 Maria Westin
Maria Westin Lisbeth I. Mirbach3
Lisbeth I. Mirbach3 Marita L. Harringe
Marita L. Harringe
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Sports Act. Living, 14 October 2022
Sec. Sports Science, Technology and Engineering
Volume 4 - 2022 | https://doi.org/10.3389/fspor.2022.961408
This article is part of the Research TopicHealth and Performance Assessment in Winter Sports - Volume IIView all 10 articles
An anterior cruciate ligament (ACL) injury is a common, severe injury in alpine skiing, and anterior cruciate ligament reconstruction (ACLR) is frequently performed in competitive alpine skiers younger than 20 years old. To reduce the reinjury rate, both intrinsic and extrinsic risk factors should be examined. The aim of this study was to investigate possible intrinsic risk factors for an ACL reinjury in competitive alpine skiers. A cohort of 384 alpine skiers (191 males/193 females) from the Swedish ski high schools were prospectively followed during their high school years. The students were clinically examined and physically tested prior to each ski season. In addition, the RAND 36-Item health survey 1.0 (SF-36, Copyright 1994 Medical Outcome Trust, distributed by RAND Corporation) and injuries were prospectively registered. Thirty-one of the skiers (five males/26 females) had undergone an ACLR before entering the ski high school. This cohort was analyzed with respect to the occurrence of, and possible risk factors for an ACL reinjury (including ipsilateral and contralateral ACL injuries). Skiers who sustained an ACL reinjury were called the “ACL reinjury group,” and those who did not sustain an ACL reinjury were called the “ACL injury group.” Notably, 12 of the 31 students (39%), ten female and two male skiers, aged 16.5 (SD 0.5) years, sustained an ACL reinjury during the two first years at the ski high school. In addition, 10 of the 12 ACL reinjuries occurred within 10–23 months from the first injury [m 14.8 (SD4.7)] and two ACL reinjuries occurred at 29 and 47 months, respectively, from the first injury. It is noted that eight of the ACL reinjuries were to the ipsilateral knee and four to the contralateral knee. There were no differences between the groups with respect to muscle flexibility in the lower extremity, Beighton score, and one leg hop for distance or square hop test. Side-to-side differences were found with respect to knee joint laxity, >3 mm, measured with KT-1000 arthrometer (p = 0.02), and the side hop test (p = 0.04). RAND 36-Item health survey did not predict an ACL reinjury. In conclusion, a side-to-side difference in the side hop test and knee joint laxity (KT-1000) may predispose an ACL reinjury in competitive adolescent alpine skiers.
Competitive alpine skiing is an injury-risk sport, and the reports on injury incidence vary depending on how and when the incidence is reported. At the World Cup 2006/2007 and 2007/2008, the injury incidence was 36.7 injuries/100 alpine skiers (1), and at the Olympic games in Sochi, the injury incidence was 20.7 injuries/100 alpine skiers (2). An investigation by Fröhlich et al. (3) studying overuse and traumatic injuries in Swiss elite level skiers over one season showed an incidence of 95.5 injuries/100 alpine skiers. In high school competitive alpine skiers, the incidence of traumatic injuries was reported at 3.11 injuries/100 months attending a ski high school, and it was concluded that half of all the students were at risk for an injury during their 3–4 years of the study period (4). Around one-third of all alpine ski injuries are to the knee and the injuries on average generate more than 28 days of absence from the sport (1, 4). One of the most severe and common injuries to the knee is an anterior cruciate ligament (ACL) injury (5, 6). In a study by Pujol et al. (5) on 379 adult elite French alpine skiers over a period of 25 years, an incidence of 8.5 ACL injuries/100 competitive alpine skiers and season was shown. A total of 157 ACL injuries were registered, and half of the ACL-injured alpine skiers sustained an ACL reinjury to the ipsilateral or the contralateral knee (5). In another study, Stevenson et al. (7) described that 22% of alpine skiers underwent a second ACL reconstruction (ACLR). The general opinion is that an ACLR is necessary to be able to continue with alpine skiing and is frequently performed in young competitive alpine skiers.
To reduce the ACL reinjury rate, both intrinsic and extrinsic risk factors should be examined. Side-to-side differences, decreased core stability, and parents' history of an ACL injury are intrinsic factors mentioned as risk factors for the first ACL injury in alpine skiing (8–10). Risk factors for an ACL reinjury in football seem to be injury events close to previous ACLR (11) or time to return after an ACLR (12) as well as whether it was a contact or non-contact ACL injury the first time. Non-contact injuries and isolated ACL injuries were injury risks for an ACL reinjury in professional footballers (13). Another risk for an ACL reinjury seems to be a young age. Paterno et al. (14) showed that 25% of the athletes returning to pivoting sports, and under the age of 25 years, sustained an ACL reinjury. In a 5-year follow-up from the Swedish National Knee Ligament Register (SNKLR), it was shown that athletes under the age of 20 years at the first ACLR had an almost three-fold risk for a contralateral ACL injury to occur (15). A review on ACL injuries showed that close to one of four athletes (23%) under the age of 25 years, returning to high-level sports with an ACLR, sustained an ACL reinjury (16).
To recover and return to sports after an ACL injury is difficult, and the perfect algorithm is still not known. Biological healing and functional performance are keys to success (17). Another key is mental health and psychological readiness to return to play (18, 19).
To the best of our knowledge, studies on risk factors for sustaining an ACL reinjury in young alpine skiers are still lacking. Therefore, the overall aim of this study was to investigate possible intrinsic risk factors for an ACL reinjury in young competitive alpine skiers during their ski high school years. The second aim was to describe this sub-cohort of students from a health perspective using the RAND 36-Item health survey 1.0 (SF-36, Copyright 1994 Medical Outcome Trust).
A cohort of 384 alpine ski students (191 males and 193 females), from ten different Swedish ski high schools, were prospectively followed from September 2006 to May 2009 with respect to performance and injury incidence. A ski student attends high school for 3 or 4 years and is exposed to approximately 200 days of skiing per year (4). The students were included in their first year at the ski high school, and this study was approved by the Swedish Ethical Review Authority, Dnr 2006/833-31/1. Oral and written consent was collected from the ski students.
Of the included 384 ski students, 31 students (five males and 26 females) had undergone an ACLR before entering the ski high school (Table 1). This subgroup of skiers was followed during their studies at the ski high school and in this study occurrence of an ACL reinjury, and possible risk factors for sustaining an ACL reinjury during the ski high school years were analyzed. In this study, the group with skiers sustaining an ACL reinjury is called the “ACL reinjury group” and includes an injury to the ipsilateral or contralateral ACL. The group of skiers that did not sustain an ACL reinjury during their high school years is called the “ACL injury group.”
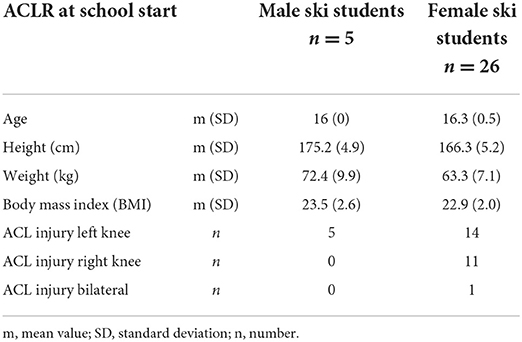
Table 1. Demographic data of the 31 ski high school students who entered the study with a previous anterior cruciate ligament reconstruction (ACLR).
All ski students were clinically examined and physically tested prior to each ski season according to a specific protocol previously described by Westin et al. (8). The protocol included muscle flexibility of hamstrings, rectus femoris, iliopsoas, gastrocnemius, soleus (8), general joint laxity measured with Beighton score (20), knee joint laxity measured with KT-1000 arthrometer (21), and functional performance tests such as the one leg hop for distance, side hop test, and square hop test (22–24). General joint laxity, the Beighton score, was classified as yes (≥ 5 of nine positive tests) and no (≤ 4 positive tests). The skiers also answered the RAND 36-Item health survey 1.0 (25) (SF-36, Copyright 1994 Medical Outcome Trust), and ACL injuries were prospectively registered.
The items in the RAND 36-Item health survey consist of 36 questions regarding physical functioning (10 questions), bodily pain (two questions), role limitations due to physical health problems (four questions), role limitations due to emotional problems (three questions), emotional wellbeing (five questions), social functioning (two questions), energy/fatigue (four questions), general health perceptions (five questions), and at last a single question regarding the perceived change in health since last year. The questions were presented in a mixed order and adapted from a more extensive instrument used in the Medical Outcomes Study (MOS) (26). The scoring system is a two-step process where all the questions in the survey are evaluated on a scale from 0 to 100, and thereafter, the questions that answer each of the eight plus one domain are summarized and averaged. When summarized, 0 represents poor health and 100 represents good health. For more information, visit RAND Corporation (https://www.rand.org/health-care/surveys_tools/mos/36-item-short-form/scoring.html).
Data were presented descriptively with mean values and standard deviation (m(SD)) or with median and interquartile (md(IQ)) or total range (md(range)). Chi-squared test was used analyzing general joint laxity, and the Mann-Whitney U-test was used comparing side-to-side differences in the preseason tests between the “ACL reinjury group” and the “ACL injury group” (27). The RAND 36-Item health survey 1.0 (SF-36, Copyright 1994 Medical Outcome Trust) was recorded and analyzed according to recommendations by RAND Corporation, and the eight domains were presented with md (total range) for both groups. The preseason measurements prior to the ACL reinjury season were used for the “ACL reinjury group,” and the preseason measurements from year 2 in the “ACL-injury group” served as control values, though in six cases, the preseason tests from year 1 were used due to missing values in year 2. The p-value was set at ≤ 0.05.
Out of 31, 12 (39%) students, ten female and two male skiers, m 16.5 (SD 0.5) years old, sustained an ACL reinjury. The injuries occurred on average 18.7 months (SD 10.8, range 10–47) from the first ACL injury. Notably, 10 of the 12 ACL reinjuries occurred within 10–23 months from the first injury [m 14.8 (SD 4.7)], and two of the ACL reinjuries occurred 29 and 47 months, respectively, after the first ACL injury. Six ACL reinjuries occurred during the first year at the ski high school (two males/four females) and six ACL reinjuries occurred during the second year (six females). Eight of the ACL reinjuries were to the ipsilateral knee and four reinjuries to the contralateral knee. Ten of the ACL reinjuries were to the left knee and two reinjuries to the right knee. One male skier reinjured his left ACL, and the other male skier injured his right knee, which was the contralateral ACL. Six female skiers reinjured their left ACL, three female skiers injured their contralateral knee of whom two injured their left ACL, and one injured her right ACL (Table 2).
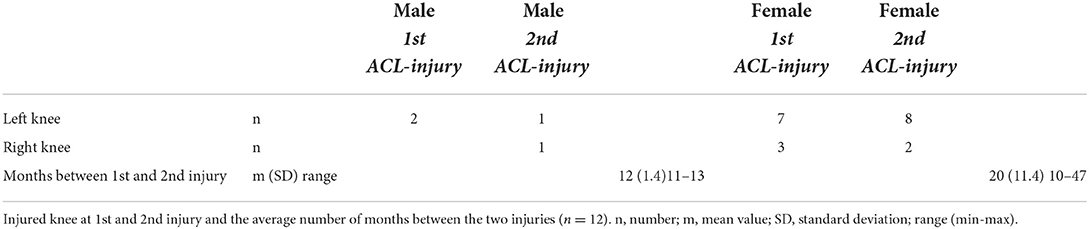
Table 2. Alpine ski high school students who sustained an ACL reinjury.
There were no differences between the “ACL reinjury group” and the “ACL injury group” with respect to muscle flexibility in hamstrings, rectus femoris, iliopsoas, gastrocnemius, or soleus measured according to the protocol presented by Westin et al. (8), or with respect to general laxity measured with Beighton score, or in the functional performance tests, one leg hops for distance or square hop test. Significant differences were found with respect to knee joint laxity measured with KT-1000 max manual where >3 mm is considered a side-to-side difference and the side-to-side differences in the side hop test. Skiers in the “ACL reinjury group” had a side-to-side difference in knee laxity of md 4 mm (IQ 3–5) compared with skiers in the “ACL injury group” with a side-to-side difference of md 1 mm (IQ 0–3) (p = 0.02). In the side hop test, the side-to-side difference was md three hops (IQ 3–4) in the “ACL reinjury group” compared with md two hops (IQ 1–3) in the “ACL injury group” (p = 0.04). The RAND 36-Item health survey did not predict an ACL reinjury (Table 3).
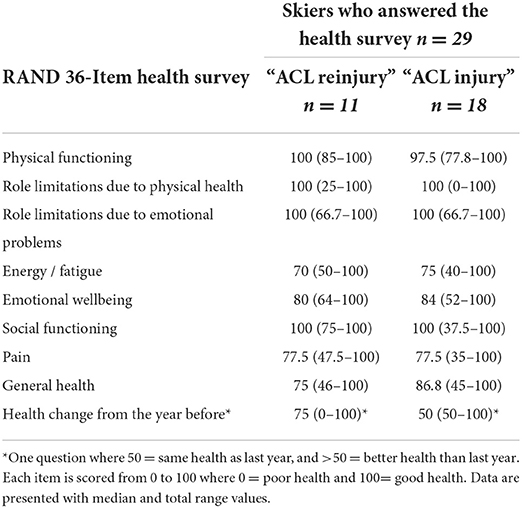
Table 3. Skiers who answered the RAND 36-Item health survey at the start of the preseason tests used in this study.
Nearly, two-fifths (39%) of the ski students entering a ski high school with an ACLR sustained an ACL reinjury within the two first years at the ski high school. The average age for an ACL reinjury was 16.5 years, and the average time from the first ACL injury was 18.7 months. However, 10 of the 12 ACL reinjuries occurred 10–23 months from the first ACL injury, which, on average, was 14.8 months from the first injury. The result is in line with previous research showing that an ACLR before the age of 20 combined with return to high level activity, predisposes an ACL reinjury (11, 16, 28, 29).
Skiing is an equilateral sport, which means that the ski turns have to be equally good to the left and to the right side, and consequently it is important to be equally good on both sides in functional performance tests. Previous research has shown a side-to-side difference to be a risk factor for an ACL injury in alpine skiing (8). This was also shown in this study where the ACL reinjury group had a larger side-to-side difference in the side hop test and in knee laxity measured with a KT-1000 arthrometer compared with those skiers who did not sustain an ACL reinjury. The side hop test may be considered a skiing-like hop test since the hop movement is performed from side to side. In this study, the difference between the groups was small, though significant, but maybe just the difference between mastering a ski turn equally good in both directions or not. Previous research has used limb symmetry index (LSI) to evaluate side-to-side differences between injured and uninjured legs in alpine skiing (30). However, in this study, where the students entered with an ACLR, this was not optional. In an injury profile study in ski high school students, the left leg was more injury prone than the right leg (4). One might speculate that, since most humans are right-sided, the left leg might be more vulnerable due to the equilateral demands of alpine skiing. Ten out of 12 ACL reinjuries in this study were in the left knee, and the reinjuries occurred more frequently in the ipsilateral knee compared with the contralateral knee, consequently more frequently to the left knee compared with the right knee. It could be of importance to understand whether a skier is right- or left-dominant in order to put special focus on the less dominant side with the aim to become equilateral.
Another highly important finding was based on the RAND 36-Item health survey all students entering the ski high school with an ACLR reported fairly low levels in the items energy/fatigue, pain, and general health compared with the other items and compared with normative data (31). Do the skiers return to skiing before fully recovered from their first injury? Nagelli and Hewett (17) suggested that return to unrestricted sports activity should be delayed until 2 years after an ACLR. This was based on biological and functional recovery. For example, the ligamentization process of the ACL autograft in humans may take up to 1 year for the patella-tendon autograft and 2 years for the hamstrings autograft (17). In addition, the neuromuscular system has to recover as well as bone and muscular strength, and sports-specific skills must be regained.
To recover and return to sports after an ACL injury is difficult. Considering the short time between the ACL injuries, one might suspect that the students were fighting with recovery from the first injury. In a study on gymnasts' experiences and perception of an ACL injury, the gymnasts described that early contact with a sports psychiatrist or likewise is important (30). They also described that one can become and feel stronger than ever, but if one does not prepare the body and mind for the specific gymnastics skills, one cannot succeed in the aim of returning to the previous level of gymnastics. Psychological readiness is a crucial part of returning to sports and may be the difference between whether the athlete returns to high-level sports or not (18, 19, 32, 33).
This study investigated students at ski high schools from year 1 to year 4. To attend a ski high school means leaving family behind and moving to a new place at a young age. In addition, these young students entered the school with a previous ACL injury and according to the health survey, with fairly low levels of energy, pain, and estimated general health. Maybe these alone are risk factors for an ACL reinjury, even if it was not shown in this study. In a study on young elite athletes, attending sports high school with a mean age of 17.1 years, it was found that sleeping 8 h or more and reaching recommended levels of nutrition intake reduces the odds to sustain an injury by more than 60% (34).
To prevent severe knee injuries in young competitive alpine skiers probably needs an algorithm including prevention based on risk factors and physical as well as psychological recovery in between training and competition. To date, only two prevention programs have been carried out on adolescent alpine skiers. In a study by Schoeb et al. (35), an off-snow injury prevention program for Swiss aged under 16 years (U16) competitive skiers performed once a week, reduced the 2-weekly prevalence of knee trauma, knee overuse, and lower back overuse complaints. Another study by Westin et al. (36) using a neuromuscular prevention program on- and off-snow, showed a reduction of first episode ACL injury in competitive alpine skiers between 16 and 20 years of age. Both these programs were carried out during the whole skiing season. In addition, psychological preparation must be included. This may be provided by the ski trainer, mental coach, medical team, family, or friends. For example, a young skier, attending a ski high school, does, in most cases, leave the secure environment at home for security provided by the school, friends, and the skiing community. Just to have someone to talk to, preferably someone with knowledge of alpine skiing, not involved in the regular ski training, could be one way of providing psychological preparation, security, and readiness to the skiers (32).
The fact that the students were followed prospectively from day 1 at the ski high school until they left the school 3–4 years later may be seen as a strength of this study. The students entered the school with a previous ACL injury, which made it possible to study ACL reinjuries. One limitation is that information about the first ACL injury is scarce, and the health status before the first ACL injury is unknown. Another limitation is the small sample size.
Out of 31, 12 ski high school students (39%) entering the school with an ACLR sustained an ACL reinjury during the first 2 years at a ski high school and on average 18.7 months from the first ACL injury. Side-to-side differences were found in the side hop test and knee joint laxity, measured with the KT-1000 arthrometer, and may predispose an ACL reinjury in competitive adolescent alpine skiers. RAND 36-Item health survey did not predict an ACL reinjury.
The original contributions presented in the study are included in the article/supplementary materials, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by Swedish Ethical Review Authority, Dnr 2006/833-31/1. Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
MW and MH have given substantial contribution to the conception, design of the study, and drafted the manuscript. Acquisition of data by MW. Analysis and interpretation by MW, LM, and MH. All authors critically revised, read, and approved the final version of the manuscript.
The authors would like to thank the Ski High Schools and all the students participating in this study. Without your kind collaboration, this study would not have been possible. We would also like to thank Karolinska Institutet and the Department for Molecular Medicine and Surgery for their support during the writing process of this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Flørenes TW, Bere T, Nordsletten L, Heir S, and Bahr R. Injuries among male and female World Cup alpine skiers. Br J Sports Med. (2009) 43:973–8. doi: 10.1136/bjsm.2009.068759
2. Soligard T, Steffen K, Palmer-Green D, Aubry M, Grant ME, Meeuwisse W, et al. Sports injuries and illnesses in the Sochi 2014 Olympic Winter Games. Br J Sports Med. (2015) 49:441–7. doi: 10.1136/bjsports-2014-094538
3. Fröhlich S, Helbling M, Fucentese SF, Karlen W, Frey WO, and Spörri J. Injury risks among elite competitive alpine skiers are underestimated if not registered prospectively, over the entire season and regardless of whether requiring medical attention. Knee Surg Sports Traumatol Arthrosc. (2021) 29:1635–43. doi: 10.1007/s00167-020-06110-5
4. Westin M, Alricsson M, and Werner S. Injury profile of competitive alpine skiers: a five-year cohort study. Knee Surg Sports Traumatol Arthrosc. (2012) 20:1175–81. doi: 10.1007/s00167-012-1921-x
5. Pujol N, Blanchi MP, and Chambat P. The incidence of anterior cruciate ligament injuries among competitive Alpine skiers: a 25-year investigation. Am J Sports Med. (2007) 35:1070–4. doi: 10.1177/0363546507301083
7. Stevenson H, Webster J, Johnson R, and Beynnon B. Gender differences in knee injury epidemiology among competitive alpine ski racers. Iowa Orthop J. (1998) 18:64–6.
8. Westin M, Harringe ML, Engström B, Alricsson M, and Werner S. risk factors for anterior cruciate ligament injury in competitive adolescent Alpine skiers. Orthop J Sports Med. (2018) 6:2325967118766830. doi: 10.1177/2325967118766830
9. Westin M, Reeds-Lundqvist S, and Werner S. The correlation between anterior cruciate ligament injury in elite alpine skiers and their parents. Knee Surg Sports Traumatol Arthrosc. (2016) 24:697–701. doi: 10.1007/s00167-014-2974-9
10. Raschner C, Platzer HP, Patterson C, Werner I, Huber R, and Hildebrandt C. The relationship between ACL injuries and physical fitness in young competitive ski racers: a 10-year longitudinal study. Br J Sports Med. (2012) 46:1065–71. doi: 10.1136/bjsports-2012-091050
11. Fältström A, Hägglund M, Magnusson H, Forssblad M, and Kvist J. Predictors for additional anterior cruciate ligament reconstruction: data from the Swedish national ACL register. Knee Surg Sports Traumatol Arthrosc. (2016) 24:885–94. doi: 10.1007/s00167-014-3406-6
12. Della Villa F, Hägglund M, Della Villa S, Ekstrand J, and Waldén M. Infographic. High rate of second ACL injury following ACL reconstruction in male professional footballers: an updated longitudinal analysis from 118 players in the UEFA elite club injury study. Br J Sports Med. (2021) 55:1379–80. doi: 10.1136/bjsports-2021-104508
13. Della Villa F, Hägglund M, Della Villa S, Ekstrand J, and Waldén M. High rate of second ACL injury following ACL reconstruction in male professional footballers: an updated longitudinal analysis from 118 players in the UEFA elite club injury study. Br J Sports Med. (2021) 55:1350–6. doi: 10.1136/bjsports-2020-103555
14. Paterno MV, Rauh MJ, Schmitt LC, Ford KR, and Hewett TE. Incidence of contralateral and ipsilateral anterior cruciate ligament (ACL) injury after primary ACL reconstruction and return to sport. Clin J Sport Med. (2012) 22:116–21. doi: 10.1097/JSM.0b013e318246ef9e
15. Hewett TE, Myer GD, Ford KR, Paterno MV, and Quatman CE. Mechanisms, prediction, and prevention of ACL injuries: cut risk with three sharpened and validated tools. J Orthop Res. (2016) 34:1843–55. doi: 10.1002/jor.23414
16. Wiggins AJ, Grandhi RK, Schneider DK, Stanfield D, Webster KE, and Myer GD. Risk of secondary injury in younger athletes after anterior cruciate ligament reconstruction: a systematic review and meta-analysis. Am J Sports Med. (2016) 44:1861–76. doi: 10.1177/0363546515621554
17. Nagelli CV, and Hewett TE. Should return to sport be delayed until 2 years after anterior cruciate ligament reconstruction? Biological and functional considerations. Sports Med. (2017) 47:221–32. doi: 10.1007/s40279-016-0584-z
18. Christino MA, Fantry AJ, and Vopat BG. Psychological aspects of recovery following anterior cruciate ligament reconstruction. J Am Acad Orthop Surg. (2015) 23:501–9. doi: 10.5435/JAAOS-D-14-00173
19. Ardern CL, Taylor NF, Feller JA, Whitehead TS, and Webster KE. Psychological responses matter in returning to preinjury level of sport after anterior cruciate ligament reconstruction surgery. Am J Sports Med. (2013) 41:1549–58. doi: 10.1177/0363546513489284
20. Beighton P, Solomon L, and Soskolne CL. Articular mobility in an African population. Ann Rheum Dis. (1973) 32:413–8. doi: 10.1136/ard.32.5.413
21. Daniel DM, Malcom LL, Losse G, Stone ML, Sachs R, and Burks R. Instrumented measurement of anterior laxity of the knee. J Bone Joint Surg Am. (1985) 67:720–6. doi: 10.2106/00004623-198567050-00006
22. Ostenberg A, Roos E, Ekdahl C, and Roos H. Isokinetic knee extensor strength and functional performance in healthy female soccer players. Scand J Med Sci Sports. (1998) 8:257–64. doi: 10.1111/j.1600-0838.1998.tb00480.x
23. Tegner Y, Lysholm J, Lysholm M, and Gillquist J. A performance test to monitor rehabilitation and evaluate anterior cruciate ligament injuries. Am J Sports Med. (1986) 14:156–9. doi: 10.1177/036354658601400212
24. Itoh H, Kurosaka M, Yoshiya S, Ichihashi N, and Mizuno K. Evaluation of functional deficits determined by four different hop tests in patients with anterior cruciate ligament deficiency. Knee Surg Sports Traumatol Arthrosc. (1998) 6:241–5. doi: 10.1007/s001670050106
25. Ware JE, Jr, and Sherbourne CD. The MOS 36-item short-form health survey (SF-36) I Conceptual framework and item selection. Med Care. (1992) 30:473–83. doi: 10.1097/00005650-199206000-00002
26. Hays RD, and Shapiro MF. An overview of generic health-related quality of life measures for HIV research. Qual Life Res. (1992) 1:91–7. doi: 10.1007/BF00439716
27. Nahm FS. Nonparametric statistical tests for the continuous data: the basic concept and the practical use. Korean J Anesthesiol. (2016) 69:8–14. doi: 10.4097/kjae.2016.69.1.8
28. Webster KE, Feller JA, Leigh WB, and Richmond AK. Younger patients are at increased risk for graft rupture and contralateral injury after anterior cruciate ligament reconstruction. Am J Sports Med. (2014) 42:641–7. doi: 10.1177/0363546513517540
29. Andernord D, Desai N, Björnsson H, Gillén S, Karlsson J, and Samuelsson K. Predictors of contralateral anterior cruciate ligament reconstruction: a cohort study of 9061 patients with 5-year follow-up. Am J Sports Med. (2015) 43:295–302. doi: 10.1177/0363546514557245
30. Steidl-Müller L, Hildebrandt C, Müller E, Fink C, and Raschner C. Limb symmetry index in competitive alpine ski racers: reference values and injury risk identification according to age-related performance levels. J Sport Health Sci. (2018) 7:405–15. doi: 10.1016/j.jshs.2018.09.002
31. Garratt AM, and Stavem K. Measurement properties and normative data for the Norwegian SF-36: results from a general population survey. Health Qual Life Outcomes. (2017) 15:51. doi: 10.1186/s12955-017-0625-9
32. Harringe ML, Höög S, and Svensson M. Gymnasts' experiences and perception of a cruciate ligament injury. J Sports Med Phys Fitness. (2021). doi: 10.23736/S0022-4707.21.12358-8
33. Cheney S, Chiaia TA, de Mille P, Boyle C, and Ling D. Readiness to return to sport after ACL reconstruction: a combination of physical and psychological factors. Sports Med Arthrosc Rev. (2020) 28:66–70. doi: 10.1097/JSA.0000000000000263
34. von Rosen P, Frohm A, Kottorp A, Fridén C, and Heijne A. Too little sleep and an unhealthy diet could increase the risk of sustaining a new injury in adolescent elite athletes. Scand J Med Sci Sports. (2017) 27:1364–71. doi: 10.1111/sms.12735
35. Schoeb T, Fröhlich S, Frey WO, Verhagen E, Farshad M, and Spörri J. The ISPA (Int) injury prevention programme for youth competitive Alpine skiers: a controlled 12-month experimental study in a real-world training setting. Front Physiol. (2022) 13:826212. doi: 10.3389/fphys.2022.826212
Keywords: ACL injury, reinjury, alpine skiing, competition, adolescent, ski high school
Citation: Westin M, Mirbach LI and Harringe ML (2022) Side-to-side differences in knee laxity and side hop test may predispose an anterior cruciate ligament reinjury in competitive adolescent alpine skiers. Front. Sports Act. Living 4:961408. doi: 10.3389/fspor.2022.961408
Received: 04 June 2022; Accepted: 16 September 2022;
Published: 14 October 2022.
Edited by:
Thomas Leonhard Stöggl, University of Salzburg, AustriaReviewed by:
Christopher Nagelli, Mayo Clinic, United StatesCopyright © 2022 Westin, Mirbach and Harringe. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marita L. Harringe, bWFyaXRhLmhhcnJpbmdlQGtpLnNl
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.