 Nuno Domingos Garrido1,2*†
Nuno Domingos Garrido1,2*† Victor Machado Reis1,2,†
Victor Machado Reis1,2,† José Manuel Vilaça-Alves1,2,†
José Manuel Vilaça-Alves1,2,† Gabriela Chaves Lucas1
Gabriela Chaves Lucas1 Ismael Lima Godinho1
Ismael Lima Godinho1 Rafael Peixoto1
Rafael Peixoto1 Alberto Fucarino3
Alberto Fucarino3 Manuela Cantoia3
Manuela Cantoia3 Enzo Iuliano3
Enzo Iuliano3 Andrea De Giorgio3
Andrea De Giorgio3 Antonio Fabbrizio3
Antonio Fabbrizio3 Martina Suasa3
Martina Suasa3 Giovanna Zimatore3
Giovanna Zimatore3 Carlo Baldari3
Carlo Baldari3 Filippo Macaluso4
Filippo Macaluso4
- 1Research Center in Sports Sciences, Health Sciences and Human Development (CIDESD), Vila Real, Portugal
- 2Sports Science, Exercise and Health Department, University of Trás-os-Montes & Alto Douro, Vila Real, Portugal
- 3Department of Theoretical and Applied Sciences, eCampus University, Novedrate, Italy
- 4Department of Biomedicine, Neuroscience and Advanced Diagnostics (BIND), University of Palermo, Palermo, Italy
Introduction: This study aimed to review the impact of tele-exercise on different adult populations, comparing synchronous and asynchronous interventions and their effects on outcomes such as quality of life, physical fitness, functional capacity, strength, and pain.
Methods: Randomised clinical trials and quasi-experimental studies published between 2014 and 2024 were included, totalling 16 studies with 1,416 participants. The interventions varied between synchronous teleexercise (via videoconference) and asynchronous (via apps and recorded videos). The review followed the PRISMA guidelines, ensuring a systematic approach to study selection, data extraction, and bias assessment.
Results: The results indicate that tele-exercise, especially synchronous, has the potential to primarily improve physical fitness, functional capacity, and pain perception, being effective for the elderly and individuals with specific conditions such as multiple sclerosis and obesity.
Discussion: However, the methodological heterogeneity of the studies and the lack of consistent data limit the generalisation of the findings, highlighting the need for more high-quality research.
Systematic Review Registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42024563241, PROSPERO (CRD42024563241).
1 Introduction
Recent advances in technology and artificial intelligence, along with the COVID-19 era, have driven the development and popularisation of various online telehealth tools (1). Telehealth, including the adaptable concept of tele-exercise, has emerged to meet the need to incorporate physical exercise into current demands, empowering individuals to take control of their health (2, 3).
Physical exercise can be defined as a structured activity aimed at improving and maintaining physical fitness (4). Tele-exercise, in turn, is an online exercise prescription methodology that can be performed synchronously or asynchronously. Among the tools that comprise tele-exercise are training apps for smartphones with personalised programs, synchronous training via videoconference or mobile calls, apps with recorded videos to guide into workouts, activity monitoring via smartwatches and smart homes, and virtual assistants that suggest and monitor activities (2, 3, 5, 6). The advancement of these tools can be a resource for exercise training and adherence for individuals with mobility restrictions, health issues, and even people with limited access to in-person exercise environments, such as many elderly or individuals with limitations and comorbidities (7–9).
Given the global trend of low physical activity levels, it is concerning that 31% of adults and 80% of adolescents do not meet the World Health Organization's recommendations for physical activity (10), representing a significant public health challenge.
Given the trend towards sedentary lifestyles, tele-exercise has been introduced as a potential tool for expanding physical exercise (9). A basic tele-exercise program consists of a central database using web services to connect healthcare providers to patients' devices virtually. With technological advancements, tele-exercise using high-speed internet, videoconferencing, and smartphone apps can allow individuals to engage in physical activities remotely under the supervision of experienced and trained professionals. Importantly, these tools can enable participants to choose their preferred exercise regimes, especially those requiring minimal supervision (6, 11), thereby catering to their individual fitness needs and making them feel considered in their fitness journey.
These regimes help maintain regularity while minimising costs. Webcams provide communication between healthcare professionals and are a method for monitoring patients' activity (12). As one of the most recent branches of telemedicine, the theoretical data on its effectiveness lacks sufficient practical data to support it.
During the COVID-19 pandemic, the importance of tele-exercise as a health alternative was put into perspective (1, 13). Although some systematic reviews have addressed the topic of tele-exercise, its role in health, particularly regarding improvements in quality of life, physical fitness, and sub-groups such as functional capacity and strength in adult populations, is not yet well defined. Thus, this study primarily aims to understand the impact of tele-exercise on different population groups. Secondarily, it seeks to compare synchronous vs. asynchronous tele-exercise and tele-exercise vs. in-person exercise, assessing whether there are differences in impact on quality of life, physical fitness, functional capacity, and strength across different adult populations based on the exercise method used. Therefore, our focus is primarily on randomised clinical trials, recognising the importance of systematic reviews that include such studies. However, acknowledging that the current literature on the topic is recent, this work also accepts quasi-experimental studies that meet the eligibility criteria to make the review more comprehensive.
2 Methods
2.1 Registration protocol
The protocol was registered with the International Prospective Register of Systematic Reviews—PROSPERO (registration number CRD42024563241) prior to the start of this review, which was drafted in accordance with the PRISMA 2020 statement (14).
2.2 Eligibility criteria
2.2.1 Inclusion criteria
The selection process was meticulous and thorough. Initially, it was considered various study designs, but upon discovering a substantial number of clinical trials and quasi-experimental studies, it was chosen to focus on these two designs. Whether randomised or not, or included control groups, it was sought study designs that most effectively address the research question while rigorously accounting for their methodological limitations through stringent risk of bias criteria. Studies published between 2014 and 2024 with no language restrictions were included. The criteria was stringent, requiring at least one tele-exercise intervention, either synchronous or asynchronous, with a minimum duration of 6 weeks.
The present review encompasses a diverse range of adult populations. Adults aged between 18 and 99 who were not hospitalised or undergoing cardiac rehabilitation or physiotherapy programs were included. There were no restrictions regarding the population, resulting in a rich heterogeneity. The population categories included elderly individuals, elderly individuals in cancer remission, pregnant women with obesity or overweight, obese adults, adults with Parkinson, adults with multiple sclerosis (MS), adults with Down syndrome, adults with recent COVID-19, and healthy adults.
Accommodating a wide range of tele-exercise interventions, it were considered studies with synchronous and/or asynchronous tele-exercise interventions of any structured training method (e.g., resistance training or yoga). Synchronous interventions were required to be conducted via live videoconferencing, either in groups or individually, using smartphones, tablets, or computers. Asynchronous interventions could utilise technologies such as recorded videos, remote training apps, or traditional methods like prescription and supervision via phone calls. Asynchronous interventions could involve either one-time or ongoing interactions.
The main outcomes of this review included data assessing changes from baseline over time by group or between groups. Studies were included if they assessed at least one outcome related to physical fitness, quality of life, functional capacity, strength, and pain, evaluated using a validated assessment tool. The presence of a control condition was not a mandatory inclusion criterion.
Studies with synchronous and/or asynchronous tele-exercise interventions of any structured training method (e.g., resistance training or yoga) were included. However, synchronous interventions needed to be conducted via live videoconferencing, either in groups or individually, using smartphones, tablets, or computers. Asynchronous interventions could utilise technologies such as recorded videos, remote training apps, or traditional methods like prescription and supervision via phone calls. Asynchronous interventions could involve either one-time or ongoing interactions.
2.2.2 Exclusion criteria
Studies were excluded if they addressed telemedicine or telerehabilitation in the context of physiotherapy or post-surgical recovery, as well as those related to virtual reality environments and e-sports. Studies without a structured tele-exercise program were also excluded. Articles published before 2014 were disregarded. Given the rapid technological advancements, we chose to prioritise more recent publications that reflect current technological tools.
2.3 Search strategy
On July 6, 2024, and July 10, 2024, searches were conducted in four databases: PUBMED (74 articles), SCOPUS (59 articles), WEB OF SCIENCE (54 articles), and SCIENCE DIRECT (53 articles), totalling initially 240 articles. The search terms used (Table 1) were “Tele-exercise,” “Remote exercise,” “Remote training,” “Tele-exercise programs,” “Synchronous exercise,” and “Asynchronous exercise,” separated by the boolean operator OR, with a filter for “Title/Abstract” and coverage from 2014 to the present. A “snowball” search was also performed in the reference lists of the full texts, identifying two studies of interest. The entire process was conducted independently by two investigators. Table 1 presents the search strategy used for PUBMED.
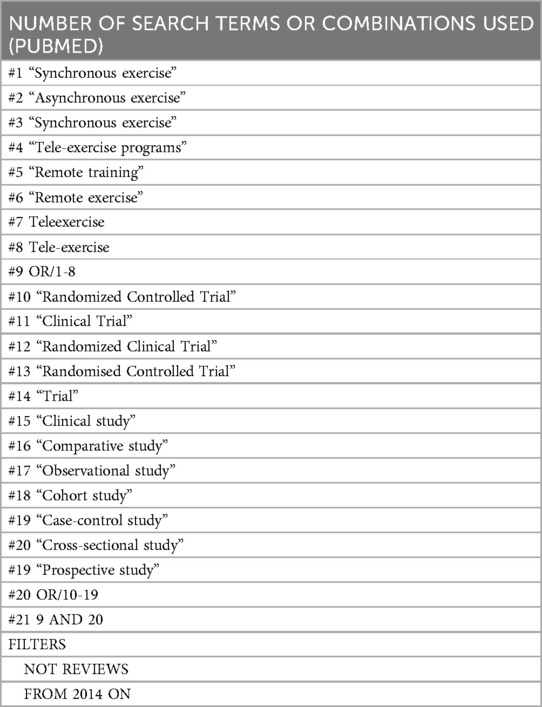
Table 1. Search strategy.
2.3.1 Permission to reuse and copyright
No permission was necessary for the use of copyrighted content.
2.4 Study selection process
The initial reference screening was conducted using the reference management software ZOTERO 6.6.27. A total of 240 studies were initially identified (the flow diagram is provided in Figure 1 in Section 3). Duplicate records were identified using software, reviewed manually, and removed accordingly. Two reviewers independently assessed the “Title and Abstract,” and any discrepancies were discussed until a consensus was reached. The same reviewers applied the inclusion and exclusion criteria during the full-text selection process and cross-checked the results. Discrepancies were resolved by consensus without needing a third reviewer (more details in Section 3.1).
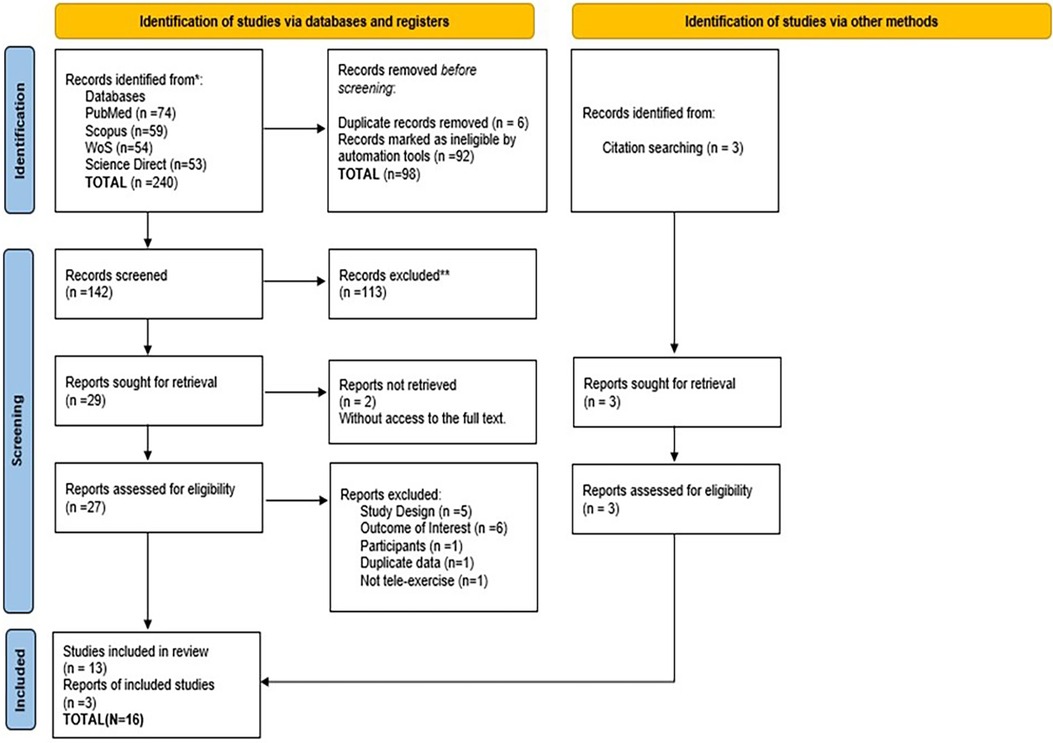
Figure 1. PRISMA flowchart outlining the flow of studies through the review.
2.5 Data extraction
After applying all exclusion criteria and finalising the list of studies, data from each study were extracted by two independent reviewers using a data extraction sheet adapted from the Critical Appraisal Skills Programme (CASP) for randomised clinical trials. Two other reviewers focused on extracting general data and study characteristics for a descriptive assessment of each study (Table 2). Discrepancies were resolved through discussion or with the assistance of a third reviewer.
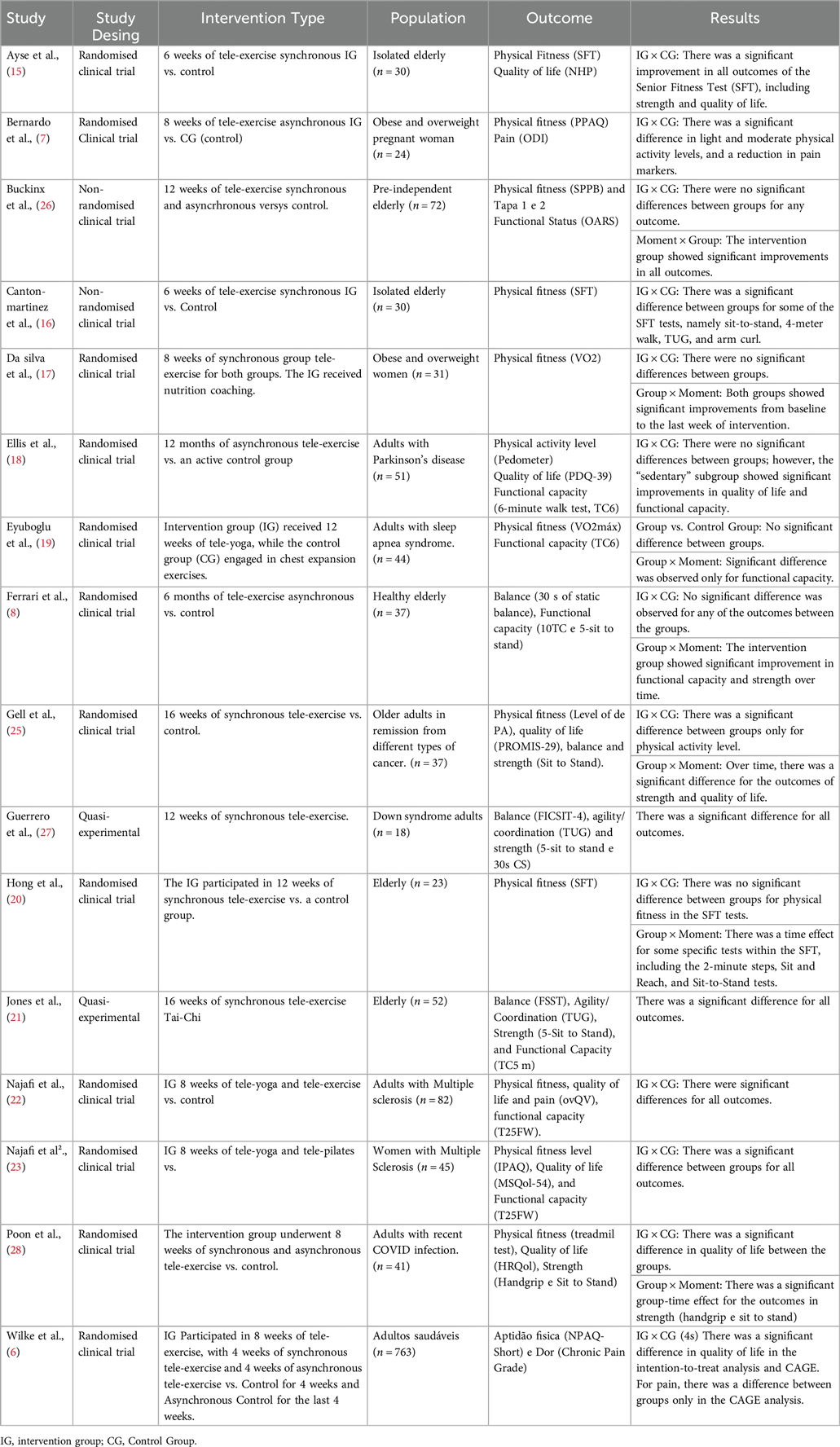
Table 2. Study characteristics.
Data was collected on:
• Report: Author and year of publication.
• Study: Type of study and research question.
• Participants: Characteristics of the population.
• Intervention: Type, duration, and FITT characteristics whenever available.
• Research design or characteristics: Outcome of interest, methodology, results, and effect size.
2.6 Quality criteria of primary studies
Two reviewers independently assessed the quality of the studies. In cases of disagreement that could not be resolved through mutual reconciliation, a third reviewer was consulted. The quality scale used was the ROB.2 Cochrane Risk-of-Bias Tool for Randomized Trials, given that randomised clinical trials are the primary focus of this study. The studies were assessed as having low, unclear, or high risk of bias (Figures 1, 2).
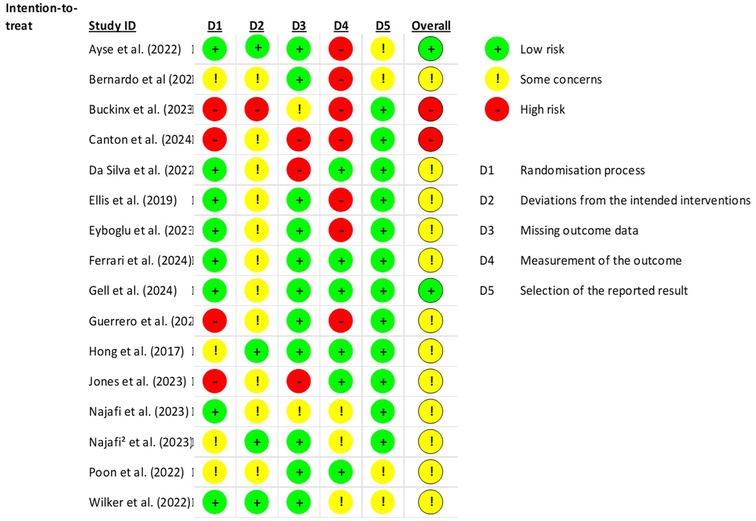
Figure 2. ROB.2 evaluation of included studies.
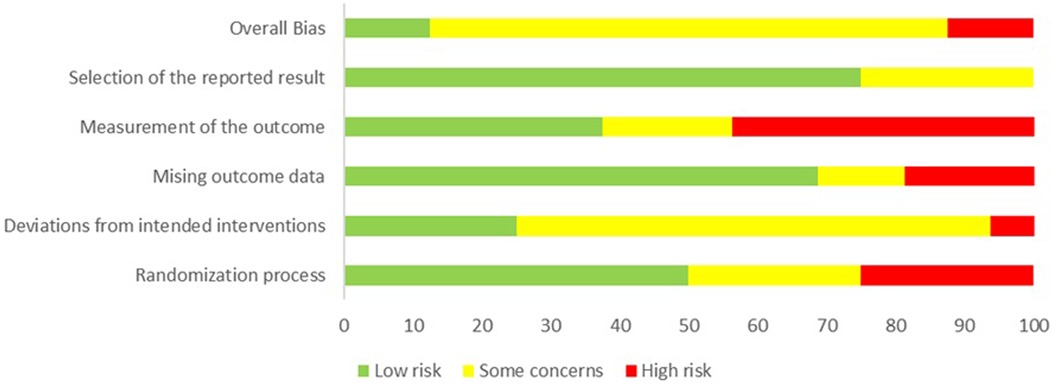
Figure 3. Risk of bias assessment with ROB.2 as percentage.
The risk of bias was assessed across five key domains: the randomization process (D1), deviations from the intended interventions (D2), missing outcome data (D3), measurement of the outcome (D4), and selection of the reported results (D5). Each domain includes subdomains designed to provide a detailed scope of each main domain.
2.7 Effect measures and data synthesis
The studies included in this systematic review exhibit heterogeneous samples, instruments, designs, and interventions, preventing the statistical precision required for a meta-analysis. Due to the heterogeneity in intervention methods and reported outcomes for different populations, we chose to present the data in tabular format, highlighting the characteristics of the interventions, population, and effect size of each article. Additionally, we summarise and present the data in a narrative synthesis in the text, by outcome in population subgroups, detailing the main characteristics of each article, results for all outcomes, and statistical significance.
The results were organised into main categories: quality of life, physical fitness, functional capacity, and strength. The secondary outcome of pain was also described within the main category of quality of life.
3 Results
3.1 Study selection
As mentioned earlier, a total of 240 studies were initially identified during the first screening in the databases. Ninety-eight duplicates were identified and removed. The “Title and Abstract” of 142 studies were examined, and 29 were selected for full-text screening. The full text of two studies could not be accessed. An email was sent to the corresponding authors, but no response was received. Of the 27 analysed studies, 5 were excluded for not being randomised or quasi-experimental trials, 6 did not have outcomes of interest, 1 did not involve an adult population, and 1 was considered not to have characteristics of structured tele-exercise. The study conducted by Jones in 2023 (24) reported results included in his other study published in 2024 (21). Only this latest was included and will be cited. Thus, 14 studies were excluded. From the full-text article list, 3 new studies were found (snowball effect). In total, we screened 242 studies, resulting in 16 eligible studies.
3.2 Characteristics of the studies
3.2.1 Tele-exercise approach
Eleven of the sixteen studies were randomised clinical trials (6–8, 15, 17–20, 22, 23, 25). Five were non-randomised clinical trials or quasi-experimental studies. Two studies used a pragmatic approach to participant allocation due to restrictions during the COVID-19 pandemic (16, 26). Two studies were quasi-experimental with a single-group pre-post design (21, 27), and the fourth study did not report a specific reason for not being randomised (28).
Three studies presented the exclusively asynchronous approach. In the study by Ferrari et al. (2024), wearable technology with inertial sensors was used, featuring an interface that allowed the trainer to remotely prescribe workouts and provide movement feedback to the trainer. Participants received workouts via the web, including videos and demonstrations. Ellis et al. (2019) used a model based on remote monitoring, where all participants received tablets with personalised workouts.
The synchronous approach studies used various videoconferencing platforms such as Skype, Zoom, and Google Meet. All of them were conducted as group training sessions, with workouts ranging from tele-Pilates, tele-Yoga, and tele-Tai Chi to exercises incorporating strength, endurance, aerobic, flexibility, and balance components (7, 15–17, 19–23, 25, 27).
3.2.2 Population
The population of the eligible studies was heterogeneous, totalling 1,416 participants. Six studies focused exclusively on the elderly. One study evaluated pre-dependent elderly individuals, four studies assessed healthy elderly individuals, one study evaluated elderly individuals with sub-groups for comorbidities (hypertension and diabetes), and one study evaluated elderly individuals in remission from various types of cancer (8, 15, 16, 20, 21, 25, 26). Ellis et al. (2019) assessed adults and elderly individuals with Parkinson's disease, with the majority being elderly (18). Two studies focused on individuals with obesity and overweight, with one study including pregnant women (7) and the other including the general obese population (17). Four studies examined the adult population, including adults with Down syndrome (27), adults with sleep apnea syndrome (19), adults with recent COVID-19 (28), and healthy adults (6).
A summary of the characteristics, intervention types and outcomes is shown in Table 2.
3.3 Quality of evidence and strength of recommendations
Two researchers independently assessed the evidence using GRADE (Grading of Recommendations, Assessment, Development and Evaluation) criteria (29) with the assistance of the GRADE PRO GDT software, available at http://gdt.gradepro.org/. The quality of evidence and strength of recommendations can be seen below (Table 3).

Table 3. Outcomes grades of evidence.
3.4 Results by outcomes
Different assessment tools, training methodologies, and statistical models were used to present the results of the eligible studies. In this section, we will synthesize these results by outcomes, specifying the population of each study and maintaining the statistical data in their original scales.
3.4.1 Physical fitness
We considered physical fitness outcomes related to the level of physical activity and/or aspects associated with physical capacity, except for strength, which will be presented separately.
All eligible studies reported results for at least one physical fitness marker. The most used marker was the level of physical activity (6, 7, 18, 22, 23, 25, 26). Bernardo et al. (2024) evaluated obese and overweight pregnant women using the Pregnancy Physical Activity Questionnaire (PPAQ) and reported significant differences for increases in light and moderate physical activity, with a moderate effect size (p = 0.025, ES = 0.50; p = 0.005, ES = 0.66). No significant difference was found in the level of vigorous physical activity.
A study evaluated the level of physical activity in the elderly. It assessed pre-dependent elderly individuals using the Telephone Assessment of Physical Activity (TAPA 1 and 2), finding no significant differences between groups (26). However, there was a moment effect for the intervention group on TAPA 1 and 2 (p = 0.06; p = 0.007), although the effect size (ES) for each outcome was not reported. In another study, the authors objectively evaluated the physical activity level of elderly cancer survivors using an accelerometer (25). There was a significant difference with an increase in light and moderate physical activity, accompanied by a significant increase in the number of daily steps, with large effect sizes in the intervention group (respectively, p = 0.03, ES = 0.72; p = 0.001, ES = 0.81; p = 0.01, ES = 0.96).
Adults with Parkinson's disease were evaluated for physical activity levels using a pedometer to measure step count. Still, no significant differences were found between groups, nor was there a moment effect (18). Two studies assessed physical activity levels in patients with Multiple Sclerosis, both subjectively, using the International Physical Activity Questionnaire (IPAQ). For adults with Multiple Sclerosis, there was a significant difference between groups for moderate physical activity (p = 0.01, η² = 0.20), and for all activity levels, there was a moment effect with small effect sizes (23). In women with Multiple Sclerosis, two distinct tele-exercise models, tele-pilates (p = 0.002, η² = 0.52) and tele-yoga (p < 0.001, η² = 0.68), showed significant differences between groups when compared to the control group.
One study assessed physical activity levels in healthy adults. Wilke et al. (2022) subjectively evaluated the levels using the Nordic Physical Activity Questionnaire-short (NPAQ) after eight weeks of tele-exercise, with four weeks of synchronous and four weeks of asynchronous sessions, measured at eight time points. The greatest gains occurred during the first four weeks of synchronous tele-exercise vs. the control group, with increases of 1.65 and 1.39 in moderate and light physical activity, respectively (6).
Two physical fitness batteries were also used to assess older adults. Buckinx et al. (2021) used the Short Physical Performance Battery (SPPB) (26). Although no group effect was observed, there was a significant moment effect in the intervention group, reflected in the increase in total SPPB score (p = 0.004). Hong et al. (2017) used the Senior Fitness Test (SFT), with only flexibility showing significant differences between groups (p = 0.019). For the moment effect, the 2 min-steps cardiorespiratory fitness test showed a significant improvement in the intervention group (p = 0.011). In the study conducted by Ayse et al. (2022), the authors identified significant differences in three SFT tests between groups: 2 min step test (p ≤ 0.001), Sit and Reach Test (p = 0.028), and 8 Step Up and Walk Test (p = 0.010). Additionally, significant differences were reported between groups in the SFT for the 4-meter Gait Speed (p = 0.011, ηp² = 0.20) and 8 Foot Up and Walk (p = 0.018, ηp² = 0.18) tests, with small effect sizes (15).
Three studies specifically evaluated balance. Ferrari et al. (2024) used the 30-second static balance test to assess older adults, but no significant differences were found between groups, nor was there a moment effect (8). However, using the Four-Square Step Test, Jones et al. (2024) observed a moment effect (p = 0.45, d = −0.37) (21). A moment effect was also observed (p = 0.019, ES = 0.569) in the balance of adults with Down syndrome, assessed with the Four Stage Balance Test (FICSIT-4) (27). The Timed Up and Go test, commonly used to assess balance and agility in adults with mobility limitations, was used in two studies. In the study mentioned before, by evaluating older adults, Jones et al. (21) did not observe significant differences. However, in adults with Down syndrome, a moment effect was observed (p = 0.043, ES = 0.569) (27).
Only three studies specifically assessed cardiorespiratory capacity. One study was conducted with overweight and obese women (17), another with adults with sleep apnea (19), and the last with adults who had recently had COVID-19 (28). No significant group effects were observed in any of the populations. However, for peak VO2, a significant difference with a small group-moment effect size was observed in overweight and obese women (p = 0.007, ES = 0.36) (17).
3.4.2 Quality of life
Six studies assessed quality of life using different tools. Ellis et al. (2019) used the Parkinson Disease Questionnaire 39 (PDQ-39) to evaluate the effect of tele-exercise on the quality of life in people with Parkinson's disease, finding no significant differences between groups. However, a significant improvement was observed in the subgroup of sedentary individuals (p = 0.03). In older adults in cancer remission, assessed with the Patient-Reported Outcomes Measurement Information System-29 (PROMIS), a moment effect was observed (p = 0.04, d = 0.33) (25).
Two studies evaluated individuals with Multiple Sclerosis using two different instruments: Overall Quality of Life and Health (ovQV), which assesses general quality of life, and Multiple Sclerosis Quality of Life-54 (MSQoL-54), specific to multiple sclerosis. Both instruments showed significant improvement with group effects (p = 0.01, η² = 0.12; p < 0.0001) respectively (22, 23).
Poon et al. (2024) used the Health-Related Quality of Life (HRQoL) scale to assess adults with recent COVID-19 and observed a significant difference between groups (p = 0.04). The last instrument used was the Nottingham Health Profile (NHP) to evaluate the quality of life related to health in isolated older adults, demonstrating significant improvement for this population (p = 0.011) (15).
3.4.3 Functional capacity
Three studies used the 6-Minute Walk Test (6MWT). Canton-Martínez et al. (2024) observed a significant improvement in the distance covered by the elderly in the intervention group (p ≤ 0.0001; ηp² = 0.39) (16). In adults with Parkinson's disease (18), only a moment effect was observed (p = 0.02), as well as in adults with sleep apnea syndrome (p = 0.003) (19).
Two other objective tests were used to evaluate older adults. Ferrari et al. (2024) used the 10-meter Walk Test and found no significant difference between groups; however, a moment effect with a moderate effect size was observed (p < 0.001, ES = 0.59) (8). For the 5-meter Walk Test, Jones et al. (2024) observed a moment effect (p = 0.02, d = 0.43) (21).
To assess functional capacity in women with multiple sclerosis, the Timed 25-Foot Walk Test was used, showing a significant difference between groups (p < 0.0001). Lastly, the Older Americans Resources and Services (OARS) functional status scale was used to evaluate functional capacity in pre-dependent elderly individuals. Although no significant difference was observed between groups, a moment effect was noted for the intervention group (p = 0.02) (26).
3.4.4 Strength
Physical capacity in terms of strength was assessed by nine studies, with the sit-to-stand test in its various forms being the most used instrument. Only two studies found significant differences between groups, both evaluating elderly individuals: Ayse et al. (2022) and Canton-Martínez et al. (2024) (respectively p ≤ 0.001 and p ≤ 0.0001, ηp² = 0.38) (15, 16). Six studies demonstrated a moment effect in the sit-to-stand test. In the sit-to-stand test, Gell et al. (2024) observed a moment effect in elderly individuals in remission from cancer (p < 0.0001) (25), Ferrari et al. (2024) in healthy elderly individuals (p = 0.009 ES = 0.26) (8), along with Hong et al. (2017) also in elderly individuals (p = 0.035) (20). Adults with recent COVID-19 also showed a moment effect (p = 0.003, d = 1.29) with a large effect size.
For the 5-sit to stand variation, a moment effect was observed in adults with Down syndrome with a moderate effect size (p = 0.014, ES = 0.55) (27), as well as in elderly individuals (p = 0.005, d = 0.51) (21). Upper limb strength was assessed in three studies. Obese and overweight women were evaluated using handgrip, and while there was no significant difference between groups, a moment effect with a small effect size was observed (p = 0.0006, ES = 0.25) (17). Similarly, adults with recent COVID-19 were also assessed using handgrip (p = 0.032, d = 0.50) (28). However, no group or moment effects were observed for arm curls in elderly individuals (20).
3.4.5 Pain
Three studies assessed the pain outcome. Wilke et al. (2022) used the Chronic Pain Grade Scale (CPGS) and found no significant differences between groups of healthy adults (6). For adults with multiple sclerosis, a significant difference between groups was observed with a small effect size (p < 0.0001, η² = 0.22) (23). Obese and overweight pregnant women were evaluated using the Oswestry Disability Index for low back pain, which showed significant differences between groups with a large effect size (p = 0.001, ES = 0.82) (7).
4 Discussion
Physical fitness was the most studied outcome, with the level of physical activity being the most frequently used assessment tool. Synchronous tele-exercise appears to be an effective method for improving physical activity levels in different populations, showing significant group effects and moment effects (p < 0.05) in various studies (6, 7, 22, 23, 25). Interaction effects between groups were highlighted in studies involving adult, elderly, and multiple sclerosis populations, indicating a specific impact of the intervention on these populations (6, 22, 23, 25) However, the study by Ellis et al. (2019), which used an asynchronous tele-exercise model, did not show any effects on physical fitness between groups or over time (18). The reviewed studies feature highly diverse populations, and this was the only study focusing on adults with Parkinson's disease. Nonetheless, in Ellis's study, when dividing the training group into active and sedentary participant subgroups, the sedentary subgroup showed significant improvements in the studied outcomes. However, it is not possible to assert that these improvements are solely attributable to the intervention.
Recent studies have correlated the level of physical activity in individuals with Parkinson's disease with walking ability and the level of disease impairment, showing that moderate to vigorous physical activity appears to have more beneficial effects in reducing this impairment (29, 30). In the study in question, participants were asked to perform 5–7 exercises for a minimum of 3 days per week, although these could be done daily for a six-month period. However, there is no report on the perceived effort level or the total weekly training volume completed by each participant. Asynchronous long-term tele-exercise programs seem to have a lower capacity for maintaining training volume (6), and intensity markers, such as perceived exertion, can be used to regulate training intensity. It is possible that the training program met the volume and intensity needs of the sedentary group but fell short of the physical capacity of the active group. Studies with more robust designs are necessary to better clarify potential intervention effects for this specific population.
For obese and overweight pregnant women, the asynchronous protocol did not appear to have a negative influence, as significant group and moment effects were observed for improvements in light and moderate physical activity levels (7). This aligns with the current literature, where structured exercise is shown to improve overall physical activity levels in pregnant women (31). The study conducted by Bernardo et al. (2024) was short in duration, lasting eight weeks, and followed FITT (frequency, intensity, type, and time) guidelines. The intervention group consisted exclusively of nutritional modifications, which may have contributed to the absence of interaction effects, as both groups followed the same asynchronous intervention protocol.
Regarding overall physical fitness levels evaluated by two test batteries (SPPB and SFT), synchronous tele-exercise proved effective in improving general fitness components in elderly populations, particularly concerning moment effects. This finding aligns with current literature on physical exercise and fitness in this population (32–34). Only one study used an asynchronous protocol, but it employed a mixed methodology, where the same group underwent both synchronous and asynchronous protocols, making it impossible to separately evaluate the effects of each type of tele-exercise (26). However, in the study by Buckinx et al. (2021), the authors observed a moment effect across all SPPB tests, which suggests a similarity with the other results (26). It is important to highlight that the observation of the moment effect indicates a modification but not necessarily one specific to intervention. Further studies using similar test batteries are needed to better clarify this issue.
When evaluating general physical fitness in populations with Down syndrome, synchronous tele-exercise appears to provide significant improvements (27), aligning with current literature (35, 36). However, more robust research with control groups and larger sample sizes is necessary to clarify potential positive effects on the physical fitness of this population, as the only study addressing this group is quasi-experimental.
Physical fitness was also specifically assessed in terms of cardiorespiratory improvement. Only synchronous tele-exercise appears to generate significant effects on peak VO2, which was observed only in the sedentary population of obese and overweight women (17). Other populations evaluated for the same outcome did not show significant differences, even when the protocol involved synchronous tele-exercise (19, 28). This result may be attributed to the characteristics of the study population, obese and overweight women who had not previously engaged in physical activity, making them more responsive to the short-term beneficial effects on cardiorespiratory capacity. The different training protocols could also influence the outcome. Similarly, the study by da Silva et al. (2022) was unique among the three studies in that it established load control and progression through perceived exertion, evolving the volume and intensity of the training protocol, which may have made the applied protocol more robust (17).
Regarding quality of life, six studies evaluated this outcome using different tools. For the elderly population, only synchronous tele-exercise protocols were used. Synchronous tele-exercise appears to improve domains related to quality of life, including loneliness (15, 25). These findings may be linked to the tele-exercise protocol being conducted in groups and in real-time, which could foster social connections between students and instructors.
Regarding synchronous tele-exercise, individuals affected by multiple sclerosis (MS) demonstrated significant interaction effects on quality of life, whether through MS-specific questionnaires or general quality of life assessments. The studies used synchronous tele-exercise protocols, specifically tele-yoga and tele-pilates (22, 23). In a recent systematic review conducted by Sánchez-Lastra et al. (2019), the authors reported significant improvements in the quality of life of people with multiple sclerosis who practised Pilates, supporting the findings of this review (37). However, only three studies evaluated quality of life improvements through Pilates, and only two reported significant differences (38, 39). For yoga, a recent systematic review (40) did not find significant differences in quality-of-life improvements for yoga practitioners, contrasting with the findings here. These cited studies have distinct methodological approaches, which may lead to conflicting results. Further research, such as high-quality randomised clinical trials, is needed to better understand the effects of these practices on the MS population.
Regarding asynchronous tele-exercise, the authors did not observe significant differences in the quality of life for people with Parkinson's (18). Nonetheless, the sedentary subgroup experienced a clinically relevant improvement in quality of life with the asynchronous tele-exercise protocol. It seems that in sedentary populations, even small doses of physical activity can lead to a noticeable improvement in perceived quality of life. The levels of motor and cognitive impairment associated with Parkinson's may contribute to the differences observed within the subgroup. Current literature suggests that physical inactivity worsens the quality of life in this population, indicating that the more inactive an individual is, the lower their quality-of-life indicators (41). However, more research is needed on the impact of both asynchronous and synchronous tele-exercise for this population.
When evaluating functional capacity, synchronous tele-exercise showed interaction effects in elderly individuals assessed with the 6 Min Walk Test (TC6) (16), and moment effect for the 10-Meter Walk Test (TC10) (21). Asynchronous tele-exercise demonstrated a moment effect for the 5-Meter Walk Test (TC5) (8), while a mixed synchronous and asynchronous tele-exercise protocol achieved a moment effect for subjective assessments (26). Despite the heterogeneity of the programs, tele-exercise appears to have the potential to improve functional capacity in the elderly, yet only one study demonstrated a significant interaction effect (16), highlighting the need for more robust studies with this population. It is important to note that current research suggests functional capacity may be influenced by the type of physical exercise program used. The literature indicates that multimodal programs may be more effective in improving the functional capacity of the elderly, which could influence the results (42, 43).
Other three different population groups showed a moment effect for synchronous tele-exercise (19, 22) and asynchronous tele-exercise (18). However, it is important to note that half of the studies addressing functional capacity are either quasi-experimental or non-randomised. More research with robust methodologies is needed to better understand the effects of tele-exercise on functional capacity.
Regarding strength outcomes, both synchronous and asynchronous tele-exercise protocols focused on lower limb strength, which was reflected in the results. Of the nine studies that assessed strength, six evaluated lower limb strength, two assessed lower and upper limb strength, and one assessed only superior limb strength. Only synchronous tele-exercise protocols (15, 16) showed significant differences between groups with interactions effects for the elderly population, aligning with current literature on the benefits of strength training for older adults (44–46). Only one study used asynchronous tele-exercise protocols. Although it did not find a significant group effect, a significant moment effect was observed (8).
Synchronous and asynchronous tele-exercise appear promising for increasing lower limb strength in the elderly population, with synchronous tele-exercise showing better results in this group. Synchronous tele-exercise appears promising for strength gains in adults with Down syndrome, aligning with current findings on resistance training for this population (35). However, the study in question lacks a control group, which renders the strength of this finding fragile, as it may not truly represent an improvement attributable to the intervention. Controlled studies are necessary to clarify whether there is an interaction effect between groups.
Only isometric strength seems to have been benefited by tele-exercise protocols for upper body strength. Women with obesity and overweight and people with recent COVID-19 showed moment effects on strength, but only with small effect sizes (17, 28). Generally, tele-exercise is performed with low load, few implements, and a focus on upper body exercises, which may influence the results regarding strength gains, particularly for upper body strength.
Finally, synchronous and asynchronous tele-exercise protocols appear to be effective regarding pain outcomes. Asynchronous tele-exercise showed significant improvement in reducing lower back pain with a large effect size in sedentary, obese, and overweight pregnant women (7). These findings align with current guidelines for pregnant women (47, 48), where structured physical exercise can help manage and reduce lower back pain. However, the study by Bernardo et al. (2024) was the only study that used asynchronous tele-exercise for the pain outcome (7).
Other studies evaluated pain with synchronous and mixed tele-exercise protocols. For people with multiple sclerosis, both tele-yoga and tele-pilates showed significant interactions effects improvements. Pilates and yoga, in their in-person form, are commonly used for pain management (49–52), and synchronous tele-exercise appears to provide similar benefits for people with multiple sclerosis. Synchronous tele-exercise also showed greater improvements in pain scales compared to asynchronous methods in adults during lockdown without specific pain complaints. However, both types of protocols reduced average perceived pain scores. The literature does not have a consensus on which type of exercise is most beneficial for pain, whether chronic, acute, or neuropathic. However, it is well-established that well-managed physical exercise is a crucial ally in reducing pain and improving the quality of life across various populations experiencing different types of pain (53). This seems to be reflected in the tele-exercise protocols. Currently, the methodological quality of studies on tele-exercise is low, and the heterogeneity of populations makes a robust analysis even more challenging. Nonetheless, tele-exercise emerges as a promising approach, particularly synchronous tele-exercise, which demonstrates more robust results and, typically, outcomes similar to those of in-person exercise when compared within the same population group. Thus, it offers a potential way to include various populations in physical exercise practices, particularly those with limited or no access to exercise environments. More studies with high methodological quality are needed to make a clearer view of the effects and limitations of tele-exercise.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
NG: Conceptualization, Formal Analysis, Investigation, Resources, Supervision, Writing – original draft. VR: Writing – review & editing, Conceptualization, Funding acquisition, Supervision. JV-A: Conceptualization, Formal Analysis, Investigation, Supervision, Writing – original draft. GL: Data curation, Formal Analysis, Investigation, Methodology, Writing – original draft. IG: Data curation, Formal Analysis, Investigation, Methodology, Writing – original draft. RP: Data curation, Formal Analysis, Investigation, Methodology, Writing – original draft. AF: Conceptualization, Validation, Visualization, Writing – review & editing. MC: Conceptualization, Funding acquisition, Project administration, Validation, Visualization, Writing – review & editing. EI: Software, Validation, Visualization, Writing – review & editing. ADG: Data curation, Methodology, Conceptualization, Writing – original draft. AF: Validation, Visualization, Writing – review & editing. MS: Validation, Visualization, Writing – review & editing. GZ: Conceptualization, Validation, Visualization, Writing – review & editing. CB: Validation, Visualization, Writing – review & editing. FM: Conceptualization, Funding acquisition, Project administration, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article by the European Union, grant number: 101089869—TELEexe4ALL—ERASMUS-SPORT-2022-SCP and by the Portuguese Foundation for Science and Technology (FCT), I.P., project number UIDB/04045/2020.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Matysiak M, Siger M, Walczak A, Ciach A, Jonakowski M, Stasiołek M. The influence of COVID-19 pandemic lockdown on the physical activity of people with multiple sclerosis. The role of online training. Mult Scler Relat Disord. (2022) 63:103843. doi: 10.1016/j.msard.2022.103843. Available online at: https://www.scopus.com/inward/record.uri?eid=2-s2.0-85129856420&doi=10.1016%2fj.msard.2022.103843&partnerID=40&md5=4ce56db2f418f9472869d8e5343fb8fb.35550480
2. Fabbrizio A, Fucarino A, Cantoia M, De Giorgio A, Garrido ND, Iuliano E, et al. Smart devices for health and wellness applied to tele-exercise: an overview of new trends and technologies such as IoT and AI. Healthcare. (2023) 11(12):1805. doi: 10.3390/healthcare11121805
3. Ho V, Merchant RA. The acceptability of digital technology and tele-exercise in the age of COVID-19: cross-sectional study. JMIR Aging. (2022) 5(2):e33165. doi: 10.2196/33165
4. Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: definitions and distinctions for health-related research. Public Health Rep. (1985) 100(2):126–31.3920711
5. Toft B, Rodkjaer L, Sorensen L, Saugbjerg M, Bekker H, Modrau I. Feasibility of early digital health rehabilitation after cardiac surgery in the elderly: a qualitative study. BMC Health Serv Res. (2024) 24(1):113. doi: 10.1186/s12913-024-10601-3
6. Wilke J, Mohr L, Yuki G, Bhundoo A, Jiménez-Pavón D, Laiño F, et al. Train at home, but not alone: a randomised controlled multicentre trial assessing the effects of live-streamed tele-exercise during COVID-19-related lockdowns. Br J Sports Med. (2022) 56(12):667–75. doi: 10.1136/bjsports-2021-104994
7. Bernardo D, Bobadilla-Agouborde C, Festas C, Carvalho C, Abdalla PP, Amezcua-Prieto C, et al. Feasibility, clinical efficacy, and maternal outcomes of a remote exercise program in pregnant women with obesity: the GROB randomized control pilot study. CEOG. (2024) 51(3):70.
8. Ferrari L, Bochicchio G, Bottari A, Scarton A, Cavedon V, Milanese C, et al. Feasibility and effectiveness of a 6-month, home-based, resistance exercise delivered by a remote technological solution in healthy older adults. Arch Gerontol Geriatr. (2024) 127:105559. doi: 10.1016/j.archger.2024.105559
9. Ho V, Merchant RA. The acceptability of digital technology and tele-exercise in the age of COVID-19: cross-sectional study. JMIR Aging. (2022) 5(2):e33165. doi: 10.2196/33165
10. Physical activity [Internet]. (2024). Available online at: https://www.who.int/news-room/fact-sheets/detail/physical-activity (Accessed July 29, 2024).
11. Silva AG, Simões P, Queirós A, Rocha N, Rodrigues M. Effectiveness of mobile applications running on smartphones to promote physical activity: a systematic review with meta-analysis. Int J Environ Res Public Health. (2020) 17(7):2251. doi: 10.3390/ijerph17072251
12. Snoswell CL, Taylor ML, Comans TA, Smith AC, Gray LC, Caffery LJ. Determining if telehealth can reduce health system costs: scoping review. J Med Internet Res. (2020) 22(10):e17298. doi: 10.2196/17298
13. Park AH, Zhong S, Yang H, Jeong J, Lee C. Impact of COVID-19 on physical activity: a rapid review. J Glob Health. (2022) 12:05003. doi: 10.7189/jogh.12.05003
14. Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 Explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. Br Med J. (2021) 372:n160. doi: 10.1136/bmj.n160
15. Ayse ZA, Kardes K, Acikbas E, Demirhan F, Sagir K, Avcil E. The effectiveness of synchronous tele-exercise to maintain the physical fitness, quality of life, and mood of older people—a randomized and controlled study. Eur Geriatr Med. (2022) 13(5):1177–85. doi: 10.1007/s41999-022-00672-y
16. Canton-Martínez E, Rentería I, Machado-Parra JP, Reyes RA, Moncada-Jiménez J, Johnson DK, et al. A virtually supervised exercise program improved fitness and mental wellness in healthy and comorbidity older adult individuals during the COVID-19 pandemic. Front Public Health. (2024) 12:1328518. doi: 10.3389/fpubh.2024.1328518
17. da Silva J, Painelli V, Santos I, Marques D, de Oliveira F, de Oliveira L, et al. No effect of combined tele-exercises and nutritional coaching on anthropometric, body composition or exercise capacity outcomes in overweight and obese women: a randomized clinical trial. Nutr Hosp. (2022) 39(2):329–36. doi: 10.20960/nh.03822
18. Ellis TD, Cavanaugh JT, DeAngelis T, Hendron K, Thomas CA, Saint-Hilaire M, et al. Comparative effectiveness of mHealth-supported exercise compared with exercise alone for people with Parkinson disease: randomized controlled pilot study. Phys Ther. (2019) 99(2):203–16. doi: 10.1093/ptj/pzy131
19. Eyuboglu F, Inal-Ince D, Karamancioglu B, Vardar-Yagli N, Kaya-Utlu D, Dalkilic O, et al. Effect of tele-yoga on aerobic capacity, respiratory muscle strength, and cognitive performance in patients with obstructive sleep apnea syndrome. Heart Lung. (2023) 62:157–67. doi: 10.1016/j.hrtlng.2023.07.005
20. Hong J, Kim J, Kim SW, Kong HJ. Effects of home-based tele-exercise on sarcopenia among community-dwelling elderly adults: body composition and functional fitness. Exp Gerontol. (2017) 87:33–9. doi: 10.1016/j.exger.2016.11.002
21. Jones D, Robinson M, Selfe T, Barnes L, Dierkes M, Shawley-Brzoska S, et al. Prepandemic feasibility of tele-exercise as an alternative delivery mode for an evidence-based, Tai Ji Quan fall-prevention intervention for older adults. J Aging Phys Act. (2024) 1(aop):1–12. doi: 10.1123/japa.2023-0226
22. Najafi P, Hadizadeh M, Cheong JPG, Mohafez H, Abdullah S, Poursadeghfard M. Effects of tele-pilates and tele-yoga on biochemicals, physical, and psychological parameters of females with multiple sclerosis. J Clin Med. (2023) 12(4):1585. doi: 10.3390/jcm12041585. Available online at: https://www.scopus.com/inward/record.uri?eid=2-s2.0-85148900660&doi=10.3390%2fjcm12041585&partnerID=40&md5=dd8bbd9cc1a90a080b9001d8ec7d78dc.36836119
23. Najafi P, Hadizadeh M, Cheong JPG, Motl RW, Abdullah S, Mohafez H, et al. Effects of tele-exercise training on physical and mental health and quality of life in multiple sclerosis: do the effects differ by modality and clinical disease course? Mult Scler Relat Disord. (2023) 80:105129. doi: 10.1016/j.msard.2023.105129. Available online at: https://www.scopus.com/inward/record.uri?eid=2-s2.0-85176944581&doi=10.1016%2fj.msard.2023.105129&partnerID=40&md5=1f1c1ca25fb388308153db5f67edcc8e.37977056
24. Jones DL, Robinson M, Dierkes M, Selfe TK. O.4.1-1 impact of a pre-pandemic, tele-exercise, fall-prevention intervention on outcomes in older adults. Eur J Public Health. (2023) 33(Supplement_1):ckad133.166. doi: 10.1093/eurpub/ckad133.166
25. Gell N, Dittus K, Caefer J, Martin A, Bae M, Patel K. Remotely delivered exercise to older rural cancer survivors: a randomized controlled pilot trial. J Cancer Surviv. (2024) 18(2):596–605. doi: 10.1007/s11764-022-01292-y
26. Buckinx F, Aubertin-Leheudre M, Daoust R, Hegg S, Martel D, Martel-Thibault M, et al. Feasibility and acceptability of remote physical exercise programs to prevent mobility loss in pre-disabled older adults during isolation periods such as the COVID-19 pandemic. J Nutr Health Aging. (2021) 25(9):1106–11. doi: 10.1007/s12603-021-1688-1
27. Guerrero K, Umagat A, Barton M, Martinez A, Ho KY, Mann S, et al. The effect of a telehealth exercise intervention on balance in adults with down syndrome. J Appl Res Intellect Disabil. (2023) 36(2):385–93. doi: 10.1111/jar.13068
28. Poon ETC, Sun F, Tse ACY, Tsang JH, Chung AYH, Lai YYY, et al. Effectiveness of tele-exercise training on physical fitness, functional capacity, and health-related quality of life in non-hospitalized individuals with COVID-19: the COFIT-HK study. J Exerc Sci Fit. (2024) 22(2):134–9. doi: 10.1016/j.jesf.2024.01.003
29. Domingues VL, Pompeu JE, de Freitas TB, Polese J, Torriani-Pasin C. Physical activity level is associated with gait performance and five times sit-to-stand in Parkinson's disease individuals. Acta Neurol Belg. (2022) 122(1):191–6. doi: 10.1007/s13760-021-01824-w
30. Tsukita K, Sakamaki-Tsukita H, Takahashi R. Long-term effect of regular physical activity and exercise habits in patients with early Parkinson disease. Neurology. (2022) 98(8):e859–71. doi: 10.1212/WNL.0000000000013218
31. Knudsen SdP, Alomairah SA, Roland CB, Jessen AD, Hergel IM, Clausen TD, et al. Effects of structured supervised exercise training or motivational counseling on pregnant women’s physical activity level: FitMum - Randomized controlled trial. J Med Internet Res. (2022) 24(7):e37699. doi: 10.2196/37699
32. Baek JE, Hyeon SJ, Kim M, Young CH, Hahm SC. Effects of dual-task resistance exercise on cognition, mood, depression, functional fitness, and activities of daily living in older adults with cognitive impairment: a single-blinded, randomized controlled trial. BMC Geriatr. (2024) 24:369. doi: 10.1186/s12877-024-04942-1
33. Buriticá-Marín ED, Daza-Arana JE, Jaramillo-Losada J, Riascos-Zuñiga AR, Ordoñez-Mora LT. Effects of a physical exercise program on the physical capacities of older adults: a quasi-experimental study. Clin Interv Aging. (2023) 18:273–82. doi: 10.2147/CIA.S388052
34. Todde F, Melis F, Mura R, Pau M, Fois F, Magnani S, et al. A 12-week vigorous exercise protocol in a healthy group of persons over 65: study of physical function by means of the senior fitness test. BioMed Res Int. (2016) 2016:7639842. doi: 10.1155/2016/7639842
35. Montalva-Valenzuela F, Castillo-Paredes A, Farias-Valenzuela C, Andrades-Ramirez O, Concha-Cisternas Y, Guzmán-Muñoz E. Effects of exercise, physical activity, and sports on physical fitness in adults with down syndrome: a systematic review. AIMS Public Health. (2024) 11(2):577–600. doi: 10.3934/publichealth.2024029
36. Paul Y, Ellapen TJ, Barnard M, Hammill HV, Swanepoel M. The health benefits of exercise therapy for patients with down syndrome: a systematic review. Afr J Disabil. (2019) 8:576. doi: 10.4102/ajod.v8i0.576
37. Sánchez-Lastra MA, Martínez-Aldao D, Molina AJ, Ayán C. Pilates for people with multiple sclerosis: a systematic review and meta-analysis. Mult Scler Relat Disord. (2019) 28:199–212. doi: 10.1016/j.msard.2019.01.006
38. Bulguroglu I, Guclu-Gunduz A, Yazici G, Ozkul C, Irkec C, Nazliel B, et al. The effects of Mat Pilates and reformer pilates in patients with multiple sclerosis: a randomized controlled study. NeuroRehabilitation. (2017) 41(2):413–22. doi: 10.3233/NRE-162121
39. van der Linden ML, Bulley C, Geneen LJ, Hooper JE, Cowan P, Mercer TH. Pilates for people with multiple sclerosis who use a wheelchair: feasibility, efficacy and participant experiences. Disabil Rehabil. (2014) 36(11):932–9. doi: 10.3109/09638288.2013.824035
40. Shohani M, Kazemi F, Rahmati S, Azami M. The effect of yoga on the quality of life and fatigue in patients with multiple sclerosis: a systematic review and meta-analysis of randomized clinical trials. Complement Ther Clin Pract. (2020) 39:101087. doi: 10.1016/j.ctcp.2020.101087
41. Khan A, Ezeugwa J, Ezeugwu VE. A systematic review of the associations between sedentary behavior, physical inactivity, and non-motor symptoms of Parkinson’s disease. PLoS One. (2024) 19(3):e0293382. doi: 10.1371/journal.pone.0293382
42. Izquierdo M, Merchant RA, Morley JE, Anker SD, Aprahamian I, Arai H, et al. International exercise recommendations in older adults (ICFSR): expert consensus guidelines. J Nutr Health Aging. (2021) 25(7):824–53. doi: 10.1007/s12603-021-1665-8
43. Valenzuela PL, Castillo-García A, Morales JS, Izquierdo M, Serra-Rexach JA, Santos-Lozano A, et al. Physical exercise in the oldest old. Compr Physiol. (2019) 9(4):1281–304. doi: 10.1002/cphy.c190002
44. Fragala MS, Cadore EL, Dorgo S, Izquierdo M, Kraemer WJ, Peterson MD, et al. Resistance training for older adults: position statement from the national strength and conditioning association. J Strength Cond Res. (2019) 33(8):2019–52. doi: 10.1519/JSC.0000000000003230
45. Lu L, Mao L, Feng Y, Ainsworth BE, Liu Y, Chen N. Effects of different exercise training modes on muscle strength and physical performance in older people with sarcopenia: a systematic review and meta-analysis. BMC Geriatr. (2021) 21(1):708. doi: 10.1186/s12877-021-02642-8
46. Schott N, Johnen B, Holfelder B. Effects of free weights and machine training on muscular strength in high-functioning older adults. Exp Gerontol. (2019) 122:15–24. doi: 10.1016/j.exger.2019.03.012
47. Ribeiro MM, Andrade A, Nunes I. Physical exercise in pregnancy: benefits, risks and prescription. J Perinat Med. (2022) 50(1):4–17. doi: 10.1515/jpm-2021-0315
48. Santos FF, Lourenço BM, Souza MB, Maia LB, Oliveira VC, Oliveira MX. Prevention of low back and pelvic girdle pain during pregnancy: a systematic review and meta-analysis of randomised controlled trials with GRADE recommendations. Physiotherapy. (2023) 118:1–11. doi: 10.1016/j.physio.2022.09.004
49. Alexander HB, Munger Clary HM, Shaltout HA, Fountain NB, Duncan P, Brubaker P, et al. Developing optimized physical activity interventions for drug-resistant epilepsy: challenges and lessons learned from a remote exercise intervention pilot trial. Epilepsy Behav Rep. (2024) 27:100693. doi: 10.1016/j.ebr.2024.100693
50. Sonmezer E, Özköslü MA, Yosmaoğlu HB. The effects of clinical pilates exercises on functional disability, pain, quality of life and lumbopelvic stabilization in pregnant women with low back pain: a randomized controlled study. J Back Musculoskelet Rehabil. (2021) 34(1):69–76. doi: 10.3233/BMR-191810
51. Taşpınar G, Angın E, Oksüz S. The effects of Pilates on pain, functionality, quality of life, flexibility and endurance in lumbar disc herniation. J Comp Eff Res. (2023) 12(1):e220144. doi: 10.2217/cer-2022-0144
52. Yu Z, Yin Y, Wang J, Zhang X, Cai H, Peng F. Efficacy of Pilates on pain, functional disorders and quality of life in patients with chronic low back pain: a systematic review and meta-analysis. Int J Environ Res Public Health. (2023) 20(4):2850. doi: 10.3390/ijerph20042850
Keywords: physical exercise, elderly, technology, health, tele-exercise
Citation: Garrido ND, Reis VM, Vilaça-Alves JM, Lucas GC, Godinho IL, Peixoto R, Fucarino A, Cantoia M, Iuliano E, De Giorgio A, Fabbrizio A, Suasa M, Zimatore G, Baldari C and Macaluso F (2025) Impact of tele-exercise on quality of life, physical fitness, functional capacity and strength in different adult populations: a systematic review of clinical trials. Front. Sports Act. Living 7:1505826. doi: 10.3389/fspor.2025.1505826
Received: 3 October 2024; Accepted: 6 January 2025;
Published: 30 January 2025.
Edited by:
Ronald F. Zernicke, University of Michigan, United StatesReviewed by:
Eduardo Carballeira, University of La Laguna, SpainHugo Vieira Pereira, Lusofona University, Portugal
Copyright: © 2025 Garrido, Reis, Vilaça-Alves, Lucas, Godinho, Peixoto, Fucarino, Cantoia, Iuliano, De Giorgio, Fabbrizio, Suasa, Zimatore, Baldari and Macaluso. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nuno Domingos Garrido, bmRnYXJyaWRvQGdtYWlsLmNvbQ==
†These authors have contributed equally to this work and share first authorship