 Jessica Rührup1*
Jessica Rührup1* Felix Preisser1Lena Theißen1Mike Wenzel1Frederik C. Roos1Andreas Becker1
Felix Preisser1Lena Theißen1Mike Wenzel1Frederik C. Roos1Andreas Becker1 Luis A. Kluth1Boris Bodelle2Jens Köllermann3Felix K. H. Chun1
Luis A. Kluth1Boris Bodelle2Jens Köllermann3Felix K. H. Chun1 Philipp Mandel1
Philipp Mandel1- 1Department of Urology, University Clinic Frankfurt, Frankfurt, Germany
- 2Department of Radiology, University Clinic Frankfurt, Frankfurt, Germany
- 3Department of Pathology, University Clinic Frankfurt, Frankfurt, Germany
Introduction: MRI-targeted biopsy (TB) increases overall prostate-cancer (PCa) detection-rates and decreases the risk of insignificant PCa detection. However, the impact of these findings on the definite pathology after radical prostatectomy (RP) is under debate.
Materials and Methods: Between 01/2014 and 12/2018, 366 patients undergoing prostate biopsy and RP were retrospectively analyzed. The correlation between biopsy Gleason-score (highest Gleason-score in a core) and the RP Gleason-score in patients undergoing systematic biopsy (SB-group) (n = 221) or TB+SB (TB-group, n = 145) was tested using the ISUP Gleason-group grading (GGG, scale 1–5). Sub analyses focused on biopsy GGG 1 and GGG ≥ 2.
Results: Proportions of biopsy GGG 1–5 in the SB-group and TB-group were 24.4, 37.6, 19, 10.9, 8.1% and 13.8, 43.4, 24.2, 13.8, 4.8%, respectively (p = 0.07). Biopsy and pathologic GGG were concordant in 108 of 221 (48.9%) in SB- and 74 of 145 (51.1%) in TB-group (p = 0.8). Gleason upgrading was recorded in 33.5 and 31.7% in SB- vs. TB-group (p = 0.8). Patients with biopsy GGG 1 undergoing RP showed an upgrading in 68.5%(37/54) in SB- and 75%(15/20) in TB-group (p = 0.8). In patients with biopsy GGG ≥ 2 concordance increased for both biopsy approaches (54.5 vs. 55.2% for SB- vs. TB-group, p = 0.9).
Discussion: Irrespective of differences in PCa detection-rates between TB- and SB-groups, no significant differences in GGG concordance and upgrading between patients of both groups undergoing biopsy, followed by RP, were recorded. Concordance rates increased in men with biopsy GGG ≥ 2. TB seems to detect more patients with PCa without a difference in concordance with final pathology.
Introduction
Prostate cancer (PCa) represents a frequently diagnosed cancer in Western countries, with a prevalence of 50–65% in men aged >60 years (1). To further improve survival in patients with PCa, it is important to diagnose PCa in localized, potential curable stages (2). In current clinical practice, detection of PCa consists of a randomized, systematic biopsy (SB) of the prostate in patients with elevated PSA-levels or suspicion of PCa at digital rectal examination (DRE) (3–5). The use of multiparametric magnetic resonance imaging (mpMRI) and MRI-targeted biopsy (TB) to improve PCa detection is a frequently debated topic (6–9), especially since current multicentric randomized trials, like the “Prostate evaluation for clinically important disease: sampling using image guidance or not?”–trial (PRECISION) and the “Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer”-trial (PROMIS), showed the superiority of TB—by increasing the overall PCa detection rate and reducing the detection of insignificant tumors (e.g., Gleason 3+3) (10, 11). These results were recently confirmed by the “Use of prostate systematic and targeted biopsy on the basis of multiparametric MRI in biopsy-naive patients” study (MRI-first), where the added value of TB was 7.6 vs. 5.2% in SB, with only 5.6% of all patients who underwent TB showing insignificant PCa (12).
Many debates on the benefit of TB often broach the issue how these findings affect the definite pathology in specimen after radical prostatectomy (RP) (13, 14). However, the effect on Gleason concordance and up-/downgrading rates between biopsy and specimen are currently a matter of debate. Moreover, a precise diagnosis is crucial for optimal treatment decision-making. A possible impact of performing TB compared to SB might be a higher concordance rate due to a more representative biopsy in TB, or a lower concordance rate because of an overestimation especially of the Gleason-4 percentage in TB. Vice versa, there might be an underestimation of significant tumors in SB and a higher amount of upgrading at final pathology in patients undergoing SB.
The aim of the present study was to correlate the biopsy ISUP Gleason-group grading (GGG) and the GGG of the RP specimen, stratified by the approach of biopsy (SB vs. TB and SB). Subgroups focused on patients with the detection of low-risk PCa.
Materials and Methods
Patients
Based on our prospective institutional review-board approved database, 366 consecutive patients who underwent prostate biopsy and RP during the period between January 2014 and December 2018 were identified and included in our retrospective analysis.
All patients gave informed consent. Ethical approval was obtained from the local ethics committee at the University hospital of Frankfurt.
Biopsy Criteria and Histology
All biopsies were taken with a transrectal approach under local anesthesia and antibiotic prophylaxis. Indication for SB was a suspicious PSA-level/rectal examination of the prostate, according to current guidelines (4, 15). SB was performed using a 12-core approach (SB-group). In patients with a PI-RADS-lesion ≥3 (according to the Prostate Imaging–Reporting and Data System “PI-RADS”-v2 classification) (16) in the mpMRI of the prostate, additional to the SB a TB was performed (TB-group). All mpMRI for targeted biopsies were reviewed by an internal specified radiologist.
All TBs were conducted as MRI-targeted ultrasound fusion biopsy using the “Ascendus Hi-Vision” system by Hitachi. There are different methods for performing TB. In our department we performed image-fusion TB; cognitive (mental) fusion TB and in-bore are therefore not subject of the present manuscript.”
The biopsy cores and specimen after RP were evaluated by dedicated uro-pathologists. The biopsy Gleason was defined as highest Gleason-score in at least one core and was reported using the ISUP Consensus Conference 2014 grading system (17).
Statistical Analysis
Descriptive statistics included medians for continuous variables and frequencies and proportions for categorical variables. Differences were analyzed with the use of two-group mean-comparison t-test, the Kruskall-Wallis test and the Pearson's chi-squared test. Univariable analysis were performed to compare concordance, upgrading and downgrading rates of the ISUP Gleason-group grading (GGG, scale 1–5) of biopsy and specimen using SPSS software (PASW Statistics 18, Software by IBM, Ehningen, Germany). A p-value of 0.05 or lower was considered statistically significant.
Results
Descriptive characteristics of the entire patient cohort and stratified by biopsy approach are depicted in Table 1. Overall, 221 patients underwent SB (60.4%) vs. 145 patients (39.6%) who constituted the TB-group. Proportion of patients undergoing TB increased over the years (Figure 1). There were no statistically significant differences regarding age, prostate volume, and median PSA-levels between the two groups (Table 1). The distribution of PI-RADS 3–5 in patients of the TB-group was 13.1, 45.5, and 41.4%, respectively. The total proportions of biopsy GGG 1–5 in patients with SB were 24.4, 37.6, 19.0, 10.9, and 8.1% and 13.8, 43.4, 24.2, 13.8, and 4.8% in patients of the TB-group, respectively (p = 0.07). At final pathology GGG 1–5 in men of the SB-group were 10.0, 54.7, 12.7, 9.5, and 13.1%, and 5.5, 49.7, 23.4, 7.6, and 13.8% of the TB-group (p = 0.06).
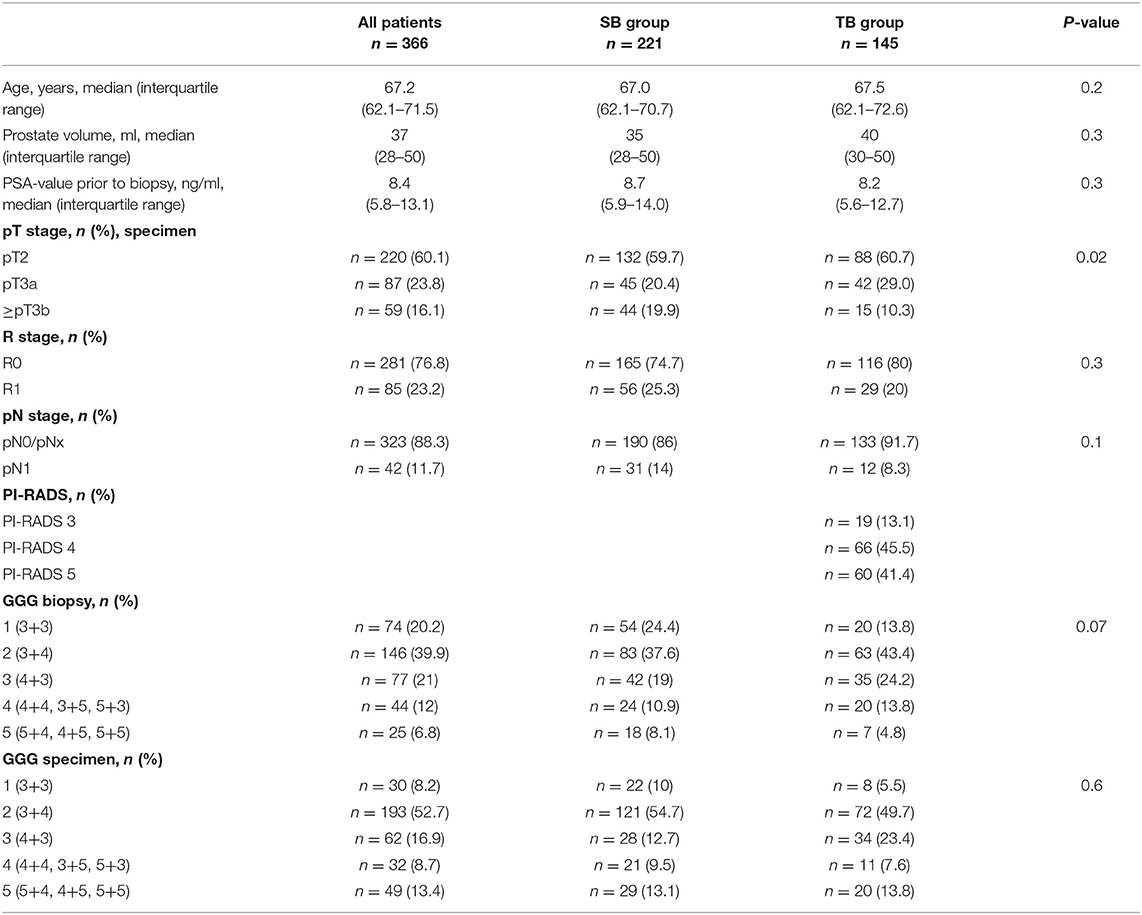
Table 1. Descriptive characteristics of patients that underwent prostate biopsy between 2014 and 2018, stratified according to systematic biopsy (SB) vs. targeted biopsy (TB).
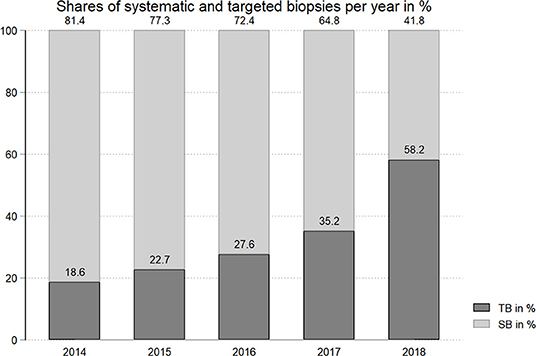
Figure 1. Distribution of SB vs. TB at our institution over the years (2014–2018) in percent.
Biopsy and pathologic GGG were concordant in 108 out of 221 (48.9%) men of the SB- and in 74 out of 145 (51.1%) of the TB-group (p = 0.8) (Tables 2A,B, 3A). Gleason upgrading/downgrading of at least one GGG was recorded in 33.5/17.6% patients of the SB-, and in 31.7/17.2% of the TB-group, respectively (all p > 0.05).
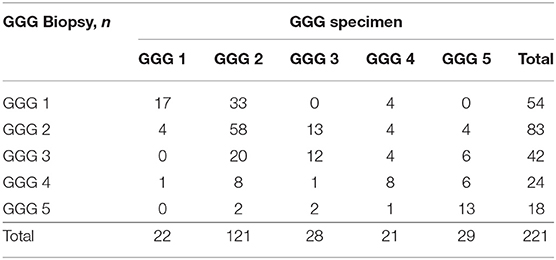
Table 2A. Biopsy vs. specimen Gleason Grade Groups (GGG) in the subgroup of patients with systematic biopsy (SB).
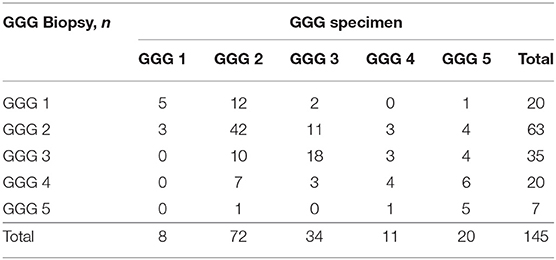
Table 2B. Biopsy vs. specimen Gleason Grade Groups (GGG) in the subgroup of patients with targeted biopsy (TB).
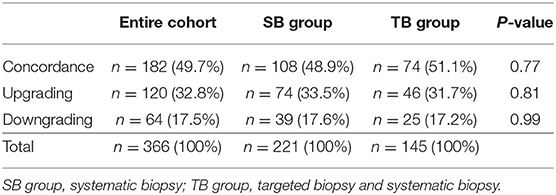
Table 3A. Concordance, upgrading and downgrading of biopsy compared to specimen Gleason Grade Groups (GGG) stratified by biopsy approach.
In patients with biopsy GGG 1 exclusively, 70.3% of all patients showed an upgrading in final pathology. Upgrading rates for patients of the SB- vs. TB-group showed an insignificant trend for a higher risk of upgrading in the TB-group (68.5 vs. 75%, p = 0.8, Table 3B). Downgrading to GGG 1 in final pathology was very rare and occurred only in eight patients (five patients of SB-group vs. three patients of TB-group).
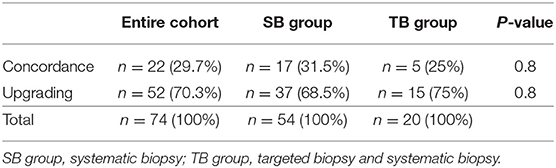
Table 3B. Concordance and upgrading of patients with biopsy Gleason Grade Group (GGG) 1 compared to specimen GGG stratified by biopsy approach.
In patients with biopsy GGG ≥ 2 concordance rates in both groups increased to 54.5 vs. 55.2% (for SB- vs. TB-group, p = 0.9, Table 3C).
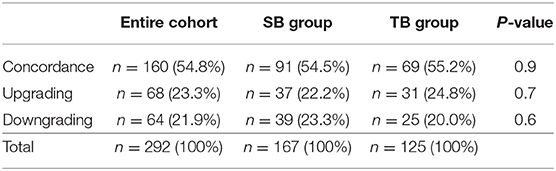
Table 3C. Concordance, upgrading, and downgrading of patients with biopsy GGG ≥ 2 compared to specimen GGG stratified by biopsy approach.
Discussion
In contemporary years, mpMRI of the prostate is becoming an integrative part in the diagnostic workup of PCa (10, 18, 19). Several prospective trials demonstrated that TB can increase PCa detection rates, especially the detection rate of clinically significant PCa (GGG ≥ 2), while lowering the detection rate of low-risk-PCa (9, 11, 20). Despite that, little is known about the concordance of biopsy GGG and GGG at RP specimen. Therefore, we investigated concordance and upgrading rates of GGG in patients who underwent SB (SB-group) vs. SB+TB (TB-group) and the specimen GGG after RP. Our study demonstrated several noteworthy findings which are discussed in the following.
Within the current analysis, based on 366 patients, no significant differences in concordance, upgrading, and downgrading rates in patients of the SB- compared to the TB-group were identified. Concordance increased for both biopsy approaches in the subgroup of patients with biopsy GGG ≥ 2. Thereby, both biopsy approaches represent the “true” GGG of the RP specimen in the same way. Patients of the TB-group in general did not show a more representative biopsy (or a high grade of downgrading as reported by some authors) (20) and SB did not underestimate significant tumors in a higher number of cases. However, besides the above mentioned higher detection rate, the availability of an mpMRI of the prostate has several other advances for patients undergoing RP, which were not tested in the present study (e.g., improvement of local T-stage evaluation, improvement of local therapeutic decision regarding nerve sparing) (21, 22). Despite the known advantages of TB, one has to keep in mind that urologists who perform TB have to undergo a certain learning curve (23).
In contrast to our findings, some authors found the use of TB to be associated with lower rates of Gleason upgrading and higher concordance (13, 14, 24, 25). The largest available study is based on a multicentric cohort published in 2019 by Diamand et al. comparing the concordance rates of TB, SB, and a combination of TB and SB in 443 men undergoing RP (24). The authors described a concordance rate of patients undergoing SB alone of 49.4, 43.1 % of patients had an upgrading at final pathology and in 7.4% a GGG downgrading was recorded. Patients who underwent SB and TB had a concordance rate of 63.2% and upgrading and downgrading rates were 23.9 and 12.9%, respectively. Whereas, concordance in the SB-group was comparable to our data (49.4 vs. 48.9%), concordance in patients undergoing SB and TB was higher compared to the present study (63.2 vs. 51.1%). While patient characteristics (such as age, prostate volume, PSA) were similar, patients analyzed by Diamand et al. had significantly lower biopsy GGG, which might have affected their results. In our series only 8.2% of the patients underwent RP with a GGG 1, but 26.6% of the men analyzed by Diamand et al.–therefore our patient cohort rather represents a contemporary “real-life” cohort, as a stage migration toward more aggressive PCa in patients undergoing RP is described in literature (26). When concentrating only on the results of patients with a GGG ≥ 2, as these patients also likely benefit from a RP, concordance in the TB-group increased in our cohort to 55.2%, which is almost identical to the rate published by Diamand et al. for this subgroup (56.7%). Moreover, patients in our cohort had more advanced disease (e.g., 8.5% in Diamand's cohort vs. 16.1% of our patients showing a pathologic stage ≥pT3b, p = 0.02), which might have especially positively affected the results in the SB-group (19.9% ≥pT3b) in terms of an increase in concordance, as it might be more likely to obtain a randomized biopsy with the “true” GGG in patients with more advanced tumor.
Interestingly, upgrading rates in patients with biopsy GGG 1 had a trend to be higher for patients of the TB- compared to the SB-group. These results corroborate a study by Kayano et al. (14). At final pathology, patients with a GGG 1 in the TB-group were upgraded in 75% compared to 65.4% of the SB-group, which is almost identical with the upgrading rates from our series (75 vs. 68.5%) in this subgroup. However, in both studies, this subgroup consisted only of a small number of patients which might lead to a selection bias.
To further improve the concordance in patients undergoing TB, one should always simultaneously perform a SB (27, 28). Arsov et al. showed a reduced risk of Gleason upgrading when performing a combined SB and TB compared to SB or TB alone (27). Moreover, upgrading rates in patients undergoing TB also seem to be dependent of the extent of TB. Calio et al. prospectively analyzed the data of 208 patients who were divided into two groups, both undergoing TB and SB. One group received a saturation biopsy of the index lesion in mpMRI, and the other group a non-saturated biopsy. The results showed significantly fewer upgrading rates in the saturated lesion group as well as higher concordance rates (13).
The present study has several limitations. First and foremost, our manuscript is based on a retrospective analysis of only one tertiary center. Even though comparable studies do not rely on larger sample sizes, our study is limited to the rather small cohort of 366 patients. Moreover, all our patients in the TB-group underwent simultaneous TB and SB and therefore we cannot measure a potential benefit of SB during TB. The decision to perform SB or a combined SB and TB was made according to current guidelines and to the discretion of the treating urologist and the patient. This might lead to a potential inclusion bias.
Finally, not all patients with histologic confirmed PCa at biopsy underwent RP, which might have led to a potential selecting bias, especially in the subgroup of patients with lower GGG.
In conclusion, irrespective of differences in PCa detection rates between SB and TB, no significant differences in GGG concordance and upgrading rates between patients of the SB- vs. TB-group, followed by RP, were detected. These results were similar in the entire cohort and in patients within the analyzed subgroups (GGG 1 and GGG ≥ 2), whereas concordance rates of the TB-group increased with higher GGG. Therefore, in general TB detects more patients with PCa without a difference in concordance rate at final pathology.
Data Availability
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
This studies involving human participants were reviewed and approved by Ethik-Kommission Fachbereich Medizin, Goethe-Universität Frankfurt. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
LT and MW: acquisition of the analyzed data. FP: acquisition and statistical analysis of data. FR, AB, and LK: final approval of the version to be published and advises during daily work-routine. BB and JK: acquisition of data and final approval of the version to be published. FC: substantial contributions to the conception of the work and final approval of the version to be published. PM: substantial contributions to the conception of the work, revising the manuscript critically for the intellectual content, interpretation of data, and final approval of the version to be published. JR: acquisition, analysis and interpretation of data, substantial contributions to the conception of the work, drafting the work, and revising the work for the intellectual content. All authors complied with all aspects of the work. They ensure that questions related to the accuracy of the work are adequately discussed and solved.
Funding
Funding was only received for open access publication fees from the Goethe University Frankfurt.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Haas GP, Delongchamps N, Brawley OW, Wang CY, de la Roza G. The worldwide epidemiology of prostate cancer: perspectives from autopsy studies. Can J Urol. (2008) 15:3866–71.
2. van den Bergh RCN, Loeb S, Roobol MJ. Impact of early diagnosis of prostate cancer on survival outcomes. Eur Urol Focus. (2015) 1:137–46. doi: 10.1016/j.euf.2015.01.002
3. Leitlinienprogramm Onkologie (Deutsche Krebsgesellschaft, AWMF). Interdisziplinäre Leitlinie der Qualität S3 zur Früherkennung, Diagnose, und Therapie der verschiedenen Stadien des Prostatakarzinoms, Langversion, 5,.0. (2018). Available online at: http://www.leitlinienprogramm-onkologie.de/leitlinien/prostatakarzinom/
4. Thompson I, Thrasher JB, Aus G, Burnett AL, Canby-Hagino ED, Cookson MS, et al. Prostate cancer–guideline for the management of clinically localized prostate cancer: 2007 update. J Urol. (2007) 177:2106–31. doi: 10.1016/j.juro.2007.03.003
5. EAU Guidelines. In: presented at the EAU Annual Congress Copenhagen 2018. Arnhem: EAU Guidelines Office (2018). Available online at: http://uroweborg/guidelines/compilations-of-all-guidelines/
6. Bratan F, Niaf E, Melodelima C, Chesnais AL, Souchon R, Mege-Lechevallier F, et al. Influence of imaging and histological factors on prostate cancer detection and localisation on multiparametric MRI: a prospective study. Eur Radiol. (2013) 23:2019–29. doi: 10.1007/s00330-013-2795-0
7. Dickinson L, Ahmed HU, Allen C, Barentsz JO, Carey B, Futterer JJ, et al. Clinical applications of multiparametric MRI within the prostate cancer diagnostic pathway. Urol Oncol. (2013) 31:281–4. doi: 10.1016/j.urolonc.2012.02.004
8. Filson CP, Natarajan S, Margolis DJ, Huang J, Lieu P, Dorey FJ, et al. Prostate cancer detection with magnetic resonance-ultrasound fusion biopsy: the role of systematic and targeted biopsies. Cancer. (2016) 122:884–92. doi: 10.1002/cncr.29874
9. Siddiqui MM, Rais-Bahrami S, Turkbey B, George AK, Rothwax J, Shakir N, et al. Comparison of MR/ultrasound fusion-guided biopsy with ultrasound-guided biopsy for the diagnosis of prostate cancer. JAMA. (2015) 313:390–7. doi: 10.1001/jama.2014.17942
10. Ahmed HU, El-Shater Bosaily A, Brown LC, Gabe R, Kaplan R, Parmar MK, et al. Diagnostic accuracy of multi-parametric MRI and TRUS biopsy in prostate cancer (PROMIS): a paired validating confirmatory study. Lancet. (2017) 389:815–22. doi: 10.1016/S0140-6736(16)32401-1
11. Kasivisvanathan V, Rannikko AS, Borghi M, Panebianco V, Mynderse LA, Vaarala MH, et al. MRI-targeted or standard biopsy for prostate-cancer diagnosis. N Engl J Med. (2018) 378:1767–77. doi: 10.1056/NEJMoa1801993
12. Rouviere O, Puech P, Renard-Penna R, Claudon M, Roy C, Mege-Lechevallier F, et al. Use of prostate systematic and targeted biopsy on the basis of multiparametric MRI in biopsy-naive patients (MRI-FIRST): a prospective, multicentre, paired diagnostic study. Lancet Oncol. (2019) 20:100–9. doi: 10.1016/S1470-2045(18)30569-2
13. Calio BP, Sidana A, Sugano D, Gaur S, Maruf M, Jain AL, et al. Risk of upgrading from prostate biopsy to radical prostatectomy pathology-does saturation biopsy of index lesion during multiparametric magnetic resonance imaging-transrectal ultrasound fusion biopsy help? J Urol. (2018) 199:976–82. doi: 10.1016/j.juro.2017.10.048
14. Kayano PP, Carneiro A, Castilho TML, Sivaraman A, Claros OR, Baroni RH, et al. Comparison of gleason upgrading rates in transrectal ultrasound systematic random biopsies versus US-MRI fusion biopsies for prostate cancer. Int Braz J Urol. (2018) 44:1106–13. doi: 10.1590/s1677-5538.ibju.2017.0552
15. Mottet NBJ, Bolla M, Briers E, Cumberbatch MG, De Santis M, Fossati N, et al. EAU-ESTRO-SIOG guidelines on prostate cancer. Part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol. (2017) 71:618–29. doi: 10.1016/jeururo201608003
16. Weinreb JC, Barentsz JO, Choyke PL, Cornud F, Haider MA, Macura KJ, et al. PI-RADS prostate imaging–reporting and data system: 2015, version 2. Eur Urol. (2016) 69:16–40. doi: 10.1016/j.eururo.2015.08.052
17. Epstein JI, Egevad L, Amin MB, Delahunt B, Srigley JR, Humphrey PA, et al. The 2014 International Society of Urological Pathology (ISUP) consensus conference on gleason grading of prostatic carcinoma: definition of grading patterns and proposal for a new grading system. Am J Surg Pathol. (2016) 40:244–52. doi: 10.1097/PAS.0000000000000530
18. Pepe P, Dibenedetto G, Garufi A, Priolo G, Pennisi M. Multiparametric pelvic MRI accuracy in diagnosing clinically significant prostate cancer in the reevaluation of biopsy microfocal tumor. Anticancer Res. (2015) 35:395–9.
19. Esen T, Turkbey B, Patel A, Futterer J. Multiparametric MRI in prostate cancer. Biomed Res Int. (2014) 2014:296810. doi: 10.1155/2014/296810
20. Maxeiner A, Kittner B, Blobel C, Wiemer L, Hofbauer SL, Fischer T, et al. Primary magnetic resonance imaging/ultrasonography fusion-guided biopsy of the prostate. BJU Int. (2018) 122:211–8. doi: 10.1111/bju.14212
21. Radtke JP, Wiesenfarth M, Kesch C, Freitag MT, Alt CD, Celik K, et al. Combined clinical parameters and multiparametric magnetic resonance imaging for advanced risk modeling of prostate cancer-patient-tailored risk stratification can reduce unnecessary biopsies. Eur Urol. (2017) 72:888–96. doi: 10.1016/j.eururo.2017.03.039
22. de Rooij M, Hamoen EH, Witjes JA, Barentsz JO, Rovers MM. Accuracy of magnetic resonance imaging for local staging of prostate cancer: a diagnostic meta-analysis. Eur Urol. (2016) 70:233–45. doi: 10.1016/j.eururo.2015.07.029
23. Kasabwala K, Patel N, Cricco-Lizza E, Shimpi AA, Weng S, Buchmann RM, et al. The learning curve for magnetic resonance imaging/ultrasound fusion-guided prostate biopsy. Eur Urol Oncol. (2019) 2:135–40. doi: 10.1016/j.euo.2018.07.005
24. Diamand R, Oderda M, Al Hajj Obeid W, Albisinni S, Van Velthoven R, Fasolis G, et al. A multicentric study on accurate grading of prostate cancer with systematic and MRI/US fusion targeted biopsies: comparison with final histopathology after radical prostatectomy. World J Urol. (2019) 2:135–40. doi: 10.1007/s00345-019-02634-9
25. Porpiglia F, Del S, Passera R, Manfredi M, Mele F, Bollito E, et al. Multiparametric-magnetic resonance/ultrasound fusion targeted prostate biopsy improves agreement between biopsy and radical prostatectomy gleason score. Anticancer Res. (2016) 36:4833–9. doi: 10.21873/anticanres.11045
26. Leyh-Bannurah SR, Karakiewicz PI, Pompe RS, Preisser F, Zaffuto E, Dell'Oglio P, et al. Inverse stage migration patterns in North American patients undergoing local prostate cancer treatment: a contemporary population-based update in light of the 2012 USPSTF recommendations. World J Urol. (2019) 37:469–79. doi: 10.1007/s00345-018-2396-2
27. Arsov C, Becker N, Rabenalt R, Hiester A, Quentin M, Dietzel F, et al. The use of targeted MR-guided prostate biopsy reduces the risk of gleason upgrading on radical prostatectomy. J Cancer Res Clin Oncol. (2015) 141:2061–8. doi: 10.1007/s00432-015-1991-5
Keywords: prostate cancer, mpMRI, biopsy, radical prostatectomy, Gleason upgrading, concordance
Citation: Rührup J, Preisser F, Theißen L, Wenzel M, Roos FC, Becker A, Kluth LA, Bodelle B, Köllermann J, Chun FKH and Mandel P (2019) MRI-Fusion Targeted vs. Systematic Prostate Biopsy–How Does the Biopsy Technique Affect Gleason Grade Concordance and Upgrading After Radical Prostatectomy? Front. Surg. 6:55. doi: 10.3389/fsurg.2019.00055
Received: 18 July 2019; Accepted: 03 September 2019;
Published: 18 September 2019.
Edited by:
Evanguelos Nicolas Xylinas, Hôpital Cochin, FranceReviewed by:
Marianne Schmid, University Medical Center Göttingen, GermanySimone Albisinni, Free University of Brussels, Belgium
Idir Pierre Ouzaid, Hôpital Bichat-Claude-Bernard, France
Copyright © 2019 Rührup, Preisser, Theißen, Wenzel, Roos, Becker, Kluth, Bodelle, Köllermann, Chun and Mandel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jessica Rührup, jessica.ruehrup@kgu.de