
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CURRICULUM, INSTRUCTION, AND PEDAGOGY article
Front. Surg. , 09 August 2016
Sec. Visceral Surgery
Volume 3 - 2016 | https://doi.org/10.3389/fsurg.2016.00047
This article is part of the Research Topic Education, Training and Centers in Surgery View all 5 articles
 Ferdinand Köckerling1*
Ferdinand Köckerling1* Michael Pass1Petra Brunner1Matthias Hafermalz1Stefan Grund1Joerg Sauer2Volker Lange1Wolfgang Schröder3
Michael Pass1Petra Brunner1Matthias Hafermalz1Stefan Grund1Joerg Sauer2Volker Lange1Wolfgang Schröder3
Introduction: The learning curve in minimally invasive surgery is much longer than in open surgery. This is thought to be due to the higher demands made on the surgeon’s skills. Therefore, the question raised at the outset of training in laparoscopic surgery is how such skills can be acquired by undergoing training outside the bounds of clinical activities to try to shorten the learning curve. Simulation-based training courses are one such model.
Methods: In 2011, the surgery societies of Germany adopted the “laparoscopic surgery curriculum” as a recommendation for the learning content of systematic training courses for laparoscopic surgery. The curricular structure provides for four 2-day training courses. These courses offer an interrelated content, with each course focusing additionally on specific topics of laparoscopic surgery based on live operations, lectures, and exercises carried out on bio simulators.
Results: Between 1st January, 2012 and 31st March, 2016, a total of 36 training courses were conducted at the Vivantes Endoscopic Training Center in accordance with the “laparoscopic surgery curriculum.” The training courses were attended by a total of 741 young surgeons and were evaluated as good to very good during continuous evaluation by the participants.
Conclusion: Training courses based on the “laparoscopic surgery curriculum” for acquiring skills in laparoscopy are taken up and positively evaluated by young surgeons.
The term “learning curve” as currently employed in surgery means that inexperienced surgeons have not only a longer operating time but also a higher complication rate (1). Mastery of the learning curve in surgery can no longer be merely left to “trial and error” in routine clinical practices but, instead, calls for the development, definition, and introduction of models suitable for training surgeons without presenting any higher risk to patients (1). Simulation-based training courses are one such model (1).
The learning curve in laparoscopic surgery is much longer than in open surgery. In the literature, the learning curve for laparoscopic cholecystectomy is given as 30 procedures (2, 3), for endoscopic inguinal hernia surgery as 60 procedures (4), for laparoscopic gastric bypass as 100 procedures (5), and for laparoscopic colorectal surgery as 88–152 procedures (6). This is thought to be due to the more exacting demands made on the surgeon’s skills (7). Among the factors militating against rapid acquisition of skills in laparoscopic surgery are the low number of cases suitable for teaching operations, difficulties with the video-eye-hand coordination, altered perceptions of depth, and laparoscopic suturing (8). This means that, often, even after completion of specialist surgical training, some surgeons have shortcomings when it comes to laparoscopic suturing techniques, bimanual coordination, and mastery of challenging anatomic situations (9).
Therefore, the question raised at the outset of training in laparoscopic surgery is how such skills, i.e., the skills and competencies to perform laparoscopic surgery, can be acquired by undergoing training outside the bounds of clinical activities to try to shorten the learning curve.
In a systematic review, Zendejas et al. (7) demonstrated that laparoscopic techniques can be learned more effectively in a simulation-based training course compared with when learning such techniques only during clinical training. Training on expensive virtual reality trainers is no better than when using the more favorably priced pelvic trainers and boxes with porcine organs models from abattoirs (7, 10).
Likewise, a Cochrane review identified advantages for acquiring skills in laparoscopic surgery by first participating in simulation-based training courses on pelvic trainers (11). Simulation-based training helps to shorten the operating time and enhance the ability to implement surgical techniques. The skills learned in training courses can be immediately applied for the patient in the operating room (12–15).
In a prospective randomized trial on learning the total extraperitoneal patch plasty (TEP) technique in endoscopic inguinal hernia surgery, Zendejas et al. (16) demonstrated that surgeons who had undergone such simulation-based training had significantly shorter operating times, better performance scores, and fewer intraoperative and postoperative complications than those surgeons who had not taken part in such a training course.
Based on evidence-based data, it is urgently recommended that young surgeons in training as general and visceral surgeons take part in such training courses. Below are now described the experiences gained in Germany with the introduction of a curricular concept for simulation-based training in minimally invasive surgery, which was offered in parallel to the normal specialist surgical training program.
Based on the evidence presented above, the board of directors (M. Strik, Berlin, K. Ludwig, Rostock, R. Bittner, Stuttgart, W. Schwenk, Hamburg, M. Walz, Essen, Ferdinand Köckerling, Berlin) of the Minimally Invasive Surgery Working Group (CAMIC) of the German Society of General and Visceral Surgery (DGAV), in 2011, adopted the “laparoscopic surgery curriculum” as a recommendation for the learning content of systematic training courses in laparoscopic surgery.
The curricular structure provides for four 2-day training courses with an interrelated content and with each course focusing additionally on specific topics of laparoscopic surgery. The following key courses are recommended:
Course I: fundamentals of minimally invasive surgery and laparoscopic cholecystectomy (Table 1)
Course II: endoscopic hernia surgery [TEP, transabdominal preperitoneal patch plasty (TAPP), laparoscopic intraperitoneal onlay mesh (lap IPOM), and laparoscopic fundoplication] (Table 2)
Course III: laparoscopic suturing, knot-tying, clipping, stapling, laparoscopic hemostasis, laparoscopic appendectomy, adhesiolysis, stomach wedge resection and gastroenterostomy, and Roux-Y anastomosis (Table 3)
Course IV: laparoscopic colorectal surgery, rectopexy, sigmoid and rectal resection, total mesorectal excision (TME), right hemicolectomy and stoma placement, and intraabdominal intestinal resection (Table 4).
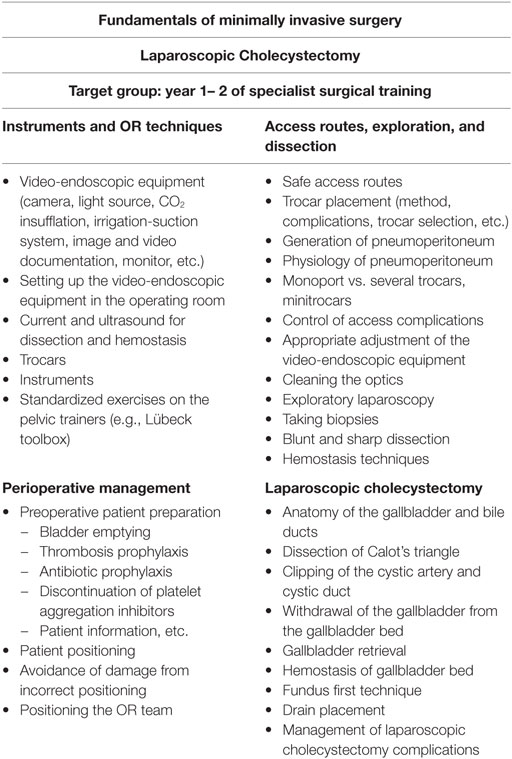
Table 1. Course I content.
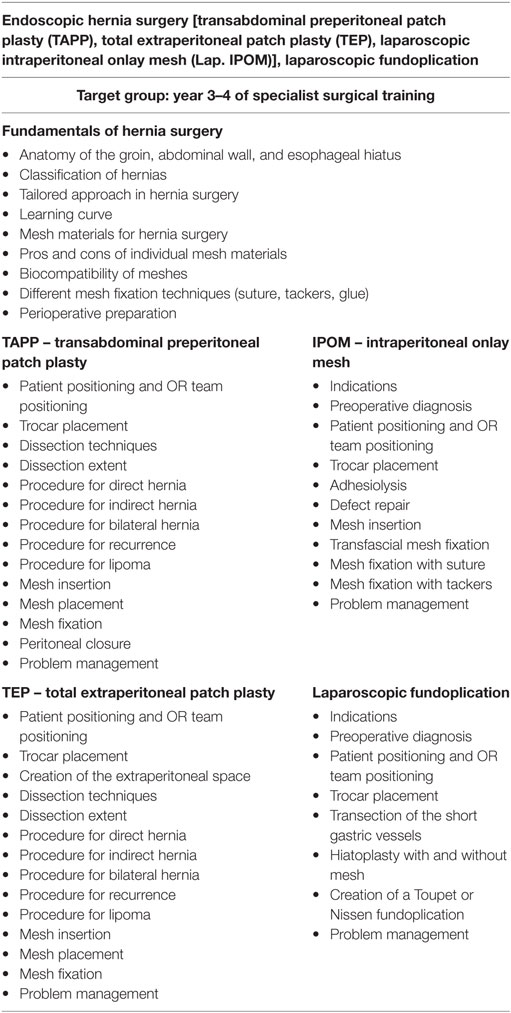
Table 2. Course II content.
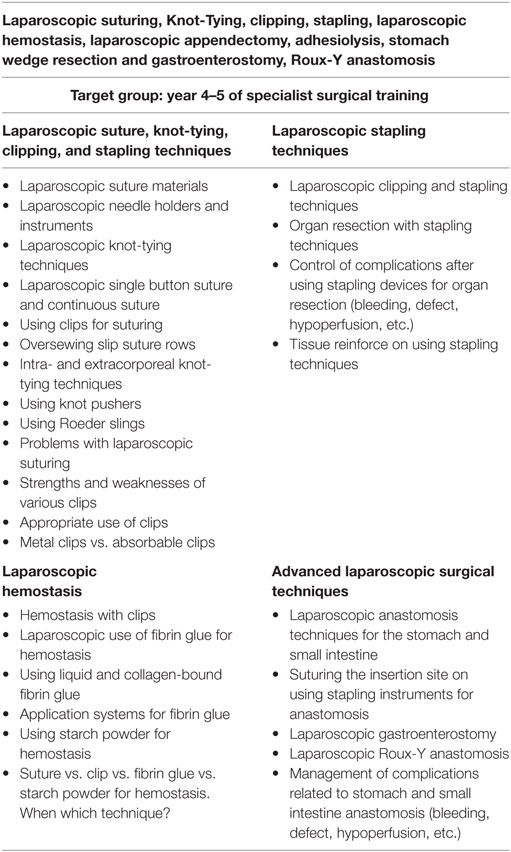
Table 3. Course III content.
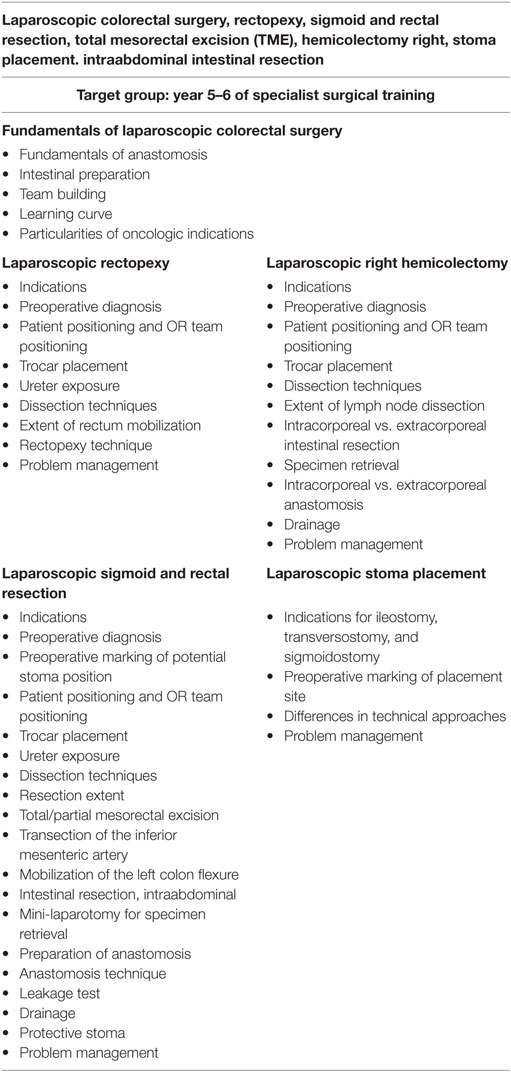
Table 4. Course IV content.
Based on that recommendation, since 2012, the Federal Association of German Surgeons (BDC) in collaboration with the CAMIC and DGAV have been running regular simulation-based training courses at the Vivantes Endoscopic Training Center of the Department of Surgery – Visceral and Vascular Surgery – of the Vivantes Hospital Berlin (Medical Director: Prof. Dr. med. Ferdinand Köckerling).
The recommendation is that young surgeons attend the training courses in the following order: “laparoscopic cholecystectomy” course in year 1–2; “endoscopic hernia surgery (TEP, TAPP, lap. IPOM)” course in year 3–4; course; “laparoscopic suturing, knot-tying, clipping, stapling, laparoscopic hemostasis, laparoscopic appendectomy, adhesiolysis, stomach wedge resection and gastroenterostomy, and Roux-Y anastomosis” course in year 4–5; and the “Laparoscopic colorectal surgery” course in year 5–6. Currently, there is no evaluation of the participants through implementation of a score to get permission for the next course level.
The course content is imparted to participants based on live operations from two operating rooms at the Vivantes Hospital Berlin (Figure 1) and lectures (Figure 2). But, the key element is the training units carried out on bio simulators (Figure 3), which give course attendees the chance to thoroughly practice all manual skills using porcine organ models from an abattoir or chickens from the supermarket. To that effect, the same video-endoscopic equipment, as used in the operating room, is available (Figure 3). The course trainers are available to assist the attendees throughout. The bio simulators confront trainees with a situation that mimics that which they have to master in an actual surgical setting. This practical test serves to make each participant aware of his/her technical shortcomings in performing surgery, which must now be overcome. Since participation in all four training courses is mandatory for attainment of the “laparoscopic surgery curriculum” overall certificate, the progress made by individual trainees can be well monitored over the years. Since 12 fully equipped working places traineeships are available at the Vivantes Endoscopic Training Center, thanks to the support from the firms Storz and Medtronic, up to 24 colleagues can participate in each training course (Figure 4).

Figure 1. Live transmission from two operating rooms to the lecture room.

Figure 2. Lectures on specific key topics.

Figure 3. Practical training on the bio simulator with (porcine) organs from the abattoir or chickens from the supermarket with assistance from experienced laparoscopic surgeons.

Figure 4. In the Vivantes Endoscopic Training Center, up to 24 young surgeons can be trained simultaneously at 12 fully equipped working places workstations.
Between 1st January, 2012 and 31st March, 2016, a total of 36 training courses were conducted at the Vivantes Endoscopic Training Center in accordance with the “laparoscopic surgery curriculum.” The training courses were attended by a total of 741 young surgeons, and each course was evaluated on completion. Attendees were asked to evaluate the course in terms of its learning content, scope of theoretical presentations, didactic concept, duration of exercises, quality of the live operations, and overall assessment. Responses were graded as follows: 1 (very good), 2 (good), 3 (satisfactory), 4 (sufficient), 5 (deficient), and 6 (insufficient). In general, participants evaluated the courses as being very good to good (Table 5). The fact that, in the meantime, 49 participants of the Professional Association of German Surgeons attained the overall certificate documenting attendance of all four courses demonstrates the high acceptance of the curricular concept for teaching minimally invasive surgery skills through the combination of live surgery, lectures, and practical training on a bio simulator.
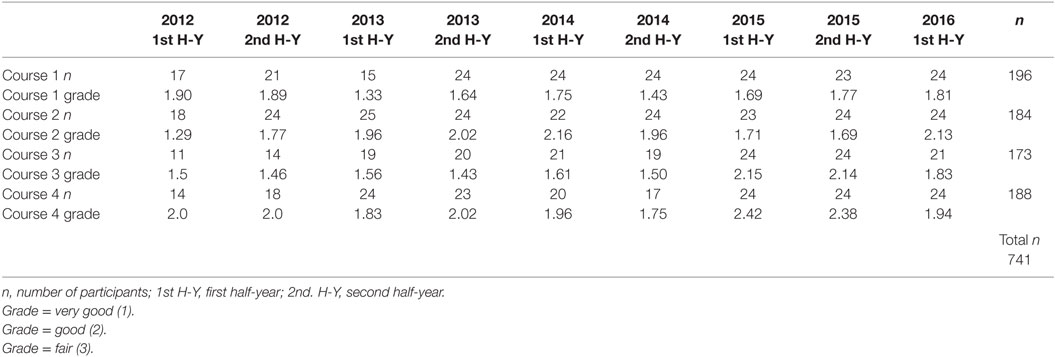
Table 5. Number of participants and their evaluation of the course content by grades.
In 2011, the German surgery societies adopted the “laparoscopic surgery curriculum” concept for simulation-based training in laparoscopic surgery. The curricular structure provides for four 2-day training courses with an interrelated, tiered content. The courses are designed to be attended in parallel to the normal specialist surgical training program. The course content is imparted based on live operations, lectures, and exercises carried out on bio simulators. In collaboration with the Professional Association of German Surgeons, 36 courses have, in the meantime, been held at the Vivantes Endoscopic Training Center in Berlin with a total of 741 participants. The courses were evaluated by attendees as being very good and good, i.e., trainees believed they had benefited from the courses. The advantage of this course concept is its direct relevance to the clinical setting with regular facilities for transmission of live operations. This also provides for close supervision by experienced surgeons in minimally invasive surgery. The dedicated training center has a training capacity for 24 trainees. Exercises carried out on biological specimens from the abattoir or supermarket permit intensive training, as resources are not limited. In a systematic review Zendejas et al. (7) demonstrated that laparoscopic techniques can be learned more effectively in a simulation-based training course compared with when learning such techniques only during clinical training.
The skills learned in simulation-based training courses can be immediately applied for the patient in the operating room (12–15). Hence, simulation-based training helps to master the learning curve in minimally invasive surgery and enhance conduct of minimally invasive surgical procedures during the learning curve. Therefore, it is urgently recommended that young surgeons in training participate in such simulation-based courses. Bio simulators, which are used for practicing surgical skills on organ models in the pelvic trainer with standard video-endoscopic equipment, are currently the most cost-effective option. As such, the satisfaction ratings reported by course participants are very high. The positive evaluation by the course attendees, thus, attests to the successful implementation of the scientifically based “laparoscopic surgery curriculum” course concept.
In summary, it can be stated that, participation in the curricular-structured courses in parallel to the normal specialist surgical training program helps to master the learning curve in minimally invasive surgery with simulation-based training and, accordingly, has been evaluated as being very positive by the young surgeons. As consequence, the implementation of such structured educational programs in laparo-endoscopic surgery in every surgical institution performing laparo-endoscopic surgery must be underlined.
All authors are actively involved for many years in the “laparoscopic surgery curriculum.”
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Aggarwal R, Mytton OT, Derbrew M, Hananel D, Heydenburg M, Issenberg B, et al. Training and simulation for patient safety. Qual Saf Health Care (2010) 19(Suppl 2):i34–43. doi: 10.1136/qshc.2009.038562
2. Cagir B, Rangraj M, Maffuci L, Herz BL. The learning curve for laparoscopic cholecystectomy. J Laparoendosc Surg (1994) 4(6):419–27. doi:10.1089/lps.1994.4.419
3. Moore MJ, Bennett CL. The learning curve for laparoscopic cholecystectomy. The Southern Surgeons Club. Am J Surg (1995) 170(1):55–9. doi:10.1016/S0002-9610(99)80252-9
4. Choi YY, Kim Z, Hur KY. Learning curve for laparoscopic totally extraperitoneal repair of inguinal hernia. Can J Surg (2012) 55(1):33–6. doi:10.1503/cjs.019610
5. Schauer P, Ikramuddin S, Hamad G, Gourash W. The learning curve for laparoscopic Roux-en-Y gastric bypass is 100 cases. Surg Endosc (2003) 17:212–5. doi:10.1007/s00464-002-8857-z
6. Miskovic D, Ni M, Wyles SM, Tekkis P, Hanna GB. Learning curve and case selection in laparoscopic colorectal surgery: systematic review and international multicenter analysis of 4852 cases. Dis Colon Rectum (2012) 55(12):1300–10. doi:10.1097/DCR.0b013e31826ab4dd
7. Zendejas B, Brydes B, Hamstra SJ, Cook DA. State of the evidence on simulation-based training for laparoscopic surgery. Ann Surg (2013) 257:586–93. doi:10.1097/SLA.0b013e318288c40b
8. Fuchs Weizman N, Maurer R, Einarsson JI, Vitonis AF, Cohen SL. Survey on barriers to adoption of laparoscopic surgery. J Surg Educ (2015) 72(5):985–94. doi:10.1016/j.jsurg.2015.04.001
9. Nepomnayshy D, Alseidi AA, Fitzbibbons SC, Stefanidis D. Identifying the need for and content of an advanced laparoscopic skills curriculum: results of a national survey. Am J Surg (2015). doi:10.1016/j.amjsurg.2015.10.009
10. Van Bruwaene S, Schijven MP, Naplitano D, De Win G, Miserez M. Porcine cadaver organ or virtual-reality simulation training for laparoscopic cholecystectomy: a randomized, controlled trial. J Surg Educ (2015) 72(3):483–90. doi:10.1016/j.jsurg.2014.11.015
11. Gurusamy KS, Nagendran M, Toon CD, Davidson BR. Laparoscopic surgical box model training for surgical trainees with limited prior laparoscopic experience. Cochrane Database Syst Rev (2014):CD010478. doi:10.1002/14651858.CD010478.pub.2
12. Dawe SR, Windsor JA, Broeders JA, Cregan PC, Hewett PJ, Maddern GJ. A systematic review of surgical skills transfer after simulation-based training: laparoscopic cholecystectomy and endoscopy. Ann Surg (2014) 259(2):236–48. doi:10.1097/SLA.0000000000000245
13. Dawe SR, Pena GN, Windsor JA, Broeders JA, Cregan PC, Hewett PJ, et al. Systematic review of skills transfer after surgical simulation-based training. Br J Surg (2014) 101(9):1063–76. doi:10.1002/bjs.9482
14. Vanderbilt AA, Grover AC, Pastis NJ, Feldman M, Granados DD, Murithi LK, et al. Randomized controlled trials: a systematic review of laparoscopic surgery and simulation-based training. Glob J Health Sci (2014) 7(2):310–27. doi:10.5539/gjhs.v7n2p310
15. Barussaud ML, Roussel B, Neurett G, Sulpice L, Meunier B, Regenet N, et al. French intensive training course in laparoscopic surgery (HUGOFirst) on live porcine models: validation of a performance assessment scale and residents’ satisfaction in a prospective study. J Visc Surg (2015). doi:10.1016/jjviscsurg.2015.10.005
Keywords: simulation-based training, laparoscopic surgery curriculum, skills in laparoscopic surgery, young surgeons, simulation-based courses
Citation: Köckerling F, Pass M, Brunner P, Hafermalz M, Grund S, Sauer J, Lange V and Schröder W (2016) Simulation-Based Training – Evaluation of the Course Concept “Laparoscopic Surgery Curriculum” by the Participants. Front. Surg. 3:47. doi: 10.3389/fsurg.2016.00047
Received: 02 June 2016; Accepted: 25 July 2016;
Published: 09 August 2016
Edited by:
Hubert Scheuerlein, Chefarzt der Klinik für Allgemein- und Visceralchirurgie, GermanyReviewed by:
Aristotelis Perrakis, University of Erlangen-Nuremberg, GermanyCopyright: © 2016 Köckerling, Pass, Brunner, Hafermalz, Grund, Sauer, Lange and Schröder. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ferdinand Köckerling, ZmVyZGluYW5kLmtvZWNrZXJsaW5nQHZpdmFudGVzLmRl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.