 Markus Gerber1*
Markus Gerber1* Konstantinia Filippou2
Konstantinia Filippou2 Florian Knappe1
Florian Knappe1 Ioannis D. Morres3Emmanouil Tzormpatzakis2Elsa Havas2Harald Seelig1Flora Colledge4Sebastian Ludyga1Marianne Meier5
Ioannis D. Morres3Emmanouil Tzormpatzakis2Elsa Havas2Harald Seelig1Flora Colledge4Sebastian Ludyga1Marianne Meier5 Yannis Theodorakis2
Yannis Theodorakis2 Roland von Känel6
Roland von Känel6 Uwe Pühse1
Uwe Pühse1 Antonis Hatzigeorgiadis2
Antonis Hatzigeorgiadis2
- 1Department of Sport, Exercise and Health, University of Basel, Basel, Switzerland
- 2Department of Physical Education and Sport Sciences, University of Thessaly, Trikala, Greece
- 3Department of Nutrition and Dietetics, University of Thessaly, Trikala, Greece
- 4Department of Health Sciences and Medicine, University of Lucerne, Lucerne, Switzerland
- 5Interdisciplinary Center for Gender Studies, University of Bern, Bern, Switzerland
- 6Department of Consultation-Liaison Psychiatry and Psychosomatic Medicine, University Hospital Zurich, University of Zurich, Zurich, Switzerland
Objectives: Refugees may have an increased risk of developing overweight/obesity as they often experience a nutritional transition. Because maintaining good cardiorespiratory fitness can help reduce the negative impact of excess weight on overall health, the objective of this study was to examine whether fitness moderates the relationship between weight status and cardiovascular and mental health outcomes in forcibly displaced individuals living in a Greek refugee camp.
Methods: A sample of 142 forcibly displaced individuals were recruited. Cardiorespiratory fitness was assessed with the submaximal Åstrand-Rhyming bicycle ergometer test. Blood pressure, blood lipids, blood glucose, and hs-CRP were assessed as physical health outcomes, whereas post-traumatic stress disorder, depression and anxiety symptoms, pain, and quality of life were assessed as mental health outcomes. Main and interaction effects were tested via analyses of covariance (ANCOVAs).
Results: Almost 50% of the participants were overweight/obese, more than 60% presented with very poor fitness levels, and the percentage of participants with very poor fitness levels was particularly high among overweight/obese participants. Whereas overweight/obesity was associated with a less favorable body composition and cardiovascular risk profile, poor fitness was associated with a higher percentage of body fat and a lower percentage of muscle mass. Cardiorespiratory fitness did not moderate the relationship between overweight/obesity and most of the assessed health outcomes.
Conclusions: Only limited support was found for the applicability of the fit-but-fat concept to our population of forcibly displaced individuals. Public health services should prioritize measures to prevent overweight/obesity and associated diseases in refugee camps. Moreover, efforts are needed to improve the fitness of camp residents via exercise/sport interventions.
1 Introduction
Refugees often face numerous challenges related to healthy nutrition (1), limited access to healthcare (2), and disrupted living conditions (3), which can contribute to the development of overweight and obesity (4). As highlighted by the United Nations Organization (5), safeguarding the health of refugees and migrants is a vital part of achieving sustainable development goal (SDG) 3 to ensure healthy lives and promote well-being for all at all ages. In a recent meta-analysis, the global prevalence rates of overweight and obesity in refugees were estimated to be 29% and 23%, respectively (6). However, the prevalence of overweight and obesity among refugees can vary depending on various factors such as their age, sex, region of origin, living conditions, and length of time spent in displacement (7–9).
Refugees may have an increased risk of developing overweight and obesity as they often experience a nutritional transition when they move from their home countries to a host country (10). Refugees often come from regions with different food cultures and availability (11). When they arrive in a new country, they may find a different range of foods, including those that were not commonly consumed in their home countries. This can lead to changes in their dietary habits as they adapt to the available food options (12). Refugees may also face challenges in adapting to the local food culture in their host countries. While some may try to maintain their traditional dietary practices, others may find it necessary to modify their diets due to the lack of familiar ingredients or cooking facilities (13, 14). In addition, refugees often face economic challenges upon arrival in a new country (15). Limited financial resources may restrict their access to a varied and balanced diet (11). In some cases, refugees may rely heavily on low-cost and processed foods, which can be high in calories, but lacking in essential nutrients (16). In this regard, studies have highlighted that overweight and obese individuals can still suffer from nutritional deficiencies if they consume energy-dense, nutrient-poor foods (17, 18). This can lead to an increased risk of malnutrition and related health problems (19).
As in any population (20), studies in different refugee and migrant populations have shown that overweight and obesity can have detrimental health implications (21, 22). Previous research with refugees revealed that overweight and obesity were associated with a higher risk of developing chronic diseases, including cardiovascular diseases (23), type 2 diabetes (24), and hypertension (25). Prior research has also shown that overweight and obesity can contribute to poor self-esteem (26), body image issues (27), and increased risk of mental health conditions such as depression and anxiety (28, 29). Refugees may already face high levels of psychological stress (30), and weight-related concerns can exacerbate their mental health difficulties (31). Conversely, mental distress can lead to increased food intake and contribute to weight gain (32). In addition, excess weight can strain joints, leading to musculoskeletal problems (33), including pain, arthritis, and mobility issues. Overweight and obese individuals may also encounter reduced physical mobility (34), resulting in a decreased capacity to engage in daily activities and may potentially limit their participation in social and community life within a refugee camp (including participation in physical activity, exercise, and sport) (35, 36). Finally, overweight and obese refugees may face challenges in accessing appropriate healthcare, as the healthcare systems in refugee camps may be overwhelmed, and thus lack resources to effectively address weight-related issues (37–39). It has therefore been concluded that addressing overweight and obesity should be a priority in refugees, with a focus on nutrition education, access to healthcare services, and physical activity programs (40, 41).
One advantage of promoting regular physical activity might be that it increases cardiorespiratory fitness (42, 43), which has been shown to mitigate the effects of overweight on health (44). While being overweight or obese is generally associated with an increased risk of various health conditions (as highlighted above), maintaining good cardiorespiratory fitness can help reduce the negative impact of excess weight on overall health (45). Cardiorespiratory fitness refers to the ability of the cardiovascular and respiratory systems to supply oxygen to the muscles during physical activity (46). Regular physical activity and aerobic exercise, such as brisk walking, jogging, or cycling, improve cardiorespiratory fitness (47, 48). Participation in aerobic exercise can moderate the effects of overweight on health by (a) lowering blood pressure, reducing the risk of cardiovascular disease, and improving overall cardiovascular health (49); (b) enhancing insulin sensitivity and glucose metabolism, which can help individuals with excess weight or obesity manage their blood sugar levels more effectively and reduce the risk of developing type 2 diabetes (50); (c) contributing to weight loss or weight maintenance, by increasing metabolism and promoting the preservation of lean muscle mass, which is beneficial for overweight individuals (51); (d) strengthening the respiratory muscles and enhancing lung capacity (52); and (e) reducing stress and improving mental health (53, 54). In the scientific literature, this positive effect of aerobic exercise in the overweight and obese is also known as the “fitness-fatness paradox” (55). It refers to the observation that individuals who are overweight or obese may nevertheless exhibit signs of good cardiorespiratory fitness. Traditionally, body mass index (BMI) has been widely used as a measure of body fatness and health (56). BMI is calculated by dividing a person's weight (in kilograms) by the square of their height (in meters). However, BMI does not differentiate between fat and lean mass (muscle, bone, and organs), nor does it account for differences in body composition (57). The fitness-fatness paradox also suggests that good cardiorespiratory fitness can be achieved independent of the degree of overweight and obesity (58). Nevertheless, it is important to recognize that the fitness-fatness paradox does not imply that excess body weight is harmless. However, the paradox emphasizes the importance of not relying solely on weight or BMI as predictors of overall health, but adopting a more comprehensive and nuanced approach by also looking at participants’ cardiorespiratory fitness (59).
Previous studies have shown that forcibly displaced individuals living in refugee camps often have lower fitness levels than the general population (60). During their flight or daily life in a refugee camp, refugees often face a range of challenges that can affect their cardiorespiratory fitness levels (61, 62). Such challenges include a disruption of physical activity routines (e.g., lack access to safe and appropriate spaces for physical activity, legal barriers to work), restricted access to healthcare (e.g., preventive care and treatment for chronic conditions), inadequate nutrition, mental health issues (with an indirect impact on cardiorespiratory fitness by affecting motivation, or energy levels), as well as environmental factors (e.g., exposure to poor air quality, extreme temperatures) (63, 64).
Given this background, the aims of our study were as follows: First, to assess the prevalence of overweight and obesity in a sample of forcibly displaced individuals living in a Greek refugee camp. Second, to assess participants cardiorespiratory fitness levels. Third, to examine whether and to what degree (a) normal weight and overweight/obese participants and (b) participants with low vs. higher fitness levels differ in body composition, cardiovascular risk markers, and mental health outcomes. Fourth, to examine whether participants’ fitness levels moderate the relationship between their weight status and cardiovascular and mental health outcomes. The present study will make an important contribution to the existing body of research since there is limited knowledge about the cardiorespiratory fitness level of residents in refugee camps. Moreover, it is unclear so far whether the “fit but fat” concept can also be observed in forcibly displaced individuals.
2 Methods
2.1 Participants and procedures
The data come from a larger pragmatic randomized controlled trial (RCT) (blinded). In this paper, cross-sectional baseline data are presented. Ethical approval was obtained from the local ethical review boards (Greece: IEC-DPESS 1701 [Internal ethics committee of the Department of Physical Education and Sport Science, University of xxx (blinded)]; Switzerland: EKNZ AO_2020–00036 [Ethic commission of Northwestern and Central Switzerland]). The study took place in a remote area in Central Greece in a refugee camp, which is under the governance of the Ministry of Migration and Asylum. In the camp, residents live in containers (equipped with a bathroom and kitchen), either together with family members or with a maximum of four individuals of the same sex and origin. The residents spend most of their time in the camp. Due to legal barriers, they are not allowed to work. Leisure activities are scarce, and the remote location makes it difficult to escape the camp's daily routine.
Participants were eligible if they met the following inclusion criteria: (a) living in the selected refugee camp, (b) 16–59 years old, (c) able to read in English, Arabic, Farsi, or French, and (d) provided written informed consent. We decided not to include children and younger adolescents to ensure that participants have the cognitive capacity to understand the questions included in the questionnaires. For pragmatic reasons, we also decided not to include older adults (≥60 years) to reduce the heterogeneity in the sample. Including children/younger adolescents and older adults would have required us to offer more exercise and sport activities that meet the specific preferences/needs of these target populations. Parental/guardian informed consent for minors (16–18 years) was not needed in the present project, because according to Swiss laws (Federal Act on Research involving Human Beings, HRA, Art. 23, 1a), legal representatives only need to provide written informed consent for their adolescent child (aged 14–17 years) if a project entails more than minimal risks and burdens (which was not the case for the present study). A screening was performed with potentially eligible households to draw a random sample stratified by sex. For the RCT, the minimal estimated sample size to demonstrate an intervention effect on post-traumatic stress disorder (PTSD) symptoms (the primary outcome of this RCT) was 136 participants (65).
The screening, recruitment, and data assessment took place in May 2021 by the research team together with 10 trained research assistants who were familiar with the residents’ cultural background and the camp's contextual setting. Both written and verbal information were given to the participants in their native languages, and participants provided written informed consent before the first data assessment. All participants were assured that participation is voluntary, and that withdrawal is possible at any time without any disadvantages, particularly with regard to the asylum process. Data assessment was carried out at the nearby Department of Physical Education and Sport Science of the University of Thessaly (65). Participants received information about their results after completion of the assessment and were referred to a specialist in case of a potential health risk. As further incentives, participants received a meal and some sport equipment.
2.2 Measures
Due to space constraints, only a concise description of the applied instruments is given here. More detailed information can be found in the published study protocol (65).
Body weight and body composition were assessed with a digital weighing scale (BC-545, Tanita, USA) that also allowed bioelectrical impedance analysis to measure the percentage of body fat and muscle mass. Body height was assessed with a stadiometer. Blood pressure was assessed three times (with a 2-min interval) with an Omron® digital blood pressure monitor after participants had rested for 5 min in a seated position (66). Finger prick methodology was applied to obtain capillary blood samples. Total cholesterol, low- (LDL) and high-density (HDL) lipoprotein cholesterol, triglycerides, and blood glucose levels (HbA1c) were analysed via Afinion 2 analysers (Abbott, Wädenswil, Switzerland). Afinion 2 point-of-care (PAC) analyser results correspond well with laboratory tests for both lipid levels and HbA1c (67, 68). In addition, 20 μm blood were collected with a Minivette® POCT EDTA (Sarstedt AG, Nümbrecht, Germany) to assess high-sensitivity C-reactive protein (hs-CRP). Analyses were done in a Cube-S Eurolyser device (Eurolyser Diagnostica GmbH, Salzburg, Austria) (69).
We applied the Åstrand-Rhyming Indirect Test of Maximal Oxygen Uptake (70), a submaximal bicycle ergometer test, to measure participants’ cardiorespiratory fitness. Based on sex, a correction factor for age, body weight, mean steady state, and power output, oxygen uptake as peak VO2max (ml/kg/min) was calculated (71). This test has been used previously in studies on refugees (62).
All psychological measures were assessed with instruments that have been previously employed in studies involving forcibly displaced adults (62, 72–74). Given that many participants had limited English skills, the questionnaires were available in English, Arabic, Farsi, and French language, and translators supported the data assessment process. All instruments have been previously validated in English, Arabic, Farsi, and French (65), and the scales had acceptable or good internal consistency (Cronbach's alpha >0.7) in our pilot study (61). PTSD symptoms were measured with the 22-item Impact of Event Scale-Revised (IES-R) (75), which refers to DSM-5 (76) and ICD-10 (77) criteria of PTSD. Answers were given on a five-point Likert scale from 0 (not at all) to 4 (extremely), resulting in an overall score between 0 and 88 points. Depressive symptoms were measured with the 9-item Patient Health Questionnaire (PHQ-9) (78), which refers to DSM-5 criteria for major depression (76). Answers were given on a four-point Likert scale from 0 (not at all) to 3 (nearly every day), with overall scores varying between 0 and 27. Anxiety symptoms were measured with the 7-item General Anxiety Disorder scale (GAD-7) (79), which refers to DSM-5 criteria for generalized anxiety disorder (76). Answers were given on a four-point Likert scale from 0 (not at all) to 3 (nearly every day), with overall scores ranging between 0 and 21. Pain was measured with the 5-item Visual Analogue Scale for Pain (VAS) (80), which asked for pain over the last week in the head, back, chest, stomach, and extremities (arms, legs, hands, feet). Item scores ranged from 0 (no pain) to 100 (pain as bad as it could be) and the average was calculated, to build a total index ranging from 0 to 100. Quality of life was measured with the 5-item World Health Organization (WHO) Index (81). Answers were given on a Likert scale ranging from 0 (at no time) to 5 (all the time). The individual item scores were summed, yielding an overall score between 0 and 25 (82).
2.3 Statistical analyses
Descriptive statistics (n, %, M, SD, Min, Max, Skew, Kurt) are presented to describe the characteristics of the sample and distribution of the study variables. Before carrying out the main analyses, data were screened for univariate outliers (>3.5 SD above the mean). Univariate outliers were excluded from all further analyses. If substantial deviations from normality (defined as Skew >2 and/or Kurt >7) (83) were observed after exclusion of univariate outliers, these variables were log-transformed before carrying out any further analyses. For mental health outcomes, the internal consistency was tested via Cronbach's alpha, which was expected to be ≥.70. Chi2-tests (χ2) and one-way analyses of covariance (ANCOVAs) were used to test differences between participants classified as normal weight and overweight/obese (due to the limited sample size, overweight and obese participants were combined in one group). Participants were classified as overweight if their BMI was ≥25 kg/m2 and as obese if their BMI was ≥30 BMI kg/m2. One-way ANCOVAs were applied to test differences between participants with different fitness levels. Classification of fitness levels are based on standards of the American College of Sports Medicine, adjusted for participants’ age and sex (84). Finally, a series of two-way ANCOVAs was used to test the interaction (moderator effect) between weight and fitness status. In these analyses, weight status and cardiorespiratory fitness were used as fixed factors (including an interaction term). Age, sex, education, time away from home country and time living in the refugee camp were considered as potential confounders. All analyses were carried out with SPSS version 28 for Mac (IBM Corporation, Armonk, USA), and the level of significance was set at p < 0.05 across all analyses. Effect sizes were interpreted as follows: small: η2 ≥ .01, medium: η2 ≥ .06, and large: η2 ≥ .138 (85).
3 Results
3.1 Sample characteristics
In total, 150 participants (76 men, 74 women) presented with valid BMI values. Of these participants, 56.7% (n = 85) completed the questionnaire in Farsi, 22.7% (n = 34) in Arabic, 14.7% (n = 22) in French, and 6.0% (n = 9) in English. The majority of the participants came from Afghanistan (n = 73), Somalia (n = 22), Congo (n = 18), or Syria (n = 12). Other reported home countries were Iran (n = 8), Iraq (n = 3), Sierra Leone (n = 2), Turkey (n = 2), Cameroon (n = 1), Guinea (n = 1), and Pakistan (n = 1) (7 participants did not answer this question). Concerning educational background, 37 participants reported not having any formal education, 51 completed primary school, 34 high school, and 20 completed higher education (university) (8 participants did not answer this question). Given the low number of underweight participants, we decided to exclude these participants from all further comparisons, resulting in a final sample of n = 144 participants (73 men, 71 women).
3.2 Descriptive results
With regard to weight status, 4.0% were classified as underweight (n = 6; 3 women, 3 men), 48.0% were normal weight (n = 72, 45 men, 27 women), 29.3% were overweight (n = 44, 22 men, 22 women), and 18.7% were obese (n = 28, 6 men, 22 women). With regard to cardiorespiratory fitness (estimated VO2max), 62.1% (n = 72) of the participants presented with very low fitness levels (1–19 percentile), 15.5% (n = 18) with poor levels (20–39 percentile), 9.5% (n = 11) with fair levels (40–59 percentile), 5.2% (n = 6) with good levels (60–79 percentiles), 4.3% (n = 5) with excellent levels (80–94 percentiles), and 3.4% (n = 4) with superior levels (≥95 percentile). Since more than six out of ten participants were classified in the lowest fitness category, in all subsequent analyses, we compared this group to their counterparts with higher fitness levels.
Means, standard deviations, minimal and maximal scores, skewness and kurtosis are reported in Table 1 for all study variables. For HbA1c and hsCRP, 3 and 7 cases were identified as univariate outliers, respectively. Because HbA1c and hsCRP still showed major deviations from normality after exclusion of outliers, these variables were log-transformed. As shown in Table 1, internal consistency (Cronbach's alpha) was satisfactory for all mental health outcomes.
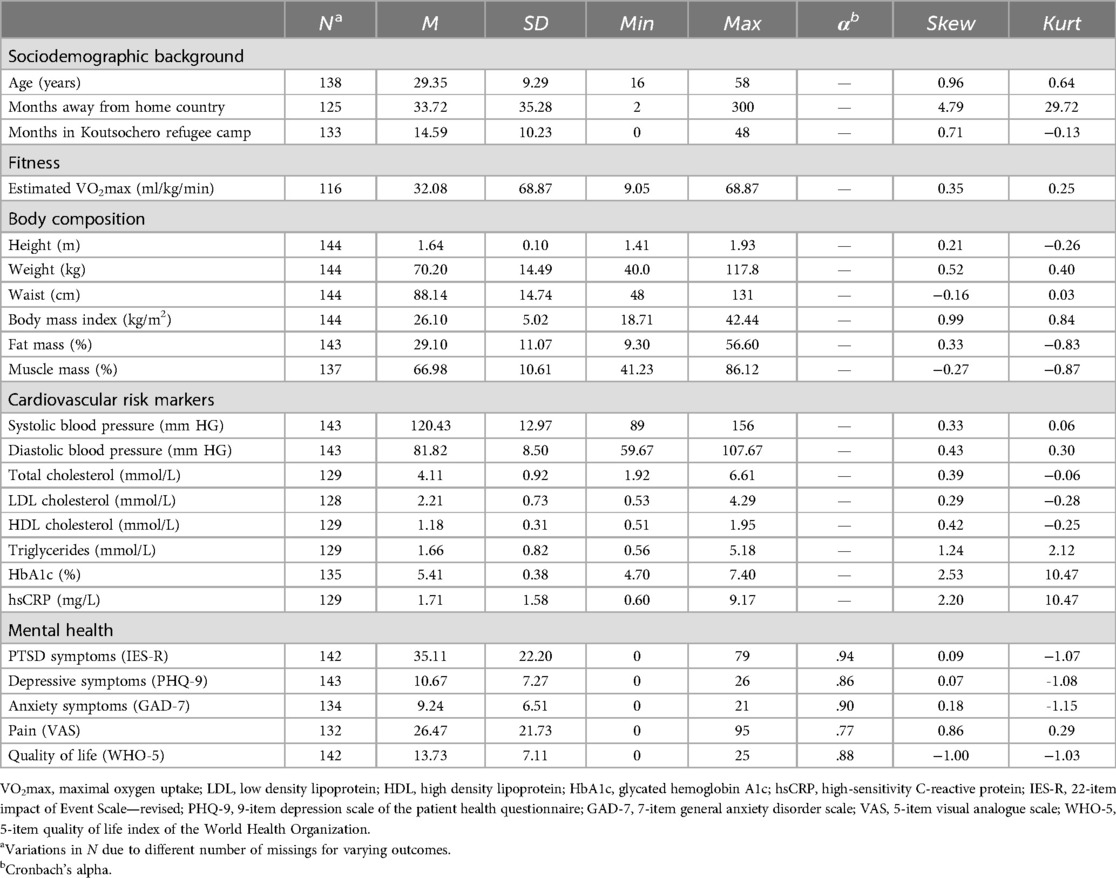
Table 1. Descriptive statistics.
3.3 Association of weight status and cardiorespiratory fitness with covariates
Compared to men (38.4%, n = 28), women were more likely to be overweight/obese (62.0%, n = 44), χ2(1,144) = 8.03, p < 0.01. No significant association was found for education (p > 0.05). Overweight/obese participants were older (M = 32.77 ± 9.75 years) than their normal weight counterparts (M = 25.93 ± 7.42 years), F(1,137) = 21.51, p < 0.001, η2 = 0.137, but did not differ in time away from their home country or time living in the Koutsochero refugee camp (p > 0.05).
Compared to men (53.1%, n = 34), women (73.1%, n = 38) were overrepresented among participants with very low fitness levels, χ2(1,116) = 4.85, p < 0.05. By contrast, no significant associations were found between cardiorespiratory fitness and education, age, months away from home country, and months living in the Koutsochero refugee camp (all p > 0.05).
3.4 Differences in health outcomes based on participants’ weight status
Table 2 shows that after controlling for age and sex, normal weight and overweight/obese participants differed in several of the assessed variables. While differences were observed in cardiorespiratory fitness, body composition, and most of the cardiovascular risk markers, no differences were found for any of the mental health outcomes. More specifically, overweight/obese participants had lower estimated VO2max (small effect), higher fat mass (large effect), lower muscle mass (large effect), higher systolic and diastolic blood pressure (small effect), higher total cholesterol (medium effect), higher LDL cholesterol (medium effect), higher HbA1c (small effect) and higher hsCRP (small effect). For anxiety and pain, initially significant group differences between normal weight and overweight/obese participants disappeared after controlling for covariates.
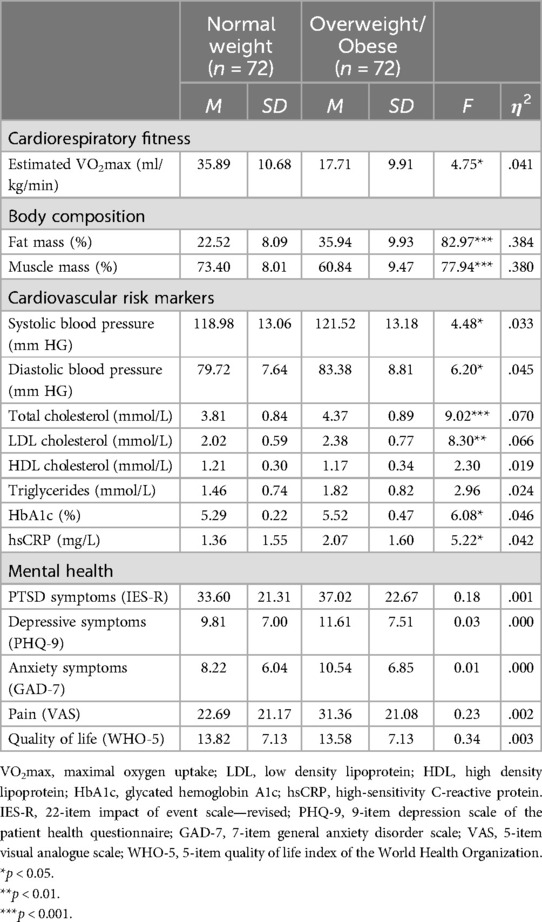
Table 2. One-way analyses of covariance (controlled for age and sex) with weight status as fixed factor, and cardiorespiratory fitness, body composition, cardiovascular risk markers, and mental health as outcome variables.
3.5 Differences in health outcomes based on participants’ fitness levels
As mentioned above, 62.1% (n = 72) of the participants presented with very low fitness levels (1–19 percentile). When these participants were compared to their fitter counterparts, differences were found in body composition and hsCRP (Table 3). More specifically, participants with very poor fitness levels had higher BMI (medium effect), higher fat mass (large effect), lower muscle mass (large effect), and higher hsCRP (medium effect). No significant differences were found in the remaining cardiovascular parameters and in any mental health outcomes.
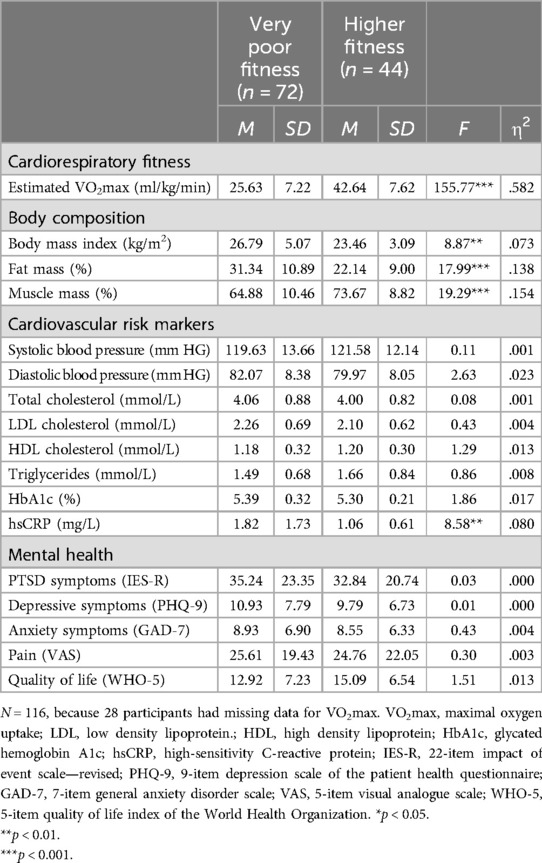
Table 3. One-way analyses of variance (controlled for age and sex) with fitness status as fixed factor, and fitness, body composition, cardiovascular risk markers, and mental health as outcome variables.
3.6 Fitness as a moderator of the relationship between participants’ weight status and health outcomes
As shown in Table 4, compared to normal weight counterparts (46.8%, n = 29), participants with overweight/obesity were more likely to have very low fitness levels (79.6%, n = 43), χ2(1,116) = 13.23, p < 0.001. Approximately one in 10 participants (9.5%, 11 of 116) was overweight/obese, but was not classified in the lowest fitness category, whereas the portion of overweight/obese participants with “good” or higher fitness was 5.6% (3 of 54). Against our expectations, only one significant interaction effect was found between weight status and fitness level. Post-hoc tests with Bonferroni correction showed that overweight/obese participants with very low fitness levels perceived more pain (p < .05) than normal weight participants with very low fitness levels. No statistically significant differences were found between the other groups.
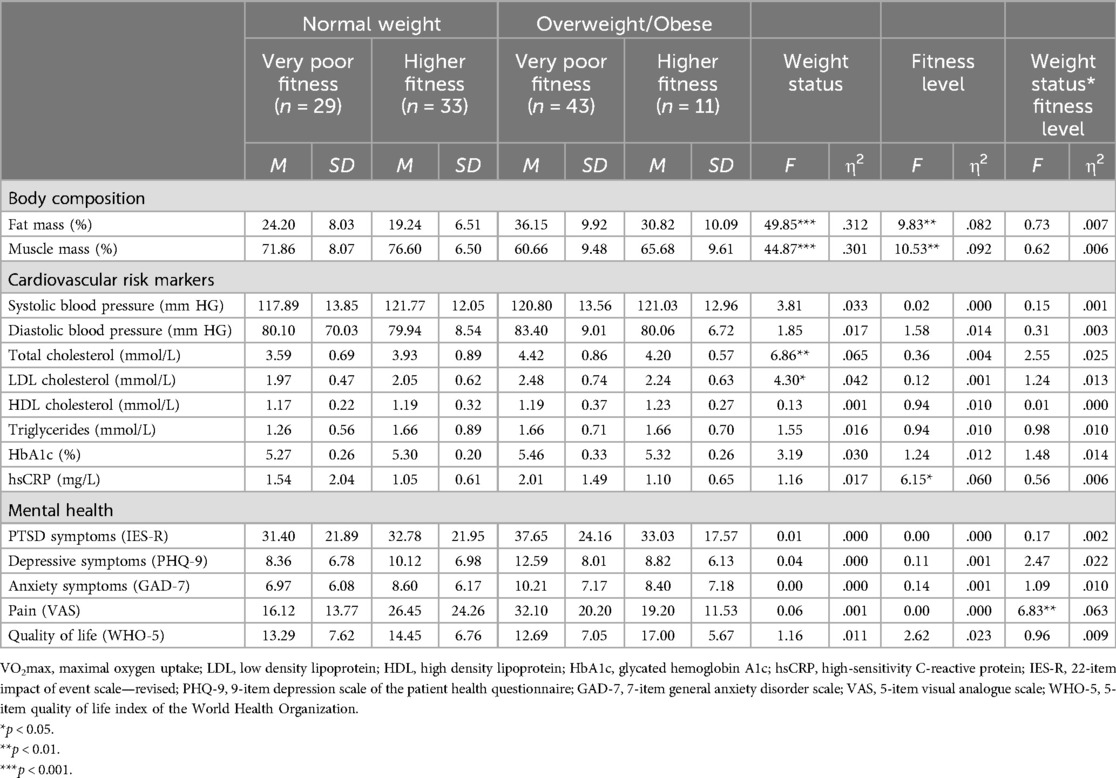
Table 4. Two-way analyses of covariance (controlled for age and sex) with weight and fitness status as fixed factors, and body composition, cardiovascular risk markers, and mental health as outcome variables.
4 Discussion
The key findings of the present study can be summarized as follows: First, in a sample of forcibly displaced individuals living in a Greek refugee camp, almost half of the participants (48.0%) were overweight or obese. Second, approximately six out of 10 participants (62.1%) presented with very poor fitness levels, and the percentage of participants with very poor fitness levels was particularly high among overweight/obese participants (79.6%). Third, overweight/obesity was associated with a less favorable body composition and cardiovascular risk profile, whereas poor fitness was associated with a higher percentage of body fat and a lower percentage of muscle mass. Fourth, overweight/obese participants reported a particularly high pain level if they were unfit.
This study addressed four distinct research questions, which will now be discussed in turn. Our first goal was to assess the prevalence of overweight and obesity in a sample of forcibly displaced individuals living in a Greek refugee camp. Our findings show that a large percentage of the participants were overweight or obese (48.0%), whereas underweight was a less prevalent issue (4.0%). This contrasts with prior research among Western Sahara refugees, where a high double burden of both over- and undernutrition was observed (86). Hence, in our study, overweight and obesity were similarly prevalent in forcibly displaced individuals as in the Greek adult population, in which the prevalence of overweight and obesity has been estimated to be 47.5% percent (87). Given the negative health consequences of overweight/obesity (88), this finding is concerning and underscores the importance of learning more about the causes of overweight/obesity in this specific population and making overweight/obesity prevention a key target for health interventions in refugee and migrant populations (41, 89). There are several effective measures to prevent overweight/obesity, including the promotion of healthy eating (e.g., reduction of sugary drinks, snacks, and fatty foods, increase of consumption of fruit and vegetables) and regular physical activity (41, 90). Programs focusing on physical activity should encourage different forms of activities, including sports, exercise, play, and physical activity in everyday life (65). Promoting healthy lifestyles could also focus on the family as a whole in order to increase physical activity or increase healthy eating (91).
Our second goal was to estimate participants cardiorespiratory fitness levels. In this regard, it was surprising that based on age and sex-adjusted norms, almost two thirds of the participants (62.1%) had very poor fitness levels. According to the reference data of the American College of Sports Medicine (84), participants with such fitness levels fall into the lowest fitness category (percentile 1–19). This is critical as previous studies have shown that low cardiorespiratory fitness levels are associated with impaired health and increased risks for both all-cause and disease-specific mortality (92, 93). In future research, it would be interesting to learn more about the underlying reasons for the low fitness level. For instance, gathering longitudinal data could help to find out whether fitness levels decline as a function of time residing in a refugee camp, as there might be little opportunity to be or become physically active.
Our third goal was to examine whether and to what degree normal weight and overweight/obese participants differ in body composition, cardiovascular risk markers, and major mental health outcomes. In agreement with the extensive body of available literature, we found that overweight/obesity was associated with lower estimated VO2max (94), higher percentage body fat (95), lower relative muscle mass (96), higher blood pressure (97), higher cholesterol levels (particularly LDL cholesterol) (98), higher HbA1c (99) and higher hsCRP (100). These health parameters are well known to contribute to the development of cardiovascular and other chronic diseases (101). Our study also reinforces previous evidence that BMI is sufficiently (>38% of explained variance) associated with participants’ body composition (95), and may thus serve as a screening tool in a refugee camp setting (102). Opposite to the evidence reported in the international literature (28, 29), no differences were found in the present study between normal weight and overweight individuals in mental health outcomes. One explanation might be that overweight is seen more positively in some cultures (103). This could particularly be true for forcibly displaced individuals who have had an arduous flight, faced many deprivations, and currently live in an environment characterized by resource poverty (104). Such an attitude can represent an important challenge in efforts to prevent overweight and obesity in this specific population. With regard to differences between participants with the poorest vs. higher fitness levels, we found only statistically significant differences in body composition and hsCRP. While this concurs well with existing research (105, 106), the lack of significant associations between fitness level and the other health outcomes might be due to a floor effect associated with the generally low fitness levels in this sample, with only 12.9% reporting “good” (or higher) fitness levels.
Finally, only limited evidence was found that among forcibly displaced individuals living in a Greek refugee camp, participants’ fitness is able to moderate the relationship between weight status and cardiovascular and mental health. This is contrary to the literature on the fitness-fatness paradox (45, 55, 59), suggesting that having adequate cardiorespiratory fitness can mitigate the adverse effects of overweight/obesity on cardiovascular health (107). To a certain degree, our study also questions the notion that cardiorespiratory fitness can be achieved independent of body weight. In our study population, among 54 overweight/obese participants with valid fitness data, only 3 (5.5%) achieved “good” (or higher) fitness levels, which is similar to what has been reported in previous studies (59). The only significant interaction between participants’ weight status and fitness was found for pain, showing that overweight/obese participants with poorest fitness perceived higher pain levels than the other study participants. This is an important finding, as chronic pain is associated with reduced quality of life (108) and increased mental health issues (109). Nevertheless, the results of the present study should be considered preliminary until data are available from studies with larger samples in which there is more variation in cardiorespiratory fitness. With other words, the fact that most participants had very low fitness levels might have complicated the detection of statistically significant interaction effects.
The strengths of the present study are that we examined the association between overweight/obesity and cardiovascular and mental health outcomes in an under-researched population. So far, few studies have assessed cardiorespiratory fitness in forcibly displaced individuals. While this is the first study that examined the fitness-fatness concept in refugees, it should be noted that the group of overweight/obese participants with higher fitness levels consisted of a comparably small number of participants. Moreover, the cross-sectional nature of our data precludes causal interpretation of the relationships. Finally, the results of this study cannot be generalized to the general population of forcibly displaced individuals because this group is characterized by high diversity and also includes individuals who have been granted asylum in the host countries. Furthermore, the living conditions in refugee camps as well as the composition of the resident populations can largely differ within and between countries. Finally, it should be noted that we did not include children, younger adolescents, or elderly people, although overweight and obesity constitutes an issue in these populations, as well.
4.1 Conclusions
Our study shows that overweight and obesity are prevalent among residents living in a refugee camp in Greece, posing potential risks to their cardiovascular health. Consequently, public health services should prioritize preventive measures and be well-prepared to address associated diseases. We have also noticed that cardiorespiratory fitness is relatively poor in this sample of forcibly displaced individuals. While efforts are needed to improve the fitness of camp residents, the evidence regarding the feasibility and effectiveness of exercise and sport interventions in refugee settings is still in its infancy. Research efforts in this area should be intensified in order to gain relevant insights and to convince political stakeholders of the importance of this issue.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Ethical commission of Northwestern and Central Switzerland (EKZN, Switzerland) and the Ethical review board of the Department of Physical Education and Sport Sciences, University of Thessaly (Greece). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants’ legal guardians/next of kin because according to Swiss laws (Federal Act on Research involving Human Beings, HRA, Art. 23, 1a), legal representatives only need to provide written informed consent for their adolescent child (aged 14 to 17 years) if a project entails more than minimal risks and burdens (which was not the case for the present study). For more information see: https://www.fedlex.admin.ch/eli/cc/2013/617/en.
Author contributions
MG: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Methodology, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing. KF: Conceptualization, Data curation, Methodology, Project administration, Writing – review & editing. FK: Conceptualization, Data curation, Methodology, Project administration, Writing – review & editing. IM: Conceptualization, Data curation, Funding acquisition, Methodology, Project administration, Supervision, Writing – review & editing. ET: Conceptualization, Data curation, Project administration, Writing – review & editing. EH: Conceptualization, Data curation, Project administration, Writing – review & editing. HS: Conceptualization, Funding acquisition, Methodology, Writing – review & editing. FC: Conceptualization, Funding acquisition, Writing – review & editing. SL: Conceptualization, Funding acquisition, Methodology, Writing – review & editing. MM: Conceptualization, Funding acquisition, Methodology, Writing – review & editing. YT: Conceptualization, Funding acquisition, Methodology, Writing – review & editing. RK: Conceptualization, Funding acquisition, Methodology, Writing – review & editing. UP: Conceptualization, Funding acquisition, Methodology, Writing – review & editing. AH: Conceptualization, Data curation, Funding acquisition, Methodology, Project administration, Resources, Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study is partly funded by the Swiss Network for International Studies (SNIS). The funding source has no influence on the design of the study, the collection, management, analysis and interpretation of the data, the writing of the manuscript or on the selection of the journal.
Acknowledgments
We thank the camp management for their support of our project. We also thank all participants for their participation in the study. We further acknowledge that the study was carried out in accordance with the ethical principles described in the Declaration of Helsinki and that the study procedures were in line with the current laws of the countries involved in the implementation of the study (Greece and Switzerland).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Nisbet C, Lestrat KE, Vatanparast H. Food security interventions among refugees around the globe: a scoping review. Nutrients. (2022) 14. doi: 10.3390/nu14030522
2. Nowak AC, Namer Y, Hornberg C. Health care for refugees in Europe: a scoping review. Int J Environ Res Public Health. (2022) 19. doi: 10.3390/ijerph19031278
3. Bjertrup PJ, Bouhenia M, Mayaud P, Perrin C, Ben Farhat J, Blanchet K. A life in waiting: refugees’ mental health and narratives of social suffering after European Union border closures in march 2016. Soc Sci Med. (2018) 215:53–60. doi: 10.1016/j.socscimed.2018.08.040
4. El Kishawi RR, Soo KL, Abed YA, Wan Muda WAM. Obesity and overweight: prevalence and associated socio demographic factors among mothers in three different areas in the Gaza Strip-Palestine: a cross-sectional study. BMC Obes. (2014) 1:7. doi: 10.1186/2052-9538-1-7
5. UNO 2015. Transforming our World: The 2030 Agenda for Sustainable Development. Geneva: United Nations Organization (2015).
6. Amiri S. Obesity and overweight prevalence in immigration: a meta-analysis. Obesity Medicine. (2021) 22:100321. doi: 10.1016/j.obmed.2021.100321
7. Davis D, Phares CR, Salas J, Scherrer J. Prevalence of overweight and obesity in US-bound refugees: 2009–2017. J Immigrant Minor Health. (2020) 22:1111–7. doi: 10.1007/s10903-020-00974-y
8. Damiri B, Abualsoud MS, Samara AM, Salameh SK. Metabolic syndrome among overweight and obese adults in Palestinian refugee camps. Diabetol Metab Syndr. (2018) 10:34. doi: 10.1186/s13098-018-0337-2
9. Belau MH, Bassil M, Laukamp A, Kraemer A. Body mass index and associated factors among refugees living in North Rhine-Westphalia, Germany: a cross-sectional study. BMC Nutr. (2021) 7:54. doi: 10.1186/s40795-021-00453-z
10. Lane G, Vatanparast H. Immigrant families’ experience of the Canadian food and nutrition environment. Appl Physiol Nutr Metab. (2023) 48:445–54. doi: 10.1139/apnm-2022-0346
11. Gingell T, Murray K, Correa-Velez I, Gallegos D. Determinants of food security among people from refugee backgrounds resettled in high-income countries: a systematic review and thematic synthesis. PLoS One. (2022) 17:e0268830. doi: 10.1371/journal.pone.0268830
12. Holmboe-Ottesen G, Wandel M. Changes in dietary habits after migration and consequences for health: a focus on South Asians in Europe. Food and Nutrition Research. (2012) 56. doi: 10.3402/fnr.v56i0.18891
13. Lee SD, Kellow NJ, Huggins CE, Choi TST. How and why diets change post-migration: a qualitative exploration of dietary acculturation among recent Chinese immigrants in Australia. Nutrients. (2022) 14. doi: 10.3390/nu14173573
14. Sauter A, Kikhia S, Von Sommoggy J, Loss J. Factors influencing the nutritional behavior of Syrian migrants in Germany: results of a qualitative study. BMC Public Health. (2021) 21:1334. doi: 10.1186/s12889-021-11268-9
15. Wood JM, Booth AO, Margerison C, Worsley A. What factors are associated with food security among recently arrived refugees resettling in high-income countries? A scoping review. Public Health Nutr. (2021) 24:4313–27. doi: 10.1017/S1368980021002925
16. Berggreen-Clausen A, Hseing Pha S, Molsted Alvesson H, Andersson A, Daivadanam M. Food environment interactions after migration: a scoping review on low- and middle-income country immigrants in high-income countries. Public Health Nutr. (2022) 25:136–58. doi: 10.1017/S1368980021003943
17. Xanthakos SA. Nutritional deficiencies in obesity and after bariatric surgery. Pediatr Clin N Am. (2009) 56:1105–21. doi: 10.1016/j.pcl.2009.07.002
18. Via M. The malnutrition of obesity: micronutrient deficiencies that promote diabetes. ISRN Endocrinol. (2012) 2012:103472. doi: 10.5402/2012/103472
19. Al Masri F, Muller M, Straka D, Hahn A, Schuchardt JP. Nutritional and health status of adult Syrian refugees in the early years of asylum in Germany: a cross-sectional pilot study. BMC Public Health. (2022) 22:2217. doi: 10.1186/s12889-022-14684-7
20. Gregg EW, Shaw JE. Global health effects of overweight and obesity. N Engl J Med. (2017) 377:80–1. doi: 10.1056/NEJMe1706095
21. Murphy M, Robertson W, Oyebode O. Obesity in international migrant populations. Curr Obes Rep. (2017) 6:314–23. doi: 10.1007/s13679-017-0274-7
22. Westgard B, Martinson BC, Maciosek M, Brown M, Xu Z, Farah F, et al. Prevalence of cardiovascular disease and risk factors among Somali immigrants and refugees. J Immigr Minor Health. (2021) 23:680–8. doi: 10.1007/s10903-020-01078-3
23. Al-Rousan T, Alheresh R, Saadi A, El-Sabrout H, Young M, Benmarhnia T, et al. Epidemiology of cardiovascular disease and its risk factors among refugees and asylum seekers: systematic review and meta-analysis. Int J Cardiol Cardiovasc Risk Prev. (2022) 12. doi: 10.1016/j.ijcrp.2022.200126
24. Renzaho AM, Bilal P, Marks GC. Obesity, type 2 diabetes and high blood pressure amongst recently arrived Sudanese refugees in Queensland, Australia. J Immigr Minor Health. (2014) 16:86–94. doi: 10.1007/s10903-013-9791-y
25. Dookeran NM, Battaglia T, Cochran J, Geltman PL. Chronic disease and its risk factors among refugees and asylees in Massachusetts, 2001–2005. Prev Chronic Dis. (2010) 7:A51.
26. Robinson E, Haynes A, Sutin A, Daly M. Self-perception of overweight and obesity: a review of mental and physical health outcomes. Obes Sci Pract. (2020) 6:552–61. doi: 10.1002/osp4.424
27. Chao HL. Body image change in obese and overweight persons enrolled in weight loss intervention programs: a systematic review and meta-analysis. PLoS One. (2015) 10:e0124036. doi: 10.1371/journal.pone.0124036
28. Luppino FS, De Wit LM, Bouvy PF, Stijnen T, Cuijpers P, Penninx BW, et al. Overweight, obesity, and depression: a systematic review and meta-analysis of longitudinal studies. Arch Dis Child. (2010) 67:220–9. doi: 10.1001/archgenpsychiatry.2010.2
29. Amiri S, Behnezhad S. Obesity and anxiety symptoms: a systematic review and meta-analysis. Neuropsychiatry. (2019) 33:72–89. doi: 10.1007/s40211-019-0302-9
30. Smeeth D, Mcewen FS, Popham CM, Karam EG, Fayyad J, Saab D, et al. War exposure, post-traumatic stress symptoms and hair cortisol concentrations in Syrian refugee children. Mol Psychiatry. (2023) 28:647–56. doi: 10.1038/s41380-022-01859-2
31. Mulugeta W, Xue H, Glick M, Min J, Noe MF, Wang YF. Burden of mental illness and non-communicable diseases and risk factors for mental illness among refugees in Buffalo, NY, 2004–2014. J Racial Ethn Health Disparities. (2019) 6:56–63. doi: 10.1007/s40615-018-0498-6
32. Geiker NRW, Astrup A, Hjorth MF, Sjodin A, Pijls L, Markus CR. Does stress influence sleep patterns, food intake, weight gain, abdominal obesity and weight loss interventions and vice versa? Obes Rev. (2018) 19:81–97. doi: 10.1111/obr.12603
33. Anandacoomarasamy A, Fransen M, March L. Obesity and the musculoskeletal system. Curr Opin Rheumatol. (2009) 21:71–7. doi: 10.1097/BOR.0b013e32831bc0d7
34. Forhan M, Gill SV. Obesity, functional mobility and quality of life. Best Pract Res Clin Endocrinol Metab. (2013) 27:129–37. doi: 10.1016/j.beem.2013.01.003
35. Brewis A, Trainer S, Han S, Wutich A. Publically misfitting: extreme weight and the everyday production and reinforcement of felt stigma. Med Anthropol Q. (2017) 31:257–76. doi: 10.1111/maq.12309
36. Schuster RC, Han SY, Brewis AA, Wutich A. Increasing overweight and obesity erodes engagement in one’s neighborhood by women, but not men. Prev Med Rep. (2018) 10:144–9. doi: 10.1016/j.pmedr.2018.02.013
37. Hunter P. The refugee crisis challenges national health care systems: countries accepting large numbers of refugees are struggling to meet their health care needs, which range from infectious to chronic diseases to mental illnesses. EMBO Rep. (2016) 17:492–5. doi: 10.15252/embr.201642171
38. Shortland T, Mcgranahan M, Stewart D, Oyebode O, Shantikumar S, Proto W, et al. A systematic review of the burden of, access to services for and perceptions of patients with overweight and obesity, in humanitarian crisis settings. PLoS One. (2023) 18:e0282823. doi: 10.1371/journal.pone.0282823
39. Boggs D, Atijosan-Ayodele O, Yonso H, Scherer N, O'fallon T, Deniz G, et al. Musculoskeletal impairment among Syrian refugees living in Sultanbeyli, Turkey: prevalence, cause, diagnosis and need for related services and assistive products. Confl Health. (2021) 15:29. doi: 10.1186/s13031-021-00362-9
40. Renzaho AM, Halliday JA, Mellor D, Green J. The healthy migrant families initiative: development of a culturally competent obesity prevention intervention for African migrants. BMC Public Health. (2015) 15:272. doi: 10.1186/s12889-015-1628-2
41. Amstutz D, Goncalves D, Hudelson P, Stringhini S, Durieux-Paillard S, Rolet S. Nutritional status and obstacles to healthy eating among refugees in Geneva. J Immigr Minor Health. (2020) 22:1126–34. doi: 10.1007/s10903-020-01085-4
42. Burn NL, Weston M, Maguire N, Atkinson G, Weston KL. Effects of workplace-based physical activity interventions on cardiorespiratory fitness: a systematic review and meta-analysis of controlled trials. Sports Med. (2019) 49:1255–74. doi: 10.1007/s40279-019-01125-6
43. Lin X, Zhang X, Guo J, Roberts CK, Mckenzie S, Wu WC, et al. Effects of exercise training on cardiorespiratory fitness and biomarkers of cardiometabolic health: a systematic review and meta-analysis of randomized controlled trials. J Am Heart Assoc. (2015) 4:e002014. doi: 10.1161/JAHA.115.002014
44. Barry VW, Baruth M, Beets MW, Durstine JL, Liu J, Blair SN. Fitness vs. Fatness on all-cause mortality: a meta-analysis. Prog Cardiovasc Dis. (2014) 56:382–90. doi: 10.1016/j.pcad.2013.09.002
45. Fogelholm M. Physical activity, fitness and fatness: relations to mortality, morbidity and disease risk factors. A systematic review. Obes Rev. (2009) 11:202–21. doi: 10.1111/j.1467-789X.2009.00653.x
46. Caspersen CJ, Powell KE, Christenson GM. Physical activity, exercise, and physical fitness: defitions and distinctions for health-related research. Public Health Rep. (1985) 100:126–31.
47. Larose J, King J, Brosseau L, Wells GA, Reid R, Maetzel A, et al. The effect of walking on cardiorespiratory fitness in adults with knee osteoarthritis. Appl Physiol Nutr Metabolism. (2013) 38:886–91. doi: 10.1139/apnm-2012-0487
48. Moller NC, Ostergaard L, Gade JR, Nielsen JL, Andersen LB. The effect on cardiorespiratory fitness after an 8-week period of commuter cycling–a randomized controlled study in adults. Prev Med. (2011) 53:172–7. doi: 10.1016/j.ypmed.2011.06.007
49. Cornelissen VA, Smart NA. Exercise training for blood pressure: a systematic review and meta-analysis. J Am Heart Assoc. (2013) 2:e004473. doi: 10.1161/JAHA.112.004473
50. Bird SR, Hawley JA. Update on the effects of physical activity on insulin sensitivity in humans. BMJ Open Sport and Exercise Medicine. (2016) 2:e000143. doi: 10.1136/bmjsem-2016-000143
51. Bellicha A, Van Baak MA, Battista F, Beaulieu K, Blundell JE, Busetto L, et al. Effect of exercise training on weight loss, body composition changes, and weight maintenance in adults with overweight or obesity: an overview of 12 systematic reviews and 149 studies. Obes Rev. (2021) 22:e13256. doi: 10.1111/obr.13256
52. Luzak A, Karrasch S, Thorand B, Nowak D, Holle R, Peters A, et al. Association of physical activity with lung function in lung-healthy German adults: results from the KORA FF4 study. BMC Pulm Med. (2017) 17:215. doi: 10.1186/s12890-017-0562-8
53. Gerber M, Börjesson M, Ljung T, Lindwall M, Jonsdottir I. Fitness moderates the relationship between stress and cardiovascular risk factors. Med Sci Sports Exercise. (2016) 48:2075–81. doi: 10.1249/MSS.0000000000001005
54. Mücke M, Ludyga S, Colledge F, Gerber M. Influence of regular physical activity and fitness on stress reactivity as measured with the trier social stress test protocol: a systematic review. Sports Med. (2018) 48:2607–22. doi: 10.1007/s40279-018-0979-0
55. Hainer V, Toplak H, Stich V. Fat or fit: what is more important? Diabetes Care. (2009) 32:S392–7. doi: 10.2337/dc09-S346
56. Nuttall FQ. Body mass Index: obesity, BMI, and health: a critical review. Nutr Today. (2015) 50:117–28. doi: 10.1097/NT.0000000000000092
57. Buss J. Limitations of body mass index to assess body fat. Workplace Health Saf. (2014) 62:264. doi: 10.1177/216507991406200608
58. Turk Y, Theel W, Kasteleyn MJ, Franssen FME, Hiemstra PS, Rudolphus A, et al. High intensity training in obesity: a meta-analysis. Obes Sci Pract. (2017) 3:258–71. doi: 10.1002/osp4.109
59. Duncan GE. The “fit but fat” concept revisited: population-based estimates using NHANES. Int J Behav Nutr Phys Act. (2010) 7:47. doi: 10.1186/1479-5868-7-47
60. Guerin PB, Elmi FH, Corrigan C. Body composition and cardiorespiratory fitness among refugee Somali women living in New Zealand. J Immigr Minor Health. (2007) 9:191–6. doi: 10.1007/s10903-006-9030-x
61. Knappe F, Colledge F, Gerber M. Impact of an 8-week exercise and sport intervention on post-traumatic stress disorder symptoms, mental health, and physical fitness among male refugees living in a Greek refugee camp. Int J Environ Res Public Health. (2019) 16. doi: 10.3390/ijerph16203904
62. Sundquist J, Hagstromer M, Johansson SE, Sundquist K. Effect of a primary health-care-based controlled trial for cardiorespiratory fitness in refugee women. BMC Fam Pract. (2010) 11:55. doi: 10.1186/1471-2296-11-55
63. Yoshino Y, Sato M, Abu-Siam I, Khost N, Honda S, Qarawi AT, et al. Assessment of physical activity and its facilitators and barriers among Syrian refugees living in Amman City, Jordan: a cross-sectional study. BMC Public Health. (2022) 22:1732. doi: 10.1186/s12889-022-14064-1
64. Chen SQ, Knoll M. Perceived environmental barriers and facilitators of refugee children’s physical activity in/around refugee accommodation: a qualitative case study in Berlin. Arch Public Health. (2022) 80:242. doi: 10.1186/s13690-022-00993-1
65. Gerber M, Colledge F, De Quervain D, Filippou K, Havas E, Knappe F, et al. Effects of an exercise and sport intervention among refugees living in a Greek refugee camp on mental health, physical fitness and cardiovascular risk markers: study protocol for the SALEEM pragmatic randomized controlled trial. Trials. (2021) 22. doi: 10.1186/s13063-021-05808-2
66. Ostchega Y, Nwankwo T, Sorlie PD, Wolz M, Zipf G. Assessing the validity of the Omron HEM-907XL oscillometric blood pressure measurement device in a national survey environment. J Clin Hypertens. (2009) 12:22–8. doi: 10.1111/j.1751-7176.2009.00199.x
67. Abbai NS, Nyirenda M, Reddy T, Ramjee G. Good correlation between the afinion AS100 analyser and the ABX pentra 400 analyser for the measurement of glycosylated haemoglobin and lipid levels in older adults in Durban, South Africa. S Afr Med J. (2018) 108:50–5. doi: 10.7196/SAMJ.2017.v108i1.12548
68. Foerster V, Severn M. Point-of-care glycated hemoglobin testing to diagnose type 2 diabetes. CADTH Issues in Emerging Health Technol. (2016) 156:1–8. doi: 10.3389/fpubh.2024.1438945
69. Brouwer N, Van Pelt J. Validation and evaluation of eight commercially available point of care CRP methods. Clin Chim Acta. (2015) 439:195–201. doi: 10.1016/j.cca.2014.10.028
70. Åstrand P-O, Rodahl K, Dahl H, Strømme SB. Textbook of Work Physiology, Champaign. Champaign: Human Kinetics (2003).
71. Buono MJ, Roby JJ, Micale FG, Sallis JF. Predicting maximal oxygen uptake in children: modification of the astrand-ryhming test. Pediatr Exerc Sci. (1989) 1:278–83. doi: 10.1123/pes.1.3.278
72. Morina N, Ehring T, Priebe S. Diagnostic utility of the impact of event scale—revised in two sample of survivors of war. PLoS One. (2013) 8. doi: 10.1371/journal.pone.0083916
73. Feyera F, Mihretie G, Bedaso A, Gedle D, Kumera G. Prevalence of depression and associated factors among Somali refugee at Melkadida camp, southeast Ethiopia: a cross-sectional study. BMC Psychiatry. (2015) 15. doi: 10.1186/s12888-015-0539-1
74. Hermansson AC, Thyberg M, Timpka T, Gerdle B. Survival with pain: an eight-year follow-up of war-wounded refugee. Med. Confl Surviv. (2001) 17:102–11. doi: 10.1080/13623690108409564
75. Weiss DS, Marmar CR. The impact of event scale—revised. In: Wilson JP, Keane TM, editors. Assessing Psychological Trauma and PTSD. New York: Guilford Press (1997). p. 399–411.
76. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders 5 (DSM-5). Washington: APA (2013).
77. WHO. ICD-10: International Statistical Classification of Diseases and Related Health Problems: Tenth Revision, 2nd ed. World Health Organization. Geneva: World Health Organization (2004).
78. Kroenke K, Spitzer RL. The PHQ-9: a new depression diagnostic and severity measure. Psychiatr Ann. (2002) 32:509–15. doi: 10.3928/0048-5713-20020901-06
79. Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. (2006) 166:1092–7. doi: 10.1001/archinte.166.10.1092
80. Carlsson AM. Assessment of chronic pain. I. Aspects of the reliability and validity of the visual analogue scale. Pain. (1983) 16:87–101. doi: 10.1016/0304-3959(83)90088-X
81. Blom EH, Bech P, HöGberg G, Larsson JO, Serlachius E. Screening for depressed mood in an adolescent psychiatric context by brief self- assessment scales—testing psychometric validity of WHO-5 and BDI-6 indices by latent trait analyses. Health Qual Life Outcomes. (2012) 10:149. doi: 10.1186/1477-7525-10-149
82. WHO. Wellbeing Measures in Primary Health Care/the DepCare Project. Report on a wHO Meeting: Stockholm, Sweden, 12–13 February 1998: Regional Office for Europe. Geneva: World Health Organization (1998).
83. West SG, Finch JF, Curran PJ. Structural equation models with nonnormal variables: problems and remedies. In: Hoyle RH, editor. Structural Equation Modeling. Concepts, Issues, and Applications. Thousand Oakes: Sage (1995). p. 56–75.
84. ACSM. ACSM’s Guidelines for Exercise Testing and Prescription, Philadelphia. Philadelphia: Lippincott Williams & Wilkins (2010).
86. Grijalva-Eternod CS, Wells JC, Cortina-Borja M, Salse-Ubach N, Tondeur MC, Dolan C, et al. The double burden of obesity and malnutrition in a protracted emergency setting: a cross-sectional study of Western Sahara refugees. PLoS Med. (2012) 9:e1001320. doi: 10.1371/journal.pmed.1001320
87. Magriplis E, Dimakopoulos I, Karageorgou D, Mitsopoulou AV, Bakogianni I, Micha R, et al. Aims, design and preliminary findings of the hellenic national nutrition and health survey (HNNHS). BMC Med Res Methodol. (2019) 19:37. doi: 10.1186/s12874-018-0655-y
88. Aune D, Sen A, Prasad M, Norat T, Janszky I, Tonstad S, et al. BMI And all cause mortality: systematic review and non-linear dose-response meta-analysis of 230 cohort studies with 3.74 million deaths among 30.3 million participants. Br Med J. (2016) 353:i2156. doi: 10.1136/bmj.i2156
89. Tovar A, Renzaho AM, Guerrero AD, Mena N, Ayala GX. A systematic review of obesity prevention intervention studies among immigrant populations in the US. Curr Obes Rep. (2014) 3:206–22. doi: 10.1007/s13679-014-0101-3
90. Wang Y, Cai L, Wu Y, Wilson RF, Weston C, Fawole O, et al. What childhood obesity prevention programmes work? A systematic review and meta-analysis. Obes Rev. (2015) 16:547–65. doi: 10.1111/obr.12277
91. Brown HE, Atkin AJ, Panter J, Wong G, Chinapaw MJ, Van Sluijs EM. Family-based interventions to increase physical activity in children: a systematic review, meta-analysis and realist synthesis. Obes Rev. (2016) 17:345–60. doi: 10.1111/obr.12362
92. Kodama S, Saito K, Tanaka S, Maki M, Yachi Y, Asumi M, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA. (2009) 301:2024–35. doi: 10.1001/jama.2009.681
93. Carrard J, Guerini C, Appenzeller-Herzog C, Infanger D, Konigstein K, Streese L, et al. The metabolic signature of cardiorespiratory fitness: a systematic review. Sports Med. (2022) 52:527–46. doi: 10.1007/s40279-021-01590-y
94. Wang CY, Haskell WL, Farrell SW, Lamonte MJ, Blair SN, Curtin LR, et al. Cardiorespiratory fitness levels among US adults 20–49 years of age: findings from the 1999–2004 national health and nutrition examination survey. Am J Epidemiol. (2010) 171:426–35. doi: 10.1093/aje/kwp412
95. Sun X, Yan N, Peng W, Nguyen TT, Ma L, Wang Y. Association between body mass index and body fat measured by dual-energy x-ray absorptiometry (DXA) in China: a systematic review and meta-analysis. Glob Health J. (2023) 7:61–9. doi: 10.1016/j.glohj.2023.03.001
96. Tomlinson DJ, Erskine RM, Morse CI, Winwood K, Onambele-Pearson G. The impact of obesity on skeletal muscle strength and structure through adolescence to old age. Biogerontology. (2016) 17:467–83. doi: 10.1007/s10522-015-9626-4
97. Leggio M, Lombardi M, Caldarone E, Severi P, D'emidio S, Armeni M, et al. The relationship between obesity and hypertension: an updated comprehensive overview on vicious twins. Hypertens Res. (2017) 40:947–63. doi: 10.1038/hr.2017.75
98. Klop B, Elte JW, Cabezas MC. Dyslipidemia in obesity: mechanisms and potential targets. Nutrients. (2013) 5:1218–40. doi: 10.3390/nu5041218
99. Hu S, Lin C, Cai X, Li Z, Lv F, Yang W, et al. Trends in baseline HbA1c and body-mass index in randomised placebo-controlled trials of type 2 diabetes from 1987 to 2022: a systematic review and meta-analysis. EClinicalMedicine. (2023) 57:101868. doi: 10.1016/j.eclinm.2023.101868
100. Santa-Paavola R, Lehtinen-Jacks S, Jaaskelainen T, Mannisto S, Lundqvist A. The association of high-sensitivity C-reactive protein with future weight gain in adults. Int J Obes. (2022) 46:1234–40. doi: 10.1038/s41366-022-01101-7
101. Adhikary D, Barman S, Ranjan R, Stone H. A systematic review of major cardiovascular risk factors: a growing global health concern. Cureus. (2022) 14:e30119. doi: 10.7759/cureus.30119
102. Khanna D, Peltzer C, Kahar P, Parmar MS. Body mass Index (BMI): a screening tool analysis. Cureus. (2022) 14:e22119. doi: 10.7759/cureus.22119
103. Masood M, Aggarwal A, Reidpath DD. Effect of national culture on BMI: a multilevel analysis of 53 countries. BMC Public Health. (2019) 19:1212. doi: 10.1186/s12889-019-7536-0
104. Dang HA, Verme P. Estimating poverty for refugees in data-scarce contexts: an application of cross-survey imputation. J Popul Econ. (2023) 36:653–79. doi: 10.1007/s00148-022-00909-x
105. Haapala EA, Lee E, Karppinen J, Skog H, Valtonen M, Kujala UM, et al. Associations of cardiorespiratory fitness, body composition, and blood pressure with arterial stiffness in adolescent, young adult, and middle-aged women. Sci Rep. (2022) 12:21378. doi: 10.1038/s41598-022-25795-x
106. Laukkanen JA, Kurl S, Voutilainen A, Makikallio T, Kunutsor SK. Cardiorespiratory fitness, inflammation, and risk of sudden cardiac death in middle-aged men. Am J Cardiol. (2022) 174:166–71. doi: 10.1016/j.amjcard.2022.03.032
107. Qiu SH, Cai X, Yang BQ, Du ZW, Cai M, Sun ZL, et al. Association between cardiorespiratory fitness and risk of type 2 diabetes: a meta-analysis. Obesity. (2019) 27:315–24. doi: 10.1002/oby.22368
108. Mills SEE, Nicolson KP, Smith BH. Chronic pain: a review of its epidemiology and associated factors in population-based studies. Br J Anaesth. (2019) 123:e273–83. doi: 10.1016/j.bja.2019.03.023
Keywords: cardiovascular risk factors, fitness, mental health, moderation, refugees
Citation: Gerber M, Filippou K, Knappe F, Morres ID, Tzormpatzakis E, Havas E, Seelig H, Colledge F, Ludyga S, Meier M, Theodorakis Y, von Känel R, Pühse U and Hatzigeorgiadis A (2024) Does cardiorespiratory fitness moderate the relationship between overweight, cardiovascular risk markers and mental health among forcibly displaced individuals living in a Greek refugee camp?. Front. Sports Act. Living 6:1334230. doi: 10.3389/fspor.2024.1334230
Received: 6 November 2023; Accepted: 30 September 2024;
Published: 21 October 2024.
Edited by:
Stefano Orlando, University of Rome Tor Vergata, ItalyReviewed by:
Fausto Ciccacci, Saint Camillus International University of Health and Medical Sciences, ItalyClaudia Mosconi, University of Rome Tor Vergata, Italy
Copyright: © 2024 Gerber, Filippou, Knappe, Morres, Tzormpatzakis, Havas, Seelig, Colledge, Ludyga, Meier, Theodorakis, von Känel, Pühse and Hatzigeorgiadis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Markus Gerber, bWFya3VzLmdlcmJlckB1bmliYXMuY2g=