
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Sports Act. Living , 10 March 2025
Sec. Injury Prevention and Rehabilitation
Volume 7 - 2025 | https://doi.org/10.3389/fspor.2025.1565900
This article is part of the Research Topic Muscle and Tendon Injuries in Sporting and Tactical Populations: Mechanisms, Prevention and Rehabilitation View all 9 articles
 Álvaro Velarde-Sotres1,2,3
Álvaro Velarde-Sotres1,2,3 Antonio Bores-Cerezal1
Antonio Bores-Cerezal1 Josep Alemany-Iturriaga4,5,6
Josep Alemany-Iturriaga4,5,6 Julio Calleja-González7*
Julio Calleja-González7*
Background: Scientific research should be carried out to prevent sports injuries. For this purpose, new assessment technologies must be used to analyze and identify the risk factors for injury. The main objective of this systematic review was to compile, synthesize and integrate international research published in different scientific databases on Countermovement Jump (CMJ), Functional Movement Screen (FMS) and Tensiomyography (TMG) tests and technologies for the assessment of injury risk in sport. This way, this review determines the current state of the knowledge about this topic and allows a better understanding of the existing problems, making easier the development of future lines of research.
Methodology: A structured search was carried out following the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines and the PICOS model until November 30, 2024, in the MEDLINE/PubMed, Web of Science (WOS), ScienceDirect, Cochrane Library, SciELO, EMBASE, SPORTDiscus and Scopus databases. The risk of bias was assessed and the PEDro scale was used to analyze methodological quality.
Results: A total of 510 articles were obtained in the initial search. After inclusion and exclusion criteria, the final sample was 40 articles. These studies maintained a high standard of quality. This revealed the effects of the CMJ, FMS and TMG methods for sports injury assessment, indicating the sample population, sport modality, assessment methods, type of research design, study variables, main findings and intervention effects.
Conclusions: The CMJ vertical jump allows us to evaluate the power capacity of the lower extremities, both unilaterally and bilaterally, detect neuromuscular asymmetries and evaluate fatigue. Likewise, FMS could be used to assess an athlete's basic movement patterns, mobility and postural stability. Finally, TMG is a non-invasive method to assess the contractile properties of superficial muscles, monitor the effects of training, detect muscle asymmetries, symmetries, provide information on muscle tone and evaluate fatigue. Therefore, they should be considered as assessment tests and technologies to individualize training programs and identify injury risk factors.
Systematic Review Registration: https://www.crd.york.ac.uk/PROSPERO/view/CRD42024607563, PROSPERO (CRD42024607563).
Scientific research should be carried out to prevent sports injuries. For this purpose, valid and reliable assessment methods are needed to reduce the number of sports injuries (1–6). As a result of the investigations (3, 5) different methods and technologies have been proposed to assess and identify injury risk factors.
Sports injuries can affect the health and performance of athletes. Therefore, studies and research should be conducted to assess the risk of injury in athletes, thus contributing new knowledge to science (3, 5). In addition, there is a need to preserve the health and well-being of professional players when faced with a high frequency of extremely demanding matches (7). Consequently, strategies must be designed to optimize player availability and minimize factors such as fatigue (7).
These risk factors for sports injuries include characteristics of the athletes, sports and the environment (4). Another factor that has a decisive influence on the probability of suffering an injury as a result of sports practice is the workload (8). Therefore, it is necessary to analyze and study the risk factors that can produce an injury (1–6).
Based on these criteria, there is a need to assess the athlete's risk of injury, taking into account the different intrinsic and extrinsic risk factors that can have a decisive influence on an injury (1, 4). Among the factors to be studied are asymmetries (9), neuromuscular imbalances between limbs (4), muscle stiffness (10, 11), postural control deficits (12, 13) or fatigue (14).
To carry out these analyses, functional tests and muscle assessment methods or technologies are used to detect fatigue, monitor the training load, detect asymmetries or functional imbalances, as possible risk factors for injury (3, 5, 8, 14, 15).
One of the functional tests used to evaluate performance during the vertical jump is the Countermovement Jump (CMJ), as it is a Gold Standard (16). The CMJ is a valid and reliable tool (16) for assessing lower limb power capacity, either unilaterally or bilaterally, as well as detecting asymmetries between limbs.
Similarly, the performance of the CMJ jump on a jumping platform allows the measurement of flight time, contact time, height and power. Starting from this fundamental database, the software designed allows to obtain in real time these parameters linked to the athlete's performance (16). The CMJ can also be used to assess neuromuscular fatigue.
Along with this test, the Functional Movement Screen (FMS) is a valid and reliable tool (12, 13, 17) to assess an individual's fundamental movement patterns. Additionally, this system can be used at the end of the rehabilitation process to help determine if an athlete is ready to return to training. The main purpose of the FMS tool is to identify functional asymmetries and postural or motor control deficits (12, 13).
The FMS is composed of 7 fundamental movement patterns (test), with a numerical value from 0 to 3 according to certain observable markers that require a balance between mobility and stability (12, 13).
Another tool used in the evaluation is Tensiomyography (TMG) is a valid and reliable tool (10, 11, 18, 19) to evaluate the contractile properties of superficial muscles. TMG is a technique to evaluate the mechanical muscle response based on the displacement of the radial muscle belly to a single electrical stimulus (9). As a result of this electrical stimulus, a displacement-time curve is recorded where the following parameters are integrated: maximum radial muscle displacement (Dm), contraction time (Tc), delay time (Td), sustained contraction time (Ts) and relaxation time (Tr) (10, 11, 18, 19).
TMG is a non-invasive tool (11, 18, 19) used to monitor the effects of training during a specific period or throughout the season, to detect bilateral muscle asymmetries, to detect fatigue and to individualize training loads for athletes (11, 18, 19).
Given the existing reality, it is expected to analyse the current technologies, considering the starting existing capacities and the experts in the physical activity and sports, biomechanics and medicine, using the application of the information technology.
Individualized training is key to improving sports performance and preventing injuries. To do so, it is necessary to use new technologies that allow for the assessment of injury risk.
To date, and to the best of our knowledge, there are no previous level studies or evidence 1A demonstrating the use of CMJ, FMS and TMG tool variables for injury assessment.
Therefore, the main aim of this systematic review was to compile, synthesize and integrate international research published in different scientific databases on CMJ, FMS and TMG tests and technologies for the assessment of injury risk in sport. This way, this review determines the current state of the knowledge about this topic and allows a better understanding of the existing problems, making easier the development of future lines of research.
This article is a systematic review focused on the methods of sports injury assessment. This systematic review was carried out following the guidelines of the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA®) (20) guidelines, which helped to improve the integrity. And registered at PROSPERO (ID = CRD42024607563). The methodological issues were solved with the guidance of the Cochrane Handbook for Systematic Reviews of Interventions (21).
The PICOS model was used to determine the inclusion criteria (22): P (Population): “athletes of different sports,” I (Intervention): “injury prevention,” C (Comparators): ““group comparison with multidisciplinary interventions and controls,” O (Outcome): “physical and/or neuromuscular performance measurements, physiological responses, and risk of injury,” and S (study design): “any type of design”.”
A structured search was conducted in MEDLINE/PubMed, Web of Science (WOS), ScienceDirect, Cochrane Library, SciELO, EMBASE, SPORTDiscus and Scopus. The investigation ended on November 30, 2024. Search terms included a mix of medical subject headings (MeSH) and free-text words for key concepts related to assessment methods, high performance athletes and sports injury prevention. Specifically, we used the following search equation: [“injury prevention” (MeSH Terms) OR “injury assessment” (All Fields) OR “sports injuries” (All Fields) OR “injury risk factors” (All Fields)] AND [“Assessment test” (MeSH Terms) OR “TMG” (All Fields)] OR “FMS” (All Fields) OR “CMJ” (All Fields)] AND [“sport” (MeSH Terms) OR “football” (All Fields)] OR “sports” (All Fields) OR “athletes” (All Fields)]. Through this equation, all relevant articles in the field were obtained. The reference sections of all identified articles were also examined by applying the “snowball methods” strategy (23), based on examining the reference sections of the identified articles. All titles and abstracts from the search were cross-referenced to identify duplicates and any potential missing studies (Á.V.-S. and J.C.-G). Titles and abstracts were screened for a subsequent full-text review. The search for published studies was independently performed by two different authors (Á.V.-S. and J.C.-G) and disagreements were resolved through discussions between them.
We selected studies providing effectivity results in terms of diagnostic accuracy or diagnostic performance for the different tests used in the assessment of sports injuries were included. The systematic review included original studies of diagnostic tests designs included and systematic reviews, meta-analysis, abstracts of conferences and opinion articles were excluded. In addition, we selected studies that contained a minimum of 10 participants. And for effectiveness studies only those that used at least one technique for the prevention and analysis of sports injuries were considered. The CMJ, the FMS and the TMG were considered as comparison techniques.
For the articles obtained in the search, the following inclusion criteria were applied to final selected studies: (I) studies published in peer-reviewed journals and full text available; (II) the articles examined the effects of sports injury assessment methods; (III) original articles published in peer-reviewed peer-reviewed journals with impact factor; (IV) participants were assessed with the CMJ, FMS or TMG; (V) the study population consisted of athletes; (VI) included the assessment of the risk of injury; (VII) performed on any number or type of athlete regardless of category, experience, competitive level or sex; (VIII) published in English. The following exclusion criteria were applied to the experimental protocols of the investigation: (I) the absence of reliable measurements; (II) studies with less than 10 participants; (III) studies conducted using participants with a previous cardiovascular or musculoskeletal disorder; (IV) studies that will not be performed with athletes; (V) abstracts, non-peer-reviewed papers, and book chapters.
Titles and abstracts of publications identified by the search strategy were screened for a subsequent full-text review and were cross-referenced to identify duplicates. All trials assessed for eligibility and classified as relevant were retrieved, and the full text was peer reviewed (Á.V.-S. and J.C.-G). Moreover, the reference section of all relevant articles was also examined using the snowball (23). Based on the information within the full articles, the inclusion and exclusion criteria were used to select the trials eligible for inclusion in this systematic review. Disagreements were resolved through discussions between two authors (Á.V.-S. and J.C.-G).
Once the inclusion/exclusion criteria were applied to each study, the following data were extracted: study source (author/authors and year of publication); population of the sample, indicating the number of participants; sport modality; assessment methods and tests; type of research design; study variables; main findings; characteristics of the intervention; significant differences among the study groups and effects of the intervention.
For each study, we carefully collected information for all eligible publications. Average (±) data and standard deviation (SD) data and size of the sample were extracted from the tables of all the included documents. Subsequently, disagreements were resolved through discussion until a consensus was achieved.
Methodological quality and risk of bias were assessed by two authors independently (Á.V.-S. and D.M.-J), and disagreements were resolved by third-party evaluation (J.C.-G), in accordance with the Cochrane Collaboration Guidelines (24).
In the Cochrane Risk of Bias tool, the following items were included and divided into different domains: (1) selection bias (items, random sequence generation, allocation and concealment), (2) performance bias (blinding of participants and personnel), (3) detection bias (blinding of outcome assessment), (4) attrition bias (incomplete outcome data), (5) reporting bias (selective reporting), and (6) other bias (other sources of bias).
For each investigation, criteria were shown as “low” if the criteria were fulfilled for a low-risk bias (improbable to severely alter the results) or “high” if the criteria were high risk bias (severely weakening the reliability of the results). If the risk of bias was unknown, it was considered “not clear” (it brings doubts about the results).
The systematic review was based on the established principles by the PRISMA statement (20), a verification list which has as main aim to look for the transparency of the important systematic reviews in the scientific rating of these studies. It has got 27 items and a flow chart with four stages, which includes items considered as essential for the transparent communication of a systematic analysis.
The “Physiotherapy Evidence Database (PEDro)” scale was also used to analyse the methodological quality of all the selected articles. This scale is a tool designed to evaluate the methodological quality of the clinical designs (Table 1) and used in many bibliographic reviews. The aforementioned tool is based on a list developed by Verhagen (25) using the Delphi technique (26).
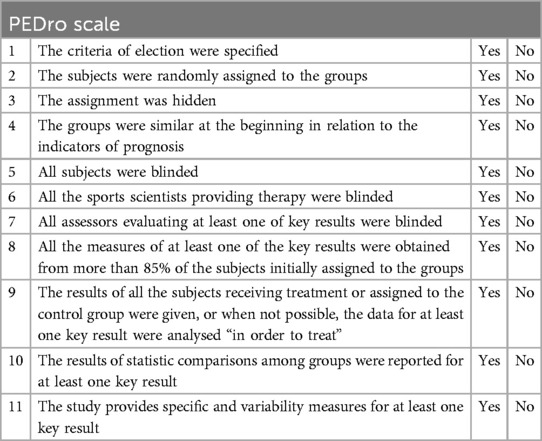
Table 1. “Physiotherapy evidence database (PEDro)” scale to analyse the methodological quality of the studies.
The PEDro scale has got a total of 11 items. Item 1 refers to the external validity of the study, while items 2–9 refer to the internal validity; items 10 and 11 show if the statistic information provided by the authors allows the accurate interpretation of the results. All items in the list are dichotomised as “yes”, “no” or “not reported”. Each “yes” item is given one point, while “no” or “not reported” items do not receive any points at all.
The first item of the PEDro scale was not taken into account in this review, as it was related to the evaluation of the external validity of the studies. Therefore, only items 2–11 were selected for the assessment of the methodological quality. Due to this, the maximum score of an article could not be higher than 10 points, and the minimum, not lower than 0 points.
The evaluation of the heterogeneity was another point to analyse. In this case, we can consider, on the one hand clinical heterogeneity, due to the differences among the types of patients, treatments and endings, and on the other hand, methodological heterogeneity, due to the variability in the designs and bias control.
The search on data base reported 510 publications. A digital search was made from sources which generated 65 relevant studies, included in the review. After the detailed review of titles, abstracts and complete articles (60), the publications which fulfilled the criteria of inclusion were a total of 40, in English. A limitation of 15 years of publication was applied. Of the 60 articles included, 5 were excluded due to the fact that they were duplicated. A limitation of 15 years of publication was applied. Of the 60 articles included, 5 were excluded due to the fact that they were duplicated, remaining 55 complete articles for the review. In the last stage of the inclusion of articles, 15 articles were excluded, which were not related to the sports area or which studied different variables.
From the final selection, 40 studies were included. A total of 21 articles were included (27–47) with significative data referring to CMJ, 12 articles (48–59) with significative data referring to the use of FMS, 12 articles (10, 27–30, 46, 60–65) referring to the use of TMG (Figure 1).
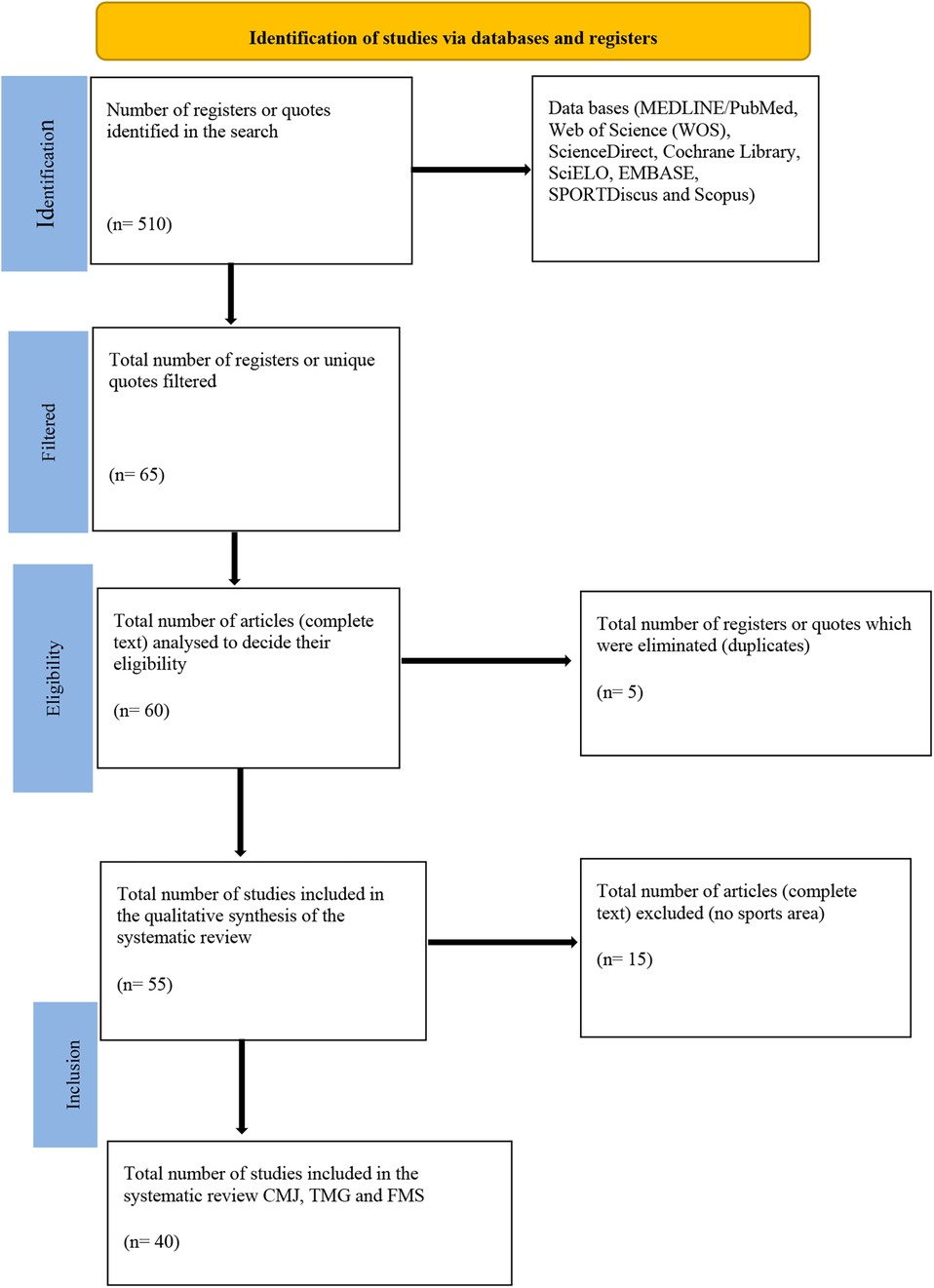
Figure 1. Flow diagram of the study selection.
The source of the study (author/authors and year of publication); population of the sample, indicating the number of participants; sport modality; assessment methods and tests; type of research design; study variables; main findings and effects of the intervention are represented on Table 2. 21 articles with significative data referring to CMJ, 12 articles were included with significative data referring to the use of FMS and 12 articles referring to the use of TMG, and Important differences were shown in size, age, gender, design of studies, sport and the evaluation methods used.
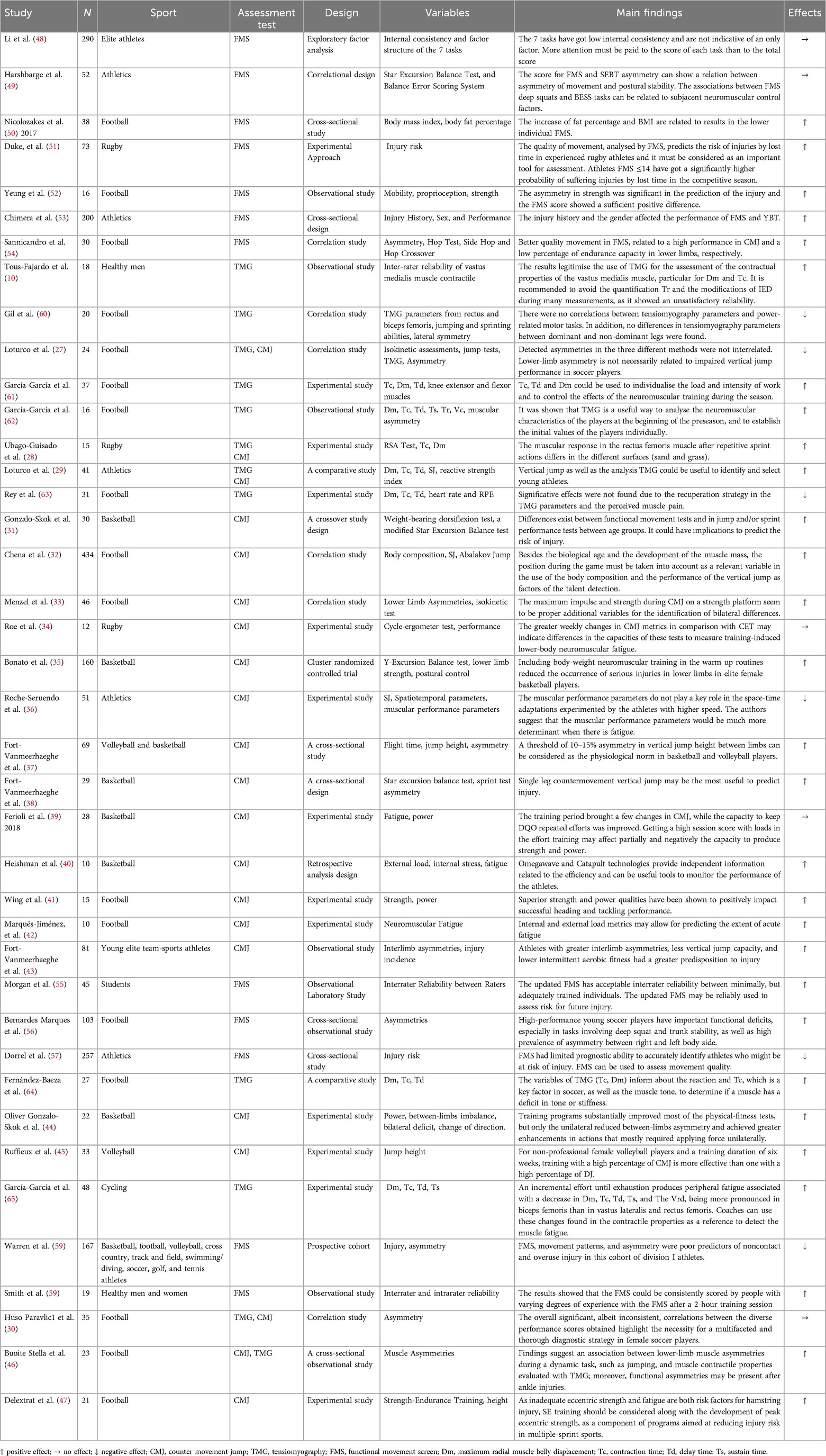
Table 2. Methodology and results of the interventions.
The methodological quality and the risk of bias were evaluated following the guidelines of the Cochrane Collaboration (24). For each investigation, criteria were shown as “low” if the criteria were fulfilled for a low risk of bias (improbable to severely alter the results) or “high” if the criteria were high risk bias (severely weakening the reliability of the results). If the risk of bias was unknown, it was considered “not clear” (it brings doubts about the results). Every included study was assessed for the risk of bias (24). The full assessments of study quality are shown in Figure 2.
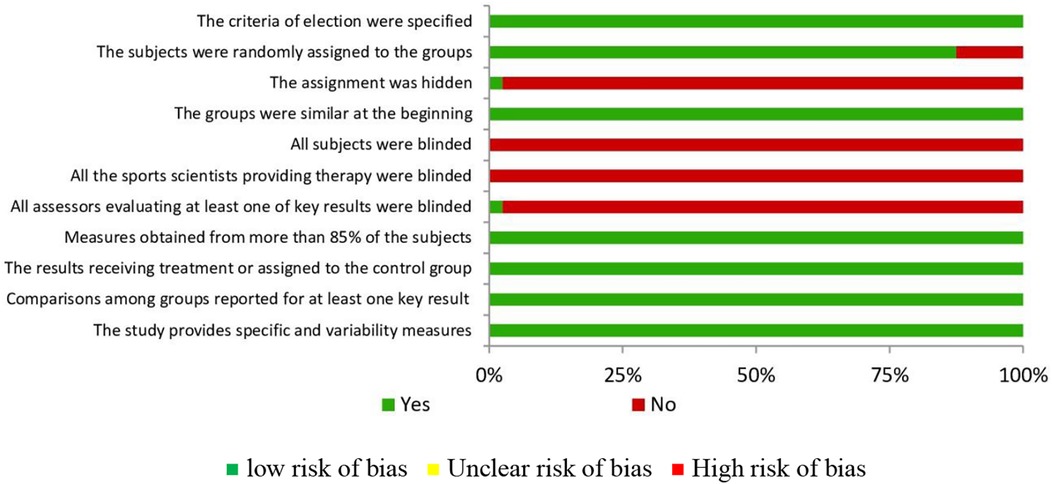
Figure 2. Risk of bias summary: review authors’ judgements about each risk of bias item for each included study.
The methodological quality of the analysed studies varied between 5 and 7 points, with an average of 5.92 points. 33 Articles got 6 points, 5 articles got 5 points and 2 article got 7 points.
Despite the relative heterogeneity of the analysed studies, certain criteria were consistent in all of them. Table 3 shows the criteria which more frequently were obtained belong to item 4, “the groups were similar at the beginning in relation to the most important indicators of prognosis”, to item 8 “the measures of at least one of the key results were obtained from more than 85% of the participants initially assigned to the groups”, followed by item 9 the results of all the subjects receiving treatment or assigned to the control group were given, or when not possible, the data for at least one key result were analysed “in order to treat”, item 10 “The results of statistic comparisons among groups were reported for at least one key result” and 11 “the study provides specific and variability measures for at least one key result”. Finally, just to indicate that none of the studies fulfilled criteria 5 and 6 (subjects and sports scientists were blinded), and only one study fulfilled item number 3 and 7 (the assignment was hidden and all assessors of at least one of the key results were blinded).
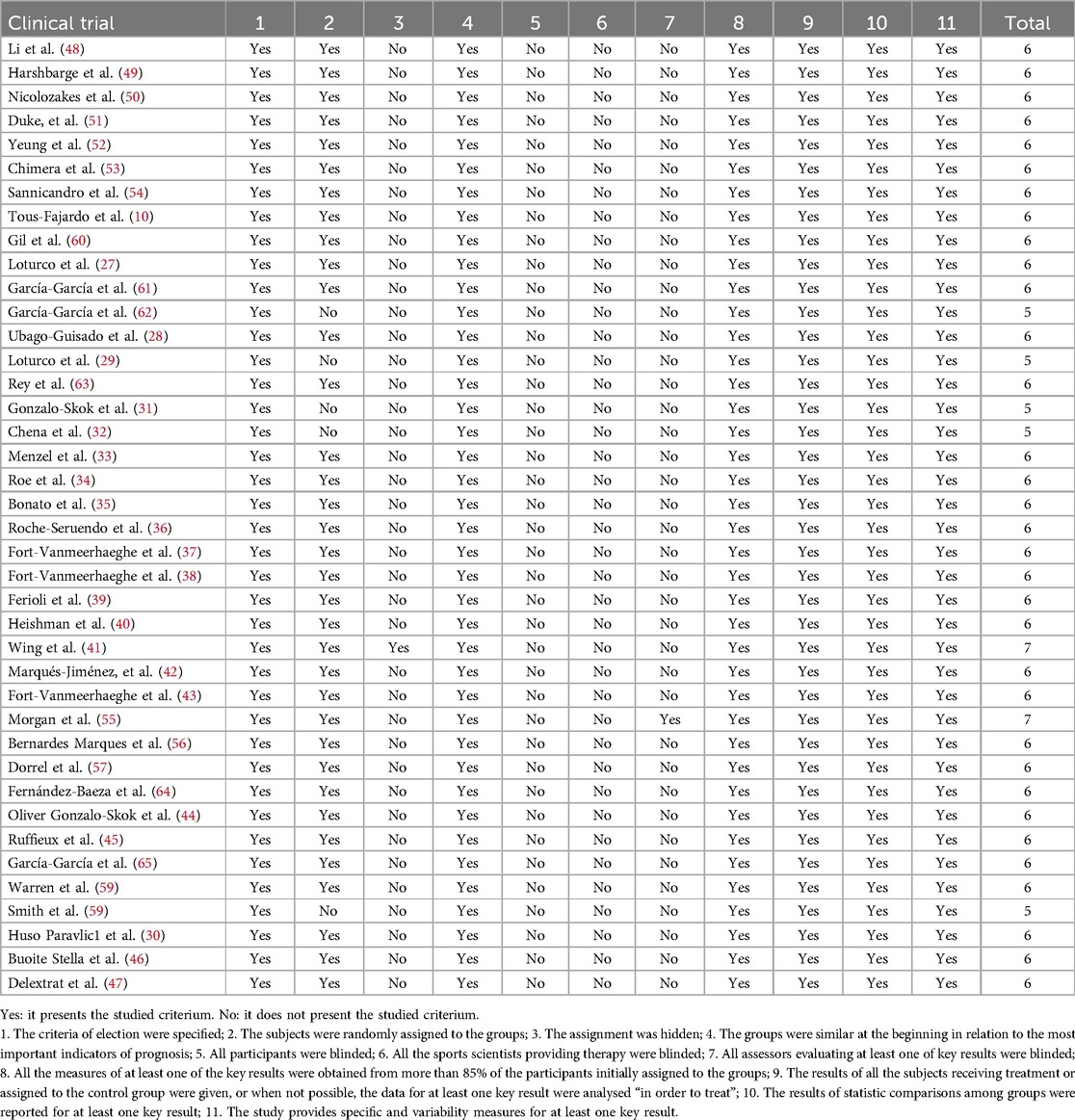
Table 3. Results according to PEDro scale (n = 40).
The main aim of this systematic review was to compile, synthesize and integrate international research published in different scientific databases on CMJ, FMS and TMG tests and technologies for the assessment of injury risk in sport. This way, this review determines the current state of the knowledge about this topic and allows a better understanding of the existing problems, making easier the development of future lines of research.
It was decided to carry out a revision of the most relevant bibliography, as well as of the most important published papers, in order to obtain the most outstanding aspects or data to which their authors refer, and this way work in all aspects to be taken into account, during and after the practice of sports, in order to avoid sports injuries.
The indicated measures were verified in terms of efficiency in the different studies analysed in this review. There currently exist many literary proposals which try to gather them in different ways in terms of prevention protocols, studying their effects in a complex way. In spite of this, it was observed that preventive actions are not currently used systematically.
Therefore, the current scientific bibliography describes different methods for the assessment and value of sports injuries, among which CMJ, FMS and TMG stand out.
Investigations reveal the validity and reliability of CMJ (16) to assess the power ability of lower extremities either unilaterally or bilaterally. For this reason, the CMJ vertical jump test can be used to monitor athletes' adaptations to training programs through measurements based on flight time, contact time, height and for estimation of lower extremity explosive power (16).
In addition to this, the studies (27, 33, 37, 38, 43, 44) indicate that the CMJ test can be used for the detection of asymmetries. In this regard, impulse and peak power during CMJ on a force platform appear to be additional variables appropriate for the identification of bilateral differences in sports such as basketball, volleyball, or football (33). Therefore, it would be appropriate to calculate the neuromuscular asymmetry of the lower extremities, because a greater neuromuscular asymmetry between legs could lead to a higher incidence of injury. To this end, some studies (37) indicate that a threshold of 10%–15% of vertical jump height asymmetry between limbs can be considered as the physiological norm in players.
As evidenced by (34, 39, 40, 42), CMJ can also be used to assess neuromuscular fatigue. The use of non-invasive strategies to monitor internal stress and external training load can be a valuable tool to identify player fatigue and stress (40). Neuromuscular fatigue can be quantified through CMJ performance, as suggested, its high repeatability and sensitivity proves its usefulness as a fatigue marker (42).
Similarly, the performance of the CMJ jump on a jumping platform allows the measurement of flight time, contact time, height and power. Starting from this fundamental database, the software designed allows to obtain in real time these parameters linked to the athlete's performance (16). Moreover, impulse and maximum strength during CMJ in a strength platform seem to be proper additional variables to identify bilateral differences. Therefore, it is relevant to carry out a vertical jump test in a strength platform to ensure a wide and reliable diagnostic information (33).
In the same way, the studies (41) support the idea that strength and power training is important for performance. It has also been indicated that CMJ training is more effective than drop jump training in improving jump height in female volleyball players (45). In addition, it has been shown that the inclusion of neuromuscular body mass training in warm-up routines can reduce the incidence of serious lower extremity injuries (35).
With respect to the risk of injury, some studies (43) indicate that athletes with greater asymmetries, lower vertical jump capacity and lower intermittent aerobic fitness have a greater predisposition to injury. Therefore, it is recommended to monitor CMJ and asymmetries given their sensitivity to detect significant differences between injured and healthy young athletes (43).
Therefore, the quantification of neuromuscular deficits through the CMJ is essential to identify individuals who may be at risk of injury (38). In addition, inadequate eccentric strength and fatigue are risk factors for injury (47). Therefore, eccentric strength development should be considered as a component of programs aimed at reducing the risk of injury (47).
Results show the use of the FMS to evaluate the quality of fundamental movement patterns, identify an individual's limitations or asymmetries as a potential risk factor for injury. This way, the studies (12, 13) show that 7 exercises (deep squat, hurdle step, lineal lunges, shoulder mobility, active straight leg raise, flexion in trunk stability and rotational stability) with a score of 0, 1, 2 and 3, allows evaluation of an athlete's basic movement patterns, mobility and stability.
In addition, the FMS could be used for asymmetry detection in athletes (58). Regarding asymmetry, some studies (52) have shown a significant difference between injured and non-injured professional football players, indicating that asymmetry could be used as a possible identifier of injury risk and has been found to be negatively associated with lower extremity injuries. This is also evidenced by relating the FMS to other assessment tests, such as the Star Excursion Balance Test (SEBT), and Balance Error Scoring System (BESS) scores (49). In this regard, it has been suggested (49) that associations between the FMS asymmetry score and the SEBT composite score may indicate a relationship between movement asymmetry and postural stability.
Also, the internal consistency and factorial structure of the 7 tasks of the functional movement test in elite athletes have been studied (48). In this regard, the results (55) of an updated version of the FMS indicate that it has acceptable inter-rater reliability among individuals with minimal but adequate training. The updated FMS can be used reliably to assess the risk of future injury (55). In addition, results have shown (59) that the FMS could be consistently scored by individuals with varying degrees of experience with the FMS after a 2-h training session. In a controlled laboratory study (66) with the FMS, intra-rater reliability was found to be strong and appears to be strengthened when individuals have experience using the FMS in addition to clinical experience.
In the same way, the different scores of FMS can be narrowly related to the athlete's height, weight, BMI and body fat percentage (50). As some studies show (50), the increase of body fat percentage and BMI is related to results in lower individual FMS, which prove potentially poor movement patterns in bigger athletes. Furthermore, other variables such as injury history or gender may influence performance on FMS tests (53). In this regard, Lower global FMS scores have been reported in athletes with a history of injury or surgery (53).
Finally, related to the results, many investigations (51, 55–57, 67) show that FMS ≤14 athletes have got a significantly higher probability of suffering injuries. In this regard, it is shown that participating subjects with scores ≤14 have a significantly higher probability of injury compared to those with higher scores.
Therefore, FMS could be used to assess the movement quality of athletes or active adults (66), with the aim of improving the movement pattern, which could reduce a risk factor for future injuries (51, 57, 58), so it should be considered as an assessment tool.
Studies show TMG as a valid and reliable (10, 11, 18, 19, 29) assessment tool to evaluate the contractile properties of superficial muscles. TMG is a technique to evaluate the mechanical muscle response based on the displacement of the radial muscle belly to a single electrical stimulus (10). As a result of this electrical stimulus, a displacement-time curve is recorded where the following parameters are integrated: maximum radial muscle displacement (Dm), contraction time (Tc), delay time (Td), sustained contraction time (Ts) and relaxation time (Tr) (10, 11, 18, 19).
In addition, TMG is shown to be a non-invasive method (11, 18, 19), which can be used to monitor the effects of training during a specific period or throughout the season, to detect muscle asymmetries in soccer players, basketball players and athletes (27, 30, 44, 46), lateral symmetry between dominant and non-dominant legs (60), provide information on muscle tone (64) and to detect fatigue (61).
Despite the reliability shown by this method, studies indicate that it is necessary to thoroughly follow a previously fixed protocol (10, 29, 46, 62–64) for each individual evaluation. In this sense, the recording of the radial displacement will be performed on the muscle belly after an external electrical stimulus (29). For this, the point of placement of the sensor must be taken into account, the placement of two adhesive electrodes, the duration of the electrical stimulus must be standardized at 1 millisecond of duration, of increasing intensity according to the protocol used, with varying intensity (50, 75 and 100 mAp) (68) and the recovery (periods of 10 s) between each electrical stimulus must be established (29, 64, 68).
Finally, it is important to highlight the results of the assessment of the variables TC and Dm in the biceps femoris and in the rectus femoris. As the studies (10, 64) conclude that the use of TMG for the evaluation of the contractile properties of the muscle, particularly for Dm and Tc, they can be an indicative to individualise the load and intensity of work. Therefore, TMG data (29, 61, 62, 64) can be used to individualize training programs, the intensity, to monitor the effects of neuromuscular training throughout the season and adjust the training load.
Our scientific research on a systematic review of original studies of diagnostic tests evidences the importance of conducting an assessment to identify the different risk factors for injury and to individualize training programs.
The sport modality, the sample, the terminology, the way to classify sports injuries and the technologies used, as it usually occurs in all the studies of similar characteristics, can be considered as limitations, as the election of some implies the rejection of others which could provide other type of data of wide interest.
The review could be biased when the bibliographic research was only carried out in classified magazines, having been rejected some published interventions which could have fulfilled the rest of the fixed requisites to be included.
It should be pointed out that the conclusions provided by our review have been carried out according to the articles found by our search strategy and selected under our eligibility criteria; therefore, there always exists the probability that there are studies which because of classification problems or search limits have not been included in this systematic review.
Future research should investigate the effectiveness of tests and assessment technologies for use in the injury rehabilitation process. Future studies should also investigate the effectiveness of a wider range of assessment technologies and test, which allow for the identification and detection of injury risk, as well as fatigue monitoring. Further studies are needed to evaluate the effectiveness of assessment technologies to individualize recovery.
We must note the importance of the assessment through valid and reliable technologies to identify the different injury risk factors. The CMJ can be used to assess lower limb power capacity unilaterally or bilaterally, to monitor athletes' adaptations to training programs through measurements based on flight time, contact time and height. In addition, it can be used to detect asymmetries, indicating that a threshold of 10%–15% of vertical jump height asymmetry between limbs can be considered the physiological norm in players, and to assess neuromuscular fatigue. FMS can be used to assess the quality of fundamental movement patterns and identify an individual's limitations as a potential risk factor for injury, through 7 exercises with a score of 0, 1, 2 and 3. Thus, the assessment of the different results which use FMS, shows that the participants with scores ≤14 have a significantly higher probability of injury compared to those with higher scores. TMG can be used for muscle assessment, particularly using Tc and Dm variables, with a variable intensity protocol (50, 75 and 100 mAp), and periods of 10 s between consecutive measurements, allowing individualization of training programs. Furthermore, inadequate strength and fatigue are risk factors for injury, so eccentric strength development should be considered as a component of programs designed to reduce injury risk. Therefore, quantification of neuromuscular deficits is essential to identify individuals who may be at risk for injury.
The results of this systematic review of the different studies presents the evidence of the technologies CMJ, FMS, and TMG, for the assessment of sports injuries. The CMJ vertical jump allows us to evaluate the power capacity of the lower extremities, both unilaterally and bilaterally, detect neuromuscular asymmetries and evaluate fatigue. Likewise, FMS could be used to assess an athlete's basic movement patterns, mobility and postural stability. Finally, TMG is a non-invasive method to assess the contractile properties of superficial muscles, monitor the effects of training, detect muscle asymmetries, symmetries, provide information on muscle tone and evaluate fatigue. Therefore, they should be considered as assessment tests and technologies to individualize training programs and identify injury risk factors.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
ÁV-S: Writing – original draft, Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing. AB-C: Project administration, Resources, Software, Supervision, Writing – original draft. JA-I: Supervision, Writing – review & editing. JC-G: Conceptualization, Formal analysis, Investigation, Methodology, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The APC was funded by Universidad Europea del Atlántico.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. McCall A, Dupont G, Ekstrand J. Injury prevention strategies, coach compliance and player adherence of 33 of the UEFA elite club injury study teams: a survey of teams’ head medical officers. Br J Sports Med. (2016) 50(12):725–30. doi: 10.1136/bjsports-2015-095259
2. Ekstrand J, Bengtsson H, Waldén M, Davison M, Khan KM, Hägglund M. Hamstring injury rates have increased during recent seasons and now constitute 24% of all injuries in men’s professional football: the UEFA elite club injury study from 2001/02 to 2021/22. Br J Sports Med. (2023) 57(5):292–8. doi: 10.1136/bjsports-2021-105407
3. Nielsen RO, Shrier I, Casals M, Nettel-Aguirre A, Møller M, Bolling C, et al. Statement on methods in sport injury research from the 1st METHODS MATTER meeting, Copenhagen, 2019. Br J Sports Med. (2020) 54(15):941. doi: 10.1136/bjsports-2019-101323
4. Ekstrand J, Ueblacker P, Van Zoest W, Verheijen R, Vanhecke B, van Wijk M, et al. Risk factors for hamstring muscle injury in male elite football: medical expert experience and conclusions from 15 European champions league clubs. BMJ Open Sport Exerc Med. (2023) 9(1):e001461. doi: 10.1136/bmjsem-2022-001461
5. Group IOCI and IEC, Bahr R, Clarsen B, Derman W, Dvorak J, Emery CA, et al. International Olympic committee consensus statement: methods for recording and reporting of epidemiological data on injury and illness in sports 2020 (including the STROBE extension for sports injury and illness surveillance (STROBE-SIIS)). Orthop J Sports Med. (2020) 8(2):2325967120902908. doi: 10.1177/2325967120902908
6. Hallén A, Tomás R, Ekstrand J, Bengtsson H, Van den Steen E, Hägglund M, et al. UEFA women’s elite club injury study: a prospective study on 1527 injuries over four consecutive seasons 2018/2019 to 2021/2022 reveals thigh muscle injuries to be most common and ACL injuries most burdensome. Br J Sports Med. (2024) 58(3):128–35. doi: 10.1136/bjsports-2023-107133
7. Calleja-González J, Mallo J, Cos F, Sampaio J, Jones MT, Marqués-Jiménez D, et al. A commentary of factors related to player availability and its influence on performance in elite team sports. Front Sports Act Living. (2023) 4:1077934. doi: 10.3389/fspor.2022.1077934
8. Gabbett TJ. The training—injury prevention paradox: should athletes be training smarter and harder? Br J Sports Med. (2016) 50(5):273–80. doi: 10.1136/bjsports-2015-095788
9. Velarde-Sotres Á, Bores-Cerezal A, Mecías-Calvo M, Barcala-Furelos M, Aparicio-Obregón S, Calleja-González J. Detection of upper limb asymmetries in athletes according to the stage of the season—a longitudinal study. Int J Environ Res Public Health. (2022) 19(2):849. doi: 10.3390/ijerph19020849
10. Tous-Fajardo J, Moras G, Rodríguez-Jiménez S, Usach R, Doutres DM, Maffiuletti NA. Inter-rater reliability of muscle contractile property measurements using non-invasive tensiomyography. J Electromyogr Kinesiol. (2010) 20(4):761–6. doi: 10.1016/j.jelekin.2010.02.008
11. Macgregor LJ, Hunter AM, Orizio C, Fairweather MM, Ditroilo M. Assessment of skeletal muscle contractile properties by radial displacement: the case for tensiomyography. Sports Med. (2018) 48:1607–20. doi: 10.1007/s40279-018-0912-6
12. Cook G, Burton L, Hoogenboom BJ, Voight M. Functional movement screening: the use of fundamental movements as an assessment of function - part 1. Int J Sports Phys Ther. (2014) 9(3):396–409.24944860
13. Cook G, Burton L, Hoogenboom BJ, Voight M. Functional movement screening: the use of fundamental movements as an assessment of function-part 2. Int J Sports Phys Ther. (2014) 9(4):549–63. doi: 10.26603/001c.115492
14. Halson SL. Monitoring training load to understand fatigue in athletes. Sports Med. (2014) 44(Suppl 2):139–47. doi: 10.1007/s40279-014-0253-z
15. Velarde-Sotres Á, Bores-Cerezal A, Mecías-Calvo M, Carvajal-Altamiranda S, Calleja-González J. Validity, reliability and reproducibility of octobalance test as tool to measure the upper limb compared to modified-upper quarter y-balance test. Int J Environ Res Public Health. (2021) 18(10):5057. doi: 10.3390/ijerph18105057
16. Markovic G, Dizdar D, Jukic I, Cardinale M. Reliability and factorial validity of squat and countermovement jump tests. J Strength Cond Res. (2004) 18(3):551–5. doi: 10.1519/1533-4287(2004)18%3C551:RAFVOS%3E2.0.CO;2
17. Bonazza NA, Smuin D, Onks CA, Silvis ML, Dhawan A. Reliability, validity, and injury predictive value of the functional movement screen: a systematic review and meta-analysis. Am J Sports Med. (2017) 45(3):725–32. doi: 10.1177/0363546516641937
18. García-García O, Cuba-Dorado A, Álvarez-Yates T, Carballo-López J, Iglesias-Caamaño M. Clinical utility of tensiomyography for muscle function analysis in athletes. Open Access J Sports Med. (2019) 2019:49–69. doi: 10.2147/OAJSM.S161485
19. Martín-Rodríguez S, Loturco I, Hunter AM, Rodríguez-Ruiz D, Munguia-Izquierdo D. Reliability and measurement error of tensiomyography to assess mechanical muscle function: a systematic review. J Strength Cond Res. (2017) 31(12):3524–36. doi: 10.1519/JSC.0000000000002250
20. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. Ann Intern Med. (2009) 151(4):W-65. doi: 10.7326/0003-4819-151-4-200908180-00136
21. Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. Cochrane (2011). p. 1–639.
22. O’Connor D, Green S, Higgins JPT. Defining the review question and developing criteria for including studies. In: Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions: Cochrane Book Series. Cochrane Library (2008). p. 81–94. doi: 10.1002/9780470712184.ch5
23. Greenhalgh T, Peacock R. Effectiveness and efficiency of search methods in systematic reviews of complex evidence: audit of primary sources. Br Med J. (2005) 331(7524):1064–5. doi: 10.1136/bmj.38636.593461.68
24. Higgins JP. Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Collaboration and John Wiley & Sons Ltd (2008).
25. Verhagen AP, de Vet HCW, de Bie RA, Kessels AGH, Boers M, Bouter LM, et al. The Delphi list: a criteria list for quality assessment of randomized clinical trials for conducting systematic reviews developed by Delphi consensus. J Clin Epidemiol. (1998) 51(12):1235–41. doi: 10.1016/S0895-4356(98)00131-0
26. Ap V, Delphi T, Alt Murphy M, Resteghini C, Feys P, Lamers I. An overview of systematic reviews on upper extremity outcome measures after stroke. BMC Neurol. (2015) 15:29. doi: 10.1186/s12883-015-0292-6
27. Loturco I, Pereira LA, Kobal R, Abad CCC, Komatsu W, Cunha R, et al. Functional screening tests: interrelationships and ability to predict vertical jump performance. Int J Sports Med. (2018) 39(03):189–97. doi: 10.1055/s-0043-122738
28. Ubago-Guisado E, Rodríguez-Cañamero S, López-Fernández J, Colino E, Sánchez-Sánchez J, Gallardo L. Muscle contractile properties on different sport surfaces using tensiomyography. J Hum Sport Exerc. (2017) 12(1):167–9. doi: 10.14198/jhse.2017.121.14
29. Loturco I, Gil S, de Souza Laurino CF, Roschel H, Kobal R, Abad CCC, et al. Differences in muscle mechanical properties between elite power and endurance athletes: a comparative study. J Strength Cond Res. (2015) 29(6):1723–8. doi: 10.1519/JSC.0000000000000803
30. Paravlic AH, Abazovic E, Milanović Z, Vučković G, Spudić D, Hadzic V, et al. The association between unilateral and bilateral performance-related measures in elite female soccer players: a multifaceted investigation. Front Physiol. (2024) 15:1298159. doi: 10.3389/fphys.2024.1298159
31. Gonzalo-Skok O, Serna J, Rhea MR, Marín PJ. Age differences in measures of functional movement and performance in highly young basketball players. Int J Sports Phys Ther. (2017) 12(5):812–21. doi: 10.26603/ijspt20170812
32. Chena M, Pérez-López A, Valverde IÁ, Cerezal AB, Ramos-Campo DJ, Rubio-Arias JA, et al. Influence of body composition on vertical jump performance according with the age and the playing position in football players. Nutr Hosp. (2015) 32(1):299–307. doi: 10.3305/nh.2015.32.1.8876
33. Menzel HJ, Chagas MH, Szmuchrowski LA, Araujo SRS, de Andrade AGP, de Jesus-Moraleida FR. Analysis of lower limb asymmetries by isokinetic and vertical jump tests in soccer players. J Strength Cond Res. (2013) 27(5):1370–7. doi: 10.1519/JSC.0b013e318265a3c8
34. Roe G, Darrall-Jones J, Till K, Phibbs P, Read D, Weakley J, et al. To jump or cycle? Monitoring neuromuscular function in rugby union players. Int J Sports Physiol Perform. (2017) 12(5):690–6. doi: 10.1123/ijspp.2016-0273
35. Bonato M, Benis R, La Torre A. Neuromuscular training reduces lower limb injuries in elite female basketball players. A cluster randomized controlled trial. Scand J Med Sci Sports. (2018) 28(4):1451–60. doi: 10.1111/sms.13034
36. Roche-Seruendo LE, García-Pinillos F, Haicaguerre J, Bataller-Cervero A V, Soto-Hermoso VM, Latorre-Román PÁ. Lack of influence of muscular performance parameters on spatiotemporal adaptations with increased running velocity. J Strength Cond Res. (2018) 32(2):409–15. doi: 10.1519/JSC.0000000000001845
37. Fort-Vanmeerhaeghe A, Gual G, Romero-Rodriguez D, Unnitha V. Lower limb neuromuscular asymmetry in volleyball and basketball players. J Hum Kinet. (2016) 50(1):135–43. doi: 10.1515/hukin-2015-0150
38. Fort-Vanmeerhaeghe A, Montalvo AM, Sitja-Rabert M, Kiefer AW, Myer GD. Neuromuscular asymmetries in the lower limbs of elite female youth basketball players and the application of the skillful limb model of comparison. Phys Ther Sport. (2015) 16(4):317–23. doi: 10.1016/j.ptsp.2015.01.003
39. Ferioli D, Bosio A, Bilsborough JC, La TA, Tornaghi M, Rampinini E. The preparation period in basketball: training load and neuromuscular adaptations. Int J Sports Physiol Perform. (2018) 13(8):991–9. doi: 10.1123/ijspp.2017-0434
40. Heishman AD, Curtis MA, Saliba E, Hornett RJ, Malin SK, Weltman AL. Non-invasive assessment of internal and external player load: implications for optimizing athletic performance. J Strength Cond Res. (2018) 32(5):1280–7. doi: 10.1519/JSC.0000000000002413
41. Wing CE, Turner AN, Bishop CJ. The importance of strength and power on key performance indicators in elite youth soccer. J Strength Cond Res. (2020) 34(7):2006–14. doi: 10.1519/JSC.0000000000002446
42. Marqués-Jiménez D, Calleja-González J, Arratibel-Imaz I, Terrados N. Match loads may predict neuromuscular fatigue and intermittent-running endurance capacity decrement after a soccer match. Int J Environ Res Public Health. (2022) 19(22):15390. doi: 10.3390/ijerph192215390
43. Fort-Vanmeerhaeghe A, Milà-Villarroel R, Pujol-Marzo M, Arboix-Alió J, Bishop C. Higher vertical jumping asymmetries and lower physical performance are indicators of increased injury incidence in youth team-sport athletes. J Strength Cond Res. (2022) 36(8):2204–11. doi: 10.1519/JSC.0000000000003828
44. Gonzalo-Skok O, Tous-Fajardo J, Suarez-Arrones L, Arjol-Serrano JL, Casajús JA, Mendez-Villanueva A. Single-leg power output and between-limbs imbalances in team-sport players: unilateral versus bilateral combined resistance training. Int J Sports Physiol Perform. (2017) 12(1):106–14. doi: 10.1123/ijspp.2015-0743
45. Ruffieux J, Wälchli M, Kim KM, Taube W. Countermovement jump training is more effective than drop jump training in enhancing jump height in non-professional female volleyball players. Front Physiol. (2020) 11:231. doi: 10.3389/fphys.2020.00231
46. Buoite Stella A, Galimi A, Martini M, Di Lenarda L, Murena L, Deodato M. Muscle asymmetries in the lower limbs of male soccer players: preliminary findings on the association between countermovement jump and tensiomyography. Sports. (2022) 10(11):177. doi: 10.3390/sports10110177
47. Delextrat A, Piquet J, Matthews MJ, Cohen DD. Strength-endurance training reduces the hamstrings strength decline following simulated football competition in female players. Front Physiol. (2018) 9:1059. doi: 10.3389/fphys.2018.01059
48. Li Y, Wang X, Chen X, Dai B. Exploratory factor analysis of the functional movement screen in elite athletes. J Sports Sci. (2015) 33(11):1166–72. doi: 10.1080/02640414.2014.986505
49. Harshbarger ND, Anderson BE, Lam KC. Is there a relationship between the functional movement screen, star excursion balance test, and balance error scoring system? Clin J Sport Med. (2018) 28(4):389–94. doi: 10.1097/JSM.0000000000000465
50. Nicolozakes CP, Schneider DK, Roewer BD, Borchers JR, Hewett TE. Influence of body composition on functional movement ScreenTM scores in collegiate football players. J Sport Rehabil. (2018) 27(5):431–7. doi: 10.1123/jsr.2015-0080
51. Duke SR, Martin SE, Gaul CA. Preseason functional movement screen predicts risk of time-loss injury in experienced male rugby union athletes. J Strength Cond Res. (2017) 31(10):2740–7. doi: 10.1519/JSC.0000000000001838
52. Yeung J, Cleves A, Griffiths H, Nokes L. Mobility, proprioception, strength and FMS as predictors of injury in professional footballers. BMJ Open Sport Exerc Med. (2016) 2(1):e000134. doi: 10.1136/bmjsem-2016-000134
53. Chimera NJ, Smith CA, Warren M. Injury history, sex, and performance on the functional movement screen and Y balance test. J Athl Train. (2015) 50(5):475–85. doi: 10.4085/1062-6050-49.6.02
54. Sannicandro I, Cofano G, Rosa AR, Traficante P, Piccinno A. Functional movement screen and lower limb strength asymmetry in professional soccer players. Br J Sports Med. (2017) 51(4):381–2. doi: 10.1136/bjsports-2016-097372.248
55. Morgan R, LeMire S, Knoll L, Schuster E, Tietz C, Weisz A, et al. The functional movement screen: exploring interrater reliability between raters in the updated version. Int J Sports Phys Ther. (2023) 18(3):737. doi: 10.26603/001c.74724
56. Marques VB, Medeiros TM, de Souza Stigger F, Nakamura FY, Baroni BM. The functional movement screen (FMSTM) in elite young soccer players between 14 and 20 years: composite score, individual-test scores and asymmetries. Int J Sports Phys Ther. (2017) 12(6):977. doi: 10.26603/ijspt20170977
57. Dorrel B, Long T, Shaffer S, Myer GD. The functional movement screen as a predictor of injury in national collegiate athletic association division II athletes. J Athl Train. (2018) 53(1):29–34. doi: 10.4085/1062-6050-528-15
58. Warren M, Smith CA, Chimera NJ. Association of the functional movement screen with injuries in division I athletes. J Sport Rehabil. (2015) 24(2):163–70. doi: 10.1123/jsr.2013-0141
59. Smith CA, Chimera NJ, Wright NJ, Warren M. Interrater and intrarater reliability of the functional movement screen. J Strength Cond Res. (2013) 27(4):982–7. doi: 10.1519/JSC.0b013e3182606df2
60. Gil S, Loturco I, Tricoli V, Ugrinowitsch C, Kobal R, Abad CCC, et al. Tensiomyography parameters and jumping and sprinting performance in Brazilian elite soccer players. Sports Biomech. (2015) 14(3):340–50. doi: 10.1080/14763141.2015.1062128
61. García-García O, Serrano-Gomez V, Hernandez-Mendo A, Tapia-Flores A. Assessment of the in-season changes in mechanical and neuromuscular characteristics in professional soccer players. J Sports Med Phys Fitness. (2016) 56(6):714–23.
62. García-García O, Serrano-Gómez V, Hernández-Mendo A, Morales-Sánchez V. Baseline mechanical and neuromuscular profile of knee extensor and flexor muscles in professional soccer players at the start of the Pre-season. J Hum Kinet. (2017) 58(1):23–34. doi: 10.1515/hukin-2017-0066
63. Rey E, Lago-Peñas C, Lago-Ballesteros J, Casáis L. The effect of recovery strategies on contractile properties using tensiomyography and perceived muscle soreness in professional soccer players. J Strength Cond Res. (2012) 26(11):3081–8. doi: 10.1519/JSC.0b013e3182470d33
64. Fernández-Baeza D, Diaz-Ureña G, González-Millán C. Differences in the contractile properties of the biceps femoris and semitendinosus muscles throughout a season in professional soccer players. J Hum Kinet. (2022) 84(1):74–81. doi: 10.2478/hukin-2022-0088
65. García-García O, Cuba-Dorado A, Riveiro-Bozada A, Carballo-López J, Álvarez-Yates T, López-Chicharro J. A maximal incremental test in cyclists causes greater peripheral fatigue in biceps femoris. Res Q Exerc Sport. (2020) 91(3):460–8. doi: 10.1080/02701367.2019.1680789
66. Gribble PA, Brigle J, Pietrosimone BG, Pfile KR, Webster KA. Intrarater reliability of the functional movement screen. J Strength Cond Res. (2013) 27(4):978–81. doi: 10.1519/JSC.0b013e31825c32a8
67. Kiesel K, Plisky PJ, Voight ML. Can serious injury in professional football be predicted by a preseason functional movement screen? N Am J Sports Phys Ther. (2007) 2(3):147.21522210
Keywords: injury prevention, risk factors, functional tests, recovery, assessment
Citation: Velarde-Sotres Á, Bores-Cerezal A, Alemany-Iturriaga J and Calleja-González J (2025) Tensiomyography, functional movement screen and counter movement jump for the assessment of injury risk in sport: a systematic review of original studies of diagnostic tests. Front. Sports Act. Living 7:1565900. doi: 10.3389/fspor.2025.1565900
Received: 23 January 2025; Accepted: 17 February 2025;
Published: 10 March 2025.
Edited by:
Myles Murphy, Edith Cowan University, AustraliaReviewed by:
Dražen Čular, University of Split, CroatiaCopyright: © 2025 Velarde-Sotres, Bores-Cerezal, Alemany-Iturriaga and Calleja-González. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julio Calleja-González, anVsaW8uY2FsbGVqYS5nb256YWxlekBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.