 Théo Caron1
Théo Caron1 Paquito Bernard
Paquito Bernard Tegwen Gadais
Tegwen Gadais- 1Faculté des Sports et de l’EP, Université D’Artois, Liévin, France
- 2Département des Sciences de l’activité physique, Université du Québec à Montréal, Montréal, QC, Canada
- 3Research Center, University Institute of Mental Health at Montreal, Montréal, QC, Canada
- 4UNESCO Chair in Curriculum Development (UCCD), Université du Québec à Montréal, Montréal, QC, Canada
Introduction: In the last couple of decades, numerous intervention strategies (ISs) have been formulated in school/community or clinical sectors using physical activity (PA) in order to prevent youth obesity because they have been highly effective in addressing this issue. These two sectors have revealed some interesting information in terms of efficient results and best practice mechanisms, but comparisons between them to learn about their functioning have been rare.
Methods: Therefore, the aim of this systematic review was to analyze and synthesize PA ISs from school/community or clinical domains for the period 2013-2017, in French or English, targeting youths aged 5-19 years old through primary, secondary, and tertiary prevention.
Results: In total, 68 full articles were reserved for data extraction and synthesis and 617 were excluded because they did not meet eligibility criteria (61 of 68 were kept for the final analysis). The results identified a number of differences between the studies of the various IS sectors and also a third type of IS, mixed sector. Mixed ISs (clinical and school-community) have a special advantage because they can benefit from the strengths of both school/community-based and clinical-based ISs. Mixed ISs showed the most promising results. This review also highlighted the differences between sectors and their ISs in terms of intervention teams, prevention objectives, duration, materials, and efficiency.
Conclusion: Future studies should focus on establishing a prevention program in a given geographical area involving all stakeholders with their respective skills/knowledge, in the area of decision-making and in the development of ISs, to ensure that the program is the most efficient and best adapted to its environment.
1. Introduction
Nowadays, it is well known that obesity is a chronic pathology with multifactorial origins, defined by the World Health Organization (WHO) as an abnormal or excessive fat accumulation that presents a risk to health (e.g., vascular, endocrine) (1, 2). A study reported that in the last four decades, the number of young obese children (aged 5–19) multiplied by 10 worldwide (3). Another study reported that the rate of youth obesity prevalence increased by 47% in the last three decades (4). To help control this disease condition, the WHO made some recommendations [e.g., physical activity (PA); nutrition] (5, 6) to be followed, in order to adopt a healthy lifestyle and reduce health problems and the risk of obesity.
In parallel, it is also known that PA has many health benefits (physical, mental, and social, among others) that can help reduce obesity and maintain a certain weight when combined with nutrition (7). Moreover, the adoption of a healthy lifestyle during childhood or adolescence tends to spill over into adulthood. Nevertheless, 80% of youths aged 13–15 do not follow those PA recommendations (8) and tend to lead a sedentary lifestyle (9). This sedentariness and inactivity could lead to overweight or obesity (10). To address this issue and curb this tendency, intervention strategies (ISs) and programs integrating PA have been developed and implemented in different settings to prevent overweight and obesity (11). According to Gadais (11), ISs are initiatives and programs with thematic content and events that directly or indirectly aim to facilitate people to adopt healthy lifestyles for the benefit of their immediate and future health. When we look closely at the literature on obesity prevention (12), a few different settings emerge, and two of them have been widely studied (13, 14): the clinical setting on how to manage childhood obesity and the school/community setting on how to deal with obesity prevention and the role of the school in such prevention. It is from this perspective that we decided to focus our work on these two promising intervention sectors.
As we suggested earlier and to quote Lydecker et al. (15), “prevention assumes that individuals have some degree of susceptibility to obesity and would benefit from medical and psychosocial interventions to counter that susceptibility” (15). If the degree of susceptibility to obesity varies from one individual to another, prevention must also take place at different levels: primary, secondary, and tertiary. Primary prevention targets every individual without any distinction, for example, advertisements on television that invite people to be active and eat better. Secondary prevention targets subsamples of the population: people at risk of becoming overweight or obese, for example, children in the upper BMI range or who engage in very little physical activity. Tertiary prevention targets specific individuals who are already overweight or obese with complications, in this case, interventions that aim to help people obtain sufficient weight loss to reduce comorbidities (15–17). These three types of interventions are generally implemented in two major sectors: clinical or school and community sectors.
A clinical setting is a place where people are treated (e.g., hospital, health center). In this context, clinical ISs seem to contain better financial resources (e.g., exergaming) (18) and human resources/expertise to act as a source of quality and reliable information (19). Clinical ISs have also shown good results in the fight against childhood obesity (20–22), making it an important contributor in the management of obesity. Nevertheless, not all studies show good results, as prevention does not involve only treatment, which is mostly the last step of prevention, thus making the ISs of the other sector also useful.
The school and community sector can be seen as a place dedicated to learning where children develop their knowledge and skills (e.g., physical, social, cognitive skills). Many authors agree that school is a privileged place for the prevention of obesity (23–25). Indeed, children and adolescents spend most of their time at school and it is “possible to globally reach the population of interest without stigmatizing or discriminating and without being primarily dependent on families” (26). According to these authors, the school/community sector could assume an important role to promote positive change in children's lifestyles, in order to make them adopt a healthy way of life (11, 27). Yet, some studies have demonstrated that school-based obesity prevention interventions with children have produced limited efficacy (28, 29), generally lacking in financial or human resources, among others.
According to the literature, school/community-based ISs and clinical ISs seem to be different because they do not employ the intervention on the same level of childhood obesity prevention. Interestingly, both seem to show promising results in preventing obesity. Therefore, a question arises: Could it be possible to consider a global prevention strategy (primary, secondary, and tertiary levels) to reduce youth obesity prevalence and incidence in the coming years by integrating the best practices from one sector into another? We, therefore, sought to know if there were relevant elements in the ISs from these two sectors that would help formulate effective strategies for the prevention of obesity among young people through mutual enrichment.
The aims of this study were to
(1) prepare an extensive inventory on the recent literature regarding programs and ISs that aimed at preventing youth obesity, from clinical or school-community perspectives;
(2) extract information in order to identify the mechanisms that make programs effective in a clinical or school/community sector;
(3) propose some recommendations from the point of view of both sectors (clinical and school/community) and improve the current ISs for future studies.
2. Methods
To conduct this systematic review, we followed the six steps of the PRISMA (30) for preparing a flow chart (Figure 1).
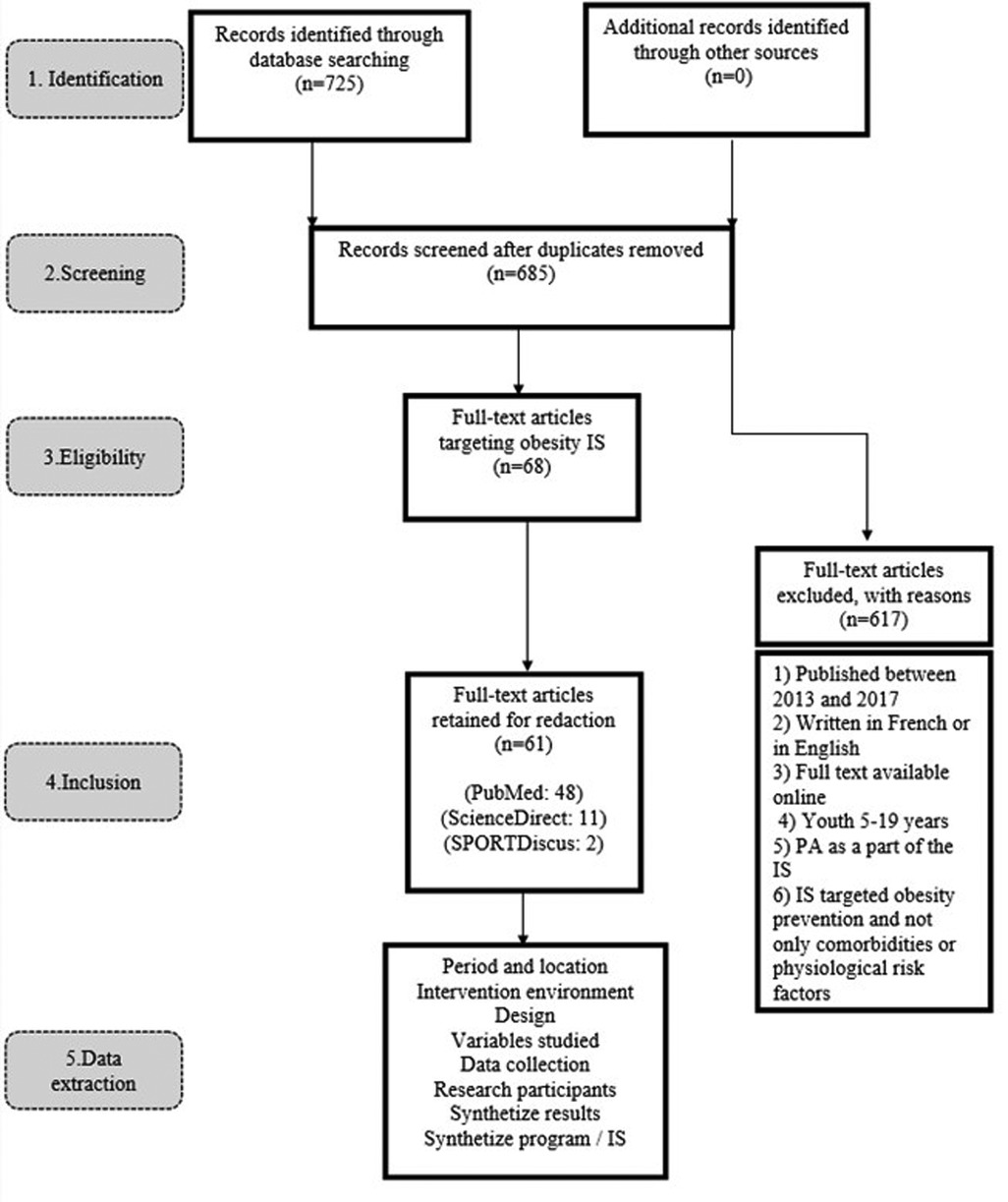
Figure 1. PRISMA flow chart.
2.1. Phase 1: Identification of studies
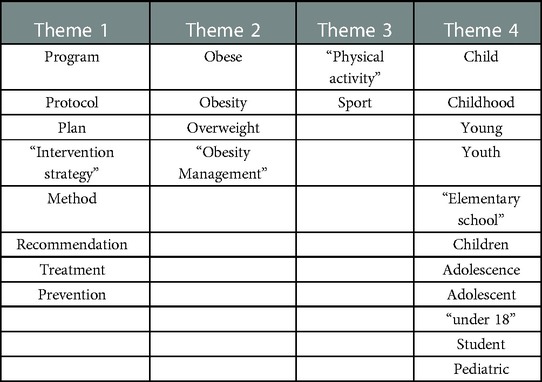
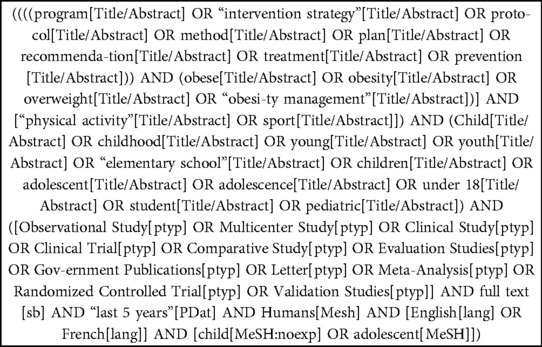
In the first phase, an exhaustive search through computerized databases was performed to identify scientific publications targeting youth obesity prevention. Particularly, we used specific search equations to conduct the first overall research. Relevant articles were identified by means of a computerized search through three databases (i.e., SPORTDiscus, PubMed, and ScienceDirect) with different combinations of keywords (e.g., program; obese; physical activity, child) (Appendix A) and Equations/Meshterms (Appendix B).
2.2. Phase 2: Screening
In phase two, 40 duplicates were eliminated and 685 papers were identified. We started looking for non-systematic reviews and prioritized peer-reviewed articles. Some reports from credible organizations such as government agencies, international agencies, or academic centers were also included in our research (e.g., WHO), but none of them were finally considered.
2.3. Phase 3: Eligibility
The selection of the abstract was done on the basis of inclusion criteria. To dispel any doubts on this process, the third author was consulted. Six inclusion criteria were applied for article eligibility: (1) articles published between 2013 and 2017, (2) those written in French or in English, (3) full text available online, (4) youths 5–19 years’ old targeted by studies, (5) PA as a part of ISs, (6) ISs that targeted obesity prevention and not only comorbidities or physiological risk factors (e.g., diabetes). In total, 68 full articles were reserved for data extraction and synthesis and 617 were excluded because they did not meet the eligibility criteria.
2.4. Phase 4: Inclusion
The fourth phase of the literature search involved obtaining copies of the articles previously identified in phase 3. After collecting the articles, the overall sample was reassessed. A complete reading was made in order to eliminate non-relevant articles (according to inclusion criteria). Finally, 61 articles were retained for data extraction by meeting all inclusion criteria and focusing on the topic of this study.
2.5. Phase 5: Data extraction
A data sheet was used to extract information concerning the date of the study; intervention sector (school/community or clinical); design (collaborative ISs or not); variables studied; data collection (equipment, hardware); participants (non-obese, overweight, obese, age); synthesized results; synthesized ISs. The first and the second author performed data extraction. To dispel any doubts on this process, data synthesis tables were discussed until agreement was reached on the presentation form and what should be extracted. The completion of phase 5 marked the start of the content analysis of the 61 articles.
2.6. Phase 6: Data analysis
To identify the differences, the results will be presented in five different categories (i.e., intervention team, prevention objective, duration, material, and efficiency). As previously mentioned, the intervention sectors (clinical and school/community) are different from each other but show interesting results (10–12). Therefore, it is interesting to see who conducted the intervention, its purpose, the means available, how long the ISs lasted, and the results.
The first author carried out the initial selection in the literature search on the basis of the abstract and title (n = 725). He also performed the initial analysis of the data and wrote the first draft of the manuscript. The second and third authors helped with data analysis and result presentation. They also revised the entire manuscript.
3. Results
3.1. School and community ISs
3.1.1. Intervention team
Of the 36 school/community-based studies (Table 1), 11 used one type of stakeholder. Of these 11, 6 studies involved only teachers (23, 31–35). For example, Grao-Cruces et al. (32) mentioned “weekly follow-up and control by PE teachers” and Sacchetti et al. (23) “taught by the ordinary classroom teacher.” The use of the teacher as the only intervener increases from 54.5% (6/11) to 75% (6/8) (36–38) if we exclude studies occurring only in the community. Twenty-five studies used at least two types of stakeholders (18, 24, 25, 39–60), and eight involved health professionals (e.g., doctors, nurses, psychiatrists) (18, 25, 39, 42, 45, 48, 59, 60). Among these eight, two relied solely on school nurses (42, 48). Globally, six studies involved non-school-based stakeholders with experience in healthcare.

Table 1. Illustrations of studies for school/community ISs.
3.1.2. Prevention objective
Of all the studies aimed at preventing childhood obesity through school/community ISs, nine dealt with secondary or tertiary obesity prevention, since they were only interested in young people who were already overweight or obese (18, 25, 37, 38, 47, 48, 51, 59, 60). For example, Larsen et al. (48) selected “One hundred fifteen 11–13 year-old children with overweight and obesity” and Wright et al. (25) mentioned, “Students (n = 251) were English or Spanish speaking, had a BMI > the 85th percentile”. The majority of the studies (23, 24, 27, 31–36, 39–46, 49, 50, 52–58, 61, 62) directed their attention toward a relatively primary prevention of obesity and did not necessarily target an overweight or obese population but rather an entire population. For example, Lau et al. (49) mentioned, “the average BMI was 17, which was within a healthy range.” These studies tended to include children “at risk” as their participants because of the absence of selection criteria. For example, Smith et al.'s (57) intervention group included 2 underweight children, 110 normal weight, 39 overweight, and 30 obese.
3.1.3. Duration
The duration of 19 of the studies was a year or more (23, 24, 31, 33, 36, 39, 41–43, 45, 51, 52, 54–56, 58, 59, 61, 62). For example, Erfle and Gamble (42) reported “30 min of daily PE throughout 1 academic year” and Santos et al. (24) mentioned, “performed during the 2009–2010 school year.” Of the 17 remaining with a shorter duration, 14 of them lasted 6 months or less (18, 25, 32, 34, 37, 38, 40, 44, 46–49, 53, 60). Larsen et al. (48) used “the six-week intervention” and Parra-Medina et al. (53) “a 12-week family focused healthy lifestyle program.”
3.1.4. Material
Studies from the school/community sector did not automatically consider BMI with age and sex in their anthropometric measurement (e.g., BMI z-score, BMI percentile). Two studies did not consider anthropometric measurement in their outcomes (40, 46) and two others considered only BMI (not for age and sex) (49, 59). Of the 34 studies with anthropometric measurements, 23 were based on a measurement related to BMI or abdominal circumferences (e.g., BMI score, waist circumference). Other studies (indicating anthropometric measurements) systematically considered at least a second objective measure such as dual energy x-ray absorptiometry (DXA) (one study), skinfold thickness (three studies), or impedance (seven studies). Ning et al. (37) mentioned that “body composition was assessed by bioelectrical impedance analysis (…) body composition was also estimated at baseline and 6 months using dual x-ray absorptiometry” and Johnston et al. (47) mentioned that “body composition was assessed using triceps skinfold thickness.” For studies that assessed PA measurement (32/36), 20 used one objective measurement (not a self-reported). Among these, the most common instruments were accelerometer (9 studies), pedometer (5 studies), and various fitness tests (13 studies) (e.g., Fitnessgram). For example, Larsen et al. (48) used a “progressive bicycle ergometer protocol (…) Actigraph GT3X + for ten consecutive days” and Grao-Cruces et al. (32) reported that “a pedometer was used for evaluation and follow-up purposes.” Finally, regarding nutrition, 19 studies collected data. Most of them were carried out through three types of instruments: survey (15 studies), recall/diary (6 studies), and interview (1 study). For example, Ning et al. (37) mentioned that it was “assessed by a 48-hr diet recall.”
3.1.5. Efficacy
In the school/community sector, the major objective tended to be the prevention of obesity, and interestingly, “lose weight” was not the first goal.
However, 26 studies still presented significant positive results regarding the anthropometric measurements of the participants (e.g., BMI, waist circumferences) (18, 23–25, 31–35, 37–39, 41, 42, 45, 47, 48, 50–52, 55, 56, 59–62). Nevertheless, some studies showed effects only on a part of the population (25, 33) or “mixed effects” (23, 41, 56). Of the 10 remaining studies, which did not clearly show an effect on BMI, 9 had, at least, a significant influence on health factors (36, 40, 43, 44, 46, 49, 54, 57, 58) (e.g., physical, psychological, or nutritional). To illustrate, Smith et al. (57) showed that “significant intervention effects were found for screen time (mean SE: −30 ± 10.08 min/day; p = 0.03), sugar-sweetened beverage consumption (mean: −0.6 ± 0.26 glass/day; p = 0.01).” Only the article by Parra-Medina et al. (53) showed no significantly interesting effect on children because “child participants that completed the program (n = 72) showed no improvements.”
3.2. Clinical ISs
3.2.1. Intervention team
Of the 19 studies we identified (Table 2) in the literature and that were carried out in a clinical setting, 3 (19, 63, 64) used a single type of contributor. It was systematically a doctor who delivered recommendations on psychological, nutritional, or PA. For Brennan et al. (63), “the clinician discussed topics such as physical activity, nutrition, helpful thoughts and emotions,” and for Davis et al. (64), “the clinician covered several topics such as self-esteem, energy balance, portion size, screen time and sedentary.” The 16 remaining studies included a multidisciplinary team composed of at least two specialists (65–80). For example, for Nemet et al. (73), “the intervention team was composed of 3 specialists: dietitian, coach and physician” and Endevelt et al. (68) used a “multidisciplinary team including a pediatrician, a dietician, a physical activity expert, and a social worker.”
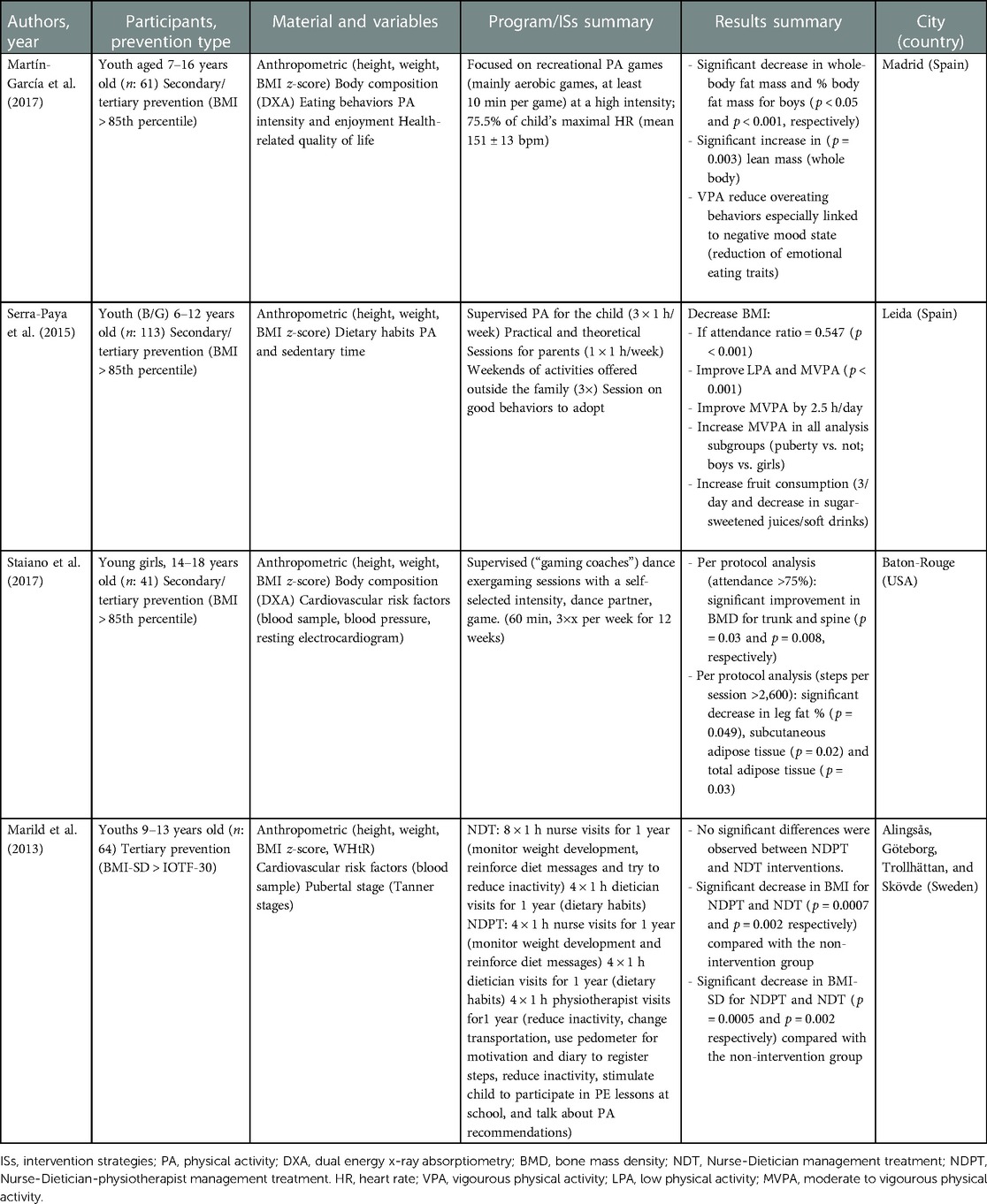
Table 2. Illustrations of studies for clinical ISs.
3.2.2. Prevention objective
None of the studies targeted the primary prevention of obesity and 18 of them worked on secondary or tertiary prevention of obesity, because they only targeted participants with a BMI >85th percentile. For example, Staiano et al. (79) selected only participants with a BMI percentile >85th, according to the Center of Disease Control (CDC) growth chart; and Serra-Paya et al. (76) selected children overweight or obese, according to the International Obesity Task Force (IOTF) criteria. Only one study (19) used a BMI between the 75th and the 95th percentiles as an inclusion criterion. Nevertheless, participants were judged at risk of weight gain due to their BMI, based on their last medical consultation.
3.2.3. Duration
For the duration of the ISs, 16 studies covered at least 1 year (63–69, 71–79). Luca et al. (70) mentioned a “2-year interdisciplinary obesity management program.” Moreover, 10/19 studies had an effective duration of less than or equal to 6 months (64, 65, 69, 72–75, 77–79). Martín-García et al. (72) implemented a 3-month vigorous physical activity plan and Staiano et al. (78) a 12-week group exergaming intervention. It should also be noted that all studies covering one or more years consisted of only a few meetings throughout the year. To illustrate, for Stettler et al. (19), the ISs consisted of 12 meetings of 15–25 min over 12 months, and for Luca et al. (70), it was 6 meetings of 2 h per week, then 1.5 h every 2 weeks the first year, and 1.5 h monthly until the 18th month.
3.2.4. Material
Anthropometric measurement at the clinical level consistently considered BMI by age and sex (BMI score). Nevertheless, in 10 studies, BMI was coupled with a second measure related to body composition and something more (19, 63, 65, 69, 71, 72, 76–79) [DXA (4 studies), skinfold thickness (2 studies), Waist to Height Ratio (WHtR) (2 studies), and impedance (1 study)]. For example, Staiano et al. (78) used DXA to assess body composition and quantify body fat, and Gerards et al. (69) measured skinfold thickness to evaluate the percentage of body fat. With regard to PA, 12 studies used one or more objective measurements (63, 65, 66, 69–74, 76, 78, 79). Of these 12, the pedometer was used in 2 studies; PA was tested in 5 studies, and accelerometers in 7 studies. Brennan et al. (63) used a cycle ergometer test to assess cardiovascular fitness and participants had to get an accelerometer fixed on them to have their physical activity assessed. With regard to nutrition, measurements were made in 14 studies (19, 63–70, 72–76) and three tools were frequently used: survey (3 studies), interview (4 studies), and dietary recall (5 studies). Nemet et al. (74) mentioned the “use of a 48-h dietary recall”; Davis et al. (64) spoke about the “use of a 24-h dietary recall,” and Brennan et al. (63) referred to the “use of a dietary checklist and of the Fat, Fruit and Vegetables Diet Questionnaire (FFVDQ).” It should be noted that some studies did not clearly mention their measurement instruments.
3.2.5. Efficacy
In the context of secondary or tertiary prevention of obesity, one of the main objectives remained BMI decrease and fat loss in favor of lean mass. Out of 19, 14 (73.68%) studies showed significant effects on BMI or participant body fat (19, 63–65, 68, 71–75, 77–80). For example, Marild et al. (71) “reported a significant reduction in BMI and BMI-SD in the Nurse-Dietician-Physiotherapist managed treatment compared to the control group with obesity (p = 0.0007 and p = 0.0005 respectively).” Nevertheless, some studies showed significant effects only on some of their participants. For example, Martín-García et al. (72) “found that, in the intervention group, boys decreased their whole-body fat mass (p < 0.04) and reduced their percentage of body fat (p < 0.001); moreover, boys’ body lean mass increased significantly (p = 0.003).” Of the five other studies that did not have a direct effect on BMI, four had at least a significant influence on physical, psychological, or nutritional health factors (66, 69, 70, 76). Furthermore, in these studies, the intervention group was compared with a control group performing a “less advanced” intervention. Serra-Paya et al. (76) mentioned that “the intervention group received organized physical activity sessions, theoretical and practical sessions for parents, behavior counselling for children and parents, 3 weekend activities organized outside the family for children; unlike the counselling group that received only the behavior counselling sessions.” Only one article showed no effects (67).
3.3. Mixed ISs
3.3.1. Intervention team
Of the six studies we identified (Table 3) and that were carried out in a “mixed” setting (school/community and clinical), all of them used at least two types of contributors, with one (or more) having health-related skills or knowledge. Rito et al. (81) reported that “four individual counselling sessions performed by trained nutritionists (…) healthy cooking workshops performed by a certified renowned ‘chef’ in a school kitchen.” All of these studies used a multidisciplinary team having in common a dietician. Maatoug et al. (82) mentioned that the ISs “included a multidisciplinary team with a pediatrician, dietician, physical activity teacher and psychologist.”

Table 3. Illustrations of studies for mixed ISs.
3.3.2. Prevention objective
All these studies were part of a secondary or a tertiary prevention of obesity, because they were interested only in children who were already overweight or obese. Four of them were based on data on overweight and obesity for age and sex of CDC (BMI > 85th percentile). For example, Morano et al. (83) selected participants “with a BMI ≥ 85th percentile for age and sex according to the CDC growth reference” and Sanders et al. (84) selected “overweight or obese based on the CDC growth chart.” The two remaining studies were based on different data from the WHO: in Maatoug et al. (82), “Z-score were derived using the world health organization references” or from English references; in Kokkvoll et al. (85), “≥98th percentile according to the UK references.” None of these studies were directly concerned with the primary prevention of the pathology.
3.3.3. Duration
With regard to these mixed studies, two had a duration above or equal to 1 year (82, 85). Kokkvol et al.'s (85) ISs lasted 2 years, and Maatoug et al.'s (82) ISs (50%) lasted 1 year and the remaining (50%) lasted 6 months or less (81, 83, 84). Sanders et al. (84) formulated a 4-week IS. Only Rieder et al.’s (86) strategies had an “intermediate” duration equal to 9 months. It should be noted that, unlike the clinical studies previously seen, the frequency of proposed activities or meetings with professionals was higher in mixed programs lasting 1 year or more. For example, Kokkvoll et al. (85) used “weekly group-based physical activity” and Maatoug et al. (82) used “twice-a-week physical activity sessions in school.”
3.3.4. Material
Anthropometric measurements, in these mixed studies, systematically considered BMI for age and sex (e.g., BMI z-score, BMI percentile). Nevertheless, it was not the only measurement, because in three studies, this was combined with at least one other measurement of body composition [WC (three studies), skinfold thickness (two studies), impedance (one study)]. For example, Kokkvoll et al. (85) used “bioelectrical impedance,” in Morano et al. (83), “Skinfold thickness was determined (…) with a skinfold caliper,” and in Rito et al. (81), “waist circumference was obtained for every child.” With regard to PA, three studies clearly used an objective measurement coupled with a second self-reported one. This helped avoid over/underestimating the results. Sanders et al. (84) mentioned that “pre- and post-intervention fitness tests were administered to participants (…) program participants and their parents completed a physical activity and nutrition behavior questionnaire.” The other studies were based only on self-reported data [Maatoug et al. (82) mentioned that participants “responded to a 24 h food and physical activity recall questionnaire”] or no PA measurement was done in them (85). Three tools were mainly used to measure nutrition: questionnaire (two studies), 24 h recall (two studies), and a 7-day dietary diary (one study). For example, Morano et al. (83) reported, “dietary habits were assessed with a 7-day food diary.” Only in one study, nutritional measurement (85) was not performed.
3.3.5. Efficacy
As mentioned previously, all mixed studies focused on secondary or tertiary prevention of obesity. One of the major objectives was therefore to influence downward BMI and weight in order to reduce the fat mass of the participants. Of the six programs, five had direct effects on BMI (81–85). One article did not show significant BMI reduction, even though it indicated a tendency to slow its growth. Rieder et al. (86) mentioned that percentile BMI measurements taken before and after the intervention indicated a general upward trend (p = 0.0003). Nevertheless, during the intervention period, the slope of the BMI percentile showed a downward trend (p = −0.0001). Moreover, a comparison of the results of the preintervention phase and the intervention phase showed significant variations (p = 0.003). “For intervals T12 to T0 vs. T0 to T9, there were significant decreases in rates of gain in BMI (0.13 vs. 0.04, p < 0.01, BMI percentile [0.0002 vs. −0.0001, p < 0.01].”
Each of these studies also presented at least one positive variation on one of the various health, physical, psychological, or nutritional factors. For example, Maatoug et al. (82) showed positive effects on PA, p-value (pre-post) = 0.001, and reduction of caloric intake; p-value (pre-post) < 0.001; Rito et al. (81) mentioned “vigorous physical activity (day/week), CI 95% 0.1–0.5, p-value = 0.008” and Morano et al. (83) showed that “Actual (p < 0.001) and perceived (p < 0.03) physical abilities, physical activity enjoyment (p = 0.03), and psychosocial HRQoL (p < 0.05) also improved from pre- to post-intervention.”
4. Discussion
4.1. Summary of the findings
This study identified a number of differences between the studies of the various IS settings (Table 4); these differences could be grouped into five elements (intervention team, prevention objective, duration, material, and results).
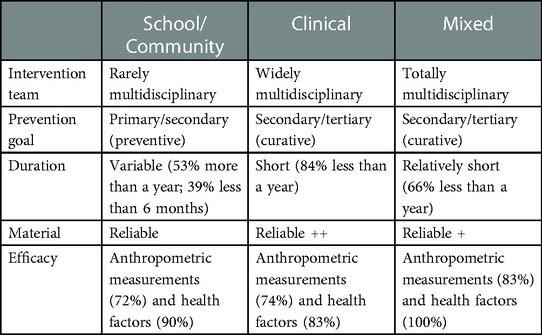
Table 4. Results summary.
Intervention team: The intervention team in the school/community was mostly composed of a single stakeholder that was often the teacher (54.5% of cases). In the clinical and mixed sectors, the ISs largely depended on a multidisciplinary team with various members specialized in health. In both sectors, stakeholders contributed to the success of the ISs as key actors.
Prevention objective: The school/community ISs mainly targeted primary prevention because there was no selection of participants, while participants in the other sector were chosen by targeted criteria such as overweight or obese (according to their BMI for age and sex), and the same was the case for mixed studies.
Duration: One interesting point in the school/community setting was that it allowed for a relatively long intervention duration, and ISs aimed at preventing obesity needed time to embed and develop before being evaluated (60). On the other hand, clinical and mixed ISs tended to last for a shorter period of time. More than three-fourths of the studies done in the clinical setting and two-third in the mixed setting lasted less than a year.
4.2. Findings: What can be understood and learned?
4.2.1. Material
Clinical and mixed ISs tended to use more objective instruments, requiring more skills and knowledge. This allowed them to associate and combine certain measurements to achieve more accurate results and not over/underestimate their results.
4.2.2. Efficacy
Many authors agreed (23–25) that school was a privileged place for prevention. Our results seem to confirm this tendency, because school/community ISs showed significant and promising results both on anthropometric measurements relative to obesity (72%) and on health-related factors (90%). The clinical setting was also a beneficial location for the treatment of obesity (secondary/tertiary preventions). This setting was seen as a source of quality and reliable information (17) and it provided important results on both obesity (74% of the studies) and health-related factors (83% of the studies) (87).
4.3. Prospects
In light of these findings, it is necessary that mixed studies should be prioritized, with a combination of school/community-based and clinical-based strengths. Indeed, our study found that mixed ISs provided the most promising results; 83% of the studies showed a positive influence on obesity and 100% on health-related factors. Nevertheless, those we considered sought to apply a relatively clinical model to the school/community setting (82) but did not participate in an exchange relationship, and therefore, the strengths of school/community-based ISs were “left behind.” To enhance global obesity prevention and in line with health recommendations to prevent childhood obesity, Table 5) proposes recommendations for future studies to be more effective.
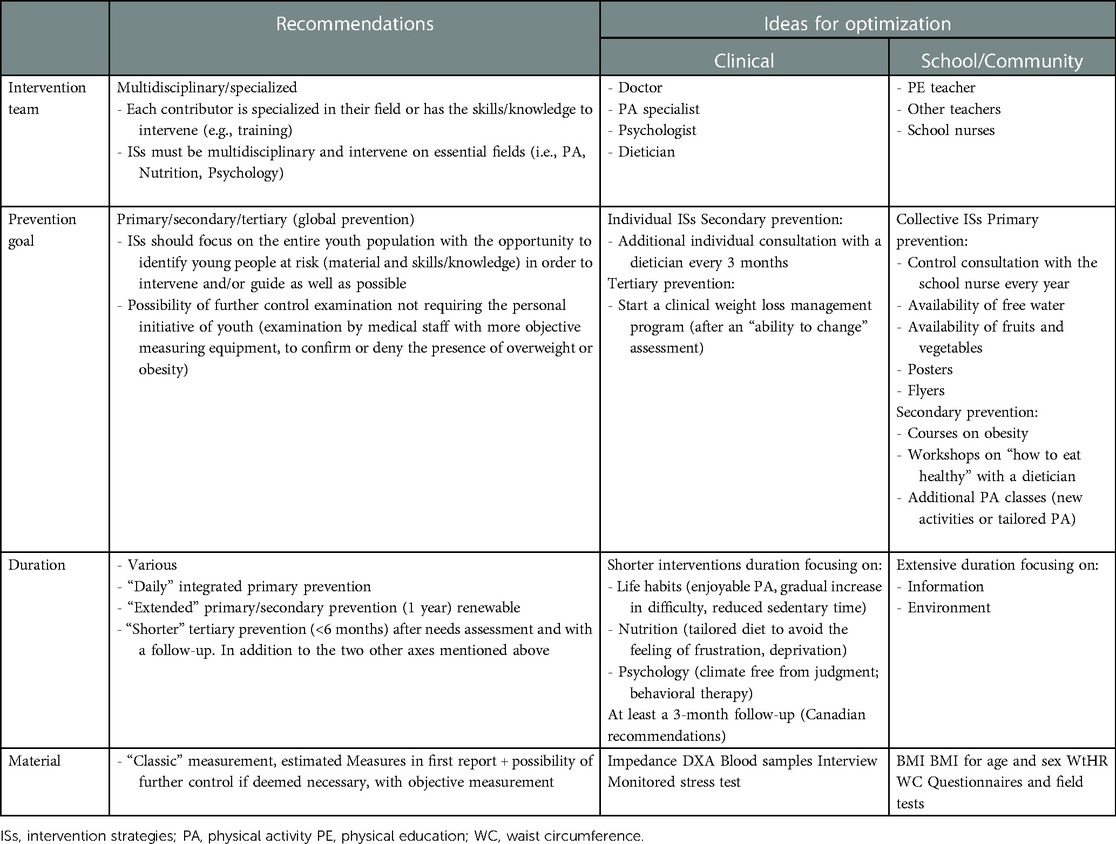
Table 5. Recommendations for future ISs.
Clinical:
- Multidisciplinary team with specialists;
- Objective measurements;
- Relative efficiency to treat.
School/Community:
- Pleasure/enjoyment;
- Various activities;
- Relative efficiency to prevent;
- Time (place where children spend most of their time).
For the purposes of synthesis (Figure 2), we recommend the implementation of a transparent local council involving the entire local community (e.g., school children, representatives, clinical specialists, stakeholders, parents, associative representatives) (25) responsible for the development, improvement, and implementation of prevention programs at the local level. The most important point here is that each intervention sector should have its own prerogatives. Nevertheless, to achieve effective obesity prevention, the different settings need to function in a more transparent manner without ignoring the three different aspects of prevention (primary secondary = school/community; secondary tertiary = clinical). Another interesting aspect is the use of new technologies in prevention. On this point, further studies are needed to evaluate the potential added value of technological tools in obesity prevention.
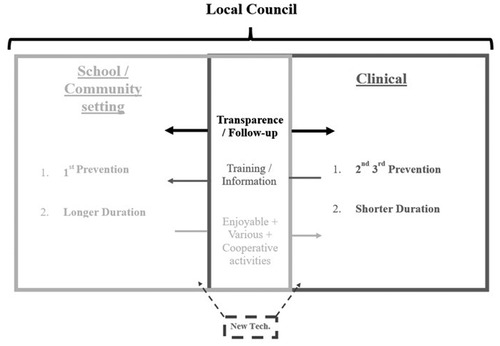
Figure 2. Modelling of physical activity ISs.
4.4. Limitations
Many studies use BMI as a measurement variable or other variables related to it. However, although it is easy to use, BMI alone is not a representative indicator of the benefits of a program. Morano et al. (83) showed that the use of multiple body composition measurements provide better indications of changes in body fat, which is more representative of expected changes. Furthermore, weight-related measurements can skew the results (72). In PA-oriented programs, which lead to positive body composition change (e.g., lean mass gain and body fat loss), the participant weight can increase (lean mass is heavier), which can induce an increase in BMI measurements. This lack of precision relative to these measurements can also distort the results of the studies that use only BMI as the measurement variable or variables relative to the weight of the participants (22).
A second limitation could be the lack of information about programs in some studies to assess the quality of the study. This sometimes makes it difficult to identify the equipment used, the staff involved, and their skills/knowledge. The duration of the program is another limitation. Indeed, all the identified studies do not last the same amount of time (e.g., more than 1 year; less than 6 months; a few weeks). Furthermore, they do not use the same evaluation time (e.g., pre-post; pre-post + follow-up). It is, therefore, difficult to evaluate the effectiveness of one IS in relation to another over a short period of time. Moreover, to assess the efficacy of ISs, more time is required to embed them (60). The number of participants in each study is also highly variable and therefore can make a generalization or a comparison with other studies impossible. The last limitation pertains to the number of studies selected for each setting. Indeed, the number of studies being relatively low in the mixed setting can lead to an over/underestimation of the results. Nevertheless, this work seems to yield promising results, and future studies must continue to move to mixed setting, to nested ISs.
5. Conclusion
The main objective of this study was to propose a first combination and comparison of obesity prevention intervention programs from the clinical and the school or community sectors. However, our review showed that comparisons are difficult to make since the standards and units used for measurements are different and vary according to the protocols and areas of application. Nevertheless, we believe that this study offers an initial proposal for bridging the gap between the clinical and the school/community sectors, the two most promising sectors in terms of outcomes for obesity prevention in youth in particular.
Future studies should focus on establishing a prevention program in a given geographical area (e.g., town, county), involving all stakeholders with their respective skills/knowledge, in the decision-making process and in the development of ISs (e.g., parent association, professors, doctors, local representatives, sports association), so that it becomes the most efficient and best adapted to its environment. Although this study focused on physical activity interventions, it would be relevant to also look at nutrition interventions, since nutrition is a major theme in obesity prevention. The main objective of this study was to propose a first combination of obesity prevention intervention programs with the clinical and the school or community sectors. Our review showed that comparisons are difficult since the standards and units used to measure are different and vary according to the protocols and areas of application. However, we believe that this study offers an initial proposal for bridging the gap between the clinical and school/community sectors, the two most promising sectors in terms of outcomes for obesity prevention in youth in particular.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
Conceptualization was done by TC and TG; the methodology of the study was prepared by TC and TG; software was provided by PB; validation was done by TC, PB, and TG; formal analysis was done by TC; investigation was performed by TC; resources were provided by TG; data curation was done by PB and TG; writing—original draft preparation—was done by TC; writing—review and editing—was done by PB and TG; supervision was carried out by TG; project administration was looked after by TC. All authors contributed to the article and approved the submitted version.
Acknowledgments
The authors would like to gratefully thank Jean Jacques Rondeau for the support and help with the literature review process and Antony Karelis and Dawn Deakin for the revision of the language and manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Haute Autorité de Santé. Surpoids et obésité de l’enfant et de l’adolescent–Actualisation des recommandations 2003, France (2011) (English version available). Retrieved from: https://www.has-sante.fr/jcms/c_964941/fr/surpoids-et-obesite-de-l-enfant-et-de-l-adolescent-actualisation-des-recommandations-2003
2. Faucher P, Poitou C. Physiopathologie de l’obésité. Revue du Rhumatisme Monographies. (2016) 83(1):6–12. doi: 10.1016/j.monrhu.2015.08.002
3. Abarca-Gómez L, Abdeen ZA, Hamid ZA, Abu-Rmeileh NM, Acosta-Cazares B, Acuin C, et al. Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: a pooled analysis of 2416 population-based measurement studies in 128·9 million children, adolescents, and adults. Lancet. (2017) 390(10113):2627–42. doi: 10.1016/S0140-6736(17)32129-3
4. Matta J, Carette C, Lange CR, Czernichow S. Épidémiologie de l’obésité en France et dans Le Monde. La Presse Médicale. (2018) 47(5):434–8. doi: 10.1016/j.lpm.2018.03.023
5. Janssen I, LeBlanc AG. Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. Int J Behav Nutr Phys Act. (2010) 7(1):40. doi: 10.1186/1479-5868-7-40
6. Organisation Mondiale de la Santé. Recommandations mondiales en matière d’activité physique pour la santé [En ligne] (2010). Retrieved from https://apps.who.int/iris/bitstream/handle/10665/44436/9789242599978_fre.pdf;jsessionid=F3EF54B6491423A5304AF5AA80555022?sequence=1
7. Duclos M, Duché P, Guezennec C-Y, Richard R, Rivière D, Vidalin H. Position de consensus: activité physique et obésité chez l’enfant et chez l’adulte. Sci Sports. (2010) 25(4):207–25. doi: 10.1016/j.scispo.2010.04.001
8. Hallal PC, Andersen LB, Bull FC, Guthold R, Haskell W, Ekelund U, et al. Global physical activity levels: surveillance progress, pitfalls, and prospects. Lancet. (2012) 380(9838):247–57. doi: 10.1016/S0140-6736(12)60646-1
9. Cooper AR, Goodman A, Page AS, Sherar LB, Esliger DW, van Sluijs EM, et al. Objectively measured physical activity and sedentary time in youth: the international children’s accelerometry database (ICAD). Int J Behav Nutr Phys Act. (2015) 12(1):113. doi: 10.1186/s12966-015-0274-5
10. Ekelund U, Ja L, Sherar LB, Esliger DW, Griew P, Cooper A, et al. Moderate to vigorous physical activity and sedentary time and cardiometabolic risk factors in children and adolescents. J Am Med Assoc. (2012) 307(7):704–12. doi: 10.1001/jama.2012.156
11. Gadais T. Les stratégies d’intervention pour aider les jeunes à gérer leur pratique d’activité physique. Une revue de la littérature. Staps. (2015) 3:57–77. doi: 10.3917/sta.109.0057
12. Lavie CJ, Laddu D, Arena R, Ortega FB, Alpert MA, Kushner RF. Healthy weight and obesity prevention: JACC health promotion series. J Am Coll Cardiol. (2018) 72(13):1506–31. doi: 10.1016/j.jacc.2018.08.1037
13. Foster C, Moore J, Singletary C, Skelton J. Physical activity and family-based obesity treatment: a review of expert recommendations on physical activity in youth. Clin Obes. (2018) 8(1):68–79. doi: 10.1111/cob.12230
14. Weihrauch-Blüher S, Kromeyer-Hauschild K, Graf C, Widhalm K, Korsten-Reck U, Jödicke B, et al. Current guidelines for obesity prevention in childhood and adolescence. Obes Facts. (2018) 11(3):263–76. doi: 10.1159/000486512
15. Lydecker JA, Cotter E, Gow RW, Kelly NR, Mazzeo SE. Preventing childhood obesity. In: Eating disorders and obesity: a counselor's guide to prevention and treatment (2015). p. 167–99. https://doi.org/10.1002/9781119221708.ch8 Wiley Library online
16. Daniels SR, Arnett DK, Eckel RH, Gidding SS, Hayman LL, Kumanyika S, et al. Overweight in children and adolescents: pathophysiology, consequences, prevention, and treatment. Circulation. (2005) 111(15):1999–2012. doi: 10.1161/01.CIR.0000161369.71722.10
17. Garvey WT. The diagnosis and evaluation of patients with obesity. Curr Opin Endocr Metab Res. (2019) 4:50–7. doi: 10.1016/j.coemr.2018.10.001
18. Staiano AE, Abraham AA, Calvert SL. Adolescent exergame play for weight loss and psychosocial improvement: a controlled physical activity intervention. Obesity. (2013) 21(3):598–601. doi: 10.1002/oby.20282
19. Stettler N, Wrotniak BH, Hill DL, Kumanyika SK, Xanthopoulos MS, Nihtianova S, et al. Prevention of excess weight gain in paediatric primary care: beverages only or multiple lifestyle factors. The smart step study, a cluster-randomized clinical trial. Pediatr Obes. (2015) 10(4):267–74. doi: 10.1111/ijpo.260
20. Most SW, Højgaard B, Teilmann G, Andersen J, Valentiner M, Gamborg M, et al. Adoption of the children’s obesity clinic’s treatment (TCOCT) protocol into another Danish pediatric obesity treatment clinic. BMC Pediatr. (2015) 15(1):13. doi: 10.1186/s12887-015-0332-9
21. Walsh AD, Lioret S, Cameron AJ, Hesketh KD, McNaughton SA, Crawford D, et al. The effect of an early childhood obesity intervention on father's obesity risk behaviors: the Melbourne InFANT program. Int J Behav Nutr Phys Act. (2014) 11:18. doi: 10.1186/1479-5868-11-18
22. Sessa F, Polito R, Monda V, Scarinci A, Salerno M, Carotenuto M, et al. Effects of a plastic-free lifestyle on urinary bisphenol A levels in school-aged children of southern Italy: a pilot study. Front Public Health. (2021) 9:626070. doi: 10.3389/fpubh.2021.626070
23. Sacchetti R, Ceciliani A, Garulli A, Dallolio L, Beltrami P, Leoni E. Effects of a 2-year school-based intervention of enhanced physical education in the primary school. J Sch Health. (2013) 83(9):639–46. doi: 10.1111/josh.12076
24. Santos RG, Durksen A, Rabbanni R, Chanoine JP, Lamboo Miln A, Mayer T, et al. Effectiveness of peer-based healthy living lesson plans on anthropometric measures and physical activity in elementary school students: a cluster randomized trial. JAMA Pediatr. (2014) 168(4):330–7. doi: 10.1001/jamapediatrics.2013.3688
25. Wright K, Giger JN, Norris K, Suro Z. Impact of a nurse-directed, coordinated school health program to enhance physical activity behaviors and reduce body mass index among minority children: a parallel-group, randomized control trial. Int J Nurs Stud. (2013) 50(6):727–37. doi: 10.1016/j.ijnurstu.2012.09.004
26. Kriemler S, Meyer U, Martin E, van Sluijs EM, Andersen LB, Martin BW. Effect of school-based interventions on physical activity and fitness in children and adolescents: a review of reviews and systematic update. Br J Sports Med. (2011) 45(11):923–30. doi: 10.1136/bjsports-2011-090186
28. Hung L-S, Tidwell DK, Hall ME, Lee ML, Briley CA, Hunt BP. A meta-analysis of school-based obesity prevention programs demonstrates limited efficacy of decreasing childhood obesity. Nutr Res. (2015) 35(3):229–40. doi: 10.1016/j.nutres.2015.01.002
29. Kain J, Concha F, Moreno L, Leyton B. School-based obesity prevention intervention in Chilean children: effective in controlling, but not reducing obesity. J Obes. (2014) 2014:1–9. doi: 10.1155/2014/618293
30. Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. (2015) 4(1):1. doi: 10.1186/2046-4053-4-1
31. Bai Y, Saint-Maurice PF, Welk GJ, Russell DW, Allums-Featherston K, Candelaria N. The longitudinal impact of NFL PLAY 60 programming on youth aerobic capacity and BMI. Am J Prev Med. (2017) 52(3):311–23. doi: 10.1016/j.amepre.2016.10.009
32. Grao-Cruces A, Ruiz-López R, Moral-García J-E, Ruiz-Ariza A, Martínez-López EJ. Effects of a steps/day programme with evaluation in physical education on body mass index in school children 11-12 years of age. Kinesiology. (2016) 48(1):132–41. doi: 10.26582/k.48.1.2
33. Grydeland M, Bjelland M, Anderssen SA, Klepp KI, Bergh IH, Andersen LF, et al. Effects of a 20-month cluster randomised controlled school-based intervention trial on BMI of school-aged boys and girls: the HEIA study. Br J Sports Med. (2014) 48(9):768–73. doi: 10.1136/bjsports-2013-092284
34. Melnyk BM, Jacobson D, Kelly SA, Belyea MJ, Shaibi GQ, Small L, et al. Twelve-month effects of the COPE healthy lifestyles TEEN program on overweight and depressive symptoms in high school adolescents. J Sch Health. (2015) 85(12):861–70. doi: 10.1111/josh.12342
35. Smith JJ, Morgan PJ, Plotnikoff RC, Stodden DF, Lubans DR. Mediating effects of resistance training skill competency on health-related fitness and physical activity: the ATLAS cluster randomised controlled trial. J Sports Sci. (2016) 34(8):772–9. doi: 10.1080/02640414.2015.1069383
36. Madsen K, Thompson H, Adkins A, Crawford Y. School-community partnerships: a cluster-randomized trial of an after-school soccer program. JAMA Pediatr. (2013) 167(4):321–6. doi: 10.1001/jamapediatrics.2013.1071
37. Ning Y, Yang S, Evans RK, Stern M, Sun S, Francis GL, et al. Changes in body anthropometry and composition in obese adolescents in a lifestyle intervention program. Eur J Nutr. (2014) 53(4):1093–102. doi: 10.1007/s00394-013-0612-9
38. Trost SG, Sundal D, Foster GD, Lent MR, Vojta D. Effects of a pediatric weight management program with and without active video games a randomized trial. JAMA Pediatr. (2014) 168(5):407–13. doi: 10.1001/jamapediatrics.2013.3436
39. Bonsergent E, Agrinier N, Thilly N, Tessier S, Legrand K, Lecomte E, et al. Overweight and obesity prevention for adolescents: a cluster randomized controlled trial in a school setting. Am J Prev Med. (2013) 44(1):30–9. doi: 10.1016/j.amepre.2012.09.055
40. Dubuy V, De Cocker K, De Bourdeaudhuij I, Maes L, Seghers J, Lefevre J, et al. Evaluation of a real world intervention using professional football players to promote a healthy diet and physical activity in children and adolescents from a lower socio-economic background: a controlled pretest-posttest design. BMC Public Health. (2014) 14:457. doi: 10.1186/1471-2458-14-457
41. Elder JP, Crespo NC, Corder K, Ayala GX, Slymen DJ, Lopez NV, et al. Childhood obesity prevention and control in city recreation centres and family homes: the MOVE/me Muevo Project. Pediatr Obes. (2014) 9(3):218–31. doi: 10.1111/j.2047-6310.2013.00164.x
42. Erfle SE, Gamble A. Effects of daily physical education on physical fitness and weight status in middle school adolescents. J Sch Health. (2015) 85(1):27–35. doi: 10.1111/josh.12217
43. Folta SC, Kuder JF, Goldberg JP, Hyatt RR, Must A, Naumova EN, et al. Changes in diet and physical activity resulting from the shape up Somerville community intervention. BMC Pediatr. (2013) 13:157. doi: 10.1186/1471-2431-13-157
44. Gesell SB, Sommer EC, Lambert EW, Vides de Andrade AR, Whitaker L, Davis L, et al. Comparative effectiveness of after-school programs to increase physical activity. J Obes. (2013) 2013:576821. doi: 10.1155/2013/576821
45. Guo H, Zeng X, Zhuang Q, Zheng Y, Chen S. Intervention of childhood and adolescents obesity in Shantou city. Obes Res Clin Pract. (2015) 9(4):357–64. doi: 10.1016/j.orcp.2014.11.006
46. Herbert PC, Lohrmann DK, Seo DC, Stright AD, Kolbe LJ. Effectiveness of the energize elementary school program to improve diet and exercise. J Sch Health. (2013) 83(11):780–6. doi: 10.1111/josh.12094
47. Johnston CA, Moreno JP, Gallagher MR, Wang J, Papaioannou MA, Tyler C, et al. Achieving long-term weight maintenance in Mexican-American adolescents with a school-based intervention. J Adolesc Health. (2013) 53(3):335–41. doi: 10.1016/j.jadohealth.2013.04.001
48. Larsen KT, Huang T, Ried-Larsen M, Andersen LB, Heidemann M, Moller NC. A multi-component day-camp weight-loss program is effective in reducing BMI in children after one year: a randomized controlled trial. PLoS One. (2016) 11(6):e0157182. doi: 10.1371/journal.pone.0157182
49. Lau C, Stevens D, Jia J. Effects of an occupation-based obesity prevention program for children at risk. Occup Ther Health Care. (2013) 27(2):163–75. doi: 10.3109/07380577.2013.783725
50. Lubans DR, Smith JJ, Plotnikoff RC, Dally KA, Okely AD, Salmon J, et al. Assessing the sustained impact of a school-based obesity prevention program for adolescent boys: the ATLAS cluster randomized controlled trial. Int J Behav Nutr Phys Act. (2016) 13:92. doi: 10.1186/s12966-016-0420-8
51. Madsen KA, Cotterman C, Crawford P, Stevelos J, Archibald A. Effect of the healthy schools program on prevalence of overweight and obesity in California schools, 2006-2012. Prev Chronic Dis. (2015) 12:E77. doi: 10.5888/pcd12.150020
52. Messiah SE, Diego A, Kardys J, Kirwin K, Hanson E, Nottage R, et al. Effect of a park-based after-school program on participant obesity-related health outcomes. Am J Health Promot. (2015) 29(4):217–25. doi: 10.4278/ajhp.120705-QUAN-327
53. Parra-Medina D, Liang Y, Yin Z, Esparza L, Lopez L. Weight outcomes of Latino adults and children participating in the Y living program, a family-focused lifestyle intervention, San Antonio, 2012-2013. Prev Chronic Dis. (2015) 12:E219. doi: 10.5888/pcd12.150219
54. Safdie M, Jennings-Aburto N, Levesque L, Janssen I, Campirano-Nunez F, Lopez-Olmedo N, et al. Impact of a school-based intervention program on obesity risk factors in Mexican children. Salud Publica Mex. (2013) 55(Suppl 3):374–87. https://www.scielosp.org/pdf/spm/v55s3/v55s3a4.pdf24643486
55. Siegrist M, Lammel C, Haller B, Christle J, Halle M. Effects of a physical education program on physical activity, fitness, and health in children: the JuvenTUM project. Scand J Med Sci Sports. (2013) 23(3):323–30. doi: 10.1111/j.1600-0838.2011.01387.x
56. Sigmund E, Sigmundova D. Longitudinal 2-year follow-up on the effect of a non-randomised school-based physical activity intervention on reducing overweight and obesity of Czech children aged 10-12 years. Int J Environ Res Public Health. (2013) 10(8):3667–83. doi: 10.3390/ijerph10083667
57. Smith JJ, Morgan PJ, Plotnikoff RC, Dally KA, Salmon J, Okely AD, et al. Smart-phone obesity prevention trial for adolescent boys in low-income communities: the ATLAS RCT. Pediatrics. (2014) 134(3):e723–31. doi: 10.1542/peds.2014-1012
58. Vander Ploeg KA, McGavock J, Maximova K, Veugelers PJ. School-based health promotion and physical activity during and after school hours. Pediatrics. (2014) 133(2):e371–8. doi: 10.1542/peds.2013-2383
59. Wang JJ, Lau WC, Wang HJ, Ma J. Evaluation of a comprehensive intervention with a behavioural modification strategy for childhood obesity prevention: a nonrandomized cluster controlled trial. BMC Public Health. (2015) 15:1206. doi: 10.1186/s12889-015-2535-2
60. Watson PM, Dugdill L, Pickering K, Owen S, Hargreaves J, Staniford LJ, et al. Service evaluation of the GOALS family-based childhood obesity treatment intervention during the first 3 years of implementation. BMJ Open. (2015) 5(2):e006519. doi: 10.1136/bmjopen-2014-006519
61. Tarro L, Llaurado E, Albaladejo R, Morina D, Arija V, Sola R, et al. A primary-school-based study to reduce the prevalence of childhood obesity—the EdAl (Educacio en Alimentacio) study: a randomized controlled trial. Trials. (2014) 15:58. doi: 10.1186/1745-6215-15-58
62. Tarro L, Llauradó E, Moriña D, Solà R, Giralt M. Follow-up of a healthy lifestyle education program (the Educació en Alimentació Study): 2 years after cessation of intervention. J Adolesc Health. (2014) 55(6):782–9. doi: 10.1016/j.jadohealth.2014.06.020
63. Brennan L, Walkley J, Wilks R, Fraser SF, Greenway K. Physiological and behavioural outcomes of a randomised controlled trial of a cognitive behavioural lifestyle intervention for overweight and obese adolescents. Obes Res Clin Pract. (2013) 7(1):e23–41. doi: 10.1016/j.orcp.2012.02.010
64. Davis AM, Sampilo M, Gallagher KS, Landrum Y, Malone B. Treating rural pediatric obesity through telemedicine: outcomes from a small randomized controlled trial. J Pediatr Psychol. (2013) 38(9):932–43. doi: 10.1093/jpepsy/jst005
65. Altman M, Cahill Holland J, Lundeen D, Kolko RP, Stein RI, Saelens BE, et al. Reduction in food away from home is associated with improved child relative weight and body composition outcomes and this relation is mediated by changes in diet quality. J Acad Nutr Diet. (2015) 115(9):1400–7. doi: 10.1016/j.jand.2015.03.009
66. Arauz Boudreau AD, Kurowski DS, Gonzalez WI, Dimond MA, Oreskovic NM. Latino families, primary care, and childhood obesity: a randomized controlled trial. Am J Prev Med. (2013) 44(Suppl 3):S247–57. doi: 10.1016/j.amepre.2012.11.026
67. Boodai SA, McColl JH, Reilly JJ. National adolescent treatment trial for obesity in Kuwait (NATTO): project design and results of a randomised controlled trial of a good practice approach to treatment of adolescent obesity in Kuwait. Trials. (2014) 15:234. doi: 10.1186/1745-6215-15-234
68. Endevelt R, Elkayam O, Cohen R, Peled R, Tal-Pony L, Michaelis Grunwald R, et al. An intensive family intervention clinic for reducing childhood obesity. J Am Board Fam Med. (2014) 27(3):321–8. doi: 10.3122/jabfm.2014.03.130243
69. Gerards SM, Dagnelie PC, Gubbels JS, van Buuren S, Hamers FJ, Jansen MW, et al. The effectiveness of lifestyle triple P in the Netherlands: a randomized controlled trial. PLoS One. (2015) 10(4):e0122240. doi: 10.1371/journal.pone.0122240
70. Luca P, Dettmer E, Khoury M, Grewal P, Manlhiot C, McCrindle BW, et al. Adolescents with severe obesity: outcomes of participation in an intensive obesity management programme. Pediatr Obes. (2015) 10(4):275–82. doi: 10.1111/ijpo.261
71. Marild S, Gronowitz E, Forsell C, Dahlgren J, Friberg P. A controlled study of lifestyle treatment in primary care for children with obesity. Pediatr Obes. (2013) 8(3):207–17. doi: 10.1111/j.2047-6310.2012.00105.x
72. Martín-García M, Alegre Durán LM, García-Cuartero B, Bryant EJ, Gutin B, Royo IA. Effects of a 3-month vigorous physical activity intervention on eating behaviors and body composition in overweight and obese boys and girls. J Sport Health Sci. (2019) 8(2):170–6. doi: 10.1016/j.jshs.2017.09.012
73. Nemet D, Ben-Haim I, Pantanowits M, Eliakim A. Effects of a combined intervention for treating severely obese prepubertal children. J Pediatr Endocrinol Metab. (2013) 26(1–2):91–6. doi: 10.1515/jpem-2012-0225
74. Nemet D, Oren S, Pantanowitz M, Eliakim A. Effects of a multidisciplinary childhood obesity treatment intervention on adipocytokines, inflammatory and growth mediators. Horm Res Paediatr. (2013) 79(6):325–32. doi: 10.1159/000348732
75. Rank M, Wilks DC, Foley L, Jiang Y, Langhof H, Siegrist M, et al. Health-related quality of life and physical activity in children and adolescents 2 years after an inpatient weight-loss program. J Pediatr. (2014) 165(4):732–7.e2. doi: 10.1016/j.jpeds.2014.05.045
76. Serra-Paya N, Ensenyat A, Castro-Vinuales I, Real J, Sinfreu-Bergues X, Zapata A, et al. Effectiveness of a multi-component intervention for overweight and obese children (Nereu Program): a randomized controlled trial. PLoS One. (2015) 10(12):e0144502. doi: 10.1371/journal.pone.0144502
77. Siwik V, Kutob R, Ritenbaugh C, Cruz L, Senf J, Aickin M, et al. Intervention in overweight children improves body mass index (BMI) and physical activity. J Am Board Fam Med. (2013) 26(2):126–37. doi: 10.3122/jabfm.2013.02.120118
78. Staiano AE, Beyl RA, Hsia DS, Katzmarzyk PT, Newton RL Jr. Twelve weeks of dance exergaming in overweight and obese adolescent girls: transfer effects on physical activity, screen time, and self-efficacy. J Sport Health Sci. 2017;6(1):4–10. doi: 10.1016/j.jshs.2016.11.005
79. Staiano AE, Marker AM, Beyl RA, Hsia DS, Katzmarzyk PT, Newton RL. A randomized controlled trial of dance exergaming for exercise training in overweight and obese adolescent girls. Pediatr Obes. (2017) 12(2):120–8. doi: 10.1111/ijpo.12117
80. Taveras EM, Marshall R, Kleinman KP, Gillman MW, Hacker K, Horan CM, et al. Comparative effectiveness of childhood obesity interventions in pediatric primary care: a cluster-randomized clinical trial. JAMA Pediatr. (2015) 169(6):535–42. doi: 10.1001/jamapediatrics.2015.0182
81. Rito AI, Carvalho MA, Ramos C, Breda J. Program obesity zero (POZ)—a community-based intervention to address overweight primary-school children from five Portuguese municipalities. Public Health Nutr. (2013) 16(6):1043–51. doi: 10.1017/S1368980013000244
82. Maatoug J, Fredj SB, Msakni Z, Dendana E, Sahli J, Harrabi I, et al. Challenges and results of a school-based intervention to manage excess weight among school children in Tunisia 2012-2014. Int J Adolesc Med Health. (2017) 29(2). doi: 10.1515/ijamh-2015-0035
83. Morano M, Rutigliano I, Rago A, Pettoello-Mantovani M, Campanozzi A. A multicomponent, school-initiated obesity intervention to promote healthy lifestyles in children. Nutrition. (2016) 32(10):1075–80. doi: 10.1016/j.nut.2016.03.007
84. Sanders K, Barield JP, Hodge K, Phillips I, Pino A. Effects of the get youth moving (GYM) intervention on health-related fitness and behaviors. J Park Recreat Admi. (2014) 32(3):106–17. https://www.researchgate.net/profile/Jp-Barfield/publication/328611178_Effect_of_the_Get_Youth_Moving_intervention_on_health_related_fitness_and_behaviors/links/618039c30be8ec17a9597f18/Effect-of-the-Get-Youth-Moving-intervention-on-health-related-fitness-and-behaviors.pdf
85. Kokkvoll A, Grimsgaard S, Steinsbekk S, Flaegstad T, Njolstad I. Health in overweight children: 2-year follow-up of Finnmark Activity School—a randomised trial. Arch Dis Child. (2015) 100(5):441–8. doi: 10.1136/archdischild-2014-307107
86. Rieder J, Khan UI, Heo M, Mossavar-Rahmani Y, Blank AE, Strauss T, et al. Evaluation of a community-based weight management program for predominantly severely obese, difficult-to-reach, inner-city minority adolescents. Childhood Obesity. (2013) 9(4):292–304. doi: 10.1089/chi.2012.0147
87. Morgan PJ, Collins CE, Plotnikoff RC, Callister R, Burrows T, Fletcher R, et al. The ‘healthy dads, healthy kids’ community randomized controlled trial: a community-based healthy lifestyle program for fathers and their children. Prev Med. (2014) 61:90–9. doi: 10.1016/j.ypmed.2013.12.019
Appendix A Keywords and meshterms
.
Appendix B Equations of research
.
Keywords: obesity, youth, clinical, school, intervention strategies, prevention
Citation: Caron T, Bernard P and Gadais T (2023) Clinical and school-based intervention strategies for youth obesity prevention: A systematic review. Front. Sports Act. Living 4:906857. doi: 10.3389/fspor.2022.906857
Received: 29 March 2022; Accepted: 31 December 2022;
Published: 27 February 2023.
Edited by:
Åsa B. Tornberg, Lund University, SwedenReviewed by:
Giovanni Messina, University of Foggia, ItalyMasoud Mohammadnezhad, School of Nursing and Healthcare Leadership, United Kingdom
© 2023 Caron, Bernard and Gadais. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tegwen Gadais Z2FkYWlzLnRlZ3dlbkB1cWFtLmNh
Specialty Section: This article was submitted to Exercise Physiology, a section of the journal Frontiers in Sports and Active Living