
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Sports Act. Living , 17 February 2022
Sec. Physical Activity in the Prevention and Management of Disease
Volume 4 - 2022 | https://doi.org/10.3389/fspor.2022.719063
This article is part of the Research Topic Physical Activity, Exercise and Vascular Health Across the Lifespan View all 7 articles
 Guilherme Tadeu de Barcelos*
Guilherme Tadeu de Barcelos* Isabel Heberle
Isabel Heberle Juliana Cavestré Coneglian
Juliana Cavestré Coneglian Bruno Allan Vieira
Bruno Allan Vieira Rodrigo Sudatti Delevatti
Rodrigo Sudatti Delevatti Aline Mendes Gerage
Aline Mendes GerageIntroduction: Aerobic training of moderate intensity is the primary modality recommended in the management of hypertension. The manipulation of training variables can be an important strategy for the continuity of health benefits; however, little is known about the effects of the progression of aerobic training variables in the adaptations of blood pressure in hypertensive adults.
Objective: To analyze, through a systematic review with meta-analysis, the effects of aerobic training with and without progression on systolic blood pressure (SBP) and diastolic blood pressure (DBP) in hypertensive adults.
Method: The search for the studies was carried out in the PubMed, Cochrane Central, SPORTDiscus and LILACS databases. Clinical trials that analyzed the effect of aerobic training, lasting at least six weeks, on blood pressure in hypertensive individuals comparing with a control group without intervention were selected. The selection of studies and data extraction were carried out independently by two pairs of researchers. The results are presented as mean difference and 95% confidence interval. Statistical significance was considered with p < 0.05.
Results: Of the 13,028 studies found, 24 were selected and included in this review, 12 with progression of training variables and 12 without progression, with a total of 1,207 participants analyzed. There was a reduction in SBP after aerobic training with progression (−10.67 mmHg; 95% CI −15.421, −5.926; p < 0.001) and without progression (−10.17 mmHg; CI −12.213, −8.120; p < 0.001). DBP also decreased after aerobic training with progression (−5.49 mmHg; 95% CI −8.663, −2.310; p < 0.001) and without progression (−6.51 mmHg; 95% CI −9.147, −3.868; p < 0.001). According to the results of the meta-regression analyses, only age showed an association with the reduction of SBP (β: −0.323; CI −0.339, −0.307; p < 0.001).
Conclusion: Aerobic training promotes a reduction in the SBP and DBP levels of adults with hypertension, regardless of whether or not the training variables progression.
Hypertension is a multifactorial chronic disease that affects more than one billion adults worldwide (Mills et al., 2016). It is considered an important cardiovascular risk factor, since it is strongly associated with the occurrence of several other cardiovascular diseases (Rapsomaniki et al., 2014) and mortality (Pan et al., 2020). In addition to medication, changes in lifestyle are essential in the treatment of hypertension and include, among other aspects, the regular practice of physical exercises (Whelton et al., 2018).
In this regard, aerobic training of moderate intensity is the primary modality recommended in the management of hypertension (class of recommendation I and level of evidence A) which should be complemented by dynamic resistance training (Brook et al., 2013; MacDonald and Pescatello, 2018; Williams et al., 2018; Barroso et al., 2020; Rabi et al., 2020; Unger et al., 2020). Previous review studies with meta-analysis showed significant mean reductions of 6.0 to 12.3 mmHg in systolic blood pressure (SBP) and 3.4 to 6.1 mmHg in diastolic blood pressure (DBP) in response to aerobic training in hypertensive individuals (Cornelissen and Smart, 2013; Igarashi et al., 2018; Cao et al., 2019). However, despite including studies with different protocols, these review studies did not analyze the influence of the progression of training variables on blood pressure (BP). Training progression can be defined as a gradual and systematic increases in training stress to maintain overload and, thus, promote continued training adaptations. As fitness improves, frequency, intensity and/or volume must be increased to induce further adaptations (Kasper, 2019). Even though progression is one of the training principles (Pfister et al., 2015), to maintain a physiological stimulus capable of causing adaptations, the guidelines regarding exercise prescription for clinical population indicate the exercise dosage (volume and intensity) to be adopted, lacking discuss whether and how training variables should progress over time.
In hypertension and exercise settings, the main guidelines recommend the practice of aerobic exercises at moderate intensity during 30 to 60 min a day or 150 min a week, in a frequency of four to seven times a week (Brook et al., 2013; Whelton et al., 2018; Sharman et al., 2019; Rabi et al., 2020; Unger et al., 2020). In general, it is recommended to gradually increase the load, especially the training intensity. However, this recommendation is superficial, without specifications indicating how and when to progress in frequency, intensity and/or volume to BP improvement. In terms of progression of intensity, for example, it is not clear if it is enough to increase the absolute load to maintain the same relative intensity or if it is necessary to progress, that is to increase the relative intensity also.
Cornelissen and Smart (2013), in a systematic review with meta-analysis, found that different training frequency and exercise session duration do not significantly affect the effect of aerobic training on BP, what the authors themselves considered counterintuitive as one would presume exercise training-induced BP reductions follow a dose–response relationship. In this sense, some studies that compared the effects of different levels of these variables on aerobic training have shown reductions in BP regardless of the duration or intensity applied (Börjesson et al., 2016; Costa et al., 2018; Gorostegi-Anduaga et al., 2018; Bahmanbeglou et al., 2019), contradicting some indications that the reductions in BP occur in greater magnitude with higher training intensities (Boutcher and Boutcher, 2017). Considering that higher intensities lead to significant benefits resulting from greater physiological adaptations (Boutcher and Boutcher, 2017), not only in BP but in other aspects related to health (Costa et al., 2018), it seems important to progress and reach higher relative intensities when planning a training program.
In addition, even though the practice of physical exercise with the recommended frequencies, durations and intensities causes beneficial effects, especially on cardiorespiratory fitness, the occurrence of a plateau in these effects interferes with the continuity of these benefits (Garber et al., 2011), possibly associated with greater levels of training. Thus, provide stimulus of volume and intensity proportional to the level of training of patients is important, even to maintain benefits already achieved.
The manipulation of training variables can be an important strategy for the continuity of health benefits. However, little is known about the effects of the progression of aerobic training variables (frequency, intensity and/or duration) in the health context, especially in the adaptations of BP in adults with hypertension. Thus, the objective of the present study was to analyze, through a systematic review with meta-analysis, the effects of aerobic training with and without progression in SBP and DBP of adults with hypertension.
This study is characterized as a systematic review with meta-analysis and meta-regression of clinical trials, that is prospective studies comparing the effect and value of intervention(s) against a control in human beings (Friedman et al., 2010). The study followed the items of PRISMA (Moher et al., 2009) and was previously registered on the PROSPERO platform (CRD42020161767).
The PubMed, Cochrane Central, SPORTDiscus and LILACS databases were used to search for articles. The searches were carried out in December 2019 and there were no restrictions for the year of publication. The terms used for the search were “hypertension,” “exercise” and “blood pressure,” applied together. The Boolean operators “OR” and “AND” were used and the search was performed using the MeSH terms with their respective synonyms.
Clinical trials published in Portuguese, Spanish and English, which included hypertensive adults (≥18 years old), of both sexes, who participated in a supervised and structured aerobic exercise intervention for at least six weeks were considered eligible. There were no restrictions on the modality, intensity, session duration, volume and weekly frequency of aerobic training. Clinical trials should compare at least one group with aerobic exercise with a control group without exercise. Studies that contained co-interventions linked to training (e.g., nutritional counseling) were only included if such intervention was applied to both groups (exercise and control). To be eligible, studies should provide data on SBP and DBP at rest before and after the intervention, or the difference between the pre- and post-intervention means with their respective dispersion values. Only studies that provided BP measurements under controlled conditions were eligible. All studies that combined aerobic exercise with another type of physical exercise, that presented only the value of ambulatory BP (24 h) or that included hypertensive individuals with other cardiovascular diseases (i.e. heart failure, coronary artery disease, peripheral artery disease) were excluded. The presence of other comorbidities (i.e. obesity or diabetes type 2) was not considered as exclusion criteria.
In the first selection step, the titles and abstracts of the studies were read by four independent researchers (G.T.B, B.A.V, I.H and J.C.C) divided into pairs. Subsequently, the selected articles were compared between the researchers of each pair. In the next step, the texts were read in full by the peers and the studies were included or excluded according to the eligibility criteria previously established. Disagreements between the two researchers of each pair regarding the inclusion or exclusion of the studies were resolved by the fifth researcher (A.M.G).
Data extraction was performed separately and independently by the same researchers, divided into pairs in the same way as in the previous steps. The extracted data were compared to avoid any error in the extraction process, with the disagreements resolved by the fifth researcher. For all studies, the extraction of data related to the characteristics of the sample included: sample size; sex; average age; body mass index (BMI); training status (according to the classification of each study); presence of comorbidities; use of medications; time of diagnosis of hypertension (time since the diagnostic of the disease—data provided by each study); nutritional co-intervention; and adverse events arising from the intervention. For the information related to the intervention, the following data were considered: time of intervention (duration of the entire aerobic training program, in weeks); modality; method (continuous or interval); session duration; weekly frequency; intensity; adherence to training (perceptual of sessions training completed); and withdrawals (dropout). In addition, the number of progressions for intensity, frequency and/or duration of the sessions was extracted. Studies that clearly reported progression in frequency, duration and/ or intensity of the session were classified as aerobic training with progression, and those that did not clearly report or did not progress in these variables were classified as aerobic training without progression. Progression of frequency was defined as any increase in the number of sessions of training during the week (e.g. from 2 times per week to 3 times per week), while progression of duration was considered as any increase in the session time (e.g. from 30 min/ session to 40 min/session). Progression of intensity was defined as any increase in the relative load (e.g. from 70% of HRmax to 80% of HRmax) or an increase in the points of perceived subjective effort (e.g. from 11 to 15 of Borg scale). Absolute increase of training load for the same rate of physiological work (internal load) was considered intensity adjustment and not progression. Regarding the study outcomes, the information extracted was: SBP and DBP, with mean and measure of dispersion, for the exercise and control groups, at pre- and post-intervention.
The assessment of risk of bias was carried out independently by the same researchers, divided into pairs and the fifth reviewer was consulted to resolve the disagreements. The risk of bias was assessed according to the Cochrane Handbook (Higgins and Green, 2008), considering the following criteria: generation of random sequence; concealment of allocation; concealment of the assessment of outcomes; conducting analysis by intention to treat; and description of withdrawals and exclusions. The risk of bias was classified as: high risk—when methodological criteria, such as the proper generation of random sequences, were not reported or were not performed; low risk—when the methodological criteria were properly carried out; unclear risk—when there was no adequate description of the criteria, it was not possible to evaluate it as high or low risk.
The combined effect estimates for SBP and DBP were calculated using the difference between baseline and post-intervention values, with their respective standard deviation values and number of participants analyzed. Studies that presented other measures of dispersion had the values converted to standard deviation. The results of the analyses are presented as mean difference with a 95% confidence interval, and the calculations were performed using the random effects model. The statistical heterogeneity of the effects was assessed using the I2 inconsistency test, considering values above 50% as high heterogeneity (Higgins and Green, 2008).
Subgroup analyses were performed considering training progression (without progression, with progression, progression in intensity, progression in duration and progression in intensity and duration), sex, presence of comorbidities, use of medications, intervention period, training method (continuous or interval), modalities (walking/running, cycle ergometer, different modalities—e.g. walking and cycle ergometer together) and the training environment (terrestrial or aquatic). The meta-regression analysis was performed to investigate the influence of possible confounding factors on the responses of SBP and DBP, namely: mean age (years); BMI (kg/m2); users of antihypertensive drugs (%); SBP baseline (mmHg); weekly frequency (number of sessions per week); weekly duration (minutes); and intervention period (weeks).
To represent the results, a forest plot was generated, with the average difference and 95% confidence interval. Statistical significance was considered to be p < 0.05. All analyses were performed using the OpenMeta Analyst Software, version 10.10.
Initially, 13,028 studies were found by searching the databases. After removing duplicates, 10,900 studies were selected to read titles and abstracts. At the end of the first stage, 173 studies were selected for full reading, with 149 being excluded. Thus, 24 studies were included in the final analysis, among which 12 studies were classified as progressive aerobic training (Hagberg et al., 1989; Kokkinos et al., 1995; Tanaka et al., 1997; Turner et al., 2000; De Meirelles et al., 2009; Farahani et al., 2010; Lamina, 2010; Latosik et al., 2014; Abdelaal and Mohamad, 2015; Baghaiee et al., 2018; Wong et al., 2018; Soltani et al., 2020) and 12 studies were classified as non-progressive aerobic training (Tanabe et al., 1989; Koga et al., 1992; Miura et al., 1994; Tsai et al., 2002, 2004; Khalid et al., 2013; Arca et al., 2014; Maruf et al., 2014; He et al., 2018; Hong et al., 2018; Izadi et al., 2018; Ramos et al., 2018). In addition, four studies were analyzed twice for presenting two groups of aerobic training (Lamina, 2010; Arca et al., 2014; Soltani et al., 2020) or for collect post-intervention data at two different times (e.g. after 16 weeks of intervention and after 32 week of intervention) (Kokkinos et al., 1995) (Figure 1).

Figure 1. Flowchart with information on the different phases of the systematic review.
Considering all studies, 1,207 participants were analyzed, of which 716 were involved in aerobic training and 491 were part of the control group. Most of the studies included adults of both sexes (41.7%), six studies analyzed only male participants (25.0%), another six analyzed only female participants (25.0%) and two studies did not report this information (8.3%). Regarding the training status, 15 studies included untrained or sedentary participants (62.5%) and nine studies did not report this information (37.5%). The average age of the participants varied between 38.1 and 73.5 years and the BMI showed values between 23.3 and 34.4 kg/m2. Eleven studies included participants using antihypertensive drugs. The general information on the characteristics of the participants is shown in Table 1.
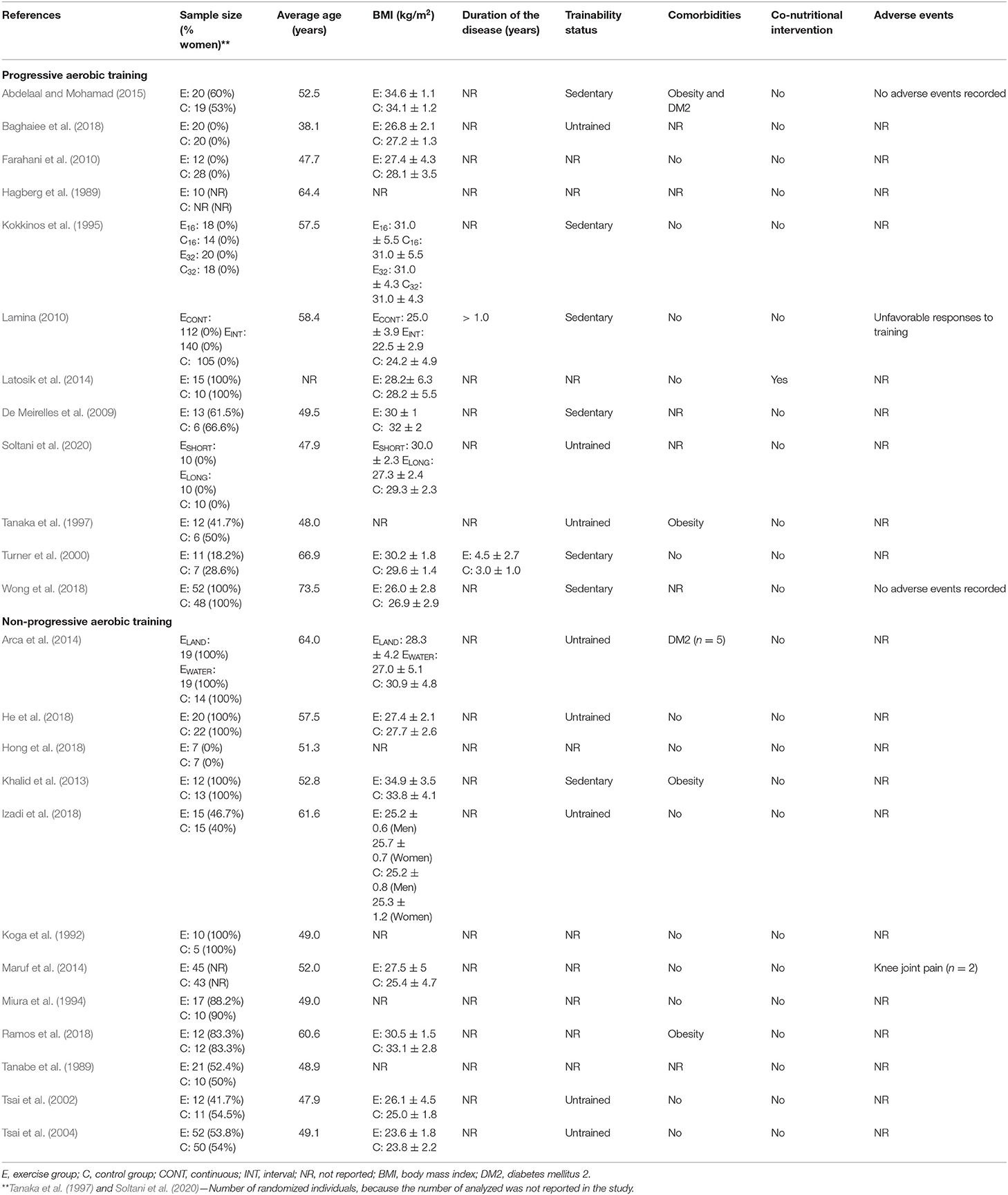
Table 1. Characteristics of the studies.
The general characteristics of the interventions is presented in Table 2. In the case of aerobic training, indoor cycling was the most reported modality (35.7%), followed by running/walking on the treadmill (25%) and soon after swimming (7.14%), aquatic exercises (7.14%) and dance (3.6%). Regarding the methods applied to training, of the 28 aerobic training groups, only five (17.9%) used interval training, while the other 23 (82.1%) used continuous training. The total duration of the interventions ranged from 6 to 37 weeks and the sessions lasted from 20 to 60 min, performed 3 to 4 times a week. Regarding the prescribed intensities, of the 28 aerobic training groups, two groups (7.14%) used percentage of VO2peak to prescribe exercise intensity, six groups (21.43%) used percentage of VO2max, 12 groups (42.86%) used percentage of HRmax, seven groups (25%) used percentage of HRres and only one group (3.57%) used both the percentage of HRmax and RPE in the prescription. One study reported 100% adherence of participants, four studies reported >90% adherence, two studies reported <80% adherence, and 17 studies did not report this information.
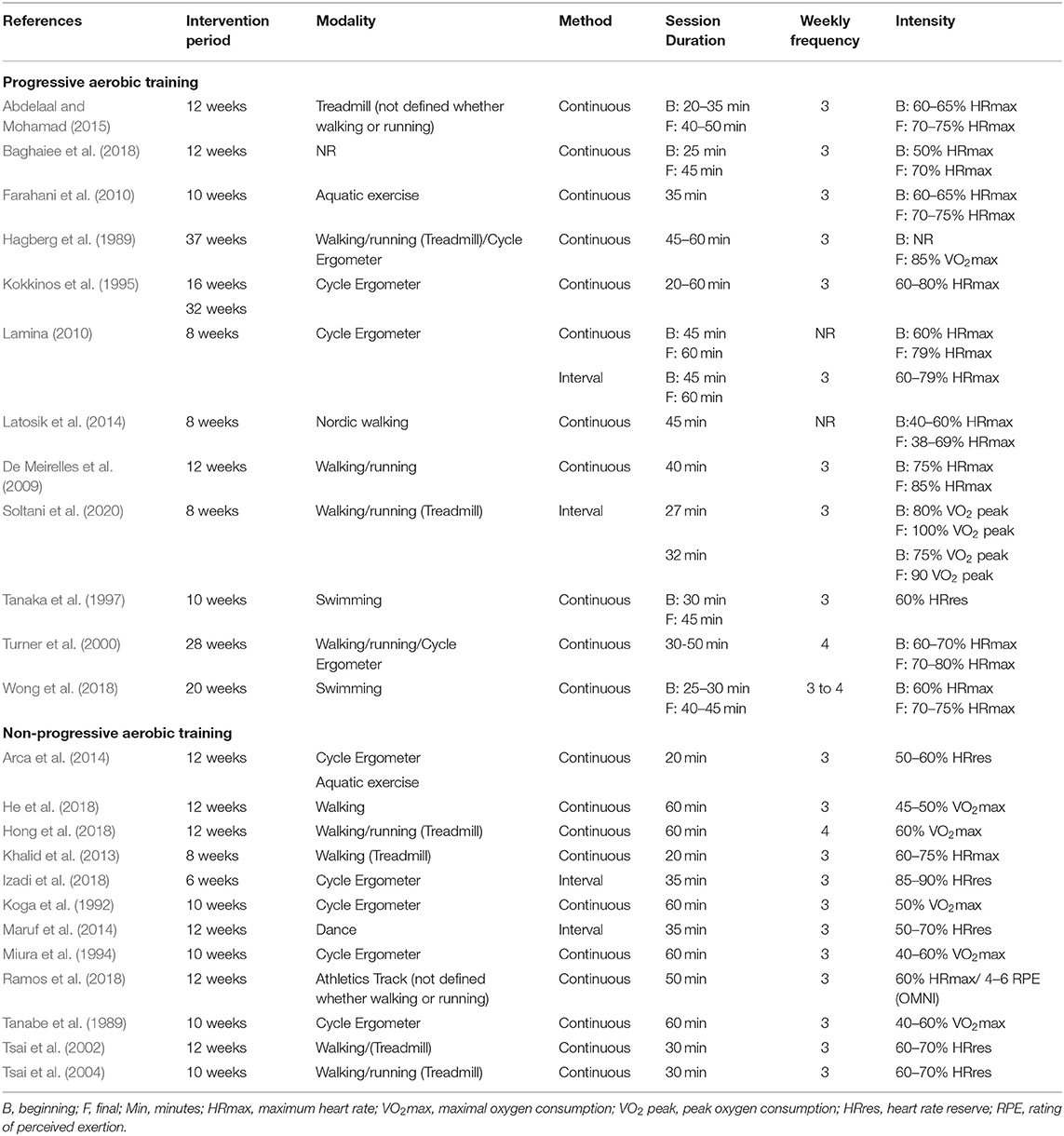
Table 2. Characteristics of the interventions.
Regarding aerobic training with progression, 15 exercise groups (Hagberg et al., 1989; Kokkinos et al., 1995; Tanaka et al., 1997; Turner et al., 2000; De Meirelles et al., 2009; Farahani et al., 2010; Lamina, 2010; Latosik et al., 2014; Abdelaal and Mohamad, 2015; Baghaiee et al., 2018; Wong et al., 2018; Soltani et al., 2020) were analyzed, with the majority (80%) of the studies applying continuous training protocols. The total duration of interventions ranged from 8 to 37 weeks and the duration of sessions from 20 to 60 min, with two studies (Tanaka et al., 1997; Lamina, 2010) that progressed only in duration not showing the number of progressions made. Regarding the weekly frequency of training sessions, one study (Turner et al., 2000) reported four weekly sessions, 11 exercise groups (Hagberg et al., 1989; Kokkinos et al., 1995; Tanaka et al., 1997; De Meirelles et al., 2009; Farahani et al., 2010; Lamina, 2010; Abdelaal and Mohamad, 2015; Baghaiee et al., 2018; Soltani et al., 2020) had three weekly sessions, one exercise group (Wong et al., 2018) had a frequency of three to four weekly sessions and two (Lamina, 2010; Latosik et al., 2014) did not report this information. No study reported progression in weekly frequency. Regarding intensity, seven exercise groups (Hagberg et al., 1989; Turner et al., 2000; De Meirelles et al., 2009; Farahani et al., 2010; Latosik et al., 2014; Soltani et al., 2020) had only progression for this variable, with the most widely used method for prescribing the maximum heart rate (HRmax), applied in 11 exercise groups (Kokkinos et al., 1995; Turner et al., 2000; De Meirelles et al., 2009; Farahani et al., 2010; Lamina, 2010; Latosik et al., 2014; Abdelaal and Mohamad, 2015; Baghaiee et al., 2018; Wong et al., 2018) ranging from 40 to 85% of HRmax, followed by peak oxygen consumption (VO2peak) ranging from 80 to 100% of VO2peak, maximum oxygen consumption (VO2max) at 85%, and reserve heart rate (HRres), at 60%.
Regarding aerobic training without progression, 13 aerobic exercise groups (Tanabe et al., 1989; Koga et al., 1992; Miura et al., 1994; Tsai et al., 2002, 2004; Khalid et al., 2013; Arca et al., 2014; Maruf et al., 2014; He et al., 2018; Hong et al., 2018; Izadi et al., 2018; Ramos et al., 2018) were analyzed, of which only two (15.4%) used interval training (Koga et al., 1992; Maruf et al., 2014; Izadi et al., 2018). A single study showed a frequency of four training sessions per week (Hong et al., 2018), while all others used three sessions per week. The total duration of the interventions ranged from 6 to 12 weeks and the duration of the sessions ranged from 20 to 60 min. For intensity, the most used method for prescription was HRres, applied in six studies (Tsai et al., 2002, 2004; Arca et al., 2014; Maruf et al., 2014; Izadi et al., 2018) ranging from 50 to 90%, followed by VO2max, ranging from 40 to 60%, HRmax, ranging from 60 to 75%, and rating of perceived exertion (RPE), ranging from 4 to 6.
Among all the included studies, only 16.7% carried out the process of randomization and allocation confidentiality of the participants in the groups in an appropriate manner, 75% did not provide enough information to determine the randomization process and almost 80% failed to provide details regarding allocation secrecy. Still, only 25% of the studies were carried out with blinded evaluators, 58.3% of the studies described sample losses and 20.8% adopted analysis by intention to treat. Data on risk of bias separated by group with and without progression can be seen in Table 3.
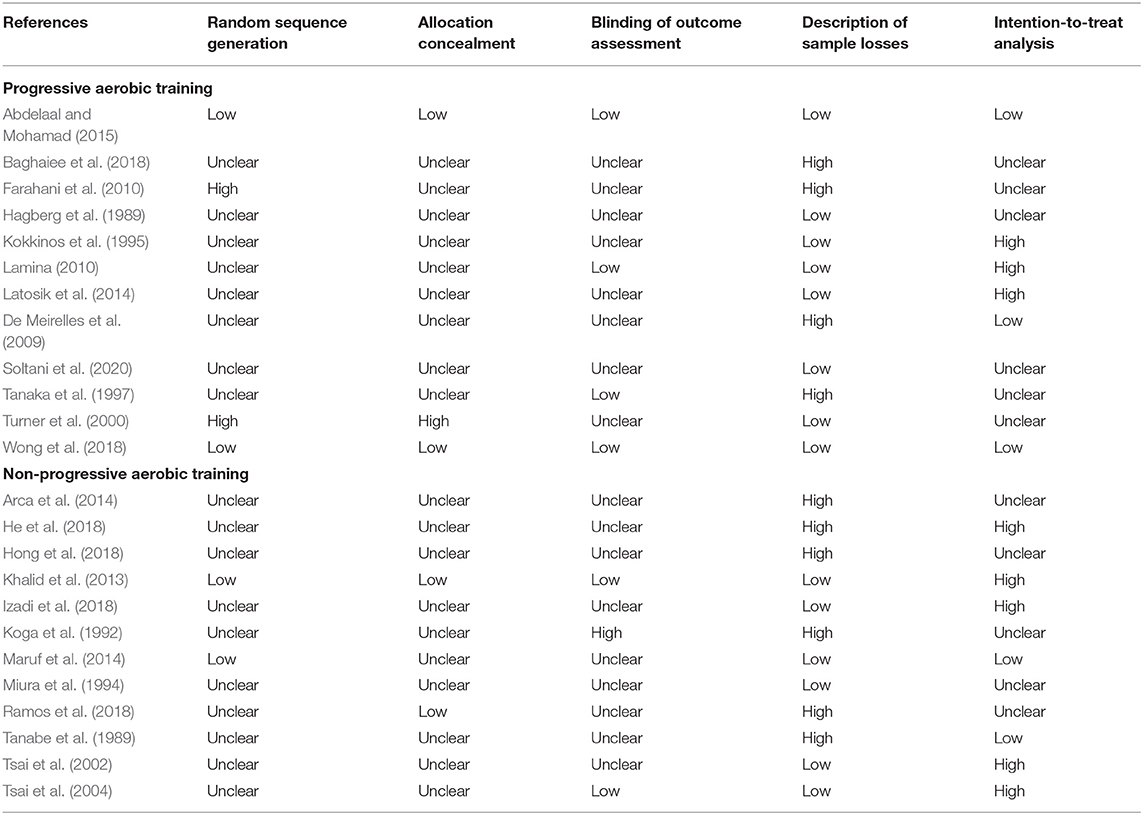
Table 3. Risk of bias.
The aerobic training analyzed in general, totaling 716 included participants, demonstrated a reduction in SBP with a magnitude of 10.56 mmHg (95% CI −14.083, −7.026; p < 0.001; I2: 98%) and in DBP of 5.84 mmHg (95% CI −8.226, −3.465; p < 0.001; I2: 97%).
The results related to aerobic training with progression were analyzed in 15 studies, showing a reduction in SBP of 10.67 mmHg (95% CI −15.421, −5.926; p < 0.001; I2: 99%) and in DBP of 5.49 mmHg (95% CI −8.663, −2.310; p < 0.001; I2: 99%) (Figure 2).

Figure 2. Mean differences in SBP (A) and DPB (B) observed between aerobic training with progression compared to control (without intervention). Study-specific estimates (black square); pooled estimates of random-effects meta-analyses (blue diamond). CI indicates confidence interval.
Analyzing only the studies that progressed in intensity, there was a decrease in SBP of 12.89 mmHg (95% CI −20.134, −5.648; p < 0.001; I2: 64%) and in DBP of 7.09 mmHg (95% CI −11.707, −2.478; p = 0.003; I2: 69%), while for progression only in duration, a reduction in SBP of 13.98 mmHg was found (95% CI −24.238, −3.716; p = 0.008; I2: 36%) and in DBP 5.07 mmHg (95% CI −7.288, −2.843; p < 0.001; I2: 0%). When analyzing the progression in the intensity and duration variables together, statistically significant reductions were found only in the SBP (−8.28 mmHg; 95% CI −15.089, −1.479; p = 0.017; I2: 100%). In DBP, the reduction was 4.48 mmHg, without statistical significance (95% CI −9.100, 0.132; p = 0.057; I2: 99%).
Regarding the effect of aerobic training without progression, adopted in 13 studies, a reduction was found in SBP of 10.17 mmHg (95% CI −12.213, −8.120; p < 0.001; I2: 0%) and in DBP of 6.51 mmHg (95% CI −9.147, −3.868; p < 0.001; I2: 61%) (Figure 3).
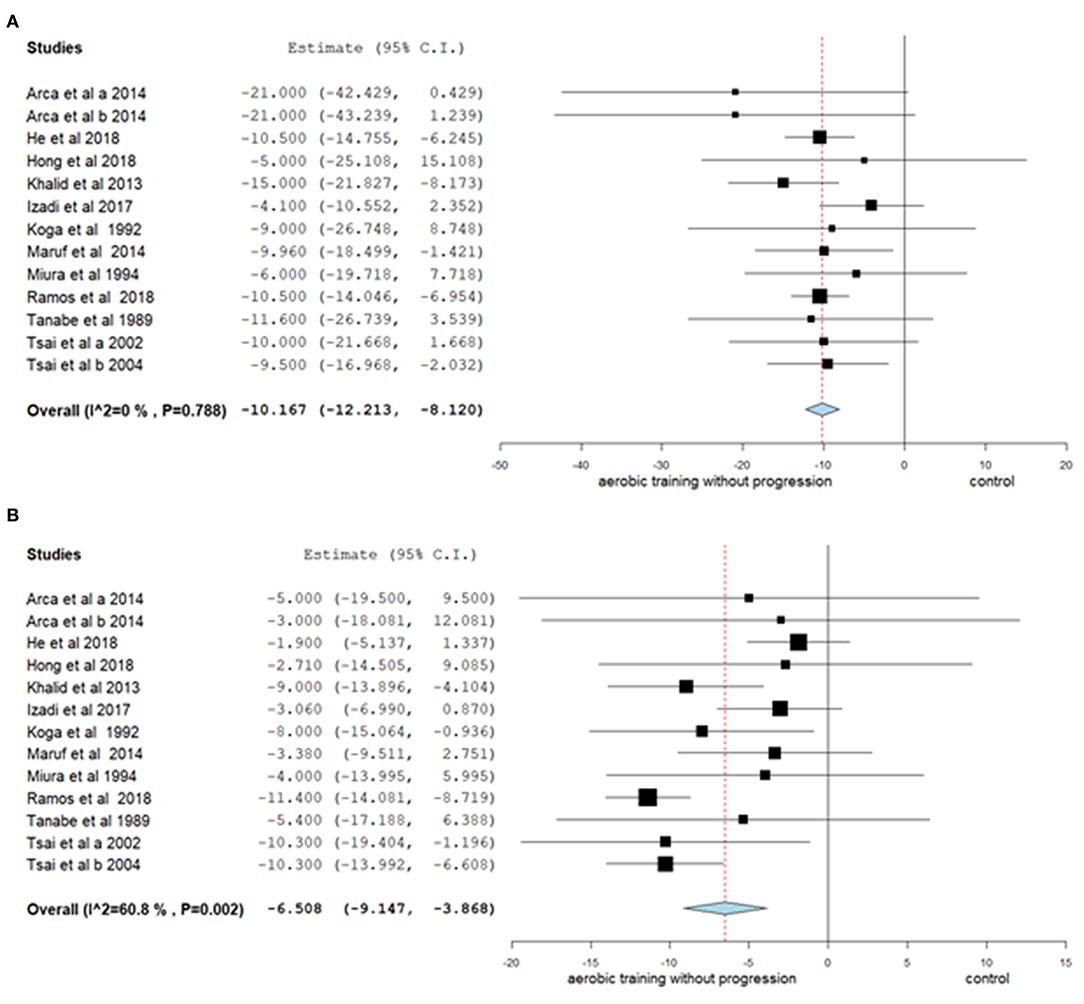
Figure 3. Mean differences in SBP (A) and DBP (B) observed between aerobic training without progression compared to control (without intervention). Study-specific estimates (black square); pooled estimates of random-effects meta-analyses (blue diamond). CI indicates confidence interval.
Subgroup analyses show the effects of aerobic training on SBP and DBP separately under different conditions, between female and male, between subjects with and without comorbidities, between subjects with and without the use of antihypertensive drugs, between different weekly durations of intervention, between methods (continuous and interval), between different modalities and between aquatic and terrestrial environment.
Among the subgroups, in absolute terms, aerobic training provided the greatest reduction magnitude both in SBP (−12.01 mmHg; 95% CI −12.56, −11.46; p < 0.001; I2: 0%) and in DBP (−7.94 mmHg; 95% CI −10.58, −5.29; p < 0.001; I2: 15%) when the exercise was performed in the aquatic environment. The lowest magnitude of SBP reduction after aerobic training was observed in those individuals who did not use any antihypertensive medication (−8.18 mmHg; 95% CI −14.58, −1.78; p = 0.012; I2: 99%). For DBP, the lowest magnitude of reduction after aerobic training was observed in the subgroup of men (−2.80 mmHg; 95% CI −4.76, −0.85; p = 0.005; I2: 76%) (Table 4).
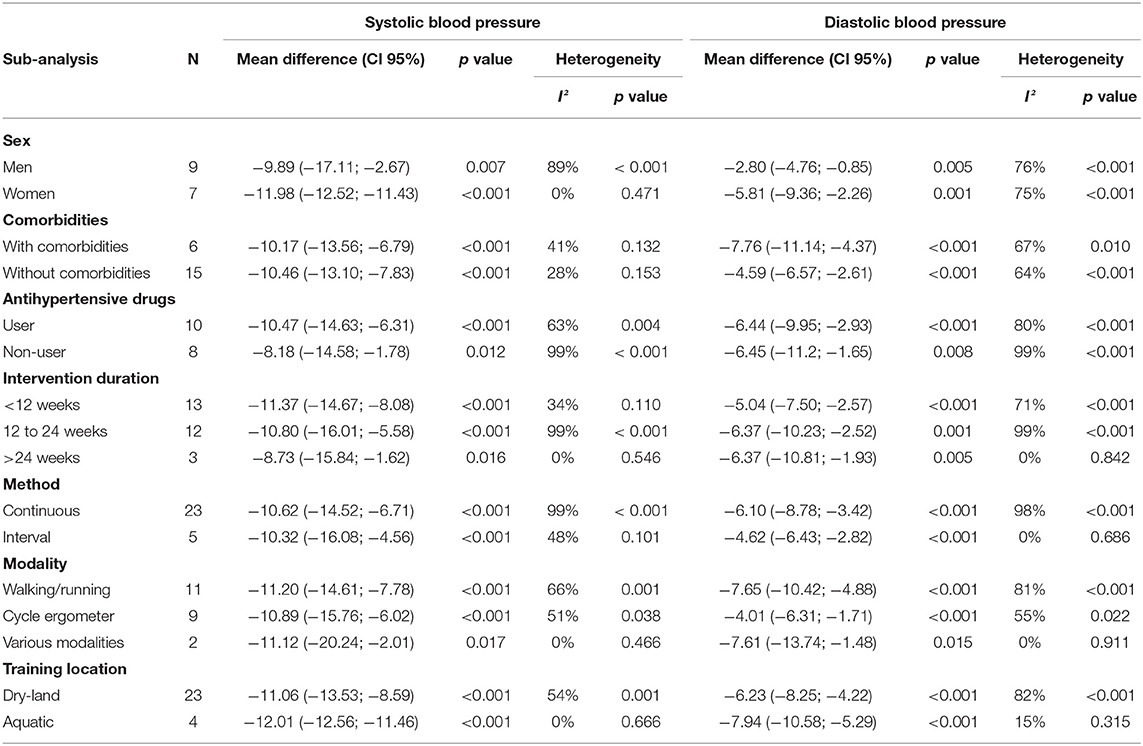
Table 4. Meta-analysis results.
According to the results of the meta-regression analyses, only age showed an association with the reduction of SBP (β: −0.323; CI −0.339, −0.307; p < 0.001), it being considered a predictor in reducing this variable as a result of aerobic training. Thus, the older the sample, the greater the reduction in SBP after the aerobic training period. The variables BMI, users of antihypertensive, baseline SBP, weekly training frequency, weekly duration and intervention period were not associated with SBP reduction. No variable was associated with a reduction in DBP due to aerobic training (Table 5).
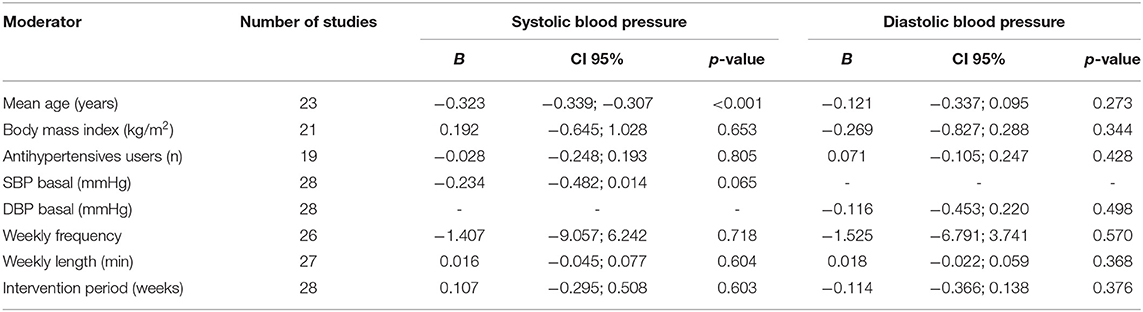
Table 5. Meta-regression results.
This systematic review with meta-analysis aimed to analyze the effects of aerobic training, with and without progression, in SBP and DBP of hypertensive adults. Our main results show that both aerobic training strategies (with and without progression) were effective in reducing BP and that older age is a factor associated with greater BP reductions due to aerobic training in patients with hypertension.
The general results of the present study (aerobic training vs. control group) are in line with results from other meta-analyses, which showed an average reduction of 8 to 12 mmHg in SBP and 5 to 6 mmHg in DBP in hypertensive adults (Cornelissen and Smart, 2013; Igarashi et al., 2018; Cao et al., 2019). Thus, our results reinforce the importance of aerobic training as a primary strategy for the treatment of hypertension, since the reduction in BP resulting from this practice is like that achieved with treatment with antihypertensive drugs (Naci et al., 2019). These results are clinically relevant since a 10 mmHg decrease in SBP is associated with 20% reduction in the risk of developing cardiovascular disease, 27% in the occurrence of stroke and 13% in the risk of mortality (Ettehad et al., 2016).
Although there is no difference in BP reduction between aerobic training with and without progression, reductions of greater magnitudes occurred in studies that progressed in the duration and intensity variables separately. The studies that progressed in intensity (Hagberg et al., 1989; Turner et al., 2000; De Meirelles et al., 2009; Farahani et al., 2010; Latosik et al., 2014; Soltani et al., 2020) showed reductions of 12.89 mmHg (SBP) and 7.09 mmHg (DBP) and achieved the highest percentages of intensity compared to the other studies. Studies that progressed in duration (Tanaka et al., 1997; Lamina, 2010), on the other hand, showed reductions of 13.98 mmHg in SBP and 5.07 mmHg in DBP, and achieved the longest durations in comparison to all studies with and without progression. The studies that progressed in both (Kokkinos et al., 1995; Lamina, 2010; Abdelaal and Mohamad, 2015; Baghaiee et al., 2018; Wong et al., 2018) showed more modest reductions in SBP (8.28 mmHg), with no significant reduction in DBP, and achieved session durations longer than the other studies, however the percentage of intensity was below that observed in general, both in with progression and without progression studies. Although the greatest reductions in SBP occur with studies that have progressed in duration, it is possible that the intensity of training is an important modulator of BP reduction, since both studies that have progressed in duration and those that have progressed in intensity have achieved or maintained a high intensity of training. In addition, our results showed a response of greater magnitude in studies with progression in duration, for SBP, and in intensity, for DBP, which may be associated with different mechanisms of action. In another study conducted in our group, with the objective of evaluating the effects of the progression of aerobic training on the BP of adults with diabetes, reductions in BP were also observed regardless of whether the training progressed (Heberle et al., 2021). Bearing in mind that the performance of these mechanisms in response to training is still unknown (Hellsten and Nyberg, 2015), it is not possible to state the reason associated with these differences.
The literature points to exercise intensity as a determining factor for BP changes in response to training programs (Pescatello et al., 2015; MacDonald and Pescatello, 2018), indicating a dose–response relationship, so that higher intensities of training promote greater reductions in BP (Cornelissen and Smart, 2013). As for the duration of the session, there seems to be no dose–response relationship, as longer durations do not necessarily indicate greater reductions in BP, with beneficial effects occurring even with shorter periods of exercise (Ishikawa-Takata et al., 2003). However, although some studies have investigated the effects of different intensities and durations of exercise, there is insufficient evidence to determine the relationship of these variables with the BP response (Pescatello et al., 2019), especially when not analyzed as isolated doses, but in relation to their manipulations throughout interventions. In the general analysis of our results, the greatest reduction occurred in the study by De Meirelles et al. (2009), both for SBP (−26.3 mmHg) and for DBP (−13.4 mmHg), having reported progression in intensity and reached high intensity (85% HRmax). In addition, although there was no progression in duration, the length of the sessions was intermediate when compared to the other studies (40 min).
Although the evidence regarding progression is not concrete, the manipulation of training variables, such as duration and intensity, are recommended, and must respect a gradual process (Garber et al., 2011), especially in intensity progression (Pescatello et al., 2015). This strategy, in addition to reducing the risks of musculoskeletal injuries and cardiovascular events, favors greater participation by the participant in training (Garber et al., 2011). In addition, other precautions must be considered in this process, such as the levels of BP the person has, recent changes in antihypertensive drugs, effects caused by exercise and medications, in addition to the presence of other diseases and related conditions (Pescatello et al., 2015).
With regard to the subgroup analysis by sex, the effects of the interventions were positive for both men and women. Although the magnitude of reduction observed for women was greater than men, in absolute terms, there was no statistical difference between the groups. Turnbull et al. (2008), in a meta-analysis, also demonstrated that men and women have BP reductions of similar magnitudes. This finding suggests that the effects of aerobic training, with and without progression, on BP are similar between sexes, but it needs to be confirmed in future studies, since the majority of studies included in this review was carried out with both men and women. For analysis between practitioners with and without comorbidities, both groups showed significant BP reductions, with similar magnitudes. This finding demonstrates great clinical relevance, considering that hypertensive patients with comorbidities, which present more serious health risks and greater chances of developing coronary artery disease (CAD) (Wang et al., 2017), benefit from the training as much as those without comorbidities.
Regarding the results by users and non-users of antihypertensive drugs (no statistical difference between groups), both showed significant and similar reductions in SBP and DBP, emphasizing that aerobic training also has great hypotensive potential, being able to further optimize the treatment of hypertension, reducing the risks of complications and improving the clinical picture of hypertensive patients (Moraes-Silva et al., 2017). Reinforcing these results, the meta-regression analysis showed that the use of antihypertensive drugs was not a moderator in reducing BP during aerobic training. However, different dosages and classes of antihypertensive drugs were used in the studies included in this review, which makes it difficult to understand the effects of these factors on the pressure responses observed. Similar to our results, meta-analysis by Sardeli et al. (2020) also found that medication use did not affect BP reduction in response to training. However, this result was not specific to aerobic training and included few studies. Studies evaluating the effects of drug therapy and exercise on BP variables mainly focus on outcomes separately and have conflicting results. Thus, the evidence regarding the interaction between the use of medications and pressure responses to exercise is still scarce (Pescatello et al., 2019).
With regard to the duration of the interventions, it was shown that regardless of the aerobic training being performed for short or long periods (<12 weeks, 12–24 weeks and >24 weeks), the BP reductions are similar (no statistical difference between groups). Likewise, a systematic review by Cao et al. (2019) demonstrated that interventions of <8 weeks, between 8 and 12 weeks and of more than 12 weeks were similarly effective in decreasing BP. On the other hand, Cornelissen and Smart (2013) observed that aerobic training periods of <12 weeks produced greater reductions in SBP and DBP when compared to longer periods, which could be related to the greater adherence of participants to shorter. However, we should consider the importance of the continuity of the training, in order to maintain the benefits achieved. Considering the divergence of the available findings, there is a need for more studies with good methodological quality to better understand the role of the duration of the intervention in the non-drug treatment of hypertensive patients.
As for the training methods, the continuous and the interval methods promoted similar reductions (no statistical difference between groups) in SBP (−10.62; −10.32 mmHg, respectively) and DBP (−6.10; −4.62 mmHg, respectively), showing that both are effective. Another recent meta-analysis, carried out with the hypertensive population (Leal et al., 2020), showed reductions in SBP for both training methods when compared to control groups (continuous: −3.70 mmHg; interval: −5.64 mmHg), but without difference between training groups. For DBP, reduction was also found after continuous (−2.41 mmHg) and interval (−4.80 mmHg) training when compared to control groups, but the magnitude of DBP reduction in the interval method was significantly greater when compared to the continuous one.
Regarding the training modality, our study shows that SBP and DBP reduce in a similar way regardless of whether the aerobic exercise is performed with walking/running (−11.20 mmHg), on cycle ergometers (−10.89 mmHg) or combining the training modalities (−11.12 mmHg) (no statistical difference between groups). This finding has an important practical application, as it demonstrates that exercise professionals can choose the form of aerobic exercise according to the patient's preference, thus being able to favor adherence due to the ease of access to a certain modality or to specific clinical conditions (i.e., using a cycle ergometer due to difficulty mobility with support of their own weight), without prejudice to the reduction in BP.
As for the training location, conducting training in water may be an alternative for the hypertensive population, as it has also shown slightly higher magnitudes of BP reductions (SBP—terrestrial: −11.06 mmHg; aquatic: −12.01 mmHg; DBP—terrestrial: −6.23 mmHg; aquatic: −7.94 mmHg) in absolute terms, without statistical differences. Another study of systematic review also observed that training in water reduces SBP and DBP in a similar way to terrestrial training in adults and the elderly, with 54.5% of the sample classified as hypertensive and 27.3% with pre-hypertensive (Reichert et al., 2018). It is noteworthy that studies comparing exercises performed in different media and evaluating different outcomes in hypertensive patients are still scarce, especially in the case of chronic effects.
The meta-regression analysis showed a significant association between age and SBP responses, indicating that older individuals showed greater magnitude of reductions in SBP after aerobic training. Since the prevalence of hypertension is higher in older adults (McConnell, 2018), the results of the present study suggest that the practice of aerobic training is an important non-drug strategy for reducing BP in the elderly, which has been observed previously (Kelley and Kelley, 2018). However, our results were different from those evidenced by previous studies (Cornelissen and Smart, 2013; Thomopoulos et al., 2018; Sardeli et al., 2020). There is still disagreement in the literature regarding the influence of age on the effects of BP reduction in response to aerobic training, so that other factors must also be considered, like time of hypertension diagnostic, presence of comorbidities, complications due to hypertension and presence of target organ injury.
An important point to be highlighted in the present study is that most studies with progression used HRmax to prescribe the intensity of exercise (Kokkinos et al., 1995; Turner et al., 2000; De Meirelles et al., 2009; Farahani et al., 2010; Lamina, 2010; Latosik et al., 2014; Abdelaal and Mohamad, 2015; Baghaiee et al., 2018; Wong et al., 2018) while only one study without progression used this method (Khalid et al., 2013). HRmax is a limited method to prescribe and control intensity, because it does not consider the HRrest, which is influenced by factors such as age and mainly the training status of the subject. Considering this, the methods for the determination of the HR training target zone that includes HRrest in the calculation, beside HRmax, like the prescription model based on HR reserve, has greater precision. Therefore, we can explain, in part, why the studies with progression did not find greater chronic reductions in BP, since the prescribed intensity may have been underestimated in these studies. That is, not progressing violates a training principle, but using more suitable methods for prescribing intensity (such as HR reserve) seems to mitigate the effects of the lack of progression in training.
Finally, our study exposes some limitations that need to be highlighted. Although the general analysis has a considerable number of studies, some sub-analyses were carried out with a small number of studies. When assessing methodological quality, the set of studies analyzed did not clearly report most of the information, and of the five evaluation criteria, three were reported unclearly in more than 50% of the studies, making it difficult to assess the risk of bias. Another limitation is related to the lack of important information in the studies, which prevent association with the results, such as disease duration, antihypertensive drugs used and the training status of the participants. Still, the search having been carried out more than a year (~18 months) is also a limitation.
On the other hand, the present study has some strengths. As far as we know, this is a first meta-analysis that assesses the effects of the progression of aerobic training in patients with hypertension, with a significant number of participants being analyzed. The analysis of possible moderators of the effect using the meta-regression analysis is also a strong point of the study. In practical terms, although some guidelines recommend the progression of training, more precise information is lacking in relation to the way to progress. In this regard, the present study presents results that will possibly assist in the prescription of exercises, such as manipulation and the increase of the variables of the training, especially session length and intensity, thus maximizing the beneficial effects of exercise on BP.
Aerobic training promotes a reduction in SBP and DBP levels in adults with hypertension, regardless of whether there is progression of the training variables. However, when manipulating the training variables, a response of greater magnitude seems to occur with the progression in duration, for SBP, and in intensity, for DBP. Nevertheless, although there is no chronic difference, the progression of the training variables must be considered, in order to potentiate the effects caused by aerobic training on the pressure response.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
GTB and IH participated in the literary search, data extraction, in data analysis, interpretation of data for the work and writing of the manuscript. JCC and BAV participated in the literary search, data extraction, interpretation of data for the work and writing of the manuscript. RSD and AMG participated in the initial study design, interpretation of data for the work and critical review of the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fspor.2022.719063/full#supplementary-material
Abdelaal, A. A. M., and Mohamad, M. A. (2015). Obesity indices and haemodynamic response to exercise in obese diabetic hypertensive patients: randomized controlled trial. Obes. Res. Clin. Pract. 9. 475–486. doi: 10.1016/j.orcp.2014.11.001
Arca, E. A., Martinelli, B., Martin, L. C., Waisberg, C. B., and Franco RJ da, S. (2014). Aquatic exercise is as effective as dry land training to blood pressure reduction in postmenopausal hypertensive women. Physiother. Res. Int. 19, 93–98. doi: 10.1002/pri.1565
Baghaiee, B., Karimi, P., Ebrahimi, K., Kheslat, S. D. N., Zali, M. H. S., and Moghaddam, A. M. D. (2018). Effects of a 12-week aerobic exercise on markers of hypertension in men. J. Cardiovasc. Thorac. Res. 10, 162–168. doi: 10.15171/jcvtr.2018.26
Bahmanbeglou, N., Ebrahim, K., Maleki, M., Nikpajouh, A., and Ahmadizad, S. (2019). Short-duration high-intensity interval exercise training is more effective than long duration for blood pressure and arterial stiffness but not for inflammatory markers and lipid profiles in patients with stage 1 hypertension. J. Cardiopulm. Rehabil. Prev. 39, 50–55. doi: 10.1097/HCR.0000000000000377
Barroso, W. K. S., Rodrigues, C. I. S., Bortolotto, L. A., Gomes, M. A. M., Brandão, A. A., and Feitosa, A. D. M. (2020). Diretrizes Brasileiras de Hipertensão Arterial – 2020. Arq. Bras. Cardiol. 116, 516–658.
Börjesson, M., Onerup, A., Lundqvist, S., and Dahlöf, B. (2016). Physical activity and exercise lower blood pressure in individuals with hypertension: narrative review of 27 RCTs. Br. J. Sports Med. 50, 356–361. doi: 10.1136/bjsports-2015-095786
Boutcher, Y. N., and Boutcher, S. H. (2017). Exercise intensity and hypertension: what's new? J. Hum. Hypertens. 31, 157–164. doi: 10.1038/jhh.2016.62
Brook, R. D., Appel, L. J., Rubenfire, M., Ogedegbe, G., Bisognano, J. D., and Elliott, W. J. (2013). Beyond medications and diet: Alternative approaches to lowering blood pressure: a scientific statement from the American Heart Association. Hypertension 61, 1360–1383. doi: 10.1161/HYP.0b013e318293645f
Cao, L., Li, X., Yan, P., Wang, X., Li, M., Li, R., et al. (2019). The effectiveness of aerobic exercise for hypertensive population: a systematic review and meta-analysis. J. Clin. Hypertens. 21, 868–876. doi: 10.1111/jch.13583
Cornelissen, V. A., and Smart, N. A. (2013). Exercise training for blood pressure: a systematic review and meta-analysis. J. Am. Heart Assoc. 2, e004473. doi: 10.1161/JAHA.112.004473
Costa, E. C., Hay, J. L., Kehler, D. S., Boreskie, K. F., Arora, R. C., and Umpierre, D. (2018). Effects of high-intensity interval training versus moderate-intensity continuous training on blood pressure in adults with pre- to established hypertension: A systematic review and meta-analysis of randomized trials. Sports Med. 48, 2127–2142. doi: 10.1007/s40279-018-0944-y
De Meirelles, L. R., Mendes-Ribeiro, A. C., Mendes, M. A. P., Da Silva, M. N. S. B., Ellory, J. C., Mann, G. E., et al. (2009). Chronic exercise reduces platelet activation in hypertension: upregulation of the l-arginine-nitric oxide pathway: Exercise in hypertension. Scand. J. Med. Sci. Sports 19, 67–74. doi: 10.1111/j.1600-0838.2007.00755.x
Ettehad, D., Emdin, C. A., Kiran, A., Anderson, S. G., Callender, T., and Emberson, J. (2016). Blood pressure lowering for prevention of cardiovascular disease and death: a systematic review and meta-analysis. Lancet 387, 957–967. doi: 10.1016/S0140-6736(15)01225-8
Farahani, A. V., Mansournia, M. A., Asheri, H., Fotouhi, A., Yunesian, M., and Jamali, M. (2010). The effects of a 10-week water aerobic exercise on the resting blood pressure in patients with essential hypertension. Asian J. Sports Med. 1, 159–167. doi: 10.5812/asjsm.34854
Friedman, L. M., Furberg, C., and DeMets, D. L. (2010). Fundamentals of clinical trials. Fifth Edition. St. Louis: Mosby-Year Book. doi: 10.1007/978-3-319-18539-2
Garber, C. E., Blissmer, B., Deschenes, M. R., Franklin, B. A., Lamonte, M. J., and Lee, I. M. (2011). Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Med. Sci. Sports Exerc. 43, 1334–1359. doi: 10.1249/MSS.0b013e318213fefb
Gorostegi-Anduaga, I., Corres, P., MartinezAguirre-Betolaza, A., Pérez-Asenjo, J., Aispuru, G. R., Fryer, S. M., et al. (2018). Effects of different aerobic exercise programmes with nutritional intervention in sedentary adults with overweight/obesity and hypertension: EXERDIET-HTA study. Eur. J. Prev. Cardiol. 25, 343–353. doi: 10.1177/2047487317749956
Hagberg, J. M., Montain, S. J., Martin, W. H., and Ehsani, A. A. (1989). Effect of exercise training in 60- to 69-year-old persons with essential hypertension. Am. J. Cardiol. 64, 348–353. doi: 10.1016/0002-9149(89)90533-X
He, L. I., Wei, W. R., and Can, Z. (2018). Effects of 12-week brisk walking training on exercise blood pressure in elderly patients with essential hypertension: a pilot study. Clin. Exp. Hypertens. 40, 673–679. doi: 10.1080/10641963.2018.1425416
Heberle, I., Barcelos, G. T., Silveira, L. M. P., Costa, R. R., Gerage, A. M., and Delevatti, R. S. (2021). Effects of aerobic training with and without progression on blood pressure in patients with type 2 diabetes: a systematic review with meta-analyses and meta-regressions. Diabetes Res. Clin. Pract. 171, 1–12 doi: 10.1016/j.diabres.2020.108581
Hellsten, Y., and Nyberg, M. (2015). Cardiovascular adaptations to exercise training. Compr. Physiol. 6, 1–32. doi: 10.1002/cphy.c140080
Higgins, J. P., and Green, S. (2008). Cochrane Handbook for Systematic Reviews of Interventions: Cochrane Book Series. Chichester: John Wiley & Sons. 674, 649. doi: 10.1002/9780470712184
Hong, S., Lee, D., and Lee, G. (2018). Effect of aerobic exercise on blood pressure and arterial compliance in patients with essential hypertension. J. Exerc. Physiol. 21, 9–18.
Igarashi, Y., Akazawa, N., and Maeda, S. (2018). Regular aerobic exercise and blood pressure in East Asians: a meta-analysis of randomized controlled trials. Clin. Exp. Hypertens. 40, 378–389. doi: 10.1080/10641963.2017.1384483
Ishikawa-Takata, K., Ohta, T., and Tanaka, H. (2003). How much exercise is required to reduce blood pressure in essential hypertensives: a dose–response study. Am. J. Hypertens. 16, 629–633. doi: 10.1016/S0895-7061(03)00895-1
Izadi, M. R., Afousi, G. A., Fard, M. A., and Bigi, M. A. B. (2018). High-intensity interval training lowers blood pressure and improves apelin and NOx plasma levels in older treated hypertensive individuals. J. Physiol. Biochem. 74, 47–55. doi: 10.1007/s13105-017-0602-0
Kasper, K (2019). Sports Training Principles. Curr. Sports Med. Rep. 18, 95–96. doi: 10.1249/JSR.0000000000000576
Kelley, G. A., and Kelley, K. S. (2018). Brief report: Exercise and blood pressure in older adults—an updated look. Int. J. Hypertens. 2018, 1–5. doi: 10.1155/2018/6548659
Khalid, T., Nesreen, E., and Ramadhan, O. (2013). Effects of exercise training on postmenopausal hypertension: implications on nitric oxide levels. Med. J. Malaysia 68, 459–464.
Koga, M., Ideishi, M., Matsusaki, M., Tashiro, E., Kinoshita, A., and Ikeda, M. (1992). Mild exercise decreases plasma endogenous digitalislike substance in hypertensive individuals. Hypertension 19(Suppl. 2), 231–236. doi: 10.1161/01.HYP.19.2_Suppl.II231
Kokkinos, P. F., Narayan, P., Colleran, J. A., Pittaras, A., Notargiacomo, A., and Reda, D. (1995). Effects of regular exercise on blood pressure and left ventricular hypertrophy in African-american men with severe hypertension. N. Engl. J. Med. 333, 1462–1467. doi: 10.1056/NEJM199511303332204
Lamina, S (2010). Effects of continuous and interval training programs in the management of hypertension: a randomized controlled trial. J. Clin. Hypertens. 12, 11, 841–849. doi: 10.1111/j.1751-7176.2010.00315.x
Latosik, E., Zubrzycki, I. Z., Ossowski, Z., Bojke, O., Clarke, A., and Wiacek, M. (2014). Physiological responses associated with nordic-walking training in systolic hypertensive postmenopausal women. J. Hum. Kinet. 43, 185–190. doi: 10.2478/hukin-2014-0104
Leal, J. M., Galliano, L. M., and Del Vecchio, F. B. (2020). Effectiveness of high-intensity interval training versus moderate-intensity continuous training in hypertensive patients: a systematic review and meta-analysis. Curr. Hypertens. Rep. 22, 26–39 doi: 10.1007/s11906-020-1030-z
MacDonald, H. V., and Pescatello, L. S. (2018). Exercise prescription for hypertension: New advances for optimizing blood pressure benefits. Lifestyle Heart Health Dis. 2018, 115–136. doi: 10.1016/B978-0-12-811279-3.00009-4
Maruf, F. A., Akinpelu, A. O., and Salako, B. L. (2014). A randomized controlled trial of the effects of aerobic dance training on blood lipids among individuals with hypertension on a thiazide. High Blood Press. Cardiovasc. Prev. 21, 275–283. doi: 10.1007/s40292-014-0063-2
McConnell, K. J (2018). 2017 ACC/AHA guidelines for BP management in adult patients. Pharmacy Today 24, 57–73. doi: 10.1016/j.ptdy.2018.03.037
Mills, K. T., Bundy, J. D., Kelly, T. N., Reed, J. E., Kearney, P. M., and Reynolds, K. (2016). Global disparities of hypertension prevalence and control: a systematic analysis of population-based studies from 90 countries. Circulation 134, 441–450. doi: 10.1161/CIRCULATIONAHA.115.018912
Miura, S., Tashiro, E., Sakai, T., Koga, M., Kinoshita, A., and Sasaguri, M. (1994). Urinary kallikrein activity is increased during the first few weeks of exercise training in essential hypertension. J. Hypertens. 12, 815–823. doi: 10.1097/00004872-199407000-00014
Moher, D., Liberati, A., Tetzlaff, J., and Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta-analyses: the PRISMA Statement. Ann. Int. Med. 151, 264–269. doi: 10.7326/0003-4819-151-4-200908180-00135
Moraes-Silva, I. C., Mostarda, C. T., Silva-Filho, A. C., and Irigoyen, M. C. (2017). Hypertension and exercise training: Evidence from clinical studies. Adv. Exp. Med. Biol. 1000, 65–84. doi: 10.1007/978-981-10-4304-8_5
Naci, H., Salcher-Konrad, M., Dias, S., Blum, M. R., Sahoo, S. A., and Nunan, D. (2019). How does exercise treatment compare with antihypertensive medications? A network meta-analysis of 391 randomised controlled trials assessing exercise and medication effects on systolic blood pressure. Br. J. Sports Med. 53, 859–869. doi: 10.1136/bjsports-2018-099921
Pan, H., Hibino, M., Kobeissi, E., and Aune, D. (2020). Blood pressure, hypertension and the risk of sudden cardiac death: A systematic review and meta-analysis of cohort studies. Eur. J. Epidemiol. 35, 443–454. doi: 10.1007/s10654-019-00593-4
Pescatello, L. S., Buchner, D. M., Jakicic, J. M., Powell, K. E., Kraus, W. E., and Bloodgood, B. (2019). Physical activity to prevent and treat hypertension: a systematic review. Med. Sci. Sports Exerc. 51, 1314–1323. doi: 10.1249/MSS.0000000000001943
Pescatello, L. S., MacDonald, H. V., Lamberti, L., and Johnson, B. T. (2015). Exercise for hypertension: a prescription update integrating existing recommendations with emerging research. Curr. Hypertens. Rep. 17, 87–97. doi: 10.1007/s11906-015-0600-y
Pfister, P. B., Bruin, E. D., Tobler-Ammann, B. C., Maurer, B., and Knols, R. H. (2015). The relevance of applying exercise training principles when designing therapeutic interventions for patients with inflammatory myopathies: a systematic review. Rheumatol. Int. 35, 1641–1654. doi: 10.1007/s00296-015-3343-9
Rabi, D. M., McBrien, K. A., Sapir-Pichhadze, R., Nakhla, M., Ahmed, S. B., Dumanski, S. M., et al. (2020). Hypertension Canada's 2020 comprehensive guidelines for the prevention, diagnosis, risk assessment, and treatment of hypertension in adults and children. Can. J. Cardiol. 36, 596–624. doi: 10.1016/j.cjca.2020.02.086
Ramos, R. M., Coelho-Júnior, H. J., Prado, R. C. R., da Silva, R. S., Asano, R. Y., Prestes, J., et al. (2018). Moderate aerobic training decreases blood pressure but no other cardiovascular risk factors in hypertensive overweight/obese elderly patients. Gerontol. Geriatr. Med. 4, 1–8. doi: 10.1177/2333721418808645
Rapsomaniki, E., Timmis, A., George, J., Pujades-Rodriguez, M., Shah, A. D., and Denaxas, S. (2014). Blood pressure and incidence of twelve cardiovascular diseases: Lifetime risks, healthy life-years lost, and age-specific associations in 1·25 million people. Lancet 383, 1899–1911. doi: 10.1016/S0140-6736(14)60685-1
Reichert, T., Costa, R. R., Barroso, B. M., da Rocha V de, M. B., Delevatti, R. S., and Kruel, L. F. M. (2018). Aquatic training in upright position as an alternative to improve blood pressure in adults and elderly: a systematic review and meta-analysis. Sports Med. 48, 1727–1737. doi: 10.1007/s40279-018-0918-0
Sardeli, A. V., Griffith, G. J., dos Santos, M. V. M. A., Ito, M. S. R., Nadruz, W., and Chacon-Mikahil, M. P. T. (2020). Do baseline blood pressure and type of exercise influence level of reduction induced by training in hypertensive older adults? A meta-analysis of controlled trials. Exp. Gerontol. 140, 111052. doi: 10.1016/j.exger.2020.111052
Sharman, J. E., Smart, N. A., Coombes, J. S., and Stowasser, M. (2019). Exercise and sport science Australia position stand update on exercise and hypertension. J. Hum. Hypertens. 33, 837–843. doi: 10.1038/s41371-019-0266-z
Soltani, M., Bahmanbeglou, N. A., and Ahmadizad, S. (2020). High-intensity interval training irrespective of its intensity improves markers of blood fluidity in hypertensive patients. Clin. Exp. Hypertens. 42, 309–314. doi: 10.1080/10641963.2019.1649687
Tanabe, Y., Urata, H., Kiyonaga, A., Ikeda, M., Tanaka, H., and Shindo, M. (1989). Changes in serum concentrations of taurine and other amino acids in clinical antihypertensive exercise therapy. Clin. Exp. Hypertens. 11, 149–165. doi: 10.3109/10641968909035297
Tanaka, H., Bassett, D. R., Howley, E. T., Thompson, D. L., Ashraf, M., and Rawson, F. L. (1997). Swimming training lowers the resting blood pressure in individuals with hypertension. J. Hypertens. 15, 651–657. doi: 10.1097/00004872-199715060-00012
Thomopoulos, C., Parati, G., and Zanchetti, A. (2018). Effects of blood pressure-lowering treatment on cardiovascular outcomes and mortality: 13 – benefits and adverse events in older and younger patients with hypertension. J. Hypertens. 36, 1622–1636. doi: 10.1097/HJH.0000000000001787
Tsai, J., Yang, H., Wang, W., Hsieh, M., Chen, P., and Kao, C. (2004). The beneficial effect of regular endurance exercise training on blood pressure and quality of life in patients with hypertension. Clin. Exp. Hypertens. 26, 255–265. doi: 10.1081/CEH-120030234
Tsai, J.-C, Chang, W-Y., Kao, C-C, Lu, M-S., et al. (2002). Beneficial effect on blood pressure and lipid profile by programmed exercise training in taiwanese patients with mild hypertension. Clin. Exp. Hypertens. 24, 315–324. doi: 10.1081/CEH-120004234
Turnbull, F., Woodward, M., Neal, B., Barzi, F., Ninomiya, T., and Chalmers, J. (2008). Do men and women respond differently to blood pressure-lowering treatment? Results of prospectively designed overviews of randomized trials. Eur. Heart J. 29, 2669–2680. doi: 10.1093/eurheartj/ehn427
Turner, M. J., Spina, R. J., Kohrt, W. M., and Ehsani, A. A. (2000). Effect of endurance exercise training on left ventricular size and remodeling in older adults with hypertension. J. Gerontol. A Biol. Sci. Med. Sci. 55, M245–M251. doi: 10.1093/gerona/55.4.M245
Unger, T., Borghi, C., Charchar, F., Khan, N. A., Poulter, N. R., and Prabhakaran, D. (2020). 2020 International society of hypertension global hypertension practice guidelines. Hypertension 75, 1334–1357. doi: 10.1161/HYPERTENSIONAHA.120.15026
Wang, J., Ma, J. J., Liu, J., Zeng, D. D., Song, C., and Cao, Z. (2017). Prevalence and risk factors of comorbidities among hypertensive patients in China. Int. J. Med. Sci. 14, 201–212. doi: 10.7150/ijms.16974
Whelton, P. K., Carey, R. M., Aronow, W. S., Casey, D. E., Collins, K. J., and Himmelfarb, D. (2018). 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: Executive summary: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines. Hypertension 71,1269–1324. doi: 10.1161/HYP.0000000000000066
Williams, B., Mancia, G., Spiering, W., Rosei, E. A., Azizi, M., and Burnier, M. (2018). 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 39, 3021–3104. doi: 10.1093/eurheartj/ehy439
Keywords: exercise, cardiovascular diseases, aerobic exercise, high blood pressure, health care
Citation: de Barcelos GT, Heberle I, Coneglian JC, Vieira BA, Delevatti RS and Gerage AM (2022) Effects of Aerobic Training Progression on Blood Pressure in Individuals With Hypertension: A Systematic Review With Meta-Analysis and Meta-Regression. Front. Sports Act. Living 4:719063. doi: 10.3389/fspor.2022.719063
Received: 01 June 2021; Accepted: 05 January 2022;
Published: 17 February 2022.
Edited by:
Mark Rakobowchuk, Thompson Rivers University, CanadaReviewed by:
Philip J. Millar, University of Guelph, CanadaCopyright © 2022 de Barcelos, Heberle, Coneglian, Vieira, Delevatti and Gerage. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Guilherme Tadeu de Barcelos, Z3VpbGhlcm1lX2JhcmNlbGxvc0Bob3RtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.