 Otaviano Oliveira-Júnior1,2,†
Otaviano Oliveira-Júnior1,2,† Tim J. Gabbett3,4,†
Tim J. Gabbett3,4,† Natalia F. N. Bittencourt5,†Roberto C. Quintão2,†Guilherme F. Reis2,†
Natalia F. N. Bittencourt5,†Roberto C. Quintão2,†Guilherme F. Reis2,† João G. Claudino6,†
João G. Claudino6,† Rodrigo C. P. Lasmar2,†
Rodrigo C. P. Lasmar2,† Amanda A. O. Leopoldino1*†
Amanda A. O. Leopoldino1*†
- 1Post Graduate Program in Health Sciences, Faculdade Ciências Médicas de Minas Gerais, Belo Horizonte, Brazil
- 2Medical Department of Professional Soccer, Clube Atlético Mineiro, Belo Horizonte, Brazil
- 3Gabbett Performance Solutions, Brisbane, QLD, Australia
- 4Health Innovation and Transformation Centre, Federation University, Ballarat, VIC, Australia
- 5Soccer Science Center, Federal University of Minas Gerais (UFMG), Belo Horizonte, Minas Gerais, Brazil
- 6Sports Science, School of Applied Sciences (FCA), University of Campinas (Unicamp), Limeira, São Paulo, Brazil
Purpose: The aim of this pilot study was to analyze the potential financial loss and a range of potential risk factors for hamstring muscle injuries in elite Brazilian soccer.
Methods: Thirty-four male players (age: 25 ± 6 years; stature: 180 ± 8 cm; body mass: 78 ± 9 kg; minutes played in matches: 2243 ± 1423 min) from an elite professional soccer club were monitored during a 12-month season. Muscle injury was identified by magnetic resonance imaging and the severity was defined according to the number of days away: minimal (1–3 days), mild (4–7 days), moderate (8–28 days), severe (>28 days). Potential financial loss due to the team's under achievements was determined. Dorsiflexion range of motion, eccentric knee flexor strength and isokinetic tests were performed during the pre-season. Association between dependent variables and the occurrence of injury was evaluated.
Results: Nine hamstring muscle injuries with moderate severity were found in 8 athletes. Recovery time was 22 days off the field on average. Potential financial loss was $-43.2 million USD and earnings on merit money was 21%. Previous injury, increased flexor deficit 60° /sec and increased flexor fatigue index 300°/sec were all associated with a greater chance of hamstring muscle injury. Ankle dorsiflexion range of motion was significantly lower in the injured group (35.6 ± 3° vs. 39.1 ± 4.9°; p = 0.017, effect size = −0.74).
Conclusion: High financial burden was found in elite Brazilian soccer during one full season. Injured athletes had high hamstring fatigue index, knee flexor strength deficit, ankle range of motion restriction and previous hamstring muscle injury when compared to non-injured athletes. Therefore, preventive approaches in professional soccer players with previous hamstring injuries should be a priority.
1 Introduction
Soccer played in the strongest national leagues in the world (1) requires increasingly high levels of physical fitness and intensive training of the athletes (2–4). Specifically, muscle strength is essential in sports with high physical demands, such as soccer (5, 6). Soccer is characterized by sequences of high-intensity actions: running, jumping, and explosive technical skills that require acceleration and deceleration (7, 8). In this context, well-developed physical qualities, such as joint mobility, muscle strength and flexibility, and the ability to perform high-speed running are essential in preparing high-performance teams (5, 9–11). Due to the intense match demands, training loads of elite soccer players are also high (12, 13), explaining around 76% of the common variance between matches and training sessions (14), which may explain, at least in part, the high incidence of muscle injuries. Ekstrand et al. (2) investigated players from the UEFA Elite Club for 21 seasons between 2001/02 and 2021/22 and observed that hamstring injuries represented 19% of all reported injuries, with the proportion of all injuries increasing from 12% during the first season to 24% in the last season. Hamstring injuries are also reported to be one of the injuries most likely to negatively impact team performance in the UEFA Champions League or Europa League (15).
Although it is frequently reported on social networks and sports channels, in the scientific literature the few studies found report that the costs involved in hamstring muscle injuries are very high (16) and the negative impacts of injuries related to team performance are responsible for most of the financial loss for soccer clubs (17). For example, an English Premier League team lost approximately ₤45 million per season due to injury–related decrements in performance (i.e., 80% <=> the team's under achievement due to injured athletes + 20% <=> salaries paid to injured athletes) (17). Due to the negative impact of hamstring muscle injuries on costs and loss of finances, different strategies have been used in order to prevent these injuries. Amateur soccer players who used the FIFA 11 Program for injury prevention incurred fewer hamstring muscle injuries and fewer severe injuries, reducing the mean cost of hamstring muscle injuries for players who performed the program (18). Researchers have also analyzed modifiable and non-modifiable risk factors1 for hamstring muscle injuries (19–33).
Regarding non-modifiable risk factors, athletes with a history of hamstring muscle injury had a three times greater risk of suffering a new injury in the same muscle group (25). Additionally, the risk increased fivefold when this injury occurred in the same season (25). The literature also describes the relationship of previous anterior cruciate ligament (ACL) injuries with hamstring muscle injuries (25). It is thought that a reduction in knee neuromuscular control may contribute to hamstring injuries post ACL rupture, and that these changes may persist for up to three years following ligament reconstruction, especially with the use of the hamstring surgical graft (19, 28).
Although there are considerably more modifiable risk factors that may influence hamstring injury risk, there is conflicting findings in the scientific literature (25, 33). Variables related to hamstring muscle strength have traditionally been measured using isokinetic dynamometer equipment (23, 29, 32, 33) and eccentrically using the NordBord Hamstring Testing® (and similar) devices (21, 22, 27, 31). Despite fatigue being described as one of the predisposing factors for muscle injuries (26), there are limited investigations within the literature (20). The range of motion of the ankle and knee have been investigated as risk factors for hamstring muscle injuries, although older age and a history of hamstring muscle injury are the strongest risk factors (25). Passive hamstring and ankle dorsiflexion ranges of motion have been described as weak risk factors for hamstring injury (33). Nevertheless, decreased ankle mobility may predispose the hamstring muscles to a greater risk of strain injury, presumably due to an alteration in the biomechanical position of the foot (34), leading to a reduction in horizontal strength during sprinting (35), generating an increase in hamstring work (33). In addition to the physical characteristics of athletes, the increased high-speed running demand may also increase injury risk, although exposure to these higher loads is necessary to develop the physical qualities to protect against injury and produce better physical and technical performance (36–41). In a recent study of elite soccer players, players who completed moderate volumes of high-speed running (701–750 m: OR: 0.12, 90%CI: 0.08–0.94) and sprint running (201–350 m: OR: 0.54, 90%CI: 0.41–0.85) were at reduced injury risk compared to those who completed low volumes of high-speed running (≤674 m) and sprinting (≤165 m) (10).
In summary, there is conflicting evidence regarding the risk factors for hamstring muscle injuries, and there is a high incidence of hamstring injuries and associated financial burden, particularly in soccer players from the strongest national leagues in the World. Therefore, this season-long prospective cohort pilot study aimed to verify the risk factors for hamstring muscle injuries assessed via isokinetic testing, weight bearing lunge testing, eccentric hamstring strength and external workload monitoring and potential financial loss in elite Brazilian soccer.
2 Methods
2.1 Study design and ethical aspects
This study used a prospective cohort experimental design. We studied a professional soccer team in the first division of the Brazilian Championship. This study was approved by the Research Ethics Committee of the Faculdade Ciências Médicas de Minas Gerais (CAAE: 15737819.6.0000.5134), according to the rules of Resolution 196/96 of the National Health Council regarding research involving human beings. All athletes manually signed the informed consent form. Consent to use the medical records was obtained by signing the club's Letter of Consent.
2.2 Sample
The study was carried out in an elite Brazilian soccer club. Sample size was calculated in order to estimate hamstring muscle injury prevalence in soccer players. The equation used is described below (42):
with p as prevalence estimated from Ekstrand et al. (3), and as percentiles of the standard normal distribution associated with the significance and power of the test, respectively, and d as minimum difference to be tested. Thus, considering the significance level of 5%, minimum power of 80% to test a minimum difference of 25% in relation to the prevalence of injury of 37% (3), at least 30 athletes were needed in the sample. Four more athletes were included to cover possible sample losses (42). All athletes on the squad were recruited and remained throughout the process, except for 5 athletes who left the club during the season. They were male, aged between 18 and 39 years, and participated in official games for 12 consecutive months in the 2019 season. Goalkeepers were excluded because of their unique physical demands relative to field players, and consequently, did not have the same risk of exposure to hamstring injuries. Athletes who left the club for any reason and were unable to undergo testing were excluded.
2.3 Procedures
Data were collected for 12 months in the 2019 season by checking medical records (season start) and applying a questionnaire to athletes containing physical parameters and past medical history. Aspects of the athlete's profile such as: age, body mass index, position, previous injuries in the last two years (muscle—hamstring muscle injury, ankle inversion sprain) and in the last three years (ACL injury in the knee) (19, 25), distance covered at high-intensity running speed monitored by GPS, congested game schedule that may be related to the physical quality and the efficient execution of game actions were verified. After collecting the sociodemographic and clinical data, a complete assessment of the lower limbs was performed to characterize their functional profile. The British classification was used to assess injury severity based on clinical examination and magnetic resonance imaging (43).
Hamstring muscle injury was defined as the micro or macro rupture of fibers of the tendon muscle complex of the biceps femoris, semitendinosus and semimembranosus, either by an eccentric mechanism during running or by excessive stretching of the thigh, including both the first episode and any recurrences which limited the athlete to participate in training or games (4). In addition, the Fédération Internationale de Football Association (FIFA) criteria were used to assess the severity of injuries according to the number of days of absence: minimal (1–3 days), mild (4–7 days), moderate (8–28 days), severe (>28 days) (44). Based on the Croisier (23), recurrent hamstring injury was identified when more than one occurrence during the season.
Potential financial loss due to the team's under achievements was determined by summing the merit money deficit and salaries paid to injured athletes. The merit money is based solely on each club's final position in the competition (17). Thus, the merit money deficit is the difference of the team position and the champion team in United States Dollar (USD). Merit money paid in Brazilian Real (BRL) was converted in USD using the yearly average exchange rate, i.e., USD 1 = BRL 3.946 (45). There were 4 competitions (i.e., Brazilian Championship Serie A, Brazil Cup, CONMEBOL Libertadores, CONEMBOL Sudamericana) that paid merit money for this club in the season and all these values are in the public domain. Due to the institution's confidentiality agreements, salaries paid to injured athletes were taken from the soccer club's financial statements which is also a public file. For the calculation, the total amount of salaries paid to athletes with image rights was used. First, the salary paid per athlete per day (i.e., salary paid/athlete/day) was calculated, and then this salary paid daily was multiplied by the total of off-field days (i.e., recovery time).
2.4 Instruments and variables
2.4.1 Isokinetic evaluation
The isokinetic strength assessment was performed using a Biodex System Pro 4® isokinetic dynamometer (Biodex, NY, USA). First, a brief familiarization and ten-minute warm-up was performed on an ergometric bicycle (46). According to the protocol, testing was performed for each knee with an angular velocity of 60° /s and 300° /s with concentric knee flexion and extension movement under intense verbal command from the examiner, with an interval of 90 s between each test. Five and 30 repetitions were used, respectively, for each velocity. Flexor and extensor peak torque, flexor fatigue index (i.e., measured by the equipment protocol that considers the fatigue index as the percentage of strength loss between the first and the last third of the 30 repetitions performed at a speed of 300° /s), and hamstring/quadriceps ratio variables were used [(47); intraclass correlation coefficient = 0.87 by (48)]. The interval time between legs was around 15 min.
2.4.2 Weight bearing lunge test (WBLT)
The Weight Bearing Lunge Test (WBLT) was performed to assess ankle dorsiflexion limitation. The WBLT is a validated test with good reliability (49, 50). The test was performed with the athlete in an orthostatic position. In this position, participants performed an anterior advancement movement of the unilateral tibia over the talus in maximum dorsiflexion until the detachment moment of the calcaneus from the ground (Figure 1A). The tibia angulation was measured with an inclinometer using the AM-2 model from Starrett. The averages of the 3 measurements for each ankle dorsiflexion range of motion were used in further analyses.

Figure 1. (A) placement of the lunge test. Source: Author's personal archive. (B) NordBord Hamstring Testing® placement. Source: Author's personal archive. *The black boxes were necessary to make this image unidentifiable.
2.4.3 Nordbord hamstring testing
The hamstring eccentric muscle strength test was performed using the NordBord Hamstring Testing® device which has previously been validated, with normative data for biceps femoris injury (27). To perform the test, the participants remained in a kneeling position on a padded plate with their ankles secured to the lateral malleolus by individual “shin guards”, which were fixed on commercially available uniaxial load cells (MLP-1K; Transducer Techniques, Inc., Temecula, CA). They were asked to perform one set of three maximal “Nordic exercises with hamstrings” bilaterally (Figure 1B) to obtain the following variables: relative peak forcehighest (highest/body mass), between-limb imbalance (highest), relative peak forceaverage (average/body mass), between-limb imbalance (average) (22).
2.4.4 External workload monitoring
Global positioning system (GPS) devices (model SPI HPU; Gpsports Systems, Australia) were used to collect external load in training and games. The system uses data interpolation from 5 Hz GPS units and 100 Hz accelerometers to provide displacement and velocity data at 15 Hz. Each player wore a device (with a weight of 76 g and dimensions of 48 × 20 × 87 mm), placed in the thoracic region. The device was turned on 15 min before the activity and turned off immediately after the session. Data were recorded and transferred to a computer, then analyzed in the equipment's software program (Team AMS R1 2016).
External workload comparison of athletes with and without hamstring muscle injury was performed using data from 28 days before the athlete's injury (51). In addition, comparisons were made with another athlete from the same position and similar physical demands, who had not sustained injury. We used the variable absolute high-speed running (HSR) distance covered above 19.8 km/h for each athlete in different time frames to analyze the difference in acute and chronic load between the groups with and without injury. The four weeks of training and game data before the injuries were sustained were compared with athletes of the same position and similar demand. We used 3 different acute and chronic loading windows: the first-time window was 7/28 days, as it is the most commonly used period in the literature (51). The time frames of 4/16 days and 1/4 days were performed to capture the training demand closest to the injury. In these analyses, all participation time from training sessions and matches (regardless of the time played) were included. Counts were performed during the 4, 16, and 28 day periods before the day the injury occurred. Absolute HSR load performed in these periods were used in the analyses.
2.5 Statistical analysis
Qualitative variables were presented as frequencies, and quantitative variables as mean ± standard deviation (median). Quantitative variables were submitted to the Shapiro–Wilk normality test and if necessary, the corresponding non-parametric test was applied.
The association between the variables and injury occurrence was evaluated by a simple binary logistic model, and the results presented as an odds ratio (OR) and respective 95% confidence intervals (CI). Variables with p < 0.20 in the association analysis were included in a multiple binary logistic model, which reached the final model using the backward strategy. The significant variables and age independent of significance remained to control effects. Quality of fit analysis was performed using the Hosmer–Lemes how test. Edges's g was used to analyze the effect size (52) and the following classifications were used to measure the magnitude of ES: ES (Large effect >0.80; moderate effect 0.20–0.80; small effect <0.20) (53). The analysis was performed using the R version 4.0.2 program and p < 0.05 was considered significant.
3 Results
The sample consisted of 34 soccer players, of which 8 (24%) sustained 9 hamstring muscle injuries. The distribution of the injury by position was: attackers = 4 (44.4%), midfield = 3 (33.3%), full-back = 1 (11.1%) and defender = 1 (11.1%). This single recurrence of the hamstring injury took 47 days to recover (i.e., severe). A total of 202 off-field days were needed for recovery time and an average of 22 days (with median of 18 days) to recovery per hamstring muscle injury. Thus, the hamstring injuries were classified as moderate severity. The average age of the athletes was 25 ± 6 years and the average Body Mass Index (BMI) was 24.07 ± 1.10 kg/m2. Thirteen players were attackers (38.2%), nine were midfield (26.5%), six were full-backs (17.6%) and six were defenders (17.6%). Previous hamstring injury (observed in 19 limbs, 27.9%), previous ACL surgery (observed in 6 limbs, 8.8%) and ankle sprain (observed in 22 limbs, 32.4%) were associated with a greater risk of hamstring injuries. Higher BMI was associated with a reduced injury risk (OR 0.14, 95% CI 0.02; 0.50, p = 0.014) and previous hamstring muscle injury was associated with an increased injury risk (OR 7.08, 95% CI 1.64; 37.36, p = 0.011) (Table 1).
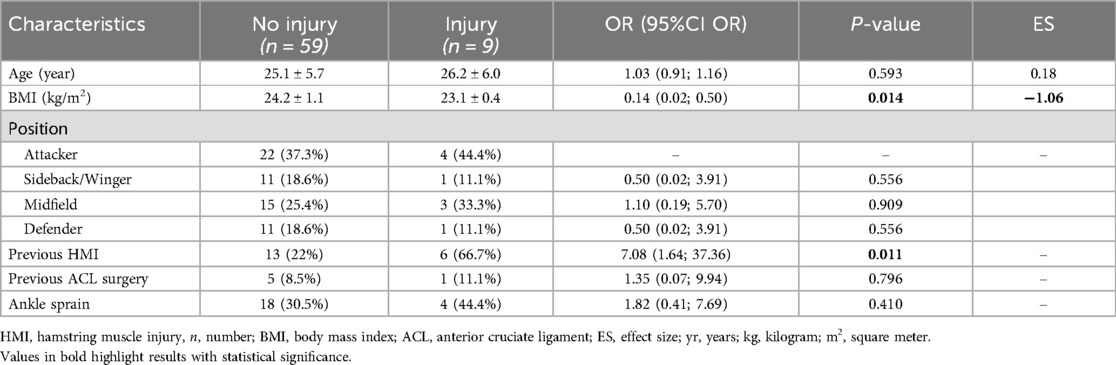
Table 1. Characterization of lower limbs according to the occurrence of hamstring injury.
In the evaluation of the balance/strength variables (Table 2), higher knee-flexor fatigue index at 300°/sec was associated with an increased risk of injury (OR 1.15, 95% CI 1.04; 1.31, p = 0.013), while increased dorsiflexion range of motion decreased the risk of injury (OR 0.80, 95% CI 0.62; 0.97, p = 0.040). There was no difference in external workload of injured athletes paired with non-injured athletes (Table 3). Furthermore, the same non-significant result was found for the minutes played in matches between groups (injured athletes: median = 1,426 [1,116–1,787] minutes vs. non-injured: median = 1,651 [678–3,309]; p-value = 0.39532).
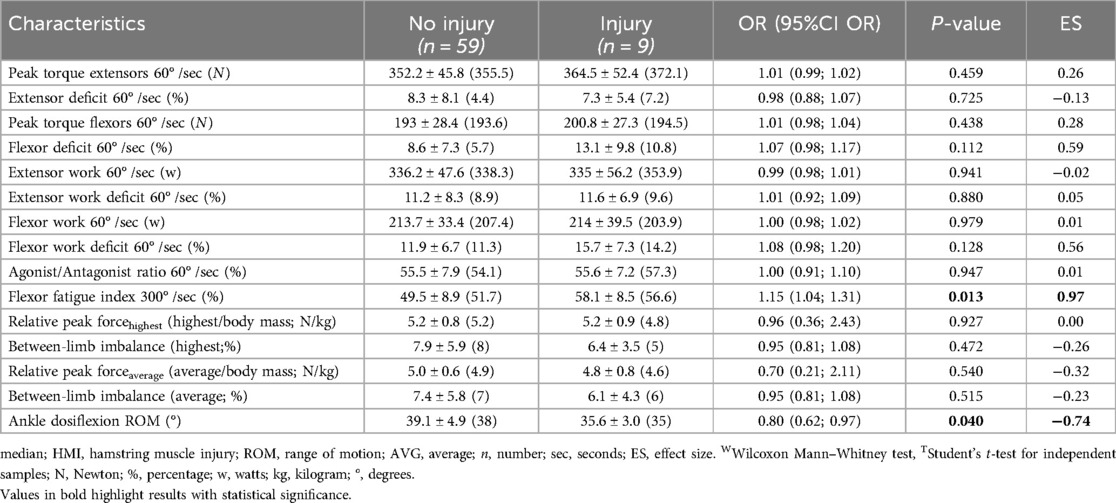
Table 2. Characterization of balance/strength variables according to the occurrence of hamstring injury.

Table 3. Comparison of the performance of athletes with and without hamstring injuries in paired GPS assessment.
Previous hamstring injury (p = 0.032), greater knee-flexor deficit 60° /sec (p = 0.005) and greater knee-flexor fatigue index 300° /sec (p = 0.009) were associated with a greater risk of hamstring muscle injury (Table 4).
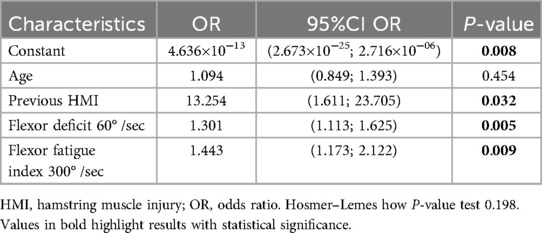
Table 4. Factors associated with hamstring injury.
Potential financial loss was approximately $ −43.2 million USD (98.7% <=> the team's under achievement due to injured athletes + 1.3% <=> salaries paid to injured athletes) and 21% of the merit money that was obtained by the soccer team (Figure 2; Supplementary Table S1).
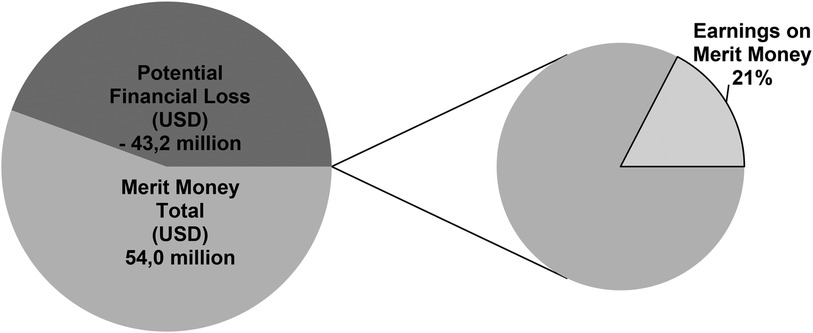
Figure 2. Potential financial loss and earnings on merit money.
4 Discussion
This pilot study aim is verifying the risk factors for hamstring muscle injuries assessed via isokinetic testing, weight bearing lunge testing, eccentric hamstring strength and external workload monitoring and potential financial loss in elite Brazilian soccer. Thus, the present pilot study showed an association between hamstring muscle injury and a higher rate of fatigue in the hamstrings, increased knee-flexor deficit at 60° /sec, dorsiflexion range of motion limitation, and previous hamstring muscle injury. It is noteworthy that there was no difference in the high-speed running variables and other isokinetic muscle variables or eccentric hamstring strength, nor previous ACL injuries, ankle sprains, and age. Thus, resistance to hamstring fatigue, knee flexor asymmetry between limbs and poor ankle mobility should be a focus of interventions in elite soccer players in Brazil, since these factors can increase the risk of hamstring muscle injury. Furthermore, the team's under achievement due to injured athletes plus salaries paid to injured athletes resulted in $ −43.2 million USD of potential financial loss and 21% receipt of merit money.
In agreement with several studies, a higher proportion of injured players had previous hamstring muscle injuries (54, 55). In a meta-analysis of 19 studies, Green et al. (25) demonstrated that previous hamstring muscle injury increased the risk of a new hamstring injury by 3 times (RR = 2.7; p < 0.001) whereas in the present study it was 7 times. Although the present study had a small sample size, 67% of the injured group had a previous hamstring muscle injury while only 22% of the uninjured group had a previous hamstring injury (p = 0.011).
Contrary to the results presented in the literature on isokinetic muscle performance (56), the data from the present study showed no difference between groups for traditional variables such as hamstrings and quadriceps concentric and eccentric torque. However, the present study showed differences between groups for hamstring fatigue index. The injured group had higher fatigue index at 300° /s compared to the non-injured group (58.1 ± 8.5 vs. 49.5 ± 8.9; ES = 0.97). Some studies demonstrate that fatigue could lead to changes in neuromuscular coordination patterns and potentially increase the risk for hamstring muscle injuries (26, 57). Fatigued muscles have a lower capacity to produce force and are more prone to injury from eccentric contractions compared to non-fatigued muscles (26). Regarding eccentric strength variables measured from the NordBord®, the current results corroborate the evidence from the last meta-analysis (25) that there is no association with hamstring muscle injuries. The NordBord® test was performed with a shortened hamstrings position, and in contrast, the most common mechanism of hamstring muscle injuries occurs in the elongated position during a sprint (3, 25). In addition, for the effective use of this device, there is still a need for consensus to identify the best procedures, definitions, and calculations for evaluation of the eccentric strength of hamstrings in different sports settings (22).
Literature exploring the association of ankle dorsiflexion range of motion and hamstring injury risk are conflicting (25, 58). In agreement with the meta-analysis by Green et al. (25), we found no association with the risk of hamstring muscle injury. However, there was a significant difference in this variable between groups in the present study. The mean range of motion in the injured group was 35.6 ± 3°; while the mean in the group without injury was 39.1 ± 4.9° (ES = −0.74; p = 0.017). The difference in range of motion between groups was above the measurement error reported in the literature (i.e., 1.3°–2.8°), reinforcing that the values were clinically relevant (58). A smaller ankle dorsiflexion range of motion can limit ipsilateral limb take-off during running, and therefore, require high force production by the hamstrings to perform the running task at high speed. Thus, this continuous overload can increase the mechanical demand on this muscle group and increase injury risk, meaning that the pre-season assessment that detects restricted ankle range of motion could possibly be used in practice as a screening tool to prevent hamstring muscle injuries. However, further studies are needed to confirm this hypothesis.
Due to the high physical demands of soccer and the congested schedule with short breaks between games, many studies have investigated the association of training load and games played with muscle injuries (46, 59). Some authors have shown that exposure to inappropriate load can increase injury risk up to 5 times (RR = 5.1), with a greater number of accelerations performed over a three-week period associated with greater injury risk in young soccer players (36). However, other studies have shown little association between training load (59) or the congested calendar (60) and injuries. The results of the present study showed that there was no difference between groups for training and game external load. Differences in findings between the present and previous studies may reflect differences between the Brazilian and European calendar, with Brazilian players competing in more games across a season (46, 61). The incidence of injury has previously been compared between South American and European teams. Findings suggest no differences between competitions, reinforcing the hypothesis that although match congestion is higher, injury risk is not increased in South American clubs (62).
According to a recent meta-analysis on the topic, some isolated risk factors were strongly correlated with hamstring muscle injury (25). Considering the multifactorial nature of the etiology of musculoskeletal injuries, investigating the interactions of factors has a crucial role in the occurrence of this injury (63). Despite recognizing the complex nature of muscle injuries, this study did not perform complex and non-linear analyses due to the sample size, as nine injuries were analyzed in just one soccer team and a single season. However, it is the first study to analyze the difference between groups using strength variables, ankle dorsiflexion range of motion, and performance data in training and games in professional Brazilian soccer athletes. Furthermore, an analysis of the external load (GPS) was performed in this study and some authors also recommend the analysis of internal load. The assessment of both the internal and external load and their association with injury risk in soccer players is warranted (64, 65). The HSR distances found in the present study (i.e., medians of 617–730 m for both groups) are in agreement with the standards found in Brazilian football (66). However, the HSR performed by players in this study were lower than previously described in the English Premier League (i.e., ∼778 m) (66). As such, our results may not be generalizable to all competitions around the world. In contrast to our findings, age, eccentric hamstring strength, previous injury history, and concentric hamstring strength at 240° /sec resulted in the best prediction of hamstring muscle injuries in male soccer players of the Kosovo National Premier League (30). Furthermore, the role of eccentric hamstring strength has been studied in soccer context (67) as well as the relationships between exercises used in the training and hamstring fatigue (68–71), thus contributing to the advancement of knowledge on the hamstring risk injury.
To the best of our knowledge, there are still few studies in the scientific literature that have analyzed the costs related to hamstring injuries. In amateur Spanish soccer players, the mean cost of hamstring muscle injuries per player who used the FIFA 11 Programme as their dynamic warm-up was 42% lower: (EUR 742: 95%CI = 410–1,074) compared with athletes who did not use the same approach (EUR 1,271: 95%CI = 929–1,613) (18). In Australian rules football (i.e., Australian Football League), the financial costs associated with recovering from a hamstring injury increased 71% compared with a 43% increase in average yearly athlete salary. From 2003 to 2012, the average financial cost of a single hamstring injury increased by 56%, despite little change in the hamstring injury rates during this period (72). Both cited studies reinforce the findings of an analysis of the financial cost of injuries (not only hamstring injuries), to all ten teams in Australian professional soccer (i.e., A-League) over six consecutive seasons. These researchers found that injury prevention remains necessary for reducing injury-induced athlete-salary costs (73). Allocation of resources for Research, Development, and Innovation is encouraged in the scientific literature aiming to reduce these financial costs and/or increase the earnings on merit money (74–78).
5 Limitations
This is a small cohort pilot study, which limits its external validity and the ability to draw firm conclusions. In our mirroring approach, confounders such as age, the number of matches played during the season, eccentric hamstring strength, and previous injury history were present. These cannot be completely controlled in elite soccer players and as such, this represents a limitation of the present study. Furthermore, we analyzed one club during one season; owing to the small sample size it was not possible to perform non-linear and interaction analyses. However, similar approaches can be found in the scientific literature (79, 80).
6 Conclusion
The results of this pilot study demonstrate the high burden associated with hamstring injuries in elite soccer players. Hamstring injuries in Brazilian soccer players were associated with a previous hamstring injury, increased fatigue index of knee-flexors, restricted ankle dorsiflexion range of motion, and increased isokinetic hamstring strength asymmetry. In addition, a high potential financial loss was found as a reduced receipt of merit money. Furthermore, our findings provide a path for future studies to analyze the interaction between hamstring muscle injury risk factors and financial burden in professional soccer. Last but not least, this pilot study does not intend to assume that the variables analyzed here are the only ones considered as risk factors for hamstring injuries in soccer.
Practical Applications
1. Significant cost reductions for teams may be achieved with less time spent in rehabilitation because of hamstring injury, and greater availability of athletes for training and games.
2. Allocation of resources for Research, Development, and Innovation (RD&I) Departments to reduce these financial costs and/or increase the earnings on merit money is recommended in soccer clubs.
3. Preventive approaches in professional soccer players with previous hamstring injuries should be a priority.
4. Improvement of ankle mobility, correction of knee-flexor strength deficits and specific training to improve knee-flexor fatigue may reduce hamstring strain injuries.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Research Ethics Committee of the Faculdade de Ciências Médicas de Minas Gerais—15737819.6.0000.5134. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
OO-J: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. TG: Writing – original draft, Writing – review & editing, Formal Analysis. NB: Writing – original draft, Writing – review & editing. RQ: Writing – original draft, Writing – review & editing. GR: Writing – original draft, Writing – review & editing. JC: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. RL: Writing – original draft, Writing – review & editing. AL: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We thank to the soccer club and all the soccer players involved in this investigation.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fspor.2024.1360452/full#supplementary-material
Footnote
1. ^Risk factors such as strength, balance, joint mobility and biomechanics are often of interest as these are modifiable, whereas risk factors such as age and previous injury are non-modifiable. (For more details see Fulton et al. Injury risk is altered by previous injury: a systematic review of the literature and presentation of causative neuromuscular factors. Int J Sports Phys Ther. 2014;9(5):583-95).
References
1. International Federation of Football History and Statistics (IFFHS). Brazilian's SERIE A is the World's Best National League in the World. Zurich: IFFHS (2022). Available online at: https://www.iffhs.com/posts/1607 (Accessed January 28, 2022).
2. Ekstrand J, Bengtsson H, Waldén M, Davison M, Khan KM, Hägglund M. Hamstring injury rates have increased during recent seasons and now constitute 24% of all injuries in men’s professional football: the UEFA elite club injury study from 2001/02 to 2021/22. Br J Sports Med. (2022) 57(5):292–8. doi: 10.1136/bjsports-2021-105407
3. Ekstrand J, Hägglund M, Waldén M. Epidemiology of muscle injuries in professional football (soccer). Am J Sports Med. (2011) 39:1226–32. doi: 10.1177/0363546510395879
4. Ekstrand J, Waldén M, Hägglund M. Hamstring injuries have increased by 4% annually in men’s professional football, since 2001: a 13-year longitudinal analysis of the UEFA elite club injury study. Br J Sports Med. (2016) 50:731–7. doi: 10.1136/bjsports-2015-095359
5. Silva JR, Nassis GP, Rebelo A. Strength training in soccer with a specific focus on highly trained players. Sports Med Open. (2015) 1:17. doi: 10.1186/s40798-015-0006-z
6. Suchomel TJ, Nimphius S, Stone MH. The importance of muscular strength in athletic performance. Sports Med. (2016) 46:1419–49. doi: 10.1007/s40279-016-0486-0
7. Navandar A, Veiga S, Torres G, Chorro D, Navarro E. A previous hamstring injury affects kicking mechanics in soccer players. J Sports Med Phys Fitness. (2018) 58:1815–22. doi: 10.23736/S0022-4707.18.07852-0
8. Portillo J, Abián P, Calvo B, Paredes V, Abián-Vicén J. Effects of muscular injuries on the technical and physical performance of professional soccer players. Phys Sportsmed. (2020) 48:437–41. doi: 10.1080/00913847.2020.1744485
9. Afonso J, Claudino JG, Fonseca H, Moreira-Gonçalves D, Ferreira V, Almeida JM, et al. Stretching for recovery from groin pain or injury in athletes: a critical and systematic review. J Funct Morphol Kinesiol. (2021) 6:73. doi: 10.3390/jfmk6030073
10. Malone S, Owen A, Mendes B, Hughes B, Collins K, Gabbett TJ. High-speed running and sprinting as an injury risk factor in soccer: can well-developed physical qualities reduce the risk? J Sci Med Sport. (2018) 21:257–62. doi: 10.1016/j.jsams.2017.05.016
11. Moreno-Pérez V, Soler A, Ansa A, López-Samanes Á, Madruga-Parera M, Beato M, et al. Acute and chronic effects of competition on ankle dorsiflexion ROM in professional football players. Eur J Sport Sci. (2020) 20:51–60. doi: 10.1080/17461391.2019.1611930
12. Ehrmann FE, Duncan CS, Sindhusake D, Franzsen WN, Greene DA. GPS and injury prevention in professional soccer. J Strength Cond Res. (2016) 30:360–7. doi: 10.1519/JSC.0000000000001093
13. Reis GF, Santos TR, Lasmar RC, Oliveira Júnior O, Lopes RF, Fonseca ST. Sports injuries profile of a first division Brazilian soccer team: a descriptive cohort study. Braz J Phys Ther. (2015) 19:390–7. doi: 10.1590/bjpt-rbf.2014.0120
14. Giménez JV, Castellano J, Lipinska P, Zasada M, Gómez MÁ. Comparison of the physical demands of friendly matches and different types on-field integrated training sessions in professional soccer players. Int J Environ Res Public Health. (2020) 17(8):2904. doi: 10.3390/ijerph17082904
15. Hägglund M, Waldén M, Magnusson H, Kristenson K, Bengtsson H, Ekstrand J. Injuries affect team performance negatively in professional football: an 11-year follow-up of the UEFA champions league injury study. Br J Sports Med. (2013) 47:738–42. doi: 10.1136/bjsports-2013-092215
16. Silvers-Granelli HJ, Cohen M, Espregueira-Mendes J, Mandelbaum B. Hamstring muscle injury in the athlete: state of the art. J ISAKOS. (2021) 6:170–81. doi: 10.1136/jisakos-2017-000145
17. Eliakim E, Morgulev E, Lidor R, Meckel Y. Estimation of injury costs: financial damage of English premier league teams’ underachievement due to injuries. BMJ Open Sport Exerc Med. (2020) 6:e000675. doi: 10.1136/bmjsem-2019-000675
18. Nouni-Garcia R, Asensio-Garcia MR, Orozco-Beltran D, Lopez-Pineda A, Gil-Guillen VF, Quesada JA, et al. The FIFA 11 programme reduces the costs associated with ankle and hamstring injuries in amateur Spanish football players: a retrospective cohort study. Eur J Sport Sci. (2019) 19:1150–6. doi: 10.1080/17461391.2019.1577495
19. Abourezk MN, Ithurburn MP, McNally MP, Thoma LM, Briggs MS, Hewett TE, et al. Hamstring strength asymmetry at 3 years after anterior cruciate ligament reconstruction alters knee mechanics during gait and jogging. Am J Sports Med. (2017) 45:97–105. doi: 10.1177/0363546516664705
20. Buckthorpe M, Wright S, Bruce-Low S, Nanni G, Sturdy T, Gross AS, et al. Recommendations for hamstring injury prevention in elite football: translating research into practice. Br J Sports Med. (2019) 53:449–56. doi: 10.1136/bjsports-2018-099616
21. Capaverde VB, Oliveira GDS, de Lima-E-Silva FX, Ribeiro-Alvares JBA, Baroni BM. Do age and body size affect the eccentric knee flexor strength measured during the nordic hamstring exercise in malesoccer players? Sports Biomech. (2021) 9:1–11. doi: 10.1080/14763141.2021.2003850
22. Claudino JG, Cardoso Filho CA, Bittencourt NFN, Gonçalves LG, Couto CR, Quintão RC, et al. Eccentric strength assessment of hamstring muscles with new technologies: a systematic review of current methods and clinical implications. Sports Med Open. (2021) 7(1):10. doi: 10.1186/s40798-021-00298-7
23. Croisier JL. Factors associated with recurrent hamstring injuries. Sports Med. (2004) 34(10):681–95. doi: 10.2165/00007256-200434100-00005
24. Croisier JL, Ganteaume S, Binet J, Genty M, Ferret JM. Strength imbalances and prevention of hamstring injury in professional soccer players: a prospective study. Am J Sports Med. (2008) 36:1469–75. doi: 10.1177/0363546508316764
25. Green B, Bourne MN, van Dyk N, Pizzari T. Recalibrating the risk of hamstring strain injury (HSI): a 2020 systematic review and meta-analysis of risk factors for index and recurrent hamstring strain injury in sport. Br J Sports Med. (2020) 54:1081–8. doi: 10.1136/bjsports-2019-100983
26. Huygaerts S, Cos F, Cohen DD, Calleja-González J, Guitart M, Blazevich AJ, et al. Mechanisms of hamstring strain injury: interactions between fatigue, muscle activation and function. Sports. (2020) 8:65. doi: 10.3390/sports8050065
27. Opar DA, Piatkowski T, Williams MD, Shield AJ. A novel device using the nordic hamstring exercise to assess eccentric knee flexor strength: a reliability and retrospective injury study. J Orthop Sports Phys Ther. (2013) 43:636–40. doi: 10.2519/jospt.2013.4837
28. Orchard JW, Driscoll T, Seward H, Orchard JJ. Relationship between interchange usage and risk of hamstring injuries in the Australian football league. J Sci Med Sport. (2012) 15:201–6. doi: 10.1016/j.jsams.2011.11.250
29. Ribeiro-Alvares JB, Dornelles MP, Fritsch CG, de Lima-E-Silva FX, Medeiros TM, Severo-Silveira L, et al. Prevalence of hamstring strain injury risk factors in professional and under-20 male football (soccer) players. J Sport Rehabil. (2020) 29:339–45. doi: 10.1123/jsr.2018-0084
30. Shalaj I, Gjaka M, Bachl N, Wessner B, Tschan H, Tishukaj F. Potential prognostic factors for hamstring muscle injury in elite male soccer players: a prospective study. PLoS One. (2020) 15:e0241127. doi: 10.1371/journal.pone.0241127
31. Timmins RG, Bourne MN, Shield AJ, Williams MD, Lorenzen C, Opar DA. Short biceps femoris fascicles and eccentric knee flexor weakness increase the risk of hamstring injury in elite football (soccer): a prospective cohort study. Br J Sports Med. (2016) 50:1524–35. doi: 10.1136/bjsports-2015-095362
32. van Dyk N, Bahr R, Whiteley R, Tol JL, Kumar BD, Hamilton B, et al. Hamstring and quadriceps isokinetic strength deficits are weak risk factors for hamstring strain injuries: a 4-year cohort study. Am J Sports Med. (2016) 44:1789–95. doi: 10.1177/0363546516632526
33. van Dyk N, Farooq A, Bahr R, Witvrouw E. Hamstring and ankle flexibility deficits are weak risk factors for hamstring injury in professional soccer players: a prospective cohort study of 438 players including 78 injuries. Am J Sports Med. (2018) 46:2203–10. doi: 10.1177/0363546518773057
34. Bezodis N, Trewartha G, Salo A. Understanding the effect of touchdown distance and ankle joint kinematics on sprint acceleration performance through computer simulation. Sports Biomech. (2015) 14:232–45. doi: 10.1080/14763141.2015.1052748
35. Morin JB, Gimenez P, Edouard P, Arnal P, Jiménez-Reyes P, Samozino P, et al. Sprint acceleration mechanics: the major role of hamstrings in horizontal force production. Front Physiol. (2015) 6:404. doi: 10.3389/fphys.2015.00404
36. Bowen L, Gross AS, Gimpel M, Li FX. Accumulated workloads and the acute: chronic workload ratio relate to injury risk in elite youth football players. Br J Sports Med. (2017) 51:452–9. doi: 10.1136/bjsports-2015-095820
37. Duhig S, Shield AJ, Opar D, Gabbett TJ, Ferguson C, Williams M. Effect of high-speed running on hamstring strain injury risk. Br J Sports Med. (2016) 50:1536–40. doi: 10.1136/bjsports-2015-095679
38. Eliakim E, Doron O, Meckel Y, Nemet D, Eliakim A. Pre-season fitness level and injury rate in professional soccer—a prospective study. Sports Med Int Open. (2018) 2(3):E84–90. doi: 10.1055/a-0631-9346
39. Jiang Z, Hao Y, Jin N, Li Y. A systematic review of the relationship between workload and injury risk of professional male soccer players. Int J Environ Res Public Health. (2022) 19(20):13237. doi: 10.3390/ijerph192013237
40. Maughan PC, MacFarlane NG, Swinton PA. Relationship between subjective and external training load variables in youth soccer players. Int J Sports Physiol Perform. (2021) 16:1127–33. doi: 10.1123/ijspp.2019-0956
41. Martins F, França C, Henriques R, Ihle A, Przednowek K, Marques A, et al. Body composition variations between injured and non-injured professional soccer players. Sci Rep. (2022) 12:20779. doi: 10.1038/s41598-022-24609-4
42. Chow S, Shao J, Wang H. Sample Size Calculations in Clinical Research. 2nd Ed. New York: Chapman & Hall/CRC Biostatistics Series (2008).
43. Pollock N, James SL, Lee JC, Chakraverty R. British Athletics muscle injury classification: a new grading system. Br J Sports Med. (2014) 48:1347–51. doi: 10.1136/bjsports-2013-093302
44. Fuller CW, Ekstrand J, Junge A, Andersen TE, Bahr R, Dvorak J, et al. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Scand J Med Sci Sports. (2006) 16:83–92. doi: 10.1111/j.1600-0838.2006.00528.x
45. Internal Revenue Service (IRS). Yearly Average Currency Exchange Rates. Washington: IRS (2022). Available online at: https://www.irs.gov/individuals/international-taxpayers/yearly-average-currency-exchange-rates (Accessed January 28, 2022).
46. Carling C, McCall A, Le Gall F, Dupont G. The impact of short periods of match congestion on injury risk and patterns in an elite football club. Br J Sports Med. (2016) 50:764–8. doi: 10.1136/bjsports-2015-095501
47. Cavalcante ML, Teixeira PR, Sousa TC, Lima PO, Oliveira RR. Index of fatigue quadriceps in soccer athletes after anterior cruciate ligament reconstruction. Rev Bras Ortop. (2016) 51:535–40. doi: 10.1016/j.rbo.2015.12.002
48. Dauty M, Menu P, Fouasson-Chailloux A, Ferréol S, Dubois C. Prediction of hamstring injury in professional soccer players by isokinetic measurements. Muscles Ligaments Tendons J. (2016) 6(1):116–23. doi: 10.32098/mltj.01.2016.14
49. Dill KE, Begalle RL, Frank BS, Zinder SM, Padua DA. Altered knee and ankle kinematics during squatting in those with limited weight-bearing-lunge ankle-dorsiflexion range of motion. J Athl Train. (2014) 49:723–32. doi: 10.4085/1062-6050-49.3.29
50. Powden CJ, Hoch JM, Hoch MC. Reliability and minimal detectable change of the weight-bearing lunge test: a systematic review. Man Ther. (2015) 20:524–32. doi: 10.1016/j.math.2015.01.004
51. Gabbett TJ. The training-injury prevention paradox: should athletes be training smarter and harder? Br J Sports Med. (2016) 50:273–80. doi: 10.1136/bjsports-2015-095788
52. Hedges LV. Distribution theory for glass’s estimator of effect size and related estimators. J Educ Stat. (1981) 6:107–28. doi: 10.3102/10769986006002107
53. Cohen J. Statistical Power Analysis for the Behavioural Sciences. 2nd ed Hillsdale: Lawrence Erlbaum (1988).
54. Ernlund L, Vieira LA. Hamstring injuries: update article. Rev Bras Ortop. (2017) 52:373–82. doi: 10.1016/j.rbo.2017.05.001
55. Schuermans J, Van Tiggelen D, Danneels L, Witvrouw E. Biceps femoris and semitendinosus–teammates or competitors? New insights into hamstring injury mechanisms in male football players: a muscle functional MRI study. Br J Sports Med. (2014) 48:1599–606. doi: 10.1136/bjsports-2014-094017
56. Marqués-Jiménez D, Calleja-González J, Arratibel I, Delextrat A, Terrados N. Fatigue and recovery in soccer: evidence and challenges. Open Sports Sci J. (2017) 10:52–70. doi: 10.2174/1875399X01710010052
57. Boyas S, Guével A. Neuromuscular fatigue in healthy muscle: underlying factors and adaptation mechanisms. Ann Phys Rehabil Med. (2011) 54:88–108. doi: 10.1016/j.rehab.2011.01.001
58. Konor MM, Morton S, Eckerson JM, Grindstaff TL. Reliability of three measures of ankle dorsiflexion range of motion. Int J Sports Phys Ther. (2012) 7:279–87.22666642
59. Malone S, Owen A, Newton M, Mendes B, Collins KD, Gabbett TJ. The acute: chonic workload ratio in relation to injury risk in professional soccer. J Sci Med Sport. (2017) 20:561–5. doi: 10.1016/j.jsams.2016.10.014
60. Folgado H, Duarte R, Marques P, Sampaio J. The effects of congested fixtures period on tactical and physical performance in elite football. J Sports Sci. (2015) 33:1238–47. doi: 10.1080/02640414.2015.1022576
61. Alves AL, Silami-Garcia E, Morandi RF, Claudino JG, Pimenta EM, Soares DD. Individual analysis of creatine kinase concentration in Brazilian elite soccer players. Rev Bra Med Esporte. (2015) 21:112–6. doi: 10.1590/1517-86922015210202167
62. Bengtsson H, Ortega Gallo PA, Ekstrand J. Injury epidemiology in professional football in South America compared with Europe. BMJ Open Sport Exerc Med. (2021) 7:e001172. doi: 10.1136/bmjsem-2021-001172
63. Bittencourt NFN, Meeuwisse WH, Mendonça LD, Nettel-Aguirre A, Ocarino JM, Fonseca ST. Complex systems approach for sports injuries: moving from risk factor identification to injury pattern recognition-narrative review and new concept. Br J Sports Med. (2016) 50:1309–14. doi: 10.1136/bjsports-2015-095850
64. Claudino JG, Cardoso Filho CA, Boullosa D, Lima-Alves A, Carrion GR, GianonI RLdS, et al. The role of veracity on the load monitoring of professional soccer players: a systematic review in the face of the big data era. App Sci. (2021) 11:6479. doi: 10.3390/app11146479
65. Vanrenterghem J, Nedergaard NJ, Robinson MA, Drust B. Training load monitoring in team sports: a novel framework separating physiological and biomechanical load-adaptation pathways. Sports Med. (2017) 47:2135–42. doi: 10.1007/s40279-017-0714-2
66. CIES Football Observatory. Centre International d’Etude du Sport/International Centre for Sports Studies (CIES). New Skill Corner data: EPL tops intensity rankings, n° 343—16/08/2021. Available online at: https://football-observatory.com/IMG/sites/b5wp/2021/wp343/en/ (accessed October 22, 2022)
67. Sannicandro I, Traficante P, Cofano G. Hamstring injury prevention: the strength assessment in young soccer players. MOJ Sports Med. (2019) 3:28–32. doi: 10.15406/mojsm.2019.03.00075
68. Marshall PW, Lovell R, Jeppesen GK, Andersen K, Siegler JC. Hamstring muscle fatigue and central motor output during a simulated soccer match. PLoS One. (2014) 9:e102753. doi: 10.1371/journal.pone.0102753
69. Madison G, Patterson SD, Read P, Howe L, Waldron M. Effects of small-sided game variation on changes in hamstring strength. J Strength Cond Res. (2019) 33:839–45. doi: 10.1519/JSC.0000000000002955
70. Wilmes E, de Ruiter CJ, Bastiaansen BJC, Goedhart EA, Brink MS, van der Helm FCT, et al. Associations between hamstring fatigue and sprint kinematics during a simulated football (soccer) match. Med Sci Sports Exerc. (2021) 53:2586–95. doi: 10.1249/MSS.0000000000002753
71. Sannicandro I, Cofano G, Raiola G. The acute effects of small-sided games on hamstring strength in young soccer players. Teor Metod Fiz Vihov. (2022) 22:77–84. doi: 10.17309/tmfv.2022.1.11
72. Hickey J, Shield AJ, Williams MD, Opar DA. The financial cost of hamstring strain injuries in the Australian football league. Br J Sports Med. (2014) 48:729–30. doi: 10.1136/bjsports-2013-092884
73. Lu D, McCall A, Jones M, Steinweg J, Gelis L, Fransen J, et al. The financial and performance cost of injuries to teams in Australian professional soccer. J Sci Med Sport. (2021) 24:463–7. doi: 10.1016/j.jsams.2020.11.004
74. Claudino JG, Capanema DO, Santiago PRP. AIM In sports medicine. In: Lidströmer N, Ashrafian H, editors. Artificial Intelligence in Medicine. Cham: Springer (2022). p. 1819–24.
75. Diniz-Silva C, Claudino JG, Silami-Garcia E. Futebol baseado em evidências: desafios e perspectivas da ciência do esporte no brasil. In: Medicina do Esporte no Futebol: Pesquisa e Práticas Contemporâneas. Guarujá: Científica Digital (2021). p. 94–117.
76. McCall A, Davison M, Carling C, Buckthorpe M, Coutts AJ, Dupont G. Can off-field ‘brains’ provide a competitive advantage in professional football? Br J Sports Med. (2016) 50:710–2. doi: 10.1136/bjsports-2015-095807
77. Ramírez-López C, Till K, Boyd A, Bennet M, Piscione J, Bradley S, et al. Coopetition: cooperation among competitors to enhance applied research and drive innovation in elite sport. Br J Sports Med. (2021) 55:522–3. doi: 10.1136/bjsports-2020-102901
78. Viveiros L, Moreira A, Bishop D, Aoki MS. Ciência do esporte no brasil: reflexões sobre o desenvolvimento das pesquisas, o cenário atual e as perspectivas futuras. Rev Bras Educ Fís Esporte. (2015) 29:163–75. doi: 10.1590/1807-55092015000100163
79. Henderson G, Barnes CA, Portas MD. Factors associated with increased propensity for hamstring injury in English premier league soccer players. J Sci Med Sport. (2010) 13:397–402. doi: 10.1016/j.jsams.2009.08.003
Keywords: muscle strain, eccentric knee flexor strength, isokinetic, football (soccer), global positioning satellite system (GPS)
Citation: Oliveira-Júnior O, Gabbett TJ, Bittencourt NFN, Quintão RC, Reis GF, Claudino JG, Lasmar RCP and Leopoldino AAO (2024) Potential financial loss and risk factors for hamstring muscle injuries in elite male Brazilian soccer players: a season-long prospective cohort pilot study. Front. Sports Act. Living 6:1360452. doi: 10.3389/fspor.2024.1360452
Received: 1 February 2024; Accepted: 6 September 2024;
Published: 24 September 2024.
Edited by:
Olivier Girard, University of Western Australia, AustraliaReviewed by:
Victor Moreno-Perez, Miguel Hernández University of Elche, SpainItalo Sannicandro, University of Foggia, Italy
Copyright: © 2024 Oliveira-Júnior, Gabbett, Bittencourt, Quintão, Reis, Claudino, Lasmar and Leopoldino. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Amanda A. O. Leopoldino, YW9saXZlaXJhbGVvcG9sZGlub0BnbWFpbC5jb20=
†ORCID:
Otaviano Oliveira-Júnior
orcid.org/0000-0001-7766-9974
Tim J. Gabbett
orcid.org/0000-0002-9950-5505
Natalia F. N. Bittencourt
orcid.org/0000-0002-7683-9270
Roberto C. Quintão
orcid.org/0000-0001-9264-8872
Guilherme F. Reis
orcid.org/0000-0001-9522-0986
João G. Claudino
orcid.org/0000-0002-0263-8118
Rodrigo C. P. Lasmar
orcid.org/0000-0001-7309-7606
Amanda A. O. Leopoldino
orcid.org/0000-0002-3958-7107