 Reece Scott
Reece Scott Ruth James
Ruth James Cleveland T. Barnett
Cleveland T. Barnett Craig Sale2,‡
Craig Sale2,‡ Ian Varley
Ian Varley
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Sports Act. Living, 25 April 2023
Sec. Elite Sports and Performance Enhancement
Volume 5 - 2023 | https://doi.org/10.3389/fspor.2023.1150052
This article is part of the Research TopicThe Application of Technology to Enhance Quantitative Feedback in SportView all 5 articles
Introduction: There is limited information regarding the association between external load and estimated bone load in sport, which may be important due to the influence exercise can have on bone accrual and injury risk. The aim of this study was to identify external load measuring tools used by support staff to estimate bone load and assess if these methodologies were supported in research.
Methods: A survey was comprised of 19 multiple choice questions and the option to elaborate on if/how they monitor external load and if/how they used them to estimate bone load. A narrative review was performed to assess how external load is associated to bone in research.
Results: Participants were required to be working as support staff in applied sport. Support staff (n = 71) were recruited worldwide with the majority (85%) working with professional elite athletes. 92% of support staff monitored external load in their organisation, but only 28% used it to estimate bone load.
Discussion: GPS is the most commonly used method to estimate bone load, but there is a lack of research assessing GPS metrics with bone load. Accelerometry and force plates were among the most prevalent methods used to assess external load, but a lack of bone specific measurements were reported by support staff. Further research exploring how external load relates to bone is needed as there is no consensus on which method of external load is best to estimate bone load in an applied setting.
Physical loading can be separated into two categories; internal load and external load (1). Internal load is the biological stress imposed upon an individual, such as heart rate or blood lactate (2), whereas external load can be described as the work completed (e.g., acceleration or force) independent of the internal characteristics (3). Biomechanical external load has an important relationship with the mechanical stresses imposed on the musculoskeletal system (4). Monitoring external load is important in sport as it provides objective data on physical attributes in response to prescribed training (5), as well as being used to optimise performance (6, 7). High intensity external loading has been associated with an increase in injury risk of up to 270% in rugby league (8) and football (9) and, as such, monitoring external load in applied settings has increased in popularity to try to mitigate against injury (10, 11). Understanding methods to measure external load in relation to bone allows support staff to gain the knowledge of how external load can be associated to bone characteristics and its applicability within an applied setting. Subjective methods (e.g., questionnaires or rating of perceived exertion) are often used to monitor load in athletes, but these metrics lack reliability and validity in comparison to objective measures as these are dependent upon the athlete's perception (12). Although invasive methods (e.g., bone mounted strain gauges and bone staples) studying bone responses are insightful, they are restricted in their applicability due to their invasiveness (13). Blood biomarkers such as N-terminal propeptide of type I procollagen and C-terminal telopeptide of type I collagen are less invasive methods of understanding the response in bone, however these do not quantify bone load but rather provide information relating to the bone (re)modelling response at the whole body level (14). Metrics derived from applied technologies (e.g., global positioning systems, GPS; inertial measurement units, IMU; force plates; motion capture) do, however, have the potential to be associated with bone characteristics. Associations between bone characteristics and physical performance (e.g., high-speed distance associated with bone mass, trabecular density and cortical density, and peak speed associated with bone mass, cortical density and thickness) indicate bone is influenced by exercise intensity. For example, acceleration and total distance derived from GPS were positively correlated with bone mineral content (BMC) and tibial strength in footballers (15). Further studies have attempted to understand the relationship between physical activity and bone, although these have been performed in nonathletic populations (16–18) or associated to injury (19) rather than bone structural characteristics.
Associations between data derived from external load measuring devices and bone are not well established in an applied setting. Accelerometery data have been linked to changes in bone with vigorous physical activity being associated to higher bone mineral density (BMD) and BMC (16). Higher ground reaction forces (GRF) are linked to greater osteogenic loading (20) with GRF intensity thought to be a better predictor of BMD and skeletal adaptations than loading volume (21). IMU's are a novel approach to monitoring bone stimulus in the field utilising site-specific segmental acceleration as opposed to whole-body loading that GPS devices measure (22–24). IMeasureU (Auckland, New Zealand) offer a bone stimulus metric that combines the number of loads and magnitude of loads to predict the stimulus response of bone (22), but these claims are unsubstantiated. GPS is a more popular method to monitor external load in the field and are often used to inform rehabilitation strategies for soft tissue injuries (10) and to determine outcomes considered pertinent to performance (6), although the use of GPS metrics and their relationship to bone adaptation is unclear. Acceleration derived metrics from IMU's and GPS are often used for quantifying external load (25), yet it is not elucidated whether these measures can be associated to bone characteristics. Therefore, the efficacy of monitoring external load to gauge bone stimulus in an applied environment is not well known.
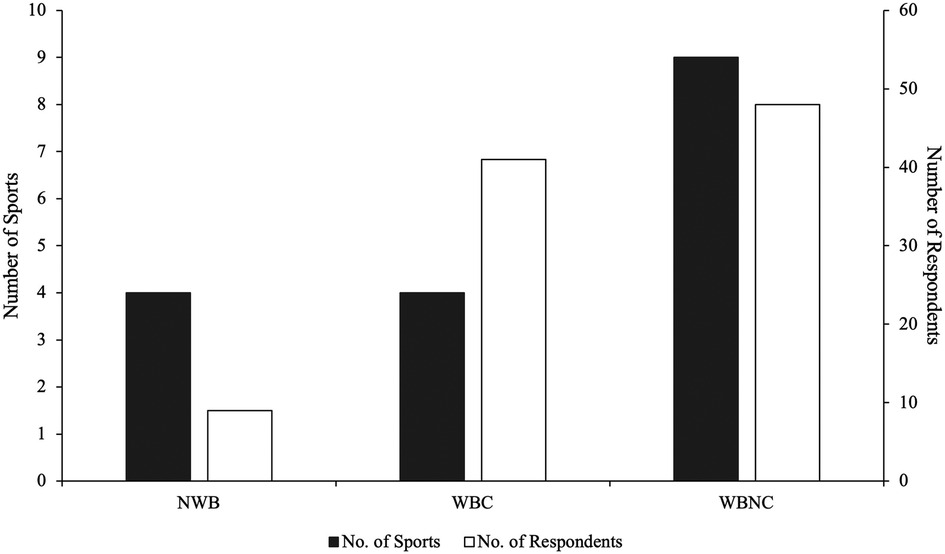
Figure 1. Number of survey respondents alongside number of sports classified into sporting conditions. Sporting conditions are classified as; non weight-bearing sports (NWB) include cycling, swimming, canoeing and rowing; weight-bearing contact sport (WBC) include Football/Soccer, Rugby, Judo and American football; weight-bearing non-contact sport (WBNC) include Cricket, Athletics, Basketball, Volleyball, Field Hockey, Baseball, Triathlon, Dance and Squash.
Bone stress injuries (BSI) are often associated with alterations within training programmes (26) and, as such, an ability to monitor external load upon the bone accurately and reliably offers the potential to support risk mitigation strategies for BSI's by helping to ensure that athletes are not exposed to sudden excessive loading cycles. It is argued that external load monitoring can be used to manage bone load and reduce the incidence of BSI, as prompt increases in load are prominent in their pathophysiology (27). Whilst this might be the case, it remains unknown to what extent athlete support staff estimate bone load, and, if they do, what methods and metrics they use to do so, given that there is no consensus on the optimal method for monitoring changes in bone.
Therefore, the aims of this study were two-fold; (1) to identify the methods used to monitor external load and ascertain if these methods are used to estimate bone load by surveying support staff, and (2) to assess the measurement tools used to estimate bone load through a narrative review.
Support staff (n = 71) from sports clubs or national governing bodies (Figure 1) were recruited worldwide (UK n = 48, 67%; Rest of Europe n = 7, 10%; North America n = 7, 10%; Australia n = 5, 7%; Africa n = 2, 3%; Asia n = 1, 1%; South America n = 1, 1%) via email or word of mouth. The role occupied by those surveyed included: Strength and Conditioning Coach (n = 29), Sports Scientist (n = 22), Physiotherapist (n = 13), Coach (n = 2), Physiologist (n = 1), Sports Therapist (n = 1), Athletic Trainer (n = 1), Researcher (n = 1) and Nutritionist (n = 1).
Participants were asked to provide informed consent and complete a survey related to external load monitoring and bone in sport between July 2020 and August 2020. The internet-based survey platform (Jisc, Bristol, UK) was used, with the survey being completed anonymously. It comprised of 19 multiple choice questions relating to external load monitoring in sport. Respondents were able to elaborate on their answer with the “Other” option if they wished to do so.
Participants met the inclusion criteria if their role involved working in a support staff capacity in an applied sporting environment. Prior to taking part in the study, each participant provided informed consent. Ethical approval was granted by the Non-Invasive Human Ethics Committee from Nottingham Trent university (126V2). The data that support the findings of this study are openly available in figshare at 10.6084/m9.figshare.21764135 or available upon request.
The survey (Appendix A) divided the topic of “external load monitoring” into two sections; (a) if/How external load is monitored and, (b) what methods/metrics are used to estimate bone load. Multiple choice and free text options were provided on the common methods identified within research for sports performance and external load quantification. Frequency based descriptive analyses were performed upon fully completed surveys.
Alongside the survey, a narrative review was performed using PubMed as a database to assess how external load is associated to bone. Google Scholar was used as a complimentary database. Articles were sourced and reviewed by two of the authors (RS, IV). The search strategy used the keywords “bone load”, “external load”, “non-invasive bone load” and “bone and exercise”. Articles were included if they met the following:
• The methodology presented in the study was non-invasive (meaning the research was performed in an applied environment and not intrusive for participants)
• Human trials only
• The loading metric used had bone health, load or injury as outcome variables.
• Fully published, peer reviewed articles
Various metrics were reported within the studies, although the methodologies adopted were consistent between each study.
The majority of support staff reported monitoring external load with their athletes (92%). For the 8% that did not monitor external load, this was primarily due to a lack of equipment (83%). The most common methods used by support staff were GPS, force plates, IMU and motion capture. Only 28% of support staff used these methods to estimate bone load, however, with 40% stating the main barrier was a lack of knowledge (Table 1).
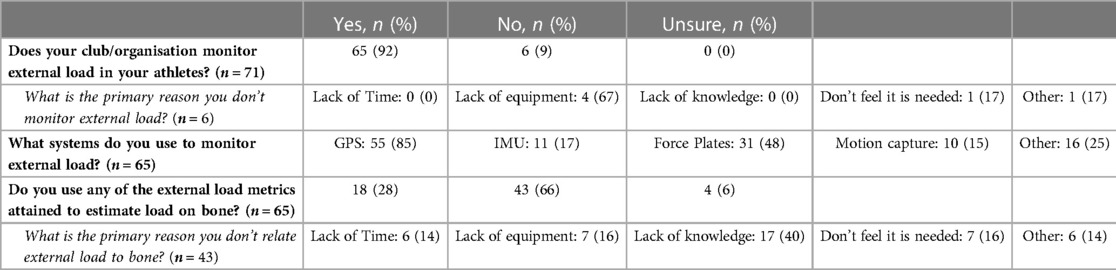
Table 1. Support staff response to using external load monitoring in sport.
GPS was the most common method for monitoring external load (n = 55, 85%) and the most commonly used to estimate bone load (n = 11, 50%). The use of GPS to inform on bone related outcomes (21%–38%) was not, however, as prevalent as the use of IMU (50%–100%) or motion capture (40%–100%) for this purpose. Force plates were reportedly well utilised to monitor external load, but the least prevalent in relation to bone related outcomes (12%; Table 2).
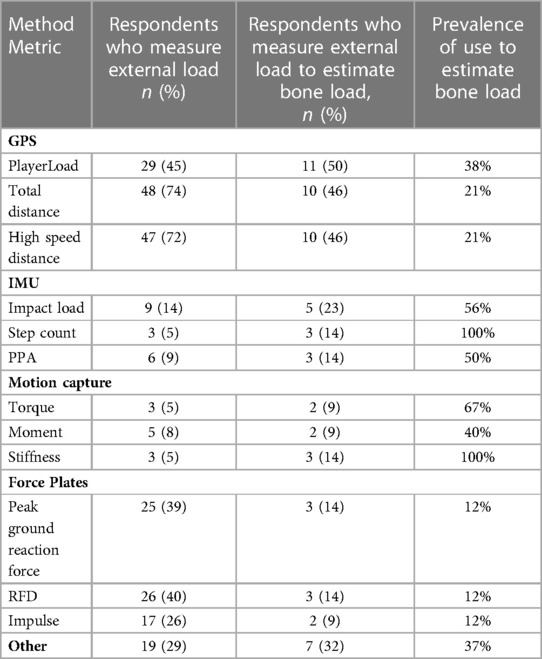
Table 2. Support staff responses to the metrics used when measuring external load and the metrics used in relation to bone.
A total of 16 articles were included in the narrative review (GPS n = 1; Force plates n = 10; IMU n = 1; Motion capture n = 4) (Table 3).
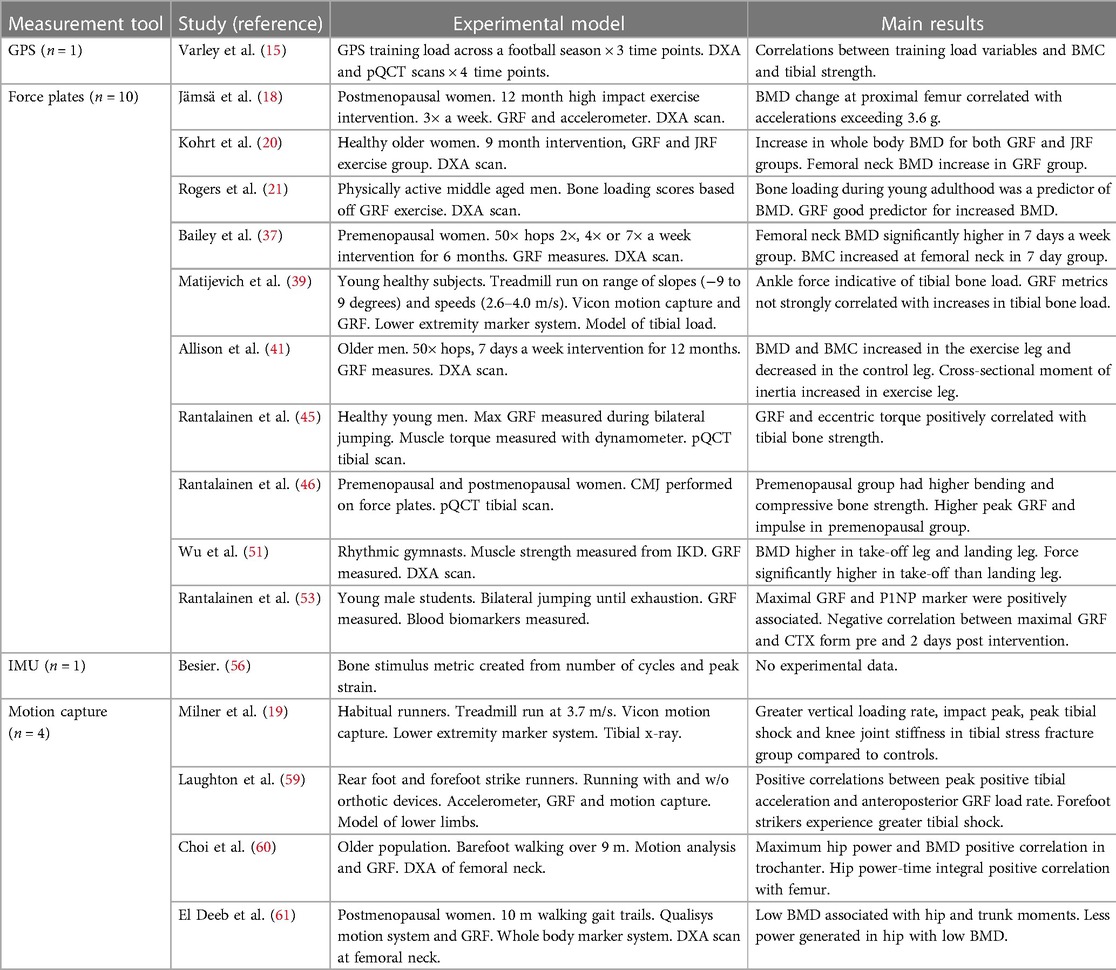
Table 3. Articles included in narrative review (n = 16).
The current study aimed to identify the methods used to monitor external load in an applied environment and ascertain if these methods were used to estimate bone load. The secondary aim of this study was to perform a narrative review to assess if any external load methods give a reflection of bone load in the literature. The key findings of the study show external load is widely monitored by support staff, primarily using GPS, force plates, IMU and motion capture (Table 1), but fewer use it to provide insight on how bone responds to exercise and training. GPS was the most often used measurement tool related bone (Table 2). Although these methods have been validated and shown to be reliable for measuring performance related variables (28, 29), the validity of associating them with changes in bone is not well established (39).
GPS was the most common method of monitoring external load used by support staff (Table 2), likely due to its capacity for real time data interpretation (30). As GPS technology has developed, micro inertial sensors (triaxial accelerometers, magnetometers, gyroscopes) have been integrated into the devices, providing support staff with a wide range of metrics to indicate external load and undertake activity profiling (31). The use of GPS has been shown to offer an accurate and reliable method to quantify the habitual movement of athletes (4), although support staff should be cautious when measuring maximal accelerations as the sampling rate of some commercially available devices used in research (∼1 Hz; GPSports, Catapult innovations) may result in missed data over a short period of time (29). Furthermore, comparing high intensity running between GPS devices may be unreliable, as differences have been shown between manufacturers (29). Therefore, high intensity metrics (i.e., high intensity running) may not be reliable between devices as a result of high coefficient of variation (32.4%) when analysing high intensity movements.
Although GPS is used to monitor physiological markers relative to performance (31), less is known about how the metrics can monitor bone. This is despite our findings that total distance and high-speed distance are commonly used to estimate the load placed upon bone by support staff (46%; Table 2), where they may assume that greater distances covered, and higher peak speeds achieved result in greater bone loading. However, bone cells desensitise to repetitive, unidirectional loading (27, 32), meaning that total distance might be a less informative metric when it comes to determining the bone stimulus. This has been reported in rats where excessive high intensity loading (14,000 loading cycles on each limb per day) did not have beneficial or detrimental effects on bone (33). There are findings in humans that are similarly suggestive (27), with low intensity running shown to half the likelihood of BSI in comparison to high intensity running at an equivalent distance. Tibial strength and BMC were positively correlated to GPS training load metrics, such as acceleration, deceleration and total distance, in professional male footballers across a season (15). This suggests dynamic, high loading movements are important for creating an osteogenic response within bone, which may be monitored using GPS. The effect sizes in this study (15) were, however, moderate to low, suggesting that the practical use of GPS to estimate bone load is yet to be established. This may be why proprietary measures are used in applied settings to assess performance.
Data are available on PlayerLoad (commercially used metric to estimate workload completed in a given period) and distance covered in relation to sports performance and fatigue (3), but there is no robust scientific evidence to suggest that these metrics can be used to estimate bone load. Despite this, our findings show that PlayerLoad is the most prevalent metric (50%; n = 11 of support staff surveyed) used to estimate bone load. Strong correlations have been shown between PlayerLoad and the rate of pulmonary oxygen uptake and heart rate within participants (.92–.98), although a mixture of positive and negative moderate correlations were shown (−.38 to .33) between participants (28). Therefore, comparing PlayerLoad between athletes may not be reliable due to the variability of the measurement. The variability between participants suggests external differences in PlayerLoad may not reflect differences of internal load. Another issue with the reproducibility of PlayerLoad results from the ambiguity surrounding the measurement (34). This ambiguity stems from the inconsistent definitions presented within the literature surrounding the metric, resulting in a lack of clarity between studies (35, 36). Some research defines the variable as a vector magnitude representing the sum of accelerations from each direction (35), whereas others define it as being the instantaneous change in rates of resultant accelerations over time representing the acceleration load for an activity (36). Thus, this limits the application of PlayerLoad as a tool for monitoring external load as well as using this as a metric to estimate bone load. Research needs to clearly present how PlayerLoad is being calculated in order to offer a standardised and reproducible metric for support staff to understand.
A clear limitation of GPS devices is the sensor location, which is commonly positioned between the shoulder blades. The range of reliability statistics of positioning a GPS at the scapulae (ICC: .60–.93, CV: 4.%6–18.2%) compared to the centre of mass (ICC: .65–.97, CV: 3.6%–14.7%) shows a moderate to high test-retest reliability for both locations (28). However, wearing the device at the scapulae can underestimate some metrics (i.e., PlayerLoad) due to the lack of sensitivity to subtle movements during high-speed running (28). Stress related bone injuries occur predominantly in the lower limbs (26) and, therefore, measuring load at the scapula may not be a valid method for understanding the forces experienced in the lower limbs due to the greater distance from ground contact. Associations between GPS derived metrics and bone characteristics are not well established. The 21%–38% of support staff who relate GPS metrics to bone should do so with caution as there is no clear evidence on how the derived metrics can be used in relation to bone outcomes. This dearth of robust scientific data should be addressed by researchers as soon as possible.
Force plates were reported to be the second most utilised method for measuring external load within the current survey (n = 31, 48%). Force plates are mechanical sensing systems that measure GRF's when contact is made with an external force (i.e., an athlete) and can be used to gather kinetic data. Support staff often use these devices within a gym environment to measure the effects of training programmes. Despite only ∼14% of support staff using GRF in relation to bone, researchers have shown associations between GRF and bone load/mechanical stimuli (20, 21).
The femoral neck, trochanter and Ward's triangle have shown an increase in BMD when daily impacts and accelerations are more frequent over a 12-month exercise intervention (18). Increases in BMD at the femoral neck have also been shown with 7 day a week hopping, offering a greater increase to BMD than hopping for 2 days or 4 days, with exposure to GRF's being the only difference between groups (37). This could be important for offering guidelines on exercise induced bone load without increasing exposure to injury. Internal forces acting upon bone are higher than surrogate measures, such as GRF, but the accessibility of GRF's means they can be used as a guide for the intensity of internal bone loading during defined exercises (41). Weight bearing exercise (walking, jogging and stair climbing) has been shown to increase BMD more than resistance training (20). This was associated with having a higher loading force and faster loading rate when performing weight bearing activity. Although this demonstrates that BMD may increase with loading, the range of load and how varying loads influence bone characteristics have not been investigated. Exercise intensity may be more important than exercise frequency for bone accrual (21). Classifying bone load into categories: 0 (GRF 1 × bodyweight); 1 (GRF between 1 and 2 × bodyweight); 2 (GRF between 2 and 4 × bodyweight) and 3 (GRF > 4 × bodyweight) has shown greater bone load (category 3) has a positive linear relationship with whole-body BMD and a positive effect on skeletal health in later life (21). The applicability of this scoring system in relation to bone load is questioned due to two points; (1) the lack of validity surrounding the biomechanical GRF (38) and (2) the retrospective measure of physical activity across the lifespan. As far as the current authors are aware there is no validation for the GRF scores relevant to bone loading and, therefore, although it might be a solid concept, it cannot be truly classified as being a bone loading metric. Furthermore, as is highlighted in the study (21), the recall of physical activity across the lifespan from a middle-aged population is likely to have significant error, which will have affected the bone loading metric. The lack of assessment for diet, hormonal status and use of medication across adolescence and adulthood, which can all effect bone, also contribute to the lack of validity of comparing bone load to bone status. Using GRF in this format has potential to inform on intervention strategies in an applicable and simple technique but further validation of GRF in relation to bone load needs to be examined for it to be attempted as a predictor of skeletal adaptation.
Contrastingly, GRF's have been shown to be misleading for monitoring load in relation to bone. Research has shown that GRF does not correlate with tibial load as it does not account for muscular contraction (39). GRF's are not representative of internal multi-axial stress and may have little influence on the mechanical behaviour of bone relative to loading magnitude (40). Although muscular force applies the highest load on bone, GRF's still account for ∼30% of bone load (39), thus it is argued that it can still be used as a guide to the relative intensity of internal bone load during hopping exercises (41). Overall, GRF is associated to changes in bone within exercise interventions. The studies are often performed on nonathletic populations (i.e., post-menopausal women or adolescents) as opposed to athletes, so there are limited data that can be applied to the active athlete.
The ability to create a high force rapidly during muscular contractions may be a relevant measurement to inform on bone adaptations due to the functional link between muscle and –bone, in which both biological structures directly influence one another (42, 43). Rate of Force Development (RFD) is reportedly used by ∼14% of staff (n = 3) who use force plates to estimate bone load. The incorporation of time-based analysis makes the measure more indicative of neuromuscular performance, as opposed to peak force which may be more indicative of movement strategies (44). Neuromuscular performance has been associated with bone strength (45) as tibial strength was higher in those that produce greater eccentric torque, as well as predicting bone strength in pre- and postmenopausal women (46). Muscular forces impose a large load on bone demonstrated by the associations shown between bone growth and muscle growth (47). Therefore, using RFD alongside other GRF derived metrics may be advantageous to assess adaptations in bone (48), as muscular forces influence bone characteristics. There is evidence of muscle disuse and reuse causing changes to bone mass (49) and positive correlations are frequently reported between muscle mass and bone mass (50). The impracticality of measuring RFD in an applied setting is a possible drawback. Force plates are challenging to employ within sports that have spontaneous movement patterns, thus somewhat limiting the applied use of the method.
Impulse is the product of a resultant force and the duration of this force. Impulse was used by ∼9% (n = 2) of support staff who use external load monitoring in relation to bone. Impulse incorporates neuromuscular performance and body mass and has been shown to have a strong linear association with maximal power. Neuromuscular performance, represented by impulse, has been related to skeletal robusticity (skeletal strength relative to body size) through a regression model (46) with a 1% improvement in impulse associating to a 0.5% increase in skeletal robusticity. This is proposed as an alternative to using body mass alone as a predictor of skeletal robusticity, thus longitudinal measurements (i.e., CoM accelerations) may offer better estimates of bone load. The sample comparison of skeletal robusticity between active premenopausal women and inactive postmenopausal women favours the active population in bone strength (46). Therefore, to understand the effects of neuromuscular performance to estimate bone load it would make sense to examine healthy athletes alongside a less active population of a similar age. Greater impulse during a leaping take-off in rhythmic gymnasts was associated with higher BMD at the femur and bone strength at the knee extensors/flexors when compared with the contralateral side that imposed a lower force (51). Furthermore, the increment attained from impulse during a CMJ strongly correlated to an increase in hip and lumbar bone mass accretion (52), demonstrating that impulse has been associated to bone characteristics in research.
Force plate metrics have been used during a variety of exercise interventions to monitor load and the effects it has on bone. However, the validity and reliability of them to determine bone load has not been shown in applied sporting environments. The logistical challenges of this method mean that it cannot be implemented in day-to-day training for most sports, but, based upon the current literature, those who can do this should consider using force plates for monitoring adaptations to bone as higher GRF has been associated to greater bone accrual (53).
IMU's were the second most used method to estimate bone load with impact load, step count and PPA (Table 2). IMU's are small, moveable devices that provide a large amount of data to collect, process, analyse and report (54). They offer a viable option as they can be used in an applied setting, due to their small size and light weight, and can be mounted on specific anatomical locations to measure segmental external loading. This allows segmental information, such as the tibia, to be gathered, which is not the case with GPS or force plates. Segmental accelerations are shown to have a weak relationship with centre of mass accelerations (55), which highlights the importance of knowing what it is the user is wanting to measure so the correct measurement tool can be chosen.
IMU's have been shown to reliably monitor impact load, step count, and step intensity during dynamic team sport tasks (22), although no studies have investigated IMU metrics in relation to bone. Bone specific metrics have been developed within IMU devices (56). A surrogate measure of bone stress labelled “bone stimulus” represents the cumulative nature of impacts and predict the mechanical stimuli responsible for bone remodelling (22), however there is no published evidence of the IMU metrics correlating with actual changes in bone.
Using IMUs on anatomical positions unspecific to the area of interest may lead to less accurate results for the movements being performed (57). Therefore, it is essential that the location of the IMU devices are accurate when using loading metrics to understand the effect sport specific tasks have on bone. Overall, a small amount (17%) of support staff use IMUs, however the prevalence of those that do use IMUs to estimate bone load is high (Table 2), which shows the applicability of the method. As further research is undertaken, the relevance of IMU devices for monitoring external load in the field, and their association to bone characteristics will become clearer.
The application of motion capture, particularly 3D analysis techniques, can create predictive models of movement patterns that may reduce injury likelihood (58). Unfortunately, motion capture is not widely employed to monitor external load by support staff, although we have shown that when it is used, the prevalence of use in relation to bone is relatively high (Table 2). In theory, this technique can offer the greatest insight into the load being applied to bone due to its ability to create internal models of the musculoskeletal system, but the application is limited in most sporting environments as this method is time consuming and does not provide real time feedback.
The metrics Torque (n = 2; 9.1%), Moments (n = 2; 9.1%) and Stiffness (n = 3; 13.6%) were used by support staff to monitor external load. Higher knee joint stiffness can create higher loading rates that have been strongly associated with the estimation of bone load (19, 38, 59), which may be why support staff use stiffness as an informative metric. Kinetic data significantly correlates with BMD in elderly women, but not men, during walking and hip power-time and maximal hip power can predict 25.4% of femoral neck BMD (60). This finding was supported by a decrease in hip power correlating with a decrease in BMD in postmenopausal women (61). However, these studies only assessed habitual walking, and therefore it could be suggested that dynamic, high intensity sporting movements may offer additional increases in BMD at specific locations since running is likely to result in greater mechanical loading compared to walking (62). Comparatively, these increases are shown to be 2-9% higher in bone compression and tension, and 10-26% higher in shear stress, when running compared to walking (62). This increase can be used to harness a positive adaptation in bone and minimise injury risk by creating training programmes that expose athletes to gradual increases in load. Therefore, the findings (60, 61) suggest metrics derived from motion capture may offer informative data relative to changes in bone and the beneficial effect loading can have on special populations.
The use of motion capture by support staff to inform themselves on bone related outcomes is low. This is likely due to the time-consuming nature and expertise required for both data collection and data analysis. For these reasons motion capture techniques are mainly used by researchers as opposed to support staff. However, the development of marker less motion capture may widen the opportunity to integrate motion capture systems into applied environments.
The responses collected offer a general consensus for support staff working alongside athletes in an applied setting. The support staff were responsible for a large number of athletes (1,000+) across 5 continents with the majority (85%) competing at a national/international level therefore the authors are confident the sample is representative of support staff working in an elite environment. Recall bias may have impacted the answers supplied by the support staff. As those who completed the survey were all currently active at their organisations, however, the recall bias should be minimal, given the fact that they would have been largely referring to current practices. This study was exploratory in attempting to understand how external load is monitored in relation to bone. As such, the survey tool used was not validated, although this is offset by the novelty of the research approach.
Despite the commonality of BSI being acknowledged (71%) by support staff in the survey, few support staff monitor external load to estimate bone load. Excessive loading is known to contribute to BSI, therefore monitoring and acting upon an athletes external load to estimate bone load may help reduce the burden of BSI. This study shows the number of support staff monitoring external load, what equipment/metrics they use and if they use those metrics to estimate bone load. There are a variety of methods that are available to support staff to inform on bone characteristics in their environments, however each of these methods are acknowledged to have their limitations which must be considered by support staff before implementing the methods.
The findings show external load monitoring is commonly used in sporting environments but is seldom used to estimate bone load. There is no consistent measurement tool or metric that is invariably applied in relation to bone by support staff or within research. GPS is the most commonly used method to estimate bone load by support staff, but there is a lack of research associating GPS metrics with bone load. Accelerometry based data were shown to be the most prevalent method in relation to bone, but lacked generic popularity amongst support staff. Force plates were reported to be the second most popular method for monitoring external load (48%), but the least prevalent to estimate bone load. The application of the methods to estimate bone load within applied environments is challenging due to the cost, time and expertise of the methods. Research exploring the most applied methods for monitoring external load to estimate bone load in applied environments are recommended.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical approval was granted by the Non-Invasive Human Ethics Committee from Nottingham Trent University (126V2). Participants were asked to provide informed consent and complete a survey related to external load monitoring and bone in sport between July 2020 and August 2020.
All authors contributed to conception and design of the study. RS organised the database. RS performed the data analysis. RS wrote the first draft of the manuscript. RS wrote sections of the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fspor.2023.1150052/full#supplementary-material.
1. Impellizzeri FM, Marcora SM, Coutts AJ. Internal and external training load: 15 years on. Int J Sports Physiol Perform. (2019) 14(2):270–73. doi: 10.1123/ijspp.2018-0935
2. Bourdon PC, Cardinale M, Murray A, Gastin P, Kellmann M, Varley MC, et al. Monitoring athlete training loads: consensus statement. Int J Sports Physiol Perform. (2017) 12(s2):S2–161. doi: 10.1123/IJSPP.2017-0208
3. Halson SL. Monitoring training load to understand fatigue in athletes. Sports Med. (2014) 44(2):139–47. doi: 10.1007/s40279-014-0253-z
4. Vanrenterghem J, Nedergaard NJ, Robinson MA, Drust B. Training load monitoring in team sports: a novel framework separating physiological and biomechanical load-adaptation pathways. Sports Med. (2017) 47(11):2135–142. doi: 10.1007/s40279-017-0714-2
5. Newton MD, Owen AD, Baker JS. Monitoring external and internal training loads: relationships with injury risk in professional soccer: a review. EC Orthop. (2019) 10(8):686–97.
6. Mooney M, O’Brien B, Cormack S, Coutts A, Berry J, Young W. The relationship between physical capacity and match performance in elite Australian football: a mediation approach. J Sci Med Sport. (2011) 14(5):447–52. doi: 10.1016/j.jsams.2011.03.010
7. Heishman AD, Curtis MA, Saliba E, Hornett RJ, Malin SK, Weltman AL. Noninvasive assessment of internal and external player load: implications for optimizing athletic performance. J Strength Cond Res. (2018) 32(5):1280–87. doi: 10.1519/JSC.0000000000002413
8. Gabbett TJ, Ullah S. Relationship between running loads and soft-tissue injury in elite team sport athletes. J Strength Cond Res. (2012) 26(4):953–60. doi: 10.1519/JSC.0b013e3182302023
9. Bacon CS, Mauger AR. Prediction of overuse injuries in professional u18-u21 footballers using metrics of training distance and intensity. J Strength Cond Res. (2017) 31(11):3067–76. doi: 10.1519/JSC.0000000000001744
10. Burgess DJ. The research doesn’t always apply: practical solutions to evidence-based training-load monitoring in elite team sports. Int J Sports Physiol Perform. (2017) 12(s2):S2–136. doi: 10.1123/ijspp.2016-0608
11. West SW, Clubb J, Torres-Ronda L, Howells D, Leng E, Vescovi JD, et al. More than a metric: how training load is used in elite sport for athlete management. Int J Sports Med. (2020) 42(04):300–06. doi: 10.1055/a-1268-8791
12. Borresen J, Lambert MI. The quantification of training load, the training response and the effect on performance. Sports Med. (2009) 39(9):779–95. doi: 10.2165/11317780-000000000-00000
13. Yang PF, Bruggemann GP, Rittweger J. What do we currently know from in vivo bone strain measurements in humans. J Musculoskelet Neuronal Interact. (2011) 11(1):8–20.21364270
14. Szulc P, Naylor K, Hoyle NR, Eastell R, Leary ET. Use of CTX-I and PINP as bone turnover markers: national bone health alliance recommendations to standardize sample handling and patient preparation to reduce pre-analytical variability. Osteoporos Int. (2017) 28:2541–56. doi: 10.1007/s00198-017-4082-4
15. Varley I, Ward M, Thorpe C, Beardsley N, Greeves J, Sale C, et al. External training load is associated with adaptation in bone and body composition over the course of a season in elite male footballers. Bone Rep. (2022) 18:101643. doi: 10.1016/j.bonr.2022.101643
16. Marin-Puyalto J, Mäestu J, Gómez-Cabello A, Lätt E, Remmel L, Purge P, et al. Frequency and duration of vigorous physical activity bouts are associated with adolescent boys’ bone mineral status: a cross-sectional study. Bone. (2019) 120:141–47. doi: 10.1016/j.bone.2018.10.019
17. Heikkinen R, Vihriälä E, Vainionpää A, Korpelainen R, Jämsä T. Acceleration slope of exercise-induced impacts is a determinant of changes in bone density. J Biomech. (2007) 40(13):2967–74. doi: 10.1016/j.jbiomech.2007.02.003
18. Jämsä T, Vainionpää A, Korpelainen R, Vihriälä E, Leppäluoto J. Effect of daily physical activity on proximal femur. Clin Biomech. (2006) 21(1):1–7. doi: 10.1016/j.clinbiomech.2005.10.003
19. Milner CE, Ferber R, Pollard CD, Hamill J, Davis IS. Biomechanical factors associated with tibial stress fracture in female runners. Med Sci Sports Exerc. (2006) 38(2):323. doi: 10.1249/01.mss.0000183477.75808.92
20. Kohrt WM, Ehsani AA, Birge SJ Jr. Effects of exercise involving predominantly either joint-reaction or ground-reaction forces on bone mineral density in older women. J Bone Miner Res. (1997) 12(8):1253–61. doi: 10.1359/jbmr.1997.12.8.1253
21. Rogers RS, Hinton PS. Bone loading during young adulthood predicts bone mineral density in physically active, middle-aged men. Phys Sportsmed. (2010) 38(2):146–55. doi: 10.3810/psm.2010.06.1793
22. Armitage M, Beato M, McErlain-Naylor SA. Inter-unit reliability of IMU step metrics using IMeasureU blue trident inertial measurement units for running-based team sport tasks. J Sports Sci. (2021) 39(13):1512–18. doi: 10.1080/02640414.2021.1882726
23. Wiig H, Raastad T, Luteberget LS, Ims I, Spencer M. External load variables affect recovery markers up to 72 h after semiprofessional football matches. Front Phys. (2019) 10:689. doi: 10.3389/fphys.2019.00689
24. Pino-Ortega J, Rojas-Valverde D, Gómez-Carmona CD, Bastida-Castillo A, Hernández-Belmonte A, García-Rubio J, et al. Impact of contextual factors on external load during a congested-fixture tournament in elite U’18 basketball players. Front Psychol. (2019) 10:1100. doi: 10.3389/fpsyg.2019.01100
25. Gabbett TJ. The training—injury prevention paradox: should athletes be training smarter and harder? Br J Sports Med. (2016) 50(5):273–80. doi: 10.1136/bjsports-2015-095788
26. Fredericson M, Jennings F, Beaulieu C, Matheson GO. Stress fractures in athletes. Top Magn Reson Imaging. (2006) 17(5):309–25. doi: 10.1097/RMR.0b013e3180421c8c
27. Warden SJ, Edwards WB, Willy RW. Preventing bone stress injuries in runners with optimal workload. Curr Osteoporos Rep. (2021) 19(3):298–307. doi: 10.1007/s11914-021-00666-y
28. Barrett S, Midgley A, Lovell R. Playerload™: reliability, convergent validity, and influence of unit position during treadmill running. Int J Sports Physiol Perform. (2014) 9(6):945–52. doi: 10.1123/ijspp.2013-0418
29. Coutts AJ, Duffield R. Validity and reliability of GPS devices for measuring movement demands of team sports. J Sci Med Sports. (2010) 13(1):133–35. doi: 10.1016/j.jsams.2008.09.015
30. Theodoropoulos JS, Bettle J, Kosy JD. The use of GPS and inertial devices for player monitoring in team sports: a review of current and future applications. Orthop Rev. (2020) 12(1):7863. doi: 10.4081/or.2020.7863
31. Malone JJ, Lovell R, Varley MC, Coutts AJ. Unpacking the black box: applications and considerations for using GPS devices in sport. Int J Sports Physiol Perform. (2017) 12(s2):S2–18. doi: 10.1123/ijspp.2016-0236
32. Burr DB, Robling AG, Turner CH. Effects of biomechanical stress on bones in animals. Bone. (2002) 30(5):781–86. doi: 10.1016/S8756-3282(02)00707-X
33. Yingling VR, Davies S, Silva MJ. The effects of repetitive physiologic loading on bone turnover and mechanical properties in adult female and male rats. Calcif Tissue Int. (2001) 68(4):235–9. doi: 10.1007/s00223-001-0007-4
34. Bredt S, Chagas M, Peixoto G, Menzel H, de Andrade A. Understanding player load: meanings and limitations. J Hum Kinet. (2020) 71(1):5–9. doi: 10.2478/hukin-2019-0072
35. Castillo D, Weston M, McLaren SJ, Cámara J, Yanci J. Relationships between internal and external match-load indicators in soccer match officials. Int J Sports Physiol Perform. (2017) 12(7):922–27. doi: 10.1123/ijspp.2016-0392
36. Schelling X, Torres L. Accelerometer load profiles for basketball-specific drills in elite players. J Sports Sci Med. (2016) 15(4):585. 27928203.27928203
37. Bailey CA, Brooke-Wavell K. Optimum frequency of exercise for bone health: randomised controlled trial of a high-impact unilateral intervention. Bone. (2010) 46(4):1043–49. doi: 10.1016/j.bone.2009.12.001
38. Groothausen J, Siemer H, Kemper HC, Twisk J, Welten DC. Influence of peak strain on lumbar bone mineral density: an analysis of 15-year physical activity in young males and females. Pediatr Exerc Sci. (1997) 9(2):159–73. doi: 10.1123/pes.9.2.159
39. Matijevich ES, Branscombe LM, Scott LR, Zelik KE. Ground reaction force metrics are not strongly correlated with tibial bone load when running across speeds and slopes: implications for science, sport and wearable tech. PLoS One. (2019) 14(1):e0210000. doi: 10.1371/journal.pone.0210000
40. Loundagin LL, Schmidt TA, Edwards WB. Mechanical fatigue of bovine cortical bone using ground reaction force waveforms in running. J Biomech Eng. (2018) 140(3):031003. doi: 10.1115/1.4038288
41. Allison SJ, Folland JP, Rennie WJ, Summers GD, Brooke-Wavell K. High impact exercise increased femoral neck bone mineral density in older men: a randomised unilateral intervention. Bone. (2013) 53(2):321–28. doi: 10.1016/j.bone.2012.12.045
42. Schoenau E. From mechanostat theory to development of the” functional muscle-bone-unit”. J Musculoskelet Neuronal Interact. (2005) 5(3):232. ISSN: 11087161.16172514
43. Ashe MC, Liu-Ambrose TYL, Cooper DML, Khan KM, McKay HA. Muscle power is related to tibial bone strength in older women. Osteoporos Int. (2008) 19(12):1725–32. doi: 10.1007/s00198-008-0655-6
44. Lombard W, Starling L, Wewege L, Lambert M. Changes in countermovement jump performance and subjective readiness-to-train scores following a simulated soccer match. Eur J Sport Sci. (2020) 21(5):647–55. doi: 10.1080/17461391.2020.1757764
45. Rantalainen T, Heinonen A, Komi PV, Linnamo V. Neuromuscular performance and bone structural characteristics in young healthy men and women. Eur J Appl Physiol. (2008) 102(2):215–22. doi: 10.1007/s00421-007-0575-8
46. Rantalainen T, Nikander R, Heinonen A, Multanen J, Häkkinen A, Jämsä T, et al. Neuromuscular performance and body mass as indices of bone loading in premenopausal and postmenopausal women. Bone. (2010) 46(4):964–69. doi: 10.1016/j.bone.2010.01.002
47. Ruff C. Growth in bone strength, body size, and muscle size in a juvenile longitudinal sample. Bone. (2003) 33(3):317–29. doi: 10.1016/S8756-3282(03)00161-3
48. Mosti MP, Carlse T, Aas E, Hoff J, Stunes AK, Syversen U. Maximal strength training improves bone mineral density and neuromuscular performance in young adult women. J Strength Cond Res. (2014) 28(10):2935–45. doi: 10.1519/JSC.0000000000000493
49. Sievänen H, Heinonen A, Kannus P. Adaptation of bone to altered loading environment: a biomechanical approach using x-ray absorptiometric data from the patella of a young woman. Bone. (1996) 19(1):55–9. doi: 10.1016/8756-3282(96)00111-1
50. Macdonald H, Kontulainen S, Petit M, Janssen P, McKay H. Bone strength and its determinants in pre-and early pubertal boys and girls. Bone. (2006) 39(3):598–608. doi: 10.1016/j.bone.2006.02.057
51. Wu J, Ishizaki S, Kato Y, Kuroda Y, Fukashiro S. The side-to-side differences of bone mass at proximal femur in female rhythmic sports gymnasts. J Bone Miner Res. (1998) 13(5):900–6. doi: 10.1359/jbmr.1998.13.5.900
52. Vicente-Rodriguez G, Ara I, Perez-Gomez J, Serrano-Sanchez JA, Dorado C, Calbet JA. High femoral bone mineral density accretion in prepubertal soccer players. Med Sci Sports Exerc. (2004) 36(10):1789–95. doi: 10.1249/01.MSS.0000142311.75866.D7
53. Rantalainen T, Heinonen A, Linnamo V, Komi PV, Takala TE, Kainulainen H. Short-term bone biochemical response to a single bout of high-impact exercise. J Sports Sci Med. (2009) 8(4):553. 24149597.24149597
54. Rojas-Valverde D, Gómez-Carmona CD, Gutiérrez-Vargas R, Pino-Ortega J. From big data mining to technical sport reports: the case of inertial measurement units. BMJ Open Sport Exerc Med. (2019) 5(1):e000565. doi: 10.1136/bmjsem-2019-000565
55. Nedergaard NJ, Robinson MA, Eusterwiemann E, Drust B, Lisboa PJ, Vanrenterghem J. The relationship between whole-body external loading and body-worn accelerometry during team-sport movements. Int J Sports Physiol Perform. (2017) 12(1):18–26. doi: 10.1123/ijspp.2015-0712
56. Besier T. Bone stimulus (2019). Available at: https://imeasureu.com/wp-content/uploads/2019/10/IMU_Bone_Stimulus.pdf
57. Tan T, Chiasson DP, Hu H, Shull PB. Influence of IMU position and orientation placement errors on ground reaction force estimation. J Biomech. (2019) 97:109416. doi: 10.1016/j.jbiomech.2019.109416
58. Hewett TE, Myer GD, Ford KR, Heidt RS Jr, Colosimo AJ, McLean SG, et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med. (2005) 33(4):492–501. doi: 10.1177/0363546504269591
59. Laughton CA, Davis IM, Hamill J. Effect of strike pattern and orthotic intervention on tibial shock during running. J Appl Biomech. (2003) 19(2):153–68. doi: 10.1123/jab.19.2.153
60. Choi W, Choi JH, Chung CY, Sung KH, Lee KM. Can gait kinetic data predict femoral bone mineral density in elderly men and women aged 50 years and older? J Biomech. (2021) 123:110520. doi: 10.1016/j.jbiomech.2021.110520
61. El Deeb AM, Khodair AS. Three-dimensional analysis of gait in postmenopausal women with low bone mineral density. J Neuroeng Rehabil. (2014) 11(1):1–7. doi: 10.1186/1743-0003-11-1
Keywords: external load, elite sport, bone load, qualitative, measuring devices
Citation: Scott R, James R, Barnett CT, Sale C and Varley I (2023) Perspectives from research and practice: A survey on external load monitoring and bone in sport. Front. Sports Act. Living 5:1150052. doi: 10.3389/fspor.2023.1150052
Received: 23 January 2023; Accepted: 28 March 2023;
Published: 25 April 2023.
Edited by:
Randall L. Jensen, Northern Michigan University, United StatesReviewed by:
Matthew A. Wyon, University of Wolverhampton, United Kingdom© 2023 Scott, James, Barnett, Sale and Varley. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Reece Scott cmVlY2Uuc2NvdHRAbnR1LmFjLnVr
†These authors have contributed equally to this work and share first authorship
‡These authors share senior authorship
§These authors share last authorship
Specialty Section: This article was submitted to Elite Sports and Performance Enhancement, a section of the journal Frontiers in Sports and Active Living
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.