 Tianzhi Liao
Tianzhi Liao Yujia Yin2
Yujia Yin2 Saizhao Tang
Saizhao Tang- 1Department of Sports Science, Guiyang University, Guiyang, China
- 2Department of Sports Sociology, Guiyang University, Guiyang, China
- 3Department of Physical Education, Guiyang University, Guiyang, China
- 4Department of Sports Medicine, Guiyang University, Guiyang, China
- 5Department of Sports Science, Soonchunhyang University, Asan, Republic of Korea
Purpose: The intent of this paper is to understand the effect of Physical Activity on university students' Subjective Well-being and to explore whether Perceived Health, Social Support, and Self-esteem play roles as mediating variables.
Methods: Self-reported data from 404 college students (147 males and 257 females) were analyzed using structural equation modeling (SEM). The relationships between the study variables were tested by mediation models and 5,000 bootstrap samples using AMOS version 24.
Results: (1) The six hypotheses were supported in the measurement model in the results (P < 0.05). Physical Activity was related to Social Support, Perceived Health, and to Self-esteem; Social Support, Perceived Health, and Self-esteem were all related to Subjective Well-being. However, the direct positive effect of Physical Activity gradually decreased in the order of Self-esteem, Social Support, and Perceived Health. The direct effect of Perceived Health, Social Support, and Self-esteem on Subjective Well-being also decreased sequentially. (2) In the Structural Equation Model (χ2 = 825.451, p < 0.001, df = 455, CMIN/df = 1.814, CFI = 0.942, RMSEA = 0.045), the three hypotheses of mediation were supported (P < 0.05), showing positive indirect effects between Physical Activity and Subjective Well-being. Of the three mediating effects, Social Support and Self-esteem were not different, and the mediating effect of Perceived Health showed the largest impact. This indicates that Social Support, Perceived Health, and Self-esteem mediate the effects of Physical Activity, and Subjective Well-being regulation has positive indirect effects.
Conclusion: This study demonstrates the importance of meeting the needs of Social Support, Perceived Health, and Self-esteem when designing interventions to promote college students' sports participation to enhance Subjective Well-being.
1. Introduction
Most college students face mental health problems such as depression and anxiety (1, 2). In the United States, almost half of college-aged individuals have a psychiatric disorder (3). The prevalence of mental health problems among U.S. college students was higher in 2011 than in 2008, with 34.5% of college students reporting depressive symptoms according to the 2015 National College Health Assessment (4). Likewise, more than 20% of Chinese college students suffer from depression, and this ratio has continued to grow over the past decade (5). Research indicates that approximately half of university students have moderate stress-related mental health concerns, including anxiety and depression (6). Physical activity (PA), as a modifiable health behavior, has been identified as an influential factor in promoting physical and mental health (7). Regular participation in PA is associated with a reduced risk of cardiovascular disease, hypertension, type 2 diabetes, and depression (8). Mental health research should study positive psychological traits such as subjective well-being (SWB) (9). Despite evidence suggesting a positive impact of PA on mental health, PA has been primarily considered a method of preventing or treating mental disorders.
“The body of research on the link between PA and SWB is still in its early stages. SWB, according to Diener et al., is “a person's cognitive and affective evaluations of their life” (10). Living satisfaction is the overall judgment people make of their living situations (11, 12), and is the cognitive component of SWB, whereas positive and negative affect are the affective components (13). Happiness, defined as a subjective psychological state characterized by enjoyment and contentment, is extensively employed as a measure of SWB and an effective component of SWB (14). Life satisfaction is an essential variable since it is related to university students” mental and physical health and has been identified as one of the basic conceptions in the field of positive psychology (15). Thus, Understanding the factors that contribute to life satisfaction is a critical problem for university students. SWB dimensions can be mixed in a variety of ways, and SWB can be studied as a rapid cognitive assessment of one's health satisfaction.”
Perceived or self-rated health refers to an individual's perception of their health status. There is evidence that perceived health correlates more with SWB than objectively measured health (16, 17). From the perspective of perceived health, perceived health and well-being in adults are positively correlated among individuals and communities in the United States (18), and perceived health status is significantly associated with well-being in Sweden (19). Although objective health indicators such as physical health and functional rate have a relatively small effect on life satisfaction in older adults (20, 21), perceived health is significantly associated with well-being (22), and perceived health in middle-aged and older adults mediates PA and SWB (23). However, whether perceived health also mediates this relationship in college students remains unknown.
Social support is the feeling or experience of being loved, cared for, respected, and valued by a person as part of a social network of mutual aid and obligation (24). Social support is widely believed to be positively related to SWB (25, 26). Some studies suggest that social support is necessary for SWB (27). Social support should promote well-being by influencing cognition, emotion, and behavior to support positive affect (28). Social support varies by partner, family, and friends (29). Social help from family and friends positively relates to life satisfaction, but the interaction between these two variables is not statistically significant (30). Diener et al. (1999) (31) suggested that the theory must be refined to identify differential effects of input variables on components of SWB-specific predictions. There are separable components of SWB that exhibit unique patterns of relationships with different variables.
Self-esteem is an individual's overall sense of worth or value (Rosenberg, 1979) (32) and is framed in the context of demographic characteristics, social relationships, and personality (33–35). In many past studies, self-esteem has been strongly correlated with each component of SWB. Individuals with higher levels of self-esteem report higher life satisfaction and positive emotions and lower negative emotions, especially in individualistic cultures (33, 34, 36, 37). Self-esteem is strongly correlated with PA in children (38), and adolescents (39–41), and adults (42–44). Rosenberg et al. (1995) (45) emphasized that specific behaviors may be related to similar explicit self-esteem. In addition, it has been proposed that participation in PA contributes indirectly to an overall sense of self-worth and may enhance perceptions of the physical self, such as perceived physical appearance and physical motor ability (46).
In addition, several studies have shown that self-esteem is one of the strongest predictors of the cognitive component of SWB in adolescents and adults (47, 48). On the other hand, past research has shown that social support appears to have direct and indirect effects on well-being through specific cognitive mechanisms, personality factors (e.g., optimism, self-efficacy), and health behaviors (49–51). Considering that social support contributes theoretically (32, 52)and empirically (53–55) to self-esteem, self-esteem contributes theoretically and empirically to SWB.
The positive effects of PA on physical and mental health are well documented. Previous research has widely documented the positive relationship between PA and various physical health parameters (56–58). PA is associated with lower overall mortality (59), improved cardiovascular and musculoskeletal health (60), lower risk of obesity and stroke (59), lower mental health burdens (61), and reduced symptoms of depression and anxiety (62–64). Studies based on a large general population suggest a positive correlation between PA and SWB (65, 66), and some studies suggest that regular PA may increase SWB in all age groups: children and adolescents (15, 67); young adults (68); adults (69, 70); and older adults (71–73). Research on this relationship among college students is limited, and only a few relevant studies exist.
The findings reveal the relationship between PA and SWB but can only provide generalizability to a limited extent. Most recent well-being studies focus on the relationship between a single factor and SWB, lacking systematic integration of various influencing factors, yet multiple factors influence SWB simultaneously. Only by considering individual factors, i.e., external environmental factors, can a multidimensional integration model be formed to explore the direct or indirect effects and contributions of individual factors on well-being. In addition, perceived health, social support, and self-esteem positively impact psychological well-being. In conclusion, given the robust evidence of a strong relationship between health and SWB and the beneficial effects of PA on health, we conclude that the relationship between PA and SWB among university students may be mediated by perceived health, social support, and self-esteem.
Research on the mediating variables of PA and SWB among the areas of university students, PA and Perceived Health, Social Support, and Self-esteem has become a significant research topic. This study uses the Physical Activity Scale, SWB Scale, Perceived Health Scale, Social Support Scale, and Self-esteem to analyze the effects of PA on university students' SWB and to explore whether Perceived Health, Social Support, and Self-esteem mediate the effects of PA on SWB, taking Chinese university students, a particular group, as its sample.
2. Method
The purpose of this study was to investigate the association between PA and SWB among university students, as well as the function of Perceived Health, Social Support, and Self-esteem in mediating the relationship between PA and SWB. As a result, the research subjects, research equipment, and data processing were carried out in accordance with the study's purpose.
2.1. Research model and research hypothesis
2.1.1. Research model
As shown in Figure 1, this study aimed to determine the effect of PA on university students' SWB and explore whether Perceived Health, Social Support, and Self-esteem mediate the effect of PA on SWB.
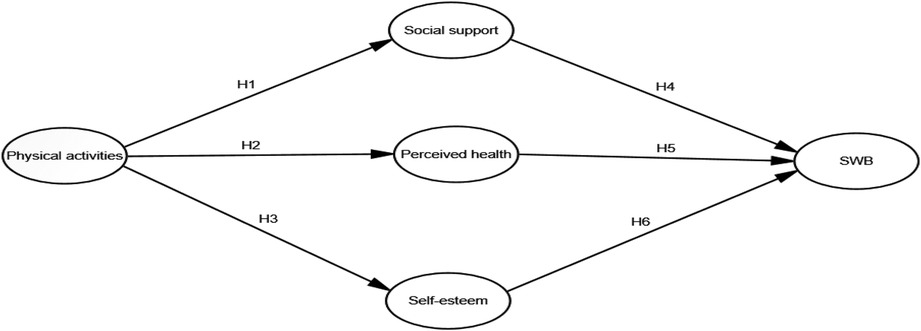
Figure 1. Research model.
2.1.2. Research hypothesis
According to the research model and the problems to be solved, we put forward nine corresponding research hypotheses, which are described as follows:
H1 Physical activity affects social support.
H2 Physical activity affects perceived health.
H3 Physical activity affects self-esteem.
H4 Social support affects subjective well-being.
H5 Perceived health affects subjective well-being.
H6 Self-esteem affects subjective well-being.
H7 Social support mediates the relationship between physical activity and subjective well-being.
H8 Perceived health mediates the relationship between physical activity and subjective well-being.
H9 Self-esteem mediates the relationship between physical activity and subjective well-being.
2.2. Participants
Participants for this study were recruited through Questionnaire Star, and 420 Chinese university students were identified from May to June 2022. An explanation of the primary purpose and content of the survey was given to participants in Questionnaire Star, and written informed consent was obtained from all participants before the survey. The study protocol was approved by the Institutional Review Board (IRB)-(1040875-202202-SB-021) in Korea. These participants completed questionnaires assessing their well-being, life satisfaction, PA, and perceived health during the assessment. As reported in Table 1, a total of 420 questionnaires were recovered, and those who skipped more than 16 questions or answered the questionnaire incorrectly were excluded, leaving 404 samples for further analysis. Looking at the individual characteristics in detail, 147 males (36.4%) and 257 females (63.6%) were included. As indicated previously, the survey captured College year groups: Freshman (28, 6.9%); Sophomore (141, 34.9%); Junior (143, 35.4%); Senior (92, 22.8%). In terms of Habit, less than 12 months (304, 75.2%), more than 12 months (100, 24.8%).
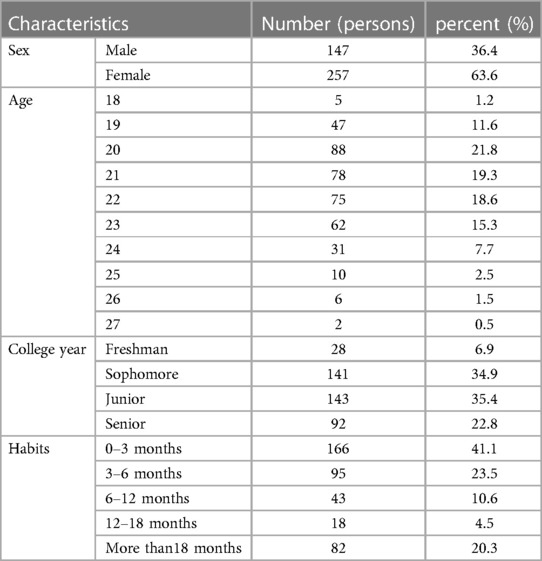
Table 1. Socio-demographic characteristics of participants (N = 404).
2.3. Measures
The Physical Activity Scale, Social Support Scale, and SWB, and Perceived Health, and Self-esteem measures were employed in this study. We investigated the effect of PA on college students' SWB using a cohort of Chinese university students as subjects. We investigated whether perceived health, social support, and self-esteem act as moderators of the effect of PA on SWB.
2.3.1. Moderate to vigorous physical activity (MVPA)
MVPA was measured using two questions adapted from the PA and physical fitness section of the 2007–2008 National Health and Nutrition Examination Survey (74):(1) “In a typical week, how much time do you usually spend doing moderate-intensity physical activities that cause small increases in breathing or heart rate?” and (2) “In a typical week, how much time do you usually spend doing vigorous-intensity physical activities that cause large increases in breathing or heart rate?” (75, 76).
2.3.2. Subjective well-being scale
2.3.2.1. Positive affect and negative affect scale
Positive affect and negative affect were assessed using the Chinese-translated version of the Scale of Positive and Negative Experience (SPANE) (77). The validity and reliability of SPANE have been tested previously among Chinese adults (78). The SPANE has twelve items describing positive and negative feelings such as “pleasant,” “joyful,” and “sad.” The respondents were asked to rate the extent to which they experienced each item using a 5-point Likert scale from 1 (very rarely or never) to 5 (very often or always). The SPANE produces a score for positive affect (Cronbach's Alpha = 0.914) and a score for negative affect (Cronbach's Alpha = 0.901) by adding the scores of the corresponding items.
2.3.2.2. Happiness scale
Happiness was measured as the affective component of SWB using the Chinese translated version of the Subjective Happiness Scale (SHS) (79). The SHS consists of four items on happiness, asking to what extent you agree or disagree with statements including (1) “In general, I consider myself a very happy person,” and (2) “Compared to most of my peers, I consider myself happier.” Response options were scaled from 1 (strongly disagree) to 7 (strongly agree). In this study, Cronbach's alpha coefficient for the Happiness Scale index was 0.871.
2.3.2.3. Life satisfaction scale
Life satisfaction was measured as the cognitive component of SWB using the Chinese translated version of the Satisfaction with Life Scale (SWLS) (80). The SWLS consists of five items to measure global cognitive judgments of life satisfaction, including (1) “In most ways, my life is close to my ideal,” (2) “The conditions of my life are excellent,” (3) “I am satisfied with life,” (4) “So far, I have gotten the important things I want in life,” and (5) “If I could live my life over, I would change almost nothing.” The score of each item ranges from 1 (strongly disagree) to 7 (strongly agree), indicating how much you agree or disagree with each statement. A mean score was computed by averaging the score of each item, with higher scores indicating greater life satisfaction. Previous studies have shown that the SWLS has good levels of reliability and validity for Chinese university students (81, 82). In this study, Cronbach's alpha coefficient for the Life Satisfaction Scale index was 0.879.
2.3.3. Perceived health scale
Perceived health was assessed using a single item: “During the past 30 days, how often did you feel very healthy and full of energy?” The predefined responses were “never,” “seldom,” “sometimes,” “oftentimes,” and “always” (coded as 1–5). This one-item question was adapted from the healthy days core module of the 2001 Behavioral Risk Factor Surveillance System (BRFSS) survey (83, 84).
2.3.4. Social support scale
To assess perceived social support in participants, we administered the Multi-Dimensional Scale of Perceived Social Support (MSPSS) (85), consisting of twelve items. The scale assesses three sources of support: significant other, family, and friends. Example items include statements like “There is a special person who is around when I am in need”, “There is a special person with whom I can share my joys and sorrows”, and “My family really tries to help me”. Each item is answered on a seven-point Likert scale ranging from 1 = strongly disagree to 7 = strongly agree. In this study, Cronbach's alpha coefficient for the Social Support Scale index was 0.865.
2.3.5. Self-Esteem scale
The Rosenberg Self-Esteem Scale contains ten items scored on a four-point Likert scale and provides an overall evaluation of one's worth or value (Rosenberg, 1965) (86). For example, items included “I feel that I have a number of good qualities,” “I feel I do not have much to be proud of,” and “I feel that I’m a person of worth, at least on an equal plane with others.” In this study, Cronbach's alpha coefficient for the Self-Esteem Scale index was 0.811.
2.4. Statistical analysis
In this study, the descriptive statistics and reliability of the demographic characteristics of the study population were studied using SPSS 23.0, and correlation analysis was performed using SPSS 23.0. The AMOS 24.0 program was used to perform validation factor analysis, construct models, etc. The main research questions and analysis were conducted in the following ways.
First, the questions were subjected to a validation factor analysis to filter out the questions suitable for representing each dimension and verify the validity of the measurement instrument. Second, Cronbach's alpha values were calculated to verify the reliability of each item of the questionnaire, such as the tools from the measurement scales for PA, SWB, perceived health, social support, and self-esteem. Third, correlation analysis was conducted using the correlation coefficient of Person to identify problems of multicollinearity in the observed variables. Fourth, descriptive statistical analysis was conducted to understand the demographic characteristics of each measured variable. Fifth, the direct effects in the model were analyzed by using structural equation modeling to predict the variables. Sixth, the PA factor of college students was used as the independent variable, the SWB factor was used as the dependent variable, and the perceived health, social support, and self-esteem of college students were used as mediating variables. The significance of indirect effects was verified by bootstrapping. All statistical tests set the statistical significance level at p < 0.05.
3. Results
In this study, AMOS 24.0 was used to construct structural equation models before structural modeling analysis to test the proposed hypotheses. Confirmatory factor analysis (CFA) was conducted first, followed structural equation modeling (SEM) estimation according to Anderson and Gerbing's (1988) (87) two-step approach and recommended principles. The consistency of all scales was assessed, with a high Cronbach's alpha of 0.70 indicating good internal consistency (Fomell & Lacker, 1981) (88). In addition, this study used χ2, df, CMIN/DF, CFI, and RMSEA to further analyze the model's fit to the data, with CMIN/DF less than 3, CFI greater than 0.9, and RMSEA less than 0.08.
3.1. Structural model
AMOS 24.0 was used to establish the structural equation model and test the hypotheses based on the theoretical model and hypotheses proposed in the study. Table 2 shows that the fitness of the structural equation model of the complete model is χ2 = 825.451, p < 0.001, df = 455, CMIN/df = 1.814, CFI = 0.942, RMSEA = 0.045. The fitness of the structural equation model can be evaluated as good. The structural equation model analysis result is shown in Figure 2.

Table 2. The result of the structural model.
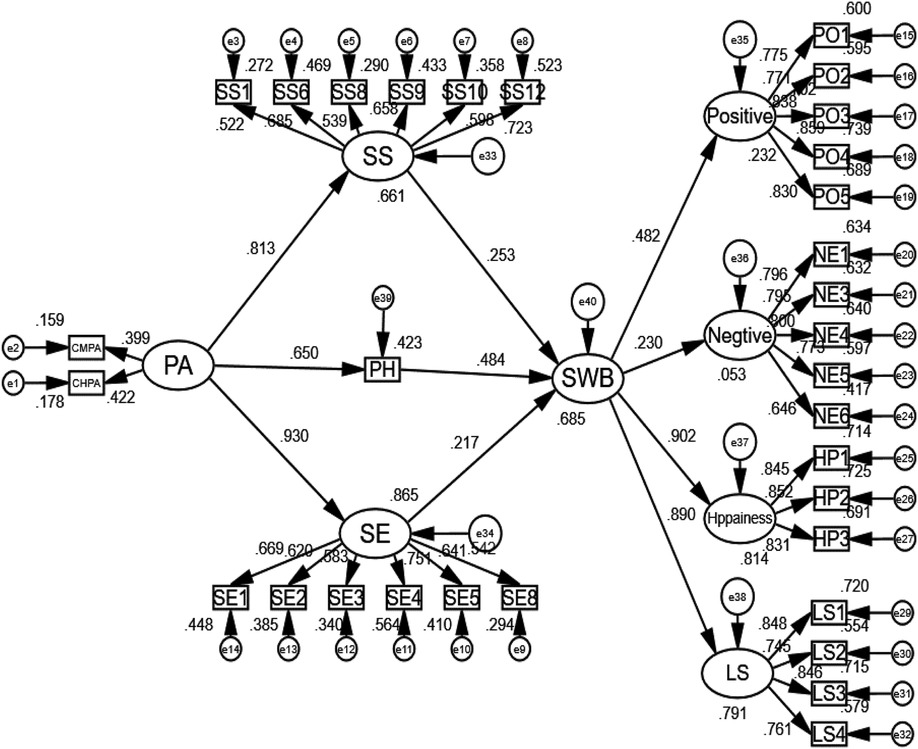
Figure 2. The result of the structural model.
Table 3 show the results of hypothesis testing.
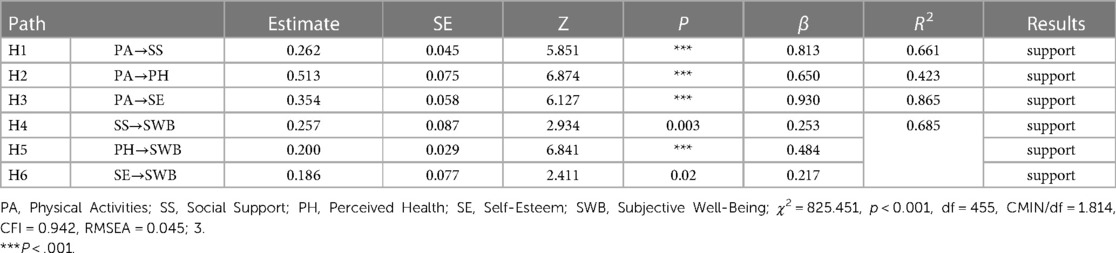
Table 3. The structural model analysis result.
The path coefficient of the effect of PA on social support was significantly positive, with a path coefficient of 0.813; hypothesis H1 was supported.
The path coefficient of the effect of PA on perceived health was significantly positive, with a path coefficient of 0.650; hypothesis H2 was supported.
The path coefficient of the effect of PA on self-esteem was significantly positive, with a path coefficient of 0.930; hypothesis H3 was supported.
The path coefficient of the effect of social support on SWB was significantly positive, with a path coefficient of 0.253; hypothesis H4 was supported.
The path coefficient of the effect of perceived health on SWB was significantly positive, with a path coefficient of 0.484; hypothesis H5 was supported.
The path coefficient of the effect of self-esteem on SWB was significantly positive, with a path coefficient of 0.217; hypothesis H6 was supported.
The R2 value was used to analyze the predictive power of each variable. The values should be sufficiently high for the model to have a minimum level of explanatory power. Chin (1998) (89) considers values of approximately 0.670 substantial, approximately 0.333 average, and values of 0.190 and lower weak. PA accounted for 66.1% of the variance in social support (R2 = .661). PA was 42.3% of the variance in perceived health (R2 = .423) and 86.5% of the variance in self-esteem (R2 = .865). Social support for SWB, perceived health, and self-esteem explained 68.5% of the variance in SWB (R2 = .685).
3.2. Mediation effect
To verify the mediation effect more accurately, the bootstrap method is adopted. The data were bootstrapped with repeated sampling 5,000 times, with the confidence interval level set at 95%, and the sampling method was a nonparametric percentile with deviation correction.
As seen in Table 4, the indirect effect of PA→SS→SWB was 0.067 with a 95% confidence interval (.019-.164), excluding zero, indicating a significant mediating impact. The indirect effect of PA→PH→SWB was 0.103, with a 95% confidence interval (.057-.180), excluding zero, marking a significant mediating effect. The immediate impact of PA→SE→SWB was 0.066, with a 95% confidence interval (.009-.172), excluding zero, indicating a significant mediating effect.
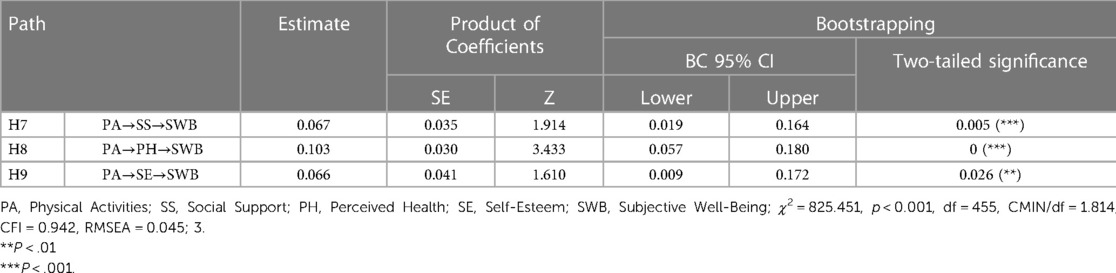
Table 4. Mediation test.
4. Discussion
There is much research on PA and SWB, and many studies and meta-analyses report a close relationship between the variables of PA and SWB (66). According to Zhang and Chen's (4) recommendations, the researchers combine PA with SWB by leveraging their theoretical advantages for describing health to improve their interpretations through the mediating effects of perceived health, and social support, and self-esteem. Predictions were made through a holistic model that promotes approach- and reality-based intervention plans. This study attempted to address the following areas: To examine the relationship between PA and the SWB of university students, and to observe whether perceived health, social support, and self-esteem played a mediating role on the relationship between PA and SWB.
This study helps to elucidate the effect of PA on SWB. The results showed that (1) according to the measurement model, all hypotheses were supported by the results. PA was related to social support, perceived health, and self-esteem; social support, perceived health, and self-esteem were related to SWB. However, the direct effect of PA observed in H1-H3 became more minor in self-esteem, social support, and perceived health. The direct effects of perceived health, social support, and self-esteem on SWB decrease sequentially. (2) According to the structural model, all three mediating hypotheses were supported. All three mediating effects showed positive indirect effects between PA and SWB. Of the three mediating effects, social support and self-esteem were not different, and the mediating result of perceived health had the greatest effect. This indicates that social support, perceived health, and self-esteem mediate PA to positively affect SWB regulation.
Studies based on a large general population have shown a positive correlation between PA and SWB and that PA is a crucial predictor of life satisfaction (90), consistent with the results of college students in this study (65, 66). It is widely accepted that social support positively relates to SWB (25, 26). Some studies have even shown that social support is necessary for SWB, consistent with the results of the college students in this study (27).
Direct impact studies in research have shown that self-esteem explains PA better than social support and perceived health, with PA contributing less to predictions of perceived health. Self-esteem was one of the strongest predictors of the cognitive component of SWB in adolescents and adults, which is consistent with the results of previous studies (35, 47, 48). Perceived health better explained SWB, with similar levels of prediction for social support and self-esteem. Perceived health was more strongly correlated with SWB than objectively measured health (16, 17), similar to previous studies. When social support, perceived health, and self-esteem were used as mediating variables, they positively influenced PA and SWB, with all three mediating effects significantly moderated. Analysis of the pathway results indicated that perceived health was the best mediator of the mediating effect. Past research has shown that social support appears to have a direct and indirect impact on wellbeing through specific cognitive mechanisms, personality factors, and health behaviors (26, 49–51). Perceived health in middle-aged and older adults mediates PA and SWB (23). This study demonstrated this relationship is mediated by perceived health also among college students.
The present study has important theoretical implications for research related to PA and SWB. In this paper, we systematically review the literature on PA and SWB to identify as many factors that affect them as possible and to provide a more comprehensive understanding of the research in this field. Some scholars have studied the relationship between PA and SWB in the past, and some studies have separately modeled the three dimensions of social support, perceived health, and self-esteem, but no scholars have developed a comprehensive structural model of social support, perceived health, and self-esteem along with PA and SWB to explore their relationship. In this paper, we explore the relationship between PA and SWB among Chinese university students through a web-based survey and verify the mediating effects of social support, perceived health, and self-esteem.
From a practical perspective, this study provides guidance for future scholars who study PA and SWB. First, based on the final results of the mediated effects, we will increase the attention brough to social support, perceived health, and self-esteem in future PA interventions for college students to enhance physical fitness and improve SWB at the same time. Second, in the context of enhancing SWB, this study strengthens the capacity of physical education teachers to give guidance to students to mobilize their own pursuits, changing traditional teaching concepts to keep up with the times, and improving the developmental consciousness of students in a comprehensive manner to better provide precise services for Chinese university sports participants.
Despite the limitations of the study, the findings are valuable. The study discovered a mediation influence between PA and SWB in terms of social support, perceived health, and self-esteem. However, there are some restrictions, most notably in the following areas: (1) To begin, the study employs a cross-sectional design, which gives a measure of past or current behavior rather than a prediction of future conduct. Because of its limitations, consistency bias may exist, making it impossible to discern causal links between variables. Longitudinal designs and randomized controlled trials may be used in future studies to assist in demonstrate causal links between SWB and PA. (2) One weakness of this study is the use of self-report tools. Because of the assessor, the context of measurement, and the content and qualities of the question items, such self-reporting can lead to changes in independent variables and changes in artifacts across variables, all of which can lead to differing participant reports. Thus, despite efforts to control for ambiguity in the question items, scale format, and questionnaire length, some uncontrollable elements in the study, such as societal expectations and subject response emotions, may have nevertheless influenced the outcomes. (3) Because this study was conducted with Chinese university students, it is crucial to exercise caution when extrapolating the findings to other populations.
5. Conclusion
This study focused on determining the relationship between physical activity and subjective well-being among Chinese university students, and the mediating effects of social support, perceived health, and self-esteem was verified in the composed integrated theoretical model. For application in physical activity research, we emphasized the role of social support, perceived health, and self-esteem in physical activity and subjective well-being based on evidence from previous studies, with theory-guided research promoting a more profound understanding among researchers and research subjects. Thus, the current study provides a valuable framework for research related to physical activity and subjective well-being. Finally, our findings suggest that creating a psychological environment that satisfies social support, perceived health, and self-esteem is essential to encouraging college students to participate in sports. This study theoretically confirms that interventions in the areas of social support, perceived health, and self-esteem ultimately results in enhancing college students' subjective well-being and quality of life and reducing conditions such as stress and depression.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Soonchunhyang Institutional Review Board on Human Subjects Research and Ethics Committees, Soonchunhyang University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
TL: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Writing – original draft. YY: Writing – original draft, Writing – review & editing. XH: Writing – original draft, Writing – review & editing. ST: Data curation, Formal Analysis, Investigation, Software, Writing – original draft. YS: Conceptualization, Funding acquisition, Methodology, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
This work was supported by the Soonchunhyang University and Guiyang University Research Fund.
Acknowledgments
We are indebted to the anonymous reviewers and editor for their comments.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Misra R, McKean M. College students’ academic stress and its relation to their anxiety, time management, and leisure satisfaction. Am J Health Stud. (2000) 16(1):41–51. http://ezproxy.staffs.ac.uk/login?url=https://search.ebscohost.com/login.aspx?direct=true&db=s3h&AN=3308416&site=ehost-live
2. Sutin AR, Terracciano A, Milaneschi Y, An Y, Ferrucci L, Zonderman AB. The trajectory of depressive symptoms across the adult life span. JAMA Psychiatry. (2013) 70(8):803–11. doi: 10.1001/jamapsychiatry.2013.193
3. Blanco C, Okuda M, Wright C, Hasin DS, Grant BF, Liu SM, et al. Mental health of college students and their non–college-attending peers: results from the national epidemiologic study on alcohol and related conditions. Arch Gen Psychiatry. (2008) 65(12):1429–37. doi: 10.1001/archpsyc.65.12.1429
4. Zhang Z, He Z, Chen W. The relationship between physical activity intensity and subjective well-being in college students. J Am Coll Health. (2022) 70(4):1241–6. doi: 10.1080/07448481.2020.1790575
5. Liu X, Gao X, Ping S. Post-1990s college students academic sustainability: the role of negative emotions, achievement goals, and self-efficacy on academic performance. Sustainability. (2019) 11(3):775. doi: 10.3390/su11030775
6. Regehr C, Glancy D, Pitts A. Interventions to reduce stress in university students: a review and meta-analysis. J Affect Disord. (2013) 148(1):1–11. doi: 10.1016/j.jad.2012.11.026
7. Rhodes RE, Janssen I, Bredin SS, Warburton DE, Bauman A. Physical activity: health impact, prevalence, correlates and interventions. Psychol Health. (2017) 32(8):942–75. doi: 10.1080/08870446.2017.1325486
8. Piercy KL, Troiano RP, Ballard RM, Carlson SA, Fulton JE, Galuska DA, et al. The physical activity guidelines for Americans. JAMA. (2018) 320(19):2020–8. doi: 10.1001/jama.2018.14854
9. Seligman ME, Csikszentmihalyi M. Positive psychology: an introduction. In. Flow and the foundations of positive psychology. Dordrecht: Springer (2014). p. 279–98. doi: 10.1037/0003-066X.55.1.5
10. Diener E, Lucas RE, Oishi S. Subjective well-being: the science of happiness and life satisfaction. In: Snyder CR, Lopez SJ, editors. Handbook of positive psychology. Oxford, UK and New York, NY: Oxford University Press (2002) p. 63–73.
11. Caprara GV, Steca P, Alessandri G, Abela JR, McWhinnie CM. Positive orientation: explorations on what is common to life satisfaction, self-esteem, and optimism. Epidemiol Psychiatr Sci. (2010) 19(1):63–71. doi: 10.1017/S1121189X00001615
12. Pavot W, Diener ED, Colvin CR, Sandvik E. Further validation of the satisfaction with life scale: evidence for the cross-method convergence of well-being measures. J Pers Assess. (1991) 57(1):149–61. doi: 10.1207/s15327752jpa5701_17
13. Ryan RM, Deci EL. On happiness and human potentials: a review of research on hedonic and eudaimonic well-being. Annu Rev Psychol. (2001) 52(1):141–66. doi: 10.1146/annurev.psych.52.1.141
14. Veenhoven R. How universal is happiness? In: Diener E, Helliwell JF, Kahneman D, editors. International Differences in Well-Being. NewYork: Oxford University Press (2010). p. 328–50. doi: 10.1093/acprof:oso/9780199732739.003.0011
15. Proctor CL, Linley PA, Maltby J. Youth life satisfaction: a review of the literature. J Happiness Stud. (2009) 10:583–630. doi: 10.1007/s10902-008-9110-9
16. Okun MA, Stock WA, Haring MJ, Witter RA. Health and subjective well-being: a meta-analyis. International J Aging Hum Dev. (1984) 19(2):111–32. doi: 10.2190/QGJN-0N81-5957-HAQD
17. Siahpush M, Spittal M, Singh GK. Happiness and life satisfaction prospectively predict self-rated health, physical health, and the presence of limiting, long-term health conditions. Am J Health Promot. (2008) 23(1):18–26. doi: 10.4278/ajhp.061023137
18. Subramanian SV, Kim D, Kawachi I. Covariation in the socioeconomic determinants of self-rated health and happiness: a multivariate multilevel analysis of individuals and communities in the USA. J Epidemiol Community Health. (2005) 59(8):664–9. doi: 10.1136/jech.2004.025742
19. Gerdtham UG, Johannesson M. The relationship between happiness, health, and socio-economic factors: results based on Swedish microdata. J Socio Econ. (2001) 30(6):553–7. doi: 10.1016/S1053-5357(01)00118-4
20. Bowling A, Farquhar M, Grundy E, Formby J. Changes in life satisfaction over a two and a half year period among very elderly people living in London. Soc Sci Med. (1993) 36:641–55. doi: 10.1016/0277-9536(93)90061-8
21. Berg AI, Hassing LB, McClearn GE, Johansson B. What matters for life satisfaction in the oldest-old? Aging Ment Health. (2006) 10:257–64. doi: 10.1080/13607860500409435
22. Despot-Lucanin J, Lucanin D. Associations of psychological, functional, and biological factors with age changes in the self-perceived health of old persons. GeroPsych: J Gerontopsychology Geriatr Psychiatry. (2012) 25:135–43. doi: 10.1024/1662-9647/a000063
23. Lera-López F, Ollo-López A, Sánchez-Santos JM. How does physical activity make you feel better? The mediational role of perceived health. Appl Res Qual Life. (2017) 12(3):511–31. doi: 10.1007/s11482-016-9473-8
24. Wills TA. Social support and interpersonal relationships. In: Clark MS, editors. Prosocial behavior (1991). p. 265–89.
25. Kahn JH, Hessling RM, Russell DW. Social support, health, and well-being among theelderly: what is the role of negative affectivity? Pers Individ Dif. (2003) 35:5–17. doi: 10.1016/S0191-8869(02)00135-6
26. Karademas EC. Self-efficacy, social support and well-being: the mediating role of optimism. Pers Individ Dif. (2006) 40:1281–90. doi: 10.1016/j.paid.2005.10.019
27. Diener E, Seligman E. Very happy people. Psychol Sci. (2002) 13:81–4. doi: 10.1111/1467-9280.00415
28. Cohen S, Gottlieb B, Underwood L. Theoretical and historical perspectives. In: Cohen S, Underwood L, Gottlieb B, editors. Social support measurement and intervention: A guide for health and social scientists. New York: Oxford University Press (2000). p. 3–28.
29. Walen HR, Lachman ME. Social support and strain from partner, family, and friends: costs and benefits for men and women in adulthood. J Soc Pers Relat. (2000) 17(1):5–30. doi: 10.1177/0265407500171001
30. Sheets RL Jr, Mohr JJ. Perceived social support from friends and family and psychosocial functioning in bisexual young adult college students. J Couns Psychol. (2009) 56(1):152. doi: 10.1037/0022-0167.56.1.152
31. Diener E, Suh EM, Lucas RE, Smith HL. Subjective well-being: three decades of progress. Psychol Bull. (1999) 125(2):276–302. doi: 10.1037/0033-2909.125.2.276
33. Diener E, Diener M. Cross-cultural correlates of life satisfaction and self-esteem. J Pers Soc Psychol. (1995) 68:653–63. doi: 10.1037/0022-3514.68.4.653
34. Bosson JK, Swann WB, Pennebaker JW. Stalking the perfect measure of implicit self-esteem: the blind men and the elephant revisited? J Pers Soc Psychol. (2000) 79:631–43. doi: 10.1037/0022-3514.79.4.631
35. Zhang L, Leung J. Moderating effects of gender and age on the relationship between self-esteem and life satisfaction in mainland Chinese. Int J Psychol. (2002) 37:83–91. doi: 10.1080/00207560143000252
36. Kwan VSY, Bond MH, Singelis TM. Pan cultural explanations for life satisfaction: adding relationship harmony to self-esteem. J Pers Soc Psychol. (1997) 73:1038–51. doi: 10.1037/0022-3514.73.5.1038
37. Oishi S, Diener E, Lucas RE, Suh EM. Cultural variation in predictors of life satisfaction: a perspective from needs and values. Pers Soc Psychol Bull. (1999) 25:980–90. doi: 10.1177/01461672992511006
38. Strauss RS, Rodzilsky D, Burack G, Colin M. Psychosocial correlates of physical activity in healthy children. Arch Pediatr Adolesc Med. (2001) 155(8):897–902. doi: 10.1001/archpedi.155.8.897
39. Daniels E, Leaper C. A longitudinal investigation of sport participation, peer acceptance, and self-esteem among adolescent girls and boys. Sex Roles. (2006) 55(11):875–80. doi: 10.1007/s11199-006-9138-4
40. Erkut S, Tracy AJ. Predicting adolescent self-esteem from participation in school sports among latino subgroups. Hisp J Behav Sci. (2002) 24(4):409–29. doi: 10.1177/0739986302238212
41. Zhang M, Xu X, Jiang J, Ji Y, Yang R, Liu Q, et al. The association between physical activity and subjective well-being among adolescents in southwest China by parental absence: a moderated mediation model. BMC psychiatry. (2023) 23(1):1–15. doi: 10.1186/s12888-022-04495-w
42. Cao M, Teng Y, Shao N, Wu Y. The relationship between home-based physical activity and general well-being among Chinese university students during the COVID-19 pandemic: the mediation effect of self-esteem. Humanit Soc Sci Commun. (2023) 10(1), 1–6. doi: 10.1057/s41599-022-01483-z
43. Iwon K, Skibinska J, Jasielska D, Kalwarczyk S. Elevating subjective well-being through physical exercises: an intervention study. Front Psychol. (2021) 12:702678. doi: 10.3389/fpsyg.2021.702678
44. McAuley E, Blissmer B, Katula J, Duncan TE, Mihalko SL. Physical activity, self-esteem, and self-efficacy relationships in older adults: a randomized controlled trial. Ann Behav Med. (2000) 22(2):131–9. doi: 10.1007/BF02895777
45. Rosenberg M, Schooler C, Schoenbach C, Rosenberg F. Global self-esteem and specific self-esteem: different concepts, different outcomes. Am Sociol Rev. (1995) 60(1):141. doi: 10.2307/2096350
46. Bowker A. The relationship between sports participation and self-esteem during early adolescence. Can J Behav Sci/Revue Canadienne des Sciences du Comportement. (2006) 38(3):214–29. doi: 10.1037/cjbs2006009
47. Neto F. Satisfaction with life among adolescents from immigrant families in Portugal. J Youth Adolesc. (2001) 30:53–67. doi: 10.1023/A:1005272805052
48. Chen S, Cheung FM, Bond MH, Leung JP. Going beyond self-esteem to predict life satisfaction: the Chinese case. Asian J Soc Psychol. (2006) 9:24–35. doi: 10.1111/j.1467-839X.2006.00182.x
49. Cohen S, Wills TA. Stress, social support and the buffering hypothesis. Psychol Bull. (1985) 98:310–57. doi: 10.1037/0033-2909.98.2.310
50. Davis MC, Swan PD. Association of negative and positive social ties with fibrinogen levels in young women. Health Psychol. (1999) 18:131–9. doi: 10.1037/0278-6133.18.2.131
51. Wills TA, Fegan MF. Social networks and social support. In: Baum A, Revenson TA, Singer JE, editors. Handbook of health psychology. Mahwah, NJ, USA: Erlbaum (2001). p. 209–34.
53. Sarason IG, Levine HM, Basham RB, Sarason BR. Assessing social support: the social support questionnaire. J Pers Soc Psychol. (1983) 44:127–39. doi: 10.1037/0022-3514.44.1.127
54. Dumont M, Provost MA. Resilience in adolescents: protective role of social support, coping strategies, self-esteem, and social activities on experience of stress and depression. J Youth Adolesc. (1999) 28:343–63. doi: 10.1023/A:1021637011732
55. Symister P, Friend R. The influence of social support and problematic support on optimism and depression in chronic illness: a prospective study evaluating self-esteem as a mediator. Health Psychol. (2003) 22(2):123–9. doi: 10.1037/0278-6133.22.2.123
56. Humphreys BR, McLeod L, Ruseski JE. Physical activity and health outcomes: evidence from Canada. Health Econ. (2014) 23(1):33–54. doi: 10.1002/hec.2900
57. Lechner M. Long-run labour market and health effects of individual sports activities. J Health Econ. (2009) 28(4):839–54. doi: 10.1016/j.jhealeco.2009.05.003
58. Reiner M, Niermann C, Jekauc D, Woll A. Long-term health benefits of physical activity–a systematic review of longitudinal studies. BMC Public Health. (2013) 13(1):1–9. doi: 10.1186/1471-2458-13-813
59. Lee IM, Shiroma EJ, Lobelo F, Puska P, Blair SN, Katzmarzyk PT, et al. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet. (2012) 380(9838), 219–29. doi: 10.1016/S0140-6736(12)61031-9
60. Curtis GL, Chughtai M, Khlopas A, Newman JM, Khan R, Shaffiy S, et al. Impact of physical activity in cardiovascular and musculoskeletal health: can motion be medicine? J Clin Med Res. (2017) 9(5):375. doi: 10.14740/jocmr3001w
61. Chekroud SR, Gueorguieva R, Zheutlin AB, Paulus M, Krumholz HM, Krystal JH, et al. Association between physical exercise and mental health in 1 2 million individuals in the USA between 2011 and 2015: a cross-sectional study. The Lancet Psychiatry. (2018) 5(9):739–46. doi: 10.1016/S2215-0366(18)30227-X
62. Kvam S, Kleppe CL, Nordhus IH, Hovland A. Exercise as a treatment for depression: a meta-analysis. J Affect Disord. (2016) 202:67–86. doi: 10.1016/j.jad.2016.03.063
63. Schuch FB, Vancampfort D, Richards J, Rosenbaum S, Ward PB, Stubbs B. Exercise as a treatment for depression: a meta-analysis adjusting for publication bias. J Psychiatr Res. (2016) 77:42–51. doi: 10.1016/j.jpsychires.2016.02.023
64. Wegner M, Helmich I, Machado S, Nardi AE, Arias-Carrion O, Budde H. Effects of exercise on anxiety and depression disorders: review of meta-analyses and neurobiological mechanisms. CNS Neurol Disord Drug Targets. (2014) 13(6):1002–14. doi: 10.2174/1871527313666140612102841
65. Ngamaba KH, Panagioti M, Armitage CJ. How strongly related are health status and subjective well-being? Systematic review and meta-analysis. Eur J Public Health. (2017) 27(5):879–85. doi: 10.1093/eurpub/ckx081
66. Buecker S, Simacek T, Ingwersen B, Terwiel S, Simonsmeier BA. Physical activity and subjective well-being in healthy individuals: a meta-analytic review. Health Psychol Rev. (2021) 15(4):574–92. doi: 10.1080/17437199.2020.1760728
67. Proctor C, Tsukayama E, Wood AM, Maltby J, Eades JF, Linley PA. Strengths gym: the impact of a character strengths-based intervention on the life satisfaction and well-being of adolescents. J Posit Psychol. (2011) 6(5):377–88. doi: 10.1080/17439760.2011.594079
68. Grant N, Wardle J, Steptoe A. The relationship between life satisfaction and health behavior: a cross-cultural analysis of young adults. Int J Behav Med. (2009) 16(3):259–68. doi: 10.1007/s12529-009-9032-x
69. Schnohr P, Kristensen TS, Prescott E, Scharling H. Stress and life dissatisfaction are inversely associated with jogging and other types of physical activity in leisure time–the Copenhagen city heart study. Scand J Med Sci Sports. (2005) 15(2):107–12. doi: 10.1111/j.1600-0838.2004.00394.x
70. Eime RM, Harvey JT, Brown WJ, Payne WR. Does sports club participation contribute to health-related quality of life? Med Sci Sports Exercise. (2010) 42(5):1022–8. doi: 10.1249/MSS.0b013e3181c3adaa
71. Clark SD, Long MM, Schiffman LG. The mind-body connection: the relationship among physical activity level, life satisfaction, and cognitive age among mature females. J Soc Behav Pers. (1999) 14(2):221–40. https://search.ebscohost.com/login.aspx?direct=true&db=psyh&AN=1999-01008-005&site=ehost-live
72. Elavsky S, McAuley E, Motl RW, Konopack JF, Marquez DX, Hu L, et al. Physical activity enhances long-term quality of life in older adults: efficacy, esteem, and affective influences. Ann Behav Med. (2005) 30(2):138–45. doi: 10.1207/s15324796abm3002_6
73. Withall J, Stathi A, Davis M, Coulson J, Thompson JL, Fox KR. Objective indicators of physical activity and sedentary time and associations with subjective well-being in adults aged 70 and over. Int J Environ Res Public Health. (2014) 11(1):643–56. doi: 10.3390/ijerph110100643
74. The National Health and Nutrition Examination Survey. (2013). Centers for disease control and prevention. http://www.cdc.gov/nchs/nhanes.htm (Accessed November 12, 2013.A 2007-2008).
75. Wanner M, Probst-Hensch N, Kriemler S, Meier F, Bauman A, Martin BW. What physical activity surveillance needs: validity of a single-item questionnaire. Br J Sports Med. (2014) 48(21):1570–6. doi: 10.1136/bjsports-2012-092122
76. Pierannunzi C, Hu SS, Balluz L. A systematic review of publications assessing reliability and validity of the behavioral risk factor surveillance system (BRFSS), 2004–2011. BMC Med Res Methodol. (2013) 13(1):1–14. doi: 10.1186/1471-2288-13-49
77. Diener E, Wirtz D, Tov W, Kim-Prieto C, Choi DW, Oishi S, et al. New well-being measures: short scales to assess flourishing and positive and negative feelings. Soc Indic Res. (2010) 97(2):143–56. doi: 10.1007/s11205-009-9493-y
78. Li F, Bai X, Wang Y. The scale of positive and negative experience (SPANE): psychometric properties and normative data in a large Chinese sample. PloS One. (2013) 8(4):e61137. doi: 10.1371/journal.pone.0061137
79. Lyubomirsky S, Lepper HS. A measure of subjective happiness: preliminary reliability and construct validation. Soc Indic Res. (1999) 46(2):137–55. doi: 10.1023/A:1006824100041
80. Diener ED, Emmons RA, Larsen RJ, Griffin S. The satisfaction with life scale. J Pers Assess. (1985) 49(1):71–5. doi: 10.1207/s15327752jpa4901_13
81. Sachs J. Validation of the satisfaction with life scale in a sample of Hong Kong university students. Psychologia. (2003) 46(4):225–34. doi: 10.2117/psysoc.2003.225
82. Wu CH, Yao G. Analysis of factorial invariance across gender in the Taiwan version of the satisfaction with life scale. Pers Individ Dif. (2006) 40(6):1259–68. doi: 10.1016/j.paid.2005.11.012
83. Centers for Disease Control and Prevention. Behavioral risk factor surveillance system survey questionnaire. Atlanta, Georgia: US Department of Health and Human Services, Centers for Disease Control and Prevention (2001). p. 22–3.
84. Horner-Johnson W., Krahn G., Andresen E., Hall T., & RRTC Expert Panel on Health Status Measurement. (2009). Developing summary scores of health-related quality of life for a population-based survey. Public Health Rep, 124(1), 103–10. doi: 10.1177/003335490912400113
85. Zimet GD, Dahlem NW, Zimet SG, Farley GK. The multidimensional scale of perceived social support. J Pers Assess. (1988) 52(1):30–41. doi: 10.1207/s15327752jpa5201_2
86. Rosenberg M. Rosenberg self-esteem scale (RSE). Acceptance and commitment therapy. Measures package. (1965). p. 61–2. doi: 10.1037/t01038-000
87. Anderson JC, Gerbing DW. Structural equation modeling in practice: a review and recommended two-step approach. Psychol Bull. (1988) 103(3):411. doi: 10.1037/0033-2909.103.3.411
88. Fornell C, Larcker DF. Structural equation models with unobservable variables and measurement error: Algebra and statistics (1981).
89. Chin WW. The partial least squares approach to structural equation modeling. Modern Methods Bus Res. (1998) 295(2):295–336.
Keywords: physical activity, subjective well-being, social support, perceived health, self-esteem
Citation: Liao T, Yin Y, Hu X, Tang S and Shim Y (2023) The relationship between physical activity and subjective well-being in Chinese university students: the mediating roles of perceived health, social support and self-esteem. Front. Sports Act. Living 5:1280404. doi: 10.3389/fspor.2023.1280404
Received: 20 August 2023; Accepted: 12 October 2023;
Published: 25 October 2023.
Edited by:
Pedro Forte, Higher Institute of Educational Sciences of the Douro, PortugalReviewed by:
Soukaina Hattabi, University of Jendouba, TunisiaJosé Eduardo Teixeira, Polytechnic Institute of Bragança (IPB), Portugal
© 2023 Liao, Yin, Hu, Tang and Shim. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yunsik Shim eXVuc2lrc2hpbUBnbWFpbC5jb20=