with a single case of thrombosis. Long-term disease-free survival was equivalent to that expected of lesser resections stage for stage (22, 23). Meta-analysis of sleeve lobectomy with pulmonary arterioplasty has also demonstrated equivalent operative risk, complication rate, and long-term mortality to isolated sleeve lobectomy and trend toward improved outcomes compared to pneumonectomy (24).
The benefits of minimally invasive surgery have been well-documented (25). As reiterated above, the advent of robotic-assisted surgery has continued to improve complication rates, length of stay, and 30-day mortality when compared to video-assisted surgery (26). Sleeve resection had previously been limited to an open approach, barring a few specialized centers, given VATS's limited maneuverability and lack of depth perception. Robotic-assisted bronchoplasty was first described in cadaver models before being applied in a hybrid VATS/RATS fashion (27). The challenges of bronchoplasty are well-suited to the robotic platform and allow for precise intrathoracic suturing.
Application robotic systems have occurred over the past decade. Few institutions have published series reviewing their results. Jiao et al. have reported the largest series with 67 patients with broad indications for sleeve lobectomy, including those with peri-bronchial lymph node metastases. They demonstrate safety and feasibility of the procedure, with no 90-day mortalities, few complications, and no conversions to open. Major complications included one anastomotic stricture, one chylothorax, one stroke, and one patient readmitted for pneumonia (28). Our group has reported the second largest series of 23 patients with no short-term mortality and minimal morbidity, consisting of one conversion to open for concern of anastomotic tension, one readmission for pneumonia, and one transfusion for asymptomatic anemia. Over a median follow-up of 18 months, no patients had locoregional recurrence (29). Pan et al. had previously reported a similar series of 21 robotic sleeve resections with similar results, although with one 30-day mortality and marginally higher rates of complications (30). Recent retrospective review of robotic sleeve compared to VATS and open show at least parity of short-term outcomes in weighted matched patients and suggest decreased bleeding, length of stay, and operative time (31) (Table 4). While short-term oncologic results seem promising, long-term data remains to be seen.
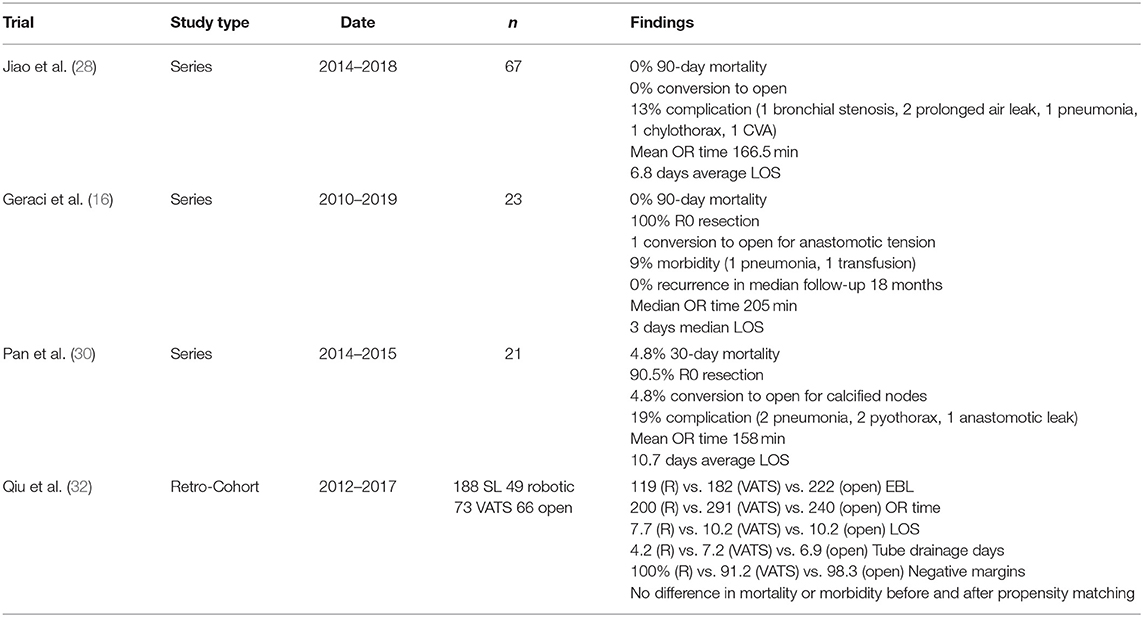
Table 4. Outcomes from robotic sleeve resection.
Our approach for robotic sleeve lobectomy consists of a completely portal robotic approach with the Da Vinci XI system (Intuitive Surgical Inc, Mountain View, CA) and a 0° camera. Prior to port placement, bronchoscopy is done to map tumor extent and endobronchial involvement. Four robotic ports are placed and one assistant port are placed in standard position for a lobectomy, as described above.
A right upper lobectomy is described as it is the most common concomitant lobectomy performed. A mediastinal lymphadenectomy is performed, with careful attention to clearing the entire subcarinal lymph node packet, in order to visualize the takeoff of the right and left mainstem bronchi. The anatomic triangle around the right upper lobe bronchus takeoff is dissected clean by resecting the level 10 lymph node associated. The fissure is then dissected free with either bipolar if complete or tunneled and the parenchyma stapled to reveal the ongoing artery. The posterior ascending artery and azygos vein are stapled to allow for complete mobilization of the trachea and to prevent fistula to the bronchial anastomosis. The FiO2 is lowered to 21%, and then the RUL bronchus is transected with unipolar scissors. The remainder of the lobectomy is completed after division of the truncus anterior and the posterior fissure. Video of this procedure is available at https://www.youtube.com/watch?v=0_k-3Sgro5E.
For lesions that require pulmonary artery reconstruction, proximal, and distal control are obtained with vessel loops and flexible vascular clamp (Cygnet; Peters Surgical, Bobigny, France) inserted through a separate incision and contoured to the chest wall or a reliance Bulldog clamp (Scanlan, Saint Paul, MN) through the robotic ports. Distal control is obtained similarly or by clamping the pulmonary vein. Heparin was not routinely given unless clamp time was prolonged. Bronchotomy was done under infrared visualization and bronchoscopy (Firefly; Intuitive Surgical, Sunnyvale, CA). Proximal bronchotomy is done first to visualize the distal extent of the lesion. Frozen section of the proximal and distal bronchus is performed, and re-resection is done if margins are positive.
For the bronchial anastomosis, the airway is oriented so the membranous portion is parallel to the spine and two continuous running Stratafix sutures (Johnson & Johnson, New Brunswick, NJ) are used. The cartilaginous portion of the anastomosis is completed first from 6 to 12 o'clock on the proximal airway (junction to junction of the cartilaginous and membranous portions) (video available at https://www.youtube.com/watch?v=HVnBIeAgXdU) before the lung is retracted superiorly and anteriorly to run a second suture along the membranous portion. Pneumostasis is tested by reinflation under saline and, if an air leak is present, a single repair stitch is placed. Routine buttressing is not done unless the patient underwent neoadjuvant therapy (29).
Pneumonectomy remains an operation of last resort given the associated morbidity and mortality (29). Of the elective pulmonary resections, it entails the highest risk with operative mortality ranging from 3 to 12% with most recent guidelines stating a risk of 7% or less as acceptable (33). Mortality risk increases with operation for inflammatory conditions and prior induction therapy with rates reported of over 12% (34). Cardiovascular complications are also significantly higher than other lesser resection with rates reported of 20–60% with many life-threatening requiring immediate intervention (35). Other morbidities include pneumonia, bronchopleural fistula, recurrent laryngeal nerve palsy, pulmonary embolus, and prolonged extubation (36, 37). Centrally located NSCLC with involvement of the hilar structures from direct tumor invasion or extensive hilar nodal disease requires pneumonectomy for R0 resection. Other indications include multi-lobar disease or metachronous lesions in remaining lobes. Pneumonectomy also remains as backup when lung preservation is found to be an unacceptable oncologic resection in patients with adequate pulmonary reserve (29).
As previously stated, the benefits of MIS have been validated and include decreased blood loss, length of stay, postoperative pain, and equivalent oncologic outcomes. The expansion of VATS or robotic pneumonectomy, however, has been slow and hindered by technical, safety, and oncologic concerns. Thus, there have been few series of VATS pneumonectomies and only case reports of robotic-assisted operations.
Thoracoscopic pneumonectomy has been described in three prior series all with fairly similar results. They largely conclude VATS pneumonectomy as a feasible and safe procedure with equivalent oncologic outcomes, albeit with a high conversion rate. Battoo et al. reviewed 107 single-center patients (67 VATS) with similar rates of postoperative complications, no major intraoperative bleeding, a conversion rate of 16%, and decreased 1-year pain (38). Liu et al. matched 64 open cases to 32 VATS pneumonectomies with similar postoperative complication rates and longer OR times (39). The only multi-center review conducted by Yang et al. included 124 VATS pneumonectomy to 235 open operations. Outcomes mirrored prior studies with a 19% conversion rate, and persistent differences are found only on the extent of lymph node dissection leaning in favor of the VATS approach (40) (Table 5). Data on robotic resections are sparse. Only six have been described with various configurations. Outcomes include two conversions and one complication/mortality from pulmonary artery bleeding (41) (Table 6).
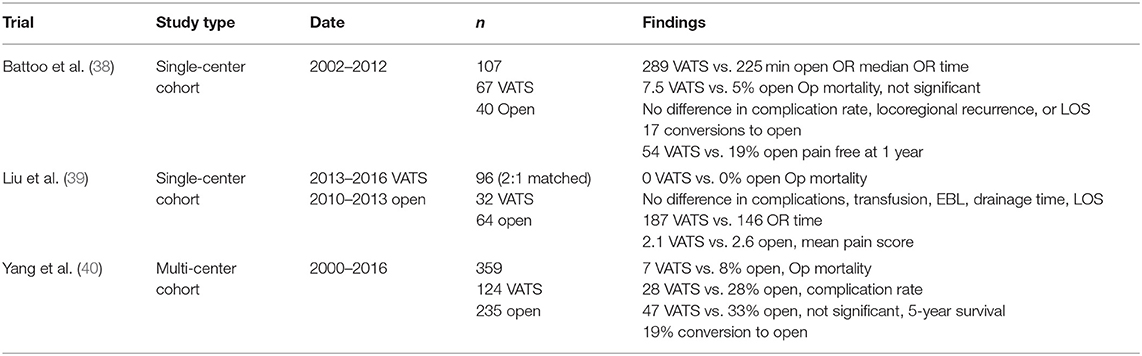
Table 5. Outcomes of video-assisted thoracoscopic pneumonectomy.

Table 6. Case series of robotic pneumonectomy.
Robotic pneumonectomy raises a number of technical concerns. Exposure of the main pulmonary artery often requires division of the superior pulmonary vein from an anterior approach. With large hilar tumors, proximal extent of dissection may require intra-pericardial dissection. Early division of the pulmonary veins can engorge the specimen and make extraction difficult, require extra maneuvers including piecemeal extraction, and threaten tumor seeding. Left pneumonectomy is hampered by the aorta and risk of a long bronchial stump. Full dissection of the aortopulmonary window lymph nodal tissue can aid in retraction and allow a more proximal staple line. However, we have now performed eight in the past 2 years with success (video of our technique available at https://www.youtube.com/watch?v=P1mrftUCBCg).
In our experience, an intra-pericardial approach is often if not always needed, since a sleeve is not possible, and can facilitate division of pulmonary vasculature. After most of the dissection around the pulmonary vascular is performed, and gross or multi-station N2 disease is ruled out, we generally divide the inferior vein first. Next, the superior pulmonary vein and then the main pulmonary artery are divided. When performing left pneumonectomy, complete dissection of the subcarinal and AP window nodes allows for a bronchial division at the carina with a black handheld staple load, which is performed last. If possible, we routinely divide the specimen prior to extraction to extract two smaller specimens, rather than one large one to limit incision side or use of rib spreaders. If the specimen is divided, we routinely divide along the fissure.
As discussed in detail above, lung cancer remains a growing source of morbidity and mortality in this country, demonstrated by its position as the leading cause of cancer death among Americans. With innovation in medical therapy, we are able to extend life and avoid morbidity in more advanced-stage NSCLC than previously. Surgical resection has always been an important therapy for NSCLC, and its role in advanced disease post-induction is an evolving endeavor that will need close attention in the coming years. With the advent of the robotic platform, these operations, as well as more extended resections, such as pneumonectomy and sleeve lobectomy, may be able to be performed in a way to reap the benefits of the more localized resections completed in a minimally invasive manner. With the data reviewed above, we were able to demonstrate that an adequate resection is indeed achievable. R0 resection rates were similar in the largest post-induction study we reviewed, and an MIS sleeve lobectomy 20-person study revealed a 100% R0 resection rate. Moreover, although only a small handful of MIS studies exist, short- and long-term survival rates appeared to be statistically similar between an MIS and open approach for these extended resections. Nonetheless, these few studies also seem to have a similar trend of low conversion-to-thoracotomy rate. This was reported to be as low as 4.5%, but tended to be on average around 20% between the reviewed studies. This most often was due to bleeding and/or heavily calcified and fibrotic hilar nodes creating a more dangerous dissection.
Overall, we believe that this review of the data and our institution's experience prove that these extended resections are feasible using a robotic platform. The most important aspect is preparation on part of the surgeon, as well as knowledge of what to expect intra-operatively. Our group has a focused strategy on these essential steps: (1) obtaining hilar control prior to proceeding with the areas of most complicated dissection, especially in the post-induction cases; (2) a thorough LN dissection to create a definitive picture of airway anatomy, as well as lining up the airway appropriately to suture; and (3) intra-pericardial hilar control for the MIS pneumonectomy. We believe that if the surgical team is able to follow these key steps, while always being prepared to open for thoracotomy (i.e., blood products on hold, thoracotomy tray in the room, sponges in the chest for pressure, senior partners nearby), these resections can be performed in a safe and efficacious manner to best treat this subset of patients.
JS and JJ: writing, editing, and research. SC, TG, and RC: writing and editing. All authors contributed to the article and approved the submitted version.
RC discloses past relationships with AstraZeneca, Bard Davol, Bovie Medical Corporation, C-SATS, ConMed, Covidien/Medtronic, Ethicon, Fruit Street Health, Google/Verb Surgical, Intuitive Surgical, KCI/Acelity, Myriad Genetics, Neomend, Pinnacle Biologics, ROLO-7, Tego, and TransEnterix.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Cancer Society. Lung Cancer Statistics. 2020). Available online at: https://www.cancer.org/cancer/lung-cancer/about/key-statistics.html (accessed July 17, 2020).
2. Society of Thoracic Surgery. General Thoracic Surgery Data. (2018). Available online at: https://www.sts.org/sites/default/files/documents/STSThoracicExecutiveSummaryFall2018.pdf (accessed July 17, 2020).
3. Geraci T, Cerfolio R. Results in robotic surgery for lung cancer. Shanghai Chest. (2018) 2:70. doi: 10.21037/shc.2018.08.07
4. Cerfolio RJ, Ghanim AF, Dylewski M, Veronesi G, Spaggiari L, Park BJ. The long-term survival of robotic lobectomy for non-small cell lung cancer: a multi-institutional study. J Thoracic Cardiovascular Surg. (2018) 155:778–86. doi: 10.1016/j.jtcvs.2017.09.016
5. National Comprehensive Cancer Network. NSCLC Treatment Guidelines. (2020). Available online at: https://www2.tri-kobe.org/nccn/guideline/lung/english/non_small.pdf (accessed July 17, 2020).
6. Pass HI, Pogrebniak HW, Steinberg SM, Mulshine J, Minna J. Randomized trial of neoadjuvant therapy for lung cancer: interim analysis. Annals Thoracic Surg. (1992) 53:992–8. doi: 10.1016/0003-4975(92)90373-C
7. Song WA, Zhou NK, Wang W, Chu XY, Liang CY, Tian XD, et al. Survival benefit of neoadjuvant chemotherapy in non-small cell lung cancer: an updated meta-analysis of 13 randomized control trials. J Thoracic Oncol. (2010) 5:510–6. doi: 10.1097/JTO.0b013e3181cd3345
8. Rosell R, Gómez-Codina J, Camps C, Maestre J, Padille J, Cantó A, et al. A randomized trial comparing preoperative chemotherapy plus surgery with surgery alone in patients with non-small-cell lung cancer. N Engl J Med. (1994) 330:153–8. doi: 10.1056/NEJM199401203300301
9. Roberts JR, Eustis C, Devore R, Carbone D, Choy H, Johnson D. Induction chemotherapy increases perioperative complications in patients undergoing resection for non-small cell lung cancer. Annals Thoracic Surg. (2001) 72:885–8. doi: 10.1016/S0003-4975(01)02836-3
10. Fang L, Wang L, Wang Y, Lv W, Hu J. Video assisted thoracic surgery vs. thoracotomy for locally advanced lung squamous cell carcinoma after neoadjuvant chemotherapy. J Cardiothoracic Surg. (2018) 13:128. doi: 10.1186/s13019-018-0813-7
11. Park BJ, Yang HX, Woo KM, Sima CS. Minimally invasive (robotic assisted thoracic surgery and video-assisted thoracic surgery) lobectomy for the treatment of locally advanced non-small cell lung cancer. J Thoracic Dis. (2016) 8(Suppl 4):S406–13. doi: 10.21037/jtd.2016.04.56
12. Huang J, Xu X, Chen H, Yin W, Shao W, Xiong X, et al. Feasibility of complete video-assisted thoracoscopic surgery following neoadjuvant therapy for locally advanced non-small cell lung cancer. J Thoracic Dis. (2013) 3(Suppl 3):S267–73.
13. Veronesi G, Park B, Cerfolio R, Dylewski M, Toker A, Fontaine JP, et al. Robotic resection of Stage III lung cancer: an international retrospective study. Eur J Cardio-Thoracic Surg. (2018) 54:912–9. doi: 10.1093/ejcts/ezy166
14. Bott MJ, Yang SC, Park BJ, Adusumilli PS, Rusch VW, Isbell JM, et al. Initial results of pulmonary resection after neoadjuvant nivolumab in patients with resectable non-small cell lung cancer. J Thoracic Cardiovascul Surg. (2019) 158:269–76. doi: 10.1016/j.jtcvs.2018.11.124
15. Cerfolio RJ, Bess KM, Wei B, Minnich DJ. Incidence, results, and our current intraoperative technique to control major vascular injuries during minimally invasive robotic thoracic surgery. Annals Thoracic Surg. (2016) 102:394–9. doi: 10.1016/j.athoracsur.2016.02.004
16. Geraci TC, Ferrari-Light D, Wang S, Mitzman B, Chang SH, Kent A, et al. Robotic sleeve resection of the airway: outcomes and technical conduct using video vignettes. Annals Thoracic Surg. (2020) 110:236–40. doi: 10.1016/j.athoracsur.2020.01.077
17. Predina JD, Kunkala M, Aliperti LA, Singhal AK, Singhal S. Sleeve lobectomy: current indications and future directions. Annals Thoracic Cardiovascul Surg. (2010) 16:310–8.
18. Pages PB, Pierre M, Renaud S, Brouchet L, Thomas PA, Dahan M, et al. Sleeve lobectomy may provide better outcomes than pneumonectomy for non-small cell lung cancer. A decade in a nationwide study. J Thorac Cardiovasc Surg. (2016) 153:184–95.e3. doi: 10.1016/j.jtcvs.2016.09.060
19. Deslauriers J, Grégoire J, Jacques LF, Piraux M, Guojin L, Lacasse Y. Sleeve lobectomy versus pneumonectomy for lung cancer: a comparative analysis of survival and sites or recurrences. Annals Thoracic Surg. (2004) 77:1152–6. doi: 10.1016/j.athoracsur.2003.07.040
20. Okada M, Yamagishi H, Satake S, Matsuoka H, Miyamoto Y, Yoshimura M, et al. Survival related to lymph node involvement in lung cancer after sleeve lobectomy compared with pneumonectomy. J Thoracic Cardiovascular Surg. (2000) 119(4 Pt 1):814–9. doi: 10.1016/S0022-5223(00)70018-3
21. Maurizi G, D'Andrilli A, Venuta F, Rendina EA. Bronchial and arterial sleeve resection for centrally-located lung cancers. J Thoracic Dis. (2016) 8(Suppl 11):S872–81. doi: 10.21037/jtd.2016.06.48
22. Rendina EA, Venuta F, De Giacomo T, Ciccone AM, Moretti M, Ruvolo G, et al. Sleeve resection and prosthetic reconstruction of the pulmonary artery for lung cancer. Annals Thoracic Surg. (1999) 68:995–1002. doi: 10.1016/S0003-4975(99)00738-9
23. Venuta F, Ciccone AM, Anile M, Ibrahim M, De Giacomo T, Coloni GF, et al. Reconstruction of the pulmonary artery for lung cancer: long-term results. J Thoracic Cardiovascular Surg. (2009) 138:1185–91. doi: 10.1016/j.jtcvs.2009.07.043
24. Ma Z, Dong A, Fan J, Cheng H. Does sleeve lobectomy concomitant with or without pulmonary artery reconstruction (double sleeve) have favorable results for non-small cell lung cancer compared with pneumonectomy? A meta-analysis. Eur J Cardio-Thoracic Surg. (2007) 32:20–8. doi: 10.1016/j.ejcts.2007.03.018
25. Gao HJ, Jiang ZH, Gong L, Ma K, Ren P, Yu ZT, et al. Video-assisted vs thoracotomy sleeve lobectomy for lung cancer: a propensity matched analysis. Annals Thoracic Surg. (2019) 108:1072–9. doi: 10.1016/j.athoracsur.2019.04.037
26. Wei S, Chen M, Chen N, Liu L. Feasibility and safety of robot-assisted thoracic surgery for lung lobectomy in patients with non-small cell lung cancer: a systematic review and meta-analysis. World J Surg Oncol. (2017) 15:98. doi: 10.1186/s12957-017-1168-6
27. Shanahan B, O'Sullivan KE, Redmond KC. Robotic sleeve lobectomy-recent advances. J Thoracic Dis. (2019) 11:1074–5. doi: 10.21037/jtd.2019.02.103
28. Jiao W, Zhao Y, Qiu T, Xuan Y, Sun X, Qin Y, et al. Robotic bronchial sleeve lobectomy for central lung tumors: technique and outcome. Annals Thoracic Surg. (2019) 108:211–8. doi: 10.1016/j.athoracsur.2019.02.028
29. Bernard A, Deschamps C, Allen MS, Miller DL, Trastek VF, Jenkins GD, et al. Pneumonectomy for malignant disease: factors affecting early morbidity and mortality. J Thoracic Cardiovascul Surg. (2001) 121:1076–82. doi: 10.1067/mtc.2001.114350
30. Pan X, Gu C, Wang R, Zhao H, Shi J, Chen H. Initial experience of robotic sleeve resection for lung cancer patients. Annals Thoracic Surg. (2016) 102:1892–7. doi: 10.1016/j.athoracsur.2016.06.054
31. Veluswamy RR, Whittaker Brown SA, Mhango G, Sigel K, Nicastri DG, Smith CB, et al. Comparative effectiveness of robotic-assisted surgery for resectable lung cancer in older patients. Chest. (2020) 157:1313–21. doi: 10.1016/j.chest.2019.09.017
32. Qiu T, Zhao Y, Xuan Y, Qin Y, Niu Z, Shen Y, et al. Robotic sleeve lobectomy for centrally located non-small cell lung cancer: a propensity score-weighted comparison with thoracoscopic and open surgery. J Thorac Cardiovasc Surg. (2019). 160:838–46.e2. doi: 10.1016/j.jtcvs.2019.10.158
33. Klemperer J, Ginsberg RJ. Morbidity and mortality after pneumonectomy. Chest Surg Clin North Am. (1999) 9:515.
34. Venuta F, Anile M, Diso D, Ibrahim M, De Giacomo T, Rolla M, et al. Operative complications and early mortality after induction therapy for lung cancer. Eur J Cardio-Thoracic Surg. (2007) 31:714–7. doi: 10.1016/j.ejcts.2007.01.017
35. Mitsudomi T, Mizoue T, Yoshimatsu T, Oyama T, Nakanishi R, Okabayashi K, et al. Postoperative complications after pneumonectomy for treatment of lung cancer: multivariate analysis. J Surg Oncol. (1996) 61:218–22. doi: 10.1002/(SICI)1096-9098(199603)61:3<218::AID-JSO11>3.0.CO;2-3
36. Darling GE, Abdurahman A, Yi QL, Johnston M, Waddell TK, Pierre A, et al. Risk of a right pneumonectomy: role of bronchopleural fistula. Annals Thoracic Surg. (2005) 79:433–7. doi: 10.1016/j.athoracsur.2004.07.009
37. Ilonen IK, Räsänen JV, Sihvo EI, Knuuttila A, Sovijärvi AR, Sintonen H, et al. Pneumonectomy: post-operative quality of life and lung function. Lung Cancer. (2007) 58:397–402. doi: 10.1016/j.lungcan.2007.07.008
38. Battoo A, Jahan A, Yang Z, Nwogu CE, Yendamuri SS, Dexter EU, et al. Thoracoscopic pneumonectomy: an 11-year experience. Chest. (2014) 146:1300–9. doi: 10.1378/chest.14-0058
39. Liu Y, Gao Y, Zhang H, Cheng Y, Chang R, Zhang W, et al. Video-assisted versus conventional thoracotomy pneumonectomy: a comparison of perioperative outcomes and short-term measures of convalescence. J Thoracic Dis. (2016) 8:3537–42. doi: 10.21037/jtd.2016.12.24
40. Yang CJ, Yendamuri S, Mayne NR, Battoo A, Wang H, Meyerhoff RR, et al. The role of thoracoscopic pneumonectomy in the management of non-small cell lung cancer: a multicenter study. J Thoracic Cardiovascular Surg. (2019) 158:252–64.e2. doi: 10.1016/j.jtcvs.2018.12.001
41. Louie BE. Robotic pneumonectomy. Thoracic Surgery Clin. (2014) 24:169–74. doi: 10.1016/j.thorsurg.2014.02.007
42. Giulianotti PC, Buchs NC, Caravaglios G, Bianco FM. Robot-assisted lung resection: outcomes and technical details. Interact Cardiovasc Thorac Surg. (2010) 11:388–92. doi: 10.1510/icvts.2010.239541
43. Spaggiari L, Galetta D. Pneumonectomy for lung cancer: a further step in minimally invasive surgery. Ann Thorac Surg. (2011) 91:e45–7. doi: 10.1016/j.athoracsur.2010.12.008
Keywords: robotic, lobectomy, non-small cell lung cancer, sleeve resection, pneumonectomy, neoadjuvant (chemo)radiotherapy
Citation: Scheinerman JA, Jiang J, Chang SH, Geraci TC and Cerfolio RJ (2021) Extended Robotic Pulmonary Resections. Front. Surg. 8:597416. doi: 10.3389/fsurg.2021.597416
Received: 21 August 2020; Accepted: 05 January 2021;
Published: 22 February 2021.
Edited by:
Christopher William Seder, Rush University Medical Center, United StatesReviewed by:
Justin Blasberg, Yale University, United StatesCopyright © 2021 Scheinerman, Jiang, Chang, Geraci and Cerfolio. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Robert J. Cerfolio, Um9iZXJ0LmNlcmZvbGlvQG55dW1jLm9yZw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.