
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Sports Act. Living, 02 June 2023
Sec. Injury Prevention and Rehabilitation
Volume 5 - 2023 | https://doi.org/10.3389/fspor.2023.1080356
This article is part of the Research TopicClinical Management of Sport-Related Concussion: From Diagnosis to PreventionView all 5 articles
 Shreya McLeod1,2
Shreya McLeod1,2 Ross Tucker3,4
Ross Tucker3,4 Suzi Edwards5
Suzi Edwards5 Ben Jones6,7,8,9,10Georgia Page1Mily Spiegelhalter6,8,9
Ben Jones6,7,8,9,10Georgia Page1Mily Spiegelhalter6,8,9 Stephen W. West11,12,13
Stephen W. West11,12,13 Grant L. Iverson14,15,16,17
Grant L. Iverson14,15,16,17 Andrew J. Gardner1,5,6,18*
Andrew J. Gardner1,5,6,18*
Objective: The tackle is the most injurious event in rugby league and carries the greatest risk of concussion. This study aims to replicate previous research conducted in professional men's rugby league by examining the association between selected tackle characteristics and head impact events (HIEs) in women's professional rugby league.
Methods: We reviewed and coded 83 tackles resulting in an HIE and every tackle (6,318 tackles) that did not result in an HIE for three seasons (2018–2020) of the National Rugby League Women's (NRLW) competition. Tackle height, body position of the tackler and ball carrier, as well as the location of head contact with the other player's body were evaluated. Propensity of each situation that caused an HIE was calculated as HIEs per 1,000 tackles.
Results: The propensity for tacklers to sustain an HIE was 6.60 per 1,000 tackles (95% CI: 4.87–8.92), similar to that of the ball carrier (6.13 per 1,000 tackles, 95% CI: 4.48–8.38). The greatest risk of an HIE to either the tackler or ball carrier occurred when head proximity was above the sternum (21.66 per 1,000 tackles, 95% CI: 16.55–28.35). HIEs were most common following impacts between two heads (287.23 HIEs per 1,000 tackles, 95% CI: 196.98–418.84). The lowest propensity for both tackler (2.65 per 1,000 tackles, 95% CI: 0.85–8.20) and ball carrier HIEs (1.77 per 1,000 tackles, 95% CI: 0.44–7.06) occurred when the head was in proximity to the opponent's shoulder and arm. No body position (upright, bent or unbalanced/off feet) was associated with an increased propensity of HIE to either tackler or ball carrier.
Conclusions: In the NRLW competition, tacklers and ball carriers have a similar risk of sustaining an HIE during a tackle, differing from men's NRL players, where tacklers have a higher risk of HIEs. Further studies involving larger samples need to validate these findings. However, our results indicate that injury prevention initiatives in women's rugby league should focus on how the ball carrier engages in contact during the tackle as well as how the tackler executes the tackle.
Rugby league is a full contact, collision sport involving multiple tackle events within a single game (1, 2). In Australia, the highest level of domestic competition for men is the National Rugby League (NRL). Recently, women's domestic club leagues have been created in Australia, with the National Rugby League Women's (NRLW) competition commencing in 2018, and in the United Kingdom, the Women's Super League, beginning in 2017. In women's rugby league, match concussions ranging between 2.3 concussions per 1,000 head contacts and 10.3 concussions per 1,000 match hours have been reported (3, 4). The incidence in professional women's rugby union has been reported as between 5 and 18.6 concussions per 1,000 match hours (5, 6). Since women's rugby league and union are at a relatively early stage, it is unclear whether such differences are the result of inequities in resourcing, access to facilities, skill and conditioning levels of players, opportunities to train and compete (7–9), or relatively immature injury surveillance systems (10). However, in other sports, it has been found that women are more likely to experience concussions, and exhibit greater susceptibility to concussions than men (11–14).
In the men's NRL, the tackle is the game play event associated with the greatest risk and number of concussions, with the tackler more frequently concussed than the ball carrier (1, 15–21). Video technology has been adopted by many professional sports to identify risk factors for head impacts (15, 22–25), providing insights into the mechanisms leading to concussions, which, in turn, may determine which tackle-based interventions might be introduced to reduce risk in rugby league. Head-to-head contact or head contact with a bony body part (e.g., shoulder) are the most common mechanisms for head impact events (HIEs) in concussed tacklers. Upright tackles approximating head-to-head contact result in a greater propensity for head impact events in laboratory evaluations, and video coding of game footage in rugby league and rugby union (17, 26–28). It remains unknown whether these risk factors are also present in women's rugby league. This is of particular interest because recent research has shown that NRLW players engaged in a greater mean number of tackle events per game (n = 512) (29) compared to women's rugby union players (n = 280) (30), with hookers recording the most tackles per game (n = 26.4) (31).
For the purposes of this study, an HIE is defined as a clear head impact sustained by a player in the tackle, reviewed on video footage. This approach was chosen to maximize the number of cases available for analysis, since the Head Injury Assessment (HIA) and confirmed concussion numbers across the three seasons is small. This is, therefore, a preliminary study, the first of its kind to explore mechanisms for head impact events in the NRLW, that may in the future be expanded to examine those head impact events that reach a level of clinical significance, requiring either temporary or permanent removal of player (HIA cases) or diagnosed concussions. The primary aim of the present study was to code and review video footage of tackles resulting in HIEs, including those that resulted in an HIA or a medically diagnosed concussion, in the highest level of Australian women's club rugby league.
This retrospective, case-control video analysis study was conducted in the NRLW competition over three seasons (2018–2020). At the time of analysis, the NRLW was comprised of four teams competing over four rounds. The NRLW was comprised of four teams competing over four rounds (a total of 7 games per season, for a total sample of 21 games) (32). NRLW squads are comprised of marquee, reserve grade, and under 20s players. Over the three seasons, a total of 154 unique players participated in at least one NRLW match. All players, in accordance with the NRL and Rugby League Players Association Collective Bargaining Agreement, consented a priori to the collection of their deidentified injury data, for the purposes of research. In addition, the study was approved by The University of Newcastle's Human Research Ethics Committee (H-2012-0344) and conducted in accordance with the standards of ethics outlined in the Declaration of Helsinki.
Head impact events were coded via the Stats Edge Platform (edge.stats.com). All tackle events were coded by a single analyst (SM) using a predefined coding matrix (26, 33). The analyst was trained by an experienced video analyst and researcher (AJG), who also conducted spot checks on all of the variables that were completed for the first season (i.e., 2018 NRLW season). The coding matrix comprised 36 categorical variables, the majority of which described characteristics of the tackle but also included pre-tackle characteristics (Appendix: Supplementary Table S1). The coding matrix was developed from the templates used in professional men's rugby union and previous work in men's rugby league (17, 26, 33, 34). A minimum of two camera view videos (25 fps) were available for each tackle, in normal speed and in slow motion. Every tackle event was coded across the three seasons of the NRLW competition. Tackles that did not result in an HIE (n = 6,318) formed a control sample that was used to calculate the frequency of each tackle characteristic in regular match play. This enabled calculation of the propensity of a given tackle scenario to cause an HIE In injuries per 1,000 tackles of each type and incidence, calculated as HIEs per 1,000 match hours.
A tackle event was defined as “any event where one or more tacklers attempted to stop or impede the ball carrier whether or not the ball carrier was brought to ground” (34). A ball carrier was defined as a player in possession of the ball when tackled by a tackler, including instances where the ball carrier offloaded the ball in the process of being tackled. Tacklers were defined as players attempting to impede the progress or divest an opponent in possession of the ball regardless of the outcome (e.g., incomplete tackles were included, defined as those where the defender made initial contact but missed the tackle due to physical contact with the ball carrier) (35).
In line with previous work in rugby union (27) and rugby league (26), this study focused specifically on the tackler and ball carrier's actions, reporting the body positions of the tackler and ball carrier, head contact during the tackle and the ball carrier's evasion methods. In accordance with Hopkinson and colleagues' (35) video analysis framework for the rugby league tackle, we considered variables from five out of the six “phases of the tackle” (i.e., the tackle event, defensive start point, pre-contact, initial contact, and post-contact, but we did not code any variable associated with the play-the-ball). In terms of tackler position, trunk posture has been defined as either upright (no flexion), bent at the waist (>60°) (36) or bent at the knees (>60° knee flexion), with a relatively upright torso. If a player was upright but had a significant bend in the knees (>60°), this was coded as bent at the knees. However, if the player's trunk was in greater flexion (>60°) than at the knees, this was coded as bent at the waist. Each of these components are summarised in categories for coded variables (see Supplementary File 1).
For the 2018–2020 seasons, two levels of in-game injury surveillance existed: (a) the sideline injury surveillance system via an independent medical bunker where spotters watched all matches with the specific objective of looking for signs of a concussion and (b) the club doctor. An HIE was defined as a clear head impact sustained by a player, which was monitored by sideline medical staff or the matchday video reviewer for potential follow-up in the form of an HIA. An HIA was identified as an HIE that necessitated a temporary exchange of a player with a suspected concussion for an off-field evaluation or the permanent removal of a player from the game with a confirmed concussion, as per the NRL concussion recognition and management process (18). Therefore, HIEs and HIAs differed in terms of the management approach adopted once a head impact was witnessed or via video review during the match. As described, for the analysis conducted in this study, HIEs (n = 83) have been used to ensure greater statistical power, given the low number of HIAs reported across the three seasons. Although HIAs do have an influence on game play, due to the temporary exchange or permanent removal of the player from the match, there were too few HIAs (n = 18) and medically diagnosed concussions (n = 6) to sufficiently power those analyses.
All analyses were conducted using IBM SPSS Statistics for Windows, version 24 (IBM Corp., Armonk, N.Y., USA). The event risk or propensity, in HIEs per 1,000 tackles for each tackle characteristic, was calculated by dividing the number of HIEs occurring from that tackle characteristic by the total number of occurrences of that tackle characteristic (obtained from the control cohort) and multiplying by one thousand. The incidence of HIEs was calculated as the number of HIEs per 1,000 hours of match play, and the period in matches per HIE for each tackle characteristic calculated. All results are presented as means and 95% confidence intervals (CIs). The probability of each tackle characteristic being associated with a player sustaining an HIE was assessed using Poisson regression with a log link function, using exposure to the characteristic as the offset variable to compare predictor/independent variables. Incident rate ratios (IRRs) were calculated to compare the propensity of two events by expressing the calculated HIE propensity relative to one another; 95% CIs were used based on the Poisson distribution and a difference was deemed to be significant if the 95% limits did not overlap (33).
All tackles during the 3 years of the NRLW (2018–2020) competition were coded. Eighty-three HIEs were identified, of which 18 were HIAs, and 6 were medically diagnosed concussions. The control cohort comprised the 6,318 non HIE-tackles. Overall HIE tackle propensity was 12.9 (95% CI: 10.4–16.0) HIEs per 1,000 tackles, with one HIE in a tackle every 30 min (95% CI: 3.9–6.0). Forty-two and 39 HIEs occurred to tacklers and ball carriers, respectively. The remaining two HIEs occurred in open play, i.e., off the ball contact. Tackler HIE propensity was 6.6 (95% CI: 4.9–8.9) per 1,000 tackles, similar to that observed for ball carriers (6.1, 95% CI: 4.5–8.4) per 1,000 tackles.
Of the 18 HIAs, tacklers experienced 8 HIAs with a propensity of 1.3 (95% CI: 0.6–2.5) per 1,000 tackles compared to ball carriers (n = 10), with a propensity of 1.6 (95% CI: 0.8–2.9) per 1,000 tackles. Overall incidence of HIAs was 33 HIAs per 1,000 match hours. Differences between tackler and ball carrier HIA propensity were not significant.
The medically diagnosed concussions (n = 6), diagnosed as part of the three stage HIA process from the match to 2 days post match, had a propensity of 0.94 (95% CI: 0.4–2.1) per 1,000 tackles. There was one concussion every 3.5 matches, an incidence of 11 concussions per 1,000 match hours.
HIE propensity as a function of player body position is shown in Figure 1. Overall HIE propensity was similar for tacklers who were upright (13.9, 95% CI: 9.1–21.1 per 1,000 tackles), bent at the waist (12.0, 95% CI: 8.5–17.0 per 1,000 tackles), bent at the knees (13.5, 95% CI: 8.7–20.9 per 1,000 tackles), or unbalanced (13.2, 95% CI: 6.9–25.3) (Figure 1A). Upright tacklers were observed in 32% of all tackle HIEs and caused a HIE to either player every one match (95% CI: 0.6–1.5 per 1,000 tackles), an incidence of 41 HIEs per 1,000 match hours.
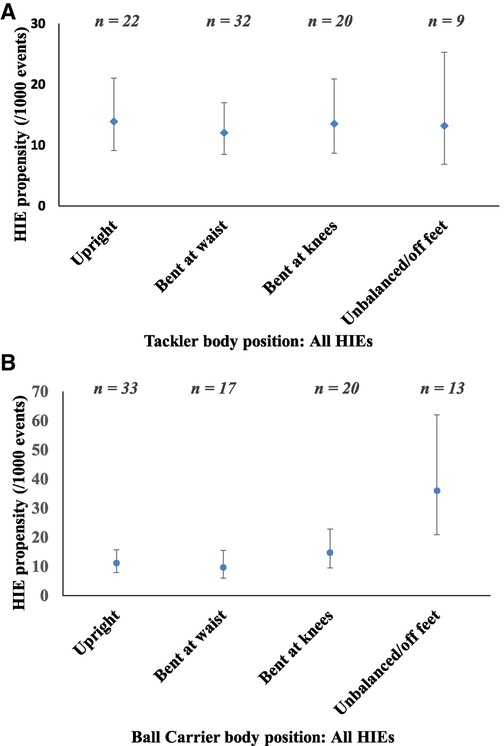
Figure 1. Tackler (A) and ball carrier (B) body position for head impact events (HIEs) to either player.
Considering ball carrier body position, overall HIE propensity was significantly greater when the ball carriers were unbalanced/ off their feet (36.0, 95% CI: 20.9–62.0 per 1,000 tackles), compared to upright (11.2, 95% CI: 7.8–15.8 per 1,000 tackles) and bent at the waist (9.7, 95% CI: 6.0–15.6 per 1,000 tackles), and similar to when the ball carriers were bent at the knees (14.8; 95% CI: 9.5–22.9 per 1,000 tackles; Figure 1B). Unbalanced/ off their feet ball carriers were observed in 15% of all tackle HIEs, with an incidence of 24 HIEs per 1,000 match hours.
The risk of an HIE to the tackler and ball carrier as a function of each player's body position were considered separately. No differences were found for tackler HIE propensity for different tackler body positions, nor for ball carrier HIE propensity, for different ball carrier body positions.
Tackles with proximity of the tackler's head to the ball carrier's head or neck resulted in the highest HIE propensity of 287.2 per 1,000 tackles (95% CI: 197.0–418.9). This was significantly greater than tackles involving contact or proximity with the lower leg, upper trunk, lower trunk, and mid trunk (p < 0.05).
When grouped into tackles involving high contact (tackler's head was in close proximity to the ball carrier's sternum or above), medium contact (tackler's head between the ball carrier's sternum to waist), and low contact (tackler's head below the ball carrier's waist), tackler HIE propensity (Figure 2A) was 2.8 times greater for high contact than for medium contact (10.8, 95% CI: 7.3–15.8) per 1,000 tackles for high contact vs. 3.8 (95% CI: 2.2–6.6) per 1,000 tackles for medium contact. There was no significant difference between high and low, or medium and low contacts, with HIE propensity for low contacts at 5.5 (95% CI: 1.8–17.0) per 1,000 tackles.
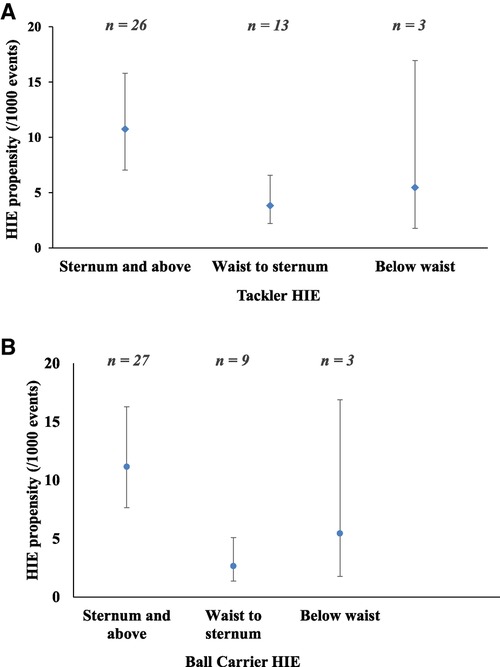
Figure 2. Propensity for head impact events (HIEs) based on head proximity location when (A) the tackler had an HIE and (B) the ball carrier had an HIE.
Propensity for HIEs to the ball carrier (Figure 2B) was significantly higher when the tackler's head was above the ball carrier's sternum (11.2 per 1,000 tackles, 95% CI: 7.7–16.3), compared to when the head was between the waist and sternum (2.7 per 1,000 tackles, 95% CI: 1.4–5.1, IRR high vs. medium = 4.2). However, HIE propensity was not different when the tackler's head was in proximity to the ball carrier's waist and below (5.5 per 1,000 tackles, 95% CI: 1.8–16.9).
For location of body contact, the HIE propensity and incidence are shown in Table 1. Tackler and ball carrier HIEs are considered separately. The highest propensity for tackler HIEs occurred with proximity between the tackler's and ball carrier's heads (214.3 per 1,000 tackles, 95% CI: 129.2–355.5), accounting for 36% of tackler HIEs. This was followed by proximity to the ball carrier's elbow (117.7 per 1,000 tackles, 95% CI: 29.4–470.4). HIEs from these impacts, however, were rare, accounting for 5% of tackler HIEs. The lowest propensity for tackler HIEs (7%) occurred with the tackler's head close to the ball carrier's arm, defined as point of contact between the shoulder and elbow (2.7 per 1,000 tackles, 95% CI: 0.8–8.2). However, contact with the ball carrier's torso had a lower propensity for tackler HIEs (4.0 per 1,000 tackles, 95% CI: 2.2–7.2, Table 1). The highest incidence for tackler HIEs was found in head-to-head impacts (27.5 HIEs per 1,000 match hours), followed by contact with the ball carrier's torso (20.1 HIEs per 1,000 hours).
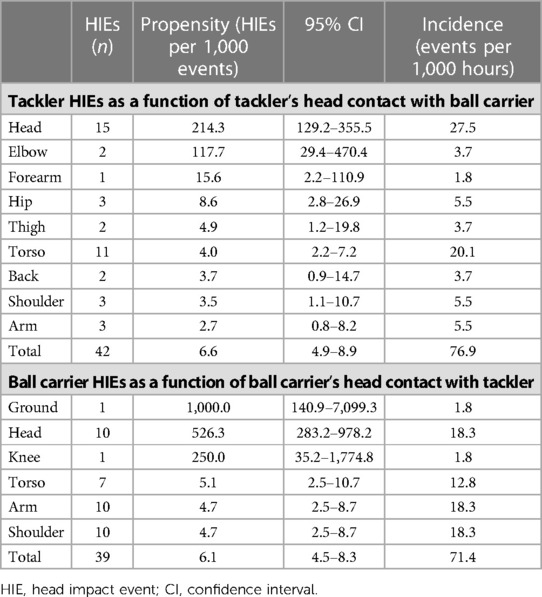
Table 1. HIEs as a function of head contact proximity with the opponent's body part.
The propensity for ball carrier HIEs was greatest when the ball carrier's head made contact with the ground, however, this was a rare event, accounting for only 2% of all ball carrier HIEs (1,000 per 1,000 tackles, 95% CI: 140.9–7,099.3). Head to head proximity with the tackler accounted for 25% of ball carrier HIEs, with a propensity of 526.3 per 1,000 tackles (95% CI: 283.2–978.2), followed by contact with the tackler's knee (250.0 per 1,000 tackles, 95% CI: 35.2–1774.8) and was lowest for contact with the tackler's arm and shoulder (4.7 per 1,000 tackles, 95% CI: 2.5–8.7). The highest incidence for ball carrier HIEs were contact with the tackler's head, arm, and shoulder, however, although head-to-head contact had a high propensity to cause ball carrier HIEs, contact with the arm and shoulder, had a relatively low propensity (4.7 per 1,000 tackles, 95% CI: 2.5–8.7, Table 1) for ball carrier HIEs.
There is a paucity of literature examining mechanisms for head injuries in women athletes (10, 37–39). This study is the first to examine the propensity, incidence, and mechanism of HIEs, in Australian women's rugby league, during the first three seasons of the NRLW competition (2018–2020). We found that HIEs in the NRLW occurred at a propensity of 12.93 per 1,000 tackles, with an incidence of 152 tackle-related HIEs per 1,000 match hours. HIA propensity was lower than HIE propensity, at 2.80 per 1,000 tackles, equating to 33 HIAs per 1,000 match hours. The concussion propensity was 0.94 per 1,000 tackles, with an incidence of 11 concussions per 1,000 match hours. This is lower than in the NRL, where concussion incidence has been reported at 14.7 concussions per 1,000 match hours (2). However, because there were only six diagnosed concussions across the three seasons (i.e., 7 games per season), comparisons with the men's game (i.e., 24 games per team, per season) must be made with caution.
Our study's first important finding was that in the NRLW, tacklers and ball carriers were equally likely to sustain an HIE. Of the 83 HIEs, tacklers sustained 51% and ball carriers 47%, with the remaining 2% being off the ball contact. This differs from the body of research carried out in the men's NRL competition, where the tackler was more likely to experience an HIA during a tackle compared with the ball carrier (15, 16, 18, 26). This is a difference that may be, in part, the result of our identification of HIEs rather than HIAs, which was necessary due to the low number of HIAs (n = 18) reported across the three seasons in the women's game. It may be that tacklers and ball-carriers are at equal risk of experiencing head impact events, as we find for women, but that the likelihood that such a head impact will cause a clinical outcome (head injury or concussion) is greater in tacklers. This cannot be ascertained in the present study, but may be a focus of future research with a larger sample of athletes with concussion.
In terms of head impacts, it is possible that NRLW players are less experienced than men in the physical contact that is inherent in a tackle (8), and that the ball carriers may not be accustomed to being tackled, particularly when upright, making them more likely to experience HIEs than their male counterparts. This may be compounded by the technique and height of the tackler, whose head may more often be in proximity with the ball carrier's head, leading to a greater number of head-to-head impacts. This has been proposed in women's rugby union, where tackle technique is influenced by playing experience (40). In addition, due to inherent differences in neck strength and girth, women may not be able to efficiently dissipate the forces imparted in a tackle in the same way as men (41–44). Further research needs to elucidate whether increases in neck strength are associated with different clinical outcomes after head impacts in women (45, 46) and/or the ability to control the head during the forces imparted in the tackle.
NRLW players, along with the other football codes have attracted women from other sports, with reduced access to training, facilities, and coaching (10, 26). Furthermore, for the inaugural season (2018), players were contracted at short notice, for an overall average contract length of just 8 weeks (47). Players had a mean age of 27 years (range 18–42) across the first three seasons, which meant that some had to balance full or part-time employment, study, and caring for children while playing elite-level rugby league in an intense, short period of time (47). These women are unlikely to follow the same athletic preparation periodization as the men playing in the NRL competition, who were provided the necessary support structures to access a professional career in the NRL (47, 48). NRLW players often have not had the same viable career opportunities to pursue, which may have compromised their preparation and training in ways that have been linked with a higher injury incidence. This lack of experience, opportunity, and inherent inequalities in resourcing have been linked with a higher incidence of injuries (6–9).
Our second important finding was that risk of a head impact created by the tackler and ball carrier body position interactions differed to the risks of head injuries in men's rugby league and rugby union. Although the variables of interest are not the same (NRLW HIEs evaluate whether the head has been contacted, and the men's NRL and rugby union studies examined clinical outcomes following head impact) we compared the findings. In men's rugby league (17) and rugby union (28, 33), upright tacklers were significantly more likely to cause an HIA to either player than bent tacklers. Upright tackles in the NRL resulted in a higher proportion of head-to-head contact (26). We found the four observed tackler and ball carrier body positions resulted in a similar propensity for HIEs, which may indicate a different mechanism for HIEs for the NRLW players compared to HIAs and concussions in men's play, and which may reveal differences in tackle execution between women and men. It is possible that the women may choose to tackle differently from the men, to avoid breast tissue contact injuries (49), placing their heads in more upright or very low positions, to avoid upper-torso contact. This is of relevance because previous research has shown that tackles aimed at the mid-torso level are considered the safest zone in men (50, 51). Research from other sports such as soccer has revealed different concussion mechanisms for men and women, with concussions in men resulting from contact with another player, whereas in women, contact with an object or equipment is the most common mechanism for a concussion (52, 53).
Similarly, in university rugby union players, 45% of head impacts for women ball carriers were from head contact with the ground, compared with 57% of tacklers' heads contacting a hard body part of the opponent (54). For male tacklers and ball carriers, direct or indirect contact with another player had the greatest propensity for head injury (44). Although, our study did not find a body position significantly related to head impact risk, 33% of HIEs were sustained when the ball carrier was either unbalanced or off their feet (i.e., falling or diving). To reduce head impact risk in NRLW players, both tacklers and ball carriers may require tackle re-education, in terms of how the tackler performs the tackle and how the ball carrier engages in contact during the tackle. Current training strategies for women athletes have been derived from male data (40) and although the rules of rugby league may be similar for both sexes, athlete considerations in women need to be reflected in tackle technique and proficiency, size of the football as well as their dynamic balance and ability to dive or fall safely. A panel of experts identified poor tackle technique as the greatest risk factor for injury, specifically, in women's rugby league players, and was also the most feasible to change (38).
Third, with respect to head contact location or proximity, the highest propensity for HIEs occurred when the tackle height was above the sternum, with tackles to the head and neck resulting in the greatest propensity for head impact (Figure 2). These high contact tackles were significantly more likely to result in HIEs than tackles where contact occurs below the sternum. This is a finding similar to that observed in men's rugby union and rugby league (1, 17, 26–28, 50). In our study, tacklers were more likely to experience head-to-head and head-to-elbow impacts, while ball carriers more likely to have head-to-head impacts, head-to-knee impacts, or contact with the ground. In combination, this analysis suggests that when tackles are either too high (sternum and above) or too low (below the waist), the risk of head impacts is greater than when tackles are executed at between the sternum and waist. Given that tackling is a highly technical skill, tackle technique education and retraining to reduce head impact events, and potentially concussion incidence, may be warranted.
It is important to emphasize that we have focused on HIEs and not HIAs or concussions, and this makes direct comparisons with previous studies in men speculative. A subset of these head impacts would require removal of a player from the field for screening, and of these, concussions are a very small subset. We do not thus assess susceptibility to clinical injury risk, but rather likelihood of a head impact as a function of different tackle behaviors. It is possible that the risk factors for injury events differ from risk factors for impact events, by virtue of a different severity for the former. However, assessing head impacts remains important, because it provides stakeholders with a preliminary understanding of HIE risk within the emerging professional competition of the NRLW, under the premise that any reduction to HIE risk might also reduce injury outcomes, as well as purported theorized effects of cumulative exposure to head impacts. The relationship between head impacts and head injuries should be explored in future research.
As our results suggest that the tackler and ball carrier are equally likely to experience an HIE in women's rugby league, tackle technique and proficiency may have a role to play, as tacklers are primarily responsible for increasing head impact risk through their actions, which may then lead to head injury risk (55, 56). The ball carrier may also act to increase head impact risk, and so both players should be considered, but our findings suggest that modification to tackle height, as has been trialed in men's rugby union (57) in an attempt to reduce head injury risk, may also be warranted in women's rugby league. Furthermore, women may benefit from physical preparation strategies that prepare them for contact, in particular the ground contact that occurs when being tackled, and when diving for a loose ball that is either spilled on the ground or in the air.
There a number of limitations associated with this study. Coding and evaluation of the tackle variables include elements of subjectivity. All events were coded by a single analyst, and the subjective nature represents a potential source of inaccuracy. When analyzing tackle characteristics, the nature of the tackle as a dynamic, multi-faceted event, occurring in real-time must be considered. Although we coded 36 individual variables that considered tackler and ball carrier interactions, head contact, and evasion methods, it is important to appreciate that tackle characteristics do interact with each other.
Second, due to the short seasons and relatively low number of games (n = 21), several tackle variables rarely occurred, leading to sparse data that should be interpreted with caution. This limitation in sample size also affects the analysis, because we cannot explore how HIE incidence and propensity may have differed between seasons, or between playing positions on the field, because any division of our data into smaller groups for this analysis means we would be statistically underpowered. However, these are important considerations for future research, which should identify whether HIE risk is changing over time, as well as which players are most at risk, and whether the HIE risk factors are similar to those that cause clinical outcomes such as HIAs and concussions.
Further research examining larger samples of women's rugby league players with quantification of head exposure risk via a combination of video analysis and instrumented mouthguard technology may be beneficial (58) to better inform our understanding of tackle collision risk. Future studies should also consider the role that level of experience, player position, and game demands play in injury risk.
Our study provides the first description of head impacts occurring in the first three seasons of the NRLW competition. Our preliminary results show that professional women's rugby league tacklers and ball carriers are at equal risk of sustaining a tackle-related HIE. Head-to-head proximity and tackles above the sternum carry the greatest risk of HIEs in the NRLW. Injury prevention initiatives for women may need to consider both the tackler's execution and ball carrier's engagement, in order to influence risk. Current player welfare strategies in women's sport are still informed by male derived data and this warrants caution in transferring evidence-based men's injury reduction strategies to the women's game. Therefore, large prospective studies focusing on the women's game would better inform head injury risk and prevention strategies.
During a tackle, in the NRLW, tacklers and ball carriers are equally at risk of sustaining a head impact. Head-to-head proximity and legal tackles at and above the sternum carry the greatest risk of HIEs in the NRLW. Consistent with men's rugby league, injury prevention initiatives aimed at reducing tackle height might reduce the HIE risk in women. Furthermore, in women, both the tackler's execution and ball carrier's engagement need to be considered from a technique re-education perspective to reduce risk.
The datasets presented in this article are not readily available because of privacy considerations. The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author. The statistical code, syntax, output, and analyses are available to qualified researchers upon request. Requests to access the datasets should be directed toYW5kcmV3LmdhcmRuZXJAc3lkbmV5LmVkdS5hdQ==.
The studies involving human participants were reviewed and approved by The University of Newcastle Human Ethics Committee (Ref No. H-2012-0344). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements. The ethics committee waived the requirement of written informed consent for participation.
SM completed the literature review, performed the coding, collated the data, and drafted the manuscript. AG and RT conceptualized the study and developed the framework for video analysis. RT conducted the statistical analysis. All authors contributed to the article and approved the submitted version.
MS is part-funded by Leeds Rhinos rugby league club. RT is a consultant to World Rugby Pty. World Rugby is the governing body for the sport of Rugby Union and responsible for law changes in the sport. BJ is employed by Leeds Rhinos, Rugby Football League and Premiership Rugby in a consultancy capacity. GLI serves as a scientific advisor for NanoDX® Sway Operations, LLC, and Highmark, Inc. He has a clinical and consulting practice in forensic neuropsychology, including expert testimony, involving individuals who have sustained mild TBIs (including former athletes). He has received research funding as a principal investigator from the National Football League, and subcontract grant funding as a collaborator from the Harvard Integrated Program to Protect and Improve the Health of National Football League Players Association Members. He acknowledges unrestricted philanthropic support from ImPACT Applications, Inc., the Mooney-Reed Charitable Foundation, Boston Bolts, the National Rugby League, and the Schoen Adams Research Institute at Spaulding Rehabilitation. None of the above entities were involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication. AJG serves as a scientific advisor for HitIQ, Ltd. He has a clinical practice in neuropsychology involving individuals who have sustained sport-related concussion (including current and former athletes). He has been a contracted concussion consultant to Rugby Australia since July 2016. He has received travel funding or been reimbursed by professional sporting bodies, and commercial organisations for discussing or presenting sport-related concussion research at meetings, scientific conferences, workshops, and symposiums. Previous grant funding includes the NSW Sporting Injuries Committee, the Brain Foundation (Australia), an Australian-American Fulbright Commission Postdoctoral Award, a Hunter New England Local Health District, Research, Innovation and Partnerships Health Research & Translation Centre and Clinical Research Fellowship Scheme, and the Hunter Medical Research Institute (HMRI), supported by Jennie Thomas, and the HMRI, supported by Anne Greaves. He has current philanthropic support from the Nick Tooth Foundation. He acknowledges unrestricted philanthropic support from the National Rugby League (NRL).
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fspor.2023.1080356/full#supplementary-material
1. Gardner AJ, Iverson GL, Quinn TN, Makdissi M, Levi CR, Shultz SR, et al. A preliminary video analysis of concussion in the national rugby league. Brain Inj. (2015) 29:1182–5. doi: 10.3109/02699052.2015.1034179
2. Gardner A, Iverson GL, Levi CR, Schofield PW, Kay-Lambkin F, Kohler RM, et al. A systematic review of concussion in rugby league. Br J Sports Med. (2015) 49:495–8. doi: 10.1136/bjsports-2013-093102
3. King DA, Hume PA, Hind K, Clark TN, Hardaker N. The incidence, cost, and burden of concussion in women's rugby league and rugby union: a systematic review and pooled analysis. Sports Med. (2022) 52:1751–64. doi: 10.1007/s40279-022-01645-8
4. Spiegelhalter M, Scantlebury S, Heyward O, Hendricks S, Cummins C, Gardner AJ, et al. The propensity of non-concussive and concussive head contacts during elite-level women's rugby league matches: a prospective analysis of over 14,000 tackle events. J Sci Med Sport. (2023) 26(3):195–201. doi: 10.1016/j.jsams.2023.03.003
5. Fuller CW, Taylor A. Women's rugby world cup 2017: summary of results. World Rugby (2017). Available at: https://playerwelfare.worldrugby.org/?documentid=181 (Accessed September 21, 2022).
6. Starling LT, Gabb N, Williams S, Kemp S, Stokes KA. Longitudinal study of six seasons of match injuries in elite female rugby union. Br J Sports Med. (2023) 57(4):212–17. doi: 10.1136/bjsports-2022-105831
7. Harvey FA, Schussler E. The effect of experience levels on injury rates in collegiate rugby players. Int J Athl Ther Train. (2021) 27:31–5. doi: 10.1123/ijatt.2020-0128
8. Peck KY, Johnston DA, Owens BD, Cameron KL. The incidence of injury among male and female intercollegiate rugby players. Sports Health. (2013) 5:327–33. doi: 10.1177/1941738113487165
9. Yeomans C, Kenny IC, Cahalan R, Warrington GD, Harrison AJ, Purtill H, et al. Injury trends in Irish amateur rugby: an epidemiological comparison of men and women. Sports Health. (2021); 13:540–7. doi: 10.1177/1941738121997145
10. Cummins C, Melinz J, King D, Sanctuary C, Murphy A. Call to action: a collaborative framework to better support female rugby league players. Br J Sports Med. (2020) 54:501–2. doi: 10.1136/bjsports-2019-101403
11. Brown DA, Elsass JA, Miller AJ, Reed LE, Reneker JC. Differences in symptom reporting between males and females at baseline and after a sports-related concussion: a systematic review and meta-analysis. Sports Med. (2015) 45:1027–40. doi: 10.1007/s40279-015-0335-6
12. Covassin T, Elbin RJ. The female athlete: the role of gender in the assessment and management of sport-related concussion. Clin Sports Med. (2011) 30:125–31. doi: 10.1016/j.csm.2010.08.001
13. Stone S, Lee B, Garrison JC, Blueitt D, Creed K. Sex differences in time to return-to-play progression after sport-related concussion. Sports Health. (2017) 9:41–4. doi: 10.1177/1941738116672184
14. Wallace J, Covassin T, Beidler E. Sex differences in high school athletes' knowledge of sport-related concussion symptoms and reporting behaviors. J Athl Train. (2017) 52:682–8. doi: 10.4085/1062-6050-52.3.06
15. Gardner AJ, Howell DR, Iverson GL. A video review of multiple concussion signs in national rugby league match play. Sports Med Open. (2018) 4:5. doi: 10.1186/s40798-017-0117-9
16. Gardner AJ, Howell DR, Levi CR, Iverson GL. Evidence of concussion signs in national rugby league match play: a video review and validation study. Sports Med Open. (2017) 3:29. doi: 10.1186/s40798-017-0097-9
17. Gardner AJ, Iverson GL, Edwards S, Tucker R. A case–control study of tackle-based head injury assessment (HIA) risk factors in the national rugby league. Sports Med Open. (2021) 7:1–11. doi: 10.1186/s40798-021-00377-9
18. Gardner A, Iverson G, Stanwell P, Moore T, Ellis J, Levi C. A video analysis of use of the new ‘concussion interchange rule' in the national rugby league. Int J Sports Med. (2016) 37:267–73. doi: 10.1055/s-0035-1565203
19. Gardner AJ, Kohler R, McDonald W, Fuller GW, Tucker R, Makdissi M. The use of sideline video review to facilitate management decisions following head trauma in super rugby. Sports Med Open. (2018) 4:20. doi: 10.1186/s40798-018-0133-4
20. Gardner AJ, Kohler RM, Levi CR, Iverson GL. Usefulness of video review of possible concussions in national youth rugby league. Int J Sports Med. (2017) 38:71–5. doi: 10.1055/s-0042-116072
21. Gardner AJ, Wojtowicz M, Terry DP, Levi CR, Zafonte R, Iverson GL. Video and clinical screening of national rugby league players suspected of sustaining concussion. Brain Inj. (2017) 31:1918–24. doi: 10.1080/02699052.2017.1358399
22. Davis GA, Makdissi M, Bloomfield P, Clifton P, Echemendia RJ, Falvey ÉC, et al. International consensus definitions of video signs of concussion in professional sports. Br J Sports Med. (2019) 53:1264–7. doi: 10.1136/bjsports-2019-100628
23. Fuller CW, Fuller GW, Kemp SP, Raftery M. Evaluation of world rugby's concussion management process: results from rugby world cup 2015. Br J Sports Med. (2017) 51:64–9. doi: 10.1136/bjsports-2016-096461
24. Hutchison MG, Comper P, Meeuwisse WH, Echemendia RJ. A systematic video analysis of national hockey league (NHL) concussions, part I: who, when, where and what? Br J Sports Med. (2015) 49:547–51. doi: 10.1136/bjsports-2013-092234
25. Davis G, Makdissi M. Use of video to facilitate sideline concussion diagnosis and management decision-making. J Sci Med Sport. (2016) 19:898–902. doi: 10.1016/j.jsams.2016.02.005
26. Edwards S, Lee R, Fuller G, Buchanan M, Tahu T, Tucker R, et al. 3D biomechanics of rugby tackle techniques to inform future rugby research practice: a systematic review. Sports Med Open. (2021) 7:1–20. doi: 10.1186/s40798-021-00322-w
27. Tucker R, Raftery M, Fuller GW, Hester B, Kemp S, Cross MJ. A video analysis of head injuries satisfying the criteria for a head injury assessment in professional rugby union: a prospective cohort study. Br J Sports Med. (2017) 51:1147–51. doi: 10.1136/bjsports-2017-097883
28. Tucker R, Raftery M, Kemp S, Brown J, Fuller G, Hester B, Cross M, Quarrie K. Risk factors for head injury events in professional rugby union: a video analysis of 464 head injury events to inform proposed injury prevention strategies. Br J Sports Med. (2017) 51:1152–7. doi: 10.1136/bjsports-2017-097895
29. Cummins C, Charlton G, Naughton M, Jones B, Minahan C, Murphy A. The validity of automated tackle detection in women's rugby league. J Strength Cond Res. (2022) 36:1951–5. doi: 10.1519/JSC.0000000000003745
30. West SW, Shill IJ, Clermont C, Pavlovic N, Cairns J, Seselja B, et al. Same name, same game, but is it different? An investigation of female rugby union match events in Canadian varsity players. Int J Sports Sci Coach. (2022) 17:1119–27. doi: 10.1177/17479541211051961
31. Newans T, Bellinger P, Buxton S, Quinn K, Minahan C. Movement patterns and match statistics in the national rugby league women's (NRLW) premiership. Front Sports Act Living. (2021) 3:618913. doi: 10.3389/fspor.2021.618913
32. NRL. Annual report 2018. (2018). Available at: https://www.nrl.com/siteassets/documents/nrl-gen19_6501-2018-annual-report-hr.pdf (Accessed September 21, 2022).
33. Cross MJ, Tucker R, Raftery M, Hester B, Williams S, Stokes KA, et al. Tackling concussion in professional rugby union: a case-control study of tackle-based risk factors and recommendations for primary prevention. Br J Sports Med. (2019) 53:1021–5. doi: 10.1136/bjsports-2017-097912
34. Fuller CW, Ashton T, Brooks JH, Cancea RJ, Hall J, Kemp SP. Injury risks associated with tackling in rugby union. Br J Sports Med. (2010) 44:159–67. doi: 10.1136/bjsm.2008.050864
35. Hopkinson M, Bissas A, Nicholson G, Beggs C, Scantlebury S, Hendricks S, et al. A video analysis framework for the rugby league tackle. Sci Med Footb. (2022) 6:15–28. doi: 10.1080/24733938.2021.1898667
36. Stokes KA, Locke D, Roberts S, Henderson L, Tucker R, Ryan D, et al. Does reducing the height of the tackle through law change in elite men’s rugby union (The Championship, England) reduce the incidence of concussion? A controlled study in 126 games. Br J Sports Med. (2021) 55:220–5. doi: 10.1136/bjsports-2019-101557
37. Emmonds S, Heyward O, Jones B. The challenge of applying and undertaking research in female sport. Sports Med Open. (2019) 5(1):1–4. doi: 10.1186/s40798-019-0224-x
38. Heyward O, Emmonds S, Roe G, Scantlebury S, Stokes K, Jones B. Applied sports science and sports medicine in women’s rugby: systematic scoping review and Delphi study to establish future research priorities. BMJ Open Sport Exerc Med. (2022) 8:e001287. doi: 10.1136/bmjsem-2021-001287
39. Scantlebury S, Ramirez C, Cummins C, Stokes K, Tee J, Minahan C, et al. Injury risk factors and barriers to their mitigation for women playing rugby league: a Delphi study. J Sports Sci. (2022) 40:1–14. doi: 10.1080/02640414.2022.2085433
40. Dane K, Simms C, Hendricks S, West SW, Griffin S, Nugent FJ, et al. Physical and technical demands and preparatory strategies in female field collision sports: a scoping review. Int J Sports Med. (2022) 43:1173–82. doi: 10.1055/a-1839-6040
41. Chavarro-Nieto C, Beaven M, Gill N, Hébert-Losier K. Neck strength in rugby union players: a systematic review of the literature. Phys Sportsmed. (2021) 49:392–409. doi: 10.1080/00913847.2021.1886574
42. Nagai T, Crowley E, Manuell E. Sex dif-ferences in multidirectional neck muscle strength characteris-tics in high school soccer athletes. Arch Sports Med. (2020) 4:224–32. doi: 10.22374/jspv.v4i1.11
43. Peek K, Elliott JM, Orr R. Higher neck strength is associated with lower head acceleration during purposeful heading in soccer: a systematic review. J Sci Med Sport. (2020) 23:453–62. doi: 10.1016/j.jsams.2019
44. Williams EM, Petrie FJ, Pennington TN, Powell DR, Arora H, Mackintosh KA, et al. Sex differences in neck strength and head impact kinematics in university rugby union players. Eur J Sport Sci. (2022) 22:1649–58. doi: 10.1080/17461391.2021.1973573
45. Benson BW, McIntosh AS, Maddocks D, Herring SA, Raftery M, Dvořák J. What are the most effective risk-reduction strategies in sport concussion? Br J Sports Med. (2013) 47:321–6. doi: 10.1136/bjsports-2013-092216
46. Daly E, Pearce AJ, Ryan L. A systematic review of strength and conditioning protocols for improving neck strength and reducing concussion incidence and impact injury risk in collision sports; is there evidence? J Funct Morphol Kinesiol. (2021) 6:8. doi: 10.3390/jfmk6010008
47. Fujak H., Taylor T., Hanlon C. and O'Connor D. Growing expectations: comparing NRLW athlete experiences. Bowes A and Culvin A, eds. The professionalisation of women’s sport (Emerald studies in sport and gender). Bingley: Emerald Publishing Ltd. (2021). 193–210.
48. Taylor T, Fujak H, Hanlon C, O’Connor D. A balancing act: women players in a new semi-professional team sport league. Euro Sport Man Quart. (2022) 22:527–47. doi: 10.1080/16184742.2020.1815821
49. Brisbine B, Steele J, Phillips E, McGhee D. Elite female athletes experience breast injuries that affect their performance. J Sci Med Sport. (2019) 22:S67–S8 doi: 10.1016/j.jsams.2019.08.274
50. Edwards S, Gardner A, Tahu T, Fuller G, Strangman G, Levi CR, Iverson GL, Tucker R. Tacklers’ head inertial accelerations can be decreased by altering the way they engage in contact with ball carriers’ torsos. Med Sci Sports Exerc. (2022) 54:1560–157 doi: 10.1249/MSS.0000000000002931
51. Edwards S, Tahu T, Buchanan M, Tucker R, Fuller G, Gardner AJ. Three-dimensional mechanics of the rugby tackle, does the ball carrier alter their movement into contact in response to the tackler’s position? Int J Sports Sci Coach. (2022) 17:298–308. doi: 10.1177/17479541211024022
52. Bretzin AC, Covassin T, Wiebe DJ, Stewart W. Association of sex with adolescent soccer concussion incidence and characteristics. JAMA Netw Open. (2021) 4:e218191–e. doi: 10.1001/jamanetworkopen.2021.8191
53. Iverson GL, Gardner AJ, Terry DP, Ponsford JL, Sills AK, Broshek DK, et al. Predictors of clinical recovery from concussion: a systematic review. Br J Sports Med. (2017) 51:941–8. doi: 10.1136/bjsports-2017-097729
54. Iverson GL, Williams MW, Gardner AJ, Terry DP. Systematic review of preinjury mental health problems as a vulnerability factor for worse outcome after sport-related concussion. Orthop J Sports Med. (2020) 8:2325967120950682. doi: 10.1177/2325967120950682
55. Hollander SD, Ponce C, Lambert M, Jones B, Hendricks S. Tackle and ruck technical proficiency in rugby union and rugby league: a systematic scoping review. Int J Sports Sci Coach. (2021) 16:421–34. doi: 10.1177/1747954120976943
56. Tierney GJ, Denvir K, Farrell G, Simms CK. Does ball carrier technique influence tackler head injury assessment risk in elite rugby union? J Sports Sci. (2019) 37:262–7. doi: 10.1080/02640414.2018.1494952
57. Tierney GJ, Simms CK. Can tackle height influence head injury assessment risk in elite rugby union? J Sci Med Sport. (2018) 21:1210 4. doi: 10.1016/j.jsams.2018.05.010
Keywords: head impact events, rugby league, tackle, female athlete, brain concussion, mild traumatic brain injury
Citation: McLeod S, Tucker R, Edwards S, Jones B, Page G, Spiegelhalter M, West SW, Iverson GL and Gardner AJ (2023) A case-control study of tackle based head impact event (HIE) risk factors from the first three seasons of the National Rugby League Women's competition. Front. Sports Act. Living 5:1080356. doi: 10.3389/fspor.2023.1080356
Received: 26 October 2022; Accepted: 11 May 2023;
Published: 2 June 2023.
Edited by:
Darin A. Padua, University of North Carolina at Chapel Hill, United StatesReviewed by:
Katie Hunzinger, University of Pennsylvania, United States© 2023 McLeod, Tucker, Edwards, Jones, Page, Spiegelhalter, West, Iverson and Gardner. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrew J. Gardner YW5kcmV3LmdhcmRuZXJAc3lkbmV5LmVkdS5hdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.