
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Sports Act. Living , 08 April 2024
Sec. Exercise Physiology
Volume 6 - 2024 | https://doi.org/10.3389/fspor.2024.1271987
 Yosuke Ishii1*Saeko Okamoto1Riko Okinaka1Takato Hashizume1Chen Xu1Kexin Zhu1Yuko Nakashima2Kaoru Okada3Kazuya Takagi3Nobuo Adachi2Makoto Takahashi1
Yosuke Ishii1*Saeko Okamoto1Riko Okinaka1Takato Hashizume1Chen Xu1Kexin Zhu1Yuko Nakashima2Kaoru Okada3Kazuya Takagi3Nobuo Adachi2Makoto Takahashi1
Purpose: Excessive mechanical stress accumulates and causes knee injury. Meniscal extrusion is a key factor in detecting the reaction to cumulative mechanical stress. The accumulation of stress strongly depends on environmental conditions such as flat ground or uphill/downhill, and accumulates in knee compartments; only a few studies have reported the effects of different environments on lateral and medial meniscus extrusion. This study aimed to investigate the effects of cumulative uphill/downhill stress on the meniscal extrusion in each compartment.
Methods: A total of 30 healthy volunteers with 30 affected knees were involved in this cohort study (mean age, 22.0 ± 1.1 years; men, n = 14). The participants were divided into flat-walking, uphill/downhill-walking, and uphill/downhill-jogging groups and their numbers of steps taken were recorded during the effort. Moreover, medial and lateral meniscal extrusions during walking were evaluated using ultrasound three times, before and after efforts (T1) and (T2), and one day after efforts (T3), respectively.
Results: In the flat-walking group, no significant differences were observed between the follow-up periods. Conversely, in the uphill/downhill-walking and jogging groups, the medial meniscus extrusion at T2 was significantly higher than that at T1. Conversely, the medial meniscus extrusion at T3 was significantly lower than that at T2. By contrast, the lateral meniscus did not show any difference between the follow-up periods in any group.
Conclusion: Temporary extrusion of the meniscus occurred after uphill/downhill tasks in healthy volunteers, and its reaction was observed only in the medial meniscus.
Cartilage homeostasis maintains the appropriate balance between mechanical and metabolic stresses in healthy individuals. However, taxing activities, including sports, can cause extreme mechanical stress and distraction of homeostasis (1, 2). Cumulative mechanical stress is believed to affect structural changes in the knee compartment, resulting in knee injuries and overwork lesions, eventually leading to the onset of knee osteoarthritis (OA) (3, 4). Therefore, the detection of abnormal cumulative mechanical stress at an early stage is required to appropriately manage the prevention of lesions in the knee.
The meniscus absorbs shock and protects the knee cartilage (5). However, meniscal extrusion associated with dysfunction leads to the aggravation of the cartilage, resulting in knee pain and OA progression (6–8); therefore, it is recognized as the target factor for clinicians. By contrast, even healthy volunteers show temporary meniscus extrusion after marathons, which correlates with the amount of cumulative mechanical stress (9, 10). Furthermore, meniscus extrusion is observed to be highly sensitive to the cumulative stresses, including the repetition steps, rather than the peak value of mechanical stress (10). Therefore, meniscal extrusion can detect cumulative mechanical stress and is an indicator for the individual knee status.
However, the level of mechanical stress varies depending on environmental factors, including flat and uphill/downhill conditions (11, 12), and it is speculated that the cumulative stress can cause the reaction of the meniscus. Moreover, these stresses affect not only the medial compartment, but also the lateral side (13). However, only a few studies have reported the effects of different environmental factors on lateral and medial meniscus extrusion (MME). Addressing this knowledge gap could help establish appropriate management strategies for individual knees, potentially prolonging the duration of healthy athletic performance by preventing certain injuries. This study aimed to investigate the effects of cumulative uphill/downhill stress on the meniscal extrusion in each compartment. It was hypothesized that both menisci presented more extrusion in the uphill/downhill conditions.
Altogether 30 healthy volunteers with 30 asymptomatic knees were involved in this study [mean age, 22.0 ± 1.1 years; body mass index (BMI), 21.3 ± 2.1; men, n = 14]. The index knee was selected randomly for each participant. The participants included both runners and those engaged in recreational sport activities once a week as a habit, with no history of leg pain at least for 6 months. By contrast, participants were excluded based on the following criteria: (1) history of knee injury and surgical interventions, (2) chronic pain, and (3) experience of sports activity on the previous day. Hence, it is necessary to control the factors that affect the impact of participants’ performance and reaction to the meniscus. The demographic data are provided in Table 1.

Table 1. Participant characteristics.
The evaluation was based on follow-up tests performed three times, including pre-effort (T1), post-effort (T2), and one day after effort (T3). This study followed an established protocol based on a previous study on the effects of mechanical stress on meniscal extrusion (10). Moreover, the effort time was observed between T1 and T2. The participants were instructed to avoid exercises such as sports and training that would affect the meniscus conditions during the study.
All participants wore the same type of shoe (ME-WE432, Boston, MA, USA), according to their foot size, to minimize biases from the shoe properties on mechanical stress. The tasks were selected randomly by walking on a flat or uphill/downhill course, or jogging on an uphill/downhill course, and the participants were divided into flat-walking, uphill/downhill-walking, and uphill/downhill-jogging groups. In particular, the uphill and downhill terrain has an altitude of 70 m. The tasks covered a distance of 5 km and were performed at comfortable speeds.
During some tasks, activity levels were measured using specialized watches (ForeAthlete 55, Taipei, Taiwan). This device was wrapped around each participant's wrist and recorded data, including steps, pitch, and length during the effort. Subjective fatigue was immediately evaluated using the visual analog scale (VAS) after efforts. These parameters were compared among the different types of efforts.
The meniscus was evaluated using ultrasonography (SNiBLE, KONICA MINOLTA, Japan) with a prototype 3–11 MHz special linear-array transducer. T2 was performed immediately after the participants returned from the load course to our lab. During the measurement, the longitudinal transducer was placed on both medial and lateral joint spaces, and the triangular meniscus appeared as an echogenic structure between the femoral condyle and the tibial plateau, respectively. Appropriate images were determined based on specific landmarks, and the medial and lateral sides were determined as clear visualizations of the medial collateral ligament or origin of the popliteal tendon, based on a previous study (14, 15) (Figure 1).
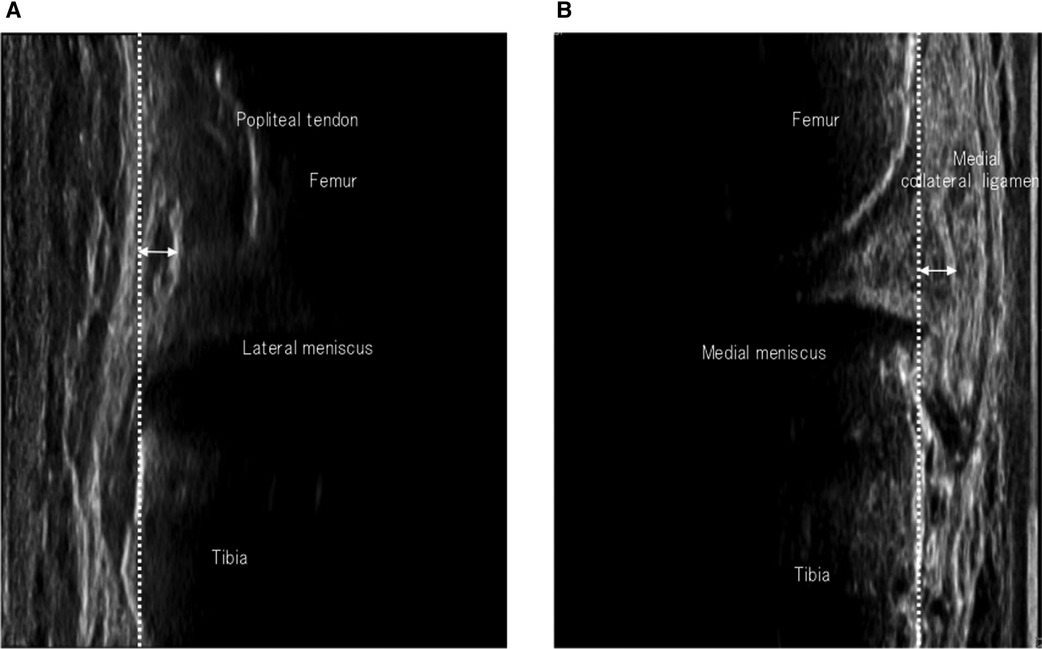
Figure 1. Images of meniscus extrusion. Coronal images of the lateral (A) and medial menisci (B). The reference lines according to the tibial plate and the distance of the meniscal extrusion are shown as dashed and arrowed lines, respectively.
The transducer was fixed using a flexible band that enabled comfortable walking. The video mode of the ultrasonography with a sampling rate of 30 Hz was recorded during walking, and an image of the meniscus was obtained. This ultrasonographic measurement was performed simultaneously with a wearable sensor using the outside signal of the device. Kinovea software (v0.8.15; Kinovea open-source project, www.kinovea.org) was used to adjust the match to the required sampling frequency.
The meniscus extrusion was defined as the quantitative value of expansion to the line of the tibial cortex. This process obtained approximately 20 images in a single trial and generated the waveform of the meniscal extrusion using the continual values of the extrusion of the meniscus. The maximum point was detected and used as a representative value for meniscal extrusion (Figure 2). These methods have been established as having high reliability in previous studies (14, 15). Moreover, the values were calculated as Δ-value based on the difference in meniscus extrusion between (T1) and (T2).
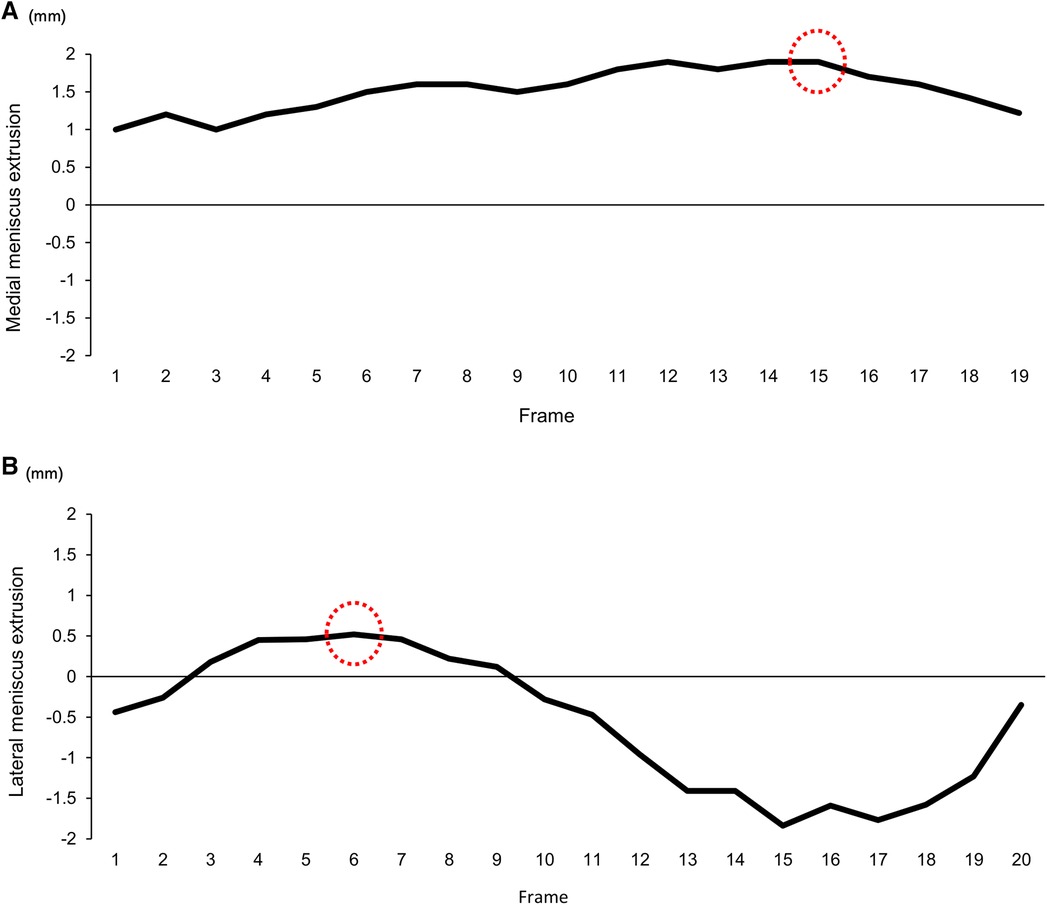
Figure 2. The waveform of meniscus extrusion during walking. A representative image of the waveform on the extrusion meniscus during walking shows the (A) medial and (B) lateral side. These waveforms were structured based on the value of the meniscus extrusion, obtaining approximately 20 continuous images. The red dot circle shows the point of the maximum value of meniscal extrusion.
In this study, a single wearable sensor including an acceleration sensor and gyroscope with rate of 100 Hz (WAA-010, ATR-Promotions, Japan) evaluated the participant's gait form. The sensor was fixed to the midpoint between the lateral tibial plateau and the head of the fibula using a belt. In particular, the sensors were carefully attached to the shank longitudinally. Joint axes showed y-axis orientation in the vertical direction and x- and z-axes in the anteroposterior and mediolateral directions (Figure 3).
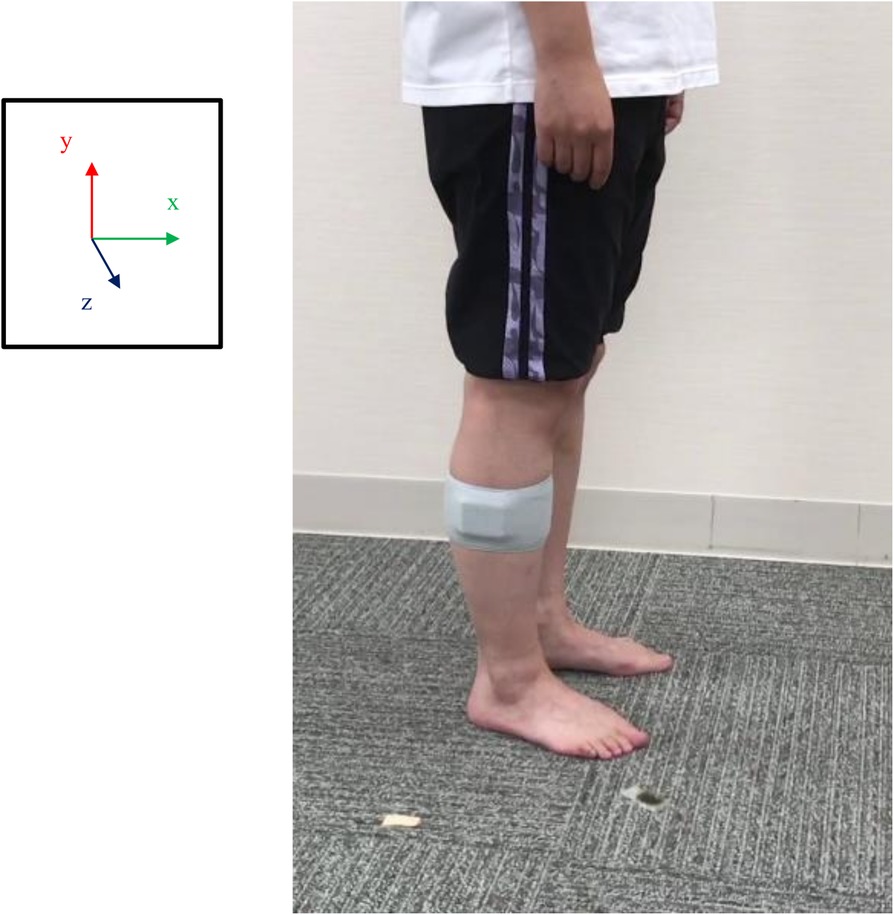
Figure 3. The location of the attached acceleration sensors. A view of the acceleration sensor attached to the shank is presented. The sensors were carefully attached to the shank on the longitudinal axis, with the midpoint between the lateral tibial plateau and the head of the fibula. The origin of the sensors was the y-axis oriented in the vertical direction and the x- and z-axes in the anteroposterior and mediolateral directions, respectively.
The participants were instructed to walk along a 10-m walkway three times. The analysis interval was set in the single-stance phase of a gait cycle and did not include gait initiation or termination. The gait event of the single-stance phase from heel contact to foot-off was estimated using the mediolateral angular velocity negative peaks, following a previous study (16). The video data were also obtained simultaneously and visually confirmed the gait events to obtain the minimum measurement error. During the analysis, raw data were filtered through a low-pass until reaching a 10 Hz cut-off, and peak values that can estimate gait events were detected using MATLAB software (MATLAB 2015a, MathWorks, Japan). Moreover, the perturbation of the shank accelerations in each direction during the stance phase was represented as root mean square (RMS), and a high value shows greater perturbation during walking. These protocols were based on a pilot study to confirm intraclass correlation coefficients (ICC), in which the RMS value was compared between test and re-test in six participants (x_ICC: 0.83, y_ICC: 0.9, z_ICC: 0.81).
Shapiro–Wilk test was used to confirm the data with or without normality. Within the group or follow-ups, VAS score, meniscus data, and walking parameters including activity and shank RMS were analyzed by multiple comparisons with the Bonferroni correction or Dunn test. The software Statistical Package for the Social Sciences (SPSS) (v23, IBM, Japan) was used to determine the critical p-value for statistical significance (p < 0.05).
Moreover, power analyses were performed as a post-hoc test to confirm the hypothesis using G-power. The differences in MME were compared between T1 and T2 in the uphill/downhill condition, and the effect size and power were 1.51 and 0.98, and 0.94 and 0.75 in the walking and jogging task, respectively.
The demographic data are provided in Table 1. No significant differences were observed between the groups. The average number of steps and the duration of effort in the flat and uphill/downhill-walking groups were significantly higher than that in uphill/downhill-jogging group. However, the pitch in uphill/downhill-jogging group was significantly higher than those in the flat and uphill/downhill-walking groups (Table 2).
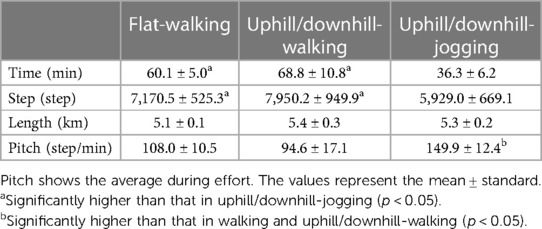
Table 2. The comparisons among activities during efforts.
In the uphill/downhill-walking and jogging groups, the MME at T2 was significantly higher than that at T1. Conversely, the MME at T3 was significantly lower than that at T2 (Figure 4A). The Δ-values in the uphill/downhill-walking and jogging were significantly higher than those in flat-waking (flat-walking: 0.1 ± 0.1, uphill/downhill-walking: 0.3 ± 0.2, uphill/downhill-jogging: 0.4 ± 0.3; flat-walking–uphill/downhill-walking: r = 1.52, flat-walking–uphill/downhill-jogging: r = 1.39, uphill/downhill-walking–uphill/downhill-jogging: r = 0.29).
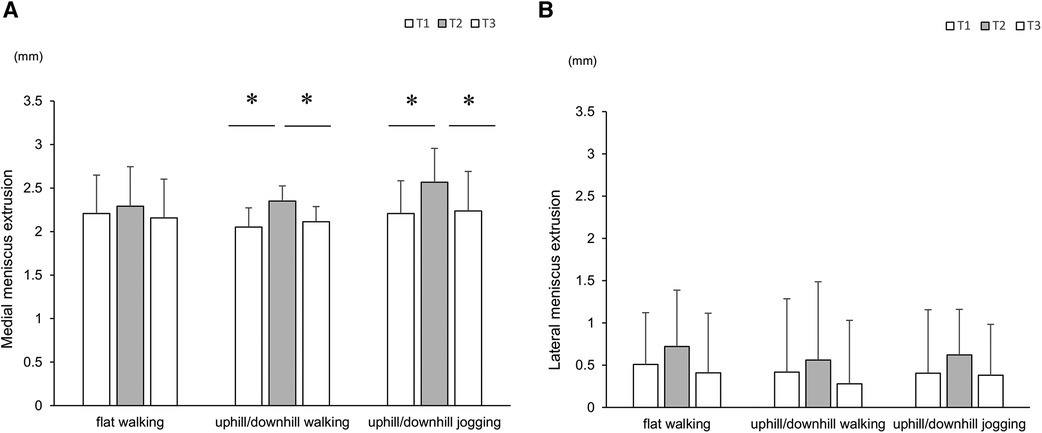
Figure 4. Comparisons of meniscus extrusion with time course. Plots showing the medial (A) and lateral menisci (B) These values are expressed as mean ± standard deviation. * indicates a significant difference between follow-up visits (p < 0.05).
In all groups, the lateral meniscus extrusions at T2 were higher than those at T1, although there were no significant differences (Figure 4B). Moreover, the Δ-value was not statistically significant among groups (flat-walking: 0.2 ± 0.3, uphill/downhill-walking: 0.1 ± 0.5, uphill/downhill-jogging: 0.2 ± 0.8).
On the medial side, in the flat-walking group, the RMS of the anteroposterior direction was significantly higher at T2 than at T1, and the reaction remained at T3. Moreover, the RMS of the mediolateral direction was significantly higher at T3 when compared with that in T2. In the uphill/downhill-walking and jogging groups, the RMS values of the anteroposterior directions were significantly higher at T3 than those at T2 (Table 3).
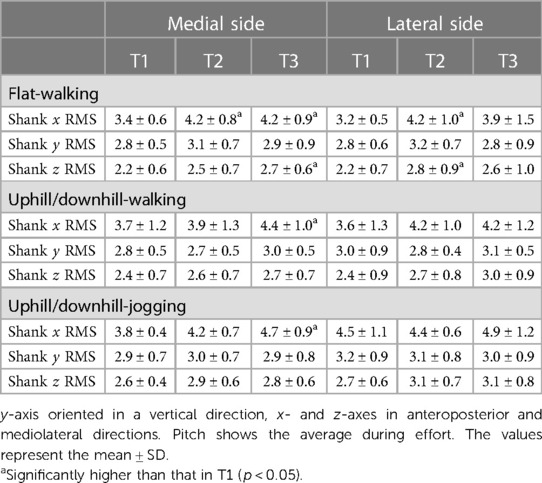
Table 3. Correlation of gait form follow-up.
On the lateral side, in the flat-walking group, the RMS values in the anteroposterior and mediolateral directions were significantly higher at T2 than at T1 (Table 3).
In all groups, the stance time of the gait cycle was not significantly different between the follow-ups. Moreover, RMS and stance time had no significant correlation with Δ-value on both the medial and lateral sides.
The values of the VAS were 32.1 ± 24.7 mm, 36.1 ± 16.8 mm, and 79.1 ± 9.2 mm in the flat-walking and the uphill/downhill-walking and jogging groups, respectively. The VAS scores in the uphill/downhill-jogging group were higher than those in the flat and uphill/downhill-walking groups. However, there was no correlation with Δ-value in any group.
The findings showed the effect of the uphill/downhill effort on the meniscus and temporary increase in meniscal extrusion, especially on the medial meniscus.
In this study, the participants performed tasks of the same length but with different time durations, steps, and pitches. However, these features were not directly related to meniscal reactions that revealed extrusion only in the uphill/downhill effort. Therefore, the uphill/downward motion itself could be a factor that affects meniscal extrusion, which partially supports the hypothesis. Greater meniscal extrusion correlates with concentrated mechanical stress in the knee compartment (8, 14, 17), and a previous study demonstrated a correlation between the amount of cumulative moment and aggravation of meniscal extrusion (10). In particular, the knee joint is strongly affected by the environment in which a high moment occurs during walking in uphill/downhill conditions rather than flat conditions (11, 12). These previous studies explain the finding that meniscal extrusion temporarily expands with greater mechanical stress.
The reaction of the meniscus on the knee compartment was observed on the medial side but not on the lateral side. A previous study investigated the amount of loading stress in each knee compartment and demonstrated that it occupied the medial compartment superiorly during walking or downhill-walking (12). Thus, it can be concluded that walking and uphill/downhill tasks mainly involve loading stress on the medial compartment and predominantly work on the medial meniscus. By contrast, the lateral meniscus shows a physiological intrusion within the tibial plateau (18) and the dynamics of drawing to the tibial plateau during walking have been observed (15). Gokkus et al. reported the relationship between the amount of meniscal extrusion and the stress distribution pattern of the meniscus using finite-element analysis. Their results showed that the meniscus experienced high mechanical stress depending on the location of the extrusion on the tibial plateau (19). In this study, the lateral meniscus showed similar dynamics and had a small extrusion value compared with the medial meniscus. Therefore, it can be concluded that the lateral meniscus may experience insufficient mechanical stress to detect changes in its location. Based on these results and those of previous studies, the medial meniscus could be concluded to serve as an indicator to reflect the cumulative mechanical stress in a knee joint.
In the present study, meniscal extrusion was caused by walking. Unfortunately, the RMS in the anterior–posterior direction was greater even after efforts according to the reaction of the MME. Thus, concerns may be raised that the change in gait form affects the meniscal extrusion rather than the cumulative mechanical stress. In the extrusion of the medial meniscus during walking, a previous study showed a significant correlation with the peak value of the knee vertical direction on the ground reaction force in healthy volunteers (14). In this study, the RMS in the vertical direction, which is associated with the ground reaction force, did not change during follow-up. Moreover, the RMS did not significantly correlate with the MME. A previous study and its findings suggest that the changes in gait form itself did not directly affect MME.
The subjective assessment did not show a significant difference between the flat and uphill/downhill-walking tasks, whereas the MME was only increased after the uphill/downhill-walking. Thus, exercise intensity obtained as a subjective assessment could not be adopted to prevent knee lesions associated with greater mechanical stress. In young athletes, medial meniscal extrusion is present and is associated with joint abnormalities such as meniscal tears and effusion; however, they do not suffer from knee pain and have no history of knee problems (20).Hence, based on several studies, a greater MME is known to be a risk factor for cartilage lesions and knee OA (7, 21). These studies support the fact that overload or diseases or injuries occur unconsciously. Thus, the findings and those of previous studies emphasize that it is necessary not only to provide information on the subjective score but also to objectively evaluate the control of mechanical stress to prevent knee lesions.
Typically, abnormal meniscus extrusion has been defined using various thresholds. Previous studies reported thresholds of 2, 3, or 4 mm under different situations, conditions, and patient populations (22–24), and did not reach a consensus on the appropriate value. By contrast, this study investigated the effect of cumulative mechanical stress on meniscus extrusion and quantified the extrusion without relying on a threshold. This method has been reported to have high reliability (8) and can detect the immediate reaction of meniscus extrusion after loading stress as the Δ-value. Therefore, this quantified evaluation could be a valuable tool for assessing the mechanical stress associated with meniscus extrusion.
This study has some limitations. First, this study had a small sample size; therefore, within-group analyses could not be performed. Second, the meniscus extrusion in the running group was measured during walking because of the low sampling rate on ultrasonography. This raises concerns about potentially underestimating the maximum value of meniscus extrusion after cumulative stress in the jogging condition. Third, this study did not obtain knee alignment. Finally, this study recruited healthy volunteers who engaged in recreational sports once a week. The athletes’ cumulative stress may not have been sufficiently reflected, and the distance was only 5 km. However, it is unknown whether these data can be applied. Future studies are needed to assess knee alignment at different effort distances with sufficient sample sizes.
Medial meniscus extrusion occurs temporarily after uphill/downhill efforts in healthy volunteers.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the Research Ethics Committee of the Hiroshima University (Approval Number: E-2495-1). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
YI: Formal Analysis, Funding acquisition, Writing – original draft, Writing – review & editing. SO: Data curation, Formal Analysis, Writing – review & editing. RO: Data curation, Writing – review & editing. TH: Data curation, Writing – review & editing. CX: Data curation, Writing – review & editing. KZ.: Data curation, Writing – review & editing. YN: Funding acquisition, Methodology, Writing – review & editing. KO: Methodology, Validation, Writing – review & editing. KT: Methodology, Validation, Writing – review & editing. NA: Supervision, Writing – review & editing. MT: Methodology, Supervision, Writing – review & editing.
The authors declare financial support was received for the research, authorship, and/or publication of this article.
This study was supported with grant from the Clinical Research Promotion Foundation and Grants-in-Aid for Scientific Research from the Japan Society for the Promotion of Science (JSPS) (Award Numbers: 0G41402 and 23K16541).
KO and KT were employed by Konica Minolta, Inc.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Andriacchi TP, Koo S, Scanlan SF. Gait mechanics influence healthy cartilage morphology and osteoarthritis of the knee. J Bone Joint Surg Am. (2009) 91(Suppl 1):95–101. doi: 10.2106/JBJS.H.01408
2. Boocock M, McNair P, Cicuttini F, Stuart A, Sinclair T. The short-term effects of running on the deformation of knee articular cartilage and its relationship to biomechanical loads at the knee. Osteoarthritis Cartilage. (2009) 17:883–90. doi: 10.1016/j.joca.2008.12.010
3. Driban JB, Hootman JM, Sitler MR, Harris KP, Cattano NM. Is participation in certain sports associated with knee osteoarthritis? A systematic review. J Athl Train. (2017) 52:497–506. doi: 10.4085/1062-6050-50.2.08
4. Gessel T, Harrast MA. Running dose and risk of developing lower-extremity osteoarthritis. Curr Sports Med Rep. (2019) 18:201–9. doi: 10.1249/JSR.0000000000000602
5. Walker PS, Arno S, Bell C, Salvadore G, Borukhov I, Oh C. Function of the medial meniscus in force transmission and stability. J Biomech. (2015) 48:1383–8. doi: 10.1016/j.jbiomech.2015.02.055
6. Berthiaume M-J, Raynauld J-P, Martel-Pelletier J, Labonté F, Beaudoin G, Bloch DA, et al. Meniscal tear and extrusion are strongly associated with progression of symptomatic knee osteoarthritis as assessed by quantitative magnetic resonance imaging. Ann Rheum Dis. (2005) 64:556–63. doi: 10.1136/ard.2004.023796
7. Choi YR, Kim JH, Chung JH, Lee DH, Ryu KJ, Ha DH, et al. The association between meniscal subluxation and cartilage degeneration. Eur J Orthop Surg Traumatol. (2014) 24:79–84. doi: 10.1007/s00590-012-1144-3
8. Ishii Y, Ishikawa M, Nakashima Y, Hayashi S, Kanemitsu M, Kurumadani H, et al. Association between medial meniscus extrusion under weight-bearing conditions and pain in early-stage knee osteoarthritis. J Med Ultrason. (2021) 2001(48):631–8. doi: 10.1007/s10396-021-01109-y
9. Diermeier T, Beitzel K, Bachmann L, Petersen W, Esefeld K, Wörtler K, et al. Mountain ultramarathon results in temporary meniscus extrusion in healthy athletes. Knee Surg Sports Traumatol Arthrosc. (2019) 27:2691–7. doi: 10.1007/s00167-018-5303-x
10. Ishii Y, Hashizume T, Okamoto S, Iwamoto Y, Ishikawa M, Nakashima Y, et al. Cumulative knee adduction moment during jogging causes temporary medial meniscus extrusion in healthy volunteers. J Med Ultrason (2001). (2023) 50:229–36. doi: 10.1007/s10396-023-01288-w
11. Kuster M, Sakurai S, Wood GA. Kinematic and kinetic comparison of downhill and level walking. Clin Biomech Bristol Avon. (1995) 10:79–84. doi: 10.1016/0268-0033(95)92043-l
12. Akpinar B, Thorhauer E, Tashman S, Irrgang JJ, Fu FH, Anderst WJ. Tibiofemoral cartilage contact differences between level walking and downhill running. Orthop J Sports Med. (2019) 7:2325967119836164. doi: 10.1177/2325967119836164
13. Shrive NG, O’Connor JJ, Goodfellow JW. Load-bearing in the knee joint. Clin Orthop. (1978) 131:279–87.
14. Ishii Y, Ishikawa M, Nakashima Y, Takahashi M, Iwamoto Y, Hashizume T, et al. Knee adduction moment is correlated with the increase in medial meniscus extrusion by dynamic ultrasound in knee osteoarthritis. Knee. (2022) 38:82–90. doi: 10.1016/j.knee.2022.07.011
15. Ishii Y, Ishikawa M, Nakashima Y, Takahashi M, Hashizume T, Okamoto S, et al. Visualization of lateral meniscus extrusion during gait using dynamic ultrasonographic evaluation. J Med Ultrason (2001). (2023) 50:531–9. doi: 10.1007/s10396-023-01330-x
16. Jasiewicz JM, Allum JHJ, Middleton JW, Barriskill A, Condie P, Purcell B, et al. Gait event detection using linear accelerometers or angular velocity transducers in able-bodied and spinal-cord injured individuals. Gait Posture. (2006) 24:502–9. doi: 10.1016/j.gaitpost.2005.12.017
17. Willinger L, Lang JJ, von Deimling C, Diermeier T, Petersen W, Imhoff AB, et al. Varus alignment increases medial meniscus extrusion and peak contact pressure: a biomechanical study. Knee Surg Sports Traumatol Arthrosc. (2019) 28:1092–8. doi: 10.1007/s00167-019-05701-1
18. Bloecker K, Wirth W, Hudelmaier M, Burgkart R, Frobell R, Eckstein F. Morphometric differences between the medial and lateral meniscus in healthy men—a three-dimensional analysis using magnetic resonance imaging. Cells Tissues Organs. (2012) 195:353–64. doi: 10.1159/000327012
19. Gokkus K, Atmaca H, Uğur L, Özkan A, Aydin AT. The relationship between medial meniscal subluxation and stress distribution pattern of the knee joint: finite element analysis. J Orthop Sci. (2016) 21:32–7. doi: 10.1016/j.jos.2015.10.001
20. Rennie WJ, Finlay DBL. Meniscal extrusion in young athletes: associated knee joint abnormalities. AJR Am J Roentgenol. (2006) 186:791–4. doi: 10.2214/AJR.04.1181
21. Emmanuel K, Quinn E, Niu J, Guermazi A, Roemer F, Wirth W, et al. Quantitative measures of meniscus extrusion predict incident radiographic knee osteoarthritis—data from the osteoarthritis initiative. Osteoarthr Cartilage. (2016) 24:262–9. doi: 10.1016/j.joca.2015.08.003
22. Boxheimer L, Lutz AM, Zanetti M, Treiber K, Labler L, Marincek B, et al. Characteristics of displaceable and nondisplaceable meniscal tears at kinematic MR imaging of the knee. Radiology. (2006) 238:221–31. doi: 10.1148/radiol.2381041234
23. Shimozaki K, Nakase J, Asai K, Yoshimizu R, Kimura M, Kanayama T, et al. Usefulness of ultrasonography for dynamic evaluation of medial meniscus hoop function in early knee osteoarthritis. Sci Rep. (2021) 11:20091. doi: 10.1038/s41598-021-99576-3
24. Debieux P, Jimenez AE, Novaretti JV, Kaleka CC, Kriscenski DE, Astur DC, et al. Medial meniscal extrusion greater than 4 mm reduces medial tibiofemoral compartment contact area: a biomechanical analysis of tibiofemoral contact area and pressures with varying amounts of meniscal extrusion. Knee Surg Sports Traumatol Arthrosc. (2020) 29:3124–32. doi: 10.1007/s00167-020-06363-0
Keywords: meniscus extrusion, ultrasonography, cumulative load, uphill/downhill loading, healthy individual
Citation: Ishii Y, Okamoto S, Okinaka R, Hashizume T, Xu C, Zhu K, Nakashima Y, Okada K, Takagi K, Adachi N and Takahashi M (2024) Temporary meniscus extrusion is caused by cumulative stress from uphill and downhill tasks in healthy volunteers. Front. Sports Act. Living 6:1271987. doi: 10.3389/fspor.2024.1271987
Received: 4 August 2023; Accepted: 18 March 2024;
Published: 8 April 2024.
Edited by:
Pedro Morouço, Polytechnic Institute of Leiria, Portugal© 2024 Ishii, Okamoto, Okinaka, Hashizume, Xu, Zhu, Nakashima, Okada, Takagi, Adachi and Takahashi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yosuke Ishii yishii77@hiroshima-u.ac.jp
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.