 Christopher Knowles
Christopher Knowles Stephen Shannon
Stephen Shannon Garry Prentice
Garry Prentice Gavin Breslin
Gavin Breslin
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Sports Act. Living, 20 May 2021
Sec. Movement Science
Volume 3 - 2021 | https://doi.org/10.3389/fspor.2021.612532
This article is part of the Research TopicThe Effects of the Covid-19 Pandemic on Sport: Mental Health Implications on Athletes, Coaches and Support StaffView all 28 articles
Athletes going through transition periods such as injury or retirement have previously reported feelings of depression and anxiety, especially when feeling unsupported. Cessation of competitive sport during the pandemic has forced athletes through a non-normative transition and has reduced many opportunities to satisfy their basic psychological needs increasing the risk of poor wellbeing and loneliness. Whilst athletes are often praised for their resilience—a trait that serves to support them during tough times—the inability to play sport can be particularly challenging for those with strong athletic identities. An online cross-sectional survey (n = 744) was conducted to capture adult athlete and non-athlete mental health factors (specifically wellbeing, depression, anxiety, loneliness) during emergence from a COVID-19 lockdown. Results showed that resilience was positively correlated with mental health but was no higher in athletes than non-athletes. Furthermore, athletes reported greater anxiety than non-athletes, a difference mediated by negative affectivity—a subfactor of athletic identity. We present evidence that after a temporary transition away from sport, athletes' resilience is comparable to non-athletes leaving them just as likely to suffer poor mental health. Moreover, athletes with strong athletic identities are likely to experience anxiety symptoms above and beyond those reported by non-athletes. Findings have implications for the development of self-management guidance for athletes as the COVID-19 pandemic and restrictions on sport participation continue.
Mental health is defined by the World Health Organisation (WHO) as, “a state of well-being in which an individual realises his or her own abilities, can cope with the normal stresses of life, can work productively, and is able to make a contribution to his or her community” (World Health Organisation, 2018). In a time when the world is on high alert due to the uncertainty and distress caused by a global pandemic, research into mental health and self-management has become increasingly important. Due to the rapid spread of COVID-19, the United Kingdom's government announced a national lockdown on 23rd March 2020 signifying a major step in a monumental transition from normal daily living to a world where mask wearing, social distancing and perpetual uncertainty have become the norm. A significant feature of “the COVID experience” (Samuel et al., 2020) has been the abrupt and repeated halting of competitive sport due to national lockdowns or outbreaks of the virus in sport teams and/or their respective institutions. The stop-start nature of many leagues and competitions that has existed over the course of the pandemic has presented a multitude of stressors detrimental not only to the personal lives of both amateur and professional athletes, but also to the development of their sporting careers.
The pandemic has constituted a long and enduring transitionary period in the life and career of an athlete (Stambulova et al., 2020). Transitions constitute critical phases for athletic development wherein stressors must be responded to positively to facilitate continued success, both within and out with sport (Stambulova, 2017; Stambulova et al., 2020). The predictability of a transition period can determine how successfully an athlete adapts and responds to stressors during this time with normative transitions typically being associated with more positive mental health outcomes than non-normative transitions (Wheaton, 1990; Stambulova, 2003, 2017). The most commonly observed mental health outcomes associated with non-normative transitions in sport (e.g., injury, de-selection, premature retirement) include feelings of depression and anxiety (Wylleman et al., 2004; Appaneal et al., 2009; Rice et al., 2016). Due to its non-normative nature, it was expected that similar outcomes would arise due to COVID-19. Moreover, during the pandemic athletes have had fewer opportunities to meet their basic psychological needs (Ryan and Deci, 2017) and/or benefit from sport-related social support networks (Ntoumanis et al., 2009; Biddle et al., 2015) which can contribute to poor wellbeing and loneliness (Lippke et al., 2021).
Often cited as a key determinant of an individual's mental health when faced with adversity is their level of resilience (Fletcher and Sarkar, 2013, 2016). To this end, it is possible that athletes may have an advantage over non-athletes given sports' long-standing association with the development of this beneficial psychological trait (Caddick and Ryall, 2012). Some studies support this notion finding athletes to be more resilient than non-athletes (Guillén and Laborde, 2014; Laborde et al., 2016). Considering this, it could be argued that athletes may be better equipped to deal with the psychological burden of the pandemic than non-athletes as a result of their conditioning to thrive in challenging environments and competition. That being said, existing resilience studies have investigated samples of athletes regularly participating in sport and so findings may not be representative of those undergoing a period of transition. Therefore, there is a need for further exploratory research in this area.
Another key determinant of athlete mental health during transitions is often their athletic identity (Ronkainen et al., 2016). Athletic identity can be understood as a multidimensional construct within the self-concept comprising of self-related information garnered from psychosocial factors that accompany the athlete role (Brewer et al., 1993; Murphy et al., 1996; Ronkainen et al., 2016). Brewer and colleagues propose a three-factor model for understanding athletic identity. Social identity considers the extent to which an individual identifies themselves as an athlete; exclusivity considers the degree to which the individual's self-worth depends on their athletic identity in comparison to other roles they fulfil (e.g., parent, student); and negative affectivity assesses the negative emotions that occur due to non-participation (Brewer et al., 1993). For some athletes, extensive involvement in sport over time can cause the athlete role to become deeply entwinned in their personal identity, engulfing their sense-of-self, social life and/or career. These individuals are often the most at risk for suffering poor mental health when going through a transition at which time the opportunity to participate in sport is unavailable (Grove et al., 1997; Alfermann et al., 2004; Wylleman et al., 2004; Sanders and Stevinson, 2017).
The aim of the current study was to investigate the relationships between resilience, athlete identity and mental health during transition periods. Specifically, the study aimed to identify whether associations existed between athlete identity, resilience, wellbeing, anxiety, depression and/or loneliness as we emerged from a national lockdown to better understand the impact of the pandemic. Hypothesis one was that resilience would be positively correlated with mental health. Hypothesis two was that athlete identity would be negatively correlated with mental health. Hypothesis three was that resilience would be higher in athletes than non-athletes. As this is an exploratory piece of research, in the event we came across unexpected results, we planned to conduct mediation and/or moderation analysis to ascertain why our findings might have occurred.
Ethical approval for the study was granted by Ulster University. All participants provided informed consent and were free to withdraw at any time. No personal identifying data was collected to ensure confidentiality. A cross-sectional survey research design was used. Data was collected between 23/06/2020-−13/07/2020 (i.e., 14–16 weeks from the start of lockdown, 2 weeks after restrictions were lifted for those shielding in their homes). All data was collected via SurveyMonkey. A total of 20 sporting organisations and governing bodies of sport from across the United Kingdom and Republic of Ireland were contacted via email to take part. Sporting associations publicly shared a link to the survey via their Twitter page, website and/or members mailing lists. Non-athlete participants were recruited by word of mouth and via an article published in a Northern Ireland online newspaper. A total of 753 participants over the age of 18 were recruited. Of these, nine respondents resided outside the United Kingdom or Ireland during lockdown thus, were not considered in final analysis. This left 744 participants over the age of 18 to be included of which 558 lived in the United Kingdom and 186 in the Republic of Ireland (male athletes = 199, female athletes = 161, male non-athletes = 148, female non-athletes = 236). Descriptive data for the gender and age split of the sample is provided in Figure 1. Of the 360 athletes recruited, 351 reported their level of participation (243 non-elite; 64 semi-elite; 44 elite) and which sport they primarily played (see Figure 2). When the survey was conducted, 38% of athletes and 47% of non-athletes had been practising social distancing for 13–15 weeks all of which, except for 1 or 2 weeks depending on their response date, was spent in lockdown (described in greater detail in Figure 3). A roughly equal proportion of athletes (8%) and non-athletes (10%) had been shielding since the beginning of the pandemic. Participants also reported the size of their lockdown bubbles. Bubbles comprised of people in the immediate household plus all those from another household with whom they were allowed to mix with whilst social distancing. The size of participants' lockdown bubbles were largely consistent across both athletes (M = 3.52, SD = 1.44) and non-athletes (M = 3.20, SD = 1.40).
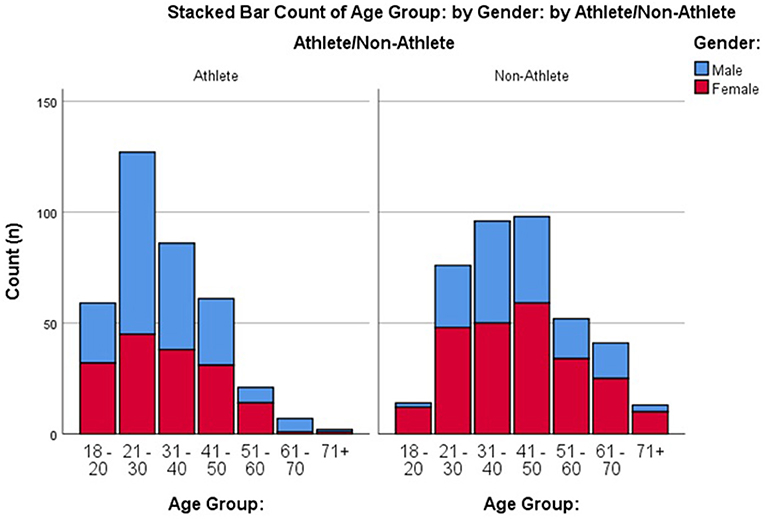
Figure 1. Histogram detailing the gender split and age ranges for athlete and non-athlete groups.
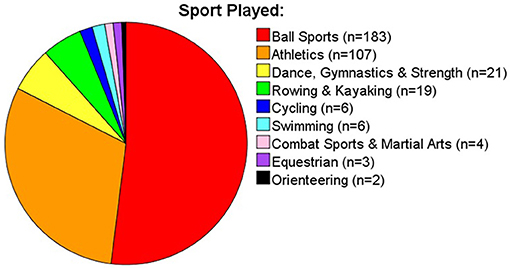
Figure 2. Pie chart of sports played by the athlete sample.
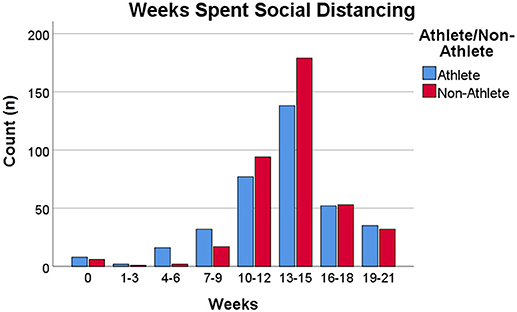
Figure 3. Weeks spent social distancing by both athletes and non-athletes.
All participants reported their gender, age range, occupation, marital status, smoking status, diet, number of weeks spent social distancing and the size of their social isolation bubble. The following question, taken from an operational definition of sport (Rejeski and Brawley, 1988; Shannon et al., 2019) was used to categorise participants as either athletes or non-athletes: “Are you an athlete involved in a structured, rule-bound, competitive physical activity?” The term “mental health” was used throughout analysis and refers collectively to participants' self-reports of wellbeing, anxiety, depression, and loneliness. Resilience and athletic identity were also surveyed via self-report measures. The following questionnaires were presented:
The MHC-SF (Keyes, 2005) is a validated three factor 14-item questionnaire measuring wellbeing. The MHC-SF provides a score for overall wellbeing and individual scores for three subscales: social, emotional, and psychological wellbeing. Using a 7-point Likert scale, the summed score for overall wellbeing and each sub factor was calculated to produce four individual variables. The MHC-SF also includes a measure of whether participants are flourishing, languishing or are moderately mentally healthy (for thresholds see Keyes, 2009). The scale had high internal consistency (Cronbach's α = 0.93) as do the social (α = 0.84), emotional (α = 0.87), and psychological (α = 0.88) subscales.
The HADS (Zigmond and Snaith, 1983) is a two-factor 14-item scale used to rate the severity of anxiety and depressive symptoms. Responses were recorded on a Likert scale ranging from 0 to 3 with the sum of participant responses providing individual scores for anxiety (HADS-A) and depression (HADS-D). Scores of 0–7 are considered within the normal range, 8–10 are evidence of mild symptoms, and 11–21 are suggestive of moderate/severe symptoms (Snaith, 2003; Breeman et al., 2015). Cronbach's α was 0.89 for the scale overall, 0.86 for HADS-A and 0.81 for the HADS-D subscales.
The BRS (Smith et al., 2008) contains 6-items that provide a single score for resilience measured on a 5-point Likert scale. The sum of participant responses gave their level of resilience. The scale had a high level of internal consistency (Cronbach's α = 0.89).
The SLS (De Jong Gierveld and Van Tilburg, 2006) is a two-factor scale containing 6-items measuring overall (Lone-O), social (Lone-S), and emotional loneliness (Lone-E). The measure has been validated cross-culturally and had an acceptable level of internal consistency in the current sample (α = 0.70). Scores were measured on a 5-point Likert scale. For negatively worded items (e.g., I often feel rejected), neutral and positive answers (i.e., more or less, agree, strongly agree) were counted. For positively worded items (e.g., there are enough people I feel close to) the neutral and negative answers were counted. A score of 0 infers complete social embeddedness whereas a score of six (or three for either subscale) is evidence of extreme loneliness.
The three factorial AIMS (Brewer et al., 1993), a 7-point Likert scale, is a measure of athletic identity in which three individual factors—social identity (AIMS-SI), negative affectivity (AIMS-NA), and exclusivity (AIMS-E)—are subordinate to one higher order factor—overall athletic identity (AIMS-O). Participants' summed scores offered a measure of their athletic identity. The AIMS had a high level of internal consistency (α = 0.89) as did each subscale: AIMS-SI (α = 0.84); AIMS-E (α = 0.86); and AIMS-NA (α = 0.78).
The mean or sum of participants' responses were calculated as per the scoring criteria for each measure. Analysis was conducted using Statistical Package for the Social Sciences 26 (copyright IBM corp., NY, USA) with the alpha level set to p < 0.05. Pearson's correlations were considered weak, moderate and strong when r = 0.20, 0.50, and 0.80, respectively. Effect sizes for t-tests were interpreted using Cohen's d where small, medium and large effects were classed as 0.20, 0.50, and 0.80, respectively. Effect size for univariate analysis was interpreted using partial eta squared where small to large effect sizes = 0.01, 0.06, and 0.14, respectively (Field, 2013). Given the sample size was large (N = 744), central limit theorem inferred the data was normally distributed. Levene's tests inferred homogeneity of variances for all statistical tests henceforth. Mediation analysis was carried out in line with Newsom's (2020) method using a series of linear regressions and Sobel tests. An initial regression was conducted to compute the unstandardised coefficient for the relationship between the predictor variable and the mediator. A second regression was then conducted to obtain the unstandardised coefficient for the path between the mediator and the outcome variable when the predictors were also included in the model. Partial mediation was observed when Sobel tests returned a positive result but the relationship between a predictor and an outcome variable remained significant after controlling for the potential mediator. Full mediation occurred in instances where Sobel tests were positive but the relationship between a predictor and dependent variable became non-significant when controlling for the mediator (Newsom, 2020).
Table 1 describes the prevalence of anxiety and depressive symptoms, extreme forms of loneliness, flourishing, languishing and moderately mentally healthy athletes and non-athletes as per the criteria of the HADS, SLS, and MHC-SF, respectively.
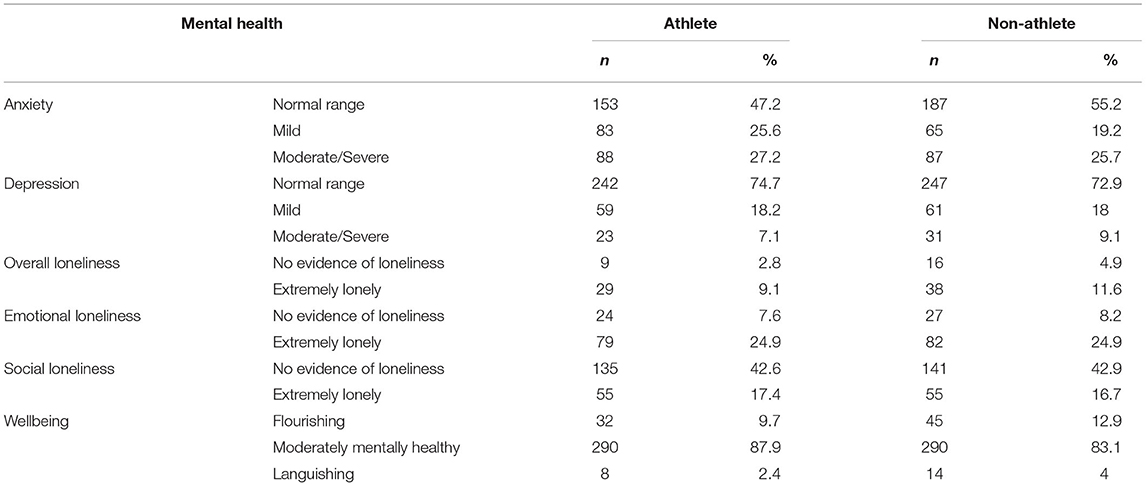
Table 1. Descriptive statistics for the severity of anxiety and depressive symptoms, and the rate of flourishing, languishing, and extreme loneliness in athletes and non-athletes.
Pearson's product moment correlations were conducted for athletes and non-athletes to measure the relationship between resilience and mental health. Findings showed that resilience was moderately positively correlated with all four MHC-SF variables (i.e., overall, social, psychological, and emotional wellbeing) and moderately negatively correlated with all SLS variables, HADS-A and HADS-D. These relationships were observed in both athletes and non-athletes which supports our first hypothesis. See Tables 2, 3 for descriptive statistics.
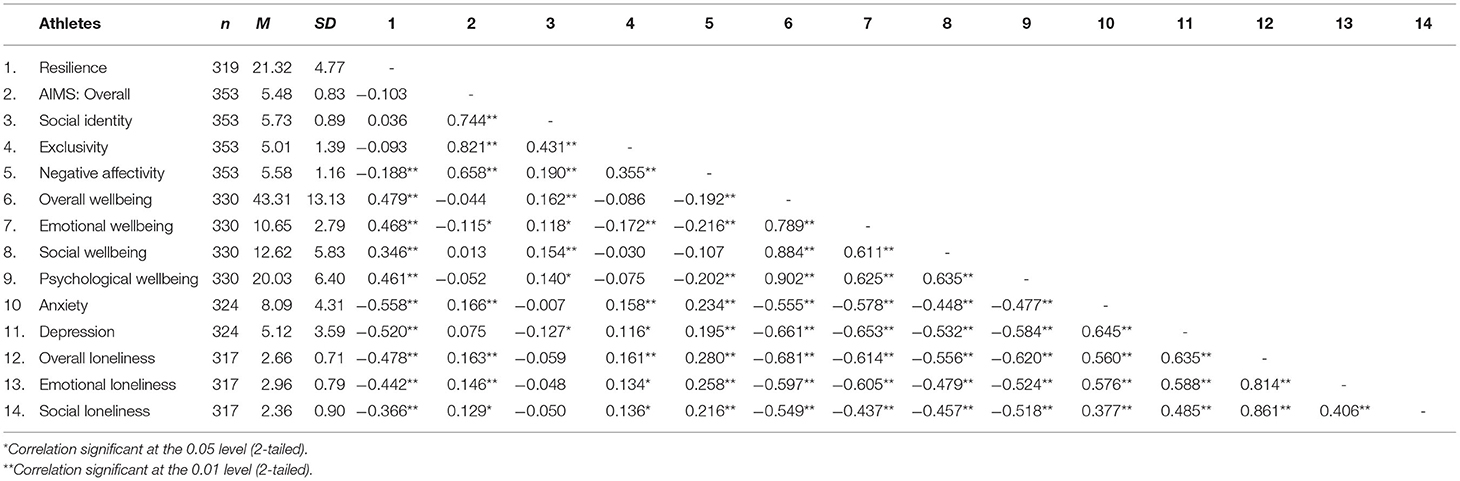
Table 2. Descriptive statistics and correlations for athletes.
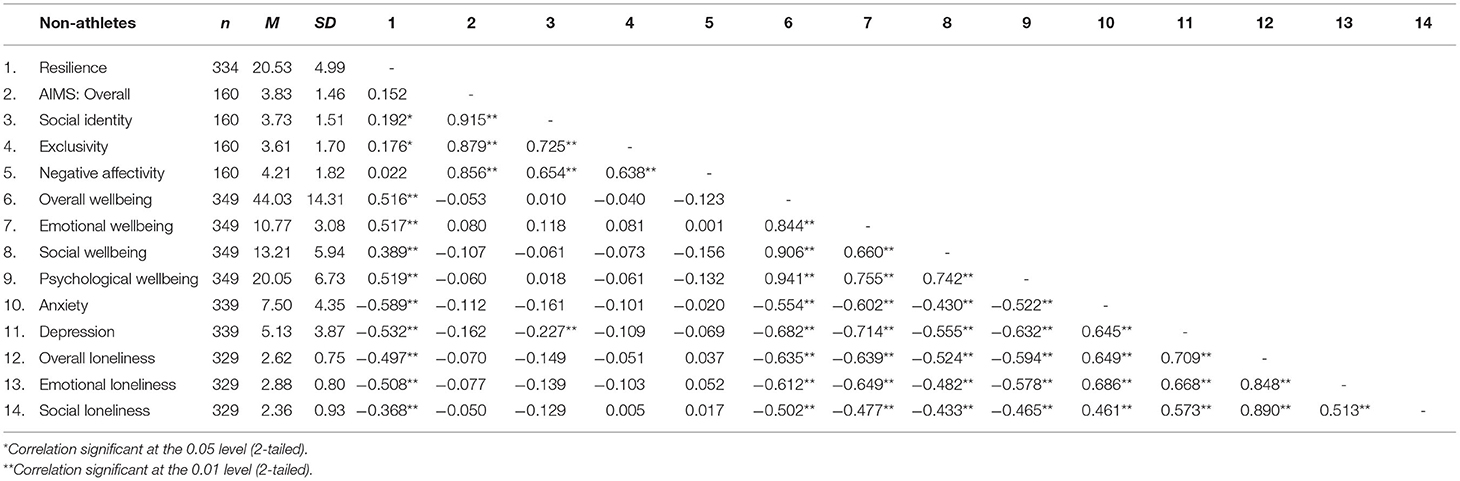
Table 3. Descriptive statistics and correlations for non-athletes.
All athletes and a subgroup of non-athletes (n = 160) were presented the AIMS. Whilst there was no correlation between non-athletes' AIMS-O and their mental health, athletes' AIMS-O a weak negative correlation with emotional wellbeing and weak positive correlations with HADS-A and each SLS variable which supports our second hypothesis. Each subfactor of AIMS was also significantly related to different aspects of mental health and illness (see Table 2 for descriptive statistics). Interestingly, AIMS-SI had a conflicting relationship with mental health and illness compared to the other AIMS variables. This meant that where significant relationships existed, increased AIMS-SI was related to better mental health whereas increased AIMS-O, AIMS-E and AIMS-NA scores were related to poorer mental health. A weak negative correlation also emerged between non-athletes' AIMS-SI and HADS-D: r(140) = −0.23, p = 0.007.
Pearson's correlations revealed that athletes' AIMS-NA and non-athletes AIMS-SI scores were related to both resilience and mental health. Therefore, a series of linear regressions (Newsom, 2020) and subsequent Sobel tests for mediation were conducted to identify whether the relationship between aspects of athletic identity and mental health remained after controlling for potential mediation from resilience (see Figures 4, 5 for regression path diagrams). Sobel tests revealed that resilience partially mediated the relationship between athletes AIMS-NA and overall wellbeing (z = −3.19, std. error = 0.30, p = 0.001), HADS-A (z = 3.26, std. error = 0.11, p = 0.001), HADS-D (z = 3.23, std. error = 0.09, p = 0.001), and Lone-O (z = 3.03, std. error = 0.03, p = 0.002) and fully mediated the relationship between non-athletes' AIMS-SI scores and their HADS-D (z = −2.17, std. error = 0.13, p = 0.030).
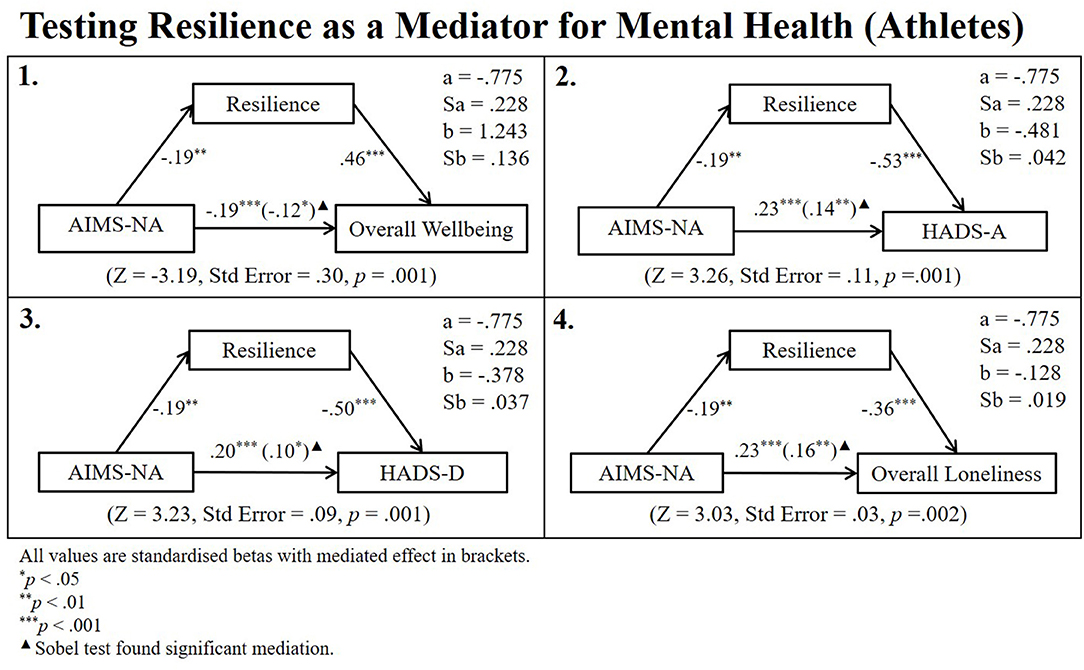
Figure 4. Regression path diagram testing resilience as a mediator for athlete sample.
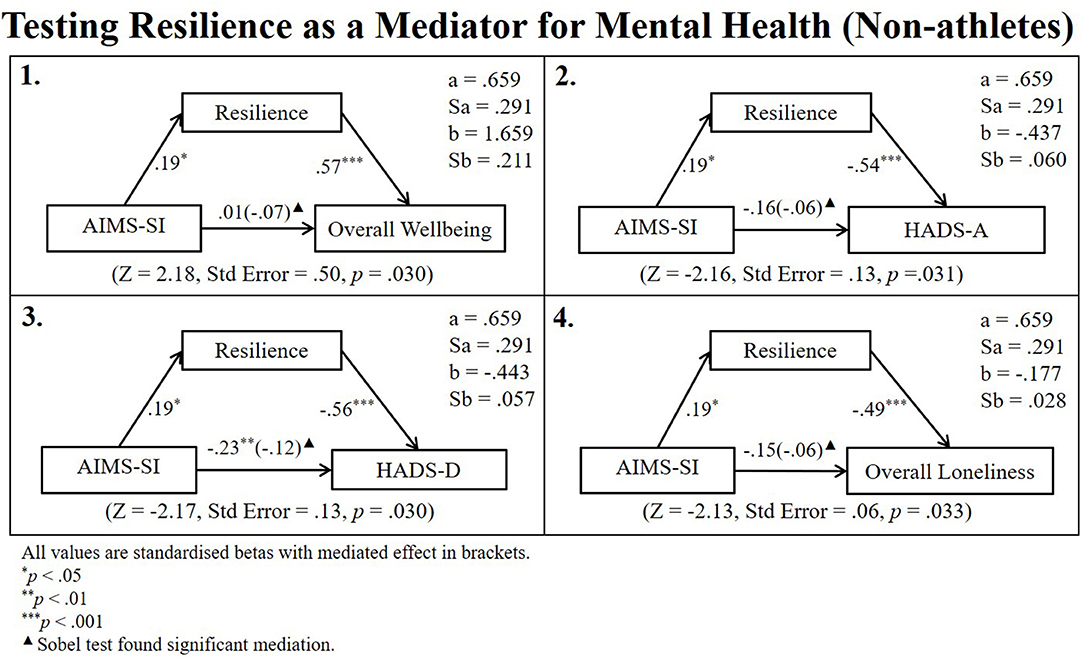
Figure 5. Regression path diagram testing resilience as a mediator for non-athlete sample.
A two-way ANOVA was conducted to explore potential differences between males and females, athletes and non-athletes. No significant interaction was observed between the independent variables nor was there a difference between athletes and non-athletes. However, a gender difference emerged with males having greater resilience (M = 21.42, n = 301, SD = 4.89) than females (M = 20.48, n = 352, SD = 4.87): [F(1, 649) = 4.37, p = 0.037, partial η2 = 0.007].
Independent sample's t-tests were conducted to test differences in athletic identity between athletes and non-athletes. As expected, there was a large effect with athletes scoring significantly higher than non-athletes on AIMS-O [t(206.39) = 13.34, d = 1.63, p < 0.001 two-tailed]; AIMS-SI [t(210.36) = 15.60, d = 1.92, p < 0.001 two-tailed]; AIMS-E [t(259.77) = 9.15, d = 1.15, p < 0.001 two-tailed]; and AIMS-NA [t(219.16) = 8.78, d = 1.17, p < 0.001 two-tailed]. These results survived Bonferroni adjustment for multiple comparisons (adjusted alpha level = 0.013).
Two-way ANOVAs reported no differences in mental health other than for HADS-A where there was an effect of group (athlete/non-athlete): [F(1, 659) = 6.05, p = 0.014, partial η2 = 0.009]; gender: [F(1, 659) = 15.16, p < 0.001, partial η2 = 0.022]; but no interaction between the two: [F(1, 659) = 0.09, p = 0.767]. Athletes (M = 8.10, n = 324, SD = 4.31) were more anxious than non-athletes (M = 7.50, n = 339, SD = 4.35) and females (M = 8.32, n = 359, SD = 4.35) were more anxious than males (M = 7.15, n = 304, SD = 4.25). A final series of regressions were conducted to test whether the difference in athlete and non-athlete HADS-A was mediated by AIMS. Figure 6 depicts the regression path diagram for these relationships. After controlling for the confounding effect of gender, there was no evidence that AIMS-O, AIMS-SI or AIMS-E mediated the difference in athlete and non-athlete HADS-A. However, the difference in athlete and non-athlete HADS-A went from significant to non-significant when AIMS-NA was added to the model. A significant Sobel test confirmed this was evidence of complete mediation by AIMS-NA (z = −2.82, Std Error = 0.20, p = 0.005).
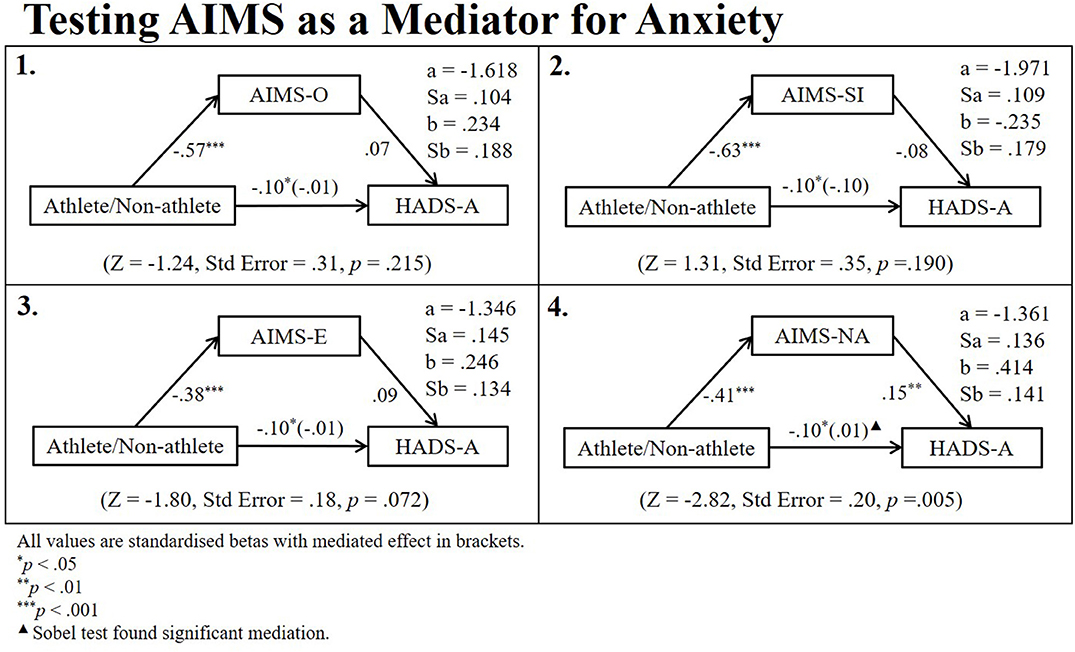
Figure 6. Regression path diagrams testing aims as mediators for the difference in athlete and non-athlete anxiety.
The current study investigated resilience and athletic identity to improve our understanding of athlete mental health as we emerged from a COVID-19 lockdown. The findings support the first hypothesis—resilience would be positively correlated with mental health. For athletes, overall athletic identity was weakly positively correlated with anxiety and loneliness but had no relationship with wellbeing or depression, which partially supports the second hypothesis. Finally, there was no difference observed in the resilience levels of athletes and non-athletes, meaning the third null hypothesis was not rejected.
Until now, there was a dearth of research on athlete resilience during non-normative transitions. Existing studies of athlete resilience have used samples of athletes who finished training shortly prior to data collection or who otherwise had regular and ongoing involvement in sport (Guillén and Laborde, 2014; Laborde et al., 2016). As such, the resilience reported by these athletes may not have been representative of those going through a transition away from sport. We present evidence that during transitionary times such as COVID-19, there is no significant difference between the resilience of athletes and non-athletes. Instead, we propose that athlete resilience is circumstantial and may fluctuate depending on their current level of involvement in sport. The high prevalence of depression and substance abuse seen in athletes (particularly those performing at an elite level) during injuries or post-retirement would offer support to this claim (Alfermann et al., 2004; Appaneal et al., 2009). As well, the stigma toward mental health in sport and the sport-ethic demanding that athletes “put on a brave face” prevents some of those who are struggling from speaking out thus masking the true extent of mental illness in this population (Caddick and Ryall, 2012; Hilliard et al., 2020). We urge caution when advocating that sport participation develops resilience as there are evidently times when this is not the case.
The comparable levels of resilience between athletes and non-athletes were reflected in their mental health. Athletes reported similar levels of depression, loneliness and wellbeing as non-athletes. Alternatively, whilst males reported greater resilience and less anxiety than females, athletes had greater levels of anxiety than non-athletes despite having more males in the sample which signals that athlete specific stressors likely influenced their mental health. Specifically, 53% of athletes reported experiencing at least mild anxiety symptoms compared to 45% of non-athletes (see Table 1). These statistics are substantial enough to be a cause for concern for both athletes and non-athletes alike with social determinants likely contributing to why these figures are so high. The pressure of having to provide for children or care for those suffering from COVID-19 amid an unprecedented economic crisis has placed an incredible burden on the population. Concomitantly, job security has been drastically reduced with many individuals still facing the threat of redundancy. Indeed, when this survey was conducted, around 25% of the UK workforce were enrolled on the furlough scheme (Office for National Statistics, 2020)—an indication that job security was a wide-spread concern shared by athletes and non-athletes alike. However, these social pressures are not unique to athletes, and so cannot explain the significant difference in athlete and non-athlete anxiety. Instead, a psychological basis for the difference in athlete and non-athlete anxiety is more likely—a difference we attribute to their heightened athletic identity.
Research has shown that over-reliance on one's status as an athlete, can cause identity foreclosure (Murphy et al., 1996) and restrict the formation of a balanced and well-rounded sense-of-self causing some athletes psychological difficulties when they cannot compete in their sport. Our findings, depicted in Figure 6, provide evidence that after controlling for gender, negative affectivity—a subfactor of overall athletic identity—fully mediated the relationship between athletic status and anxiety. This finding infers that pandemic lockdown posed a significantly greater risk for athletes than non-athletes due to the high level of negative affectivity that comes with the athlete role. Alas, the cross-sectional nature of our study and lack of comparison data from before the lockdown limits the extent to which we can attribute these findings explicitly to the pandemic. To validate this evidence, future research should aim to follow athletes over time to try and capture athletic identity and mental health as athletes move from a period of uninhibited participation through a non-normative transition away from sport.
Another interesting finding was that whilst negative affectivity and exclusivity were associated with poor mental health, greater social identity was associated with more positive outcomes. Exclusivity and negative affectivity consider the degree to which an athlete's self-worth and emotional state are dependent on their ability to excel at sport (Brewer et al., 1993; Murphy et al., 1996). Moreover, an athlete's self-worth and their emotional state are more heavily influenced by the ability to play sport when they are intrinsically rather than extrinsically motivated to do so through social or societal pressures (Pelletier et al., 1995; Ryan and Deci, 2017). It is possible that athlete motives influence which aspects of athletic identity are developed thus causing different athletes to experience transitions differently. Research investigating the impact of motivation for athletic identity development would greatly enhance our understanding of athlete mental health and the risk factors for poor adaptation to transitions.
Our study comes with a number of limitations. First, we relied heavily on the use of self-report measures which in the past has led to under-reporting of disorders due to the stigma surrounding mental health in sport (Bauman, 2016; Hilliard et al., 2020). We mitigated this risk by preserving participant anonymity throughout making under-reporting of symptoms unlikely. Concurrently, collecting a large sample supports the likelihood that these findings offer an accurate and reliable representation of athlete mental health. Nevertheless, an additional (virtual) face-to-face interview would have improved the reliability of our findings. Second, it is possible that highly active non-athletes may have experienced some benefits of exercise for mental health and as such could have obscured significant differences between groups. Our ability to capture highly active individuals in the non-athlete group was limited as non-athletes were not asked how frequently they exercised. Having said that, these individuals were likely few in number and by strict definition, not athletes in sport and are therefore beyond our research questions. Finally, without pre-pandemic data for comparison, we cannot explicitly say that mental health has been significantly affected since the outbreak of COVID-19. Also, the dynamic nature of mental health means these statistics are liable to have changed in the months since the lockdown and will continue to change in perpetuity. Despite this, our findings make an important contribution to the field by “time-stamping” athlete mental health as the country emerged from an unprecedented national lockdown situation.
This research contributes to the growing body of literature on sport participation and mental health, with the novel addition of capturing demographic and psychological factors during emergence from a national lockdown. Contrary to existing literature, athletes did not have greater resilience than non-athletes, possibly explained by the complex and likely uncomplimentary role that a narrow athletic identity with high negative affectivity serves during transitionary periods. Given social distancing measures are being intermittently eased and reinstated, the fate of both professional and amateur sport still hangs in the balance. Our findings have shown that it is now particularly important for research to continue to monitor and support the mental health of athletes.
Cohen's d was calculated using the following formula (Howell, 2002):
The square root of pooled variance was calculated using:
Sobel tests used the following formula presented by MacKinnon and Dwyer (1993) where a = raw, unstandardised regression co-efficient for the relationship between the IV and mediator; Sa = standard error of a; b = raw coefficient for the relationship between mediator and DV when controlling for all other IVs; Sb = Standard error of b:
The data has been made available on Figshare online repository. The following DOI can be used to access the data: https://doi.org/10.6084/m9.figshare.14501361.v1.
The studies involving human participants were reviewed and approved by Ulster University Research Ethics Filter Committee. The patients/participants provided their written informed consent to participate in this study.
CK, GB, and SS conceptualised the study with the same authors conducting early pilot work and data collection. CK processed the data. Analysis was conducted by CK and GP. All authors contributed to writing the paper.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Thank you to the sporting organisations and governing bodies that aided the authors in participant recruitment. In particular, the following organisations supported the authors by publicly promoting the study via their social media channels: Athletics NI, Hockey Ireland, the Irish Football Association, Netball NI, NI Running, Rowing Ireland, Swim Ireland. Thank you also to Gareth Fullerton at Belfast live for taking interest in our research and aiding recruitment through publication of his newspaper article. Finally, thanks to all participants who gave their time to complete our survey.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fspor.2021.612532/full#supplementary-material
Alfermann, D., Stambulova, N., and Zemaityte, A. (2004). Reactions to sport career termination: a cross-national comparison of German, Lithuanian, and Russian athletes. Psychol. Sport Exerc. 5, 61–75. doi: 10.1016/S1469-0292(02)00050-X
Appaneal, R. N., Levine, B. R., Perna, F. M., and Roh, J. L. (2009). Measuring post-injury depression among male and female competitive athletes. J. Sport Exerc. Psychol. 31, 60–76. doi: 10.1123/jsep.31.1.60
Bauman, N. J. (2016). The stigma of mental health in athletes: are mental toughness and mental health seen as contradictory in elite sport? Br. J. Sports Med. 50, 135–136. doi: 10.1136/bjsports-2015-095570
Biddle, S. J., Mutrie, N., and Gorely, T. (2015). Psychology of Physical Activity: Determinants, Well-Being, and Interventions. London: Routledge.
Breeman, S., Cotton, S., Fielding, S., and Jones, G. T. (2015). Normative data for the hospital anxiety and depression scale. Qual. Life Res. 24, 391–398. doi: 10.1007/s11136-014-0763-z
Brewer, B. W., Van Raalte, J. L., and Linder, D. E. (1993). Athletic identity: Hercules' muscles or Achilles heel? Int. J. Sport Psychol. 24, 237–254. doi: 10.1037/t15488-000
Caddick, N., and Ryall, E. (2012). The social construction of “mental toughness”—a fascistoid ideology? J. Philos. Sport 39, 137–154. doi: 10.1080/00948705.2012.675068
De Jong Gierveld, J. D. J., and Van Tilburg, T. V. (2006). A 6-item scale for overall, emotional, and social loneliness: confirmatory tests on survey data. Res. Aging 28, 582–598. doi: 10.1177/0164027506289723
Field, A. (2013). Discovering Statistics Using IBM SPSS Statistics. Thousand Oaks, CA: Sage. Available online at: https://us.sagepub.com/en-us/nam/discovering-statistics-using-ibm-spss-statistics/book260423
Fletcher, D., and Sarkar, M. (2013). Psychological resilience: a review and critique of definitions, concepts, and theory. Eur. Psychol. 18:12. doi: 10.1027/1016-9040/a000124
Fletcher, D., and Sarkar, M. (2016). Mental fortitude training: an evidence-based approach to developing psychological resilience for sustained success. J. Sport Psychol. Action 7, 135–157. doi: 10.1080/21520704.2016.1255496
Grove, J. R., Lavallee, D., and Gordon, S. (1997). Coping with retirement from sport: the influence of athletic identity. J. Appl. Sport Psychol. 9, 191–203. doi: 10.1080/10413209708406481
Guillén, F., and Laborde, S. (2014). Higher-order structure of mental toughness and the analysis of latent mean differences between athletes from 34 disciplines and non-athletes. Pers. Individ. Dif. 60, 30–35. doi: 10.1016/j.paid.2013.11.019
Hilliard, R. C., Watson, J. C., and Zizzi, S. J. (2020). Stigma, attitudes, and intentions to seek mental health services in college student-athletes. J. Am. Coll. Health 1–10. doi: 10.1080/07448481.2020.1806851
Keyes, C. L. (2005). Mental illness and/or mental health? Investigating axioms of the complete state model of health. J. Consult. Clin. Psychol. 73:539. doi: 10.1037/0022-006X.73.3.539
Keyes, C. L. M. (2009). Atlanta: Brief Description of the Mental Health Continuum Short Form (MHC-SF). Available online at: https://www.aacu.org/sites/default/files/MHC-SFEnglish.pdf (accessed March 30, 2021).
Laborde, S., Guillén, F., and Mosley, E. (2016). Positive personality-trait-like individual differences in athletes from individual-and team sports and in non-athletes. Psychol. Sport Exerc. 26, 9–13. doi: 10.1016/j.psychsport.2016.05.009
Lippke, S., Fischer, M. A., and Ratz, T. (2021). Physical activity, loneliness, and meaning of friendship in young individuals: a mixed-methods investigation prior to and during the COVID-19 pandemic with three cross-sectional studies. Front. Psychol. 12:146. doi: 10.3389/fpsyg.2021.617267
MacKinnon, D. P., and Dwyer, J. H. (1993). Estimating mediated effects in prevention studies. Eval. Rev. 17, 144–158. doi: 10.1177/0193841X9301700202
Murphy, G. M., Petitpas, A. J., and Brewer, B. W. (1996). Identity foreclosure, athletic identity, and career maturity in intercollegiate athletes. Sport Psychol. 10, 239–246. doi: 10.1123/tsp.10.3.239
Newsom, J. T. (2020). Psy 523/623 Structural Equation Modelling. Available online at: http://web.pdx.edu/~newsomj/semclass/ho_mediation.pdf (accessed April 8, 2021).
Ntoumanis, N., Edmunds, J., and Duda, J. L. (2009). Understanding the coping process from a self-determination theory perspective. Br. J. Health Psychol. 14, 249–260. doi: 10.1348/135910708X349352
Office for National Statistics (2020). Comparison of Furloughed Jobs Data: May to July 2020. Available online at: https://www.ons.gov.uk/businessindustryandtrade/business/businessservices/articles/comparisonoffurloughedjobsdata/maytojuly2020 (accessed March 30, 2021).
Pelletier, L. G., Tuson, K. M., Fortier, M. S., Vallerand, R. J., Briere, N. M., and Blais, M. R. (1995). Toward a new measure of intrinsic motivation, extrinsic motivation, and amotivation in sports: the Sport Motivation Scale (SMS). J. Sport Exerc. Psychol. 17, 35–53. doi: 10.1123/jsep.17.1.35
Rejeski, W. J., and Brawley, L. R. (1988). Defining the boundaries of sport psychology. Sport Psychol. 2, 231–242. doi: 10.1123/tsp.2.3.231
Rice, S. M., Purcell, R., De Silva, S., Mawren, D., McGorry, P. D., and Parker, A. G. (2016). The mental health of elite athletes: a narrative systematic review. Sports Med. 46, 1333–1353. doi: 10.1007/s40279-016-0492-2
Ronkainen, N. J., Kavoura, A., and Ryba, T. V. (2016). A meta-study of athletic identity research in sport psychology: current status and future directions. Int. Rev. Sport Exerc. Psychol. 9, 45–64. doi: 10.1080/1750984X.2015.1096414
Ryan, R. M., and Deci, E. L. (2017). Self-Determination Theory: Basic Psychological Needs in Motivation, Development, and Wellness. New York, NY: Guilford Publications.
Samuel, R. D., Tenenbaum, G., and Galily, Y. (2020). The 2020 coronavirus pandemic as a change-event in sport performers' careers. Front. Psychol. 11:567966. doi: 10.3389/fpsyg.2020.567966
Sanders, G., and Stevinson, C. (2017). Associations between retirement reasons, chronic pain, athletic identity, and depressive symptoms among former professional footballers. Eur. J. Sport Sci. 17, 1311–1318. doi: 10.1080/17461391.2017.1371795
Shannon, S., Breslin, G., Haughey, T., Sarju, N., Neill, D., Lawlor, M., et al. (2019). Predicting student-athlete and non-athletes' intentions to self-manage mental health: testing an integrated behaviour change model. Mental Health Prevent. 13, 92–99. doi: 10.1016/j.mhp.2019.01.006
Smith, B. W., Dalen, J., Wiggins, K., Tooley, E., Christopher, P., and Bernard, J. (2008). The brief resilience scale: assessing the ability to bounce back. Int. J. Behav. Med. 15, 194–200. doi: 10.1080/10705500802222972
Snaith, R. P. (2003). The hospital anxiety and depression scale. Health Qual. Life Outcomes 1, 1–4. doi: 10.1186/1477-7525-1-1
Stambulova, N. B. (2003). Symptoms of a Crisis-Transition: A Grounded Theory Study. Available online at: http://urn.kb.se/resolve?urn=urn:nbn:se:hh:diva-5911 (accessed February 26, 2021).
Stambulova, N. B. (2017). Crisis-transitions in athletes: current emphases on cognitive and contextual factors. Curr. Opin. Psychol. 16, 62–66. doi: 10.1016/j.copsyc.2017.04.013
Stambulova, N. B., Schinke, R. J., Lavallee, D., and Wylleman, P. (2020). The COVID-19 pandemic and Olympic/Paralympic athletes' developmental challenges and possibilities in times of a global crisis-transition. Int. J. Sport Exerc. Psychol. 1–10. doi: 10.1080/1612197X.2020.1810865
Wheaton, B. (1990). Life transitions, role histories, and mental health. Am. Sociol. Rev. 55, 209–223. doi: 10.2307/2095627
World Health Organisation (2018). Mental Health: A State of Well-Being. Available online at: https://www.who.int/news-room/fact-sheets/detail/mental-health-strengthening-our-response (accessed March 30, 2021).
Wylleman, P., Alfermann, D., and Lavallee, D. (2004). Career transitions in sport: European perspectives. Psychol. Sport Exerc. 5, 7–20. doi: 10.1016/S1469-0292(02)00049-3
Keywords: athlete, athletic identity, resilience, wellbeing, depression, anxiety, loneliness
Citation: Knowles C, Shannon S, Prentice G and Breslin G (2021) Comparing Mental Health of Athletes and Non-athletes as They Emerge From a COVID-19 Pandemic Lockdown. Front. Sports Act. Living 3:612532. doi: 10.3389/fspor.2021.612532
Received: 30 September 2020; Accepted: 14 April 2021;
Published: 20 May 2021.
Edited by:
Robert Morris, University of Stirling, United KingdomReviewed by:
Emily Cartigny, Talented Athlete Scholarship Scheme, United KingdomCopyright © 2021 Knowles, Shannon, Prentice and Breslin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christopher Knowles, a25vd2xlcy1jMkB1bHN0ZXIuYWMudWs=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.