 Nikolaos Patelis
Nikolaos Patelis Athanasios Katsargyris
Athanasios Katsargyris Chris Klonaris1
Chris Klonaris1

95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Surg. , 12 June 2017
Sec. Vascular Surgery
Volume 4 - 2017 | https://doi.org/10.3389/fsurg.2017.00032
This article is part of the Research Topic Contemporary Strategies in the Management of Civilian Vascular Trauma View all 8 articles
Injury of the aortic isthmus is the second most frequent cause of death in cases of blunt traumatic injury. Conventional open repair is related to significant morbidity and mortality. Thoracic endovascular aortic repair (TEVAR) has increasing role in traumatic isthmic rupture, as it avoids the thoracotomy-related morbidity, aortic cross clamping, and cardiopulmonary bypass. Additionally to the technical difficulties of open repair, multi-trauma patients may not tolerate the manipulations necessary to undergo open surgery, due to concomitant injuries. TEVAR is a procedure easier to perform compared to open surgery, despite that a considerable degree of expertise is necessary. Direct comparison of the two methods is difficult, but TEVAR appears to offer better results than open repair in terms of mortality, incidence of spinal cord ischemia, renal insufficiency, and graft infection. TEVAR is related to a—statistically not significant—trend for higher re-intervention rates during the follow-up period. Current guidelines support TEVAR as a first-line repair method for traumatic isthmic rupture. Certain specific considerations related to TEVAR, such as the timing of the procedure, the type and oversizing of the endograft, heparinization during the procedure, the necessity of cerebrospinal fluid drainage, type of anesthesia, and the necessary follow-up strategy remain to be clarified. TEVAR should be considered advantageous compared to open surgery, but future developments in endovascular materials, along with accumulating long-term clinical data, will eventually improve TEVAR results in traumatic aortic isthmic rupture (TAIR) cases. This publication reviews the role, outcomes, and relevant issues linked to TEVAR in the repair of TAIR.
Blunt traumatic thoracic aortic injury of the aortic isthmus is the second most frequent cause of trauma-related mortality (1, 2). Open repair usually consists of a high posterolateral thoracotomy and cardiopulmonary bypass to maintain distal perfusion. This procedure is linked to significant mortality, morbidity, and paraplegia incidence (3–5).
Thoracic endovascular aortic repair (TEVAR) has already been proven to be an accepted option in thoracic aneurysm repair, but it can play a significant a role in other pathologies of the thoracic aorta, such as the traumatic aortic isthmic rupture (TAIR) (6–8). TEVAR demonstrates lower morbidity rates compared to that related to the steps of open repair: thoracotomy, aortic cross clamping, and cardiopulmonary bypass. No commercially available stent-graft exists, which is specifically designed for TEVAR in patients with traumatic thoracic aortic injuries, but off-label use of endografts designed for elective TEVAR cases could potentially be used to treat these gravely injured acute patients. This manuscript reviews the role, outcomes, and relevant issues linked to TEVAR in the repair of TAIR.
Isthmus is the segment of the aorta affected in the vast majority of blunt thoracic injury cases, reaching 80% of TAIR patients (9). Other aortic segments, such as the aortic arch, the ascending and the descending aorta are affected significantly less frequently. A number of multiple different forces contribute to the high incidence of TAIR. Posterior movement of the thoracic wall and more specifically of the sternum with simultaneous compression of the aorta onto the spine, sudden hydrostatic pressure increase within the aortic lumen, and massive deceleration altogether lead to shearing and torsion forces on the fixed aortic segments (10). TAIR is related to an approximately 75% mortality rate at the place of injury or during patient transfer to trauma centers, and approximately half of TAIR patients die within the first 24 h after initial medical evaluation (3, 11). The ideal timing for treatment of TAIR patients who reach trauma centers has been constantly changing over the last decades. In the past, these lesions were routinely treated on an emergency basis right after the diagnosis was established, but in recent years, treatment has been shifted toward a more expectant strategy in combination with thorough radiological surveillance and proper pharmaceutical regime, aiming at a strict blood pressure control (12–14).
Although there is no Level I evidence, TEVAR is gradually gaining ground in treatment of TAIR cases, as the advantages of this procedure in terms of operative complexity when compared to open surgical repair are clear. Open repair usually requires left thoracotomy, single lung ventilation, and aortic cross-clamping with complex cardiorespiratory support. However, in most cases, multi-trauma patients may not tolerate most of the necessary surgical or anesthesiologic periprocedural manipulation, while cervical instability and synchronous presence of multiple fractures could make positioning for left thoracotomy on the surgical table problematic or even impossible (10). Grave concomitant injuries and increased bleeding risk may also render up the use of heparin.
Additionally, multi-trauma patients usually arrive at a hospital with limited or no experience in open surgical treatment of thoracic aortic injuries (3, 15). On the other hand, TEVAR is a more commonly performed procedure and available in most hospitals; therefore it can be more easily applied to TAIR patients. Obviously, TEVAR performed in TAIR patients under emergency circumstances requires considerable endovascular expertise. As the majority of first-line trauma centers do not have appropriately trained surgical teams ready to perform complex open surgery and due to the complexity of the required set-up for extensive surgical thoracic aortic repair, TEVAR can be considered a far more accessible option for treating TAIR patients. Therefore, TEVAR should be considered more applicable compared to open surgery in this group of patients.
Published comparative data between open surgery and TEVAR show a significant advantage of the latter in terms of perioperative morbidity and mortality (5, 13, 16, 17). Perioperative morbidity of open surgery remains high (4, 18) with post thoracotomy pneumonia, paralysis or paresis, and injury to the intrathoracic nerves occurring in 60, 6–30, and 20% of cases, respectively (11, 19–21).
On the other hand, data published in multiple single-center studies reports promising outcomes of TEVAR for TAIR. Feezor et al. reported a 0% 30-day mortality and only one serious endograft-related complication in a series of 22 patients undergoing TEVAR for TAIR (22). In a case series of similar size, Urgnani et al. reported technical success in all 20 cases (100%), no neurological complications and only one (5%) TEVAR-unrelated death (23).
A direct comparison of outcomes between open and endovascular repair for TAIR is difficult. Prospective randomized trials have not been published to date. Systematic reviews and meta-analysis of already published literature is the only source of evidence (24, 25).
The largest systematic review was conducted by Murad et al. (26) under the auspices of the Society for Vascular Surgery (SVS). Data were drawn from 7,768 patients, 77% of which were males. TEVAR was reported to present with a significantly lower mortality rate, compared to that of open surgery (9 vs 19%, respectively, p < 0.01). End-stage renal disease (ESRD) and spinal cord ischemia (SCI) incidence was reported to be lower in TEVAR compared to open repair (SCI: 3 vs 9%; ESRD: 5 vs 8%; p < 0.01 for all results). Both systemic and graft infections occurred less frequently in patients treated with TEVAR compared to open surgery (Graft: 3 vs 11%; Systemic: 5 vs 13%: p < 0.01 for all results). During the follow-up period, TEVAR showed a higher re-intervention trend compared to open surgery, although this trend was not statistically significant (p = 0.07). Under the light of the above mentioned findings, the SVS committee published clinical practice guidelines suggesting that TEVAR in patients presenting with traumatic thoracic aortic injuries is linked to better results regarding mortality and morbidity compared to open repair and, therefore, can be considered the first line of treatment (27). This recommendation, however, was based on low-quality evidence (Level C, Grade 2). Up-to-date guidelines published by the European Society of Cardiology (ESC) and the European Society for Vascular Surgery (ESVS) support TEVAR as the primary method for TAIR repair, now based on stronger evidence (Class I, Level B) (28, 29). A recent review of 5 meta-analyses, 2 prospective, and 7 retrospective studies also supported the abovementioned guidelines concluding that TEVAR is the most suitable treatment for TAIR where expertise exists (30).
TEVAR demonstrates a number of advantages in the treatment of TAIR cases, but some special issues should be addressed and merit further discussion.
Given the 46% mortality rate noted in non-operatively managed patients with TAIR (26), the SVS committee suggested urgent (<24 h) repair simultaneously or immediately after other injuries have been addressed, but at the latest prior to hospital discharge (27, 31). In some series, TAIR patients underwent delayed TEVAR up to 7–14 days after sustaining the injury and the published data is promising, although the small number of patients in these series might bias the results (32). Expectant strategy with thorough imaging surveillance and proper pharmaceutical treatment might be appropriate for “minimal aortic injury” cases showing limited periadventitial defect or hematoma (32, 33). ESVS suggests that delayed aortic repair for TAIR should be considered only in patients with periaortic hematoma less than 15 mm and when no rupture is present, but better evidence is necessary to support this suggestion (Class IIa, Level C) (29). In contrast with open aortic surgery, TEVAR can be performed in both stable and unstable patients with high technical success rates and good results, making it an attractive modality for unstable patients who urgently need to undergo TEVAR (34).
The timing of aortic repair in patients with TAIR in relation to other injuries should also be addressed. In the majority of TAIR cases, lung contusion, rib fractures, and limb injuries are also present and these can be addressed after the aortic repair (32, 35). Life-threatening injuries such as central neural system damage and/or other uncontrolled bleeding should be addressed probably before any aortic repair. Published data is scarce and more is necessary to answer the question of in what order injuries should be treated in relation to aortic repair.
This dilemma has also been addressed by the relevant SVS Committee, which underlined that in acute situations, such as TAIR, patient’s age should not play a significant role in decision-making on the type of repair. Despite the fact that younger patients have been reported to present with a higher risk for late complications, the lower mortality and SCI incidence after TEVAR compared to open repair render these long-term postoperative considerations insignificant (25, 36, 37). On the other hand, younger or fit patients with aortic anatomy unsuitable for TEVAR should consider undergoing open repair (27, 29). To date, it has been accepted that endovascular repair does not have a role in children and teenagers (38). The mismatch between vessel diameter and available stent sizes; the smaller arteries for access and the necessity for surgical exposure of the iliac artery; and finally, the fact that vessels of young individuals will outgrow the placed stents are some of the problems of endovascular repair in children and teenagers. These difficulties may lead vascular surgeons to think twice before proceeding to endovascular repair of isthmic ruptures in such young patients, but successful aortic repair with balloon-expandable stents has already been reported (38).
Most of the TAIR patients are of young age, usually younger than 40 years (26). With age, the aorta goes through normal changes such as diameter expansion and decrease of the aortic arch angulation. Available thoracic endografts have been developed to treat aneurysmal disease as they were designed to, and, therefore, they are suitable for larger aortic diameters and less angulated aortic arches. As a result, the “off-label” use of available thoracic endografts in TAIR cases may have anatomic limitations. Poor adaptation of a stent-graft to increased arch angulation could result in bad apposition and sealing, leading to endoleak and migration or collapse of the stent-graft (35, 39). Stent-graft collapse is a life-threatening complication that could lead to acute aortic occlusion and distal organ malperfusion (22). In TAIR cases after TEVAR, stent-grafts are more prone to collapse due to their larger size compared to the smaller aortic diameter of younger patients as mentioned above. Additionally, hypovolemic shock in trauma patients resulting in vasospasm and cyclic diameter variation of 10–20% in synchronization with the heart cycle can result in significant underestimation of the “real” aortic diameter and inaccurate preoperative stent-graft measurements (35, 40). More aggressive oversizing should be applied in gravely hypotensive patients, but it should not exceed 20% (29). All the above pose additional difficulties to optimal stent-graft sizing in TAIR, but endovascular bioengineers have already started to address the need of thoracic endografts that could fit TAIR patients (41).
Two of the most controversial issues related to TEVAR is the coverage of the LSA and whether routine or selective LSA revascularization should be preferred. In TAIR cases, the landing zone requirements for TEVAR are different to that of thoracic aneurysmal disease, but the proximity of the isthmic injury to the LSA origin makes coverage necessary in up to 50% of TAIR patients (26, 42, 43). Distal arm ischemia, possible vertebrobasilar pathology, and possible occlusion of thyrocervical collateral arteries to anterior spinal arteries increase the risk of SCI occurrence after LSA coverage. To date, no clear consensus regarding preoperative LSA revascularization has been reached and published data are controversial. Some authors suggest LSA coverage when necessary and expectant strategy, and others suggesting the opposite (32, 35, 44). Suggested indications include patent left internal mammary artery to left anterior descending coronary artery bypass or any anatomic variation that renders a patent left vertebral artery necessary. In any case, decision should be made on an individual basis and take into account the level of expertise in either open or endovascular technique, the patient’s general condition, and the presence of concomitant injuries (27, 45).
Open TAIR repair with cardiopulmonary bypass requires a large dose of systemic heparin to perform; a disadvantage that TEVAR does not have. Published data partially support performing TEVAR without the use of heparin in TAIR cases with presence of grave concomitant injuries and high risk for bleeding (13, 46). On the other hand, the majority of currently available sheaths are 22–24 F in diameter and occlude the blood flow at the access vessel. Without the use of heparin, this diminished blood flow caused by the sheath could potentially lead to lower limb ischemia, especially when TEVAR procedural time is prolonged by less experienced operators. Routine heparinization in these cases is frequently based on local experience, as available evidence is very limited. Individualizing the decision and balancing the thrombophylic and hemorrhagic potential of each particular patient is currently suggested (27, 32).
Spinal cord ischemia occurs rarely (3%) after TEVAR for traumatic aortic rupture, significantly lower than open thoracic aortic repair (26, 47). To our opinion, routine CSF drainage is not justified by a number of characteristics of TEVAR for TAIR, such as the limited length of the covered thoracic aorta and the substantial risk of epidural bleeding in the multi-trauma patient, who frequently presents with synchronous coagulopathy. CSF drainage should be considered only in the presence of SCI symptoms (27). Recognizing signs of SCI in a multi-trauma patient who possibly presents with concomitant TAIR and central and/or peripheral neural system trauma can be challenging, therefore, an objective diagnostic and treatment algorithm should be developed.
Despite the fact that TEVAR could be performed under local anesthesia in elective cases, in emergency settings with a multi-trauma patient who is often agitated, non-cooperative, and presents with a number of concomitant injuries of various gravity, local anesthesia is less favorable. Published data support that TEVAR for TAIR should always be performed under general anesthesia (27).
The ideal strategy for long-term follow-up of TAIR patients after TEVAR is still in evolution. Annually performed CTA control for life is considered the best method for elective TEVAR surveillance, but this strategy might not suit patients who underwent TEVAR for TAIR. Opposite to the nature of degenerative thoracic aortic aneurysms, TAIR is not an evolving aortic disease process, but rather a stable injury as a direct result of trauma. Despite current guidelines suggesting the contrary, annual CTA might not be mandatory if TEVAR in TAIR cases is successfully completed and no complications occurred in the short- and midterm follow-up periods (28). The RESCUE trial results suggest that annual follow-up is mandatory only for a period of 5 years (48). This becomes more important given, the younger age of these patients, and the concerns of cumulative radiation and iodinated contrast exposure (49, 50). Other alternative follow-up strategies have been suggested, such as the combination of plain X-ray and MRA that could be of benefit for the long-term surveillance of these patients (28). Follow-up timing and preferred imaging method after TEVAR in TAIR cases should be individualized, tailored, and adapted to the specific conditions of each particular patient.
Anatomic variations and anomalies of the arch and its branches are considered rare, but they are reported to reach as high as 15–34% in published TAIR case series (43). These variations include aberrant right subclavian artery, bovine arch type, Kommerell’s diverticulum, right-sided aortic arch, left vertebral artery, and others. Endovascular specialists should carefully examine the pre-procedural CTA in order to recognize aortic arch anomalies or variations, and consequently avoid complications such as cerebrovascular events, endoleaks, upper extremity ischemia, and SCI. Customized TEVAR materials can address difficult aortic anatomies in elective cases, but in the emergency settings of TAIR, customization is not possible. Therefore, in patients presenting with TAIR and existing arch variations, TEVAR might not be a technically feasible solution, leaving open or hybrid repairs the only way to address the aortic trauma (43).
Endovascular repair of TAIR should be considered advantageous compared to open repair linked to lower operative mortality, morbidity, and SCI incidence. The quality of evidence though remains relatively low. Besides, current stent-grafts are not designed for use in TAIR and, therefore, they cannot always optimally accommodate the unique anatomy of these young patients. Current key points regarding TEVAR in TAIR can be seen in Table 1. Future developments in endovascular materials along with accumulating long-term clinical data will probably improve the outcomes and enhance the role of TEVAR in TAIR repair.
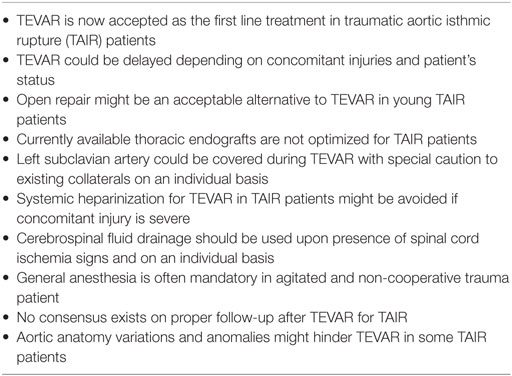
Table 1. Key points.
NP is the corresponding author and has contributed in literature research and manuscript writing. AK has contributed in literature research and manuscript writing. CK has the overall responsibility of the manuscript. All authors have accepted the final (submitted) version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Clancy TV, Gary Maxwell J, Covington DL, Brinker CC, Blackman D. A statewide analysis of level I and II trauma centers for patients with major injuries. J Trauma (2001) 51(2):346–51. doi: 10.1097/00005373-200108000-00021
2. Richens D, Field M, Neale M, Oakley C. The mechanism of injury in blunt traumatic rupture of the aorta. Eur J Cardiothorac Surg (2002) 21(2):288–93. doi:10.1016/S1010-7940(01)01095-8
3. Jamieson WR, Janusz MT, Gudas VM, Burr LH, Fradet GJ, Henderson C. Traumatic rupture of the thoracic aorta: third decade of experience. Am J Surg (2002) 183(5):571–5. doi:10.1016/S0002-9610(02)00851-6
4. Cowley RA, Turney SZ, Hankins JR, Rodriguez A, Attar S, Shankar BS. Rupture of thoracic aorta caused by blunt trauma. A fifteen-year experience. J Thorac Cardiovasc Surg (1990) 100(5):652–60; discussion 660–1.
5. Ott MC, Stewart TC, Lawlor DK, Gray DK, Forbes TL. Management of blunt thoracic aortic injuries: endovascular stents versus open repair. J Trauma (2004) 56(3):565–70. doi:10.1097/01.TA.0000114061.69699.A3
6. Canaud L, Alric P, Branchereau P, Marty-Ané C, Berthet JP. Lessons learned from midterm follow-up of endovascular repair for traumatic rupture of the aortic isthmus. J Vasc Surg (2008) 47(4):733–8. doi:10.1016/j.jvs.2007.12.008
7. Estrera AL, Gochnour DC, Azizzadeh A, Miller CC 3rd, Coogan S, Charlton-Ouw K, et al. Progress in the treatment of blunt thoracic aortic injury: 12-year single-institution experience. Ann Thorac Surg (2010) 90(1):64–71. doi:10.1016/j.athoracsur.2010.03.053
8. Hoornweg LL, Dinkelman MK, Goslings JC, Reekers JA, Verhagen HJ, Verhoeven EL, et al. Endovascular management of traumatic ruptures of the thoracic aorta: a retrospective multicenter analysis of 28 cases in The Netherlands. J Vasc Surg (2006) 43(6):1096–102; discussion 1102. doi:10.1016/j.jvs.2006.01.034
9. Borsa JJ, Hoffer EK, Karmy-Jones R, Fontaine AB, Bloch RD, Yoon JK, et al. Angiographic description of blunt traumatic injuries to the thoracic aorta with specific relevance to endograft repair. J Endovasc Ther (2002) 9(Suppl 2):II84–91. doi:10.1177/15266028020090S214
10. Brinster DR. Endovascular repair of blunt thoracic aortic injuries. Semin Thorac Cardiovasc Surg (2009) 21(4):393–8. doi:10.1053/j.semtcvs.2009.11.003
11. Fabian TC, Richardson JD, Croce MA, Smith JS Jr, Rodman G Jr, Kearney PA, et al. Prospective study of blunt aortic injury: multicenter trial of the American Association for the Surgery of Trauma. J Trauma (1997) 42(3):374–80; discussion 380–3. doi:10.1097/00005373-199703000-00003
12. Pierangeli A, Turinetto B, Galli R, Caldarera L, Fattori R, Gavelli G. Delayed treatment of isthmic aortic rupture. Cardiovasc Surg (2000) 8(4):280–3. doi:10.1016/S0967-2109(00)00015-6
13. Pacini D, Angeli E, Fattori R, Lovato L, Rocchi G, Di Marco L, et al. Traumatic rupture of the thoracic aorta: ten years of delayed management. J Thorac Cardiovasc Surg (2005) 129(4):880–4. doi:10.1016/j.jtcvs.2004.10.012
14. Langanay T, Verhoye JP, Corbineau H, Agnino A, Derieux T, Menestret P, et al. Surgical treatment of acute traumatic rupture of the thoracic aorta a timing reappraisal? Eur J Cardiothorac Surg (2002) 21(2):282–7. doi:10.1016/S1010-7940(01)01133-2
15. Azizzadeh A, Keyhani K, Miller CC 3rd, Coogan SM, Safi HJ, Estrera AL. Blunt traumatic aortic injury: initial experience with endovascular repair. J Vasc Surg (2009) 49(6):1403–8. doi:10.1016/j.jvs.2009.02.234
16. Broux C, Thony F, Chavanon O, Bach V, Hacini R, Sengel C, et al. Emergency endovascular stent graft repair for acute blunt thoracic aortic injury: a retrospective case control study. Intensive Care Med (2006) 32(5):770–4. doi:10.1007/s00134-006-0115-8
17. Lin CC, Liu KS, Chen HW, Huang YK, Chu JJ, Tsai FC, et al. Blunt aortic injury: risk factors and impact of surgical approaches. Surg Today (2016) 46(2):188–96. doi:10.1007/s00595-015-1152-0
18. Sturm JT, Billiar TR, Dorsey JS, Luxenberg MG, Perry JF Jr. Risk factors for survival following surgical treatment of traumatic aortic rupture. Ann Thorac Surg (1985) 39(5):418–21. doi:10.1016/S0003-4975(10)61947-9
19. Kwon CC, Gill IS, Fallon WF, Yowler C, Akhrass R, Temes RT, et al. Delayed operative intervention in the management of traumatic descending thoracic aortic rupture. Ann Thorac Surg (2002) 74(5):S1888–91. doi:10.1016/S0003-4975(02)04148-6
20. Razzouk AJ, Gundry SR, Wang N, del Rio MJ, Varnell D, Bailey LL. Repair of traumatic aortic rupture: a 25-year experience. Arch Surg (2000) 135(8):913–8; discussion 919. doi:10.1001/archsurg.135.8.913
21. Chung J, Owen R, Turnbull R, Chyczij H, Winkelaar G, Gibney N. Endovascular repair in traumatic thoracic aortic injuries: comparison with open surgical repair. J Vasc Interv Radiol (2008) 19(4):479–86. doi:10.1016/j.jvir.2007.10.022
22. Feezor RJ, Hess PJ Jr, Martin TD, Klodell CT, Beaver TM, Lottenberg L, et al. Endovascular treatment of traumatic thoracic aortic injuries. J Am Coll Surg (2009) 208(4):510–6. doi:10.1016/j.jamcollsurg.2009.01.012
23. Urgnani F, Lerut P, Da Rocha M, Adriani D, Leon F, Riambau V. Endovascular treatment of acute traumatic thoracic aortic injuries: a retrospective analysis of 20 cases. J Thorac Cardiovasc Surg (2009) 138(5):1129–38. doi:10.1016/j.jtcvs.2008.10.057
24. Hoffer EK, Forauer AR, Silas AM, Gemery JM. Endovascular stent-graft or open surgical repair for blunt thoracic aortic trauma: systematic review. J Vasc Interv Radiol (2008) 19(8):1153–64. doi:10.1016/j.jvir.2008.05.012
25. Xenos ES, Abedi NN, Davenport DL, Minion DJ, Hamdallah O, Sorial EE, et al. Meta-analysis of endovascular vs open repair for traumatic descending thoracic aortic rupture. J Vasc Surg (2008) 48(5):1343–51. doi:10.1016/j.jvs.2008.04.060
26. Murad MH, Rizvi AZ, Malgor R, Carey J, Alkatib AA, Erwin PJ, et al. Comparative effectiveness of the treatments for thoracic aortic transection [corrected]. J Vasc Surg (2011) 53(1):193–199.e1–21. doi:10.1016/j.jvs.2010.08.028
27. Lee WA, Matsumura JS, Mitchell RS, Farber MA, Greenberg RK, Azizzadeh A, et al. Endovascular repair of traumatic thoracic aortic injury: clinical practice guidelines of the Society for Vascular Surgery. J Vasc Surg (2011) 53(1):187–92. doi:10.1016/j.jvs.2010.08.027
28. Erbel R, Aboyans V, Boileau C, Bossone E, Bartolomeo RD, Eggebrecht H, et al. 2014 ESC guidelines on the diagnosis and treatment of aortic diseases: document covering acute and chronic aortic diseases of the thoracic and abdominal aorta of the adult. The Task Force for the diagnosis and treatment of aortic diseases of the European Society of Cardiology (ESC). Eur Heart J (2014) 35(41):2873–926. doi:10.1093/eurheartj/ehu281
29. Writing Committee, Riambau V, Böckler D, Brunkwall J, Cao P, Chiesa R, et al. Editor’s choice – management of descending thoracic aorta diseases: clinical practice guidelines of the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg (2017) 53(1):4–52. doi:10.1016/j.ejvs.2016.06.005
30. Bottet B, Bouchard F, Peillon C, Baste JM. When and how should we manage thoracic aortic injuries in the modern era? Interact Cardiovasc Thorac Surg (2016) 23(6):970–5. doi:10.1093/icvts/ivw247
31. Demetriades D, Velmahos GC, Scalea TM, Jurkovich GJ, Karmy-Jones R, Teixeira PG, et al. Blunt traumatic thoracic aortic injuries: early or delayed repair – results of an American Association for the Surgery of Trauma prospective study. J Trauma (2009) 66(4):967–73. doi:10.1097/TA.0b013e31817dc483
32. Shan JG, Zhai XM, Liu JD, Yang WG, Xue S. Thoracic endovascular aortic repair for traumatic thoracic aortic injury: a single-center initial experience. Ann Vasc Surg (2016) 32:104–10. doi:10.1016/j.avsg.2015.09.023
33. Dubose JJ, Azizzadeh A, Estrera AL, Safi HJ. Contemporary management of blunt aortic trauma. J Cardiovasc Surg (Torino) (2015) 56(5):751–62.
34. Jonker FH, Giacovelli JK, Muhs BE, Sosa JA, Indes JE. Trends and outcomes of endovascular and open treatment for traumatic thoracic aortic injury. J Vasc Surg (2010) 51(3):565–71. doi:10.1016/j.jvs.2009.10.046
35. Martinelli O, Malaj A, Gossetti B, Bertoletti G, Bresadola L, Irace L. Outcomes in the emergency endovascular repair of blunt thoracic aortic injuries. J Vasc Surg (2013) 58(3):832–5. doi:10.1016/j.jvs.2013.02.243
36. Tang GL, Tehrani HY, Usman A, Katariya K, Otero C, Perez E, et al. Reduced mortality, paraplegia, and stroke with stent graft repair of blunt aortic transections: a modern meta-analysis. J Vasc Surg (2008) 47(3):671–5. doi:10.1016/j.jvs.2007.08.031
37. Neschis DG, Scalea TM, Flinn WR, Griffith BP, et al. Blunt aortic injury. N Engl J Med (2008) 359(16):1708–16. doi:10.1056/NEJMra0706159
38. Goldstein BH, Hirsch R, Zussman ME, Vincent JA, Torres AJ, Coulson J, et al. Percutaneous balloon-expandable covered stent implantation for treatment of traumatic aortic injury in children and adolescents. Am J Cardiol (2012) 110(10):1541–5. doi:10.1016/j.amjcard.2012.06.063
39. Raupach J, Ferko A, Lojik M, Krajina A, Harrer J, Dominik J. Endovascular treatment of acute and chronic thoracic aortic injury. Cardiovasc Intervent Radiol (2007) 30(6):1117–23. doi:10.1007/s00270-007-9053-2
40. van Prehn J, van Herwaarden JA, Muhs BE, Arnofsky A, Moll FL, Verhagen HJ, et al. Difficulties with endograft sizing in a patient with traumatic rupture of the thoracic aorta: the possible influence of hypovolemic shock. J Vasc Surg (2008) 47(6):1333–6. doi:10.1016/j.jvs.2007.12.036
41. Starnes BW, Dwivedi AJ, Giglia JS, Woo K, Yeh C; TRANSFIX Study Investigators. Endovascular repair of blunt thoracic aortic injuries with the Zenith Alpha thoracic device: updated outcomes from the TRANSFIX study. J Vasc Surg (2016) 64(2):550–1. doi:10.1016/j.jvs.2016.05.035
42. Peterson BG, Eskandari MK, Gleason TG, Morasch MD. Utility of left subclavian artery revascularization in association with endoluminal repair of acute and chronic thoracic aortic pathology. J Vasc Surg (2006) 43(3):433–9. doi:10.1016/j.jvs.2005.11.049
43. Piffaretti G, Carrafiello G, Ierardi AM, Mariscalco G, Macchi E, Castelli P, et al. Thoracic endovascular aortic repair for blunt thoracic aortic injuries in complex aortic arch vessels anatomies. Ann Vasc Surg (2015) 29(6): 1320.e11–5. doi:10.1016/j.avsg.2015.03.052
44. Piffaretti G, Benedetto F, Menegolo M, Antonello M, Tarallo A, Grego F, et al. Outcomes of endovascular repair for blunt thoracic aortic injury. J Vasc Surg (2013) 58(6):1483–9. doi:10.1016/j.jvs.2013.05.096
45. Matsumura JS, Lee WA, Mitchell RS, Farber MA, Murad MH, Lumsden AB, et al. The Society for Vascular Surgery Practice Guidelines: management of the left subclavian artery with thoracic endovascular aortic repair. J Vasc Surg (2009) 50(5):1155–8. doi:10.1016/j.jvs.2009.08.090
46. Midgley PI, Mackenzie KS, Corriveau MM, Obrand DI, Abraham CZ, Fata P, et al. Blunt thoracic aortic injury: a single institution comparison of open and endovascular management. J Vasc Surg (2007) 46(4):662–8. doi:10.1016/j.jvs.2007.05.061
47. Ktenidis K, Lioupis A, Giannopoulos A, Ginis G, Kiskinis D. Management of traumatic aortic isthmus rupture in case of aberrant right subclavian artery (arteria lusoria). Ann Vasc Surg (2012) 26(3):e1–5. doi:10.1016/j.avsg.2011.05.041
48. Khoynezhad A, Azizzadeh A, Donayre CE, Matsumoto A, Velazquez O, White R, et al. Results of a multicenter, prospective trial of thoracic endovascular aortic repair for blunt thoracic aortic injury (RESCUE trial). J Vasc Surg (2013) 57(4):899–905.e1. doi:10.1016/j.jvs.2012.10.099
49. Katsargyris A, Verhoeven EL. Part two: against the motion. All TEVAR patients do not require lifelong follow-up by annual CTA/MRA.[Con]. Eur J Vasc Endovasc Surg (2012) 44(6):538–41. doi:10.1016/j.ejvs.2012.09.014
Keywords: aortic, isthmic, blunt trauma, rupture, endovascular, TEVAR
Citation: Patelis N, Katsargyris A and Klonaris C (2017) Endovascular Repair of Traumatic Isthmic Ruptures: Special Concerns. Front. Surg. 4:32. doi: 10.3389/fsurg.2017.00032
Received: 16 April 2017; Accepted: 26 May 2017;
Published: 12 June 2017
Edited by:
Efthymios Avgerinos, University of Pittsburgh Medical Center, United StatesReviewed by:
Efstratios Georgakarakos, Democritus University of Thrace, GreeceCopyright: © 2017 Patelis, Katsargyris and Klonaris. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nikolaos Patelis, cGF0ZWxpc25AZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.