 Kathryn E. Coakley
Kathryn E. Coakley David T. Lardier
David T. Lardier Kelley R. Holladay
Kelley R. Holladay Fabiano T. Amorim
Fabiano T. Amorim Micah N. Zuhl
Micah N. Zuhl
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Sports Act. Living , 09 July 2021
Sec. Physical Activity in the Prevention and Management of Disease
Volume 3 - 2021 | https://doi.org/10.3389/fspor.2021.682175
Background: The coronavirus disease 2019 (COVID-19) pandemic placed social, travel, school access, and learning restrictions on University students. Excessive restriction measures have been shown to have negative impacts on mental health. Physical activity preserves mental health, and may be useful during quarantines.
Purpose: Explore physical activity and sedentary behavior and associations with depression and anxiety symptoms among University students during COVID-19 restrictions in the Fall 2020 semester.
Methods: Six hundred and ninety-seven undergraduates (18–25 years) from a U.S. public University completed a cross-sectional survey in fall 2020. The survey included demographic questions, the Generalized Anxiety Disorder Scale 7 (GAD-7), the Patient Health Questionnaire 9 (PHQ-9), and questions about meeting moderate to vigorous physical activity (MVPA) recommendations and sedentary behavior.
Results: Forty-nine percent did not meet MVPA guidelines. Patient Health Questionnaire 9 (p = 0.002) and GAD-7 (p = 0.024) scores were higher among those who did not achieve MVPA. Sitting time (h/day) was a significant associated with depression (B = 0.29 (0.06), p < 0.05, 95% CI = 0.18, 0.41) and anxiety (B = 0.24 (0.05), p < 0.05, 95% CI = 0.13, 0.34) severity.
Conclusion: Physical activity was associated with mental health among University students during COVID-19 lockdowns.
The Coronavirus disease 2019 (COVID-19) pandemic has led to more than 100 countries implementing various forms of restriction measures during 2020 (Dunford et al., 2020). Social distancing, travel restrictions, curfews, and school closures have been combined with hygienic efforts to slow the spread of COVID-19. Modeling studies have reported that these public health measures are important to reduce virus incidence and mortality, and may proceed into 2022 (Kissler et al., 2020; Nussbaumer-Streit et al., 2020). While effective, the social and economic impacts of lockdowns may have negative consequences for psychological health. Excessive quarantining is linked to symptoms of depression, anxiety, irritability, and insomnia (Brooks et al., 2020). Factors such as boredom, misinformation, supply concerns, frustration, and financial loss are stressors that trigger a change in mood state and may also lead to a decline in mental health (Brooks et al., 2020). Survey results among individuals from pre and during the pandemic reported a three-fold increase in depression, and those with lower social and economic resources had higher levels of depression (Ettman et al., 2020). These are all correlated with increased suicidal ideations, particularly amid Covid-19 lockdowns (Chen et al., 2020).
Of particular concern are University and college students, who have been faced with the stress of remote learning and rapid life adjustments due to COVID-19-related restrictions (Husky et al., 2020; Sahu, 2020). A small survey of 195 University students noted increased stress and anxiety among 71% of the participants (Son et al., 2020). Further, the Centers for Disease Control and Prevention (CDC) reported 63% of college-aged young adults (18–24 years of age) in the U.S. had elevated depression or anxiety between May and June 2020 (Czeisler et al., 2020). Elevated mental stress among young people may result from inadequate coping skills in the face of COVID-19-related social isolation and boredom; and, even more exacerbated among University students who may have been displaced from the traditional campus setting, leading to learning challenges and grade insecurities (Son et al., 2020; Torales et al., 2020).
Physical activity is often overlooked as a lifestyle habit to preserve mental health. Individuals who are regularly active are less likely to be diagnosed with depression or anxiety (Goodwin, 2003). Moreover, those who met moderate to vigorous physical activity (MVPA) guidelines (defined as either 150 min/week of moderate intensity exercise or 75 min/week of vigorous intensity exercise; or, an equivalent combination of both, by the United States Health and Human Services and World Health Organization) reported a 39% reduction in monthly days of poor mental health (Piercy et al., 2018; Bull et al., 2020). Individuals who were active but did not meet guidelines demonstrated a 25% reduction in days of poor mental health as well, indicating even a small amount of exercise is beneficial (Piercy et al., 2018; Fluetsch et al., 2019). In light of these findings, the World Health Organization (WHO) recently stated that adults should limit the amount of sedentary time and replace it with physical activity of any intensity or type (Bull et al., 2020; Dempsey et al., 2020). These data suggest that University students who consistently participate in physical activity may be less likely to experience depression and anxiety related to COVID-19 restrictions. Unfortunately, evidence has demonstrated a high prevalence of sedentary behavior among University students (Arias-Palencia et al., 2015). This may inadvertently influence mental health among this group (Lee and Kim, 2019).
Therefore, the aim of this study was to explore physical activity and sedentary behavior associations with depression and anxiety symptoms among young adult University students during COVID-19 restrictions in the Fall 2020 semester.
Undergraduate students 18–25 years of age at a large public University in the southwest region of the U.S were recruited for the observational cross-sectional study. Participants were enrolled at the University in spring 2020, at the start of the COVID-19 pandemic, and in fall 2020, during a second wave of cases. Four thousand students were contacted via email during a 2-week period in October–November 2020. Selection was random to create a representative sample of the University population by gender, race/ethnicity, and campus enrollment. At the end of the survey, participants could provide their email address to receive one of twenty US$50 gift card incentives. Consent was obtained when the survey was started; no consent signature was required. The study was approved by the University's Institutional Review Board (protocol 1654391). The STROBE statement was utilized as a guide to report results (see Supplemental File).
Data were collected via Opinio, an online survey tool approved for research. The survey included screening questions assessing age and student status (current student and student in spring 2020). The survey then included demographic questions (age, race/ethnicity, gender, campus enrollment, academic standing, employment). The seven-item Generalized Anxiety Disorder Scale-7 (GAD-7), a validated measure of anxiety symptoms in the past 2 weeks, was used to assess anxiety within the survey (Löwe et al., 2008). All seven questions were administered and the 3-point scoring system was used to assess anxiety (0–3 for each question). The Patient Health Questionnaire-9 (PHQ-9) a validated measure of depressive symptoms in the past 2 weeks was also administered (Kroenke et al., 2001). Nine questions were asked and a 0- to 3-point scale was used to score the outcome. For both the GAD-7 and PHQ-9 questionnaires, the scores for each individual could not be validated by a clinician due to the survey nature of the study (Kroenke et al., 2001). Physical activity measures included moderate intensity exercise minutes per week; vigorous intensity exercise minutes per week; walking days per week; and number sitting hours per day. Questions examining moderate and vigorous intensity exercise were based on the International Physical Activity Questionnaire (IPAQ), which is validated for young adults (Craig et al., 2003). Specifically, only Part 4 of the IPAQ was used, which assesses recreation, sport, and leisure -time physical activity over the previous seven days (Craig et al., 2003).
Those who reported 150 min or more of moderate intensity exercise per week (≥150 min/week) and, or 75 min or more of vigorous intensity exercise per week (≥75 min/week), or an equivalent combination of both moderate- and vigorous-intensity aerobic exercise were considered to meet physical activity guidelines (USDHHS, 2018). Combination was calculated by adding moderate minutes per week plus two times vigorous minutes per week. Meeting MVPA was determined if combination equated to ≥150. Number of hours sitting per day was examined as a continuous variable (0–24).
A-priori power analyses were conducted in G*Power (Erdfelder et al., 1996) to determine adequate sample size to identify medium to large effect sizes based on Cohen's criteria (Cohen, 1988). Power analyses indicated that with a desired power of 0.80, two-tailed, alpha = 0.05, medium effect size of 0.30, a sample size >100 was adequate to identify significant effects cross-sectionally. Power estimates ranged from 0.65 (d = 0.24) and 0.95 (d = 0.38). Only those who completed the physical activity portion of the survey were included in the analyses. Baseline demographic data are presented descriptively. Those who reported meeting moderate intensity guidelines (≥150 min/week) or vigorous intensity guidelines (≥75 min/week), or an equivalent combination of both moderate and vigorous intensity exercise were considered to meet MVPA recommendations. Those that did not achieve either moderate or vigorous intensity guidelines were categorized into not meeting MVPA. The GAD-7 and PHQ-9 were scored according to standard guidelines. Generalized Anxiety Disorder Scale 7 scores range from 0 to 21 and were used to categorize anxiety symptoms severity: mild (5–9), moderate (10–14), or severe (>15). Patient Health Questionnaire 9 scores range from 0 to 27 and were used to categorize depression symptom severity: mild (5–9), moderate (10–14), moderately severe (15–19), or severe (>20). Age, GAD-7 score, PHQ-9 score, minutes of exercise, and sitting time were compared between groups (meeting MVPA recommendations vs. not meeting MVPA recommendations) using Mann-Whitney U-tests. The relationships between GAD-7 and PHQ-9 scores and physical activity intensity (moderate and vigorous min/week) and sitting time (h/day) were analyzed using Spearman rank-order correlation. Last, multivariate linear regression analyses examined associations between exercise intensity (including both moderate and vigorous intensity min/week), walking time (min/week), and sitting times and PHQ-9 score indicating depression severity and GAD-7 score indicating anxiety severity, adjusted for sociodemographic covariates. Covariates were retained based on meaningful contribution and statistical significance to the final analytical model (Aneshensel, 2012). Gender was the only covariate that contributed significantly. Both age and employment status were evaluated but did not qualify.
The survey was distributed via email to 4,000 randomly selected students in late October 2020. A total of 852 started the survey, 75 were removed due to not meeting exclusion criteria designating a sample of 777 participants in the parent study (Coakley et al., 2021). For the current study, another 80 did not complete the physical activity section of the survey and were removed from subsequent analyses. Therefore, 697 undergraduates 18–25 years of age were included. Average age was 21.29 ± 1.62 years. Sixty-two percent (n = 431) were female; 31.6% (n = 220) were White; 29% were Hispanic, Latino, or Spanish (n = 204); and 22.7% (n = 158) reported being multiracial. Of note, in Fall 2020 the undergraduate population was 57% female; 30% white, 50% Hispanic, 3% African American, and 4% were multiracial. The majority of survey responders (47.2%, n = 329) were employed part-time, and 35% were not employed (see Table 1). No missing data were present among main analytic variables including GAD-7 (measure of anxiety) and PHQ-9 (measure of depression).
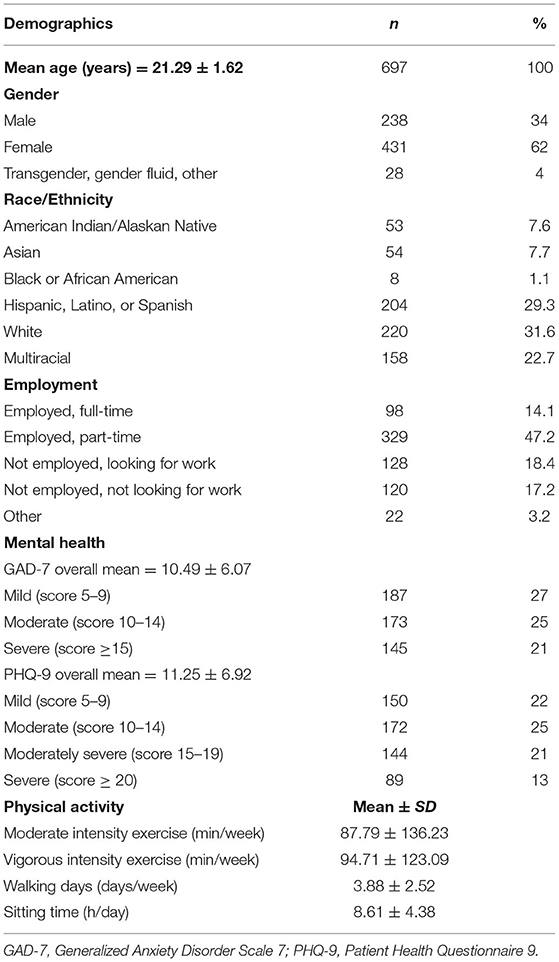
Table 1. Demographic characteristics of study participants.
A total of 350 participants (51%) achieved either ≥150 min/week of moderate intensity or ≥75 min/week aerobic exercise, or combination of both (Table 2). Those who met MVPA guidelines, reported a total of 334.22 ± 213.98 min/week of aerobic activity compared to 28.26 ± 36.28 min/week among those who did not meet MVPA guidelines (p < 0.0001). Both moderate intensity exercise minutes (156.48 ± 162.98 vs. 18.27 ± 31.80 min/week, p < 0.0001) and vigorous intensity exercise minutes (177.80 ± 126.23 vs. 9.98 ± 17.21 min/week, p < 0.0001) were higher among individuals who met MVPA guidelines. Those who did not meet MVPA guidelines reported significantly higher sitting time per day (p < 0.0001), along with PHQ-9 (p = 0.004) and GAD-7 (p = 0.024) scores.
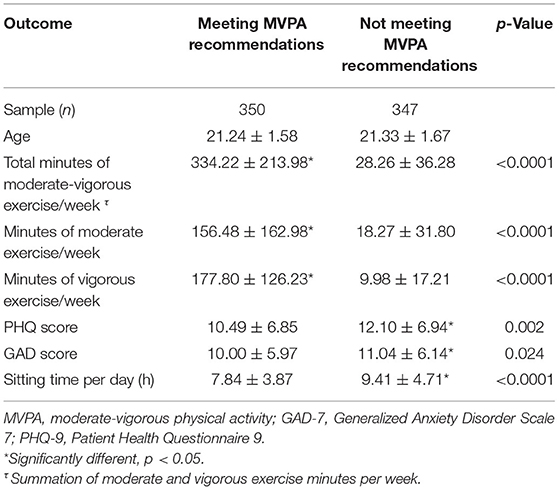
Table 2. Students who reportedly met physical activity weekly MVPA recommendations (reported as either moderate, ≥ 150 min/week); and, or vigorous, ≥ 75 min/week) compared to those that did not meet guidelines.
Generalized Anxiety Disorder Scale 7 scores were positively correlated with sitting time (rs = 0.17, p < 0.0001), and had a negative association with vigorous exercise min/week (rs = 0.082, p = 0.03). Similarly, PHQ-9 were correlated with sitting time (rs = 0.19, p < 0.0001); and negatively correlated with moderate exercise min/week (rs = −0.080, p = 0.03); and with vigorous exercise min/week (rs = −0.10, p = 0.007).
Multivariate regression analyses for PHQ-9 score indicating depression symptom severity are presented in Table 3. Results indicated that sitting time per day (h) was positively associated with depression symptoms [B = 0.29 (0.06), p < 0.05, 95% CI = 0.17, 0.41]; and vigorous intensity exercise (min/week) and depression symptoms had a negative association that trended near significance [B = −0.28 (0.15), p = 0.054, 95% CI = −0.56, −0.01]. Gender was included as a covariate. Female participants displayed a positive association with depression symptom severity [B = 2.21 (0.48), p < 0.05, 95% CI = 1.27, 3.15].
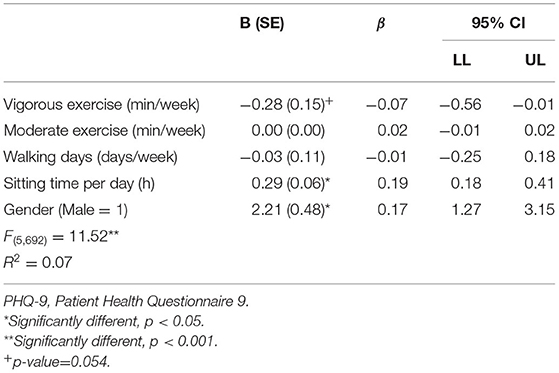
Table 3. Multivariate regression analyses between exercise intensity, walking days, sitting times, and depression severity (based on PHQ-9 score).
Multivariate regression analyses for GAD-7 score indicating anxiety symptom severity are presented in Table 4. Results indicated that sitting time per day (h) was positively associated with anxiety (GAD-7 score) severity [B = 0.24 (0.05), p < 0.05, 95% CI = 0.13, 0.34]. Gender was included as a covariate. Female participants showed a positive association with anxiety symptom severity [B = 2.25 (0.42), p < 0.05, 95% CI = 1.43, 3.07].
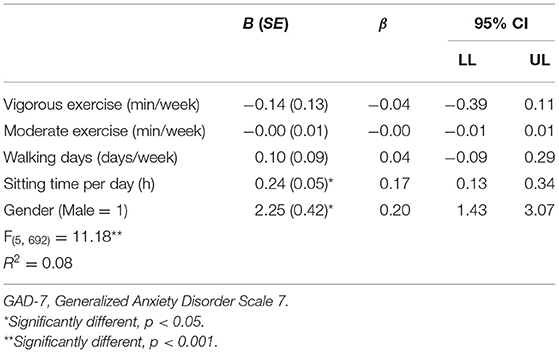
Table 4. Multivariate regression analyses between exercise intensity, walking intensity, sitting times, and anxiety severity (based on GAD-7 score).
A physically active lifestyle supports mental health (Goodwin, 2003). This study identified that University students that did not achieve recommended MVPA weekly targets had higher PHQ-9 and GAD-7 scores indicating more severe symptoms of depression and anxiety, respectively. In addition, through multivariate regression analysis, amount of daily sitting time had a significant association with both more severe depression and anxiety symptoms during the COVID-19 restrictions among University students in fall 2020.
In 2018, the U.S Department of Health and Human Services, along with the WHO in 2020 updated physical activity guidelines (Piercy et al., 2018; USDHHS, 2018). The recommendations suggest that adults should aim to achieve at least 150–300 min of moderate intensity aerobic exercise, or 75–150 min of vigorous intensity aerobic exercise per week, or an equivalent of both. For the first time, the new guidelines highlight the benefits of physical activity for several conditions affecting the brain, such as depression, anxiety, and Alzheimer's disease; however, nearly 80% of Americans do not meet guidelines. Data from this study demonstrated that 49% of University student participants did not meet MVPA exercise goals. Those who reported less than MVPA targets, determined by evaluating weekly moderate intensity (150 min/week) and vigorous intensity (75 min/week) exercise behavior, scored higher on the PHQ-9 for depression and GAD-7 for anxiety, compared to those who achieved the MVPA targets. Correlation analysis also revealed that PHQ-9 scores were negatively associated moderate exercise minutes per week, and trended with weekly vigorous intensity exercise. Accordingly, individuals with more severe symptoms of depression and anxiety reported lower moderate and, or, vigorous exercise minutes per week. These data suggest that University students who achieve PA recommendations during COVID-19 restrictions were likely to have a lower depression and anxiety symptoms. However, reverse causality cannot be ruled out based on these data. It is possible that elevated depression related to COVID-19 lockdown measures contributed to lack of physical activity. While less studied, data has suggested a link between depression and development of a sedentary lifestyle (Roshanaei-Moghaddam et al., 2009). Specifically, individuals with elevated baseline depressive symptoms were 1.79 times more likely to be physically inactive (Allan et al., 2007). In addition, young people with mood disorders are at increased risk of developing poor health behaviors such as smoking and excessive weight gain (Katon, 2003; McElroy et al., 2004). Young adults with symptoms such as low energy levels, irritability, anxiousness, and lack of self-esteem, along with co-existing negative health habits would likely lack motivation to exercise, nor see the mental health-related benefits of being physically active.
Several observational studies have demonstrated a positive impact of PA on symptoms of depression among women, minority populations, men, and University students (Wise et al., 2006; McKercher et al., 2009; Currier et al., 2020; Tao et al., 2020). Of note, the majority of survey responders in the current study were female (62%), and of minority ethnic backgrounds (~66%). These findings suggest that physical activity may protect against mental health decline in young adults during COVID-19 lockdowns. Limited comparative data exists regarding the role of PA on symptoms of depression during the COVID-19 pandemic among young people. Pieh et al., reported a higher prevalence of depression (PHQ-9 > 10) among adult Austrians, and particularly young adults (<35 years of age) after 4-weeks of lockdowns, and a nearly five-fold increase compared to pre-pandemic times (Pieh et al., 2020).
To date, there have been no accurate evaluations of PA and depressive symptoms during the COVID-19 pandemic among only young adults. In Spain, it was demonstrated that those who met PA guidelines for moderate or vigorous exercise had lower depression scores during COVID-19 lockdowns, but only older adults 60–92 years of age were included (Carriedo et al., 2020). Similar relationships between PA and depressive symptoms were reported in Norway among 1,281 adults, aged 19–90 years (Ernstsen and Havnen, 2020). Early pandemic data from spring and summer 2020 have suggested an alarming mental health decline, notably among young adults, which may be due to a lack of developed coping and emotional behaviors (Compas et al., 2014; Czeisler et al., 2020). In addition, young people are less likely to recognize their mood/behavior changes, and seek therapeutic assistance (Pedersen and Paves, 2014). The current data support the notion that young University students who exercise more and achieve PA recommendations are less likely to experience symptoms of depression. Therefore, encouraging PA behavior may be a therapeutic option. However, the causal effect cannot be evaluated.
Symptoms of anxiety were higher among those that did not meet MVPA recommendations, and anxiety symptoms severity was inversely associated with weekly minutes of vigorous exercise. A similar relationship between physical activity and perceived anxiety was observed among 2,250 middle-aged adults during the Fall 2020 COVID-19 lockdown in Spain (López-Bueno et al., 2020). Those who met WHO physical activity recommendations were nearly half as likely to report elevated anxiety (López-Bueno et al., 2020). Meta analytical findings have demonstrated a small reductive effect of physical activity on symptoms of anxiety among non-clinical populations (Rebar et al., 2015). Mechanisms include psychological changes such as mood enhancement and self-efficacy, along with neurophysiological adaptations (Portugal et al., 2013). However, conflicting data regarding the benefits of exercise on symptoms of anxiety have been reported (Bartley et al., 2013). The multivariate analyses in the current study revealed a non-association between physical activity (both moderate and vigorous intensity) and symptoms of anxiety. One explanation is that the anxiolytic effect of exercise is transient, termed the “endorphin effect,” and is diminished after a short period of time (Anderson and Shivakumar, 2013). In addition, the impact of exercise training may be more evident among those who have clinically diagnosed anxiety (Herring et al., 2010).
Sitting time (h/week) was positively associated of depression symptom severity and vigorous intensity exercise had a negative association that was trending toward significance (p = 0.054). Female gender identity was also associated with depression severity. Sitting time and female gender identity were also significantly associated with anxiety symptom severity. The average sitting time per day for this cohort of University students was 8.61 h/day, which is similar to the 7.59 h/day reported in a recent survey among 244 students (Lee and Kim, 2019). Activities performed while sitting were not evaluated in the current study, but recent data suggest that passive behaviors such as watching television worsened depressive symptoms, and television watching time has surged since the COVID-19 pandemic (Dixit et al., 2020; Huang et al., 2020). Among University students, an increase in sitting time has been linked to both anxiety and depression (Lee and Kim, 2019). Moreover, due to COVID-19 restrictions, physical activity may have been replaced by sedentary behavior and sleep among young adults (Zheng et al., 2020). The current data reveals that every additional hour of sitting time was associated with an increase in PHQ-9 score by 0.19, and GAD-7 score by 0.17 while holding other predictors constant. Interestingly, in a study published in 2001, low levels of physical activity such as achieving at least 75 min per week of any type of PA was associated with 45% lower prevalence of depression among women (Dunn et al., 2001). This equates to ~10 min per day of activity and could be accomplished by simply walking outside. Therefore, fully achieving PA recommendations may not be required to prevent an increase in symptoms of depression and anxiety; however, avoiding sitting time is very important for mental health (Dempsey et al., 2020).
The results of the study should be interpreted with several limitations in mind. First, the response rate was lower (17%) than desired for an online survey; however, the sample size is comparable to similar survey studies that analyzed PA and mental health during COVID-19 lockdowns (Nulty, 2008; Barkley et al., 2020; Carriedo et al., 2020). Second, the survey was conducted at one University in the Southwest region of the U.S., and may not be generalizable to all undergraduate students. Third, survey completers may not have understood the difference between moderate and vigorous exercise, which may have influence reported data. Fourth, the IPAQ was used to assess moderate and vigorous exercise, and groups were allocated based on their physical activity. The IPAQ is reported to be reliable among young adults, but has also been reported to overestimate PA (Papathanasiou et al., 2009; Lee et al., 2011). Fifth, the PA and sedentary behavior was assessed by self-report, which is potentially subject to misreporting. However, this study used a short-term recall of PA activity (last 2 weeks) which may reduce the magnitude of reporting errors (Matthews et al., 2012). Lastly, no previous or current diagnoses or treatment of depression and anxiety was assessed.
It is clear that COVID-19 restrictions and the prolonged nature of a global pandemic are linked to a decline in mental health among young adult University students (Czeisler et al., 2020; Son et al., 2020). Social isolation, campus displacement, and academic-related stress (assignments and online transitions) may be linked to elevations in symptoms of depression and anxiety. Physical activity is an important stress relieving behavior, and students that achieved recommended MVPA guidelines had lower levels of depression, but the majority of University students do not meet PA recommendations. Moreover, sedentary behavior (evaluated as sitting time per day) was significantly associated with both depression and anxiety symptom severity. Efforts should be made to encourage students to engage in some form of PA each day, and to avoid sitting time. As little as 10 min per day of exercise has been shown to support mental health, and the implementation of home-based exercise training protocols such as bodyweight exercises may be a simple strategy to reducing symptoms of depression and anxiety (Rebar and Taylor, 2017).
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by University of New Mexico IRB. The patients/participants provided their written informed consent to participate in this study.
KC conceived the study and carried out methodology and data collection. DL performed data collection and data analyses. KH and FA assisted with methodology, data collection, and analyses. MZ contributed to methodology and data analyses and also complete the first draft of manuscript. All authors contributed to manuscript revisions, and table/figure development.
This work was funded by University of New Mexico College of Education and Human Sciences Grant.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fspor.2021.682175/full#supplementary-material
Allan, J. L., Johnston, D. W., Johnston, M., and Mant, D. (2007). Depression and perceived behavioral control are independent predictors of future activity and fitness after coronary syndrome events. J. Psychosom. Res. 63, 501–508. doi: 10.1016/j.jpsychores.2007.08.001
Anderson, E. H., and Shivakumar, G. (2013). Effects of exercise and physical activity on anxiety. Front. Psychiatry 4:27. doi: 10.3389/fpsyt.2013.00027
Aneshensel, C. S. (2012). Theory-Based Data Analysis for the Social Sciences. Thousands Oaks, CA: Sage Publications. doi: 10.4135/9781506335094
Arias-Palencia, N. M., Solera-Martinez, M., Gracia-Marco, L., Silva, P., Martinez-Vizcaino, V., Canete-Garcia-Prieto, J., et al. (2015). Levels and patterns of objectively assessed physical activity and compliance with different public health guidelines in University students. PLoS ONE 10:e0141977. doi: 10.1371/journal.pone.0141977
Barkley, J. E., Lepp, A., Glickman, E., Farnell, G., Beiting, J., Wiet, R., et al. (2020). The acute effects of the COVID-19 pandemic on physical activity and sedentary behavior in University students and employees. Int. J. Exerc. Sci. 13, 1326–1339.
Bartley, C. A., Hay, M., and Bloch, M. H. (2013). Meta-analysis: aerobic exercise for the treatment of anxiety disorders. Prog. Neuropsychopharmacol. Biol. Psychiatry 45, 34–39. doi: 10.1016/j.pnpbp.2013.04.016
Brooks, S. K., Webster, R. K., Smith, L. E., Woodland, L., Wessely, S., Greenberg, N., et al. (2020). The psychological impact of quarantine and how to reduce it: rapid review of the evidence. Lancet 395, 912–920. doi: 10.1016/S0140-6736(20)30460-8
Bull, F. C., Al-Ansari, S. S., Biddle, S., Borodulin, K., Buman, M. P., Cardon, G., et al. (2020). World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 54, 1451–1462. doi: 10.1136/bjsports-2020-102955
Carriedo, A., Cecchini, J. A., Fernandez-Rio, J., and Méndez-Giménez, A. (2020). COVID-19, psychological well-being and physical activity levels in older adults during the nationwide lockdown in Spain. Am. J. Geriatr. Psychiatry 28, 1146–1155. doi: 10.1016/j.jagp.2020.08.007
Chen, F., Ghosh, A., Lin, J., Zhang, C., Pan, Y., Thakur, A., et al. (2020). 5-lipoxygenase pathway and its downstream cysteinyl leukotrienes as potential therapeutic targets for Alzheimer's disease. Brain Behav. Immun. 88, 844–855. doi: 10.1016/j.bbi.2020.03.022
Coakley, K. E., Lardier, D. T., Holladay, K. R., Amorim, F. T., Mechler, H., and Zuhl, M. N. (2021). Mental health severity is associated with increases in alcohol consumption in young adult students during the COVID-19 pandemic. Alcohol. Treat. Q. 2021, 1–14. doi: 10.1080/07347324.2021.1917325
Cohen, J. (1988). Statistical Power Analysis for the Behavioral Sciences, 2nd Edn. Hillsdle, NJ: Lawrence Erlbaum Associates, Publishers.
Compas, B. E., Jaser, S. S., Dunbar, J. P., Watson, K. H., Bettis, A. H., Gruhn, M. A., et al. (2014). Coping and emotion regulation from childhood to early adulthood: points of convergence and divergence. Aust. J. Psychol. 66, 71–81. doi: 10.1111/ajpy.12043
Craig, C. L., Marshall, A. L., Sjöström, M., Bauman, A. E., Booth, M. L., Ainsworth, B. E., et al. (2003). International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 35, 1381–1395. doi: 10.1249/01.MSS.0000078924.61453.FB
Currier, D., Lindner, R., Spittal, M. J., Cvetkovski, S., Pirkis, J., and English, D. R. (2020). Physical activity and depression in men: increased activity duration and intensity associated with lower likelihood of current depression. J. Affect. Disord. 260, 426–431. doi: 10.1016/j.jad.2019.09.061
Czeisler, M. É., Lane, R. I., Petrosky, E., Wiley, J. F., Christensen, A., Njai, R., et al. (2020). Mental health, substance use, and suicidal ideation during the COVID-19 pandemic—United States, June 24–30, 2020. Morb. Mortal. Wkly. 69:1049. doi: 10.15585/mmwr.mm6932a1
Dempsey, P. C., Biddle, S. J., Buman, M. P., Chastin, S., Ekelund, U., Friedenreich, C. M., et al. (2020). New global guidelines on sedentary behaviour and health for adults: broadening the behavioural targets. Int. J. Behav. Nutr. Phys. Activ. 17, 1–12. doi: 10.1186/s12966-020-01044-0
Dixit, A., Marthoenis, M., Arafat, S. Y., Sharma, P., and Kar, S. K. (2020). Binge watching behavior during COVID 19 pandemic: a cross-sectional, cross-national online survey. Psychiatry Res. 289:113089. doi: 10.1016/j.psychres.2020.113089
Dunford, D., Dale, B., Stylianou, N., Lowther, E., Ahmed, M., and De la Torre Arenas, I. (2020) (April, 2020). Coronavirus: the world in lockdown in maps charts. BBC News.
Dunn, A. L., Trivedi, M. H., and O'Neal, H. A. (2001). Physical activity dose-response effects on outcomes of depression and anxiety. Med Sci Sports Exerc. 33(6 Suppl), S587–S597; discussion 609–610. doi: 10.1097/00005768-200106001-00027
Erdfelder, E., Faul, F., and Buchner, A. (1996). GPOWER: a general power analysis program. Behav. Res. Methods Instrum. Comput. 28, 1–11. doi: 10.3758/BF03203630
Ernstsen, L., and Havnen, A. (2020). Mental health and sleep disturbances in physically active adults during the COVID-19 lockdown in Norway: does change in physical activity level matter? Sleep Med. 77, 309–312. doi: 10.1016/j.sleep.2020.08.030
Ettman, C. K., Abdalla, S. M., Cohen, G. H., Sampson, L., Vivier, P. M., and Galea, S. (2020). Prevalence of depression symptoms in US adults before and during the COVID-19 pandemic. JAMA Network Open. 3:e2019686. doi: 10.1001/jamanetworkopen.2020.19686
Fluetsch, N., Levy, C., and Tallon, L. (2019). The relationship of physical activity to mental health: a 2015 behavioral risk factor surveillance system data analysis. J. Affect. Disord. 253, 96–101. doi: 10.1016/j.jad.2019.04.086
Goodwin, R. D. (2003). Association between physical activity and mental disorders among adults in the United States. Prev. Med. 36, 698–703. doi: 10.1016/S0091-7435(03)00042-2
Herring, M. P., O'Connor, P. J., and Dishman, R. K. (2010). The effect of exercise training on anxiety symptoms among patients: a systematic review. Arch. Intern. Med. 170, 321–331. doi: 10.1001/archinternmed.2009.530
Huang, Y., Li, L., Gan, Y., Wang, C., Jiang, H., Cao, S., et al. (2020). Sedentary behaviors and risk of depression: a meta-analysis of prospective studies. Transl. Psychiatry 10, 1–10. doi: 10.1038/s41398-020-0715-z
Husky, M. M., Kovess-Masfety, V., and Swendsen, J. D. (2020). Stress and anxiety among University students in France during Covid-19 mandatory confinement. Compr. Psychiatry 102:152191. doi: 10.1016/j.comppsych.2020.152191
Katon, W. J. (2003). Clinical and health services relationships between major depression, depressive symptoms, and general medical illness. Biol. Psychiatry 54, 216–226. doi: 10.1016/S0006-3223(03)00273-7
Kissler, S. M., Tedijanto, C., Goldstein, E., Grad, Y. H., and Lipsitch, M. (2020). Projecting the transmission dynamics of SARS-CoV-2 through the postpandemic period. Science 368, 860–868. doi: 10.1126/science.abb5793
Kroenke, K., Spitzer, R. L., and Williams, J. B. (2001). The PHQ-9: validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 606–613. doi: 10.1046/j.1525-1497.2001.016009606.x
Lee, E., and Kim, Y. (2019). Effect of University students' sedentary behavior on stress, anxiety, and depression. Perspect. Psychiatr. Care 55:164. doi: 10.1111/ppc.12296
Lee, P. H., Macfarlane, D. J., Lam, T. H., and Stewart, S. M. (2011). Validity of the international physical activity questionnaire short form (IPAQ-SF): a systematic review. Int. J. Behav. Nutr. Phys. Act. 8, 1–11. doi: 10.1186/1479-5868-8-115
López-Bueno, R., Calatayud, J., Ezzatvar, Y., Casajús, J. A., Smith, L., Andersen, L. L., et al. (2020). Association between current physical activity and current perceived anxiety and mood in the initial phase of COVID-19 confinement. Front. Psychiatry 11:729. doi: 10.3389/fpsyt.2020.00729
Löwe, B., Decker, O., Müller, S., Brähler, E., Schellberg, D., Herzog, W., et al. (2008). Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Med. Care 46, 266–274. doi: 10.1097/MLR.0b013e318160d093
Matthews, C. E., Steven, C. M., George, S. M., Sampson, J., and Bowles, H. R. (2012). Improving self-reports of active and sedentary behaviors in large epidemiologic studies. Exerc. Sport Sci. Rev. 40, 118–126. doi: 10.1097/JES.0b013e31825b34a0
McElroy, S. L., Kotwal, R., Malhotra, S., Nelson, E. B., Keck, P. E., and Nemeroff, C. B. (2004). Are mood disorders and obesity related? A review for the mental health professional. J. Clin. Psychiatry 65, 634–651. doi: 10.4088/JCP.v65n0507
McKercher, C. M., Schmidt, M. D., Sanderson, K. A., Patton, G. C., Dwyer, T., and Venn, A. J. (2009). Physical activity and depression in young adults. Am. J. Prev. Med. 36, 161–164. doi: 10.1016/j.amepre.2008.09.036
Nulty, D. D. (2008). The adequacy of response rates to online and paper surveys: what can be done? Assess. Eval. High. Educ. 33, 301–314. doi: 10.1080/02602930701293231
Nussbaumer-Streit, B., Mayr, V., Dobrescu, A. I., Chapman, A., Persad, E., Klerings, I., et al. (2020). Quarantine alone or in combination with other public health measures to control COVID-19: a rapid review. Cochrane Database Syst Rev. 4:CD013574. doi: 10.1002/14651858.CD013574
Papathanasiou, G., Georgoudis, G., Papandreou, M., Spyropoulos, P., Georgakopoulos, D., Kalfakakou, V., et al. (2009). Reliability measures of the short International Physical Activity Questionnaire (IPAQ) in Greek young adults. Hellenic J. Cardiol. 50, 283–294.
Pedersen, E. R., and Paves, A. P. (2014). Comparing perceived public stigma and personal stigma of mental health treatment seeking in a young adult sample. Psychiatry Res. 219, 143–150. doi: 10.1016/j.psychres.2014.05.017
Pieh, C., Budimir, S., and Probst, T. (2020). The effect of age, gender, income, work, and physical activity on mental health during coronavirus disease (COVID-19) lockdown in Austria. J. Psychosom. Res. 136:110186. doi: 10.1016/j.jpsychores.2020.110186
Piercy, K. L., Troiano, R. P., Ballard, R. M., Carlson, S. A., Fulton, J. E., Galuska, D. A., et al. (2018). The physical activity guidelines for Americans. JAMA 320, 2020–2028. doi: 10.1001/jama.2018.14854
Portugal, E. M. M., Cevada, T., Monteiro-Junior, R. S., Guimarães, T. T., da Cruz Rubini, E., Lattari, E., et al. (2013). Neuroscience of exercise: from neurobiology mechanisms to mental health. Neuropsychobiology 68, 1–14. doi: 10.1159/000350946
Rebar, A. L., Stanton, R., Geard, D., Short, C., Duncan, M. J., and Vandelanotte, C. (2015). A meta-meta-analysis of the effect of physical activity on depression and anxiety in non-clinical adult populations. Health Psychol. Rev. 9, 366–378. doi: 10.1080/17437199.2015.1022901
Rebar, A. L., and Taylor, A. (2017). Physical activity and mental health; it is more than just a prescription. Ment. Health Phys. Act. 13, 77–82. doi: 10.1016/j.mhpa.2017.10.004
Roshanaei-Moghaddam, B., Katon, W. J., and Russo, J. (2009). The longitudinal effects of depression on physical activity. Gen. Hosp. Psychiatry. 31, 306–315. doi: 10.1016/j.genhosppsych.2009.04.002
Sahu, P. (2020). Closure of universities due to coronavirus disease 2019 (COVID-19): impact on education and mental health of students and academic staff. Cureus 12:e7541. doi: 10.7759/cureus.7541
Son, C., Hegde, S., Smith, A., Wang, X., and Sasangohar, F. (2020). Effects of COVID-19 on college students' mental health in the United States: interview survey study. J. Med. Internet. Res. 22:e21279. doi: 10.2196/21279
Tao, S., Wu, X., Yang, Y., and Tao, F. (2020). The moderating effect of physical activity in the relation between problematic mobile phone use and depression among University students. J. Affect. Disord. 273, 167–172. doi: 10.1016/j.jad.2020.04.012
Torales, J., O'Higgins, M., Castaldelli-Maia, J. M., and Ventriglio, A. (2020). The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 66, 317–320. doi: 10.1177/0020764020915212
Wise, L. A., Adams-Campbell, L. L., Palmer, J. R., and Rosenberg, L. (2006). Leisure time physical activity in relation to depressive symptoms in the Black Women's Health Study. Ann. Behav. Med. 32, 68–76. doi: 10.1207/s15324796abm3201_8
Keywords: exercise, depression, sedentary behavior, COVID-19, students
Citation: Coakley KE, Lardier DT, Holladay KR, Amorim FT and Zuhl MN (2021) Physical Activity Behavior and Mental Health Among University Students During COVID-19 Lockdown. Front. Sports Act. Living 3:682175. doi: 10.3389/fspor.2021.682175
Received: 17 March 2021; Accepted: 04 June 2021;
Published: 09 July 2021.
Edited by:
Julia H. Goedecke, South African Medical Research Council, South AfricaReviewed by:
Amy E. Mendham, University of Cape Town, South AfricaCopyright © 2021 Coakley, Lardier, Holladay, Amorim and Zuhl. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Micah N. Zuhl, enVobDFtQGNtaWNoLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.