 Nathali Carvajal-Tello1,†
Nathali Carvajal-Tello1,† José Guillermo Ortega2,†
José Guillermo Ortega2,† Andrés Fabricio Caballero-Lozada3,4,5*†
Andrés Fabricio Caballero-Lozada3,4,5*† María Juliana Devia-Quiñonez1,†Isabella González-Calzada1,†Daniela Rojas-Hernández1,†
María Juliana Devia-Quiñonez1,†Isabella González-Calzada1,†Daniela Rojas-Hernández1,† Alejandro Segura-Ordoñez1,3,†
Alejandro Segura-Ordoñez1,3,†
- 1Grupo de Investigación Salud y Movimiento, Faculty of Health, Universidad Santiago de Cali, Cali, Colombia
- 2Grupo de Investigación de Ciencias Básicas y Clínicas de la Salud, Department of Basic Health Sciences, Pontificia Universidad Javeriana, Cali, Colombia
- 3Grupo de Investigación en Anestesia INVANES, Department of Anesthesiology and Resuscitation, Universidad del Valle, Cali, Colombia
- 4Department of Anesthesiology, Hospital Universitario del Valle, Cali, Colombia
- 5Intensive Care Unit, Fundación Hospital San José de Buga, Buga, Colombia
Background: This systematic review and meta-analysis aimed to assess the impact of inspiratory muscle training (IMT) on lung function parameters (MIP, MEP, FEV1, and FVC) between both elite and non-elite swimmers.
Methods: We searched for controlled clinical trials (CCT) and prospective longitudinal studies (PLS) in elite and non-elite swimmers following an inspiratory muscle training (IMT) protocol with a standardized device, published between 2012 and 2023. The databases used in the search were PubMed, Science Direct, Scopus, Springer, Cochrane Central Register of Controlled Trials, and Google Scholar. The primary outcome assessed was the impact of IMT on lung function parameters, including MIP, MEP, FEV1, and FVC.
Results: We selected 13 articles involving 277 subjects aged 11–21 years, with 61.4% being male, and 84.6% being elite swimmers. The most commonly used IMT device was the PowerBreathe®, prescribed for 3–12 weeks, 1–2 sessions per day, 3–6 times per week, with 30 repetitions, starting at 50% of MIP and progressing up to 80%. The meta-analysis showed that IMT was associated with a higher MIP (MD = 29.35 cmH2O, 95% CI: 13.04–45.65 cmH2O, p < 0.01) without affecting FEV1 and FVC.
Conclusion: The swimmers that used IMT improved muscle strength, specifically MIP, without changes in MEP, FEV1, and FVC.
1 Introduction
Swimming is an activity performed for recreational or competitive purposes that involves exercising while submerged in water. It imposes significant demands on the respiratory muscles due to the higher hydrostatic pressure surrounding the thoracic cavity. This leads to an increase in the speed of inspiratory muscle contraction and tidal volume (1, 2). The workload on respiratory muscles during swimming can lead to fatigue and dyspnea. This is primarily due to these muscles having to overcome the hydrostatic pressure which limits the thoracic expansion, ultimately reducing performance (3, 4). During vigorous exercise, the demands on the respiratory system to function properly rise significantly (5). The respiratory system acts as one of the main metabolic buffers by increasing the strength of the respiratory muscles to ensure ventilation and maintain normal acid-base balance in the blood (6). The efficiency of the respiratory muscles is crucial; if they are inefficient, it could lead to a hypercapnic state where working muscles tire faster because the removal of metabolites cannot keep up with the production of CO2 (1). The high levels of sustained work required from the respiratory muscles during intense exercise can lead to respiratory muscle fatigue. However, having respiratory muscles with enhanced contractile responsiveness and increased force generation capacity could result in better fatigue tolerance and a reduced perception of breathlessness during exercise (7).
Hence, improving lung function and respiratory muscle strength has been recommended as a potential strategy to enhance physical performance in swimming (8). One suggested strategy to increase the strength of respiratory muscles, including the diaphragm, is Inspiratory Muscle Training (IMT), which compels the inspiratory muscles to overcome increased force, thereby enhancing their overall strength by introducing resistance during inspiration (9). It is well known that when postural demands increase, the activation of the diaphragm increases (10). Diaphragmatic and abdominal stability and contraction can increase glide performance by boosting gliding ability which plays a significant part in race performance, preserving the aerodynamic body posture, which is critical for swimmers (11).
Thus, is expected that IMT has an impact on parameters of pulmonary function in swimmers, including maximum inspiratory pressure (MIP), which represents the maximal force generated by the inspiratory muscles against resistance (12), reflecting their strength and endurance; the maximum expiratory pressure (MEP), an indicator of the maximal force exerted during expiration (13); the forced expiratory volume in 1 s (FEV1) which is the parameter of the volume of air forcefully exhaled within the first second of forced expiration (14); and forced vital capacity (FVC), which encompasses the total volume of air forcibly exhaled after maximum inhalation (15).
However, there is currently no consensus on the effects of Inspiratory Muscle Training (IMT) on lung function in swimmers. Therefore, knowing the impact of this type of training on physiological lung parameters is crucial to support the practice and prescription of IMT in swimming training programs. For this reason, this systematic review and meta-analysis aimed to evaluate the effect of IMT on lung function parameters (MIP, MEP, FEV1, and FVC) in both elite and non-elite swimmers.
2 Materials and methods
2.1 Literature search
We included data from CCT and PLS published in the period 2012–2023, the search was carried out in the electronic databases: PubMed, Science Direct, Scopus, Springer, Cochrane Central Register of Controlled Trials, and Google Scholar, between 01/11/2022 and 31/05/2023, without language restriction. The study complies with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) (16). Mesh terms with combinations of boolean operators according to the database were used to search: (athletes OR professional athlete OR professional athletes OR athletic performance) AND (water sport OR swimming OR diving) AND (respiratory muscle OR diaphragm OR intercostal muscles OR ventilatory muscle OR muscles) AND (Respiratory Muscle Training OR muscle training, respiratory OR training OR resistance).
2.2 Inclusion criteria and selection process
After removing duplicated reports, two researchers independently assessed the titles and abstracts for eligibility criteria. Any disagreements were resolved by a third researcher. We included studies with elite or non-elite swimmers where IMT was performed using standardized devices such as Threshold IMT®, Threshold PEP®, and PowerBreathe®. We excluded studies that included subjects diagnosed with pulmonary, cardiac, or musculoskeletal disease, chronic or acute illness, and cognitive disorders. Additionally, we excluded systematic reviews, case series, and case reports.
2.3 Methodological quality
The quality of the CCT was evaluated using the PEDro scale, which consists of 11 items. A score of 1 is given if the item complies and 0 if it does not comply. The methodological quality is classified as low, intermediate or high based on the sum of the score. The aspects considered include an adequate control group, blinding, and randomization (17). The Minors scale was used to assess PLS. This scale consists of 12 items, with a score of 0 for not reported, 1 for reported but inadequate, and 2 for reported and adequate. The scale considers aspects such as objectives, prospective data collection, blinding, sample size calculation, and adequate statistical analysis, the ideal score for non-comparative studies is 16, and for comparative studies, it is 24 (18).
2.4 Data extraction and analysis
Two authors independently extracted data from eligible studies. The data extracted were recorded on a standardized data collection form. We included bibliographic characteristics such as authors, title, database, journal, type of study, country, continent, language, year and objective. Participant characteristics, such as sex, age, height, weight, and competitive level, were also collected. Intervention characteristics, such as the type of training, starting intensity, intensity progression, frequency per week, session, and intervention duration, were documented. The evaluation of respiratory muscle training on performance included parameters such as Maximum Inspiratory Pressure (MIP), Maximum Expiratory Pressure (MEP), Forced Expiratory Volume in the first second (FEV1), and Forced Vital Capacity (FVC). Disagreements were resolved by consensus.
2.5 Statistical analysis
A qualitative summary was carried out according to study design, characteristics, sample characteristics, number of subjects, type of instruments used to measure respiratory muscle training (Threshold®, PowerBreathe®), swimming performance (maximum apnea test, 50, 100, 200, 200, 3000-m pool), dyspnea (Borg scale), and lung capacity and, volumes (spirometry).
The primary outcomes for the meta-analysis, were the mean differences (MD) for MIP, FEV, and FVC. Quantitative analyses were only conducted if comparable outcome data from four or more studies were available. In cases where study data were only available from figures, we extracted the data using the validated software Plot Digitizer (19). When baseline and final values were given, we computed changes from the baseline. Missing standard deviation (SD) values were imputed using an imputed correlation coefficient (20). When a study presents multiple interventions with IMT and a unique control group, the groups IMT were combined into a single group (21). For quantitative synthesis, we used a random effects model with restricted maximum likelihood to estimate between-study variability (τ2) and Knapp-Hartung adjustment was used for small numbers of studies with considerable heterogeneity (22, 23). The I2 index was used to determine the heterogeneity, an I2 ≥ 75% indicated high variation. For all MDs, the reference group was the control group. The publication bias for a few studies was examined qualitatively via visual inspection of the Doi plot, and quantitatively using the Luis Furuya-Kanamori (LFK) index. LFK indices <1, between 1 and 2, and >2, represent no, minor, and major asymmetry, respectively (24). To evaluate the robustness of the results, we performed a sensitivity analysis by excluded one study at a time (Leave-one-out analysis). Additionally, subgroup analysis was conducted according to the type of control group. For outcomes with significant effects we performed a meta-regression, to know if some factors (age, outcome at baseline, duration of intervention) influenced the effects. The results were considered statistically significant if p ≤ 0.05. The statistical analyses were conducted with the statistical software R (version 4.0.3), and the packages meta (Version 6.5.0) and metasens (Version 1.5.2) (25, 26).
3 Results
In this systematic search, we obtained a total of 2016 reports. After eliminating 1,212 duplicates, 804 articles were assessed based on titles and abstracts, of which 755 were excluded. Subsequently, 49 full-text articles were reviewed, and 36 studies were excluded either because they did not meet the inclusion criteria or because they had one or more exclusion criteria. A total of 13 articles were selected for the meta-analysis (Figure 1).
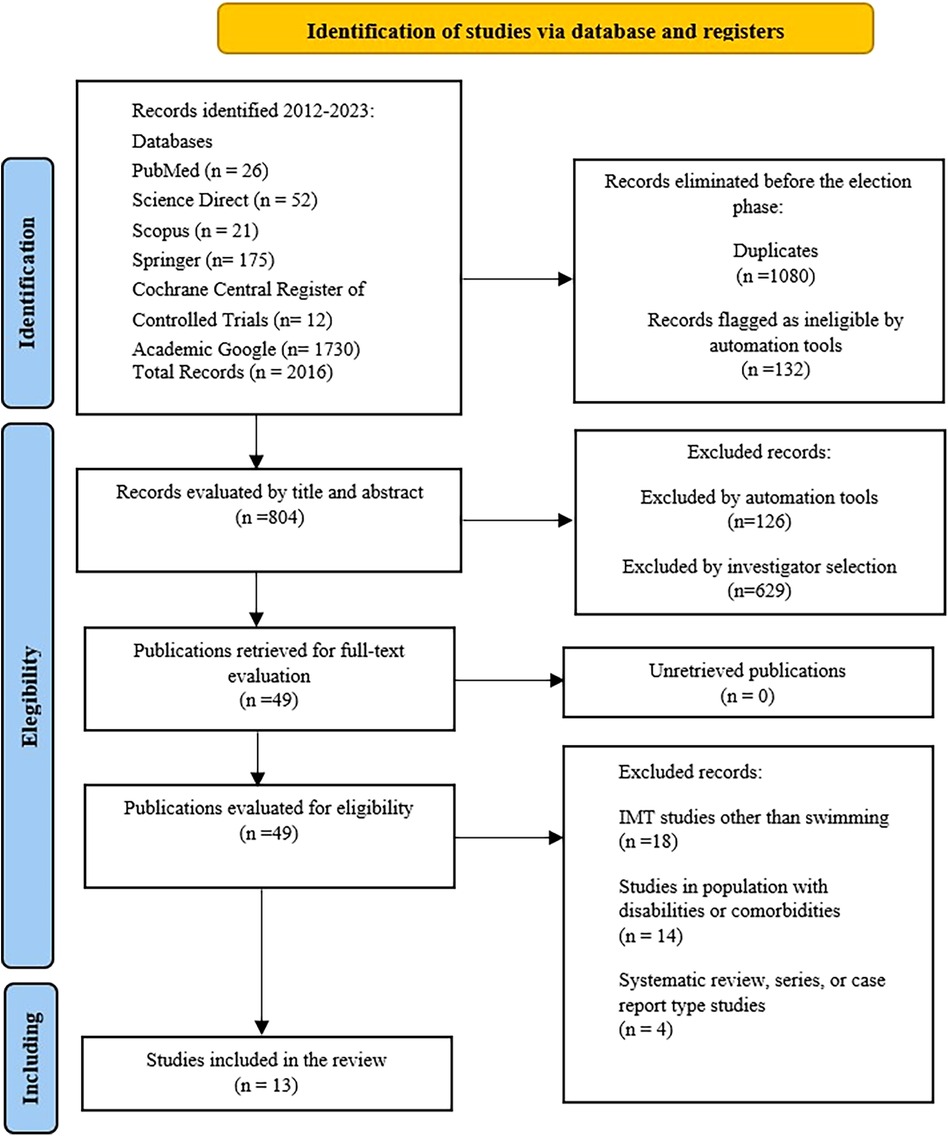
Figure 1. Prisma flow diagram.
3.1 Characteristics of the studies
Of the 13 studies selected, 54% (n = 7) were found in Pubmed and 42% (n = 4) in Google Scholar. According to design, 11 studies were controlled clinical trials (CCT) and 2 studies were prospective longitudinal studies (PLS). Considering a geographical region, 54% (n = 7) were from Europe, 23% (n = 3) from Asia, 23% (n = 3) from America, 92% (n = 12) of the articles were written in the English language (Table 1).
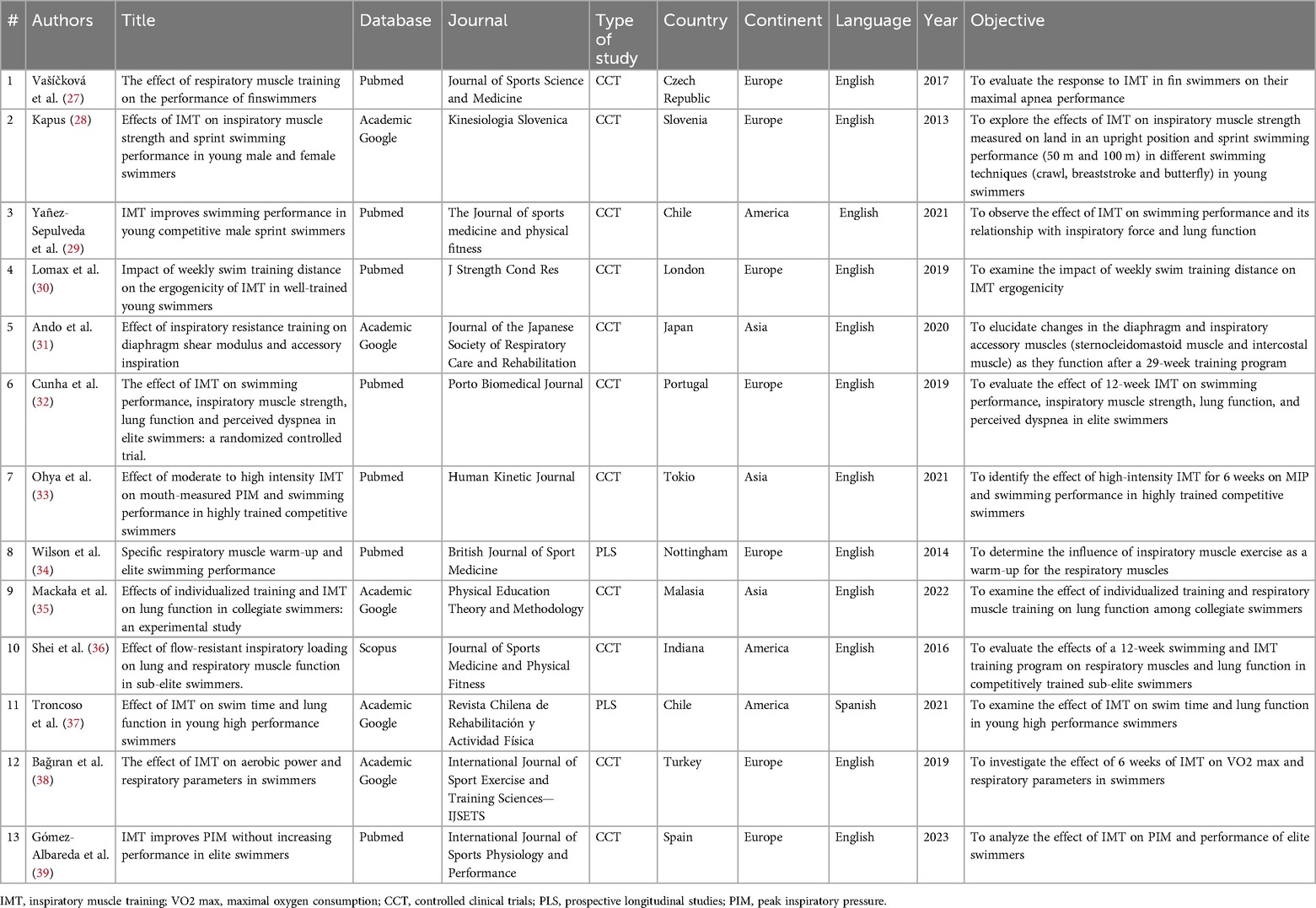
Table 1. Characteristics of the studies included.
The study included a total of 277 subjects aged between 11 and 21 years, with 61.4% (n = 170) being male. Four studies exclusively included male subjects, while 9 studies included both sexes. The height of the subjects ranged from 153 ± 0.18 to 179.42 ± 0.74, and their weight ranged from 47.4 ± 10.5 to 75.2 ± 9.05 kg (Table 2). The participants were predominantly elite swimmers, comprising 84.6% (n = 11), with 1–10 years of experience and a training time of 6–35 h per week. Two studies (15.4%; n = 2) were conducted on non-elite swimmers who trained three times per week.
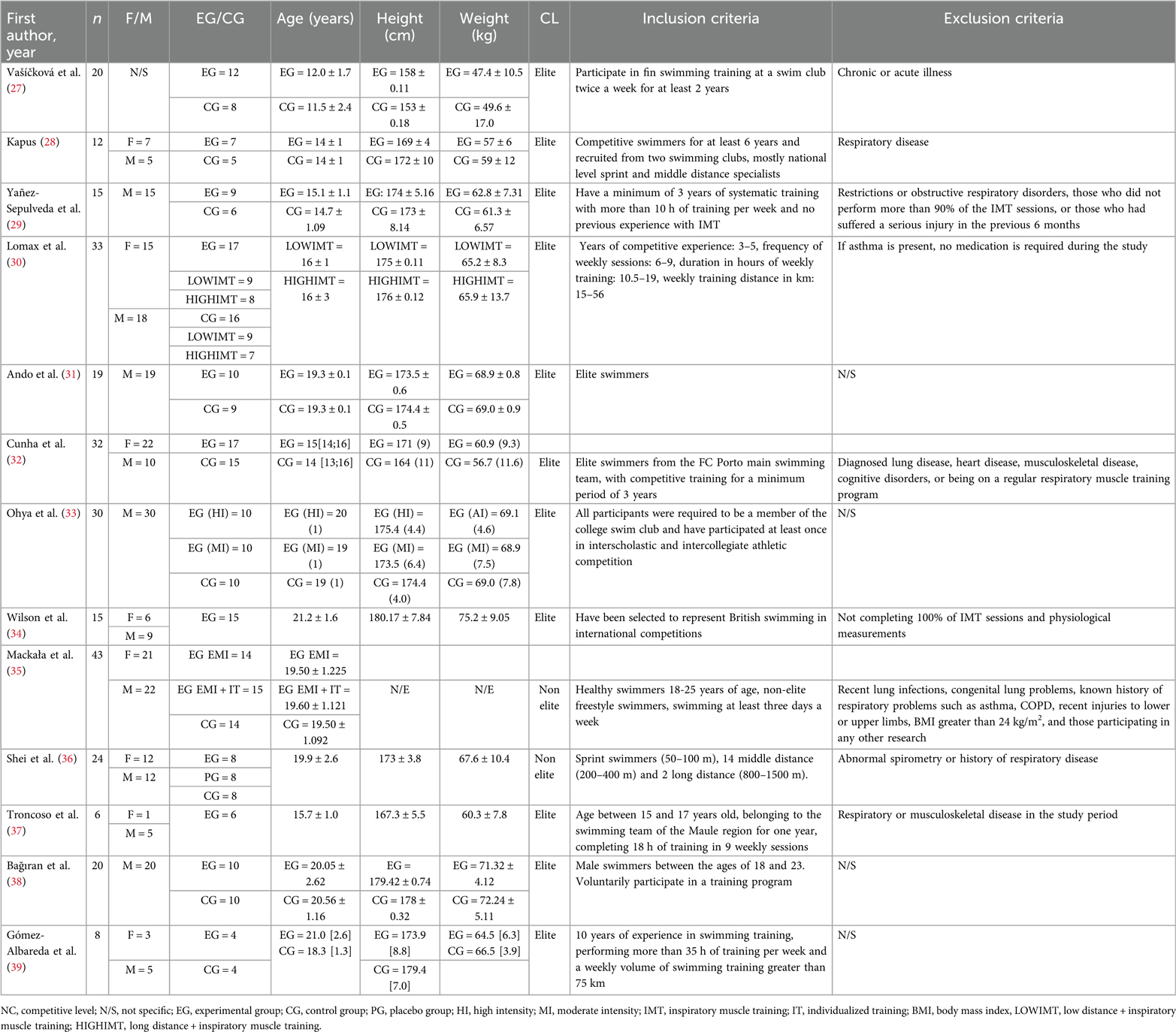
Table 2. Characteristics of the participants of the studies included.
3.2 Characteristics of interventions
The IMT training was conducted using the PowerBreathe® device in 92.3% (n = 12) of the studies (Table 3). The initial intensity of IMT ranged from 15% to 80% of the MIP, with a progression in training intensity and loads from 5% to 50% per week; in two studies, no progression protocol was specified (30, 31). Concerning the frequency and duration of IMT application, the majority of the reports (27–33, 37–39) implemented 2 sessions/day, 6 times/week over 4–12 weeks, with the duration of the session varying between 10 and 30 inspiratory efforts. One study reported a 15-min duration with the training device (27).
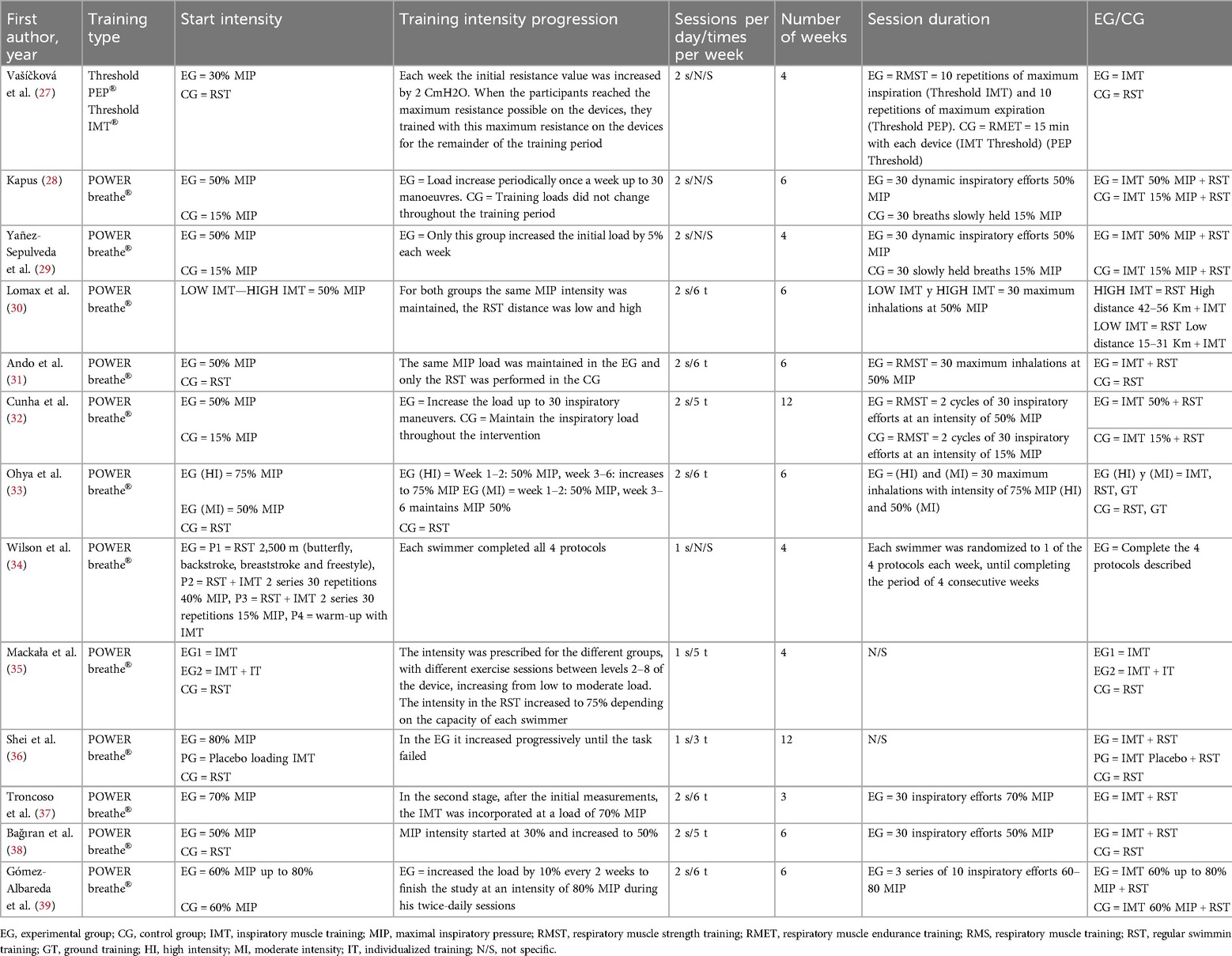
Table 3. Description of the interventions included in the studies.
3.3 Evaluation of the effect of respiratory muscle training on performance in swimming athletes
Regarding the evaluation of the effect of IMT on performance in swimming athletes, we found that they used crawl tests at distances of 50, 100, and 200 m (28–30, 34, 35, 37). Kapus (28) showed that he performed two additional tests in butterfly and breaststroked 50 m, Vašíčková et al. (27), who performed apnea test and Gómez-Albareda et al. (39) carry out 3,000 m crawl test. Only 3 studies with measurements pre- and post-IMT found statistically significant changes in test performance (28, 29, 37) (Table 4).
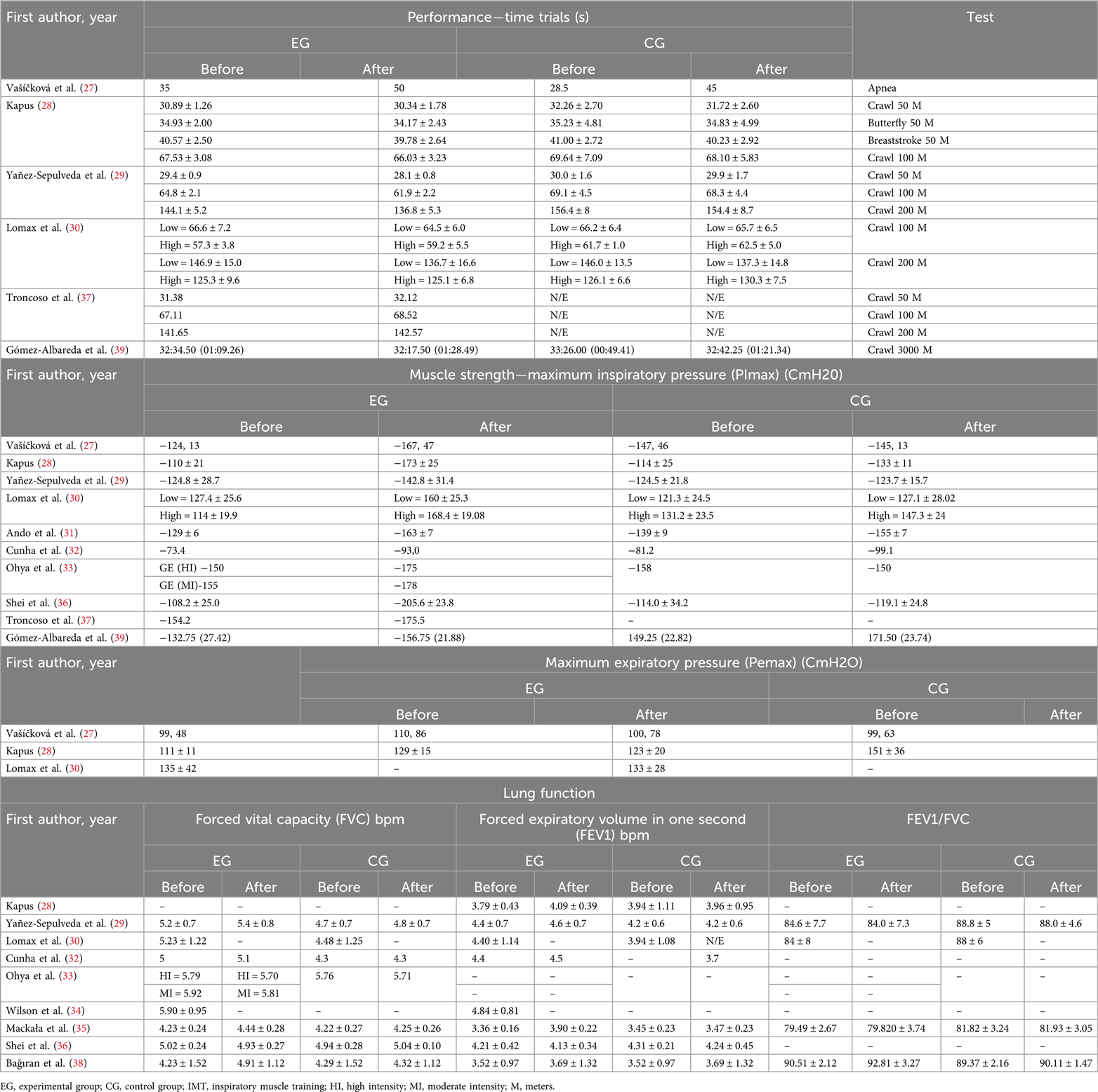
Table 4. Evaluation of the effect of IMT on performance, muscle strength and lung function in athlete swimmers.
3.4 Evaluation of the effect of respiratory muscle training on strength in swimming athletes
In the experimental group the baseline values of MIP ranged from −73.4 CmH2O (28) to −154.2 CmH2O (37), after IMT, the values ranged from −93.0 CmH2O (32) to −205.6 ± 23.80 CmH2O (37). For the control group were reported baseline values between −81.2 CmH2O (32) and −149.25 CmH2O (39), and post-IMT the range was between −99.1 CmH2O (29) and −171.5 CmH2O (39). Three studies did not report results on MIP (34, 35, 38).
Only three studies reported MEP values (27, 28, 30). In the IMT group, initial values were reported from 99.48 CmH2O (27) to 135 ± 42 CmH2O (30) and post-IMT 110.86 CmH2O (27) to 129 ± 15 CmH2O (28). One study did not report final values after training (30). While in the control group, basal values ranged from 100.78 CmH2O (27) to 133 ± 28 CmH2O (30) and subsequent values ranged from 99.63 CmH2O (27) to 151 ± 36 CmH2O (28). Ten articles (29, 31–39) did not report MEP results (Table 4).
3.5 Evaluation of respiratory muscle training on pulmonary function in swimming athletes
Table 4 shows the results of FVC, FEV1, and FEV1/FVC ratios. The FVC baseline in the IMT group had a range of 4.23 ± 0.24 L (35) to 5.92 L (33), and post-IMT a range of 4.44 ± 0.28 L (35) to 5.81 L (33). In the control group, the initial values ranged from 4.22 ± 0.27 L (35) to 4.94 ± 0.28 L (36) and later from 4.25 ± 0.26 L (35) to 5.04 ± 0.10 L (36). One study reported no subsequent values (30) and 6 studies reported no baseline or subsequent values (27, 28, 31, 34, 37, 39).
The FEV1 results for the IMT group showed baseline values ranging from 3.36 ± 0.16 L (35) to 4.84 ± 0.81 L (33). On the other hand, the control group had baseline values ranging from 3.45 ± 0.23 L (35) to 4.31 ± 0.21 L (36), and post-measurement values ranging from 3.47 ± 0.23 L (35) to 4.24 ± 0.45 L (36). Post-intentions values were not reported in two studies (30, 34) while five studies did not report either baseline or post-values (27, 31, 33, 37, 39).
The FEV1/FVC ratio in the IMT group had a baseline range of 79.49 ± 2.67 L (27) to 90.51 ± 2.12 L (38), and post-IMT values ranged from 79.820 ± 3.74 L (35) to 92.81 ± 3.27 L (38). Meanwhile, the control group had a baseline range of 81.82 ± 3.24 L (35) to 89.37 ± 2.16 L (38), and post-measurement values ranged from 81.93 ± 3.05 L (35) to 90.11 ± 1.47 L (38). However, it is worth noting that nine studies did not report these results (27, 28, 31, 32, 36, 37, 39).
3.6 Quality of the studies
The mean PEDro score for the CCTs described in Table 5 was High for two studies (27–32) and Intermediate for 9 studies (28–33, 35, 36, 38, 39). The Minor mean score for the PLS for these two studies was 13 and 17, respectively (Table 5), where the ideal score would be 16 for non-comparative studies. The most frequent omissions in the study design or its reporting were the following: the randomization process was not concealed and the non-blinding of subjects and evaluators.

Table 5. Methodological quality of the studies controlled clinical trials (PEDro score) and prospective longitudinal observational studies (minors scale).
3.7 Association of IMT with MIP, FEV1, and FVC
For the quantitative synthesis of MIP, we selected 9 articles (28–33, 35, 36, 38, 39) (IMT group n = 104 and control group n = 78). The results showed that IMT in swimmers increased the MIP 29.35 cmH2O (CI-95%: 13.04–45.65 cmH2O, p < 0.01), the heterogeneity of this result was high (I2 = 78%) (Figure 2A).
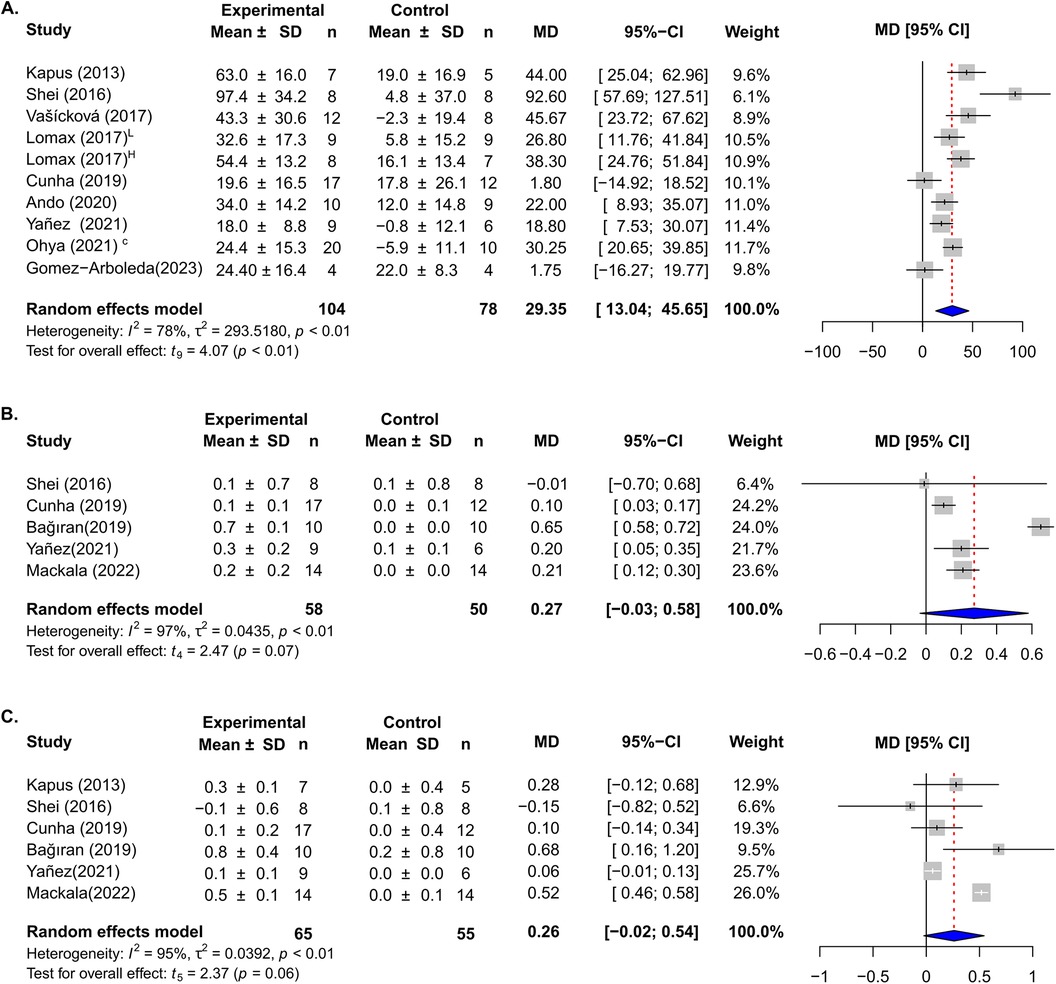
Figure 2. Forest plots of the effect of IMT on maximal inspiratory pressure (A); forced expiratory volume (B) and forced vital capacity (C). Horizontal lines indicate confidence intervals for each study. Horizontal diamonds of blue color show overall confidence intervals and the midline in red color indicates the mean difference (MD).
The effect of IMT on FEV1 was assessed in six studies (28, 29, 32, 35, 36, 38) (IMT group n = 65 and control group n = 55), the analysis showed that the intervention increased by 0.26 L, but did not reach to be significant and showed a substantial heterogeneity (CI-95%: −0.02 to 0.54, p = 0.06, I2 = 95%) (Figure 2B).
For FVC we pooled five studies (27, 29, 30, 37, 38) (IMT group = 58 and control group n = 50), and quantitative synthesis showed a not significant increase of 0.27 L (CI-95%: −0.03 to 0.58, p = 0.07) with high variation (I2 = 97%) (Figure 2C).
3.8 Sensitivity and meta-regression analysis
The meta-analysis showed a high heterogeneity (I2 > 75%) in all the outcomes studied. The sensitivity analysis suggests that the results for MIP are robust, and the removal of studies did not affect considerably the effect and the heterogeneity of the meta-analysis (Supplementary Material 1). In the case of FEV1, the omission of Mackala et al. (35) reduced the heterogeneity (I2 = 42%) but without a significant effect (MD = 0.08 L, CI-95%: −0.05 L to 0.20 L, p = 0.16) (Supplementary Material 1). The sensitivity analysis for FVC after removing the study of Bağiran et al. (38) showed a significant effect (MD = 0.15l, CI-95%: 0.05–0.25l, p = 0.02) and a substantial reduction of the heterogeneity (I2 = 31%) (Supplementary Material 1). We performed a subgroup analysis considering the type of control group; control group with IMT sham or control group with regular swimming training. We found that the pooled effect for MIP in studies with an IMT sham group was not significant (MD = 16.35, CI-95%: −14.32 to 47.02, I2 = 78%) (Supplementary Material 2), while for FEV we found a significant effect in the studies with a control group with regular swimming training (MD = 0.52, CI-95%: 0.33–0.71, I2 = 52%) (Supplementary Material 3).
Meta-regression analyses for potential factors related to the effect of IMT on MIP revealed no significant relationship with MIP basal (P = 0.88), age (P = 0.90), and duration of intervention (P = 0.76) (Supplementary Material 4).
3.9 Publication bias
The LFK index showed minor asymmetry for MIP (LFK = 1.26), no asymmetry for FEV (LFK = −0.92), and FVC (LFK = −0.93) (Supplementary Material 5), indicating no obvious publication bias.
4 Discussion
This systematic review and meta-analysis found that training with IMT in elite and non-elite swimmers significantly increased MIP, this effect was not related to age, duration of intervention, or basal MIP of the participants. We also found that IMT was not associated with changes in MEP, FEV1, and FVC.
Schoenfeld et al. (40), suggested that different training regimens can maximize performance or hypertrophy in athletes. Evidence shows that different exercise volumes, intensity, and timing, induce different degrees of hypertrophy and muscular strength (41). In our study, we found a significant increase in the MIP post-IMT, when training was carried out with intensity progression. This finding is similar to those reported by Kilding et al. (8) (a study not included in the meta-analysis because its publication date was outside the inclusion criteria) who evaluated the effect of IMT on the performance in the 100 and 200-m free events and found an increase in both the performance and the strength of the inspiratory muscles in swimmers. Respiratory muscle training is linked to enhanced endurance performance in intermittent incremental tests, constant load tests, and time trials. It also boosts respiratory muscle endurance and strength, decreases the perceived exertion or breathlessness, and lessens respiratory fatigue during exercise in hypoxic conditions (42).
The increase in respiratory muscle strength can improve the ventilatory function of the rib cage, allowing for greater and faster thoracic excursion. It is well known that there is greater lung ventilation to higher the thoracic excursion. The thoracic wall excursion is determined by several factors, such as compliance of soft tissue structures surrounding the thorax, chest form, and respiratory muscle strength (43). The most important component of the increase in lung volume is the rise in the chest cavity's rostral-caudal diameter and the anterior-posterior and transverse diameter, as a result of the action of the diaphragm and the external and internal intercostal muscles respectively (5). The increase in lung volume has two direct effects on the alveolar-capillary membrane: it increases the area and decreases the thickness of the alveolar-capillary membrane, both processes favoring gas diffusion capacity. Stronger inspiratory muscles, reflected by increased MIP, can influence the athlete's performance associated with increased gas exchange and tissue oxygen bioavailability (44).
Although the increase in the strength of the respiratory muscles is associated with an increase in lung volumes and capacities (45), this was not reflected in our study. We did not find an increase in pulmonary function assessed by FVC and FEV1 after IMT. The fact that training mainly affects the respiratory musculature and not the resistance and distensibility of the air conduction zones of the lung could explain the no effect on the FVC and FEV, despite exerting more power and having a higher thoracic excursion (46). However, other studies in other sports disciplines have shown significant differences in lung volumes and capacities after IMT. Vasconcelos et al. (47), on basketball athletes, using a Threshold IMT® device, 5 times a week, for 4 weeks, 30 repetitions at 50% of the MIP, reported a significant change in FEV1, FVC, and peak expiratory flow. Koç et al. (48), in taekwondo athletes, showed significant changes in FVC, slow FVC, and maximal voluntary ventilation. On the other hand, during the research process of the systematic review, other forms of IMT were found, such as the use of a Respiratory Dead Space Addition Device (ARDS®). Szczepan et al. (49) used ARDS in recreational swimmers, for 6 weeks, twice a week, for 50 min in freestyle, however, the study reports no differences in muscle strength or spirometric parameters, and only one of the groups showed an increase in peak tidal volume.
We found that the protocols of IMT in swimmers included durations between 3 and 12 weeks, 1–2 sessions per day, 3–6 times per week, and 10–30 dynamic respiratory efforts, starting with 50% of MIP with progression up to 80% and the most common IMT device used was the Power Breathe®. This protocol is similar to reported in other studies as the Kilding et al. (8), in which the group of swimmers performed training for 6 weeks, 2 times a day, using Power Breathe®, however, the progression of MIP was not described. De Asís-Fernández et al. (50), applied IMT in divers, 3 times a week for 4 weeks, once a day, with a PowerBreathe® device. We found that protocols of IMT sessions ranged from 10 to 30 dynamic inspiratory efforts, with an initial pressure threshold load in most studies at 50% of MIP, and a progression of intensity between 70% and 80%. Studies in other sports show similar patterns in starting intensity and progression. Cavalcante-Silva et al. (51) on soccer players used a protocol of 15–30 dynamic respiratory efforts, starting at 50% of the MIP, although the progression was not specified. In runners, Rozek-Piechura et al. (52) used a protocol of 30 repetitions, starting with 50% of the MIP and progressing to 60% of the MIP between weeks 4 and 6 and, reaching 70% in weeks 7 and 8. The above suggests that the IMT protocols in elite, and non-elite swimmers are very similar to those used in athletes’ aquatic and land sports.
Our study had limitations such as not all included studies measured simultaneously performance, strength and pulmonary function tests. In addition, some studies did not perform measurements before and after the IMT intervention, which made comparative analysis challenging. A second difficulty was the classification of elite and non-elite athletes, due to different ways of reporting details about the athlete's condition. Besides. some studies could not be included because used IMT devices other than Threshold IMT®, or PowerBreathe®, such as normocapnic hyperpnea or ARDS®, or because were performed in swimmers with some disabilities (53).
The results of this meta-analysis can be valuable to designing training protocols for the respiratory muscles with IMT, especially in swimming to improve respiratory function in athletes. However, further studies are required to evaluate the effects of different IMT modalities, lung volumes, muscle strength, and their impact on technique and athletic performance.
5 Conclusions
Incorporating IMT in the training of elite and non-elite swimmers contributes to improvements in muscle strength, particularly MIP. This effect can be achieved by practicing IMT for 3–12 weeks, with 1–2 daily sessions, 3–6 times per week, performing 30 repetitions, and starting at 50% of MIP and gradually progressing up to 80% of MIP.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
MC-T: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. JO: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AC-L: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MD-Q: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. IG-C: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. DR-H: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AS-O: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research has been funded by Dirección General de Investigaciones of the Universidad Santiago de Cali under call No. 01-2024.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fspor.2024.1429902/full#supplementary-material
References
1. Lavin KM, Guenette JA, Smoliga JM, Zavorsky GS. Controlled-frequency breath swimming improves swimming performance and running economy. Scand J Med Sci Sports. (2015) 25(1):16–24. doi: 10.1111/sms.12140
2. Shei RJ. Respiratory muscle training and aquatic sports performance. J Sports Sci Med. (2018) 17(1):161–62. Available online at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5844203/29535590
3. Illidi CR, Stang J, Melau J, Hisdal J, Stensrud T. Does cold-water endurance swimming affect pulmonary function in healthy adults? Sports (Basel). (2021) 9(1):7. doi: 10.3390/sports9010007
4. Yilmaz ÖF, Özdal M. Acute, chronic, and combined pulmonary responses to swimming in competitive swimmers. Respir Physiol Neurobiol. (2019) 259:129–35. doi: 10.1016/j.resp.2018.09.002
5. Aliverti A. The respiratory muscles during exercise. Breathe (Sheff). (2016) 12(2):165–8. doi: 10.1183/20734735.008116
6. Stickland MK, Lindinger MI, Olfert IM, Heigenhauser GJ, Hopkins SR. Pulmonary gas exchange and acid-base balance during exercise. Compr Physiol. (2013) 3(2):693–739. doi: 10.1002/cphy.c110048
7. Lemaitre F, Coquart JB, Chavallard F, Castres I, Mucci P, Costalat G, et al. Effect of additional respiratory muscle endurance training in young well-trained swimmers. J Sports Sci Med. (2013) 12(4):630–8.24421721
8. Kilding AE, Brown S, McConnell AK. Inspiratory muscle training improves 100 and 200 m swimming performance. Eur J Appl Physiol. (2010) 108(3):505–11. doi: 10.1007/s00421-009-1228-x
9. Päivinen M, Keskinen K, Tikkanen H. Swimming-induced changes in pulmonary function: special observations for clinical testing. BMC Sports Sci Med Rehabil. (2021) 13(1):55. doi: 10.1186/s13102-021-00277-1
10. Hellyer NJ, Andreas NM, Bernstetter AS, Cieslak KR, Donahue GF, Steiner EA, et al. Comparison of diaphragm thickness measurements among postures via ultrasound imaging. PM R. (2017) 9(1):21–5. doi: 10.1016/j.pmrj.2016.06.001
11. Yoshida N, Ota H, Higuchi S, Sekiguchi Y, Kakihana T, Sato H, et al. Gliding performance is affected by cranial movement of abdominal organs. Sci Rep. (2020) 10(1):21430. doi: 10.1038/s41598-020-78609-3
12. Rehder-Santos P, Minatel V, Milan-Mattos JC, Signini ÉDF, de Abreu RM, Dato CC, et al. Critical inspiratory pressure—a new methodology for evaluating and training the inspiratory musculature for recreational cyclists: study protocol for a randomized controlled trial. Trials. (2019) 20(1):258. doi: 10.1186/s13063-019-3353-0
13. Hackett DA. Lung function and respiratory muscle adaptations of endurance- and strength-trained males. Sports. (2020) 8(12):160. doi: 10.3390/sports8120160
14. John LH, Bill E, Mary T, Janet S, Philip HQ. Use of forced vital capacity and forced expiratory volume in 1 s quality criteria for determining a valid test. Eur Respir J. (2015) 45(5):1283. doi: 10.1183/09031936.00116814
15. Moon SM, Lim JH, Hong YS, Shin KC, Lee CY, Kim DJ, et al. Clinical impact of forced vital capacity on exercise performance in patients with chronic obstructive pulmonary disease. J Thorac Dis. (2021) 13(2):837–46. doi: 10.21037/jtd-20-1098a
16. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Br Med J. (2021) 372:n71. doi: 10.1136/bmj.n71
17. Moseley AM, Elkins MR, Van der Wees PJ, Pinheiro MB. Using research to guide practice: the physiotherapy evidence database (PEDro). Braz J Phys Ther. (2020) 24(5):384–91. doi: 10.1016/j.bjpt.2019.11.002
18. Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg. (2003) 73(9):712–6. doi: 10.1046/j.1445-2197.2003.02748.x
19. Jelicic KA, Vucic K, Dosenovic S, Sapunar D, Puljak L. Extracting data from figures with software was faster, with higher interrater reliability than manual extraction. J Clin Epidemiol. (2016) 74:119–23. doi: 10.1016/j.jclinepi.2016.01.002
20. Follmann D, Elliott P, Suh I, Cutler J. Variance imputation for overviews of clinical trials with continuous response. J Clin Epidemiol. (1992) 45:769–73. doi: 10.1016/0895-4356(92)90054-q
21. Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane handbook for systematic reviews of interventions. Chichester: John Wiley & Sons (2019).
22. Hartung J, Knapp G. On tests of the overall treatment effect in meta-analysis with normally distributed responses. Stat Med. (2001) 20:1771–82. doi: 10.1002/sim.791
23. IntHout J, Ioannidis JPA, Borm GF. The Hartung-Knapp-Sidik-Jonkman method for random effects meta-analysis is straightforward and considerably outperforms the standard DerSimonian-Laird method. BMC Med Res Methodol. (2014) 14(25). doi: 10.1186/1471-2288-14-25
24. Furuya-Kanamori L, Barendregt JJ, Doi SAR. A new improved graphical and quantitative method for detecting bias in meta-analysis. Int J Evid Based Healthc. (2018) 16:195–203. doi: 10.1097/XEB.0000000000000141
25. Team RC. A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing. Available online at: https://www.r-project.org/ (Accessed February 15, 2023).
26. Balduzzi S, Rücker G, Schwarzer G. How to perform a meta-analysis with R: a practical tutorial. Evid Based Ment Health. (2019) 22:153–60. doi: 10.1136/ebmental-2019-300117
27. Vašíčková J, Neumannová K, Svozil Z. The effect of respiratory muscle training on fin-swimmers’ performance. J Sports Sci Med. (2017) 16(4):521–6.
28. Kapus J. Effects of inspiratory muscle training on inspiratory muscle strength and sprint swimming performance in young female and male swimmers. Kinesiol Slov. (2013) 19(1):53–61.
29. Yañez-Sepulveda R, Alvear-Ordenes I, Tapia-Guajardo A, Verdugo-Marchese H, Cristi-Montero C, Tuesta M. Inspiratory muscle training improves the swimming performance of competitive young male sprint swimmers. J Sports Med Phys Fitness. (2021) 61(10):1348–53. doi: 10.23736/S0022-4707.21.11769-4
30. Lomax M, Kapus J, Brown PI, Faghy M. Impact of weekly swimming training distance on the ergogenicity of inspiratory muscle training in well-trained youth swimmers. J Strength Cond Res. (2019) 33(8):2185–93. doi: 10.1519/JSC.0000000000002375
31. Ando R, Ohya T, Kusanagi K, Koizumi J, Ohnuma H, Katayama K, et al. Effect of inspiratory resistive training on diaphragm shear modulus and accessory inspiratory muscle activation. Appl Physiol Nutr Metab. (2020) 45(8):851–6. doi: 10.1139/apnm-2019-0906
32. Cunha M, Mendes F, Paciência I, Rodolfo A, Carneiro-Leão L, Rama T, et al. The effect of inspiratory muscle training on swimming performance, inspiratory muscle strength, lung function, and perceived breathlessness in elite swimmers: a randomized controlled trial. Porto Biomed J. (2019) 4(6):e49. doi: 10.1097/j.pbj.0000000000000049
33. Ohya T, Kusanagi K, Koisumi J, Ando R, Katayama K, Suzuki Y. Effect of moderate- or high-intensity inspiratory muscle strength training on maximal inspiratory. Hum Kinet J. (2021) 17(3):343–9. doi: 10.1123/ijspp.2021-0119
34. Wilson EE, McKeever TM, Lobb C, Sherriff T, Gupta L, Hearson G, et al. Respiratory muscle-specific warm-up and elite swimming performance. Br J Sports Med. (2014) 48(9):789–91. doi: 10.1136/bjsports-2013-092523
35. Mackała K, Kurzaj M, Okrzymowska P, Stodółka J, Coh M, Rożek-Piechura K. The effect of respiratory muscle training on the pulmonary function, lung ventilation, and endurance performance of young soccer players. Int J Environ Res Public Health. (2020) 17(1):234. doi: 10.3390/ijerph17010234
36. Shei RJ, Lindley M, Chatham K, Mickleborough TD. Effect of flow-resistive inspiratory loading on pulmonary and respiratory muscle function in sub-elite swimmers. J Sports Med Phys Fitness. (2016) 56(4):392–8.25503711
37. Troncoso G, Rojas G, González R, Vicuña M. Efecto del entrenamiento muscular inspiratorio sobre El Tiempo de nado y función pulmonar en jóvenes nadadores de alto rendimiento. RevChiREAF. (2021) 1(1):1–12. doi: 10.32457/reaf1.1731
38. Bağıran Y, Dağlıoğlu Ö, Bostancı Ö. The effect of respiratory muscle training on aerobic power and respiratory parameters in swimmers. Int J Sport Exer Train Sci. (2019) 5(4):214–20. doi: 10.18826/useeabd.647449
39. Gómez-Albareda E, Viscor G, García I. Inspiratory muscle training improves maximal inspiratory pressure without increasing performance in elite swimmers. Int J Sports Physiol Perform. (2023) 18(3):320–5. doi: 10.1123/ijspp.2022-0238
40. Schoenfeld BJ, Contreras B, Krieger J, Grgic J, Delcastillo K, Belliard R, et al. Resistance training volume enhances muscle hypertrophy but not strength in trained men. Med Sci Sports Exerc. (2019) 51(1):94–103. doi: 10.1249/MSS.0000000000001764
41. Reggiani C, Schiaffino S. Muscle hypertrophy and muscle strength: dependent or independent variables? A provocative review. Eur J Transl Myol. (2020) 30(3):9311. doi: 10.4081/ejtm.2020.9311
42. Kowalski T, Granda D, Klusiewicz A. Practical application of respiratory muscle training in endurance sports. Strength Cond J. (2024). doi: 10.1519/SSC.0000000000000842
43. Padkao T, Boonla O. Relationships between respiratory muscle strength, chest wall expansion, and functional capacity in healthy nonsmokers. J Exerc Rehabil. (2020) 16(2):189–96. doi: 10.12965/jer.2040080.040
44. Matuszak J, Tabuchi A, Kuebler WM. Ventilation and perfusion at the alveolar level: insights from lung intravital microscopy. Front Physiol. (2020) 11:291. doi: 10.3389/fphys.2020.00291
45. Shadmehri S, Kazemi N, Heydari FZ. Comparison of effect of high-intensity interval training and aerobic training on respiratory volumes in female students. Tanaffos. (2021) 20(4):337–44.36267926
46. Stanojevic S, Kaminsky DA, Miller MR, Thompson B, Aliverti A, Barjaktarevic I, et al. ERS/ATS technical standard on interpretive strategies for routine lung function tests. Eur Respir J. (2022) 60(1):2101499. doi: 10.1183/13993003.01499-2021
47. Vasconcelos T, Hall A, Viana R. The influence of inspiratory muscle training on lung function in female basketball players—a randomized controlled trial. Porto Biomed J. (2017) 2(3):86–9. doi: 10.1016/j.pbj.2016.12.003
48. Koç M, Saritaş N. The effect of respiratory muscle training on aerobic and anaerobic strength in adolescent taekwondo athletes. J Educ Train Stud. (2019) 7(2):103–10. doi: 10.11114/jets.v7i2.3764
49. Szczepan S, Danek N, Michalik K, Wróblewska Z, Zatoń K. Influence of a six-week swimming training with added respiratory dead space on respiratory muscle strength and pulmonary function in recreational swimmers. Int J Environ Res Public Health. (2020) 17(16):5743. doi: 10.3390/ijerph17165743
50. de Asís-Fernández F, Del Corral T, López-de-Uralde-Villanueva I. Effects of inspiratory muscle training versus high-intensity interval training on the recovery capacity after a maximal dynamic apnoea in breath-hold divers. A randomised crossover trial. Diving Hyperb Med. (2020) 50(4):318–24. doi: 10.28920/dhm50.4.318-324
51. Silva RLC, Hall E, Maior AS. Inspiratory muscle training improves performance of a repeated sprints ability test in professional soccer players. J Bodyw Mov Ther. (2019) 23(3):452–5. doi: 10.1016/j.jbmt.2019.01.016
52. Rożek-Piechura K, Kurzaj M, Okrzymowska P, Kucharski W, Stodółka J, Maćkała K. Influence of inspiratory muscle training of various intensities on the physical performance of long-distance runners. J Hum Kinet. (2020) 75(1):127–37. doi: 10.2478/hukin-2020-0031
Keywords: athletes, swimming, muscle strength, respiratory muscles, sports performance
Citation: Carvajal-Tello N, Ortega JG, Caballero-Lozada AF, Devia-Quiñonez MJ, González-Calzada I, Rojas-Hernández D and Segura-Ordoñez A (2024) Effects of inspiratory muscle training on lung function parameter in swimmers: a systematic review and meta-analysis. Front. Sports Act. Living 6:1429902. doi: 10.3389/fspor.2024.1429902
Received: 8 May 2024; Accepted: 26 August 2024;
Published: 16 September 2024.
Edited by:
Susanna Rampichini, Università degli studi di Milano, ItalyReviewed by:
Luca Cavaggioni, Italian Auxological Institute (IRCCS), ItalyGonzalo Márquez, University of A Coruña, Spain
Copyright: © 2024 Carvajal-Tello, Ortega, Caballero-Lozada, Devia-Quiñonez, González-Calzada, Rojas-Hernández and Segura-Ordoñez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrés Fabricio Caballero-Lozada, YW5kcmVzLmNhYmFsbGVyb0Bjb3JyZW91bml2YWxsZS5lZHUuY28=
†These authors have contributed equally to this work