
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Sports Act. Living, 01 August 2022
Sec. Movement Science
Volume 4 - 2022 | https://doi.org/10.3389/fspor.2022.903777
This article is part of the Research TopicPsychological and Behavioral Determinants of Physical Activity Participation Across the Lifespan Volume IIView all 6 articles
 Björn Gunnarsson1
Björn Gunnarsson1 Artin Entezarjou2,3
Artin Entezarjou2,3 Fernando Fernández-Aranda4,5,6,7
Fernando Fernández-Aranda4,5,6,7 Susana Jiménez-Murcia4,5,6,7
Susana Jiménez-Murcia4,5,6,7 Göran Kenttä8,9,10
Göran Kenttä8,9,10 Anders Håkansson11,12*
Anders Håkansson11,12*Background: The purpose of this paper was to explore maladaptive behaviors among physically active individuals, including exercise dependence and use of anabolic steroids. Both exercise addiction (EA) and use of anabolic androgenic steroids (AAS) correlate to high amounts of exercise and EA have been linked to eating disorders and other mental health problems.
Methods: An internet survey was spread through fitness-related social media. Inclusion criteria were age ≥ 15 years and exercise frequency ≥ thrice weekly. Exercise addiction inventory identified those at-risk of EA (rEA). Characteristics of rEA were compared to those not at risk. In a separate analysis, AAS users were compared to AAS-naïve individuals.
Results: In total, 3,029 participants completed the questionnaire. Of these, 11% screened positive for being rEA, and 23% for ED. Factors associated with EA included daily exercise, social phobia, eating disorders and OCD. Risk consumption of alcohol was a negative predictor. Thirty seven participants had taken AAS the last year. These were mainly men, bodybuilders/powerlifters and more often used amphetamines and opioids.
Discussion: This exploratory study supports EA being strongly associated with eating disorders. Identified associations between EA and compulsive or anxiety disorders warrant further research to clarify if these associations arise prior to, together with, or secondary to EA.
Exercise has shown many positive effects (Bouchard et al., 1994; McAuley and Rudolph, 1995), including cardiovascular benefits (Zimmer and Bloch, 2015; Wewege et al., 2018) and efficacy in treatment of several mental health disorders (Zschucke et al., 2013; Gordon et al., 2018). However, already in the 1970s negative effects from compulsive exercise were examined, whereas exercise addiction (EA) was first clearly described in a case study by Griffiths (Griffiths, 2009). It is suggested that EA is based on six criteria; salience, mood modification, tolerance, withdrawal, conflicts and relapse. It is described as a condition where the exercising individual is acting in a compulsive manner and exhibits dependence which leads to maladaptive effects for the individual – both socially and mentally (Griffiths et al., 2005).
The prevalence of EA in the general population is still disputed, with inconsistent findings in research. There appears to be a sport-specific variation in prevalence, with endurance sports ranging from 2.7 to 20% (Hausenblas and Downs, 2002; Youngman and Simpson, 2014; Zeulner et al., 2016; Mayolas-Pi et al., 2017). In more typical fitness populations symptoms of EA have been reported in the range of 6.8 to 10.2% (Lichtenstein et al., 2017; Rudolph, 2017). Moreover, sports such as CrossFit (5.0%) (Lichtenstein and Jensen, 2016) and soccer (7.1%) (Lichtenstein et al., 2014) have also been examined. Importantly, existing studies on exercising populations must critically discuss the ability to estimate the prevalence of EA in the general population, given that 31% of the world population does not meet the physical activity recommendations (Kohl et al., 2012). One study has, however, suggested an EA-prevalence of 3.6% in the “general exercising population” (Szabo and Griffiths, 2007). When looking at a general population in Hungary, it was found that between 0.3–0.5% of the general population were at risk of EA (Mónok et al., 2012).
EA has been linked to several other psychiatric diagnoses. It is believed that eating disorders (ED) such as anorexia nervosa or bulimia nervosa could lead to secondary EA in the form of compulsive exercise (Veale, 1987; Dalle Grave et al., 2008; Zeulner et al., 2016; Levallius et al., 2017). In these cases, ED should be treated together with EA, rather than separately, as the ED is most likely the major concern and the secondary EA is a sign of more severe ED (Strober et al., 1997; Solenberger, 2001; Dalle Grave et al., 2008; Levallius et al., 2017; Young et al., 2018). Combined ED and EA has previously been studied (Veale, 1987; Strober et al., 1997; Solenberger, 2001; Dalle Grave et al., 2008; Zeulner et al., 2016; Rudolph, 2017; Young et al., 2018) and there is an obvious correlation, although it is unclear whether EA always is secondary to ED. Muscle dysmorphia (MD), an assumingly underdiagnosed and more common disease, could potentially show signs of ED but is rather secondary to the exercise (Phillips et al., 2010; Giardino and Procidano, 2012; Tod et al., 2016; Klimek et al., 2018). Previous studies show that among weightlifters, 13–44% have a lifetime prevalence of MD (dos Santos Filho et al., 2015) and they rarely identify with the disorder (Olivardia, 2001).
Other addictive behaviors, such as the use of anabolic androgenic steroids (AAS) are also more common among recreational athletes than the general population (Parkinson and Evans, 2006) and associated with higher exercise frequency and training load (Ip et al., 2011). However, these performance-enhancing drugs have negative consequences, such as higher risk of tendon injury (Kanayama et al., 2015; Lindqvist Bagge et al., 2017), depression (Pope and Katz, 1994; Kicman and Gower, 2003; Ip et al., 2012; Lindqvist Bagge et al., 2017) and anxiety (Ip et al., 2011, 2012; Lindqvist Bagge et al., 2017), all with a dose-response-dependent increase in risk (Lindqvist Bagge et al., 2017). Liver dysfunction is common when AAS is orally administered (Kicman and Gower, 2003). Prolonged use is believed to be associated with risk of cardiovascular events (Sullivan et al., 1998; Pärssinen et al., 2000; Kicman and Gower, 2003; Hartgens et al., 2004; Bonetti et al., 2008; Baggish et al., 2017; Rasmussen et al., 2018), hypogonadism and infertility (Bonetti et al., 2008; Christou et al., 2017). It is however disputed whether these effects are reversible (Kicman and Gower, 2003; Christou et al., 2017; Rasmussen et al., 2018), but the psychiatric consequences are evident (Pärssinen et al., 2000; Ip et al., 2011, 2012; Piacentino et al., 2015).
Historically, only substance-related disorders have been recognized as addictive disorders by the international diagnostic systems (DSM-5, ICD-10). However, since DSM-5, the first non-substance use disorder is recognized as an addictive disorder – gambling addiction (Grant and Chamberlain, 2016). This calls for further investigation on behavioral addictions, such as EA, to possibly determine and recognize other behavioral addictions as mental disorders. The main purpose of this study is to examine EA and AAS-use among regular exercisers by using a cross-sectional survey with a large cohort. More specifically, it will be examined whether EA co-occurs with other addictive or obsessive conditions or not by comparing the characteristics of those at-risk of EA compared to other regular exercisers who are not at risk of EA. As a secondary aim, the prevalence and characteristics of active AAS users are compared to AAS-naïve regular exercisers.
This study was conducted with ethical approval from the regional ethics board, Lund, Sweden (file number 2017/822).
The survey addressed individuals in the general population but addressed those responding that they exercised regularly, at least three times weekly, and who were above the age of 15, and the survey opened only if the individual provided informed consent. Participants were recruited from April 1 through April 10, 2018, by spreading the survey through social media pages of several major Swedish health- and exercise-related blogs. Data was collected anonymously by Patient Information Broker (PIB) and I-Mind, Sweden.
The survey consisted of several screening tools and questions were translated into Swedish. The exercise addiction inventory (EAI) is a six-question based screening tool for EA where the participant chooses from 1–5 on a Likert scale where 1 = “strongly disagree”, 5 = “strongly agree” (total scores between 6 and 30). This tool was chosen as it is not sport-specific, and easy to use. The cut-off level used for the screening of being at-risk if EA has been reported to be a score of 24 and above (at-risk of EA) (Griffiths et al., 2005).
The SCOFF (Sick, Control, One stone, Fat, Food) was used for the screening for ED, and consists of five yes-or-no questions screening for ED. Two or more affirmative answers indicate a likely ED. The test has both a high specificity and sensitivity (Morgan et al., 1999).
The AUDIT alcohol consumption questions (AUDIT-C) is a short 3-question screening version of the Alcohol Use Disorders Identification Test (AUDIT) and only focuses on consumption. Two items result in 0–4 points per question (total score between 0 and 12). Women with three or more points, or men with four or more points, are considered to have a hazardous use of alcohol (Bush et al., 1998).
Besides the screening tools listed above, the survey contained questions multiple choice-questions about exercise type (body-builder, runner, other endurance training, other) and exercise frequency (days per week, 3–7). Yes/no questions regarding a variety of psychiatric disorders, smoker status and past-year use of illicit drugs or AAS were given with the third option “would not like to respond”. Two questions were used to screen for problematic gambling, this was used for a separate study regarding problematic gambling among athletes. Demographic information included questions about gender (male/female/transgender) and age (categorized into age categories: 15–18, 19–24, 25–29, 30–39, 40–49, 50–59, and 60+ years). A categorical age distribution was chosen in order to facilitate the reporting by subjects on an online screen format, and age categories choses were the same as used in previous online surveys distributed through the same instrument (for example by Broman and co-workers in 2018 (Broman and Håkansson, 2018).
The participants accessed the study survey online through a link on social media. Before starting the questionnaire, the participants had to read the terms and consent to them. After the survey was finished, participants were given the results regarding EAI and if they felt they had a problematic relationship to exercise they were encouraged to contact a health professional.
IBM SPSS 24.0.0.1 was used to analyse all data.
Participants were divided into two groups based on EAI score: those not at risk of EA (score of 6–23) and at-risk of EA (scores >23). The characteristics of these groups were then compared with each other using the Pearson chi-square test. Factors significantly associated with being at risk of EA (p < 0.05) were forwarded to a binary logistic egression analysis. Due to the relatively elevated number of factors controlled for, a conservative cut-off was set for significant levels in the logistic regression analysis, applying a Bonferroni correction.
Those who answered they had used AAS were separated and compared to those who reported being AAS-naïve using Fisher's exact test (due to the lower number of respondents endorsing this problem behavior). Due to the limited sample size in this analysis, only factors with p < 0.001 were inserted in a regression analysis, and a Bonferroni correction was applied in the interpretation of the logistic regression.
In Table 1, the characteristics of all participants are shown. Out of the 3,419 who started the survey, 3,029 (89%) completed all the questions. The majority of participants were between 25–39 years of age (54.4%), of male gender (63.8%), working (80.4%) and reported that their primary type of exercise was bodybuilding/powerlifting (58.7%). The mean EAI-score was 18.06 (SD ± 4.347). Among participants, 344 (11.0%) had an EAI-score >23 and qualified as at-risk. Table 1 displays the binary comparisons made between subjects being at-risk of EA compared to subjects not at risk of EA. After moving variables with significant associations to a binary logistic regression analysis, Table 2 shows the results of the regression analysis of potential correlates of being at risk of EA. The significant risk-factors were daily exercise and a high SCOFF-score. None of the substance use variables were related to being at risk of EA after the Bonferroni correction, although a high consumption of alcohol was negatively associated with being at-risk of EA in the uncorrected analysis. Having felt a need for psychiatric treatment, and being diagnosed with an eating disorder, social phobia, or OCD, were associated with being at risk of EA in the uncorrected analysis, but lost their significant associations after the Bonferroni correction.
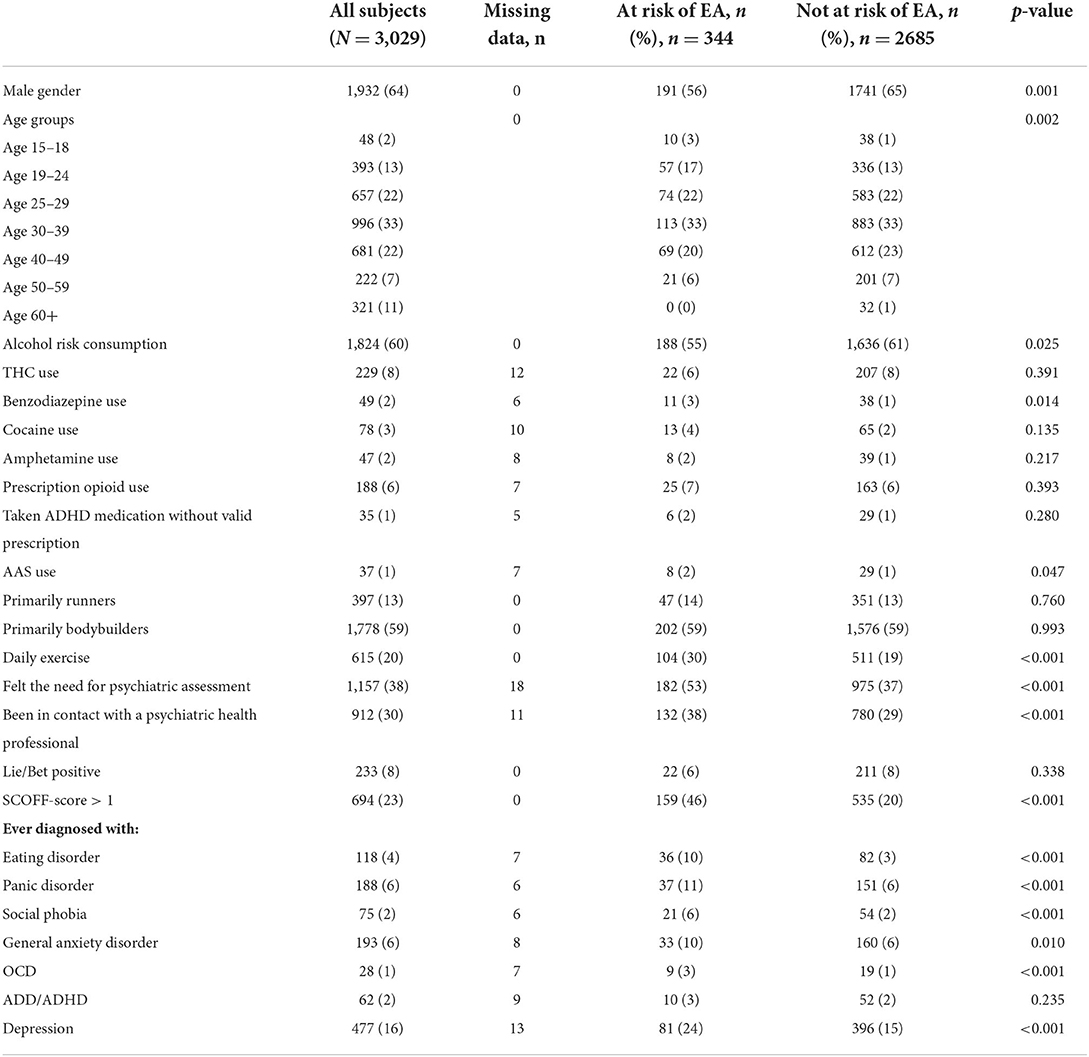
Table 1. Descriptive characteristics of 3,029 athletes who exercise more than three times a week comparing those at risk of exercise addiction (EA) to those not at risk based on the exercise addiction inventory >23.
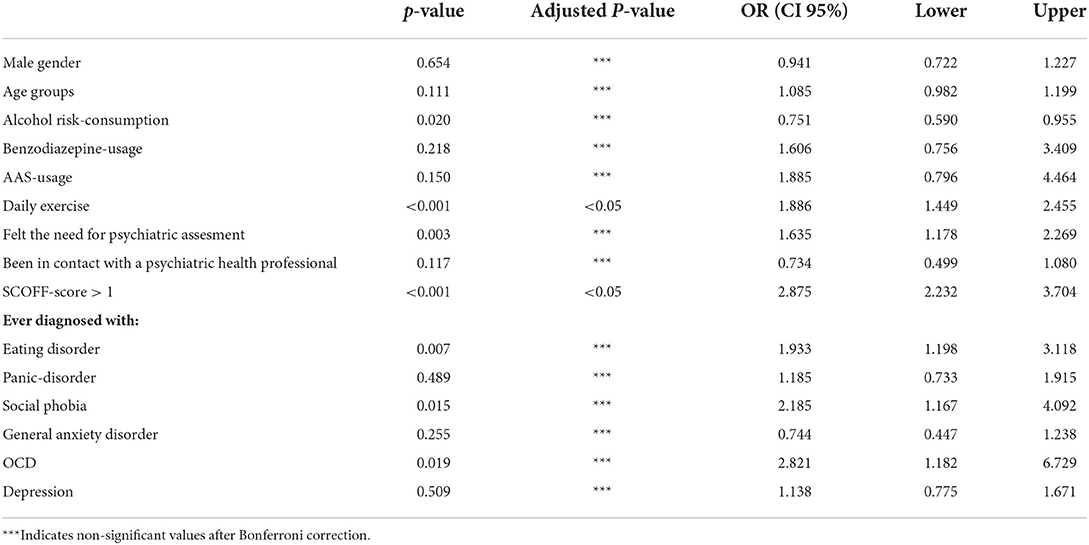
Table 2. Binary logistic regression of factors significantly associated with being at-risk of exercise addiction compared to participants not at risk of exercise addiction.
Out of the 3,029 participants, 37 responded they had been taking AAS the past year and seven chose not to respond. In Table 3 the characteristics of those using AAS are shown, compared to those who responded as AAS-naïve, the seven non-responders excluded. Table 4 displays the results of a regression analysis of the factors with a p-value < 0.001, showing a substantial correlation to bodybuilding and male gender as well as a positive correlation to taking prescription opioids and amphetamine, but not other substances.
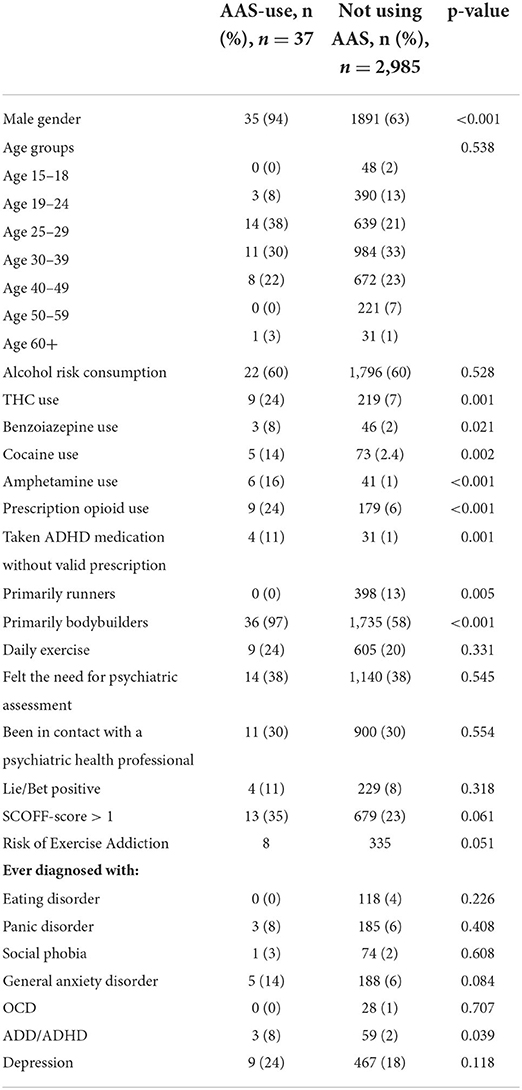
Table 3. Descriptive characteristics of 3,022 athletes who exercise more than three times a week comparing those who reported using anabolic androgenic steroids (AAS-use) to those reporting not using anabolic androgenic steroids the last year, p-value after using Fisher's exact test.
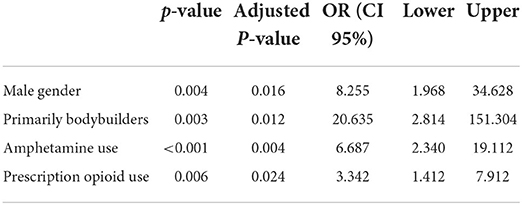
Table 4. Binary logistic regression of factors associated with having used anabolic androgenic steroids the last year compared to participants reporting not using anabolic androgenic steroids the last year.
There were 118 participants who reported being diagnosed with ED; their mean EAI-score was 21.36 (SD ± 4.404). Of those at risk of EA there were 36 (10.7%) diagnosed with an ED, 33 female and 3 males. A post-hoc analysis of those who said bodybuilding/powerlifting was their primary form of exercise showed a significantly increased risk of having a SCOFF-score>1 (p < 0.005), compared to those who said they primarily participated in running, endurance sports or other sports.
The main result of this study is that 11% of a physically active self-selected population are at-risk of EA. In the same group, AAS use was primarily used by bodybuilders/powerlifters. A prevalence of 11% at-risk of EA is quite high, but still within the estimates of previous studies (Hausenblas and Downs, 2002; Lichtenstein et al., 2014, 2017; Youngman and Simpson, 2014; Lichtenstein and Jensen, 2016; Zeulner et al., 2016; Mayolas-Pi et al., 2017; Rudolph, 2017). What might have influenced, giving the somewhat higher prevalence could be the fact that this study used a minimum of exercising days as inclusion, especially since daily exercise was associated to EA and increasing amount of exercise has previously been shown to be associated with EA (Lichtenstein and Jensen, 2016; Lichtenstein et al., 2017; Rocks et al., 2017). Even though this study did not specify the amount in hours like previous studies, the same correlation can be seen in amount of days exercised. It can, however, not be excluded that some individuals exercised more than once on exercise days.
In our results, no correlation could be found between at-risk of EA and depression, while a Danish study found that not only did those at-risk of EA more frequently show symptoms of depression compared to the general population, but also that the risk of depression was significantly increased in case of injury (Lichtenstein et al., 2018). This explorative study specifically asked for diagnosed mental disorders, while the Danish one used the self-report questionnaire HADS. It is believed that many use exercise as a form of relief of emotional distress (i.e., reducing anxiety), and might not have contacted any medical expertise. Thus, it is possible that undiagnosed depression is more prevalent even in our study population. Exercise withdrawal has shown to lead to mood-disturbances among regular exercisers (Chan and Grossman, 1988; Szabo, 1995; Mondin et al., 1996), and in case of a dependence the risk of suffering from psychological distress could be worse. Moreover, the finding that those at-risk of EA felt the need to seek out a mental health professional – but did not – could be argued to further support this notion.
Among the mental disorders asked for, social phobia and OCD had equally strong correlation as ED to EA. A previous study found that anxiety of body appearance often was associated to EA (Cook et al., 2015), but to the authors knowledge, social anxiety disorder is a variable never studied before, and should be further investigated. OCD and ED, being compulsive disorders which correlate to EA, could open for a discussion about whether EA might rather be characterized as a compulsive disorder rather than an addictive disorder.
In this study population 23% had a positive SCOFF-test, which is relatively high, but in agreement with previous studies among athletes. Up to 45% of female and up to 19% of male athletes showed symptoms of ED (Bratland-Sanda and Sundgot-Borgen, 2013), whilst among the general population the lifetime prevalence is 1% (Jie et al., 2013). Because of the difficulty to differentiate between secondary EA and ED due to exercise, this study only focused on EA rather than dividing them into separate groups. However, the majority of participants were bodybuilders/powerlifters, a group more susceptible to MD (Phillips et al., 2010; Skemp et al., 2013) which has been shown to involve restricted eating (Murray et al., 2010; Giardino and Procidano, 2012; Devrim et al., 2018). Both MD and ED are associated with EA (Giardino and Procidano, 2012), and it is clear in the results that this group should be further investigated regarding ED as only 36 were diagnosed, whilst 164 had a SCOFF-score > 1 without diagnosis.
Previous data in both animal and human studies has suggested exercise to reduce drug seeking behavior on a neurological level (Robertson et al., 2016; Robison et al., 2018). In our sample a negative correlation between high alcohol consumption and being at-risk of EA was found, which could further support this claim. Participants taking AAS were however more frequently using other substances, which is in agreement with previous studies (Ip et al., 2011, 2012; Kersey et al., 2012; Mhillaj et al., 2015; McDuff et al., 2019) and it has been shown that the effects of stimulants is decreased and the drug-seeking behavior in general is increased (Mhillaj et al., 2015). This group of individuals should most likely be examined selectively because of the comorbidity they may develop based on the AAS-use alone.
This study has several limitations. Firstly, the self-report of diagnoses referred to a history of receiving an actual diagnosis, which requires the participant to have sought medical attention, compared to using self-report questionnaires where even undiagnosed disorders can be found. This could influence the results of mental disorders in this study. Being a retrospective survey, nothing can be said about the causality, only the correlation can be examined.
In conclusion, looking at the results from this study, many respondents at-risk of EA also had one or more psychiatric diagnoses. A causality could not be determined in this study, but the risk of depression in case of withdrawal is known since before (Lichtenstein et al., 2018). Screening and assessing those with EA for other mental illnesses could enable treatment and help them achieve a healthier relationship to exercise, and the risk of adverse reactions in case of withdrawal should lessen. Those using AAS should be separately investigated, as their use of other substances makes it more complex and they are probably in need of different assessments than those at-risk of EA. Being at-risk of EA is particularly strongly associated with being at-risk of ED, while associations to compulsive or anxiety components warrants further prospective research to clarify if these associations arise prior to, together with, or secondary to EA.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Regionala etikprövningsnämnden Lund/Regional Ethics Board Lund, Sweden. Written informed consent from the participants' legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
BG, AE, FF-A, SJ-M, and AH planned the study. AH was responsible of the ethics application. AH, BG, and AE were part of the data collection procedure. BG conducted the statistical analyses, wrote the draft of the paper, and which was edited by all authors. GK added interpretations regarding sports psychology. FF-A and SJ-M added interpretations of clinical behavioral addiction aspects. Results were discussed by all authors. All authors contributed to the article and approved the submitted version.
The study was finance using the general research funding of AH, from the regional health care organization and from the state-owned gambling operator AB Svenska Spel.
We would like to thank Jacob Gudiol of Träningslära, Daniel Richter of Styrkelabbet, and the team at EBT (Evidence Based Training) for aiding in the distribution of the online questionnaire. We also would like to thank Userneeds, Patient Information Broker, and I-Minds for the data collection.
Author AH has overall research funding from the state-owned gambling operator Svenska Spel, which however was not involved in the present study, which did not received any project-specific funding. Authors FF-A and SJ-M received consultancy honoraria from Novo Nordisk and editorial honoraria as EIC from Wiley (FF-A), which had no role in the study.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Baggish, A. L., Weiner, R. B., Kanayama, G., Hudson, J. I., Lu, M. T., Hoffmann, U., et al. (2017). Cardiovascular toxicity of illicit anabolic-androgenic steroid use. Circulation 135, 1991–2002. doi: 10.1161/CIRCULATIONAHA.116.026945
Bonetti, A., Tirelli, F., Catapano, A., Dazzi, D., Dei Cas, A., Solito, F., et al. (2008). Side effects of anabolic androgenic steroids abuse. Int. J. Sports Med. 29, 679–687. doi: 10.1055/s-2007-965808
Bouchard, C. E., Shephard, R. J., and Stephens, T. E. (1994). “Physical activity, fitness, and health: International proceedings and consensus statement,” in International Consensus Symposium on Physical, Activity, Fitness, and Health, 2nd, May, 1992 (Toronto, ON, Canada: Human Kinetics Publishers).
Bratland-Sanda, S., and Sundgot-Borgen, J. (2013). Eating disorders in athletes: overview of prevalence, risk factors and recommendations for prevention and treatment. Eur. J. Sport Sci. 13, 499–508. doi: 10.1080/17461391.2012.740504
Broman, N., and Håkansson, A. (2018). Problematic gaming and internet use but not gambling may be overrepresented in sexual minorities - a pilot population web survey study. Front. Psychol. 9, 2184. doi: 10.3389/fpsyg.2018.02184
Bush, K., Kivlahan, D. R., McDonell, M. B., Fihn, S. D., Bradley, K. A., and For the Ambulatory Care Quality Improvement P. (1998). The audit alcohol consumption questions (audit-c): an effective brief screening test for problem drinking. Arch. Int. Med. 158, 1789–1795. doi: 10.1001/archinte.158.16.1789
Chan, C. S., and Grossman, H. Y. (1988). Psychological effects of running loss on consistent runners. Percept. Mot. Skills. 66, 875–883. doi: 10.2466/pms.1988.66.3.875
Christou, M. A., Christou, P. A., Markozannes, G., Tsatsoulis, A., Mastorakos, G., Tigas, S., et al. (2017). Effects of anabolic androgenic steroids on the reproductive system of athletes and recreational users: a systematic review and meta-analysis. Sports Med. 47, 1869–1883. doi: 10.1007/s40279-017-0709-z
Cook, B., Karr, T. M., Zunker, C., Mitchell, J. E., Thompson, R., Sherman, R., et al. (2015). The influence of exercise identity and social physique anxiety on exercise dependence. J. Behav. Addict. 4, 195–199. doi: 10.1556/2006.4.2015.020
Dalle Grave, R., Calugi, S., and Marchesini, G. (2008). Compulsive exercise to control shape or weight in eating disorders: prevalence, associated features, and treatment outcome. Compr. Psychiatry. 49, 346–352. doi: 10.1016/j.comppsych.2007.12.007
Devrim, A., Bilgic, P., and Hongu, N. (2018). Is there any relationship between body image perception, eating disorders, and muscle dysmorphic disorders in male bodybuilders? Am. J. Men's Health 12, 1746–1758. doi: 10.1177/1557988318786868
dos Santos Filho, C. A., Tirico, P. P., Stefano, S. C., Touyz, S. W., and Claudino, A. M. (2015). Systematic review of the diagnostic category muscle dysmorphia. Aust. New Zealand J. Psychiatry 50, 322–333. doi: 10.1177/0004867415614106
Giardino, J. C., and Procidano, M. E. (2012). Muscle dysmorphia symptomatology: a cross-cultural study in Mexico and the United States. Int. J. Men's Health 11, 83–103. doi: 10.3149/jmh.1101.83
Gordon, B. R., McDowell, C. P., Hallgren, M., Meyer, J. D., Lyons, M., Herring, M. P., et al. (2018). Association of efficacy of resistance exercise training with depressive symptoms: meta-analysis and meta-regression analysis of randomized clinical trials. JAMA Psychiat. 75, 566–576. doi: 10.1001/jamapsychiatry.2018.0572
Grant, J. E., and Chamberlain, S. R. (2016). Expanding the definition of addiction: DSM-5 vs. ICD-11. CNS Spectr. 21, 300–303. doi: 10.1017/S1092852916000183
Griffiths, M. (2009). Exercise addiction: a case study. Addict. Res. 5, 161–8. doi: 10.3109/16066359709005257
Griffiths, M. D., Szabo, A., and Terry, A. (2005). The exercise addiction inventory: a quick and easy screening tool for health practitioners. Br. J. Sport Med. 39, e30. doi: 10.1136/bjsm.2004.017020
Hartgens, F., Rietjens, G., Keizer, H. A., Kuipers, H., and Wolffenbuttel, B. H. (2004). Effects of androgenic-anabolic steroids on apolipoproteins and lipoprotein (a). Br. J. Sports Med. 38, 253–259. doi: 10.1136/bjsm.2003.000199
Hausenblas, H. A., and Downs, D. S. (2002). How much is too much? The development and validation of the exercise dependence scale. Psychol Health 17, 387–404. doi: 10.1080/0887044022000004894
Ip, E. J., Barnett, M. J., Tenerowicz, M. J., and Perry, P. J. (2011). The anabolic 500 survey: characteristics of male users versus nonusers of anabolic-androgenic steroids for strength training. Pharmacotherapy J. Hum. Pharmacol. Drug Therapy. 31, 757–766. doi: 10.1592/phco.31.8.757
Ip, E. J., Lu, D. H., Barnett, M. J., Tenerowicz, M. J., Vo, J. C., Perry, P. J., et al. (2012). Psychological and physical impact of anabolic-androgenic steroid dependence. Pharmacotherapy J. Hum. Pharmacol. Drug Therapy. 32, 910–919. doi: 10.1002/j.1875-9114.2012.01123
Jie, Q., Qiang, H. U., Yumei, W. A. N., Ting, L. I., Mudan, W. U., Zhiqun, R. E. N., et al. (2013). Prevalence of eating disorders in the general population: a systematic review. Shanghai Arch. Psychiatry. 25, 212–223.
Kanayama, G., DeLuca, J., Meehan, W. P. 3rd, Hudson, J. I., Isaacs, S., Baggish, A., et al. (2015). Ruptured tendons in anabolic-androgenic steroid users: a cross-sectional cohort study. Am. J. Sports Med. 43, 2638–2644. doi: 10.1177/0363546515602010
Kersey, R. D., Elliot, D. L., Goldberg, L., Kanayama, G., Leone, J. E., Pavlovich, M., et al. (2012). National athletic trainers' association position statement: anabolic-androgenic steroids. J. Athl. Train. 47, 567–588. doi: 10.4085/1062-6050-47.5.08
Kicman, A. T., and Gower, D. (2003). Anabolic steroids in sport: biochemical, clinical and analytical perspectives. Ann. Clin. Biochem. 40, 321–356. doi: 10.1258/000456303766476977
Klimek, P., Murray, S. B., Brown, T., Gonzales, I. V. M., and Blashill, A. J. (2018). Thinness and muscularity internalization: associations with disordered eating and muscle dysmorphia in men. Int. J. Eat. Disord. 51, 352–357. doi: 10.1002/eat.22844
Kohl, H. W., Craig, C. L., Lambert, E. V., Inoue, S., Alkandari, J. R., Leetongin, G., et al. (2012). The pandemic of physical inactivity: global action for public health. Lancet 380, 294–305. doi: 10.1016/S0140-6736(12)60898-8
Levallius, J., Collin, C., and Birgegård, A. (2017). Now you see it, Now you don't: compulsive exercise in adolescents with an eating disorder. J. Eat. Disord. 5, 9. doi: 10.1186/s40337-016-0129-8
Lichtenstein, M. B., Emborg, B., Hemmingsen, S. D., and Hansen, N. B. (2017). Is exercise addiction in fitness centers a socially accepted behavior? Addict. Behav. Rep. 6, 102–105. doi: 10.1016/j.abrep.2017.09.002
Lichtenstein, M. B., and Jensen, T. T. (2016). Exercise addiction in crossfit: prevalence and psychometric properties of the exercise addiction inventory. Addict. Behav. Rep. 3, 33–37. doi: 10.1016/j.abrep.2016.02.002
Lichtenstein, M. B., Larsen, K. S., Christiansen, E., Støving, R. K., and Bredahl, T. V. G. (2014). Exercise addiction in team sport and individual sport: prevalences and validation of the exercise addiction inventory. Addict. Res. Theory. 22, 431–437. doi: 10.3109/16066359.2013.875537
Lichtenstein, M. B., Nielsen, R. O., Gudex, C., Hinze, C. J., and Jørgensen, U. (2018). Exercise addiction is associated with emotional distress in injured and non-injured regular exercisers. Addict. Behav. Rep. 8, 33–39. doi: 10.1016/j.abrep.2018.06.001
Lindqvist Bagge, A. S., Rosén, T., Fahlke, C., Ehrnborg, C., Eriksson, B. O., Moberg, T., et al. (2017). Somatic effects of AAS abuse: a 30-years follow-up study of male former power sports athletes. J. Sci. Med. Sport. 20, 814–818. doi: 10.1016/j.jsams.2017.03.008
Mayolas-Pi, C., Simón-Grima, J., Peñarrubia-Lozano, C., Munguía-Izquierdo, D., Moliner-Urdiales, D., Legaz-Arrese, A., et al. (2017). Exercise addiction risk and health in male and female amateur endurance cyclists. J. Behav. Addict. 6, 74–83. doi: 10.1556/2006.6.2017.018
McAuley, E., and Rudolph, D. (1995). Physical activity, aging, and psychological well-being. J. Aging Phys. Act. 3, 67–96. doi: 10.1123/japa.3.1.67
McDuff, D., Stull, T., Castaldelli-Maia, J. M., Hitchcock, M. E., Hainline, B., Reardon, C. L., et al. (2019). Recreational and ergogenic substance use and substance use disorders in elite athletes: a narrative review. Br. J. Sports Med. 53, 754. doi: 10.1136/bjsports-2019-100669
Mhillaj, E., Morgese, M. G., Tucci, P., Bove, M., Schiavone, S., Trabace, L., et al. (2015). Effects of anabolic-androgens on brain reward function. Front. Neurosci. 9, 295. doi: 10.3389/fnins.2015.00295
Mondin, G. W., Morgan, W. P., Piering, P. N., Stegner, A. J., Stotesbery, C. L., Trine, M. R., et al. (1996). Psychological consequences of exercise deprivation in habitual exercisers. Med. Sci. Sport Exerc. 28, 1199–1203. doi: 10.1097/00005768-199609000-00018
Mónok, K., Berczik, K., Urbán, R., Szabo, A., Griffiths, M. D., Farkas, J., et al. (2012). Psychometric properties and concurrent validity of two exercise addiction measures: a population wide study. Psychol. Sport Exerc. 13, 739–746. doi: 10.1016/j.psychsport.2012.06.003
Morgan, J. F., Reid, F., and Lacey, J. H. (1999). The SCOFF questionnaire: assessment of a new screening tool for eating disorders. BMJ. 319, 1467–1468. doi: 10.1136/bmj.319.7223.1467
Murray, S. B., Rieger, E., Touyz, S. W., and De la Garza García, L. Y. (2010). Muscle dysmorphia and the DSM-V conundrum: where does it belong? A review paper. Int. J. Eat. Disorders. 43, 483–491. doi: 10.1002/eat.20828
Olivardia, R. (2001). Mirror, mirror on the wall, who's the largest of them all? The features and phenomenology of muscle dysmorphia. Harvard Rev. Psychiatry. 9, 254. doi: 10.1080/10673220127900
Parkinson, A. B., and Evans, N. A. (2006). Anabolic androgenic steroids: a survey of 500 users. Med. Sci. Sports Exerc. 38, 644–651. doi: 10.1249/01.mss.0000210194.56834.5d
Pärssinen, M., Kujala, U., Vartiainen, E., Sarna, S., and Seppälä, T. (2000). Increased premature mortality of competitive powerlifters suspected to have used anabolic agents. Int. J. Sports Med. 21, 225–227. doi: 10.1055/s-2000-304
Phillips, K. A., Wilhelm, S., Koran, L. M., Didie, E. R., Fallon, B. A., Feusner, J., et al. (2010). Body dysmorphic disorder: some key issues for DSM-V. Depress. Anxiety. 27, 573–591. doi: 10.1002/da.20709
Piacentino, D., Kotzalidis, G. D., Del Casale, A., Aromatario, M. R., Pomara, C., Girardi, P., et al. (2015). Anabolic-androgenic steroid use and psychopathology in athletes. a systematic review. Curr. Neuropharmacol. 13, 101–121. doi: 10.2174/1570159X13666141210222725
Pope, H. G., and Katz, D. L. (1994). Psychiatric and medical effects of anabolic-androgenic steroid use: a controlled study of 160 athletes. Arch. Gen. Psychiatry 51, 375–382. doi: 10.1001/archpsyc.1994.03950050035004
Rasmussen, J. J., Schou, M., Madsen, P. L., Selmer, C., Johansen, M. L., Ulriksen, P. S., et al. (2018). Cardiac systolic dysfunction in past illicit users of anabolic androgenic steroids. Am. Heart J. 203, 49–56. doi: 10.1016/j.ahj.2018.06.010
Robertson, C. L., Ishibashi, K., Chudzynski, J., Mooney, L. J., Rawson, R. A., Dolezal, B. A., et al. (2016). Effect of exercise training on striatal dopamine D2/D3 receptors in methamphetamine users during behavioral treatment. Neuropsychopharmacology 41, 1629. doi: 10.1038/npp.2015.331
Robison, L. S., Swenson, S., Hamilton, J., and Thanos, P. K. (2018). Exercise reduces dopamine D1R and increases D2R in rats: implications for addiction. Med. Sci. Sports Exerc. 50, 1596–1602. doi: 10.1249/MSS.0000000000001627
Rocks, T., Pelly, F., Slater, G., and Martin, L. A. (2017). Prevalence of exercise addiction symptomology and disordered eating in australian students studying nutrition and dietetics. J. Acad. Nutr. Diet. 117, 1628–1636. doi: 10.1016/j.jand.2017.04.001
Rudolph, S. (2017). The connection between exercise addiction and orthorexia nervosa in German fitness sports. Eat. Weight Disord. Stud. Anorexia Bulimia Obesity 23, 581–586. doi: 10.1007/s40519-017-0437-2
Skemp, K. M., Mikat, R. P., Schenck, K. P., and Kramer, N. A. (2013). Muscle dysmorphia: risk may be influenced by goals of the weightlifter. J. Strength Condition. Res. 27, 2427–2432. doi: 10.1519/JSC.0b013e3182825474
Solenberger, S. E. (2001). Exercise and eating disorders: a 3-year inpatient hospital record analysis. Eat. Behav. 2, 151–168. doi: 10.1016/S1471-0153(01)00026-5
Strober, M., Freeman, R., and Morrell, W. (1997). The long-term course of severe anorexia nervosa in adolescents: survival analysis of recovery, relapse, and outcome predictors over 10–15 years in a prospective study. Int. J. Eat. Disord. 22, 339–360.
Sullivan, M. L., Martinez, C. M., Gennis, P., and Gallagher, E. J. (1998). The cardiac toxicity of anabolic steroids. Prog. Cardiovasc. Dis. 41, 1–15. doi: 10.1016/S0033-0620(98)80019-4
Szabo, A. (1995). The impact of exercise deprivation on well-being of habitual exercisers. Aust. J. Sci. Med. Sport. 27, 68–77.
Szabo, A., and Griffiths, M. D. (2007). Exercise addiction in british sport science students. Int. J. Ment. Health Addict. 5, 25–28. doi: 10.1007/s11469-006-9050-8
Tod, D., Edwards, C., and Cranswick, I. (2016). Muscle dysmorphia: current insights. Psychol. Res. Behav. Manag. 9, 179–188. doi: 10.2147/PRBM.S97404
Veale, D. M. W. C. (1987). Exercise dependence. Br. J. Addict. 82, 735–740. doi: 10.1111/j.1360-0443.1987.tb01539.x
Wewege, M., Thom, J., Rye, K.-A., and Parmenter, B. (2018). Aerobic, resistance or combined training: A systematic review and meta-analysis of exercise to reduce cardiovascular risk in adults with metabolic syndrome. Atherosclerosis 274, 162–171. doi: 10.1016/j.atherosclerosis.2018.05.002
Young, S., Touyz, S., Meyer, C., Arcelus, J., Rhodes, P., Madden, S., et al. (2018). Relationships between compulsive exercise, quality of life, psychological distress and motivation to change in adults with anorexia nervosa. J. Eat. Disord. 6, 2. doi: 10.1186/s40337-018-0188-0
Youngman, J., and Simpson, D. (2014). Risk for exercise addiction: a comparison of triathletes training for sprint-, Olympic-, half-ironman-, and ironman-distance triathlons. J. Clin. Sport Psychol. 8, 19–37. doi: 10.1123/jcsp.2014-0010
Zeulner, B., Ziemainz, H., Beyer, C., Hammon, M., and Janka, R. (2016). Disordered eating and exercise dependence in endurance athletes. Adv. Phys. Edu. 6, 76–87. doi: 10.4236/ape.2016.62009
Zimmer, P., and Bloch, W. (2015). Physical exercise and epigenetic adaptations of the cardiovascular system. Herz 40, 353–360. doi: 10.1007/s00059-015-4213-7
Keywords: exercise dependence, anabolic androgenic steroids, behavioral addiction, sports psychology, mental health
Citation: Gunnarsson B, Entezarjou A, Fernández-Aranda F, Jiménez-Murcia S, Kenttä G and Håkansson A (2022) Understanding exercise addiction, psychiatric characteristics and use of anabolic androgenic steroids among recreational athletes – An online survey study. Front. Sports Act. Living 4:903777. doi: 10.3389/fspor.2022.903777
Received: 24 March 2022; Accepted: 06 July 2022;
Published: 01 August 2022.
Edited by:
Paolo Emilio Adami, World Athletics, MonacoCopyright © 2022 Gunnarsson, Entezarjou, Fernández-Aranda, Jiménez-Murcia, Kenttä and Håkansson. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anders Håkansson, YW5kZXJzX2MuaGFrYW5zc29uQG1lZC5sdS5zZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.