
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Sports Act. Living , 06 October 2022
Sec. Biomechanics and Control of Human Movement
Volume 4 - 2022 | https://doi.org/10.3389/fspor.2022.1015394
This article is part of the Research Topic Perturbation-based Balance Training View all 16 articles
 Christopher McCrum1,2*
Christopher McCrum1,2* Tanvi S. Bhatt3
Tanvi S. Bhatt3 Marissa H. G. Gerards4,5
Marissa H. G. Gerards4,5 Kiros Karamanidis6
Kiros Karamanidis6 Mark W. Rogers7
Mark W. Rogers7 Stephen R. Lord8,9
Stephen R. Lord8,9 Yoshiro Okubo8,9
Yoshiro Okubo8,9Since the mid-2000s, perturbation-based balance training has been gaining interest as an efficient and effective way to prevent falls in older adults. It has been suggested that this task-specific training approach may present a paradigm shift in fall prevention. In this review, we discuss key concepts and common issues and questions regarding perturbation-based balance training. In doing so, we aim to provide a comprehensive synthesis of the current evidence on the mechanisms, feasibility and efficacy of perturbation-based balance training for researchers and practitioners. We address this in two sections: “Principles and Mechanisms” and “Implementation in Practice.” In the first section, definitions, task-specificity, adaptation and retention mechanisms and the dose-response relationship are discussed. In the second section, issues related to safety, anxiety, evidence in clinical populations (e.g., Parkinson's disease, stroke), technology and training devices are discussed. Perturbation-based balance training is a promising approach to fall prevention. However, several fundamental and applied aspects of the approach need to be further investigated before it can be widely implemented in clinical practice.
Large mechanical destabilizing disturbances during walking (such as slips and trips) lead to most falls among community-dwelling older adults (1–8). Interventions to reduce falls among older adults and clinical populations with balance impairment have received much attention in the literature, with multiple Cochrane reviews on the topic (9–14). Physical exercise is the most evidence-based approach for preventing falls, with challenging balance exercise among the most successful approaches (13, 15, 16). This aligns with the notion of task-specificity in exercise-based fall prevention (17–24), and the development of perturbation-based balance training (PBT).
Interest in the use of large mechanical perturbations as a method of preventing falls has steadily increased since the mid-2000s. In this period: Pai and Bhatt (18) presented a framework for using repeated slip perturbations to reduce slip-related falls; Grabiner et al. (19) presented evidence and theory on how the task-specific training of limiting trunk motion during slips and trips might reduce fall risk; Oddsson et al. (17) presented a balance training programme with a focus on training specificity, incorporating perturbations; and Mansfield et al. (25) published the first protocol for an RCT of PBT in older adults. Two subsequent large trials showed promising effects of PBT interventions on daily life fall incidence in older adults (26, 27) and another highlighted the clinical feasibility of this approach (28). Subsequent reviews and meta-analyses have further supported these encouraging results (29–33). More recently, a large, pragmatic RCT conducted in a clinical setting (34) and a smaller experimental trial (35) also reported positive fall-related outcomes. In contrast, a recent trial conducted in individuals with chronic stroke reported inconclusive results (36). Further RCTs of PBT are currently underway (37–41).
Despite the accumulating research on PBT, there is much still to be learned. Even so, practitioners are open to implementing PBT (42, 43) and desire more knowledge on the topic (43). In this review, we discuss some of the key concepts and common issues and questions around PBT. In doing so, we aim to provide a comprehensive synthesis of the current evidence on the mechanisms, feasibility, and efficacy of perturbation-based balance training for researchers and practitioners. We address this in two sections: “Principles and Mechanisms” and “Implementation in Practice.”
Various names for the same, or similar, training concepts to PBT can be found in the literature. These include reactive balance training, perturbation training, reactive step training and fall-resisting skills training, and there is not yet clear consensus on the best terminology. Here, we define PBT as balance training that uses repeated, externally applied mechanical perturbations to trigger rapid reactions to regain postural stability in a safe and controlled environment. The goal of PBT is to specifically target and improve the ability to recover stability in destabilizing situations like those that lead to falls in daily life. To meet this definition of PBT, the training should meet two key criteria (Figure 1): (1) the training should use external perturbations that induce a sudden motor response and, (2) these perturbations should be of sufficient magnitude to induce a loss of stability that would lead to a fall without a sufficient motor response (or use of the safety harness). Biomechanically, a loss of stability occurs when the position and motion characteristics of the center of mass exceed certain spatial and temporal limits relative to the base of support, whereby a fall becomes imminent without further action (44, 45). For this article and from a functional standpoint, we use the term balance as an umbrella term for all mechanisms and skills contributing to the maintenance of stability, with the term stability referring to the outcome or state (e.g., mechanically stable/unstable, fall/no fall).
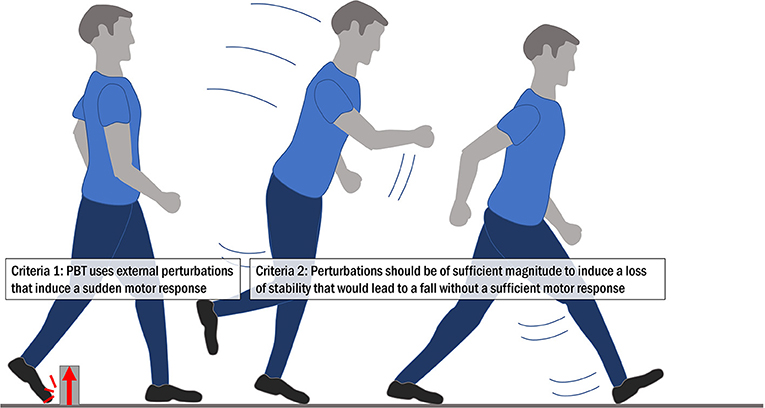
Figure 1. The two key criteria for perturbation-based balance training.
Our criteria for defining training as PBT, described in What is PBT?, specify that the training should use external perturbations that induce a sudden response and that are of sufficient magnitude to induce a loss of stability. In other words, if the perturbations used do not, (a) require a sudden response to compensate for the disturbance or, (b) lead to a loss of stability, we contend they are not sufficiently similar to the common causes of falls in daily life and are therefore, not task specific. For example, “internal perturbations” or instability induced by narrowing one's base of support or standing on an unstable wobbly surface are not considered PBT. A second consideration is that the method of perturbation delivery should be similar to common perturbations experienced in daily life. In this regard, pop-up obstacles on a walkway [like those used by Pavol et al. (46), Pavol et al. (47), Pijnappels et al. (48), Pijnappels et al. (49), Pijnappels et al. (50), Okubo et al. (51), Okubo et al. (52)] more closely simulate real life trips than a treadmill belt acceleration or deceleration [like those used by Sessoms et al. (53), Owings et al. (54), Grabiner et al. (55), McCrum et al. (56), for example], with cable-trip systems [e.g., as in Senden et al. (57), McCrum et al. (58) or Epro et al. (59)] lying in-between. While some studies suggest that the kinematics of the recovery actions triggered by treadmill-delivered perturbations are similar to more ecologically valid perturbations (53, 54), another study that directly compared treadmill belt accelerations with obstacle-induced trips while walking reported significant differences in trunk and stepping kinematics and their adaptations (60). As discussed in sections How does PBT lead to the retention and generalization of fall-resisting skills? and What technology is required for PBT?, the degree of similarity between the training and real-life trips and slips may have implications for the generalizability of PBT training approaches.
A third aspect of task specificity relates to whether perturbations are applied during standing, walking or other common movements (i.e., sit-to-stand transitions). As most falls in community-dwelling older adults occur during walking (1–6, 8, 61), this may be the most relevant task for PBT training for this group. However, frail older people, such as those living in residential care facilities, often experience falls during transitions (62–65), thus may benefit from standing and sit-to-stand perturbation training. Finally, due to the task-specific nature of PBT, training benefits may be restricted to improvements in dynamic and perturbed balance tasks with little or no transfer to less dynamic / static balance tasks (66–68). Some examples of various task-specific elements to consider are shown in Figure 2.
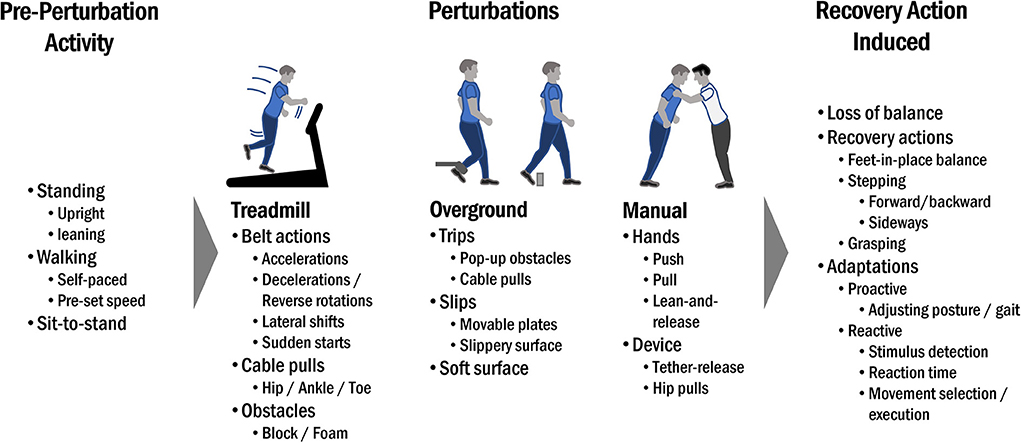
Figure 2. Examples of various task-specific elements to consider in PBT.
Task-specific walking or balance training, even in the narrowed context of fall prevention, may take many forms. In addition to PBT these include: volitional step training with responses to various stepping targets, cues and constraints [for a review see: Okubo et al. (32)]; gait adaptability training using virtual or real obstacles [for example tasks see Geerse et al. (69) or Timmermans et al. (70)]; adapted forms of agility training [e.g., Donath et al. (71) and Lichtenstein et al. (72)]; and training with ongoing disturbances, simulating situations like uneven ground (73–75). Our criteria for PBT described above, however, distinguish PBT from these complementary approaches, in that regardless of how the perturbation is delivered (trip, slip, push, pull, to the trunk, to the foot, etc.), the participant must quickly identify and respond to a ‘sudden' perturbation. In contrast, in the other approaches, changes in the environment can be perceived prior to contact or the response is to a cue separate from a loss of stability. During PBT, the “cue” is destabilization, detected by the sensory systems, which triggers rapid stability-recovery responses. PBT facilitates sensorimotor adaptations in these stability-recovery responses through trial-and-error practice. Coupled with the criteria that PBT triggers a sudden response is the requirement that the perturbation causes a loss of stability. This element is conceptually similar to the definition of “challenging balance training” in previous reviews [e.g., balance training including two or three of the following criteria: movement of the center of mass; narrowing of the base of support; minimizing upper limb support (76)]. However, during PBT, usually conducted with a safety harness, participants' stability can and should be further challenged so that destabilization always occurs. This is also distinct from volitional step training and gait adaptability training, where appropriate stepping behavior to avoid stability loss is trained. Practically, in PBT, this sudden response following a loss of stability during standing or walking usually manifests as reactive stepping or reaching (when an appropriate support is available), as described by Maki and McIlroy (77) as a change-in-support strategy. If participants cannot retain their stability following a perturbation, they are caught by a safety harness or therapist. Such events form part of the sensorimotor skill learning, although whether complete recovery failure is necessary for successful intervention is currently unclear. There are also practical considerations that may affect how perturbation intensities leading to these failures are administered. These issues are addressed in sections What is the dose-response relationship for PBT?, How can anxiety be alleviated during PBT? and What is the evidence for PBT in clinical populations. Finally, while muscle strength training can't be considered a task-specific fall prevention intervention, strength training targeting functionally relevant muscle groups and actions could potentially be used in conjunction with PBT. One RCT (35) reported that PBT combined with hip muscle strengthening may further improve stepping performance and reduce daily life falls compared to PBT alone or strength training alone. This may suggest possible synergistic benefits of using PBT and targeted strengthening approaches. However, another study found no synergistic effects of PBT and training of plantar flexor muscles stability following trip perturbations (59), thus further investigation into such combined approaches is required.
Early research demonstrated that a single session of repeated-perturbations (such as slip- or trip-like perturbations) results in acquisition of fall-resisting skills through implicit learning (without instruction) (78–81) across age-groups (young and old) (78) and tasks (standing, sit-to-stand transitions and walking) (82). In such single training sessions, the reduction of “in-task” falls can occur rapidly, i.e., in three–five trials (83). These improvements in recovery are associated with rapid improvements in both the feedforward/proactive control of stability (anterior shift of the center of mas) (83, 84) and the provision of proper limb support against collapse (78, 85–87), reflected in the form of improved recovery stepping responses, both during stance and walking perturbations. Depending on the perturbation type, the control of stability and limb support is achieved via changes in kinematic parameters such as recovery step length, trunk angle and velocity resulting from changes in neuromuscular output (88–90).
Motor adaptations, like those induced by PBT, may be predictive or reactive in nature (91–94). Predictive adaptation to a perturbation utilizes prior experience and knowledge of the upcoming perturbation in a feedforward manner to proactively adjust locomotor control and output (e.g., modifications of the base of support and/or center of mass position). Predictive adaptation can reduce the impact of a perturbation, reducing the magnitude of the required balance recovery response (95). Reactive adaptation, conversely, is a change in the motor responses to an unexpected perturbation. Reactive adaptation can manifest as: earlier detection of the perturbation or stability loss and faster stability recovery initiation (96, 97); optimization of motor programmes for stability recovery including facilitation and suppression of functionally relevant and irrelevant reflexes and reactions, respectively (98–100); and altered coordination in skeletal (especially weight bearing) muscles for rapid motor actions (18, 88, 94, 101–103). As discussed in section How does PBT differ from other task-specific approaches to fall prevention?, only PBT aims to improve the reactive stability recovery responses to destabilizing perturbations, as opposed to other task-specific approaches (e.g., gait adaptability training) that target predictive adaptations only. However, predictive adaptation, to some extent, is likely inherent in most PBT programmes (92). As such, PBT programmes should consider, and possibly monitor and account for, the role and influence of predictive adaptation, since it might reduce the impact of the administered perturbations and reduce generalization effects (31, 104, 105). Indeed, it has been demonstrated that perturbation impact might be significantly reduced if participants are aware they might encounter an unspecified hazard that may perturb their balance (105–107). Okubo et al. (108) also found that predictive adaptations are less readily observed when perturbation type, location and timing are unpredictable. However, other studies have shown that awareness of upcoming perturbations (109) or even observation training (watching videos of the perturbation task) (110) can lead to predictive adaptations but their effects were not comparable with those from actual physical experience of the perturbations.
Promising results from early studies using overground slip perturbation training revealed that the skills acquired during a single repeated-slip training session can be retained for up to a year by developing protocols incorporating random practice [contextual interference (111–113)] and overlearning [continued task practice after reaching a success criterion (114–116)] via high intensity training (24 repeated slips) among healthy (young and older) adults (86, 117). Several other studies have subsequently shown good retention after exposure to repeated perturbations in healthy young adults (84, 86, 118, 119), older adults (59, 119), people with stroke (120–123) and Parkinson's disease (124–126). In terms of training dose, studies have included single sessions (117–119, 124, 127) and multiple sessions (59, 122, 123, 128) and retention intervals from as short as 30 min to up to 1.5 years post intervention.
A vital function of the central nervous system is its ability to apply motor adaptations obtained in one situation to a different situation. The central nervous system can generalize response adaptations to similar perturbations to an untrained limb (56, 129–131); untrained tasks [e.g., gait-slip to sit-to-stand slip (82)]; untrained contexts [e.g., moveable platform to vinyl floor (132–135)]; and to different perturbation types [slips to trips (136) and waist pull perturbations to treadmill slips (137), though minor interference has also been reported (81, 136)]. Generalization between contexts (treadmill to overground slips) may also be retained over longer periods (138). Based on evidence from locomotor training studies it is postulated that when an acquired internal representation is more general (i.e., not specific to certain effectors, environments or tasks) more motor transfer will ensue (139–143). This postulation seems applicable for PBT as well for fall prevention.
In summary, most reports indicate a positive transfer of adaptations between different conditions of the same perturbation, i.e., from treadmill gait-slips to a ‘novel' overground slip, or from training gait-slips on a moveable platform to an untrained slip on an oily surface (97, 133, 135, 144–146). However, several recent investigations have shown that improved balance skills resulting from repeated exposure to trip-like perturbations does not transfer to the recovery response to a similar large mechanical perturbation in the anterior direction (60, 119, 147). Critical components in neuromotor control (e.g., module composition and time-coordinated recruitment of motor modules) due to different neuromechanical task constraints (e.g., muscle activity patterns and body dynamics) may discriminate between perturbation types, possibly explaining the discrepancy between findings for generalization of adaptations from repeated gait perturbation exposure. Thus, although generalization is possible within the human stability control system, it may require a certain degree of similarity, if not consistency, between tasks which may be determined by factors other than shared limb mechanics. A recent study investigated potential factors limiting inter-task generalization within the stability control system (147). Differences were detected in the synergistic spatiotemporal organization of muscle activations indicating a diverging modular response to different perturbations, seemingly covered by the same main balance skill (i.e., rapid stepping). Hence, it may be argued that the transfer of adaptations in stability control between different balance tasks may be influenced by differences in muscle synergies in the perturbation recovery responses. Thus, while generalization of adaptation is in principle possible within the human stability control system, it seems limited if neuromotor factors discriminate perturbation responses in different motor tasks e.g., discrepancies in the spatiotemporal organization of the motor system between balance tasks (147).
For a training protocol to be clinically accepted and implemented, the training dose-response relationship in addition to the training effect needs to be established (21, 148). A training dose can be varied by altering the intensity of the perturbation (making it more challenging), the amount of practice per session (increasing the number of perturbations) or the number of training sessions provided (148, 149).
For overground slip perturbations, earlier studies showed that a high practice dose (in terms of intensity) provided in a single session led to significant retention over the longer-term (4-6 months) (117, 128). Increasing the session frequency in terms of providing a booster dose did not lead to greater retention in younger adults (86, 150) but did so in older adults (128). However, increasing intensity, frequency and duration of such protocols could also have disadvantages such as activity-induced fatigue and reduced participation, particularly in certain clinical populations with significant health issues and balance impairments (151, 152). Another alternative for those unable to tolerate a high dose within a single session is to provide more sessions with fewer training trials or min per session (152). For example, studies have shown that a single slip exposure administered in separate, frequent sessions can induce lasting effects within the same environment (i.e., laboratory) (80, 150). No studies have examined dose effects for overground trip perturbations (148).
Several studies involving young adults, older adults and people with stroke have used different practice durations per session and number of sessions in their studies using treadmill belt perturbations. The number of trials per session have ranged from 11 to 80 and number of sessions have ranged from 1 to 24 (144, 145, 149, 153, 154). Retention periods have ranged from 30 min (144, 153, 155) to 6 months (138, 154).
There is a clear need for further dose-response studies (in particular, for the more clinically applicable treadmill-based protocols) to examine retention and generalization of the adaptations made, as the optimal dose for within-session or within-training programme adaptation may not necessarily be the same as the optimal dose for long term retention and generalization. Further, most studies have used only a single type of perturbation direction which may result in the limited real-life generalization observed. More studies are needed to examine the effect of bidirectional or multidirectional perturbation training on longer-term retention and generalization. Lastly, the type of perturbation training that yields maximum efficacy also remains unknown. These gaps are important to fill to provide recommendations to clinicians and develop clinical practice guidelines.
PBT requires additional safety measures compared to conventional balance training. In this regard, safety harnesses are often used when administering large external perturbations. The benefit of a safety harness is that the participant can move in an almost unrestricted manner, and the therapist can focus on training delivery, with the assurance that any unsuccessful balance recovery will be safely arrested by the harness. Many different options are available, ranging from a fixed harness which can be attached to the ceiling in the middle of the exercise room or above a treadmill, or ceiling rail system harnesses which enable the wearer to move freely through a room. A portable/movable support frame is another option if appropriately certified for supporting a participant's body weight and does not interfere with reactive stepping responses. Harnesses also need to be well-fitted and comfortable to prevent harness-induced bruising and soreness after training.
Few adverse events from PBT training have been reported in the literature. Most studies report no or relatively minor adverse events such as soreness at the contact points between the body and the harness or muscle soreness (156–160). In 12 RCTs (20, 36, 52, 97, 122, 159, 161–165) summarized by Mansfield et al. (166), pain and delayed onset muscle soreness were the most commonly reported adverse events (16.4% of participants), with no severe adverse events reported in these trials. One other study reported 6 mild to moderate adverse events related to lateral waist-pull perturbations, including knee pain and groin injury, although the authors stated that this perturbation approach was generally well tolerated by the participants (35). Muscle soreness during or after training cannot be entirely prevented but may be decreased by adjusting training intensity for each individual. If an individual experiences a fall into the safety harness, follow-up assistance is often required to help them regain their stability and composure.
When working with less intensive external perturbations, such as therapist-applied perturbations, training is possible without additional safety equipment. However, it is crucial that both the therapist and patient know their limits and having a second therapist present to provide stability support is advised. Transfer belts can also assist the therapist apply perturbations as well as support their patients as required.
Anxiety and fear about upcoming perturbations and/or falling is a practical challenge in PBT (167). In their overview of 12 RCTs of PBT, Mansfield et al. (166) noted that about 5% of the included participants reported PBT-related fear or anxiety (some of which withdrew for this reason) and a more recent meta-analysis confirms that anxiety and fear occur more frequently in PBT than in control interventions (33). Anxiety during training is higher in older adults compared to younger adults and increases with greater uncertainty about the upcoming perturbations (51). In one study, older adults reported higher anxiety during PBT on a treadmill compared to PBT on an overground walkway (60). The authors suggest that this higher anxiety may have been due to unfamiliarity with treadmill walking and the elevated surface of the treadmill. Anxiety is higher in those with poor reactive balance, but heightened anxiety can also impair reactive balance control via delayed, more rigid and/or (poorly adapted) startle responses (168–170), and thus should be minimized for a better training outcome. Monitoring of anxiety levels using a custom 5-point scale and adjustments of training intensity (e.g., 5–10% reduction in gait speed) have been effective in easing anxiety during reactive balance training using overground trips and slips (52). Interviews with participants who underwent PBT using an instrumented treadmill system (171) revealed that while some participants experienced anxiety during training, most described feeling a “good kind of nervousness” during training, rather than anxiety. Participants that reported being initially anxious often found that their anxiety diminished or resolved after the first training session when they had experienced PBT and were confident they could recover from the perturbations, a finding also reported by Jagroop et al. (167). The presence of safety equipment (especially a safety harness), and ensuring participants are heard and informed during the training sessions have been identified as important factors that mitigate anxiety (171). In cases where sufficiently large destabilizing perturbations increase anxiety and possibly prompt withdrawal, it may be prudent to administer training intensities that are less threatening until anxiety is reduced. This may reduce the effectiveness of the initial training period and may not qualify as PBT as per our definition but may retain patients in training and allow them to become more comfortable with the training regime and take part in higher intensity PBT in subsequent trials. Uncertainty about the timing, location, type or direction of perturbations (in situations in which these are modifiable options) can also be gradually increased congruent with the comfort and performance levels of participants.
To date, PBT has been studied primarily in healthy community-dwelling older adults. However, there is also emerging evidence for the effectiveness of PBT in ‘high risk' older adults (for example assisted living residents, or older adults with a history of falls or balance problems), and people with Parkinson's disease, stroke and multiple sclerosis (121–123, 156, 158, 159, 172–176). PBT trials have also been conducted in people with chronic obstructive pulmonary disorder (152) and incomplete spinal cord injury (165), but due to limited findings will not be discussed in detail in this article. Previous reviews (29, 30) showed significant fall reductions in community-dwelling older adults, frail/high-risk older adults and people with Parkinson's disease and stroke following PBT. PBT has also been found to improve perturbation recovery measures (156, 159, 160, 177) and some studies have reported improvements in clinical balance tests such as the Berg Balance Scale in people with Parkinson's disease (173, 174, 178). However, while there appears to be interest in the potential for PBT to improve a broad range of gait and balance measures in clinical populations [see reviews of Hulzinga et al. (179), Coelho et al. (180)], as outlined in section What is task-specificity in the context of PBT? and How does PBT differ from other task-specific approaches to fall prevention?, the effects do not necessarily generalize to less-reactive balance and gait measures. To our knowledge, no current studies in clinical populations have reported non-responders in terms of adaptation of the stability recovery response to PBT. However, on an individual level, those who cannot tolerate being exposed to perturbations (due to, for example, anxiety or pain) may not be able to benefit from PBT immediately, and perhaps initially require more basic balance training.
There are some important factors to consider before applying PBT in less able populations. First, decreasing training intensity to an acceptable level for the participant may mean that the total training volume is increased to compensate. Second, frailer people may require a walking aid in daily life. To our knowledge, no studies have focused on the feasibility of using walking aids during PBT, but we hypothesize that the use of a full-body harness with partial bodyweight support may enable PBT for these people. Future studies may focus on this gap in knowledge.
Several mechanical perturbation systems can evoke the balance disturbances required for PBT and trigger error-driven motor learning in the control of postural balance. As there is a growing body of evidence suggesting both the efficacy and efficiency of PBT for improving fall resisting skills, there is also a need to further develop devices which are capable of mimicking disturbances experienced during daily-life mobility in clinical settings.
An ideal system for training reactive balance recovery should be capable of applying unpredictable mechanical perturbations of different magnitudes and directions and/or types at pre-specified timepoints that elicit a loss of balance and thus mimic near-fall situations in a safe, controllable environment (31, 181, 182). This system should also be able to measure the participant's stability and stability recovery to facilitate assessment and personalized training.
Several perturbation systems have been used to disturb stability during walking, including floor obstacles in both overground (46, 51, 113, 183–186) and treadmill setups (181, 187), unexpected surface compliance changes [overground; (188)], overground slips or surface translations (133, 189, 190), cable or rope trips both in overground (191, 192) and treadmill setups (57, 88, 193–196), as well treadmill-based belt speed changes (53, 55, 61, 118, 197–199), platform translations or tilts (200) and waist/torso pushes and pulls (137, 201–204). Several commercially available systems are also available (e.g., BalanceTutor, ActiveStep, C-Mill React). It is important to highlight that no system is without its limitations. For example, overground setups suffer from the limitation of limited walkway length and that the location of the perturbations may not be entirely unpredictable (31), though this limitation can be, at least partly, addressed by including multiple possible perturbation locations [see, for example, (108)]. The obvious advantage of the treadmill in comparison to such overground setups is that predicting when a perturbation will be applied is more difficult, as there is no location-based reference point (31), which ensures that predictive adjustments in in anticipation of perturbations are reduced [though not necessarily completely absent (123, 155)]. However, walking on a treadmill can provide additional challenges in some populations at increased fall risk, due to lack of familiarity and the requirement to maintain a specific speed [walking speed can be instantaneously adjusted in an overground setup but maintaining it provides an additional challenge during perturbed treadmill walking (205)]. Another inherent limitation in some setups is that the perturbations themselves may not strictly mimic common causes of falls like slips and trips (60) despite the subsequent recovery mechanics being suggested to be similar (53, 54) (see also Figure 2 in section What is task-specificity in the context of PBT?). A recent study reported that adaptations observed with repeated treadmill belt accelerations did not transfer to obstacle-induced trips while walking (60). However, it is not currently known if and how this affects transfer to daily life situations. Another factor that should be considered is the ease with which PBT dose can be altered. The number of perturbations and training sessions can be easily manipulated but not all systems can provide a wide range of perturbation magnitudes which is critical to ensure that participants are safely and sufficiently destabilized, even late in their training. This is of particular relevance for the conceptualization of fall prevention interventions in clinical settings because the hypothesis of a non-linear dose-response relationship (148) implies that adaptation may not be directly related to the applied practice dose and that a dose threshold exists beyond which any additional stimuli may not induce further changes.
In summary, based on current evidence, we believe that the primary factors for a successful PBT system are that it can; (a) administer perturbations that are difficult for participants to predict (in time of onset but perhaps also in body location, mode or magnitude of application); (b) suddenly destabilize participants with these perturbations; and (c) easily adjust the magnitude of perturbations.
Despite the potential advantage of using such systems to destabilize participants and create near fall situations, the costs associated with the equipment, as well as the expertise required to operate PBT systems may hinder their application in clinical settings. Thus, there is a need to develop alternative, feasible PBT programmes that do not require these devices. Therapist-applied perturbations, as described above, are the natural alternative and can be easily applied if appropriate safety measures are followed. However, managing the training and perturbation dosage may be problematic due to the perturbations being more predictable and the intensity of therapist-applied perturbations being less precise. Such limitations, however, do not discount the potential effectiveness of this approach when they constitute the only feasible option in at least the short term. For a useful resource on the therapist-applied perturbation approach, we refer readers to Mansfield et al. (166).
The application of PBT in home or group settings has been little investigated to date. Clearly, it is not safe to apply large external perturbations, with the possibility of an unsuccessful balance recovery in the absence of a safety harness. Smaller perturbations however, such as therapist-applied perturbations, may be applied in home and group settings. For example, Oddsson et al. (17) successfully applied perturbations in a group setting through training in couples with partner or therapist-applied perturbations.
As discussed above, it is crucial the participant feels safe during training, and everyone involved know their limits. Portable safety equipment, such as a transfer belts, can assist the therapist apply the perturbations as well as support patients during training. However, if an appropriate training stimulus cannot be reached this way, transferring the training to a one-on-one basis, or using more specific equipment should be considered. Future studies are necessary to elucidate the feasibility of PBT in a group or semi-supervised setting.
Taking the previous sections into account, several recommendations for both research and clinical application of perturbation-based balance training can be made.
Studies are required to:
• Determine optimal training doses and the potential effects of repeated training or booster sessions.
• Identify the relative contribution of different aspects of training dose (e.g., perturbation impact, perturbation training intensity (displacement, velocity, acceleration settings), perturbation number, training session number) to the training effects.
• Compare the effects of different laboratory-based PBT methods with respect to stability outcomes and daily life fall prevention.
• Further elucidate and compare the criteria by which adaptations gained by training one type of perturbation transfer to other similar perturbations (e.g., between legs, a movable plate to a slippery floor; see How does PBT lead to the retention and generalization of fall-resisting skills? above).
There is a need to:
• Develop effective, affordable and clinically feasible methods for applying perturbations.
• Conduct feasibility studies to explore opportunities and barriers for implementation.
• Determine strategies to alleviate anxiety in participants undertaking PBT to ensure clinical feasibility.
• Identify which clinical populations with balance impairment benefit from PBT
• Elucidate PBT dose-response relationships in these populations.
Finally, it is worth highlighting that there have been only a few randomized controlled trials with sample sizes large enough to have statistical power to evaluate the role of PBT in reducing daily life falls. Lurie et al. (34) with their multicenter pragmatic (non-standardized protocol based on therapist judgement) trial is the largest. This 12-month trial included 187 participants (of 253 allocated) who received PBT and 190 (of 253 allocated) participants who received standard balance training. Once some of the issues relating to training and practice mentioned above have been further elucidated, we recommend large, definitive trials following CONSORT guidelines are conducted. In the meantime, we recommend that studies on PBT collect and report prospective falls data as secondary outcomes to assist future meta-analyses. Template forms for collecting falls information following recommendations by Lamb et al. (206) and Lord et al. (207) can be downloaded at http://doi.org/10.17605/OSF.IO/HMJEF (208).
Perturbation-based balance training is a promising approach to fall prevention. This task-specific training of balance using repeated exposure to sudden perturbations may present a paradigm shifting approach that may improve effectiveness and efficiency of a fall prevention exercise intervention. However, several fundamental and applied aspects of the approach need to be further investigated before this approach can be widely implemented in clinical practice.
CM and YO: conceptualization, project administration, writing-original draft, and writing-review and editing. TB, MG, and KK: writing-original draft and writing-review and editing. MR: writing-review and editing. SL: conceptualization and writing-review and editing. All authors contributed to the article and approved the submitted version.
A preprint version of this work is available at OSF Preprints (209).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sheldon JH. On the Natural History of Falls in Old Age. BMJ. (1960) 2:1685–90. doi: 10.1136/bmj.2.5214.1685
2. Tinetti ME, Speechley M, and Ginter SF. Risk factors for falls among elderly persons living in the community. N Engl J Med. (1988) 319:1701-7. doi: 10.1056/NEJM198812293192604
3. Lord SR, Ward JA, Williams P, and Anstey KJ. An epidemiological study of falls in older community-dwelling women: the Randwick falls and fractures study. Aust J Public Health. (1993) 17:240–5. doi: 10.1111/j.1753-6405.1993.tb00143.x
4. Berg WP, Alessio HM, Mills EM, and Tong C. Circumstances and consequences of falls in independent community-dwelling older adults. Age Ageing. (1997) 26, 261–8. doi: 10.1093/ageing/26.4.261
5. Talbot LA, Musiol RJ, Witham EK, and Metter EJ. Falls in young, middle-aged and older community dwelling adults: perceived cause, environmental factors and injury. BMC Public Health. (2005) 5:86. doi: 10.1186/1471-2458-5-86
6. Crenshaw JR, Bernhardt KA, Achenbach SJ, Atkinson EJ, Khosla S, and Kaufman KR„ et al. The circumstances, orientations, and impact locations of falls in community-dwelling older women. Arch Gerontol Geriatr. (2017) 73:240–7. doi: 10.1016/j.archger.2017.07.011
7. Mccrum C. A Trip to Remember: Assessing and Improving Walking Stability in Older Adults. Maastricht University. (2019). doi: 10.26481/dis.20191219cm
8. Niino N, Tsuzuku S, Ando F, and Shimokata H. Frequencies and circumstances of falls in the National Institute for Longevity Sciences, Longitudinal Study of Aging (NILS-LSA). J Epidemiol. (2000) 10(1 Supp):90-4. doi: 10.2188/jea.10.1sup_90
9. Cameron ID, Dyer SM, Panagoda CE, Murray GR, Hill KD, Cumming RG, et al. Interventions for preventing falls in older people in care facilities and hospitals. Cochrane Database Syst Rev. (2018) 389. doi: 10.1002/14651858.CD005465.pub4
10. Hopewell S, Adedire O, Copsey BJ, Boniface GJ, Sherrington C, Clemson L, et al. Multifactorial and multiple component interventions for preventing falls in older people living in the community. Cochrane Database Syst Rev. (2018) 311. doi: 10.1002/14651858.CD012221.pub2
11. Williams AD, Bird ML, Hardcastle SG, Kirschbaum M, Ogden KJ, and Walters JA. Exercise for reducing falls in people living with and beyond cancer. Cochrane Database Syst Rev. (2018) 68. doi: 10.1002/14651858.CD011687.pub2
12. Denissen S, Staring W, Kunkel D, Pickering RM, Lennon S, and Geurts AC. Interventions for preventing falls in people after stroke. Cochrane Database Syst Rev. (2019) 68. doi: 10.1002/14651858.CD008728.pub3
13. Sherrington C, Fairhall NJ, Wallbank GK, Tiedemann A, Michaleff ZA, Howard K, et al. Exercise for preventing falls in older people living in the community. Cochrane Database Syst Rev. (2019) 587. doi: 10.1002/14651858.CD012424.pub2
14. Allen NE, Canning CG, Almeida LR, Bloem BR, Keus SH, Löfgren N, et al. Interventions for preventing falls in Parkinson's disease. Cochrane Database Syst Rev. (2022) 6:Cd011574. doi: 10.1002/14651858.CD011574.pub2
15. Hamed A, Bohm S, Mersmann F, and Arampatzis A. Follow-up efficacy of physical exercise interventions on fall incidence and fall risk in healthy older adults: a systematic review and meta-analysis. Sports Med-Open. (2018) 4:19. doi: 10.1186/s40798-018-0170-z
16. Sibley KM, Thomas SM, Veroniki AA, Rodrigues M, Hamid JS, Lachance CC, et al. Comparative effectiveness of exercise interventions for preventing falls in older adults: a secondary analysis of a systematic review with network meta-analysis. Exp Gerontol. (2021) 143:111151. doi: 10.1016/j.exger.2020.111151
17. Oddsson LI, Boissy P, and Melzer I. How to improve gait and balance function in elderly individuals—compliance with principles of training. Eur Rev Aging Phys Act. (2007) 4:15–23. doi: 10.1007/s11556-007-0019-9
18. Pai YC, and Bhatt TS. Repeated-slip training: an emerging paradigm for prevention of slip-related falls among older adults. Phys Ther. (2007) 87:1478–91. doi: 10.2522/ptj.20060326
19. Grabiner MD, Donovan S, Bareither ML, Marone JR, Hamstra-Wright K, Gatts S, et al. Trunk kinematics and fall risk of older adults: translating biomechanical results to the clinic. J Electromyogr Kinesiol. (2008) 18:197–204. doi: 10.1016/j.jelekin.2007.06.009
20. Maki BE, Cheng KC, Mansfield A, Scovil CY, Perry SD, Peters AL, et al. Preventing falls in older adults: new interventions to promote more effective change-in-support balance reactions. J Electromyogr Kinesiol. (2008) 18:243–54. doi: 10.1016/j.jelekin.2007.06.005
21. Grabiner M. D., Crenshaw J. R., Hurt C. P., Rosenblatt N. J., and Troy K. L. (2014). Exercise-based fall prevention: can you be a bit more specific? Exerc Sport Sci Rev 42, 161–168. doi: 10.1249/JES.0000000000000023
22. McCrum C. Falls among older people-are intervention duration and specificity the keys to making a difference? BMJ. (2018) 361:1. doi: 10.1136/bmj.k2213
23. McCrum C. Fall prevention in community-dwelling older adults. N Engl J Med. (2020) 382:2579–80. doi: 10.1056/NEJMc2005662
24. Tang PF, and Woollacott MH. Balance Control in Older Adults: Training Effects on Balance Control and the Integration of Balance Control into Walking. In:Ferrandez A-M., and Teasdale N. (eds.) Advances in Psychology. North-Holland (1996). doi: 10.1016/S0166-4115(96)80015-X
25. Mansfield A, Peters AL, Liu BA, and Maki BE. A perturbation-based balance training program for older adults: study protocol for a randomised controlled trial. BMC Geriatr. (2007) 7:12. doi: 10.1186/1471-2318-7-12
26. Rosenblatt NJ, Marone J, and Grabiner MD. Preventing trip-related falls by community-dwelling adults: a prospective study. J Am Geriatr Soc. (2013) 61:629–31. doi: 10.1111/jgs.12428
27. Pai YC, Bhatt T, Yang F, Wang E, and Kritchevsky S. Perturbation training can reduce community-dwelling older adults' annual fall risk: a randomized controlled trial. J Gerontol A Biol Sci Med Sci. (2014) 69:1586–94. doi: 10.1093/gerona/glu087
28. Lurie JD, Zagaria AB, Ellis L, Pidgeon D, Gill-Body KM, and Burke C. Pilot comparative effectiveness study of surface perturbation treadmill training to prevent falls in older adults. BMC Geriatr. (2013) 13:49. doi: 10.1186/1471-2318-13-49
29. Mansfield A, Wong JS, Bryce J, Knorr S, and Patterson KK. Does perturbation-based balance training prevent falls? Systematic review and meta-analysis of preliminary randomized controlled trials. Phys Ther. (2015) 95:700–9. doi: 10.2522/ptj.20140090
30. Gerards MH, McCrum C, Mansfield A, and Meijer K. Perturbation-based balance training for falls reduction among older adults: current evidence and implications for clinical practice. Geriatr Gerontol Int. (2017) 17:2294–303. doi: 10.1111/ggi.13082
31. McCrum C, Gerards MH, Karamanidis K, Zijlstra W, and Meijer K. A systematic review of gait perturbation paradigms for improving reactive stepping responses and falls risk among healthy older adults. Eur Rev Aging Phys Act. (2017) 14:3. doi: 10.1186/s11556-017-0173-7
32. Okubo Y, Schoene D, and Lord SR. Step training improves reaction time, gait and balance and reduces falls in older people: a systematic review and meta-analysis. Br J Sports Med. (2017) 51:586–93. doi: 10.1136/bjsports-2015-095452
33. Devasahayam AJ, Farwell K, Lim B, Morton A, Fleming N, Jagroop D, et al. The effect of reactive balance training on falls in daily life: an updated systematic review and meta-analysis. medRxiv. Preprint. (2022). doi: 10.1101/2022.01.27.22269969
34. Lurie JD, Zagaria AB, Ellis L, Pidgeon D, Gill-Body KM, Burke C, et al. Surface perturbation training to prevent falls in older adults: a highly pragmatic, randomized controlled trial. Phys Ther. (2020) 100:1153-62. doi: 10.1093/ptj/pzaa023
35. Rogers MW, Creath RA, Gray V, Abarro J, McCombe Waller S, Beamer BA, et al. Comparison of lateral perturbation-induced step training and hip muscle strengthening exercise on balance and falls in community-dwelling older adults: a blinded randomized controlled trial. J Gerontol A Biol Sci Med Sci. (2021) 76:e194-202. doi: 10.1093/gerona/glab017
36. Mansfield A, Aqui A, Danells CJ, Knorr S, Centen A, DePaul VG, et al. Does perturbation-based balance training prevent falls among individuals with chronic stroke? A randomised controlled trial. BMJ Open. (2018) 8:e021510. doi: 10.1136/bmjopen-2018-021510
37. Barzideh A, Marzolini S, Danells C, Jagroop D, Huntley AH, Inness EL, et al. Effect of reactive balance training on physical fitness poststroke: study protocol for a randomised non-inferiority trial. BMJ Open. (2020) 10:e035740. doi: 10.1136/bmjopen-2019-035740
38. Mansfield A, Inness EL, Danells CJ, Jagroop D, Bhatt T, and Huntley AH. Determining the optimal dose of reactive balance training after stroke: study protocol for a pilot randomised controlled trial. BMJ Open. (2020) 10:e038073. doi: 10.1136/bmjopen-2020-038073
39. Rieger MM, Papegaaij S, Steenbrink F, Van Dieën JH, and Pijnappels M. Perturbation-based gait training to improve daily life gait stability in older adults at risk of falling: protocol for the REACT randomized controlled trial. BMC Geriatr. (2020) 20:167. doi: 10.1186/s12877-020-01566-z
40. Gerards MH, Marcellis RG, Poeze M, Lenssen AF, Meijer K, and de Bie RA. Perturbation-based balance training to improve balance control and reduce falls in older adults - study protocol for a randomized controlled trial. BMC Geriatr. (2021) 21:9. doi: 10.1186/s12877-020-01944-7
41. Nørgaard JE, Andersen S, Ryg J, Stevenson AJT, Andreasan J, Danielsen MB, et al. Effects of treadmill slip and trip perturbation-based balance training on falls in community-dwelling older adults (STABILITY): study protocol for a randomised controlled trial. BMJ Open. (2022) 12:e052492. doi: 10.1136/bmjopen-2021-052492
42. Sibley KM, Inness EL, Straus SE, Salbach NM, and Jaglal SB. Clinical assessment of reactive postural control among physiotherapists in Ontario, Canada. Gait Posture. (2013) 38:1026–31. doi: 10.1016/j.gaitpost.2013.05.016
43. Mansfield A, Danells CJ, Inness EL, Musselman K, and Salbach NM. A survey of Canadian healthcare professionals' practices regarding reactive balance training. Physiother Theory Pract. (2019) 37:787–80. doi: 10.1080/09593985.2019.1650856
44. Pai YC, and Patton J. Center of mass velocity-position predictions for balance control. J Biomech. (1997) 30:347–54. doi: 10.1016/S0021-9290(96)00165-0
45. Hof AL, Gazendam MG, and Sinke WE. The condition for dynamic stability. J Biomech. (2005) 38:1–8. doi: 10.1016/j.jbiomech.2004.03.025
46. Pavol MJ, Owings TM, Foley KT, and Grabiner MD. Mechanisms leading to a fall from an induced trip in healthy older adults. J Gerontol A Biol Sci Med Sci. (2001) 56:M428–37. doi: 10.1093/gerona/56.7.M428
47. Pavol MJ, Owings TM, Foley KT, and Grabiner MD. Influence of lower extremity strength of healthy older adults on the outcome of an induced trip. J Am Geriatr Soc. (2002) 50:256–62. doi: 10.1046/j.1532-5415.2002.50056.x
48. Pijnappels M, Bobbert MF, and van Dieën JH. Push-off reactions in recovery after tripping discriminate young subjects, older non-fallers and older fallers. Gait Posture. (2005) 21:388–94. doi: 10.1016/j.gaitpost.2004.04.009
49. Pijnappels M, Bobbert MF, and van Dieën JH. How early reactions in the support limb contribute to balance recovery after tripping. J Biomech. (2005) 38:627–34. doi: 10.1016/j.jbiomech.2004.03.029
50. Pijnappels M, Bobbert MF, and van Dieën JH. Control of support limb muscles in recovery after tripping in young and older subjects. Exp Brain Res. (2005) 160:326–33. doi: 10.1007/s00221-004-2014-y
51. Okubo Y, Brodie MA, Sturnieks DL, Hicks C, and Lord SR. A pilot study of reactive balance training using trips and slips with increasing unpredictability in young and older adults: Biomechanical mechanisms, falls and clinical feasibility. Clin Biomech. (2019) 67:171–9. doi: 10.1016/j.clinbiomech.2019.05.016
52. Okubo Y, Sturnieks DL, Brodie MA, Duran L, and Lord SR. Effect of reactive balance training involving repeated slips and trips on balance recovery among older adults: a blinded randomized controlled trial. J Gerontol A Biol Sci Med Sci. (2019) 74:1489–96. doi: 10.1093/gerona/glz021
53. Sessoms PH, Wyatt M, Grabiner M, Collins JD, Kingsbury T, Thesing N, et al. Method for evoking a trip-like response using a treadmill-based perturbation during locomotion. J Biomech. (2014) 47:277–80. doi: 10.1016/j.jbiomech.2013.10.035
54. Owings TM, Pavol MJ, and Grabiner MD. Mechanisms of failed recovery following postural perturbations on a motorized treadmill mimic those associated with an actual forward trip. Clin Biomech. (2001) 16:813–9. doi: 10.1016/S0268-0033(01)00077-8
55. Grabiner MD, Bareither ML, Gatts S, Marone J, and Troy KL. Task-specific training reduces trip-related fall risk in women. Med Sci Sports Exerc. (2012) 44:2410–4. doi: 10.1249/MSS.0b013e318268c89f
56. McCrum C, Karamanidis K, Grevendonk L, Zijlstra W, and Meijer K. Older adults demonstrate interlimb transfer of reactive gait adaptations to repeated unpredictable gait perturbations. GeroScience. (2020) 42:39–49. doi: 10.1007/s11357-019-00130-x
57. Senden R, Savelberg HH, Adam JJ, Grimm B, Heyligers IC, and Meijer K. The influence of age, muscle strength and speed of information processing on recovery responses to external perturbations in gait. Gait Posture. (2014) 39:513–7. doi: 10.1016/j.gaitpost.2013.08.033
58. McCrum C, Eysel-Gosepath K, Epro G, Meijer K, Savelberg HH, Brüggemann GP, et al. Associations between bipedal stance stability and locomotor stability following a trip in unilateral vestibulopathy. J Appl Biomech. (2017) 33:112–7. doi: 10.1123/jab.2016-0004
59. Epro G, Mierau A, McCrum C, Leyendecker M, Brüggemann GP, and Karamanidis K. Retention of gait stability improvements over 1.5 years in older adults: effects of perturbation exposure and triceps surae neuromuscular exercise. J Neurophysiol. (2018) 119:2229–40. doi: 10.1152/jn.00513.2017
60. Song PY, Sturnieks DL, Davis MK, Lord SR, and Okubo Y. Perturbation-based balance training using repeated trips on a walkway vs. belt accelerations on a treadmill: a cross-over randomised controlled trial in community-dwelling older adults. Front Sports Act Living. (2021) 3:702320. doi: 10.3389/fspor.2021.702320
61. McCrum C, Willems P, Karamanidis K, and Meijer K. Stability-normalised walking speed: a new approach for human gait perturbation research. J Biomech. (2019) 87:48–53. doi: 10.1016/j.jbiomech.2019.02.016
62. Robinovitch SN, Feldman F, Yang Y, Schonnop R, Leung PM, Sarraf T, et al. Video capture of the circumstances of falls in elderly people residing in long-term care: an observational study. Lancet. (2013) 381:47–54. doi: 10.1016/S0140-6736(12)61263-X
63. Robinovitch S. Ecology of falls. Handb Clin Neurol. (2018) 159:147–54. doi: 10.1016/B978-0-444-63916-5.00009-4
64. van Schooten KS, Yang Y, Feldman F, Leung M, McKay H, Sims-Gould J, et al. The association between fall frequency, injury risk, and characteristics of falls in older residents of long-term care: do recurrent fallers fall more safely? J Gerontol A Biol Sci Med Sci. (2018) 73:786–91. doi: 10.1093/gerona/glx196
65. Yang Y, van Schooten KS, Sims-Gould J, McKay HA, Feldman F, and Robinovitch SN. Sex differences in the circumstances leading to falls: evidence from real-life falls captured on video in long-term care. J Am Med Dir Assoc. (2018) 19:130–5. e1. doi: 10.1016/j.jamda.2017.08.011
66. Freyler K, Krause A, Gollhofer A, and Ritzmann R. Specific stimuli induce specific adaptations: sensorimotor training vs. reactive balance training. PLoS ONE. (2016) 11:e0167557. doi: 10.1371/journal.pone.0167557
67. Chien JE, and Hsu WL. Effects of dynamic perturbation-based training on balance control of community-dwelling older adults. Sci Rep. (2018) 8:17231. doi: 10.1038/s41598-018-35644-5
68. Krause A, Freyler K, Gollhofer A, Stocker T, Brüderlin U, and Colin R. Neuromuscular and kinematic adaptation in response to reactive balance training - A randomized controlled study regarding fall prevention. Front Physiol. (2018) 9, 1075. doi: 10.3389/fphys.2018.01075
69. Geerse DJ, Roerdink M, Marinus J, and van Hilten JJ. Walking adaptability for targeted fall-risk assessments. Gait Posture. (2019) 70:203–10. doi: 10.1016/j.gaitpost.2019.02.013
70. Timmermans C, Roerdink M, Janssen TW, Beek PJ, and Meskers CG. Automatized, standardized, and patient-tailored progressive walking-adaptability training: a proof-of-concept study. Phys Ther. (2019) 99:882–92. doi: 10.1093/ptj/pzz013
71. Donath L, van Dieën J, and Faude O. Exercise-based fall prevention in the elderly: what about agility? Sports Med. (2016) 46:143–9. doi: 10.1007/s40279-015-0389-5
72. Lichtenstein E, Morat M, Roth R, Donath L, and Faude O. Agility-based exercise training compared to traditional strength and balance training in older adults: a pilot randomized trial. PeerJ. (2020) 8:17. doi: 10.7717/peerj.8781
73. Santuz A, Ekizos A, Eckardt N, Kibele A, and Arampatzis A. Challenging human locomotion: stability and modular organisation in unsteady conditions. Sci Rep. (2018) 8:2740. doi: 10.1038/s41598-018-21018-4
74. Van Hooren B, Meijer K, and McCrum C. Attractive gait training: applying dynamical systems theory to the improvement of locomotor performance across the lifespan. Front Physiol. (2018) 9:1934. doi: 10.3389/fphys.2018.01934
75. Voloshina AS, and Ferris DP. Design and validation of an instrumented uneven terrain treadmill. J Appl Biomech. (2018) 34:236–9. doi: 10.1123/jab.2016-0322
76. Sherrington C, Tiedemann A, Fairhall N, Close JC, Lord SR, et al. Exercise to prevent falls in older adults: an updated systematic review and meta-analysis. Br J Sports Med. (2017) 51:1750–8. doi: 10.1136/bjsports-2016-096547
77. Maki BE, and Mcilroy WE. The role of limb movements in maintaining upright stance: the “change-in-support” strategy. Phys Ther. (1997) 77:488–507. doi: 10.1093/ptj/77.5.488
78. Pai YC, Bhatt T, Wang E, Espy D, and Pavol MJ. Inoculation against falls: rapid adaptation by young and older adults to slips during daily activities. Arch Phys Med Rehabil. (2010) 91:452–9. doi: 10.1016/j.apmr.2009.10.032
79. Wang TY, Bhatt T, Yang F, and Pai YC. Adaptive control reduces trip-induced forward gait instability among young adults. J Biomech. (2012) 45:1169–75. doi: 10.1016/j.jbiomech.2012.02.001
80. Liu X, Bhatt T, Wang S, Yang F, and Pai YC. Retention of the “first-trial effect” in gait-slip among community-living older adults. GeroScience. (2017) 39:93–102. doi: 10.1007/s11357-017-9963-0
81. Bhatt T, Wang Y, Wang S, and Kannan L. perturbation training for fall-risk reduction in healthy older adults: interference and generalization to opposing novel perturbations post intervention. Front Sports Act Living. (2021). 3:697169. doi: 10.3389/fspor.2021.697169
82. Wang TY, Bhatt T, Yang F, and Pai YC. Generalization of motor adaptation to repeated-slip perturbation across tasks. Neuroscience. (2011) 180:85–95. doi: 10.1016/j.neuroscience.2011.02.039
83. Bhatt T, Wening JD, and Pai YC. Adaptive control of gait stability in reducing slip-related backward loss of balance. Exp Brain Res. (2006) 170:61–73. doi: 10.1007/s00221-005-0189-5
84. Bhatt T, and Pai YC. Long-term retention of gait stability improvements. J Neurophysiol. (2005) 94:1971–9. doi: 10.1152/jn.00266.2005
85. Pavol MJ, Runtz EF, and Pai YC. Diminished stepping responses lead to a fall following a novel slip induced during a sit-to-stand. Gait Posture. (2004) 20:154–62. doi: 10.1016/j.gaitpost.2003.08.004
86. Bhatt T, Wang E, and Pai YC. Retention of adaptive control over varying intervals: prevention of slip- induced backward balance loss during gait. J Neurophysiol. (2006) 95:2913–22. doi: 10.1152/jn.01211.2005
87. Pavol MJ, and Pai YC. Deficient limb support is a major contributor to age differences in falling. J Biomech. (2007) 40:1318–25. doi: 10.1016/j.jbiomech.2006.05.016
88. Epro G, McCrum C, Mierau A, Leyendecker M, Brueggemann GP, Karamanidis K, et al. Effects of triceps surae muscle strength and tendon stiffness on the reactive dynamic stability and adaptability of older female adults during perturbed walking. J Appl Physiol. (2018) 124:1541–9. doi: 10.1152/japplphysiol.00545.2017
89. Wang S, Pai YC, and Bhatt T. Is There an optimal recovery step landing zone against slip-induced backward falls during walking? Ann Biomed Eng. (2020) 48:1768–78. doi: 10.1007/s10439-020-02482-4
90. Wang S, Wang Y, Pai YC, Wang E, and Bhatt T. Which are the key kinematic and kinetic components to distinguish recovery strategies for overground slips among community-dwelling older adults? J Appl Biomech. (2020) 36:217-27 doi: 10.1123/jab.2019-0285
91. Wolpert DM, and Miall RC. Forward models for physiological motor control. Neural Netw. (1996) 9:1265–79. doi: 10.1016/S0893-6080(96)00035-4
92. Patla AE. Strategies for dynamic stability during adaptive human locomotion. IEEE Eng Med Biol Mag. (2003) 22:48–52. doi: 10.1109/MEMB.2003.1195695
93. Shadmehr R, Smith MA, and Krakauer JW. Error correction, sensory prediction, and adaptation in motor control. Annu Rev Neurosci. (2010) 33:89–108. doi: 10.1146/annurev-neuro-060909-153135
94. Rogers MW, and Mille ML. Balance perturbations. Handb Clin Neurol. (2018) 159:85–105. doi: 10.1016/B978-0-444-63916-5.00005-7
95. Ting LH, van Antwerp KW, Scrivens JE, McKay JL, Welch TD, Bingham JT, et al. Neuromechanical tuning of non-linear postural control dynamics. Chaos. (2009) 19:026111. doi: 10.1063/1.3142245
96. Nashner LM. Balance adjustments of humans perturbed while walking. J Neurophysiol. (1980) 44:650–64. doi: 10.1152/jn.1980.44.4.650
97. Parijat P, and Lockhart TE. Effects of moveable platform training in preventing slip-induced falls in older adults. Ann Biomed Eng. (2012) 40:1111–21. doi: 10.1007/s10439-011-0477-0
98. Nashner LM. Adapting reflexes controlling the human posture. Exp Brain Res. (1976) 26:59–72. doi: 10.1007/BF00235249
99. Dietz V, Quintern J, and Sillem M. Stumbling reactions in man: significance of proprioceptive and pre-programmed mechanisms. J Physiol. (1987) 386:149–63. doi: 10.1113/jphysiol.1987.sp016527
100. Haridas C, Zehr EP, and Misiaszek JE. Adaptation of cutaneous stumble correction when tripping is part of the locomotor environment. J Neurophysiol. (2008) 99:2789–97. doi: 10.1152/jn.00487.2007
101. Eng JJ, Winter DA, and Patla AE. Strategies for recovery from a trip in early and late swing during human walking. Exp Brain Res. (1994) 102:339–49. doi: 10.1007/BF00227520
102. Pijnappels M, Bobbert MF, and van Dieën JH. Contribution of the support limb in control of angular momentum after tripping. J Biomech. (2004) 37:1811–8. doi: 10.1016/j.jbiomech.2004.02.038
103. Pijnappels M, Reeves ND, Maganaris CN, and Van Dieen JH. Tripping without falling; lower limb strength, a limitation for balance recovery and a target for training in the elderly. J Electromyogr Kinesiol. (2008) 18:188–96. doi: 10.1016/j.jelekin.2007.06.004
104. Marigold DS, and Patla AE. Strategies for dynamic stability during locomotion on a slippery surface: effects of prior experience and knowledge. J Neurophysiol. (2002) 88:339–53. doi: 10.1152/jn.00691.2001
105. Heiden TL, Sanderson DJ, Inglis JT, and Siegmund GP. Adaptations to normal human gait on potentially slippery surfaces: the effects of awareness and prior slip experience. Gait Posture. (2006) 24:237–46. doi: 10.1016/j.gaitpost.2005.09.004
106. Pater ML, Rosenblatt NJ, and Grabiner MD. Expectation of an upcoming large postural perturbation influences the recovery stepping response and outcome. Gait Posture. (2015) 41:335–7. doi: 10.1016/j.gaitpost.2014.10.026
107. Oludare SO, Pater ML, Rosenblatt NJ, and Grabiner MD. Trip-specific training enhances recovery after large postural disturbances for which there is NO expectation. Gait Posture. (2018) 61:382–6. doi: 10.1016/j.gaitpost.2018.02.001
108. Okubo Y, Brodie MA, Sturnieks DL, Hicks C, Carter H, Toson B, et al. Exposure to trips and slips with increasing unpredictability while walking can improve balance recovery responses with minimum predictive gait alterations. PLoS ONE. (2018) 13:e0202913. doi: 10.1371/journal.pone.0202913
109. Siegmund GP, Heiden TL, Sanderson DJ, Inglis JT, and Brault JR. The effect of subject awareness and prior slip experience on tribometer-based predictions of slip probability. Gait Posture. (2006) 24:110–9. doi: 10.1016/j.gaitpost.2005.08.005
110. Bhatt T, and Pai YC. Can observational training substitute motor training in preventing backward balance loss after an unexpected slip during walking? J Neurophysiol. (2008) 99:843–52. doi: 10.1152/jn.00720.2007
111. Del Rey P. Training and contextual interference effects on memory and transfer. Res Q Exerc Sport. (1989) 60:342–7. doi: 10.1080/02701367.1989.10607461
112. Wrisberg CA, and Liu Z. The effect of contextual variety on the practice, retention, and transfer of an applied motor skill. Res Q Exerc Sport. (1991) 62:406–12. doi: 10.1080/02701367.1991.10607541
113. Dail TK, and Christina RW. Distribution of practice and metacognition in learning and long-term retention of a discrete motor task. Res Q Exerc Sport. (2004) 75:148–55. doi: 10.1080/02701367.2004.10609146
114. Markowitsch HJ, Kessler J, and Streicher M. Consequences of serial cortical, hippocampal, and thalamic lesions and of different lengths of overtraining on the acquisition and retention of learning tasks. Behav Neurosci. (1985) 99:233–56. doi: 10.1037/0735-7044.99.2.233
115. Lemoine HE, and Levy BA. Increasing the naming speed of poor readers: representations formed across repetitions. J Exp Child Psychol. (1993) 55:297–328. doi: 10.1006/jecp.1993.1018
116. Hart M, Poremba A, and Gabriel M. The nomadic engram: overtraining eliminates the impairment of discriminative avoidance behavior produced by limbic thalamic lesions. Behav Brain Res. (1997) 82:169–77. doi: 10.1016/S0166-4328(97)80986-2
117. Pai YC, Yang F, Bhatt T, and Wang E. Learning from laboratory-induced falling: long-term motor retention among older adults. Age. (2014). 36:9640. doi: 10.1007/s11357-014-9640-5
118. McCrum C, Karamanidis K, Willems P, Zijlstra W, and Meijer K. Retention, savings and interlimb transfer of reactive gait adaptations in humans following unexpected perturbations. Commun Biol. (2018) 1:230. doi: 10.1038/s42003-018-0238-9
119. König M, Epro G, Seeley J, Potthast W, and Karamanidis K. Retention and generalizability of balance recovery response adaptations from trip perturbations across the adult life span. J Neurophysiol. (2019) 122:1884–93. doi: 10.1152/jn.00380.2019
120. Van Duijnhoven HJ, Roelofs JM, Den Boer JJ, Lem FC, Hofman R, Van Bon GE, et al. Perturbation-based balance training to improve step quality in the chronic phase after stroke: a proof-of-concept study. Front Neurol. (2018) 9:12. doi: 10.3389/fneur.2018.00980
121. Bhatt T, Dusane S, and Patel P. Does severity of motor impairment affect reactive adaptation and fall-risk in chronic stroke survivors? J Neuroeng Rehabil. (2019) 16:43. doi: 10.1186/s12984-019-0510-3
122. Handelzalts S, Kenner-Furman M, Gray G, Soroker N, Shani G, and Melzer I. Effects of perturbation-based balance training in subacute persons with stroke: a randomized controlled trial. Neurorehabil Neural Repair. (2019) 33:213–24. doi: 10.1177/1545968319829453
123. Dusane S, and Bhatt T. Effect of multisession progressive gait-slip training on fall-resisting skills of people with chronic stroke: examining motor adaptation in reactive stability. Brain Sci. (2021) 11. doi: 10.3390/brainsci11070894
124. Peterson DS, Dijkstra BW, and Horak FB. Postural motor learning in people with Parkinson's disease. J Neurol. (2016) 263:1518–29. doi: 10.1007/s00415-016-8158-4
125. Barajas JS, and Peterson DS. First-trial protective step performance before and after short-term perturbation practice in people with Parkinson's disease. J Neurol. (2018) 265:1138–44. doi: 10.1007/s00415-018-8821-z
126. Monaghan AS, Finley JM, Mehta SH, and Peterson DS. Assessing the impact of dual-task reactive step practice in people with Parkinson's disease: a feasibility study. Hum Mov Sci. (2021) 80:102876. doi: 10.1016/j.humov.2021.102876
127. Patel P, and Bhatt T. Adaptation to large-magnitude treadmill-based perturbations: improvements in reactive balance response. Physiol Rep. (2015) 3. doi: 10.14814/phy2.12247
128. Bhatt T, Yang F, and Pai YC. Learning to resist gait-slip falls: long-term retention in community-dwelling older adults. Arch Phys Med Rehabil. (2012) 93:557–64. doi: 10.1016/j.apmr.2011.10.027
129. Van Hedel HJ, Biedermann M, Erni T, and Dietz V. Obstacle avoidance during human walking: transfer of motor skill from one leg to the other. J Physiol. (2002) 543:709–17. doi: 10.1113/jphysiol.2002.018473
130. Bhatt T, and Pai YC. Immediate and latent interlimb transfer of gait stability adaptation following repeated exposure to slips. J Mot Behav. (2008) 40:380–90. doi: 10.3200/JMBR.40.5.380-390
131. Marcori AJ, Teixeira LA, Mathias KR, Dascal JB, and Okazaki VH. Asymmetric interlateral transfer of motor learning in unipedal dynamic balance. Exp Brain Res. (2020) 238:2745–51. doi: 10.1007/s00221-020-05930-8
132. Pai YC, Wening JD, Runtz EF, Iqbal K, and Pavol MJ. Role of feedforward control of movement stability in reducing slip-related balance loss and falls among older adults. J Neurophysiol. (2003) 90:755–762. doi: 10.1152/jn.01118.2002
133. Bhatt T, and Pai YC. Generalization of gait adaptation for fall prevention: from moveable platform to slippery floor. J Neurophysiol. (2009) 101:948–57. doi: 10.1152/jn.91004.2008
134. Yang F, Bhatt T, and Pai YC. Role of stability and limb support in recovery against a fall following a novel slip induced in different daily activities. J Biomech. (2009) 42:1903–8. doi: 10.1016/j.jbiomech.2009.05.009
135. Yang F, Bhatt T, and Pai YC. Generalization of treadmill-slip training to prevent a fall following a sudden (novel) slip in over-ground walking. J Biomech. (2013) 46:63–9. doi: 10.1016/j.jbiomech.2012.10.002
136. Bhatt T, Wang TY, Yang F, and Pai YC. Adaptation and generalization to opposing perturbations in walking. Neuroscience. (2013) 246, 435–50. doi: 10.1016/j.neuroscience.2013.04.013
137. Martelli D, Kang J, and Agrawal SK. Perturbation-based Gait training with multidirectional waist-pulls generalizes to split-belt treadmill slips. In: 7th IEEE International Conference on Biomedical Robotics and Biomechatronics (Biorob) 2018. pp. 7–12. doi: 10.1109/BIOROB.2018.8487618
138. Liu X, Bhatt T, Wang Y, Wang S, Lee A, and Pai YC. The retention of fall-resisting behavior derived from treadmill slip-perturbation training in community-dwelling older adults. GeroScience. (2021) 43:913–26. doi: 10.1007/s11357-020-00270-5
139. Morton SM, Lang CE, and Bastian AJ. Inter- and intra-limb generalization of adaptation during catching. Exp Brain Res. (2001) 141:438–45. doi: 10.1007/s002210100889
140. Lam T, and Dietz V. Transfer of motor performance in an obstacle avoidance task to different walking conditions. J Neurophysiol. (2004) 92:2010–6. doi: 10.1152/jn.00397.2004
141. Morton SM, and Bastian AJ. Prism adaptation during walking generalizes to reaching and requires the cerebellum. J Neurophysiol. (2004) 92:2497–509. doi: 10.1152/jn.00129.2004
142. Seidler RD, Noll DC, and Thiers. Feedforward and feedback processes in motor control. NeuroImage. (2004) 22:1775–1783. doi: 10.1016/j.neuroimage.2004.05.003
143. Reisman DS, Bastian AJ, and Morton SM. Neurophysiologic and rehabilitation insights from the split-belt and other locomotor adaptation paradigms. Phys Ther. (2010) 90:187–95. doi: 10.2522/ptj.20090073
144. Lee A, Bhatt T, Liu X, Wang Y, and Pai YC. Can higher training practice dosage with treadmill slip-perturbation necessarily reduce risk of falls following overground slip? Gait Posture. (2018) 61:387–92. doi: 10.1016/j.gaitpost.2018.01.037
145. Yang F, Cereceres P, and Qiao M. Treadmill-based gait-slip training with reduced training volume could still prevent slip-related falls. Gait Posture. (2018) 66:160–5. doi: 10.1016/j.gaitpost.2018.08.029
146. Wang, Y., Bhatt T., Liu X., Wang S., Lee A., Wang E., et al. (2019). Can treadmill-slip perturbation training reduce immediate risk of over-ground-slip induced fall among community-dwelling older adults? J Biomech. 84, 58–66. doi: 10.1016/j.jbiomech.2018.12.017
147. König M, Santuz A, Epro G, Werth J, Arampatzis A, and Karamanidis K. Differences in muscle synergies among recovery responses limit inter-task generalisation of stability performance. Hum Mov Sci. (2022) 82:102937. doi: 10.1016/j.humov.2022.102937
148. Karamanidis K, Epro G, McCrum C, and König M. Improving trip- and slip-resisting skills in older people: perturbation dose matters. Exerc Sport Sci Rev. (2020) 48:40–7. doi: 10.1249/JES.0000000000000210
149. König M, Epro G, Seeley J, Catalá-Lehnen P, Potthast W, and Karamanidis K. Retention of improvement in gait stability over 14weeks due to trip-perturbation training is dependent on perturbation dose. J Biomech. (2019) 84:243–6. doi: 10.1016/j.jbiomech.2018.12.011
150. Bhatt T, and Pai YC. Prevention of slip-related backward balance loss: the effect of session intensity and frequency on long-term retention. Arch Phys Med Rehabil. (2009) 90:34–42. doi: 10.1016/j.apmr.2008.06.021
151. Romberg A, Virtanen A, Aunola S, Karppi SL, Karanko H, and Ruutiainen J. Exercise capacity, disability and leisure physical activity of subjects with multiple sclerosis. Mult Scler. (2004) 10:212–8. doi: 10.1191/1352458504ms1001oa
152. McCrum C, Vaes AW, Delbressine JM, Koopman M, Liu WY, Willems P, et al. A pilot study on the feasibility and effectiveness of treadmill-based perturbations for assessing and improving walking stability in chronic obstructive pulmonary disease. Clin Biomech. (2022) 91:105538. doi: 10.1016/j.clinbiomech.2021.105538
153. Liu X, Bhatt T, and Pai YC. Intensity and generalization of treadmill slip training: High or low, progressive increase or decrease? J Biomech. (2016) 49:135–40. doi: 10.1016/j.jbiomech.2015.06.004
154. Lee A, Bhatt T, Liu X, Wang Y, Wang S, and Pai YC. Can treadmill slip-perturbation training reduce longer-term fall risk upon overground slip exposure? J Appl Biomech. (2020) 6:298-306. doi: 10.1123/jab.2019-0211
155. Wang Y, Wang S, Lee A, Pai YC, and Bhatt T. Treadmill-gait slip training in community-dwelling older adults: mechanisms of immediate adaptation for a progressive ascending-mixed-intensity protocol. Exp Brain Res. (2019) 237:2305–17. doi: 10.1007/s00221-019-05582-3
156. Shimada H, Obuchi S, Furuna T, and Suzuki T. New intervention program for preventing falls among frail elderly people: the effects of perturbed walking exercise using a bilateral separated treadmill. Am J Phys Med Rehabil. (2004) 83:493–9. doi: 10.1097/01.PHM.0000130025.54168.91
157. Wong-Yu IS, and Mak MK. Task- and Context-Specific Balance Training Program Enhances Dynamic Balance and Functional Performance in Parkinsonian Nonfallers: A Randomized Controlled Trial With Six-Month Follow-Up. Arch Phys Med Rehabil. (2015) 96:2103–11. doi: 10.1016/j.apmr.2015.08.409
158. Mansfield A, Schinkel-Ivy A, Danells CJ, Aqui A, Aryan R, Biasin L, et al. Does perturbation training prevent falls after discharge from stroke rehabilitation? A prospective cohort study with historical control. J Stroke Cerebrovasc Dis. (2017) 26:2174–80. doi: 10.1016/j.jstrokecerebrovasdis.2017.04.041
159. Aviles J, Allin LJ, Alexander NB, Van Mullekom J, Nussbaum MA, Madigan ML, et al. Comparison of treadmill trip-like training vs. Tai Chi to improve reactive balance among independent older adult residents of senior housing: a pilot controlled trial. J Gerontol A Biol Sci Med Sci. (2019) 74:1497-503. doi: 10.1093/gerona/glz018
160. Pigman J, Reisman DS, Pohlig RT, Wright TR, and Crenshaw JR. The development and feasibility of treadmill-induced fall recovery training applied to individuals with chronic stroke. BMC Neurol. (2019) 19:11. doi: 10.1186/s12883-019-1320-8
161. Mansfield A, Peters AL, Liu BA, and Maki BE. Effect of a perturbation-based balance training program on compensatory stepping and grasping reactions in older adults: a randomized controlled trial. Phys Ther. (2010) 90:476–91. doi: 10.2522/ptj.20090070
162. Schlenstedt C, Paschen S, Kruse A, Raethjen J, Weisser B, and Deuschl G. Resistance vs. Balance Training to Improve Postural Control in Parkinson's Disease: A Randomized Rater Blinded Controlled Study. PLoS ONE. (2015) 10:e0140584. doi: 10.1371/journal.pone.0140584
163. Steib S, Klamroth S, Gaßner H, Pasluosta C, Eskofier B, Winkler J, et al. Perturbation during treadmill training improves dynamic balance and gait in parkinson's disease: a single-blind randomized controlled pilot trial. Neurorehabil Neural Repair. (2017) 31:758–68. doi: 10.1177/1545968317721976
164. Esmaeili V, Juneau A, Dyer JO, Lamontagne A, Kairy D, Bouyer L, et al. Intense and unpredictable perturbations during gait training improve dynamic balance abilities in chronic hemiparetic individuals: a randomized controlled pilot trial. J Neuroeng Rehabil. (2020) 17:79. doi: 10.1186/s12984-020-00707-0
165. Unger J, Chan K, Lee JW, Craven BC, Mansfield A, Alavinia M, et al. The effect of perturbation-based balance training and conventional intensive balance training on reactive stepping ability in individuals with incomplete spinal cord injury or disease: a randomized clinical trial. Front Neurol. (2021) 12:620367. doi: 10.3389/fneur.2021.620367
166. Mansfield A, Inness EL, Danells CJ, Jagroop D, Musselman KE, Salbach NM, et al. Implementing reactive balance training in rehabilitation practice: a guide for healthcare professionals (2021).
167. Jagroop D, Houvardas S, Danells CJ, Kochanowski J, French E, Salbach NM, et al. Rehabilitation clinicians' perspectives of reactive balance training. Disabil Rehabil. (2021) 1–7. doi: 10.1080/09638288.2021.2004246
168. Carpenter MG, Frank JS, Adkin AL, Paton A, and Allum JH. Influence of postural anxiety on postural reactions to multi-directional surface rotations. J Neurophysiol. (2004) 92:3255–65. doi: 10.1152/jn.01139.2003
169. Sanders O, Hsiao HY, Savin DN, Creath RA, and Rogers MW. Aging changes in protective balance and startle responses to sudden drop perturbations. J Neurophysiol. (2019) 122:39–50. doi: 10.1152/jn.00431.2018
170. Okubo Y, Duran L, Delbaere K, Sturnieks DL, Richardson JK, Pijnappels M, et al. Rapid inhibition accuracy and leg strength are required for community-dwelling older people to recover balance from induced trips and slips: an experimental prospective study. J Geriatr Phys Ther. (2021) 45:160-6. doi: 10.1519/JPT.0000000000000312
171. Gerards MH, Sieben J, Marcellis R, de Bie RA, Meijer K, and Lenssen AF. Acceptability of a perturbation-based balance training programme for falls prevention in older adults: a qualitative study. BMJ Open. (2022) 12:e056623. doi: 10.1136/bmjopen-2021-056623
172. Protas, and E. J., Mitchell, K., Williams, A., Qureshy, H., and Caroline, K., and Lai, E. C. (2005). Gait and step training to reduce falls in Parkinson's disease. NeuroRehabilitation 20, 183–190. doi: 10.3233/NRE-2005-20305
173. Smania N, Corato E, Tinazzi M, Stanzani C, Fiaschi A, Girardi P, et al. Effect of balance training on postural instability in patients with idiopathic Parkinson's disease. Neurorehabil Neural Repair. (2010) 24:826–84. doi: 10.1177/1545968310376057
174. Shen X, and Mak MK. Technology-assisted balance and gait training reduces falls in patients with Parkinson's disease: a randomized controlled trial with 12-month follow-up. Neurorehabil Neural Repair. (2015) 29:103–11. doi: 10.1177/1545968314537559
175. Dusane S, and Bhatt T. Mixed slip-trip perturbation training for improving reactive responses in people with chronic stroke. J Neurophysiol. (2020) 124:20–31. doi: 10.1152/jn.00671.2019
176. Mohamed Suhaimy MS, Okubo Y, Hoang PD, and Lord SR. Reactive balance adaptability and retention in people with multiple sclerosis: a systematic review and meta-analysis. Neurorehabil Neural Repair. (2020) 34:675–85. doi: 10.1177/1545968320929681
177. Bieryla KA, and Madigan ML. Proof of concept for perturbation-based balance training in older adults at a high risk for falls. Arch Phys Med Rehabil. (2011) 92:841–3. doi: 10.1016/j.apmr.2010.12.004
178. Wong-Yu ISK, and Mak MKY. Multi-dimensional balance training programme improves balance and gait performance in people with Parkinson's disease: a pragmatic randomized controlled trial with 12-month follow-up. Parkinsonism Relat Disord. (2015) 21:615–21. doi: 10.1016/j.parkreldis.2015.03.022
179. Hulzinga F, de Rond V, Vandendoorent B, Gilat M, Ginis P, D'Cruz N, et al. repeated gait perturbation training in parkinson's disease and healthy older adults: a systematic review and meta-analysis. Front Hum Neurosci. (2021) 15:732648. doi: 10.3389/fnhum.2021.732648
180. Coelho DB, de Oliveira CE, Guimarães MV, de Souza CR, Dos Santos ML, and de Lima-Pardini AC. A systematic review on the effectiveness of perturbation-based balance training in postural control and gait in Parkinson's disease. Physiotherapy. (2022) 116:58–71. doi: 10.1016/j.physio.2022.02.005
181. King ST, Eveld ME, Martínez A, Zelik KE, and Goldfarb M. A novel system for introducing precisely-controlled, unanticipated gait perturbations for the study of stumble recovery. J Neuroeng Rehabil. (2019) 16:69. doi: 10.1186/s12984-019-0527-7
182. Tan GR, Raitor M, and Collins SH. Bump'em: an open-source, bump-emulation system for studying human, balance, and gait. In: IEEE International Conference on Robotics and Automation (ICRA). (2020). pp. 9093–9. doi: 10.1109/ICRA40945.2020.9197105
183. Eng JJ, Winter DA, and Patla AE. Intralimb dynamics simplify reactive control strategies during locomotion. J Biomech. (1997) 30:581–8. doi: 10.1016/S0021-9290(97)84507-1
184. Roos PE, McGuigan MP, Kerwin DG, and Trewartha G. The role of arm movement in early trip recovery in younger and older adults. Gait Posture. (2008) 27:352–6. doi: 10.1016/j.gaitpost.2007.05.001
185. Lawson BE, Varol HA, Sup F, and Goldfarb M. Stumble detection and classification for an intelligent transfemoral prosthesis. In: Annual International Conference of the IEEE Engineering in Medicine and Biology. (2010). pp. 511–4. doi: 10.1109/IEMBS.2010.5626021
186. Crenshaw JR, Kaufman KR, and Grabiner MD. Trip recoveries of people with unilateral, transfemoral or knee disarticulation amputations: Initial findings. Gait Posture. (2013) 38:534–6. doi: 10.1016/j.gaitpost.2012.12.013
187. Schillings AM, Van Wezel BM, and Duysens J. Mechanically induced stumbling during human treadmill walking. J Neurosci Methods. (1996) 67:11–7. doi: 10.1016/0165-0270(95)00149-2
188. Bierbaum S, Peper A, Karamanidis K, and Arampatzis A. Adaptational responses in dynamic stability during disturbed walking in the elderly. J Biomech. (2010) 43:2362–8. doi: 10.1016/j.jbiomech.2010.04.025
189. Tang PF, and Woollacott MH. Inefficient postural responses to unexpected slips during walking in older adults. J Gerontol A Biol Sci Med Sci. (1998) 53:M471–80. doi: 10.1093/gerona/53A.6.M471
190. Bhatt T, Wening JD, and Pai YC. Influence of gait speed on stability: recovery from anterior slips and compensatory stepping. Gait Posture. (2005) 21:146–56. doi: 10.1016/j.gaitpost.2004.01.008
191. Blumentritt S, Schmalz T, and Jarasch R. The safety of C-Leg: biomechanical tests. J Prosthet Orthot. (2009). 21:2–15. doi: 10.1097/JPO.0b013e318192e96a
192. Weber A, Werth J, Epro G, Friemert D, Hartmann U, Lambrianides Y, et al. Head-mounted and hand-held displays diminish the effectiveness of fall-resisting skills. Sensors. (2022) 22:344. doi: 10.3390/s22010344
193. Cordero AF, Koopman HF, and Van der Helm FC. Multiple-step strategies to recover from stumbling perturbations. Gait Posture. (2003) 18:47–59. doi: 10.1016/S0966-6362(02)00160-1
194. Shirota C, Simon AM, Rouse EJ, and Kuiken TA. The effect of perturbation onset timing and length on tripping recovery strategies. In: 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society. (2011). p. 7833–7836. doi: 10.1109/IEMBS.2011.6091930
195. Süptitz F, Catalá MM, Brüggemann GP, and Karamanidis K. Dynamic stability control during perturbed walking can be assessed by a reduced kinematic model across the adult female lifespan. Hum Mov Sci. (2013) 32:1404–14. doi: 10.1016/j.humov.2013.07.008
196. McCrum C, Eysel-Gosepath K, Epro G, Meijer K, Savelberg HH, Brüggemann GP, et al. Deficient recovery response and adaptive feedback potential in dynamic gait stability in unilateral peripheral vestibular disorder patients. Physiol Rep. (2014) 2:e12222. doi: 10.14814/phy2.12222
197. Kaufman KR, Wyatt MP, Sessoms PH, and Grabiner MD. Task-specific fall prevention training is effective for warfighters with transtibial amputations. Clin Orthop Relat Res. (2014) 472:3076–84. doi: 10.1007/s11999-014-3664-0
198. Debelle H, Maganaris CN, and O'Brien TD. Biomechanical mechanisms of improved balance recovery to repeated backward slips simulated by treadmill belt accelerations in young and older adults. Front Sports Act Living. (2021) 3:708929. doi: 10.3389/fspor.2021.708929
199. Grevendonk L, Connell NJ, McCrum C, Fealy CE, Bilet L, Bruls YM, et al. Impact of aging and exercise on skeletal muscle mitochondrial capacity, energy metabolism, and physical function. Nat Commun. (2021) 12:4773. doi: 10.1038/s41467-021-24956-2
200. Roeles S, Rowe PJ, Bruijn SM, Childs CR, Tarfali GD, Steenbrink F, et al. Gait stability in response to platform, belt, and sensory perturbations in young and older adults. Med Biol Eng Comput. (2018) 56:2325–35. doi: 10.1007/s11517-018-1855-7
201. Bruijn SM, Meijer OG, Beek PJ, and Van Dieen JH. The effects of arm swing on human gait stability. J Exp Biol. (2010) 213:3945–52. doi: 10.1242/jeb.045112
202. Vlutters M, Van Asseldonk EH, and Van der Kooij H. Center of mass velocity-based predictions in balance recovery following pelvis perturbations during human walking. J Exp Biol. (2016) 219:1514–23. doi: 10.1242/jeb.129338
203. Martelli D, Luo L, Kang J, Kang UJ, Fahn S, and Agrawal SK. Adaptation of stability during perturbed walking in Parkinson's disease. Sci Rep. (2017) 7:17875. doi: 10.1038/s41598-017-18075-6
204. Martelli D, Aprigliano F, and Agrawal SK. Gait Adjustments Against Multidirectional Waist-Pulls in Cerebellar Ataxia and Parkinson's Disease. In: International Conference on NeuroRehabilitation. Cham: Springer (2019). pp. 283-6 doi: 10.1007/978-3-030-01845-0_57
205. Gerards MH, Meijer K, Karamanidis K, Grevendonk L, Hoeks J, Lenssen AF, et al. Adaptability to balance perturbations during walking as a potential marker of falls history in older adults. Front Sports Act Living. (2021) 3:682861. doi: 10.3389/fspor.2021.682861
206. Lamb SE, Jørstad-Stein EC, Hauer K, and Becker C. Development of a common outcome data set for fall injury prevention trials: the prevention of falls network europe consensus. J Am Geriatr Soc. (2005) 53:1618–22. doi: 10.1111/j.1532-5415.2005.53455.x
207. Lord SR, Sherrington C, Menz HB, and Close JCT. Falls in Older People: Risk Factors and Strategies for Prevention, New York, USA, Cambridge University Press (2011).
208. McCrum C. Falls History Questionnaire Material in English, German and Dutch. (2020). doi: 10.17605/OSF.IO/HMJEF
Keywords: aged, slips, trips, gait adaptation, balance disorders, rehabilitation, accidental falls
Citation: McCrum C, Bhatt TS, Gerards MHG, Karamanidis K, Rogers MW, Lord SR and Okubo Y (2022) Perturbation-based balance training: Principles, mechanisms and implementation in clinical practice. Front. Sports Act. Living 4:1015394. doi: 10.3389/fspor.2022.1015394
Received: 09 August 2022; Accepted: 20 September 2022;
Published: 06 October 2022.
Edited by:
Fabio Augusto Barbieri, São Paulo State University, BrazilReviewed by:
Daniela Godoi Jacomassi, Federal University of São Carlos, BrazilCopyright © 2022 McCrum, Bhatt, Gerards, Karamanidis, Rogers, Lord and Okubo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christopher McCrum, Y2hyaXMubWNjcnVtQG1hYXN0cmljaHR1bml2ZXJzaXR5Lm5s
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.