 Myoung-Hwee Kim
Myoung-Hwee Kim Chiao-I Lin
Chiao-I Lin Tilman Engel
Tilman Engel Michael Cassel
Michael Cassel- University Outpatient Clinic, Sports Medicine & Sports Orthopaedics, University of Potsdam, Potsdam, Germany
Exercise interventions are evident in the treatment of mid-portion Achilles tendinopathy (AT). However, there is still a lack of knowledge concerning the effect of different exercise treatments on improving a specific function (e.g., strength) in this population. Thus, this study aimed to systematically review the effect of exercise treatments on different functional outcomes in mid-portion AT. An electronic database of Pubmed, Web of Science, and Cochrane Central Register of Controlled Trials were searched from inception to 21 February 2023. Studies that investigated changes in plantar flexor function with exercise treatments were considered in mid-portion AT. Only randomized controlled trials (RCTs) and clinical controlled trials (CCTs) were included. Functional outcomes were classified by kinetic (e.g., strength), kinematic [e.g., ankle range of motion (ROM)], and sensorimotor (e.g., balance index) parameters. The types of exercise treatments were classified into eccentric, concentric, and combined (eccentric plus concentric) training modes. Quality assessment was appraised using the Physiotherapy Evidence Database scale for RCTs, and the Joanna Briggs Institute scale for CCTs. The search yielded 2,260 records, and a total of ten studies were included. Due to the heterogeneity of the included studies, a qualitative synthesis was performed. Eccentric training led to improvements in power outcomes (e.g., height of countermovement jump), and in strength outcomes (e.g., peak torque). Concentric training regimens showed moderate enhanced power outcomes. Moreover, one high-quality study showed an improvement in the balance index by eccentric training, whereas the application of concentric training did not. Combined training modalities did not lead to improvements in strength and power outcomes. Plantarflexion and dorsiflexion ROM measures did not show relevant changes by the exercise treatments. In conclusion, eccentric training is evident in improving strength outcomes in AT patients. Moreover, it shows moderate evidence improvements in power and the sensorimotor parameter “balance index”. Concentric training presents moderate evidence in the power outcomes and can therefore be considered as an alternative to improve this function. Kinematic analysis of plantarflexion and dorsiflexion ROM might not be useful in AT people. This study expands the knowledge what types of exercise regimes should be considered to improve the functional outcomes in AT.
Introduction
Achilles tendinopathy is a type of degenerative tendon disease that causes functional impairment and morbidity (1). According to epidemiological data, a prevalence of 2.16 cases per 1,000 patient-years was estimated in the general population and 6.2%–9.5% in athlete population (2, 3). According to its anatomical location, it is divided into two primary categories: insertional, which occurs at the calcaneus Achilles tendon junction, and mid-portion, which occurs 2–6 cm proximal to the calcaneus (4). The characteristic of mid-portion tendinopathy is diffuse or localized swelling, degenerated tendon morphology and pain caused by repetitive loading without adequate compensation of the plantar flexor muscle function (1, 5).
In consequence, one of the most effective management strategies for mid-portion AT have been proposed to be exercise-based therapy (6). To date, several exercise interventions have been reported for AT, such as the “Alfredson protocol” which is also known as heavy eccentric calf training (7), concentric training (8), the “Stanish protocol” (9), and the “Silbernagel protocol” (10). These interventions can be classified as three different loading protocols: eccentric, concentric, and combined (eccentric plus concentric) training, respectively. Among those, eccentric loading has emerged as one of the primary conservative approaches for AT rehabilitation over the past twenty years. It is hypothesized to influence the formation in carboxyterminal propeptide of type I collagen, boosting tendon volume and tensile strength (11, 12). Eccentric exercises may also have the potential to reduce the neovascularization and related nerve ingrowth being responsible for pain development (13). A recent meta-analysis examined the relationship between eccentric exercise treatments and tendon volume in healthy and pathological tendons (14). In healthy tendons no significant immediate volume changes following acute exercise interventions were apparent. In pathological tendons, immediate and short-term volume reductions were reported, while no long-term adaptations were found as investigated in one study only. Based on the limited number of studies examining long-term changes in tendon morphology, the proclaimed effect of eccentric training on tendon volume remains inconclusive (14).
Research indicates that both concentric and combined exercise treatments can also be effective in improving plantar flexor functions such as power (e.g., height of countermovement jump) (10) in the AT population, which is believed to occur through the strengthening of the affected tendon (9). Therefore, it remains unclear whether the effects of eccentric loading are different from other types of loadings, such as slow concentric loading (15). The primary cause for these similar adaptations may be explained by the “time-under-tension” hypothesis, which states that positive adaptations could be achieved regardless of contraction type, as long as the mechanical strain is performed slowly and heavy enough (16, 17). Since the tendinopathic regions can be subjected to mechanical strain that restores normal fibril alignment and cell morphology, different types of loading may have a comparable impact to eccentric exercise.
In conclusion, different types of exercise treatments have reported positive findings in varying functional outcomes in addition to eccentric training (8–10). Nevertheless, there is a lack of knowledge concerning the effect of specific exercise treatments for improving specific functional outcomes (e.g., strength) in mid-portion AT. Being able to differentiate the effects of different types of exercises on functional outcomes might allow for more tailored treatment in people with AT. Therefore, the purpose of this systematic review was to analyze the effect of various exercise treatments (eccentric, concentric, combined) on different functional outcomes (strength, power, range of motion, balance) in people with mid-portion AT.
Methods
Data sources and search criteria
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used to conduct and report this study (18). The electronic databases Pubmed, Web of Science, and Cochrane Central Register of Controlled Trials were searched for relevant studies from inception to 21 February 2023. The search was performed by combining the three main categories: intervention, pathology, and anatomical location (Table 1 shows the search terms used in Pubmed). Each search term was mapped to the “title and abstract” heading that has this feature in the databases. Quotation marks were not used to allow any word variations. Filters such as article type (clinical trial, RCTs, etc.) and language (English) were also applied. Animal studies were excluded using a filter or adding the Boolean operator “NOT” if there was no filter for this. This study was not pre-registered.
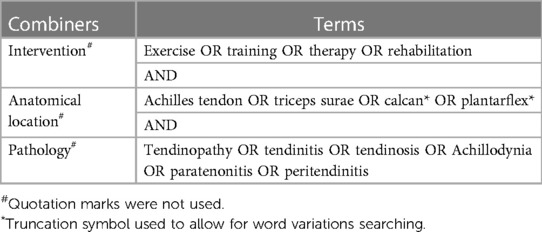
Table 1. Search terms used in pubmed.
Eligibility criteria
Studies investigating direct functional measures of kinetic, kinematic, and sensorimotor outcomes were included following exercise treatments in mid-portion AT (mean age ≥18 years) diagnosed by clinical or sonography method. The kinetic parameters included analysis of forces such as strength (5), power, or ground reaction force outcomes. The kinematic parameters included outcomes of segmental movement characteristics such as joint moments, angles, positions, accelerations, velocities, or range of motion [ROM] (10). The sensorimotor parameters included any sensorimotor-related analysis such as balance (8), reflex, or muscle activity measures. Studies that measured a minimum of one outcome in kinetic, kinematic or sensorimotor parameters with exercise interventions were considered. Exercise interventions that were prescribed with specific guidelines (e.g., volume, type, progression, and training period) that loaded the Achilles tendon for more than four weeks were considered. The interventions might be described as eccentric, concentric, combined (eccentric & concentric), or isometric training. At least one group should have conducted an exercise intervention as a single treatment. Other non-exercise treatments (e.g., manual therapy, injections, electrotherapy, etc.) were not considered, including sports activity, and co-interventions with exercise treatments were also excluded. Studies that did not measure the outcomes at the end point of an exercise intervention were excluded to minimize biases. Included study designs were randomized controlled trials (RCTs) or controlled clinical trials (CCTs).
Study selection
Once all the searched articles were combined in an Excel file, two authors (MHK, CIL) independently screened titles and abstracts for eligibility based on the inclusion and exclusion criteria. After the procedure, the remaining articles underwent full-text reviews to determine the final inclusion. The corresponding authors were contacted for inaccessible articles to acquire the full text. During the process, disagreements between the authors were resolved by discussion.
Methodological quality assessment
The Physiotherapy Evidence Database (PEDro) scale was used to assess the quality of the RCTs. This scale has shown good validity and reliability in evaluating RCTs (19). The PEDro scale consists of 11 criteria. Without the first criterion asking about the eligibility of a respective study, the rest 10 criteria were calculated for the total score. Studies with scores of ≥6 were considered “high-quality”, 4–5 were considered “medium-quality”, and scores <4 were considered “low-quality” (20).
For assessing non-randomized clinical controlled trials (CCTs), the Joanna Briggs Institute (JBI) non-randomized experimental studies tool was used. This tool has 9 criteria to assess the quality of studies. There is no standardized total scoring for the tool. Hence, same as the PEDro scale, studies were classified as “high-quality”, “medium-quality”, and “low-quality” based on the score criteria explained above.
Two reviewers (MHK, CIL) assessed the methodological quality independently, and discrepancies were resolved by discussion. In the case of unreached agreements, the third reviewer (JH) was involved.
Data extraction
Two reviewers (MHK, CIL) independently extracted data using a standardized form. Characteristics including study information (i.e., author, year, design), participant [i.e., sample size, sex, mean age (years), mean duration of symptoms, diagnosis method of AT], interventions (i.e., duration, type of intervention, sets/repetitions, frequency, progression, pain allowance during exercise), outcomes of function measures (name, scale), and results [mean ± standard deviation (SD), p-value] were extracted. If there was no applicable mean and SD, mean difference (MD) and confidence interval (CI) were extracted. For studies that did not provide any numeric data, at least p-values were taken. Disagreements between the authors were resolved by discussion.
Data synthesis and analysis
A qualitative synthesis was performed to analyze the change of plantar flexor function measures due to the clinical heterogeneity of outcome parameters and exercise interventions. Subgroup analysis was performed according to exercise intervention types [eccentric, concentric, and combined (eccentric plus concentric) training]. To enable synthesis of outcome parameters within each pre-defined category (i.e., kinetic, kinematic, sensorimotor), outcomes were sub-categorized by task features (e.g., strength, power, balance index) considering the exercise treatments applied. Where studies covered several relevant tasks, the results from the single study were categorized accordingly. Finally, the levels of evidence (21) based on the methodological quality assessment was added. To indicate changes in the outcomes, delta changes from pre to post exercise were calculated in percentage (%) where possible.
Results
Study selection
The search found a total of 2,260 studies which excluded 329 duplicates by automatic title matchings and 37 more duplicates were removed by manual confirmation using Excel. Following 1,867 articles were excluded by the title and abstract screening process. The remaining 27 articles were gone through a full-text eligibility check. Among them, 9 studies were removed due to inappropriate outcome parameters, 1 study for not providing no original data, 3 studies for missing responses from the authors, 1 study for no suitable study design, 2 studies for no suitable subjects, and 1 study for co-intervention allowance. Six corresponding authors were contacted for inaccessible articles, and three authors provided the full text. Finally, 10 articles were included in this study (Figure 1). Detailed information on the included and excluded articles is shown in the Supplementary File S2.
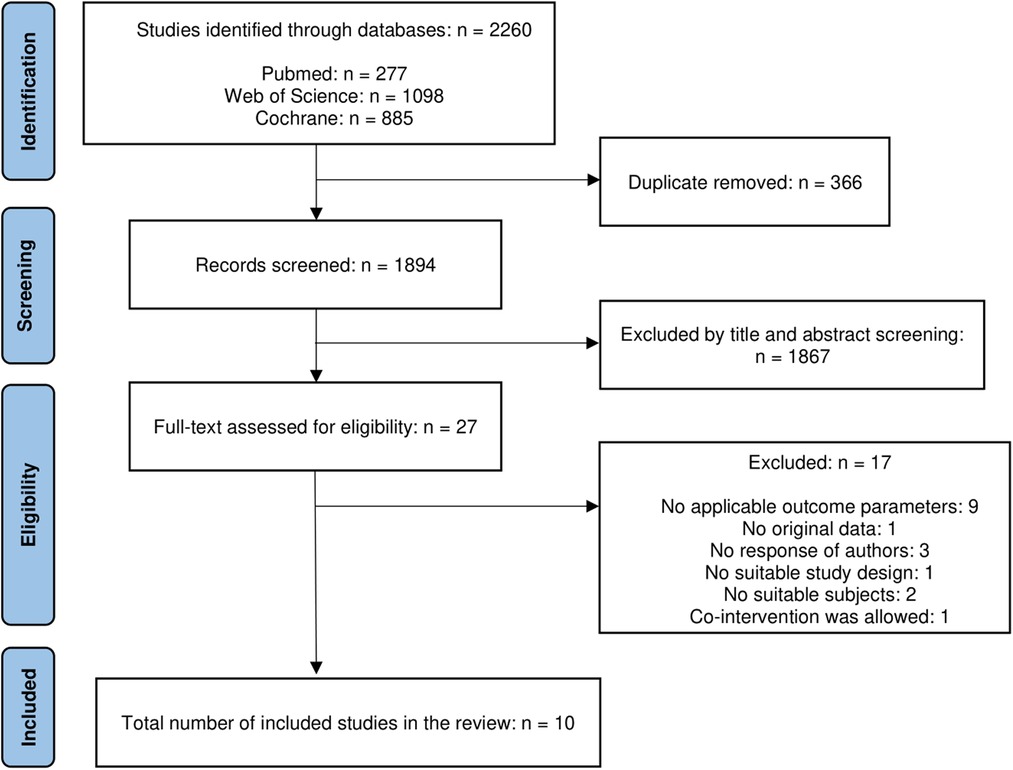
Figure 1. Study selection flowchart according to the PRISMA statements.
Methodological quality
A total of eight RCTs studies were included (8–10, 22–27). The mean quality score of the PEDro scale was 6 ± 0.83 points, ranging from 5 to 7 points. Six studies were ranked as high-quality (67%) (8, 10, 22, 24–26), and three studies were medium-quality (33%) (9, 23, 27). All the eight studies performed blinding of the assessors but blinding of therapists was performed by two studies covering the group assignments (8, 26). Blinding of subjects was not conducted in all the studies due to the nature of exercise treatments. Subjects' allocation was concealed by two studies (25–27), whereas six studies acquired data from more than 85% of subjects initially allocated to the groups (8–10, 22, 24, 26) (Table 2).
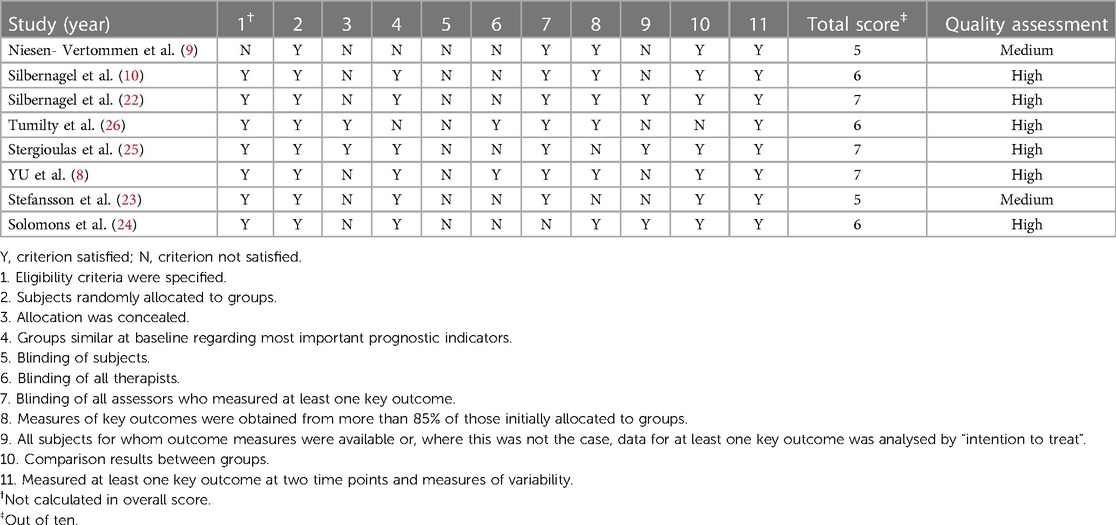
Table 2. Physiotherapy evidence database (PEDro) scale assessment for randomized controlled trials (RCTs).
In comparison to the RCTs, two CCTs were appraised (7, 28). The mean quality score was 7, and both studies scored 7 points that were ranked as high-quality (100%). These studies clearly stated the effect of exercise treatments with pre- and post-measurements. The outcomes were measured in a reliable way using machine devices, and it was measured in the same way for the intervention and control groups. However, none of the studies were satisfied with conducting appropriate statistical analysis because the number and type of dependent and independent variables were not considered (Table 3).
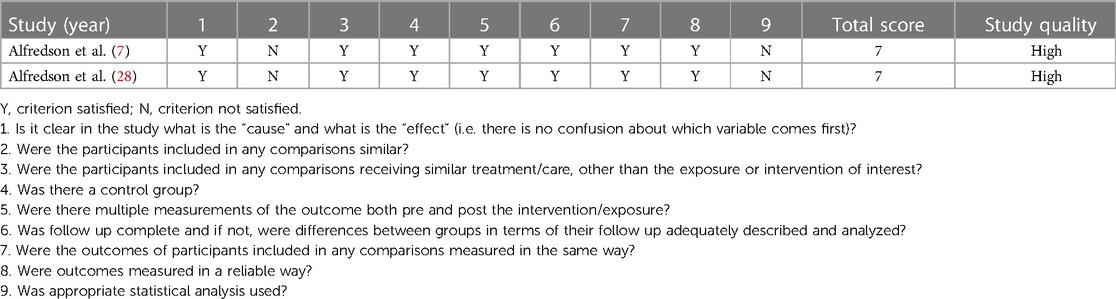
Table 3. Joanna briggs institute (JBI) non-randomized experimental studies tool assessment for clinical controlled trials (CCTs).
Characteristics of included studies
The total number of females and males was 48 (24%) and 137 (68%), respectively, with 16 (8%) unknown sex. The mean age of the subjects was 38 years, ranging from 20 ± 2 years (8) to 48 ± 7 years (22). Seven studies reported their subjects were in their 40 s (7, 10, 22–24, 26, 28), whereas one study reported them to by in their 30 s (9) and the other two in their 20 s (8, 25). The mean duration of symptoms was 16.5 months, ranging from 3.7 ± 1 (9) to 48 ± 6.8 months (22), except one study that did not report the symptom duration (26). Ultrasonography was performed to diagnose AT with or without the clinical methods in six studies (7, 8, 22, 23, 25, 28), whereas the other four studies only utilized the clinical methods (9, 26), such as reported pain (10, 24). The detailed characteristics of the included studies are summarized in Tables 5.
Characteristics of exercise treatments
The exercise treatments used in the included studies can be categorized into three types based on the loading mode: eccentric, concentric, and combined training. Eccentric exercise was widely applied in 6 studies (7–9, 23, 25, 26, 28), concentric training was applied in 3 studies (8–10), and combined training was also applied in 3 studies (10, 22, 24). Among the eccentric training protocols, three studies applied the “Alfredson protocol” (7, 26, 28), while the others implemented “supervised eccentric training” (8, 25), “modified Alfredson protocol” (23), and “Stanish and Curwin protocol” (9). There were no other special names used for the concentric mode training protocols. Combined training protocols were named the “Silbernagel protocol” or “physiotherapy exercise protocol” that mainly utilized the combination of eccentric and concentric contraction modes. The intervention period was mostly 12 weeks, except for two studies that implemented an 8 week training intervention period (8, 25). The overview of the exercise treatment types is summarized in Table 4.
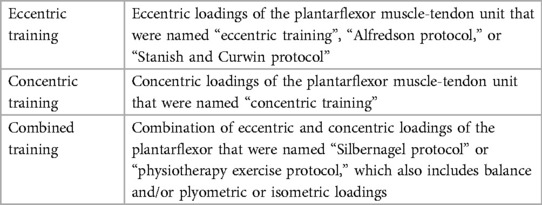
Table 4. Overview of the exercise treatment types that have been included in this study.
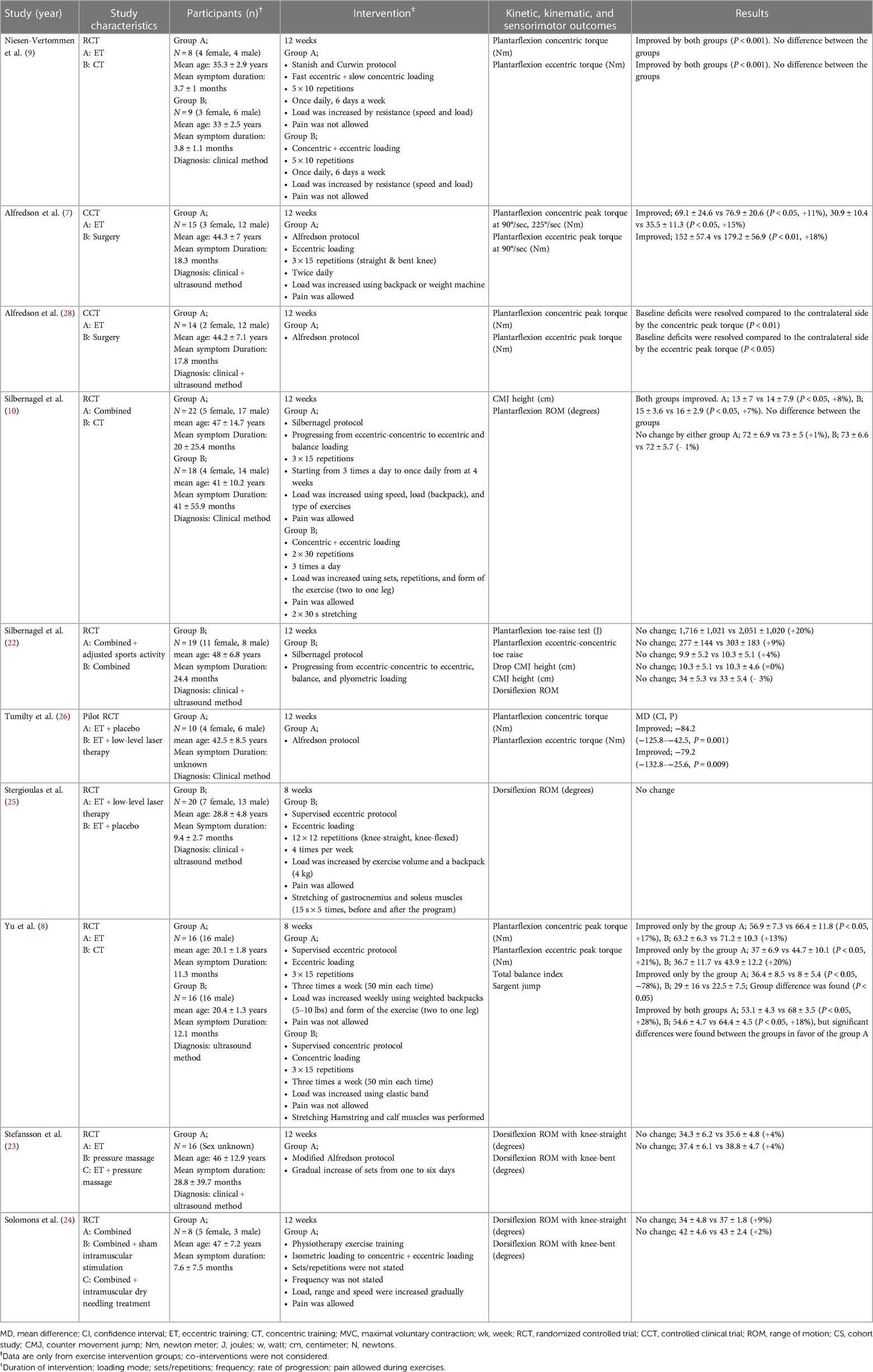
Table 5. Characteristics of the included studies.
Kinetic parameters
Plantar flexor strength
Two high-quality studies using eccentric training showed significant improvements in concentric & eccentric torque at 12 weeks measurement point (26), concentric peak torque at 90°/sec (+11%) & at 225°/sec (+15%), and eccentric peak torque at 90°/sec (+18%) (7). One high-quality study also showed improvements in concentric (+17%) & eccentric (+21%) peak torque at 8 weeks by eccentric training (8). Moreover, one medium-quality study with eccentric training reported an improvement in concentric & eccentric torque at 12 weeks (9). One high-quality study showed the baseline eccentric & concentric peak torque deficits were resolved when compared with the contralateral side by eccentric training at 12 weeks (28). One medium-quality study using concentric training showed an improvement in concentric & eccentric torque at 12 weeks (9), whereas one high-quality study reported an insignificant improvement in concentric (+13%) & eccentric (+20%) peak torque at 8 weeks (8). One high-quality study with combined training reported an insignificant improvement in toe-raise test at 12 weeks (+20%) (22).
Plantar flexor power
One high-quality study using eccentric training showed an improvement (+28%) in sargent jump at 8 weeks (8). Two high-quality studies using concentric training showed improvements (+18%) in sargent jump at 8 weeks (8), and countermovement jump (+7%) at 12 weeks (10). One high-quality study with combined training reported an improvement (+8%) in countermovement jump (10), whereas one high-quality study showed an insignificant improvement in eccentric-concentric toe raise (+9%), drop countermovement jump (+4%), and countermovement jump (=0%) at 12 weeks (22).
Kinematic parameters
Ankle range of motion
One high-quality (25) showed no change in dorsiflexion ROM at 8 weeks by eccentric training, and one moderate-quality study (23) reported insignificant improvement dorsiflexion ROM in knee-straight (+4%) and knee-bend positions (+4%) by eccentric training at 12 weeks. By use of concentric training one high-quality study reported insignificant decrease in plantarflexion ROM (−1%) at 12 weeks (10). Three high-quality studies with combined training reported insignificant improvement in plantarflexion ROM (+1%) (10), insignificant decrease in dorsiflexion ROM (−3%) (22), and insignificant improvement in knee-straight (+9%) and knee-bend (+2%) dorsiflexion ROM (24) at 12 weeks.
Sensorimotor parameters
Balance index
One high-quality study using eccentric training showed an improvement (−78%) in total balance index, while concentric training showed an insignificant improvement (−22%) at 8 weeks (8).
Discussion
The purpose of this systematic review was to analyze the effect of various exercise treatments (eccentric, concentric, combined) on different functional outcomes (strength, power, range of motion, balance) in the subjects of mid-portion AT. A variety of exercise interventions were categorized into eccentric, concentric, and combined training modes, and the effects on functional outcomes were investigated. In kinetic parameters, eccentric training showed moderate to strong evidence in power and strength outcomes, respectively. Concentric training showed conflicting evidence in strength outcomes but moderate evidence in power outcomes. Combined training revealed moderate evidence of no improvement in strength outcomes and conflict evidence of power outcomes. Concerning kinematic parameters, only plantarflexion and dorsiflexion ROM measures were available by the exercise treatments that no study reported improvements. Regarding sensorimotor parameters, eccentric training showed moderate evidence in the balance index. In contrast, moderate evidence of insignificant improvement was revealed by concentric training. There was no study that applied combined training to measure a sensorimotor parameter.
Kinetic parameters with the exercise treatments
For improving kinetic parameters of strength outcomes such as peak torque or power outcomes such as height of sargent jump, eccentric training was found to have strong and moderate evidence, respectively. For subjects who are not responsive to this type of loading training, however, concentric training could be an option since moderate evidence was found to improve power outcomes. Nevertheless, eccentric training should be the primary choice to improve power outcomes as the high-quality RCT study that directly compared supervised eccentric training vs. concentric training showed a significant difference of the sargent jump in favor of the eccentric training group, despite the concentric training group has significantly improved after the training (8). The possibility of greater mechanical load from eccentric loading over concentric loading has been proposed (8), as eccentric loading may cause the tendon to extend more and result in greater mechanical strain on the tendon (29–31). However, the actual efficacy of eccentric over concentric loading for improving kinetic parameters in AT remains inconclusive. It is argued that positive adaptations can be achieved through heavy mechanical strain regardless of the type of contraction (16, 17). Additional research has demonstrated that eccentric loadings do not cause more stress on the Achilles tendon compared to concentric exercises, suggesting that this mechanism may not be a contributing factor (32). In eccentric training, stimulating collagen synthesis and remodeling in the tendon were suggested as one possible hypothesis (33) which might eventually lead to an increased plantar flexor strength capacity, and pain reduction was deemed to be involved with tendon structure re-organization mechanism (12). Contrarily, a recent systematic review (34) and the overall inference from the available literature (35) support the idea that tendon structure does not change considerably during the course of treatment and the alterations do not lead to improvements in pain or function (34). Together, these findings imply that clinical advancements during rehabilitation take place via a mechanism different from structural adaptation. One other hypothesis is the elimination of new blood vessels in the tendon that may contribute to pain (12, 36). During the heel-drop eccentric loadings, the flow in the neovessels was stopped when compared to the resting position. Thus, the effect of cessations might directly affect the neovessels which were relevant for the resolution of pain (12, 36). Regarding concentric training, it is possible that this form of loading increases blood flow and oxygen delivery to the Achilles tendon that may enhance healing (37). In conclusion, both of the training regimes could bring positive improvements to kinetic parameters for AT, but further high-quality studies are required to confirm the effects with concentric training.
The result of no improvement in strength outcomes and conflicting evidence of power outcomes by combined training was unexpected because it is generally believed to bring more advantages compared to isolated eccentric or concentric training since contraction mode is known to affect training gains (38). Nevertheless, these results may be explained by the aberrant neural commands that are seen in AT due to the pathological condition (39). The eccentric and concentric combined contractions are similar to the movements that are involved in daily walking or running, since they incorporate stretch-shortening cycles (SSC). SSC is defined as pre-activated muscle contraction that undergoes an eccentric lengthening followed by a concentric contraction (40). It increases mechanical overload on the tendon through elevated stress. During SSC, Achilles tendon force reached 12.5 times as body weight (41), generating tendon strain as low as 4.1% to as high as 12.8% (42, 43). By nature, the Achilles tendon always undergoes SSC during functional tasks. However, the uncoordinated motor activities in AT (39) could impose higher stress on the Achilles tendon (44, 45) following this kind of activity. Thus, the combined exercise treatment, like the “Silbernagel protocol” (22), may not be as effective as eccentric loading protocols in improving kinetic outcomes.
Kinematic parameters with the exercise treatments
This study identified the lack of kinematic outcome parameters except for the outcome of plantarflexion and dorsiflexion ROM by the exercise treatments in five studies (10, 22–25) that reported no improvements. Although decreased ankle dorsiflexion is regarded as natural history following the onset of AT (46), the assessment of the ankle ROM to analyze the effect of exercise treatments requires caution in this population. There were studies that showed increased dorsiflexion ROM as a risk factor for AT that may impose higher loads on the Achilles tendon (47). In contrast, with currently available evidence, it is unclear whether decreased ankle ROM after an exercise treatment represents a functional improvement in AT. In this review, one study measured plantarflexion (10), and four studies examined dorsiflexion ROM following the exercise treatments (22–25). Since no significant changes were reported, the assessment of ankle ROM may not be a defining factor of recovery in AT. However, from a clinical point of view, a higher ankle ROM can be caused by higher compliancy of the tendon, which may be a sign of impaired loading capacity. Overall, the limited availability of kinematic outcome parameters, in line with the uncertainty in the role of ankle ROM in exercise treatments for mid-portion AT, highlights the need for more comprehensive evaluations for future studies.
Sensorimotor parameters with the exercise treatments
In terms of the sensorimotor outcome parameters, only the total balance index measurement was available from one high-quality RCT study that compared eccentric training to concentric training (8). While the eccentric training showed an improvement, the concentric training showed no notable change, which resulted in a significant group difference. Under eccentric contractions, the muscle is actively extended through external stress, which differs from concentric contractions in several neurological ways (48, 49). Motor unit discharge rates were more varied during eccentric contractions than concentric contractions (50), which is derived from the high motor unit discharge rate variability, and selective recruitment of motor unit threshold. This supports the belief that eccentric loadings inspire different patterns of brain activity compared to concentric loadings, suggesting a distinct neuromuscular processing strategy. According to Latella et al. (2019), the long-lasting influence on the cortical process by eccentric loading reflects the complexity of the motor control required to conduct the movements (51). That means eccentric contractions require challenging motor control (52), which provokes the neuromuscular system more than concentric contractions. During eccentric contractions, cortical excitability appears to be heightened, and a larger brain region seems to be engaged (53).
Limitations
There were a couple of limitations of the study. One limitation was the stage of the tendon pathology. The continuum model of tendon pathology was suggested by Cook and Purdam (1), and thereby diagnostic subgroups might have existed between the included studies (relatively short duration of symptom [3.7 months (9)], and low age [in the 20 s (8, 25)] compared to the other studies).
It is also worth mentioning the modalities of exercise treatments. There were exercise protocols engaged in both eccentric and concentric loading components, but those protocols were named as either “eccentric” or “concentric” training following the mainstream of the loading mode (9, 10). Moreover, the combined training protocols also have involved balance (10, 22), plyometric (22, 54), and isometric (24) loading components. These combinations of training modes make it difficult to determine which type of loading protocol is beneficial for which type of functional outcomes.
Moreover, the present study excluded the endurance measurements such as heel raise tests that counting the number of repetitions a subject can perform until experiencing fatigue or discomfort. It was deemed unsuitable for inclusion since it does not directly assess the pre-defined categories of kinetic, kinematic, or sensorimotor parameters. However, future research may consider to include this test to provide a more comprehensive overview of the effect of different exercise treatments on various functional outcomes in mid-portion AT.
Lastly, this study has illustrated the need for assessing outcome measures in the kinematic and sensorimotor outcome parameters. Measurements in broad outcome variables, including joint moments, angles, and positions in the kinematic parameter, and reflex and muscle activities in the sensorimotor parameter with exercise treatments will provide a clear picture of what loading types should be considered to improve these functional outcomes.
Clinical implications
It is worth to underline the total volume reduced eccentric training protocol (8). Unlike the traditional Alfredson protocol (7), which is widely accepted as the gold standard of exercise treatment for AT subjects, the total volume reduced eccentric training was conducted three times a week for eight weeks but showed significant improvements in strength, power, and balance outcomes (8). Being considered the time efficiency and the burden of compliance with the Alfredson protocol, the result is certainly meant for the subjects. The Alfredson protocol requires a high amount of training volume, but there is no rationale for this much training volume (55). It can be extra work and even can induce delayed-onset muscle soreness. Future studies should consider applying total volume reduced eccentric training protocol with the outcomes of kinetic and sensorimotor parameters.
During exercise interventions, the pain was not a required feature since the studies showed improvements in the functional outcomes without allowance of pain (8, 9). In contrast, Alfredson protocol (7) allows some degree of pain while conducting the protocol. Although it is debatable whether pain should be allowed during an exercise intervention to lead to a functional improvement, training-induced pain ought to be informed for subjects before conducting any exercise treatments.
Conclusion
This is the first study to investigate the effect of different exercise treatments on the different functional outcome parameters in mid-portion AT. Eccentric training showed moderate to strong evidence in the kinetic parameters of power and strength outcomes, respectively. Also, moderate evidence was found in the sensorimotor parameters of the balance index through eccentric training. Concentric training showed moderate evidence in the power outcomes, so it could be considered for the subjects who are not responsive to eccentric training to improve this function. In contrast, combined training modalities did not lead to improvements in strength and power outcomes. In terms of kinematic parameters, there were only plantarflexion and dorsiflexion ROM measures examined showing no changes by different training modes (eccentric, concentric, and combined). Thus, ankle ROM measurement is not recommended with the subjects of mid-portion AT. This study identified supportive evidence of eccentric training in the functional outcomes of strength and power as well as the sensorimotor ability “balance index”. Concentric training modalities can be considered optional in order to improve the outcome of power. Future studies applying the different training modalities with kinematic outcome parameters such as joint moments and angles instead of plantarflexion and dorsiflexion ROM will expand the knowledge what types of exercise treatments should be considered to improve the function.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
MHK: Conceptualization, data curation, formal analysis, investigation, methodology, project administration, resources, roles/writing - original draft, and writing - review & editing. CIL: data curation and investigation. JH and AQ: methodology and writing - review & editing. TE: conceptualization and writing - review & editing. MC: conceptualization, writing - review & editing, resources, project administration, and project supervision. All authors contributed to the article and approved the submitted version.
Funding
Deutsche Forschungsgemeinschaft (DFG, German Research Foundation) — Projektnummer 491466077.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fspor.2023.1144484/full#supplementary-material.
References
1. Cook JL, Rio E, Purdam CR, Docking SI. Revisiting the continuum model of tendon pathology: what is its merit in clinical practice and research? Br J Sports Med. (2016) 50:1187–91. doi: 10.1136/bjsports-2015-095422
2. Albers IS, Zwerver J, Diercks RL, Dekker JH, van den Akker-Scheek I. Incidence and prevalence of lower extremity tendinopathy in a Dutch general practice population: a cross sectional study. BMC Musculoskelet Disord. (2016) 17(1):16. doi: 10.1186/s12891-016-0885-2
3. Lopes AD, Hespanhol LC, Yeung SS, Costa LOP. What are the main running-related musculoskeletal injuries? Sports Med. (2012) 42(10):891–905. doi: 10.1007/BF03262301
4. Singh A, Calafi A, Diefenbach C, Kreulen C, Giza E. Noninsertional tendinopathy of the Achilles. Foot Ankle Clin. (2017) 22(4):745–60. doi: 10.1016/j.fcl.2017.07.006
5. van der Vlist AC, Breda SJ, Oei EHG, Verhaar JAN, de Vos RJ. Clinical risk factors for Achilles tendinopathy: a systematic review. Br J Sports Med. (2019) 53(21):1352–61. doi: 10.1136/bjsports-2018-099991
6. Murphy MC, Travers MJ, Chivers P, Debenham JR, Docking SI, Rio EK, et al. Efficacy of heavy eccentric calf training for treating mid-portion Achilles tendinopathy: a systematic review and meta-analysis. Br J Sports Med. (2019) 53(17):1070–7. doi: 10.1136/bjsports-2018-099934
7. Alfredson H, Pietilä T, Jonsson P, Lorentzon R. Heavy-load eccentric calf muscle training for the treatment of chronic Achilles tendinosis. Am J Sports Med. (1998) 26(3):360–6. doi: 10.1177/03635465980260030301
8. Yu J, Park D, Lee G. Effect of eccentric strengthening on pain, muscle strength, endurance, and functional fitness factors in male patients with achilles tendinopathy. Am J Phys Med Rehabil. (2013) 92(1):68–76. doi: 10.1097/PHM.0b013e31826eda63
9. Niesen-Vertommen S, Taunton J, Clement D, Mosher R. The effect of eccentric versus concentric exercise in the management of Achilles tendonitis. Clin J Sport Med. (1992) 2:109–13. doi: 10.1097/00042752-199204000-00006
10. Silbernagel KG, Thomeé R, Thomeé P, Karlsson J. Eccentric overload training for patients with chronic Achilles tendon pain—a randomised controlled study with reliability testing of the evaluation methods. Scand J Med Sci Sports. (2001) 11(4):197–206. doi: 10.1034/j.1600-0838.2001.110402.x
11. Langberg H, Ellingsgaard H, Madsen T, Jansson J, Magnusson SP, Aagaard P, et al. Eccentric rehabilitation exercise increases peritendinous type I collagen synthesis in humans with Achilles tendinosis. Scand J Med Sci Sports. (2006) 17(1):61–6. doi: 10.1111/j.1600-0838.2006.00522.x
12. Ohberg L, Alfredson H. Effects on neovascularisation behind the good results with eccentric training in chronic mid-portion Achilles tendinosis? Knee Surg Sports Traumatol Arthrosc. (2004) 12(5):465–70. doi: 10.1007/s00167-004-0494-8
13. de Vos RJ, Weir A, Tol JL, Verhaar JAN, Weinans H, van Schie HTM. No effects of PRP on ultrasonographic tendon structure and neovascularisation in chronic midportion Achilles tendinopathy. Br J Sports Med. (2011) 45(5):387–92. doi: 10.1136/bjsm.2010.076398
14. Merza E, Pearson S, Lichtwark G, Ollason M, Malliaras P. Immediate and long-term effects of mechanical loading on Achilles tendon volume: a systematic review and meta-analysis. J Biomech. (2021) 30(118):110289. doi: 10.1016/j.jbiomech.2021.110289 33556887
15. Kjaer M, Heinemeier KM. Eccentric exercise: acute and chronic effects on healthy and diseased tendons. J Appl Physiol (1985). (2014) 116(11):1435–8. doi: 10.1152/japplphysiol.01044.2013
16. Hasani F, Haines T, Munteanu SE, Schoch P, Vicenzino B, Malliaras P. LOAD-intensity and time-under-tension of exercises for men who have Achilles tendinopathy (the LOADIT trial): a randomised feasibility trial. BMC Sports Sci Med Rehabil. (2021) 13(1). doi: 10.1186/s13102-021-00279-z
17. Beyer R, Kongsgaard M, Hougs Kjær B, Øhlenschlæger T, Kjær M, Magnusson SP. Heavy slow resistance versus eccentric training as treatment for Achilles tendinopathy: a randomized controlled trial. Am J Sports Med. (2015) 43(7):1704–11. doi: 10.1177/0363546515584760
18. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. (2021) 88:105906. doi: 10.1016/j.ijsu.2021.105906
19. Yamato TP, Maher C, Koes B, Moseley A. The PEDro scale had acceptably high convergent validity, construct validity, and interrater reliability in evaluating methodological quality of pharmaceutical trials. J Clin Epidemiol. (2017) 86:176–81. doi: 10.1016/j.jclinepi.2017.03.002
20. Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. (2003) 83(8):713–21. doi: 10.1093/ptj/83.8.713
21. van Tulder M, Furlan A, Bombardier C, Bouter L. Updated method guidelines for systematic reviews in the cochrane collaboration back review group. Spine (Phila Pa 1976). (2003) 28(12):1290–9. doi: 10.1097/01.BRS.0000065484.95996.AF
22. Silbernagel KG, Thomeé R, Eriksson BI, Karlsson J. Continued sports activity, using a pain-monitoring model, during rehabilitation in patients with achilles tendinopathy: a randomized controlled study. Am J Sports Med. (2007) 35(6):897–906. doi: 10.1177/0363546506298279
23. Stefansson SH, Brandsson S, Langberg H, Arnason A. Using pressure massage for Achilles tendinopathy: a single-blind, randomized controlled trial comparing a novel treatment versus an eccentric exercise protocol. Orthop J Sports Med. (2019) 7(3). doi: 10.1177/232596711983428. Available from: https://journals.sagepub.com/doi/pdf/10.1177/2325967119834284.30915381
24. Solomons L, Lee JJY, Bruce M, White LD, Scott A. Intramuscular stimulation vs sham needling for the treatment of chronic midportion Achilles tendinopathy: a randomized controlled clinical trial. PLoS One. (2020) 15(9 September). doi: 10.1371/journal.pone.0238579
25. Stergioulas A, Stergioula M, Aarskog R, Lopes-Martins RAB, Bjordal JM. Effects of low-level laser therapy and eccentric exercises in the treatment of recreational athletes with chronic achilles tendinopathy. Am J Sports Med. (2008) 36(5):881–7. doi: 10.1177/0363546507312165
26. Tumilty S, Munn J, Abbott JH, McDonough S, Hurley DA, Baxter GD. Laser therapy in the treatment of achilles tendinopathy: a pilot study. Photomed Laser Surg. (2008) 26(1):25–30. doi: 10.1089/pho.2007.2126
27. Hasani F, Haines TP, Munteanu SE, Vicenzino B, Malliaras P. Efficacy of different load intensity and time-under-tension calf loading protocols for Achilles tendinopathy (the LOADIT trial): protocol for a randomised pilot study. Pilot Feasibility Stud. (2020) 6(1):1–12. doi: 10.1186/s40814-020-00639-5
28. Alfredson H, Nordström P, Pietilä T, Lorentzon R. Bone mass in the calcaneus after heavy loaded eccentric calf-muscle training in recreational athletes with chronic Achilles tendinosis. Calcif Tissue Int. (1999) 64(5):450–5. doi: 10.1007/PL00005827
29. Alfredson H. The chronic painful Achilles and patellar tendon: research on basic biology and treatment. Scand J Med Sci Sports. (2005) 15(4):252–9. doi: 10.1111/j.1600-0838.2005.00466.x
30. Mafi N, Lorentzon R, Alfredson H. Superior short-term results with eccentric calf muscle training compared to concentric training in a randomized prospective multicenter study on patients with chronic Achilles tendinosis. Knee surgery, sports traumatology. Arthroscopy. (2001) 9(1):42–7. doi: 10.1007/s001670000148
31. Allison GT, Purdam C. Eccentric loading for Achilles tendinopathy--strengthening or stretching? Br J Sports Med. (2009) 43(4):276–9. doi: 10.1136/bjsm.2008.053546
32. Rees JD, Lichtwark GA, Wolman RL, Wilson AM. The mechanism for efficacy of eccentric loading in Achilles tendon injury; an in vivo study in humans. Rheumatology. (2008) 47(10):1493–7. doi: 10.1093/rheumatology/ken262
33. Woodley BL, Newsham-West RJ, David Baxter G, Woodley B. Chronic tendinopathy: effectiveness of eccentric exercise. ACP J Club. (2007) 41:188–99. doi: 10.1136/bjsm.2006.029769
34. Drew BT, Smith TO, Littlewood C, Sturrock B. Do structural changes (e.g., collagen/matrix) explain the response to therapeutic exercises in tendinopathy: a systematic review. Br J Sports Med. (2014) 48(12):966–72. doi: 10.1136/bjsports-2012-091285
35. de Vos RJ, Heijboer MP, Weinans H, Verhaar JAN, van Schie HTM. Tendon structure’s lack of relation to clinical outcome after eccentric exercises in chronic midportion Achilles tendinopathy. J Sport Rehabil. (2012) 21(1):34–43. doi: 10.1123/jsr.21.1.34
36. Knobloch K, Alfredson H. Eccentric training in Achilles tendinopathy: is it harmful to tendon microcirculation? Br J Sports Med. (2007) 41(6):e2. doi: 10.1136/bjsm.2006.030437
37. Couppé C, Svensson RB, Silbernagel KG, Langberg H, Magnusson SP, … KS journal of orthopaedic, et al. Eccentric or concentric exercises for the treatment of tendinopathies? J Orthop Sports Phys Ther. (2015) 45(11):853–63. doi: 10.2519/jospt.2015.5910
38. Morrissey MC, Harman EA, Johnson MJ. Resistance training modes: specificity and effectiveness. Med Sci Sports Exerc. (1995) 27(5):648–60. doi: 10.1249/00005768-199505000-00006
39. Chang YJ, Kulig K. The neuromechanical adaptations to Achilles tendinosis. J Physiol. (2015) 593(15):3373–87. doi: 10.1113/JP270220
40. Baur H, Müller S, Hirschmüller A, Cassel M, Weber J, Mayer F. Comparison in lower leg neuromuscular activity between runners with unilateral mid-portion Achilles tendinopathy and healthy individuals. J Electromyogr Kinesiol. (2011) 21(3):499–505. doi: 10.1016/j.jelekin.2010.11.010
41. Komi P v., Fukashiro S, Jarvinen M. Biomechanical loading of Achilles tendon during normal locomotion. Clin Sports Med. (1992) 11(3):521–31. doi: 10.1016/S0278-5919(20)30506-8
42. Magnusson SP, Hansen P, Aagaard P, Brønd J, Dyhre-Poulsen P, Bojsen-Moller J, et al. Differential strain patterns of the human gastrocnemius aponeurosis and free tendon, in vivo. Acta Physiol Scand. (2003) 177(2):185–95. doi: 10.1046/j.1365-201X.2003.01048.x
43. Finni T, Hodgson JA, Lai AM, Edgerton VR, Sinha S. Nonuniform strain of human soleus aponeurosis-tendon complex during submaximal voluntary contractions in vivo. J Appl Physiol. (2003) 95(2):829–37. doi: 10.1152/japplphysiol.00775.2002
44. Grigg NL, Wearing SC, O’Toole JM, Smeathers JE. Achilles tendinopathy modulates force frequency characteristics of eccentric exercise. Med Sci Sports Exerc. (2013) 45(3):520–6. doi: 10.1249/MSS.0b013e31827795a7
45. Wyndow N, Cowan SM, Wrigley Tv, Crossley KM. Neuromotor control of the lower limb in Achilles tendinopathy: implications for foot orthotic therapy. Sports Med. (2010) 40(9):715–27. doi: 10.2165/11535920-000000000-00000
46. Becker J, James S, Wayner R, Osternig L, Chou LS. Biomechanical factors associated with achilles tendinopathy and medial tibial stress syndrome in runners. Am J Sports Med. (2017) 45(11):2614–21. doi: 10.1177/0363546517708193
47. Yeh CH, Calder JD, Antflick J, Bull AMJ, Kedgley AE. Maximum dorsiflexion increases Achilles tendon force during exercise for midportion Achilles tendinopathy. Scand J Med Sci Sports. (2021) 31:1674–82. doi: 10.1111/sms.13974
48. Duchateau J, Enoka RM. Neural control of lengthening contractions. J Exp Biol. (2016) 219(Pt 2):197–204. doi: 10.1242/jeb.123158
49. Papitsa A, Paizis C, Papaiordanidou M, Martin A. Specific modulation of presynaptic and recurrent inhibition of the soleus muscle during lengthening and shortening submaximal and maximal contractions. J Appl Physiol (1985). (2022) 133(6):1327–40. doi: 10.1152/japplphysiol.00065.2022
50. Duchateau J, Baudry S. Insights into the neural control of eccentric contractions. J Appl Physiol. (2014) 116:1418–25. doi: 10.1152/japplphysiol.00002.2013
51. Latella C, Goodwill AM, Muthalib M, Hendy AM, Major B, Nosaka K, et al. Effects of eccentric versus concentric contractions of the biceps brachii on intracortical inhibition and facilitation. Scand J Med Sci Sports. (2019) 29(3):369–79. doi: 10.1111/sms.13334
52. Perrey S. Brain activation associated with eccentric movement: a narrative review of the literature. Eur J Sport Sci. (2018) 18(1):75–82. doi: 10.1080/17461391.2017.1391334
53. Fang Y, Siemionow V, Sahgal V, Xiong F, Yue GH. Distinct brain activation patterns for human maximal voluntary eccentric and concentric muscle actions. Brain Res. (2004) 1023(2):200–12. doi: 10.1016/j.brainres.2004.07.035
54. Silbernagel KG, Thomeé R, Eriksson BI, Karlsson J, Silbernagel G. Full symptomatic recovery does not ensure full recovery of muscle-tendon function in patients with Achilles tendinopathy. Br J Sports Med. (2007) 41:276–80. doi: 10.1136/bjsm.2006.033464
Keywords: exercise treatments, eccentric training, concentric training, combined training, kinetic parameters, kinematic parameters, sensorimotor parameters, mid-portion achilles tendinopathy
Citation: Kim M-H, Lin C-I, Henschke J, Quarmby A, Engel T and Cassel M (2023) Effects of exercise treatment on functional outcome parameters in mid-portion achilles tendinopathy: a systematic review. Front. Sports Act. Living 5:1144484. doi: 10.3389/fspor.2023.1144484
Received: 14 January 2023; Accepted: 24 April 2023;
Published: 17 May 2023.
Edited by:
Giuseppe D’Antona, University of Pavia, ItalyReviewed by:
Saúl Martín Rodríguez, University of Las Palmas de Gran Canaria, SpainIker J. Bautista, Catholic University of Valencia San Vicente Mártir, Spain
© 2023 Kim, Lin, Henschke, Quarmby, Engel and Cassel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Myoung-Hwee Kim, em9raW1yb0BnbWFpbC5jb20=