
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Sports Act. Living, 25 April 2022
Sec. Exercise Physiology
Volume 4 - 2022 | https://doi.org/10.3389/fspor.2022.879860
This article is part of the Research TopicClinical Application and Impact of Blood-Flow-Restriction TrainingView all 10 articles
 Ian Burton1*
Ian Burton1* Aisling McCormack2
Aisling McCormack2Objective: To identify current evidence on blood flow restriction training (BFRT) in tendon injuries and healthy tendons, evaluating physiological tendon effects, intervention parameters, and outcomes.
Methods: This scoping review was reported in accordance with the PRISMA Extension for Scoping Reviews (PRISMA-ScR). Databases searched included MEDLINE, CINAHL, AMED, EMBase, SPORTDiscus, Cochrane library (Controlled trials, Systematic reviews), and five trial registries. Two independent reviewers screened studies at title/abstract and full text. Following screening, data was extracted and charted, and presented as figures and tables alongside a narrative synthesis. Any study design conducted on adults, investigating the effects of BFRT on healthy tendons or tendon pathology were included. Data were extracted on physiological tendon effects, intervention parameters and outcomes with BFRT.
Results: Thirteen studies were included, three on tendinopathy, two on tendon ruptures, and eight on healthy Achilles, patellar, and supraspinatus tendons. A variety of outcomes were assessed, including pain, function, strength, and tendon morphological and mechanical properties, particularly changes in tendon thickness. BFRT intervention parameters were heterogeneously prescribed.
Conclusion: Despite a dearth of studies to date on the effects of BFRT on healthy tendons and in tendon pathologies, preliminary evidence for beneficial effects of BFRT on tendons and clinical outcomes is encouraging. As BFRT is a relatively novel method, definitive conclusions, and recommendations on BFRT in tendon rehabilitation cannot be made at present, which should be addressed in future research, due to the potential therapeutic benefits highlighted in this review.
Tendinopathy is a disease entity which can cause significant pain and functional limitations for individuals and collectively places a tremendous burden on society through high healthcare costs (Hopkins et al., 2016; Dean et al., 2017). In chronic tendinopathy, tendons experience morphological changes and can present with increased tendon thickness, fibril disorganization, and neovascularization caused by repetitive tendon microtrauma (Magnusson and Kjaer, 2019; Millar et al., 2021). Tendinopathy prevalence has been shown to be higher in athletes due to frequent jumping, landing, running and change of direction movements (Zwerver et al., 2011). Collectively, tendinopathies can account for up to 30% of all musculoskeletal conditions requiring medical attention, with up to 22% of elite athletes having patellar tendinopathy at least once during their sporting careers (Lian et al., 2005; Skjong et al., 2012; Canosa-Carro et al., 2022). Complete and partial tendon ruptures are also common in both athletes and the general population with the Achilles tendon having the highest prevalence of ruptures (Nyyssonen et al., 2008). Like tendinopathy, tendon ruptures can also cause significant pain, disability and functional limitations and are associated with significant societal and healthcare costs, whether treated surgically or conservatively, with there being a lack of consensus on optimal treatment methods (Holm et al., 2015).
Resistance training has long been considered the treatment of choice in the rehabilitation of chronic tendinopathies, with both eccentric and heavy slow resistance training (HSRT) demonstrating positive clinical effects, for both improving symptoms and tendon structure (Kongsgaard et al., 2010; Beyer et al., 2015). Progressive resistance training is also considered an essential element of rehabilitation following tendon rupture to counteract muscle atrophy and stimulate tendon repair, whether treated conservatively or surgically (Christensen et al., 2020). The application of progressive tendon loads during rehabilitation is essential to not compromise tendon healing, with the precise dosage parameters of resistance training loading a critical consideration (Bohm et al., 2015). Prolonged time under tension with traditional heavy loads during the early phase of tendon rehabilitation could be counterproductive and compromise tendon healing (Loenneke et al., 2012a; Couppe et al., 2015). Blood flow restriction training (BFRT) is a method of resistance training which utilizes pneumatic cuffs or straps around a limb to partially restrict arterial blood flow, while simultaneously occluding venous outflow until the cessation of cuff pressure (Lorenz et al., 2021). BFRT also known as occlusion, hypoxic or Kaatsu training has become increasingly popular over the last decade as a method for enhancing strength gains in healthy populations such as athletes and more recently as a rehabilitation tool in those with musculoskeletal pathologies (Hughes et al., 2017; Barber-Westin and Noyes, 2019; Nitzsche et al., 2021). For example, BFRT has been found to be an efficacious method for increasing strength gains and muscle hypertrophy in rehabilitation following surgery for anterior cruciate ligament (ACL) rupture (Hughes et al., 2018; Caetano et al., 2021). The physiological benefits associated with BFRT, include beneficial adaptations to the cardiovascular, endocrine, and musculoskeletal systems with psychosocial benefits also reported such as mood and performance improvement (Karabulut et al., 2013, 2021; Neto et al., 2016; Silva et al., 2018; Bowman et al., 2019; da Silva et al., 2019; Okita et al., 2019; Freitas et al., 2021a; Miller et al., 2021).
Whilst traditional eccentric or HSRT for tendinopathy utilizes heavy training loads of up to 70% of 1 repetition maximum (1-RM), low-load BFRT (LL-BFRT) typically uses lower training intensities, and loads in the range of 20–40% of 1RM, which may be more tolerable for patients not able to tolerate high muscle-tendon training loads, while still preventing muscle atrophy and promoting hypertrophy (Centner et al., 2019a; Krzysztofik et al., 2019; Shiromaru et al., 2019; Kataoka et al., 2022). Interventional studies have found superior or similar clinical outcomes with LL-BFRT compared to conventional high-load resistance training (HL-RT) in knee rehabilitation for ACL reconstruction, patellofemoral pain, and knee osteoarthritis (Ohta et al., 2003; Bryk et al., 2016; Giles et al., 2017; Ferraz et al., 2018; Korakakis et al., 2018a; Ferlito et al., 2020; Grantham et al., 2021). BFRT has been shown to cause exercise-induced hypoalgesia through endogenous opioid and endocannabinoid mechanisms, so could therefore be a useful pain management tool in early musculoskeletal rehabilitation, particularly in the presence of an acute pain response (Korakakis et al., 2018b; Hughes and Patterson, 2019, 2020; Hughes et al., 2021). Recent evidence suggests that LL-BFRT may be a superior method for augmenting muscular adaptations in early musculoskeletal rehabilitation, which has been found to be comparably effective for inducing muscular hypertrophy and only minimally inferior for increasing muscular strength compared to HL-RT (Manini and Clark, 2009; Abe et al., 2012; Loenneke et al., 2012b; Yasuda et al., 2012; Martin-Hernandez et al., 2013; Lixandrao et al., 2018; Hughes et al., 2019a). The mechanisms of action of BFRT in muscular adaptation are thought to be related to increased inflammation and metabolic stress which can increase blood supply to muscles potentially stimulating muscle growth (Loenneke et al., 2012c; Pearson and Hussain, 2015; Rossi et al., 2018; Freitas et al., 2021a). Other speculated physiological mechanisms explaining muscle hypertrophy adaptations in response to BFRT includes activation of chemoreceptors, muscle swelling, and increased protein synthesis (Freitas et al., 2021a). Due to a paucity of research, it is unclear what effects BFRT may have on tendons, but the induced ischemic muscular milieu may facilitate morphological and mechanical tendon properties through enhanced collagen metabolism and tendon remodeling (Klein et al., 2001; Boesen et al., 2013). Despite these potential beneficial physiological mechanisms of BFRT on tendon healing, the method of training has received a dearth of attention in tendon rehabilitation, despite the clinical benefits found for other musculoskeletal conditions and the knowledge of resistance training being the most evidence-based treatment available for tendinopathies. Therefore, the objective of this scoping review is to evaluate current research on the use of BFRT for treating tendon injuries. The scoping review will be guided by addressing the following review questions on specific aspects of BFRT interventions within tendon rehabilitation: 1. What outcomes have been reported for BFRT in healthy tendons and rehabilitation for tendon injuries and which outcome measures have been used? 2. What BFRT intervention and cuff parameters have been used in published studies? 3. What physiological mechanisms explaining effects of BFRT on tendons and tendon injuries have been investigated in published studies?
Due to the exploratory nature of the research questions a scoping review was conducted as they are recommended for mapping key concepts, evidence gaps and types of evidence within a particular field and can help guide future research and the possibility of conducting systematic reviews on the topic (Tricco et al., 2018). The scoping review is reported in accordance with the Preferred Reporting Items for Systematic reviews and Meta-analysis extension for Scoping reviews known as the PRISMA-ScR (Tricco et al., 2018). This scoping review aimed to evaluate current BFRT interventions in healthy tendons and the rehabilitation of tendon injuries for the first time in the literature. The results will allow dissemination of the parameters of research BFRT interventions to clinical practitioners through peer-reviewed journal publication, allowing increased likelihood of implementation in clinical practice. The review will also outline future research and exercise reporting needs within BFRT interventions in tendon rehabilitation.
The inclusion criteria for the scoping review were guided by a modified PICO (PCoCo) as recommended for scoping reviews (Tricco et al., 2018). Studies including adults aged 18 years or older with a diagnosis of a tendon injury for any time duration were considered. Tendon injuries included both acute partial or full tendon tears or ruptures and any chronic tendon injuries diagnosed as any tendinopathy. Any tendon condition characterized by common tendinopathy symptoms, including full thickness tendon rupture were considered for inclusion. Studies including healthy participants with no history of tendon pathology were also included. Studies including participants with other concurrent injuries or medical conditions not tendon related were excluded. The concept of interest was BFRT for healthy tendons or for the treatment of any tendon related injury, including any type or format such as BFRT performed with bodyweight or external resistance. BFRT may be delivered across a range of settings by health or exercise professionals, delivered in a supervised or unsupervised manner, using any methods for training progression and monitoring. This scoping review considered both experimental and quasi-experimental study designs including randomized controlled trials and non-randomized controlled. In addition, prospective and retrospective cohort studies, case series and case reports were considered for inclusion. Unpublished studies, reviews or reports were not considered for inclusion.
The search was carried out using a uniform search strategy across all databases (Appendix 1) and it included key words from two main concepts: Blood Flow Restriction (“Kaatsu,” “Occlusion training”), and Tendon (“tendon,” “tendinopathy,” “tendon rupture”). The Boolean operators “Or” and “And” were used to link the key words from each concept and to link the concepts themselves, respectively. A 3-step search strategy was implemented in this scoping review. It incorporated the following: (1) a limited search of MEDLINE and CINAHL using initial keywords as, followed by analysis of the text words in the title/abstract and those used to describe articles to develop a full search strategy; (2) The full search strategy was adapted to each database and applied to MEDLINE, CINAHL, AMED, EMBase, SPORTDiscus, and the Cochrane library (Controlled trials, Systematic reviews). The following trial registries were also searched: ClinicalTrials.gov, ISRCTN, The Research Registry, EU-CTR (European Union Clinical Trials Registry), ANZCTR (Australia and New Zealand Clinical Trials Registry). Databases were searched from inception to March 1st, 2022 (Search performed on March 1st, 2022). The search for relevant gray literature included Open Gray, MedNar, Cochrane central register of controlled trials (CENTRAL), EThOS, CORE, and Google Scholar. (3) For each article located in steps 1 and 2, a search of cited and citing articles using Scopus and hand-searching where necessary, was conducted. Studies published in a language other than English were only considered if a translation was available as translation services are not available to the authors.
Following the search, all identified citations were collated and uploaded into RefWorks and duplicates removed. Titles and abstracts were then screened by two independent reviewers for assessment against the inclusion criteria for the review. Potentially relevant studies were retrieved in full, and their citation details imported into Covidence (Veritas Health Innovation, Melbourne, Australia). Two independent reviewers assessed the full text of selected citations in detail against the inclusion criteria. Any disagreements that arose between the reviewers at each stage of the study selection process were resolved through discussion or by input from a third reviewer. The results of the search are reported in accordance with the PRISMA-ScR (Tricco et al., 2018). In accordance with guidance on conducting scoping reviews, critical appraisal was not conducted (Tricco et al., 2018).
Data were extracted from sources included in the scoping review by one reviewer, with independent data extraction by a second reviewer for at least 10% of studies. The data extracted included specific details regarding the population, concept, context, study methods and key findings relevant to the review questions. The data extracted included dimensions such as study type, purpose, population and sample size, methods, details of the BFRT intervention, specific exercises and outcome measures used. Details of the BFRT interventions included type, dosage, cuff parameters, and methods used to progress and adjust the training stimulus. Data were also be extracted on any physiological mechanisms which have been investigated to explain the effects of BFRT on tendons, and positive clinical outcomes. Decreased muscle size and strength are associated with tendon injuries, both for risk and a consequence of pathology. Therefore, data on muscle strength and size outcomes will also be extracted as improvements in muscle size and strength would be positive clinical outcomes in tendon rehabilitation, although not directly related to physiological tendon changes. The extracted data are presented in Table 1 with a narrative synthesis accompanying the tabulated results.
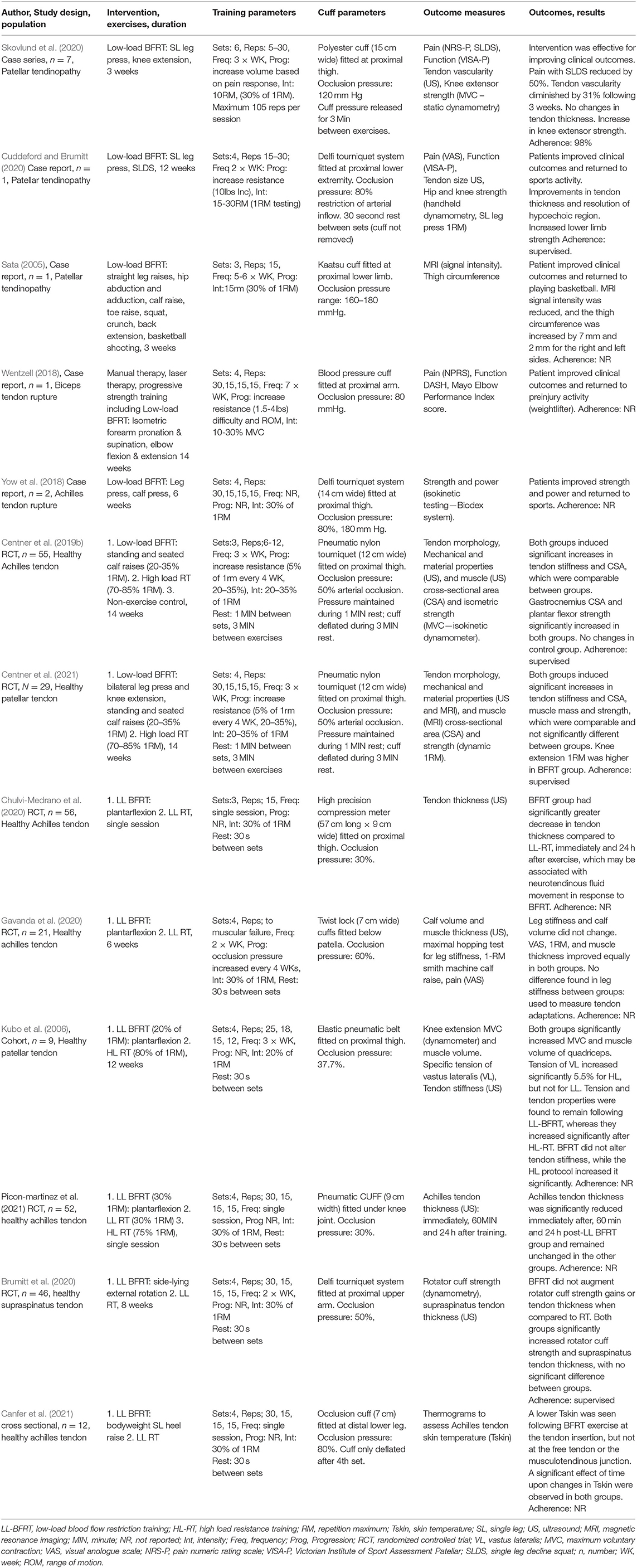
Table 1. Characterizes of included studies and BFRT intervention parameters.
The literature search yielded 29 articles, of which 13 met the inclusion criteria and were included in the review, which is summarized in the PRISMA flow chart (Figure 1), with an overview of the characteristics and outcomes of the included studies provided in Table 1. Five studies investigated the effects of BFRT on tendon pathologies, three on patellar tendinopathy, including one case series (Skovlund et al., 2020) and two case reports (Sata, 2005; Cuddeford and Brumitt, 2020). Two case reports investigated BFRT with tendon ruptures, one on biceps tendon rupture (Wentzell, 2018) and one on Achilles tendon rupture (Yow et al., 2018). Eight studies investigated the effects of BFRT on healthy tendons, five on the Achilles tendon, including four RCTs (Centner et al., 2019b; Chulvi-Medrano et al., 2020; Gavanda et al., 2020; Picon-Martinez et al., 2021) and one cross-sectional study (Canfer et al., 2021), one RCT on the patellar tendon (Centner et al., 2021), one RCT on the supraspinatus tendon (Brumitt et al., 2020), and one cohort study on the patellar tendon (Kubo et al., 2006). The sample sizes of included studies ranged from 1 to 56, with only 12 participants in total for tendon pathologies out of a total of 292 participants, with most included participants having healthy tendons. All included studies investigated the effects of a LL-BFRT intervention, five in isolation (Sata, 2005; Wentzell, 2018; Yow et al., 2018; Cuddeford and Brumitt, 2020; Skovlund et al., 2020) four compared with LL-RT (Brumitt et al., 2020; Chulvi-Medrano et al., 2020; Gavanda et al., 2020; Canfer et al., 2021), three compared with HL-RT (Kubo et al., 2006; Centner et al., 2019b, 2021), and one with both LL-RT and HL-RT (Picon-Martinez et al., 2021). The duration of BFRT interventions ranged from a single session to 14 weeks. The most common exercises used for the BFRT interventions were, plantarflexion calf raises (8), leg press (4), and knee extension (2).
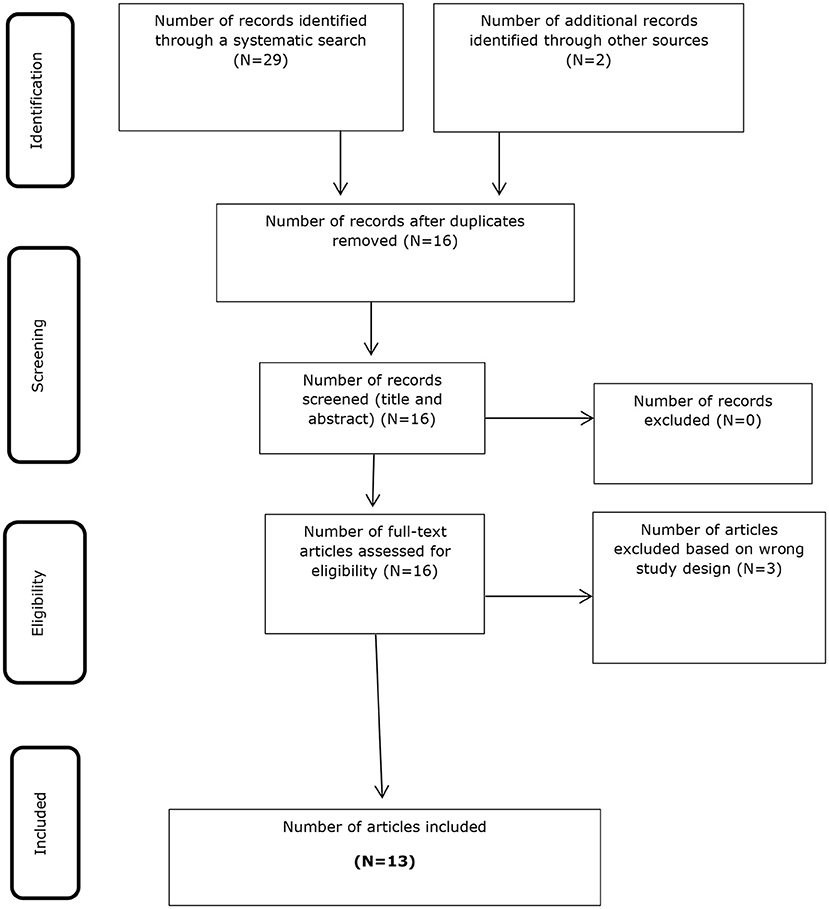
Figure 1. PRISMA study flow diagram.
Four studies assessed pain as an outcome measure with BFRT, two with VAS scales and two with NRS-P scales. Patient reported function scales were assessed in three studies, with two using the Victorian Institute of Sport Assessment Patellar (VISA-P) for patellar tendinopathy and one using both the Disabilities of the Arm, Shoulder, and Hand (DASH) and Mayo Elbow Performance Index score for biceps tendon rupture. Seven studies assessed strength as an outcome, with five using dynamometry, one using 1-RM testing and one using an isokinetic Biodex system. Eight studies used ultrasound (US) to assess tendon mechanical and morphological properties, with tendon thickness the most assessed tendon outcome, measured in five studies, with four studies also assessing tendon stiffness. Muscle properties were assessed in four studies, with three studies using US to assess muscle volume or cross-sectional area and one using magnetic resonance imaging (MRI). One study used thermograms to assess Achilles tendon skin temperature. One study assessed power using an isokinetic Biodex system. One study used MRI to assess tendon signal intensity (echogenicity).
The five studies that investigated the effects of a BFRT intervention on a tendon pathology, all found clinical improvements in pain, function, and muscle strength for included patients, with athletic patients being able to return to sport. The eight studies that investigated BFRT on populations with healthy tendons, all found beneficial physiological effects on tendon morphology and mechanical properties, including beneficial changes in tendon stiffness, thickness, vascularity, signal intensity, and skin temperature. However, two studies did not find changes in tendon stiffness following BFRT. Several studies also found increases in muscle volume and cross-sectional area which was associated with increases in muscular strength and decreased pain levels.
All included studies applied a BFRT cuff to either the proximal or distal limb of the targeted joint, however there were wide variances in the type and size of cuffs used, with cuff width ranging from 7 to 15 cm. Occlusion pressure was calculated as either absolute pressure ranging from 80 to 180 mm Hg, or a percentage of arterial occlusion ranging from 30 to 80%. There were wide variances in the sets and repetitions of prescribed exercises, with the commonly recommended BFRT protocol of four sets of 30, 15, 15, and 15 repetitions being implemented in seven studies. The number of sets across studies ranged from 3-6, with repetitions ranging from 5 to 30, with one study using muscular failure instead of predefined repetitions. Training frequency ranged from 2 to 7 times per week, with training intensity most commonly at 30% of 1-RM, as applied in nine studies. Most studies did not report how the training stimulus was progressed, with two studies progressively increasing occlusion pressure, one increasing percentage of 1-RM (20–35%), and two studies reported using small increases in external weight. Rest time between exercises was 30 s in seven studies and 1 min in two studies, with four studies reporting 3 min rest between different exercises, with three of these studies deflating cuff pressure between exercises.
The main findings of this scoping review were that despite the dearth of studies available on the effects of BFRT on tendons, studies do indicate that BFRT can produce beneficial effects on tendons. Preliminary evidence from case series and case reports indicates that BFRT may be helpful for improving clinical outcomes such as pain in function in rehabilitation of tendinopathy and tendon ruptures, however no RCTs have been conducted in these populations. The evidence for beneficial changes in healthy tendons is more robust due to several RCTs on the topic, showing beneficial physiological effects on tendon morphology and mechanical properties, including increases in tendon stiffness, with reductions in tendon thickness, vascularity, signal intensity (echogenicity) and skin temperature. Although it is unclear if these beneficial effects found in healthy tendons would also occur with pathological tendons, the preliminary evidence suggesting clinical improvement with BFRT in tendon pathology, is suggestive of potential comparable physiological benefits in tendon pathology. There is a clear need for further interventional studies of BFRT in tendinopathy and tendon rupture rehabilitation, with high quality large scale RCTs required to reach definitive conclusions and recommendations for BFRT in tendon pathology. However, there is a clear scientific rationale for the potential of clinical improvements in tendon pathology with BFRT as evidenced by the beneficial effects seen in healthy tendons, and the improvement of clinical outcomes with BFRT in other musculoskeletal disorders (Ohta et al., 2003; Bryk et al., 2016; Giles et al., 2017; Ferraz et al., 2018; Korakakis et al., 2018a; Ferlito et al., 2020; Grantham et al., 2021). Given the increased research interest and clinical use of BFRT in musculoskeletal rehabilitation for non-tendon pathologies, the dearth of available studies applying BFRT to tendon pathologies could be considered somewhat surprising. This is particularly relevant considering resistance training is considered the gold-standard first-line treatment intervention for tendinopathies, particularly Achilles and patellar tendinopathy, due to a plethora of evidence showing the clinical efficacy of resistance training such as eccentric and heavy slow resistance training (Burton and McCormack, 2021). Perhaps the belief that resistance training in tendinopathy must include high training loads has been a limiting factor in the application of LL-BFRT and could explain why it is an underutilized tool in tendon rehabilitation.
The evidence from RCTs comparing LL-BFRT with HL-RT, suggests comparable outcomes for improving muscle and tendon properties (Centner et al., 2019b, 2021), with these changes possibly serving as the mechanisms to explain the clinical benefit seen with BFRT in the case reports in tendinopathy and tendon rupture rehabilitation. The first RCT investigating the effects of LL-BFRT compared to HL-RT in patellar tendinopathy has been registered in Denmark, by the authors who conducted the positive case series included in this review (Skovlund et al., 2020). This trial will be the first step in determining if a shift is required in the tendinopathy rehabilitation field, from the belief that HL-RT is a prerequisite for improving outcomes in tendinopathy, to a possible future where both HL-RT and LL-BFRT are both viable rehabilitation methods, giving clinicians and patients more options and choice during rehabilitation. This may be particularly relevant for non-athletic patients who are unaccustomed to training with heavy loads, sedentary elderly patients, or those who may have contraindications to heavy training and those with an acute painful or reactive tendinopathy or recent tendon rupture, who would be unable to tolerate the loads required with HL-RT. In the rehabilitation of ACL ruptures, LL-BFRT has been found to be a beneficial training method for increasing muscular adaptations in those who have difficultly performing HL-RT (Palmieri-Smith and Lepley, 2015). Furthermore, LL-BFRT has been shown to attenuate pain, increase strength and improve function in rehabilitation for hospital inpatients (Ladlow et al., 2018), ACL rupture (Patterson et al., 2019), patellofemoral pain (Constantinou et al., 2022), rheumatoid arthritis (Rodrigues et al., 2020), ankle fractures (Larsen et al., 2021), and knee osteoarthritis (Ferraz et al., 2018), suggesting pain improvement may be possible with lower training loads in tendon injuries without requiring all patients to undertake HL-RT.
Included studies used low training intensities, with most programming training based on a percentage of an individual's 1-RM, typically 30%, which is congruent with loads between 20 and 40% of 1RM which are typically recommended in the BFRT literature (Kilgas et al., 2019). It is well-established that LL-BFRT requires a higher volume of repetitions to derive physiological adaptations (Kraemer and Ratamess, 2004), with the 30-15-15-15 program of 75 repetitions per set, completed with four sets typically recommended (Patterson et al., 2019). Whilst seven studies implemented this regime, the number of sets across studies ranged from 3 to 6, with repetitions ranging from 5 to 30, with one study using muscular failure instead of predefined repetitions. It is unclear if training to volitional muscular failure with BFRT is required to derive adaptations, with previous BFRT studies suggesting it may be unnecessary (Patterson et al., 2019). Previous studies have shown that muscular failure is not required for muscle hypertrophy, with overall training load volume considered more relevant for augmenting hypertrophy (Schoenfeld et al., 2017, 2019; Lasevicius et al., 2018, 2019). Details on rest periods and whether cuff pressure was maintained or deflated between sets and exercises varied across studies. However, previous research has shown that rest with an inflated or deflated cuff are viable options (Yasuda et al., 2013), although longer rest periods may reduce metabolic stress and therefore limit potential adaptations compared to short rest periods (Loenneke et al., 2010a,b; Patterson et al., 2019). Despite large variances in the BFRT arterial occlusion pressure of included studies which ranged from 30 to 80%, recommendations for occlusion pressure in the literature do range from 40 to 80% (Loenneke et al., 2011; Patterson et al., 2019), suggesting pressure should be individualized based on measures of arterial pressure and comfort levels (Jessee et al., 2016; Mattocks et al., 2017).
This review has several limitations, particularly the small number of studies included, with only five studies on tendon pathology, all being case series or case reports, highlighting the need for future high-quality studies with larger sample sizes, as there are no RCTs on BFRT in tendon pathology currently available. Future studies should also investigate the effects on specific subgroups known to be at increased risk for tendon injuries such as athletes. There was considerable heterogeneity of the BFRT parameters implemented in studies, with standardized methods and reporting of interventions required in future BFRT studies in tendon rehabilitation to enhance clinical translation of the research interventions. The longest follow-up times of included BFRT interventions were 14 weeks, with much longer follow up times required to assess the long-term adaptations and outcomes of BFRT on healthy and pathological tendons. Methods for monitoring and recording adherence to BFRT should also be emphasized in future studies as several included studies did not report the adherence level to BFRT, which may vary due to perceptual responses and comfort which may affect reported clinical outcomes (Loenneke et al., 2011; Martin-Hernandez et al., 2017; Freitas et al., 2021b; Suga et al., 2021).
The superiority of LL-BFRT over standard LL-RT for muscular adaptations have been previously highlighted (Takarada et al., 2002; Madarame et al., 2008; Abe et al., 2010a,b; Yasuda et al., 2010; Centner et al., 2019c; Lambert et al., 2021), with findings from this review suggesting the same may be true for tendon adaptations. However, it remains unclear whether LL-BFRT or standard HL-RT is a superior method for inducing muscular adaptations, with some studies finding equal benefit for muscle strength gains (Lixandrao et al., 2015; Vechin et al., 2015; Curran et al., 2020; Gronfeldt et al., 2020; Hill et al., 2020) and others suggesting HL-RT is a superior method (Hughes et al., 2019b). Some studies included in this review suggest that the tendon adaptations in the healthy Achilles and patellar tendon following LL-BFRT are comparable to those evoked by HL-RT, which is an encouraging finding for the field of tendon rehabilitation (Centner et al., 2019b, 2021). However, these comparable beneficial tendon adaptations found in the high-quality RCTs on healthy tendons need to be investigated in high-quality RCTs in tendon pathology before conclusions can be drawn and recommendations made. Such findings, if found to be comparable and translate in tendon pathology may require a paradigm shift in the tendinopathy rehabilitation field in relation to the prescription of resistance training interventions, particularly for select populations not able to tolerate the standard and proven HL-RT interventions (Loenneke et al., 2013).
Despite a dearth of studies to date on the effects of BFRT on healthy tendons and in tendon pathologies such as tendinopathy, preliminary evidence for beneficial effects of BFRT on tendons and clinical outcomes is encouraging. As BFRT is a relatively novel method, particularly its application in musculoskeletal rehabilitation, definitive conclusions, and recommendations on BFRT in tendon rehabilitation cannot be made at present, which should be addressed in future research, due to the potential therapeutic benefits highlighted in this review. The addition of LL-BFRT as a viable rehabilitation method in tendinopathy rehabilitation would be complimentary to currently utilized HL-RT interventions and provide more rehabilitation options for patients unable to tolerate HL-RT during tendon rehabilitation.
IB conceptualized the work, developed the methods, search strategy, and framework for the review. IB and AM contributed to the development of the research questions and the study design. Both authors developed the first and subsequent drafts of the manuscript and reviewed and approved the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fspor.2022.879860/full#supplementary-material
Abe, T., Fujita, S., Nakajima, T., Sakamaki, M., Ozaki, H., Ogasawara, R., et al. (2010a). Effects of low-intensity cycle training with restricted leg blood flow on thigh muscle volume and VO2MAX in young men. J. Sports Sci. Med. 9, 452–458.
Abe, T., Loenneke, J. P., Fahs, C. A., Rossow, L. M., Thiebaud, R. S., and Bemben, M. G. (2012). Exercise intensity and muscle hypertrophy in blood flow-restricted limbs and non-restricted muscles: a brief review. Clin. Physiol. Funct. Imag. 32, 247–252. doi: 10.1111/j.1475-097X.2012.01126.x
Abe, T., Sakamaki, M., Fujita, S., Ozaki, H., Sugaya, M., Sato, Y., et al. (2010b). Effects of low-intensity walk training with restricted leg blood flow on muscle strength and aerobic capacity in older adults. J. Geriatr. Phys. Ther. 33, 34–40.
Barber-Westin, S., and Noyes, F. R. (2019). Blood flow-restricted training for lower extremity muscle weakness due to knee pathology: a systematic review. Sports Health 11, 69–83. doi: 10.1177/1941738118811337
Beyer, R., Kongsgaard, M., Hougs Kjaer, B., Ohlenschlaeger, T., Kjaer, M., and Magnusson, S. P. (2015). Heavy slow resistance versus eccentric training as treatment for achilles tendinopathy: a randomized controlled trial. Am. J. Sports Med. 43, 1704–1711. doi: 10.1177/0363546515584760
Boesen, A. P., Dideriksen, K., Couppe, C., Magnusson, S. P., Schjerling, P., Boesen, M., et al. (2013). Tendon and skeletal muscle matrix gene expression and functional responses to immobilisation and rehabilitation in young males: effect of growth hormone administration. J. Physiol. 591, 6039–6052. doi: 10.1113/jphysiol.2013.261263
Bohm, S., Mersmann, F., and Arampatzis, A. (2015). Human tendon adaptation in response to mechanical loading: a systematic review and meta-analysis of exercise intervention studies on healthy adults. Sports Med. Open 1:7-015-0009-9. doi: 10.1186/s40798-015-0009-9
Bowman, E. N., Elshaar, R., Milligan, H., Jue, G., Mohr, K., Brown, P., et al. (2019). Proximal, distal, and contralateral effects of blood flow restriction training on the lower extremities: a randomized controlled trial. Sports Health 11, 149–156. doi: 10.1177/1941738118821929
Brumitt, J., Hutchison, M. K., Kang, D., Klemmer, Z., Stroud, M., Cheng, E., et al. (2020). Blood flow restriction training for the rotator cuff: a randomized controlled trial. Int. J. Sports Physiol. Perform. 2020, 1–6. doi: 10.1123/ijspp.2019-0815
Bryk, F. F., Dos Reis, A. C., Fingerhut, D., Araujo, T., Schutzer, M., Cury Rde, P., et al. (2016). Exercises with partial vascular occlusion in patients with knee osteoarthritis: a randomized clinical trial. Knee Surg. Sports Traumatol. Arthrosc. 24, 1580–1586. doi: 10.1007/s00167-016-4064-7
Burton, I., and McCormack, A. (2021). The implementation of resistance training principles in exercise interventions for lower limb tendinopathy: a systematic review. Phys. Ther. Sport 50, 97–113. doi: 10.1016/j.ptsp.2021.04.008
Caetano, D., Oliveira, C., Correia, C., Barbosa, P., Montes, A., and Carvalho, P. (2021). Rehabilitation outcomes and parameters of blood flow restriction training in ACL injury: a scoping review. Phys. Ther. Sport 49, 129–137. doi: 10.1016/j.ptsp.2021.01.015
Canfer, R. J., Chaudry, S., and Miller, S. C. (2021). Thermographic assessment of the immediate and short term-effects of blood flow restriction exercise on achilles tendon skin temperature. Phys. Ther. Sport 49, 171–177. doi: 10.1016/j.ptsp.2021.01.009
Canosa-Carro, L., Bravo-Aguilar, M., Abuin-Porras, V., Almazan-Polo, J., Garcia-Perez-de-Sevilla, G., Rodriguez-Costa, I., et al. (2022). Current understanding of the diagnosis and management of the tendinopathy: an update from the lab to the clinical practice. Dis. Month 2021:101314. doi: 10.1016/j.disamonth.2021.101314
Centner, C., Jerger, S., Lauber, B., Seynnes, O., Friedrich, T., Lolli, D., et al. (2021). Low-load blood flow restriction and high-load resistance training induce comparable changes in patellar tendon properties. Med. Sci. Sports Exerc. 2021:2824. doi: 10.1249/MSS.0000000000002824
Centner, C., Lauber, B., Seynnes, O. R., Jerger, S., Sohnius, T., Gollhofer, A., et al. (2019b). Low-load blood flow restriction training induces similar morphological and mechanical achilles tendon adaptations compared with high-load resistance training. J. Appl. Physiol. 127, 1660–1667. doi: 10.1152/japplphysiol.00602.2019
Centner, C., Wiegel, P., Gollhofer, A., and Konig, D. (2019a). Effects of blood flow restriction training on muscular strength and hypertrophy in older individuals: a systematic review and meta-analysis. Sports Med. 49, 95–108. doi: 10.1007/s40279-018-0994-1
Centner, C., Zdzieblik, D., Roberts, L., Gollhofer, A., and Konig, D. (2019c). Effects of blood flow restriction training with protein supplementation on muscle mass and strength in older men. J. Sports Sci. Med. 18, 471–478.
Christensen, M., Zellers, J. A., Kjaer, I. L., Silbernagel, K. G., and Rathleff, M. S. (2020). Resistance exercises in early functional rehabilitation for achilles tendon ruptures are poorly described: a scoping review. J. Orthopaed. Sports Phys. Ther. 50, 681–690. doi: 10.2519/jospt.2020.9463
Chulvi-Medrano, I., Picon-Martinez, M., Cortell-Tormo, J. M., Tortosa-Martinez, J., Alonso-Aubin, D. A., and Alakhdar, Y. (2020). Different time course of recovery in achilles tendon thickness after low-load resistance training with and without blood flow restriction. J. Sport Rehabil. 30, 300–305. doi: 10.1123/jsr.2019-0403
Constantinou, A., Mamais, I., Papathanasiou, G., Lamnisos, D., and Stasinopoulos, D. (2022). Comparing hip and knee focused exercises versus hip and knee focused exercises with the use of blood flow restriction training in adults with patellofemoral pain: a randomized controlled trial. Eur. J. Phys. Rehabil. Med. 2022:6. doi: 10.23736/S1973-9087.22.06691-6
Couppe, C., Svensson, R. B., Silbernagel, K. G., Langberg, H., and Magnusson, S. P. (2015). Eccentric or concentric exercises for the treatment of tendinopathies? J. Orthopaed. Sports Phys. Ther. 45, 853–863. doi: 10.2519/jospt.2015.5910
Cuddeford, T., and Brumitt, J. (2020). In-season rehabilitation program using blood flow restriction therapy for two decathletes with patellar tendinopathy: a case report. Int. J. Sports Phys. Ther. 15, 1184–1195. doi: 10.26603/ijspt20201184
Curran, M. T., Bedi, A., Mendias, C. L., Wojtys, E. M., Kujawa, M. V., and Palmieri-Smith, R. M. (2020). Blood flow restriction training applied with high-intensity exercise does not improve quadriceps muscle function after anterior cruciate ligament reconstruction: a randomized controlled trial. Am. J. Sports Med. 48, 825–837. doi: 10.1177/0363546520904008
da Silva, J. C. G., Silva, K. F., Domingos-Gomes, J. R., Batista, G. R., da Silva Freitas, E. D., Torres, V. B. C., et al. (2019). Aerobic exercise with blood flow restriction affects mood state in a similar fashion to high intensity interval exercise. Physiol. Behav. 211:112677. doi: 10.1016/j.physbeh.2019.112677
Dean, B. J. F., Dakin, S. G., Millar, N. L., and Carr, A. J. (2017). Review: emerging concepts in the pathogenesis of tendinopathy. Surgeon 15, 349–354. doi: 10.1016/j.surge.2017.05.005
Ferlito, J. V., Pecce, S. A. P., Oselame, L., and De Marchi, T. (2020). The blood flow restriction training effect in knee osteoarthritis people: a systematic review and meta-analysis. Clin. Rehabil. 34, 1378–1390. doi: 10.1177/0269215520943650
Ferraz, R. B., Gualano, B., Rodrigues, R., Kurimori, C. O., Fuller, R., Lima, F. R., et al. (2018). Benefits of resistance training with blood flow restriction in knee osteoarthritis. Med. Sci. Sports Exerc. 50, 897–905. doi: 10.1249/MSS.0000000000001530
Freitas, E. D. S., Karabulut, M., and Bemben, M. G. (2021a). The evolution of blood flow restricted exercise. Front. Physiol. 12, 747759. doi: 10.3389/fphys.2021.747759
Freitas, E. D. S., Miller, R. M., Heishman, A. D., Aniceto, R. R., Larson, R., Pereira, H. M., et al. (2021b). The perceptual responses of individuals with multiple sclerosis to blood flow restriction versus traditional resistance exercise. Physiol. Behav. 229:113219. doi: 10.1016/j.physbeh.2020.113219
Gavanda, S., Isenmann, E., Schloder, Y., Roth, R., Freiwald, J., Schiffer, T., et al. (2020). Low-intensity blood flow restriction calf muscle training leads to similar functional and structural adaptations than conventional low-load strength training: a randomized controlled trial. PLoS ONE 15:e0235377. doi: 10.1371/journal.pone.0235377
Giles, L., Webster, K. E., McClelland, J., and Cook, J. L. (2017). Quadriceps strengthening with and without blood flow restriction in the treatment of patellofemoral pain: a double-blind randomised trial. Br. J. Sports Med. 51, 1688–1694. doi: 10.1136/bjsports-2016-096329
Grantham, B., Korakakis, V., and O'Sullivan, K. (2021). Does blood flow restriction training enhance clinical outcomes in knee osteoarthritis: a systematic review and meta-analysis. Phys. Ther. Sport 49, 37–49. doi: 10.1016/j.ptsp.2021.01.014
Gronfeldt, B. M., Lindberg Nielsen, J., Mieritz, R. M., Lund, H., and Aagaard, P. (2020). Effect of blood-flow restricted vs. heavy-load strength training on muscle strength: systematic review and meta-analysis. Scand. J. Med. Sci. Sports 30, 837–848. doi: 10.1111/sms.13632
Hill, E. C., Housh, T. J., Keller, J. L., Smith, C. M., Anders, J. V., Schmidt, R. J., et al. (2020). Low-load blood flow restriction elicits greater concentric strength than non-blood flow restriction resistance training but similar isometric strength and muscle size. Eur. J. Appl. Physiol. 120, 425–441. doi: 10.1007/s00421-019-04287-3
Holm, C., Kjaer, M., and Eliasson, P. (2015). Achilles tendon rupture–treatment and complications: a systematic review. Scand. J. Med. Sci. Sports 25, e1–10. doi: 10.1111/sms.12209
Hopkins, C., Fu, S. C., Chua, E., Hu, X., Rolf, C., Mattila, V. M., et al. (2016). Critical review on the socio-economic impact of tendinopathy. Asia-Pacific J. Sports Med. Arthrosc. Rehabil. Technol. 4, 9–20. doi: 10.1016/j.asmart.2016.01.002
Hughes, L., Grant, I., and Patterson, S. D. (2021). Aerobic exercise with blood flow restriction causes local and systemic hypoalgesia and increases circulating opioid and endocannabinoid levels. J. Appl. Physiol. 131, 1460–1468. doi: 10.1152/japplphysiol.00543.2021
Hughes, L., Paton, B., Haddad, F., Rosenblatt, B., Gissane, C., and Patterson, S. D. (2018). Comparison of the acute perceptual and blood pressure response to heavy load and light load blood flow restriction resistance exercise in anterior cruciate ligament reconstruction patients and non-injured populations. Phys. Ther. Sport 33, 54–61. doi: 10.1016/j.ptsp.2018.07.002
Hughes, L., Paton, B., Rosenblatt, B., Gissane, C., and Patterson, S. D. (2017). Blood flow restriction training in clinical musculoskeletal rehabilitation: a systematic review and meta-analysis. Br. J. Sports Med. 51, 1003–1011. doi: 10.1136/bjsports-2016-097071
Hughes, L., and Patterson, S. D. (2019). Low intensity blood flow restriction exercise: rationale for a hypoalgesia effect. Medical Hypotheses 132:109370. doi: 10.1016/j.mehy.2019.109370
Hughes, L., and Patterson, S. D. (2020). The effect of blood flow restriction exercise on exercise-induced hypoalgesia and endogenous opioid and endocannabinoid mechanisms of pain modulation. J. Appl. Physiol. 128, 914–924. doi: 10.1152/japplphysiol.00768.2019
Hughes, L., Patterson, S. D., Haddad, F., Rosenblatt, B., Gissane, C., McCarthy, D., et al. (2019a). Examination of the comfort and pain experienced with blood flow restriction training during post-surgery rehabilitation of anterior cruciate ligament reconstruction patients: a UK national health service trial. Phys. Ther. Sport 39, 90–98. doi: 10.1016/j.ptsp.2019.06.014
Hughes, L., Rosenblatt, B., Haddad, F., Gissane, C., McCarthy, D., Clarke, T., et al. (2019b). Comparing the effectiveness of blood flow restriction and traditional heavy load resistance training in the post-surgery rehabilitation of anterior cruciate ligament reconstruction patients: a UK national health service randomised controlled trial. Sports Med. 49, 1787–1805. doi: 10.1007/s40279-019-01137-2
Jessee, M. B., Buckner, S. L., Dankel, S. J., Counts, B. R., Abe, T., and Loenneke, J. P. (2016). The influence of cuff width, sex, and race on arterial occlusion: Implications for blood flow restriction research. Sports Med. 46, 913–921. doi: 10.1007/s40279-016-0473-5
Karabulut, M., Esparza, B., Dowllah, I. M., and Karabulut, U. (2021). The impact of low-intensity blood flow restriction endurance training on aerobic capacity, hemodynamics, and arterial stiffness. J. Sports Med. Phys. Fitness 61, 877–884. doi: 10.23736/S0022-4707.20.11526-3
Karabulut, M., Sherk, V. D., Bemben, D. A., and Bemben, M. G. (2013). Inflammation marker, damage marker and anabolic hormone responses to resistance training with vascular restriction in older males. Clin. Physiol. Funct. Imag. 33, 393–399. doi: 10.1111/cpf.12044
Kataoka, R., Vasenina, E., Hammert, W. B., Ibrahim, A. H., Dankel, S. J., and Buckner, S. L. (2022). Muscle growth adaptations to high-load training and low-load training with blood flow restriction in calf muscles. Eur. J. Appl. Physiol. 2022:7. doi: 10.1007/s00421-021-04862-7
Kilgas, M. A., Lytle, L. L. M., Drum, S. N., and Elmer, S. J. (2019). Exercise with blood flow restriction to improve quadriceps function long after ACL reconstruction. Int. J. Sports Med. 40, 650–656. doi: 10.1055/a-0961-1434
Klein, M. B., Pham, H., Yalamanchi, N., and Chang, J. (2001). Flexor tendon wound healing in vitro: the effect of lactate on tendon cell proliferation and collagen production. J. Hand Surg. 26, 847–854. doi: 10.1053/jhsu.2001.26185
Kongsgaard, M., Qvortrup, K., Larsen, J., Aagaard, P., Doessing, S., Hansen, P., et al. (2010). Fibril morphology and tendon mechanical properties in patellar tendinopathy: effects of heavy slow resistance training. Am. J. Sports Med. 38, 749–756. doi: 10.1177/0363546509350915
Korakakis, V., Whiteley, R., and Epameinontidis, K. (2018b). Blood flow restriction induces hypoalgesia in recreationally active adult male anterior knee pain patients allowing therapeutic exercise loading. Phys. Ther. Sport 32, 235–243. doi: 10.1016/j.ptsp.2018.05.021
Korakakis, V., Whiteley, R., and Giakas, G. (2018a). Low load resistance training with blood flow restriction decreases anterior knee pain more than resistance training alone. A pilot randomised controlled trial. Phys. Ther. Sport 34, 121–128. doi: 10.1016/j.ptsp.2018.09.007
Kraemer, W. J., and Ratamess, N. A. (2004). Fundamentals of resistance training: progression and exercise prescription. Med. Sci. Sports Exerc. 36, 674–688. doi: 10.1249/01.MSS.0000121945.36635.61
Krzysztofik, M., Wilk, M., Wojdala, G., and Golas, A. (2019). Maximizing muscle hypertrophy: a systematic review of advanced resistance training techniques and methods. Int. J. Environ. Res. Public Health 16:10.3390/ijerph16244897. doi: 10.3390/ijerph16244897
Kubo, K., Komuro, T., Ishiguro, N., Tsunoda, N., Sato, Y., Ishii, N., et al. (2006). Effects of low-load resistance training with vascular occlusion on the mechanical properties of muscle and tendon. J. Appl. Biomech. 22, 112–119. doi: 10.1123/jab.22.2.112
Ladlow, P., Coppack, R. J., Dharm-Datta, S., Conway, D., Sellon, E., Patterson, S. D., et al. (2018). Low-load resistance training with blood flow restriction improves clinical outcomes in musculoskeletal rehabilitation: a single-blind randomized controlled trial. Front. Physiol. 9:1269. doi: 10.3389/fphys.2018.01269
Lambert, B., Hedt, C., Daum, J., Taft, C., Chaliki, K., Epner, E., et al. (2021). Blood flow restriction training for the shoulder: a case for proximal benefit. Am. J. Sports Med. 49, 2716–2728. doi: 10.1177/03635465211017524
Larsen, P., Platzer, O. J., Lollesgaard, L., Pedersen, S. K., Nielsen, P. K., Rathleff, M. S., et al. (2021). Blood-flow restricted exercise following ankle fractures - a feasibility study. Foot Ankle Surg. 8:10. doi: 10.1016/j.fas.2021.08.010
Lasevicius, T., Schoenfeld, B. J., Silva-Batista, C., Barros, T. S., Aihara, A. Y., Brendon, H., et al. (2019). Muscle failure promotes greater muscle hypertrophy in low-load but not in high-load resistance training. J. Strength Condition. Res. 2019:3454. doi: 10.1519/JSC.0000000000003454
Lasevicius, T., Ugrinowitsch, C., Schoenfeld, B. J., Roschel, H., Tavares, L. D., De Souza, E. O., et al. (2018). Effects of different intensities of resistance training with equated volume load on muscle strength and hypertrophy. Eur. J. Sport Sci. 18, 772–780. doi: 10.1080/17461391.2018.1450898
Lian, O. B., Engebretsen, L., and Bahr, R. (2005). Prevalence of jumper's knee among elite athletes from different sports: a cross-sectional study. Am. J. Sports Med. 33, 561–567. doi: 10.1177/0363546504270454
Lixandrao, M. E., Ugrinowitsch, C., Berton, R., Vechin, F. C., Conceicao, M. S., Damas, F., et al. (2018). Magnitude of muscle strength and mass adaptations between high-load resistance training versus low-load resistance training associated with blood-flow restriction: a systematic review and meta-analysis. Sports Med. 48, 361–378. doi: 10.1007/s40279-017-0795-y
Lixandrao, M. E., Ugrinowitsch, C., Laurentino, G., Libardi, C. A., Aihara, A. Y., Cardoso, F. N., et al. (2015). Effects of exercise intensity and occlusion pressure after 12 weeks of resistance training with blood-flow restriction. Eur. J. Appl. Physiol. 115, 2471–2480. doi: 10.1007/s00421-015-3253-2
Loenneke, J. P., Abe, T., Wilson, J. M., Ugrinowitsch, C., and Bemben, M. G. (2012a). Blood flow restriction: how does it work? Front. Physiol. 3:392. doi: 10.3389/fphys.2012.00392
Loenneke, J. P., Balapur, A., Thrower, A. D., Barnes, J. T., and Pujol, T. J. (2011). The perceptual responses to occluded exercise. Int. J. Sports Med. 32, 181–184. doi: 10.1055/s-0030-1268472
Loenneke, J. P., Fahs, C. A., Rossow, L. M., Abe, T., and Bemben, M. G. (2012b). The anabolic benefits of venous blood flow restriction training may be induced by muscle cell swelling. Medical Hypotheses 78, 151–154. doi: 10.1016/j.mehy.2011.10.014
Loenneke, J. P., Kearney, M. L., Thrower, A. D., Collins, S., and Pujol, T. J. (2010a). The acute response of practical occlusion in the knee extensors. J. Strength Condition. Res. 24, 2831–2834. doi: 10.1519/JSC.0b013e3181f0ac3a
Loenneke, J. P., Wilson, G. J., and Wilson, J. M. (2010b). A mechanistic approach to blood flow occlusion. Int. J. Sports Med. 31, 1–4. doi: 10.1055/s-0029-1239499
Loenneke, J. P., Wilson, J. M., Balapur, A., Thrower, A. D., Barnes, J. T., and Pujol, T. J. (2012c). Time under tension decreased with blood flow-restricted exercise. Clin. Physiol. Funct. Imag. 32, 268–273. doi: 10.1111/j.1475-097X.2012.01121.x
Loenneke, J. P., Young, K. C., Wilson, J. M., and Andersen, J. C. (2013). Rehabilitation of an osteochondral fracture using blood flow restricted exercise: a case review. J. Bodywork Mov. Ther. 17, 42–45. doi: 10.1016/j.jbmt.2012.04.006
Lorenz, D. S., Bailey, L., Wilk, K. E., Mangine, R. E., Head, P., Grindstaff, T. L., et al. (2021). Blood flow restriction training. J. Athletic Train. 56, 937–944. doi: 10.4085/418-20
Madarame, H., Neya, M., Ochi, E., Nakazato, K., Sato, Y., and Ishii, N. (2008). Cross-transfer effects of resistance training with blood flow restriction. Med. Sci. Sports Exerc. 40, 258–263. doi: 10.1249/mss.0b013e31815c6d7e
Magnusson, S. P., and Kjaer, M. (2019). The impact of loading, unloading, ageing and injury on the human tendon. J. Physiol. 597, 1283–1298. doi: 10.1113/JP275450
Manini, T. M., and Clark, B. C. (2009). Blood flow restricted exercise and skeletal muscle health. Exerc. Sport Sci. Rev. 37, 78–85. doi: 10.1097/JES.0b013e31819c2e5c
Martin-Hernandez, J., Marin, P. J., Menendez, H., Ferrero, C., Loenneke, J. P., and Herrero, A. J. (2013). Muscular adaptations after two different volumes of blood flow-restricted training. Scand. J. Med. Sci. Sports 23, e114–e120. doi: 10.1111/sms.12036
Martin-Hernandez, J., Ruiz-Aguado, J., Herrero, A. J., Loenneke, J. P., Aagaard, P., Cristi-Montero, C., et al. (2017). Adaptation of perceptual responses to low-load blood flow restriction training. J. Strength Condition. Res. 31, 765–772. doi: 10.1519/JSC.0000000000001478
Mattocks, K. T., Jessee, M. B., Counts, B. R., Buckner, S. L., Grant Mouser, J., Dankel, S. J., et al. (2017). The effects of upper body exercise across different levels of blood flow restriction on arterial occlusion pressure and perceptual responses. Physiol. Behav. 171, 181–186. doi: 10.1016/j.physbeh.2017.01.015
Millar, N. L., Silbernagel, K. G., Thorborg, K., Kirwan, P. D., Galatz, L. M., Abrams, G. D., et al. (2021). Tendinopathy. Nat. Rev. Dis. Prim. 7:1-020-00234-1. doi: 10.1038/s41572-020-00234-1
Miller, B. C., Tirko, A. W., Shipe, J. M., Sumeriski, O. R., and Moran, K. (2021). The systemic effects of blood flow restriction training: a systematic review. Int. J. Sports Phys. Ther. 16, 978–990. doi: 10.26603/001c.25791
Neto, G. R., Sousa, M. S., Costa e Silva, G. V., Gil, A. L., Salles, B. F., and Novaes, J. S. (2016). Acute resistance exercise with blood flow restriction effects on heart rate, double product, oxygen saturation and perceived exertion. Clin. Physiol. Funct. Imag. 36, 53–59. doi: 10.1111/cpf.12193
Nitzsche, N., Stauber, A., Tiede, S., and Schulz, H. (2021). The effectiveness of blood-flow restricted resistance training in the musculoskeletal rehabilitation of patients with lower limb disorders: a systematic review and meta-analysis. Clin. Rehabil. 35, 1221–1234. doi: 10.1177/02692155211003480
Nyyssonen, T., Luthje, P., and Kroger, H. (2008). The increasing incidence and difference in sex distribution of achilles tendon rupture in finland in 1987-1999. Scand. J. Surg. 97, 272–275. doi: 10.1177/145749690809700312
Ohta, H., Kurosawa, H., Ikeda, H., Iwase, Y., Satou, N., and Nakamura, S. (2003). Low-load resistance muscular training with moderate restriction of blood flow after anterior cruciate ligament reconstruction. Acta Orthopaed. Scand. 74, 62–68. doi: 10.1080/00016470310013680
Okita, K., Takada, S., Morita, N., Takahashi, M., Hirabayashi, K., Yokota, T., et al. (2019). Resistance training with interval blood flow restriction effectively enhances intramuscular metabolic stress with less ischemic duration and discomfort. Appl. Physiol. Nutr. Metabol. 44, 759–764. doi: 10.1139/apnm-2018-0321
Palmieri-Smith, R. M., and Lepley, L. K. (2015). Quadriceps strength asymmetry after anterior cruciate ligament reconstruction alters knee joint biomechanics and functional performance at time of return to activity. Am. J. Sports Med. 43, 1662–1669. doi: 10.1177/0363546515578252
Patterson, S. D., Hughes, L., Warmington, S., Burr, J., Scott, B. R., Owens, J., et al. (2019). Blood flow restriction exercise: considerations of methodology, application, and safety. Front. Physiol. 10:533. doi: 10.3389/fphys.2019.00533
Pearson, S. J., and Hussain, S. R. (2015). A review on the mechanisms of blood-flow restriction resistance training-induced muscle hypertrophy. Sports Med. 45, 187–200. doi: 10.1007/s40279-014-0264-9
Picon-Martinez, M., Chulvi-Medrano, I., Cortell-Tormo, J. M., Alonso-Aubin, D. A., Alakhdar, Y., and Laurentino, G. (2021). Acute effects of resistance training with blood flow restriction on achilles tendon thickness. J. Hum. Kinet. 78, 101–109. doi: 10.2478/hukin-2021-0032
Rodrigues, R., Ferraz, R. B., Kurimori, C. O., Guedes, L. K., Lima, F. R., de Sa-Pinto, A. L., et al. (2020). Low-load resistance training with blood-flow restriction in relation to muscle function, mass, and functionality in women with rheumatoid arthritis. Arthr. Care Res. 72, 787–797. doi: 10.1002/acr.23911
Rossi, F. E., de Freitas, M. C., Zanchi, N. E., Lira, F. S., and Cholewa, J. M. (2018). The role of inflammation and immune cells in blood flow restriction training adaptation: a review. Front. Physiol. 9:1376. doi: 10.3389/fphys.2018.01376
Sata, S.. (2005). Kaatsu training for patella tendinitis patient. Int Jkaatsu Train Res. 1, 29–32. doi: 10.3806/ijktr.1.29
Schoenfeld, B. J., Contreras, B., Krieger, J., Grgic, J., Delcastillo, K., Belliard, R., et al. (2019). Resistance training volume enhances muscle hypertrophy but not strength in trained men. Med. Sci. Sports Exerc. 51, 94–103. doi: 10.1249/MSS.0000000000001764
Schoenfeld, B. J., Grgic, J., Ogborn, D., and Krieger, J. W. (2017). Strength and hypertrophy adaptations between low- vs. high-load resistance training: a systematic review and meta-analysis. J. Strength Condition. Res. 31, 3508–3523. doi: 10.1519/JSC.0000000000002200
Shiromaru, F. F., de Salles Painelli, V., Silva-Batista, C., Longo, A. R., Lasevicius, T., Schoenfeld, B. J., et al. (2019). Differential muscle hypertrophy and edema responses between high-load and low-load exercise with blood flow restriction. Scand. J. Med. Sci. Sports 29, 1713–1726. doi: 10.1111/sms.13516
Silva, J. C. G., Aniceto, R. R., Oliota-Ribeiro, L. S., Neto, G. R., Leandro, L. S., and Cirilo-Sousa, M. S. (2018). Mood effects of blood flow restriction resistance exercise among basketball players. Percept. Motor Skills 125, 788–801. doi: 10.1177/0031512518776847
Skjong, C. C., Meininger, A. K., and Ho, S. S. (2012). Tendinopathy treatment: where is the evidence? Clin. Sports Med. 31, 329–350. doi: 10.1016/j.csm.2011.11.003
Skovlund, S. V., Aagaard, P., Larsen, P., Svensson, R. B., Kjaer, M., and Magnusson, S. P. (2020). The effect of low-load resistance training with blood flow restriction on chronic patellar tendinopathy—a case series. Transl. Sports Med. 3:151. doi: 10.1002/tsm2.151
Suga, T., Dora, K., Mok, E., Sugimoto, T., Tomoo, K., Takada, S., et al. (2021). Exercise adherence-related perceptual responses to low-load blood flow restriction resistance exercise in young adults: a pilot study. Physiol. Rep. 9:e15122. doi: 10.14814/phy2.15122
Takarada, Y., Sato, Y., and Ishii, N. (2002). Effects of resistance exercise combined with vascular occlusion on muscle function in athletes. Eur. J. Appl. Physiol. 86, 308–314. doi: 10.1007/s00421-001-0561-5
Tricco, A. C., Lillie, E., Zarin, W., O'Brien, K. K., Colquhoun, H., Levac, D., et al. (2018). PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann. Intern. Med. 169, 467–473. doi: 10.7326/M18-0850
Vechin, F. C., Libardi, C. A., Conceicao, M. S., Damas, F. R., Lixandrao, M. E., Berton, R. P., et al. (2015). Comparisons between low-intensity resistance training with blood flow restriction and high-intensity resistance training on quadriceps muscle mass and strength in elderly. J. Strength Condition. Res. 29, 1071–1076. doi: 10.1519/JSC.0000000000000703
Wentzell, M.. (2018). Post-operative rehabilitation of a distal biceps brachii tendon reattachment in a weightlifter: a case report. J. Can. Chiropract. Assoc. 62, 193–201.
Yasuda, T., Fujita, S., Ogasawara, R., Sato, Y., and Abe, T. (2010). Effects of low-intensity bench press training with restricted arm muscle blood flow on chest muscle hypertrophy: a pilot study. Clin. Physiol. Funct. Imag. 30, 338–343. doi: 10.1111/j.1475-097X.2010.00949.x
Yasuda, T., Loenneke, J. P., Ogasawara, R., and Abe, T. (2013). Influence of continuous or intermittent blood flow restriction on muscle activation during low-intensity multiple sets of resistance exercise. Acta Physiol. Hungar. 100, 419–426. doi: 10.1556/APhysiol.100.2013.4.6
Yasuda, T., Loenneke, J. P., Thiebaud, R. S., and Abe, T. (2012). Effects of blood flow restricted low-intensity concentric or eccentric training on muscle size and strength. PLoS ONE 7:e52843. doi: 10.1371/journal.pone.0052843
Yow, B. G., Tennent, D. J., Dowd, T. C., Loenneke, J. P., and Owens, J. G. (2018). Blood flow restriction training after achilles tendon rupture. J. Foot Ankle Surg. 57, 635–638. doi: 10.1053/j.jfas.2017.11.008
Keywords: blood flow restriction, tendinopathy, resistance training, exercise, physiotherapy, tendon
Citation: Burton I and McCormack A (2022) Blood Flow Restriction Resistance Training in Tendon Rehabilitation: A Scoping Review on Intervention Parameters, Physiological Effects, and Outcomes. Front. Sports Act. Living 4:879860. doi: 10.3389/fspor.2022.879860
Received: 20 February 2022; Accepted: 31 March 2022;
Published: 25 April 2022.
Edited by:
Luke Hughes, Northumbria University, United KingdomReviewed by:
Martin Flück, University of Zurich, SwitzerlandCopyright © 2022 Burton and McCormack. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ian Burton, aWFuYnVydG9uXzEwQGhvdG1haWwuY28udWs=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.