 Ruth Amaabadek Atengdem
Ruth Amaabadek Atengdem Seth Mensah Abobi
Seth Mensah Abobi Elliot Haruna Alhassan
Elliot Haruna Alhassan- 1Institute of Local Government Studies, Tamale, Ghana
- 2Department of Aquaculture & Fisheries Sciences, Faculty of Biosciences, University for Development Studies, Tamale, Ghana
Access to improved water and sanitation is a major conduit to meeting global development goals. This has resulted in the proliferation of various improved water and sanitation interventions in most communities of the world. Little evidence, however, exists in Ghana to reveal the extent to which these interventions are being adopted and sustained by the communities they are intended to benefit. This study, therefore, sought to assess the adoption of water and sanitation interventions and their sustainability. The mixed method approach, guided by the concurrent mixed method design was implemented in the Bongo District. Quantitative data were obtained from 389 sampled households in the District with the aid of a survey. Thereafter, univariate and bivariate statistics were used to analyze the quantitative data with the aid of STATA version 15. The qualitative data on the other hand was collected from officials of the District Water and Sanitation Management Team (DWSMT) and members of the water and sanitation management committees at the community level through key informant interviews and focus group discussions. The qualitative data was analyzed manually using thematic analysis. The study found a high adoption rate of both water and sanitation interventions in the Bongo District. The household demographic characteristics that were found to have a strong positive association with the adoption of improved water or sanitation interventions included the sex of household head, age, level of education and household size among others. Major factors influencing the adoption of water and sanitation interventions found included the knowledge of the derived benefits of the facilities and education on the use of the facilities. The study also found that as part of activities geared towards sustainability, most community members were involved in deciding the appropriateness of these water and sanitation facilities; siting of the facilities; and cash contributions. The study, therefore, concludes that the extent of adoption of water and sanitation in the Bongo District is relatively high and communities were involved to some extent to engender the sustainability of the facilities.
Introduction
Over the years, the standard of living of communities which goes beyond their basic human needs can be sustainable only if their demand for improved water and sanitation as well as consumption standards have regard for socio-demographic variability and ecological sustainability (Bazaanah, 2019). Yet many peri-urban and rural communities in Africa most especially Sub-Saharan Africa (SSA) live below the world’s ecological means, regarding their adoption, utilization and sustainability of quality drinking water and improved sanitation (United Nations, 2018).
Many countries across the world have embraced approaches towards achieving sustainable local development by ensuring that basic needs such as water and sanitation opportunities are available and extended to households in deprived communities to satisfy their aspirations for a better life through the ability to adopt and utilize water and sanitation facilities available to them (Brundtland Commission, 2014). Furthermore, the effective distribution of water resources and promotion of water quality at the community level can only be pursued if demographic developments and population increases are in harmony with the changing productive potential of their ecosystems (Solane and Jouravlev, 2006). This is essential for poverty reduction and human development, especially in sub-Saharan Africa where poverty is more widespread in rural areas than in cities (World Bank, 2018). Households in rural communities are powerless concerning common constraints of which access to water production and sanitation are not an exception (Food and Agriculture Organization – FAO, 2017). Also, water and sanitation are human rights and common goods, yet rural households have difficulties in accessing and adopting/utilizing portable water and improved sanitation (Bazaanah, 2019). According to Todaro and Smith (2014), water and sanitation are at the very core of sustainable development, and pivotal to the survival of people and their ecosystems. As a result, civil society actors are advocating for better rural water, sanitation and ecological management (Kramer and Pahl-Wostl, 2014). Furthermore, universal access to portable water and curtailing open defecation seem to be eluding rural areas of sub-Saharan Africa (United Nations Economic and Social Council – UNESCO, 2017). Significant inequalities persist within countries including between urban and rural, between sub-national regions and between the richest and the poorest. For instance, in urban areas of Africa, 2 out of 5 people lack safely managed drinking water, 2 out of 3 people lack safely managed sanitation, and half the population lacks basic hygiene services. In rural areas, 4 out of 5 people lack safely managed drinking water, 3 out of 4 people lack safely managed sanitation, and 7 out of 10 lack basic hygiene services (UNICEF/WHO, 2022). This puts the health of populations at risk of disease infection (World Health Organization – WHO, 2014) since access to quality drinking water relates to all aspects of human growth and development (Awoke, 2012). Also, most households in sub-Saharan Africa lack proper sanitation and which over the years has seen an increase in open defecation from 204 million to 220 million resulting in several environmentally endemic health problems (Osumanu et al., 2019). For instance, 200, 000 children under the age of five die from diarrhoea annually in sub-Saharan Africa, whilst the numbers dying from cholera are similarly high because of poor sanitation and unsafe water supplies (World Health Organization – WHO, 2014).
Globally, access to potable water and improved sanitation services has become a topical issue in the community development agenda due to their acknowledgement as basic needs and their ability to support human life development (Fielmua et al., 2019). Yet, 884 million people worldwide do not have access to improved sources of drinking water whilst 2.5 billion lack access to improved sanitation facilities (World Health Organization – WHO, 2014). Whilst these numbers shed light on a worrying situation, the reality is much worse, as millions of poor people living in informal settlements are simply missing from national statistics (Bazaanah, 2019). The essential needs of a vast number of people in developing countries most importantly Africa regarding food, water, clothing, shelter, jobs and sanitation are not being met, and worst still, beyond these basic needs, rural people have legitimate aspirations for improved quality of life. A world in which poverty and water inequity are endemic would always be predisposed to ecological and other crises (United Nations, 2018).
In Ghana, adoption and utilization of improved sanitation appear better in urban areas (25%) than rural communities (17%) and open defecation is more widespread (70%) among the poorest rural household population in Ghana (Ghana Statistical Service – GSS, 2018 cited in Bazaanah, 2019). Moreover, according to Bazaanah (2019), about (12%) of residents in northern Ghana lack basic sanitation whilst (50%) lack safe drinking water and therefore use unimproved water as drinking water sources. “An improved source includes a public standpipe or outdoor tap, a protected well, a protected spring, or rainwater. However, these sources do not completely prevent water borne diseases. Children have high mortality rates and serious health issues due to the lack of safe water and sanitation access” (German Industry and Commerce in Ghana – GICG, 2018).
The situation is clear in the Bongo District of Ghana, the study area where communities are constrained with access to improved water and sanitation. Communities in the Bongo District do not only need “improved” but also “safe” water and sanitation sources and facilities as well as the ability of households to adopt such facilities or interventions for sustainability. In ensuring sustainability, the Community Water and Sanitation Agency (CWSA) and the District Assemblies (DAs) have established decentralized sub-structures including the Water and Sanitation (WATSAN) Committees and Water and Sanitation Management Teams (WSMTs) to manage water and sanitation delivery at the local level (Community Water and Sanitation Agency – CWSA, 2015).
There have been several studies on access to water and sanitation in deprived Districts and communities in Ghana. Studies by Asiedu (2015), Bazaanah (2019), Osumanu (2010), Braimah et al. (2016), Fielmua et al. (2019) and Osumanu et al. (2019) have enhanced the literature on the importance of household access and utilization of improved water and sanitation sources and facilities and the effective local management systems of these facilities to enhance household living conditions.
However, there is a paucity of information on household adoption and sustainability of water and sanitation facilities interventions. It is to address this gap in the literature that this study sought to assess the socio-demographic factors affecting the adoption of water and sanitation facilities and their sustainability among households in the Bongo District of the Upper East Region of Ghana.
Bongo District is one of the districts located in the Upper East Region of Ghana. The District has recorded the implementation and execution of most water and sanitation programmes in the Region by government and Non-Governmental Organizations (NGOs) yet the issue of adoption/utilization and sustainability of facilities still lingers among beneficiaries in most of the communities in the District (Ghana Statistical Service – GSS, 2018). According to Issah-Bello (2011), access to water and sanitation and lack of coordination among NGOs do not engender sustainability but instead community involvement coupled with proactive WSMTs can promote the adoption, utilization and above all sustainability of water and sanitation facilities among households.
Despite water and sanitation playing an essential role in meeting the basic needs of human life as well as instigating human growth and development, there is little attention paid in the literature to household adoption, utilization and sustainability of water and sanitation facilities. In other words, there is limited literature on the subject. It is therefore against this background that the study seeks to assess the socio-demographic factors affecting the adoption/utilization and sustainability of water and sanitation facilities interventions among households in the Bongo District of Ghana.
The main objective of the study was to assess the factors that affect the adoption and sustainability of water and sanitation facilities interventions in the Bongo District. Specifically, the study sought to (i) determine the association between the demographic characteristics of beneficiaries and their adoption of water and sanitation interventions; (ii) assess the factors that affect the adoption of water and sanitation facilities in the Bongo District; and (iii) describe the level of community involvement in water and sanitation facilities’ interventions.
Methodology
Study area
Bongo District is one of the 15 Districts of the Upper East Region. It was established in 1988 by Legislative Instrument 1,446 (LI 1446) with Bongo as its capital (Ghana Statistical Service, 2014) as indicated in Figure 1. The District lies between the longitude 0.45° W and the latitude 10.50° N and has a complete land area of 459.5 square kilometres (Ghana Statistical Service, 2014). The Bongo District shares borders with Burkina Faso to the north, Kassena-Nankana East District to the west, Bolgatanga Municipal to the southwest and Nabdam District to the southeast (Ghana Statistical Service, 2014). The climate of the District is similar to that experienced in other parts of the Region, semi-arid with one period of rainfall followed by a long dry season with mean temperatures between 25 and 40°C (Ghana Statistical Service, 2014).
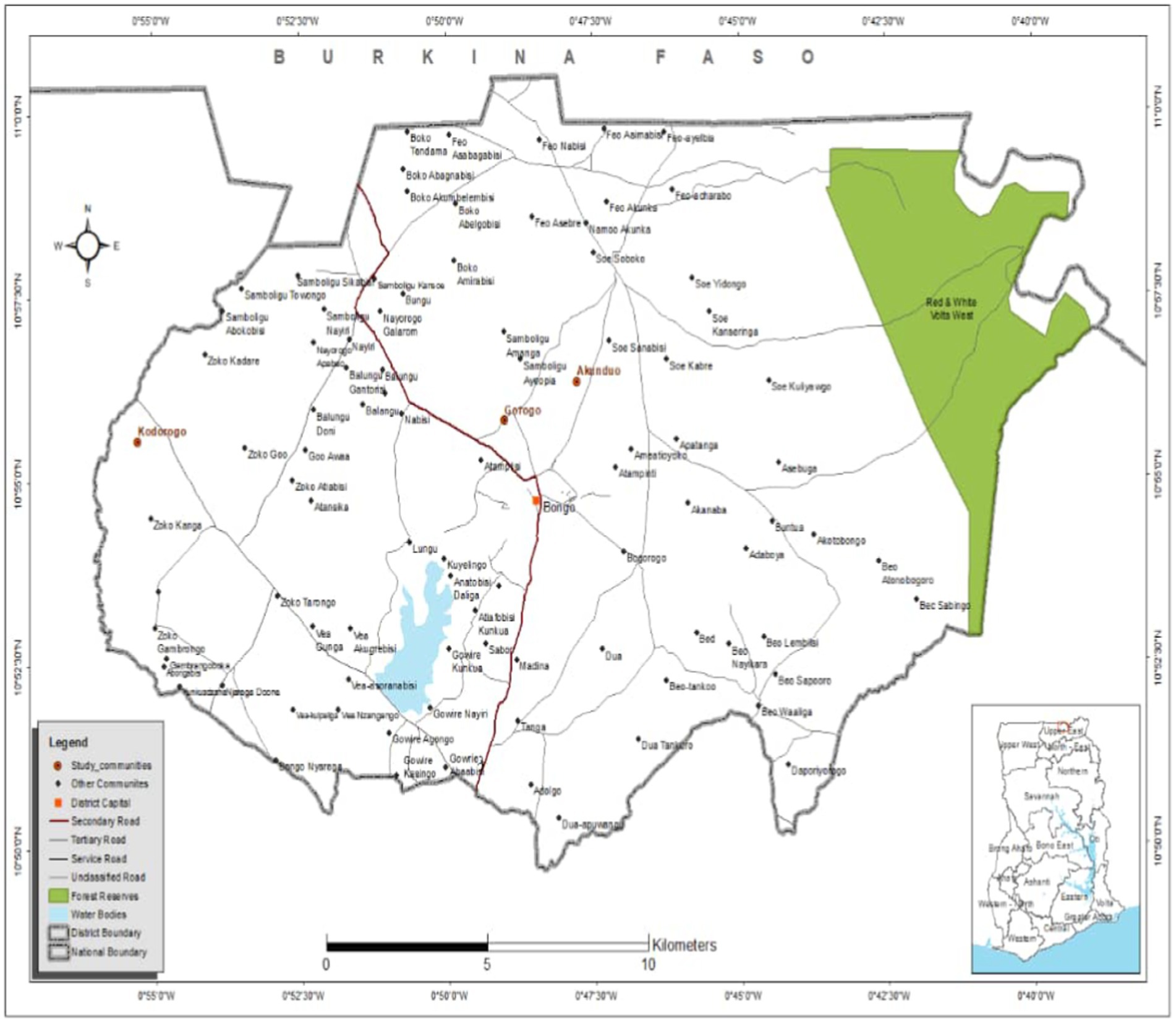
Figure 1. A map of the study area.
The Bongo District comprises 56 communities with 15, 188 households (Ghana Statistical Service, 2014). Most households rely on groundwater collected from drilled boreholes or hand-dug open wells for their domestic water. Beneath the entire District lies a bedrock of fluoride-rich granitoid. These rocks have well-developed fractures that make the drilling of boreholes and wells possible. Nonetheless, about half of the boreholes in Bongo District have unsafe fluoride contamination levels. As many as 46% exceeded the maximum limit of 1.5 mg/L of fluorides considered safe for human consumption by the WHO. According to a 2009 water quality study on 278 functional boreholes in the District, less than 4% of boreholes within the expanse known as the Bongo Granite Formation have fluoride levels within the safe margin (Alfredo et al., 2014). As of 2016, 93% of the District’s 498 boreholes were functional whilst 7% were broken down. The District, in addition, has three small-town water systems and three limited mechanized small-town water systems (Bonda, 2016).
On sanitation, the District is constrained with household toilet facilities. Meanwhile, some institutions including health care facilities and schools lack access to toilets and other sanitary facilities. The District, as of August 2019, recorded Open Defecation Free (ODF) status in 53 communities out of 157 communities (UNICEF et al., 2019).
Research design and approach
The study adopted the mixed method approach and is guided by the concurrent mixed method design. The mixed method approach to research is ideal for this study because of the nature of the objectives. Thus, the issue under evaluation in this study can best be examined using both quantitative and qualitative methods. Concerning the specific objectives of the study, objective one that was analytical required only quantitative information, first on the demographic characteristics of beneficiary households and then their adoption or otherwise of improved water and sanitation sources/interventions. Objectives two and three, however, were addressed with both quantitative and qualitative data from the study participants. For instance, objective two specifically required both numerical and textual data on the factors affecting the adoption of improved water and sanitation interventions whilst objective three required data on the level of community involvement in the design and implementation of water and sanitation projects/interventions.
Among the different types of mixed-method designs, this study employed the parallel convergent design (Hesse-Biber, 2010; Creswell, 2014). The study was designed in line with parallel convergence because of the need to supplement statistical evidence relating to variables on factors affecting the adoption/utilization of water and sanitation facilities as well as the level of community involvement in water and sanitation facilities’ interventions (Creswell, 2014). In order words, the parallel convergent design facilitated bringing clarity to the research problem and as well offer a deeper understanding of the findings on factors influencing the adoption/utilization of water and sanitation facilities and also the level at which communities were involved in the programme design leading to the provision of improved water and sanitation interventions in the Bongo District (Hesse-Biber, 2010).
Against this backdrop, two different investigations were carried out to find answers to the research questions of the study. Thus, both the qualitative and the quantitative investigations were carried out during the same phase of data collection and data analysis.
Types and sources of data
The study relied on both primary and secondary sources of data. Primary data sources included quantitative and qualitative data that were obtained from households in the District. The quantitative data comprised the socio-demographic information of the respondents, adoption/utilization of water and sanitation interventions, factors affecting adoption/utilization of water and sanitation facilities and the level of community involvement in the sustainability of water and sanitation interventions whilst the secondary data sources were information obtained from peer-reviewed journal articles, reports, thesis and conference proceedings to augment the primary data.
Study population and sampling
Target population
The target population of the study were divided into three groups. The first group included household heads in the Bongo District. The second group were members of the WSMTs at the local or community level whilst the third category comprised officials of the District Water and Sanitation Management Team (DWSMT). Household heads were included in the study because of their oversight responsibility in superintending over decisions regarding access to water and sanitation and their adoption and utilization. Additionally, since they represent the mouthpiece of each household in the District, they most likely were well informed of whether their various communities were consulted for their inputs leading to the establishment of improved water and sanitation facilities in the District. As such, their opinions on these matters were crucial to the success of the study, hence the justification for their inclusion. Members of the WSMTs at the community level and officials of the DWSMT were equally included in the study because they play the role of facilitating the provisioning and maintenance of improved water and sanitation interventions and as well ensuring that these interventions last longer in beneficiary communities to make them sustainable. Their expert views on the extent to which beneficiary communities were involved in the conception and design of water and sanitation interventions were therefore imperative to achieving the aim of this study.
Sampling strategy and sample size determination
Quantitative sample
A variety of sampling techniques were employed in this study to ensure a representative sample of the rather complex population of the study area. The sampling frame for the quantitative strand of the study therefore comprised all the households in the Bongo District from which household heads were selected. The data from the Ghana Statistical Service (2014), a total number of 15, 188 households was used as the sampling frame for the study. Given this, the study used the Yamane formula for the determination of sample sizes (Osahon and Kingsley, 2016) to arrive at the quantitative sample for the study. The determination of the sample size of households in the Bongo District for this study using Yamane’s formulae was therefore executed as follows.
Where n = sample size, N = sampling frame (15, 188) and α represent the margin of error which is 0.05 with a confidence level of 95%. By substituting 15, 188 and 0.05 into the formula:
A simple random sampling procedure was then employed to select three communities out of the fifty-six communities in the District for the study. This was done by putting in a basket, a list of all the fifty-six communities where the lottery method without replacement was used to select only 3 communities among the many. These communities included Kodorogo-Gingirigo, Gorogo-Asalako and Akunduo-Apeelinga. A household listing exercise revealed a total household population of 1,452 in these three communities (Table 1). A quota/proportionate sampling technique was therefore used to apportion the sample size among the three communities that were randomly sampled.

Table 1. Sample size from the selected communities in Bongo District that benefited from various forms of water and sanitation interventions.
Qualitative sample
The qualitative study employed a purposive sampling technique to select key informants and focus group discussants for the qualitative component of the study. Five key informants were included in the study comprising of persons with technical expertise on water and sanitation interventions or projects. Similarly, focus group participants were selected based on purposeful sampling comprising members of the WSMTs in study communities.
Methods and techniques of data collection
Survey
A questionnaire was used to survey household heads to collect quantitative data on all three objectives of the study. The questionnaire was fully structured with close-ended questions in nature. It was digitized electronically using the kobo toolbox where research assistants were recruited and trained on the concepts, study protocol and how to use the Computer Assisted Personal Interviewing approach (CAPI) to enhance easier administration and achieve quality data. The method of data collection, therefore, was the use of a face-to-face interviewer administration approach. The questionnaire contained three different parts. The first part comprised the social and demographic characteristics of households in the District. Part two comprised questions on factors affecting the adoption and utilization of water and sanitation interventions which were measured by assessing factors such as the distance to the water/sanitation facility, technical designs of the facilities, social norms/beliefs, personal habits, and knowledge of derived benefits among other factors. The final part, part three of the quantitative instrument specifically detailed questions on the level at which communities were involved in conceiving the design, implementation and sustainability of water and sanitation interventions. Indicators for measuring this objective included assessing their involvement in deciding the appropriateness of the water/sanitation facility, involvement in negotiating the siting of the facilities, involvement in cash contributions and labour, attendance to meetings relating to water and sanitation projects in the community among other indicators of community involvement in project implementation and sustainability. A Likert scale was therefore developed to measure the level of community involvement in water and sanitation interventions in the District. The scale for measuring ranged from “not involved at all” to “highly involved.”
Key informant interviews
Key informant interviews were used to collect qualitative data from 5 officials from the DWSMT on the level of community involvement in the design, implementation and sustainability of water and sanitation interventions. An in-depth interview guide was developed and sent to the respondents by mail where they self-administered the interview questions and returned them to the principal investigator. The questions contained in the interview guide were open-ended and unstructured in nature which ensured that the views of the key informants were explicitly sourced on how they engaged communities from the conception of ideas on water and sanitation interventions to the sustainability of the facilities. The instrument was in English since the target population for the key informant interview were all literate and could read and write in English.
Focus group discussion
Focus group discussions were held with the members of the water and sanitation management to collect qualitative data on the factors affecting the adoption of improved water and sanitation interventions. A total of three focus groups were constituted (Plates 1-3), thus one in each of the study communities of the District. Focus group participants usually range from six to twelve participants (Smithson, 2008). For this study, the focus groups ranged from 6 to 8 members and were held at times convenient to discussants and at an agreed location.
Data analysis
The study employed different data analytical tools to manage and analyze the raw data. The quantitative data was first thoroughly cleaned for errors, coded and assigned value labels using STATA version 15. Both descriptive and inferential analyses were carried out with the aid of the STATA analytical software. First and foremost, descriptive statistics were used to analyze the data on the demographic characteristics of household heads, sources of water for households, factors affecting the adoption/utilization of improved water and sanitation interventions and the level of community involvement in water and sanitation facilities’ interventions. These were all later presented using frequency and percentage distribution tables or bar graphs. Also, inferential statistics were used to analyze the association between the demographic characteristics of beneficiary households and their adoption of improved water and sanitation interventions. The chi-square statistical test and p-values aided the bivariate analysis where the data on the demographic characteristics was cross-tabulated with data on the adoption/utilization of improved water and sanitation interventions. These were later presented using chi-squared distribution tables. For the bivariate analysis, statistical significance was determined for each of the associations at a 95% confidence (5% significance) level.
Concerning the qualitative analysis, data collected from key informants and the focused group discussants/participants were organized into themes consistent with the quantitative data and then discussed to establish trends and patterns following the research question. The method of presentation was the use of narrative text.
Results and discussions
Demographic characteristics of beneficiary households
The results show that households headed by males constituted the majority (75.3%) of the study sample. For age categories of the household heads, those within the age group of 42–53 years were the majority (37.0%) whilst those in the age category of 18–29 recorded the least (13.9%). Household heads who were married were greater (69.2%) than those who were single (9.3%) or divorced/separated/widowed (21.6%) (Table 2). In terms of the level of education, the findings reveal that the highest form of education most of the household heads had attained was basic education (40.9%) whilst those with the educational attainment of Senior High School (SHS) and above recorded the least (20.6%). On average, the highest number of children in a household ranged from 0 to 3 (48.3%), households with 4–7 children were 47.0% whilst the least number of children in a household were households with 8 children and above (4.6%). Most of the households were about 6–10 members representing 54.38% of the sample whilst households with members above 10 constituted the least (8.0%). On average, most households reported earning monthly incomes below GHȻ 500 (66.6%). Christianity was the most dominant religion (66.1%) practised among households in the study area whilst Islam recorded the least (7.7%). Fewer numbers of households (8.2%) reported having known persons with disabilities than those without (91.8%).
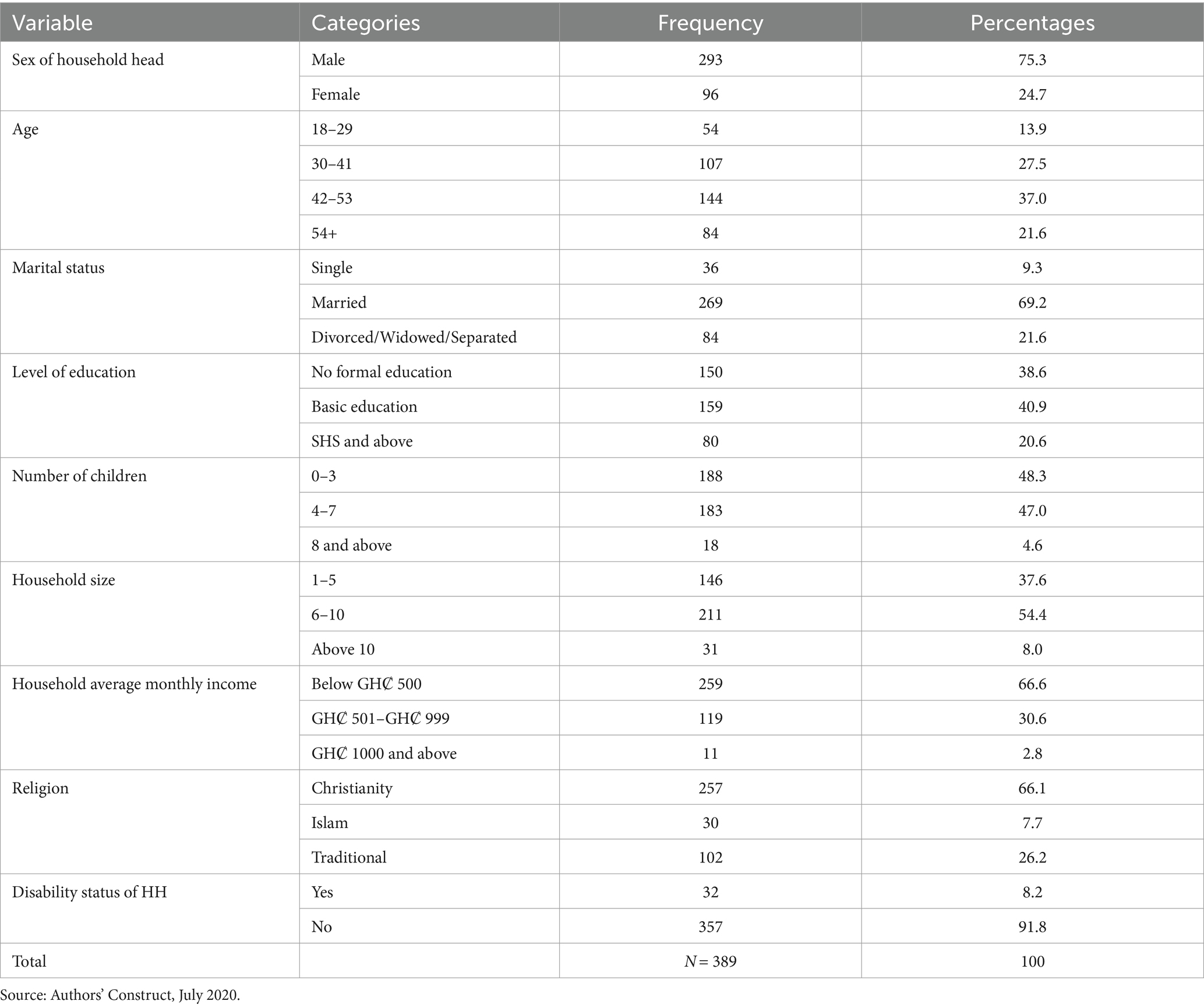
Table 2. Demographic characteristics of households in communities in Bongo District that benefited from various forms of water and sanitation interventions.
Adoption of water and sanitation interventions
The study revealed that majority of households representing 83.6 percent had adopted and were utilizing improved sources/interventions as against 16.5 percent that was still utilizing unimproved sources such as wells and rivers (Figure 2). The results corroborate the findings of Nyanza et al. (2018) who reported that households have access to improved water sources. In the case of sanitation interventions specifically the adoption/utilization of improved toilet facilities, the results further revealed that most households (82.3%) adopted and were utilizing improved sanitation interventions whilst 17.7 percent of households were still using unimproved sources. This finding also shares the position of Asiedu (2015) who averred that households use pit latrines outside their homes and hence have an improved sanitation source compared to open defecation. On the contrary, the findings do not corroborate those of Angoua et al. (2018) and Fielmua et al. (2019) who asserted that households in peri-urban and rural areas do not have access to improved water and sanitation. Similar contrary positions have been reported by Food and Agriculture Organization – FAO (2017) and Bazaanah (2019) that rural households are powerless and have difficulties in accessing and adopting/utilizing portable water and improved sanitation.
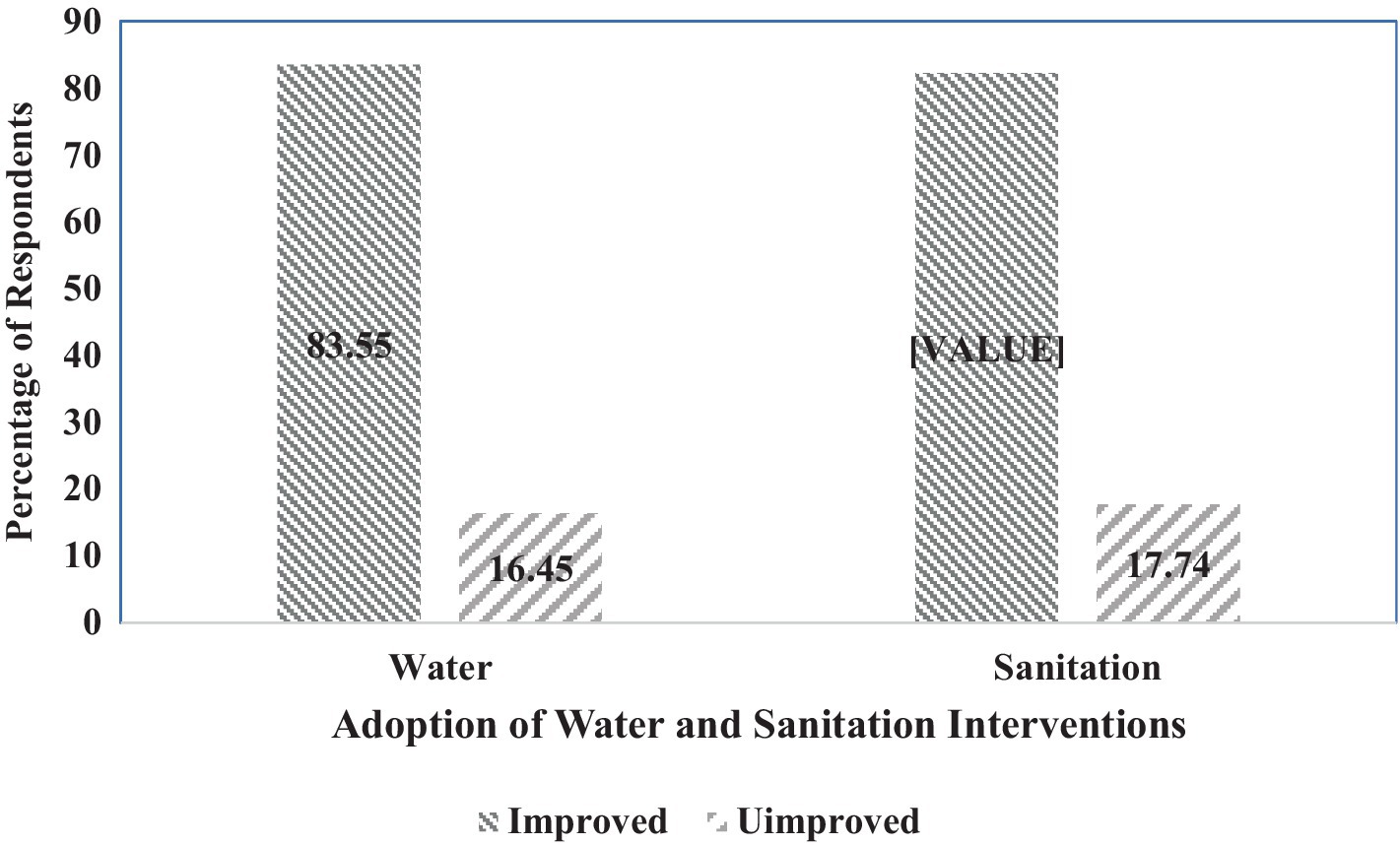
Figure 2. Main sources of water and sanitation (toilet) for households.
Basic drinking water services are defined as drinking water from an improved source, if the collection time is not more than half an hour for a roundtrip, including queuing time. German Industry and Commerce in Ghana – GICG (2018) posited that improved sources of water do not completely prevent waterborne diseases. Children have high mortality rates and serious health issues due to the lack of safe water and sanitation access. Thus, households with limited access to improved sources of water are at risk of waterborne diseases. Basic sanitation services are defined as the use of improved sanitation facilities that are not shared with other households. Such improved sanitation facilities are defined as those that hygienically separate human waste from human contact. Improved sanitation includes flush or pour-flush to piped sewer systems, septic tank pit latrines, ventilated-improved pit latrines, or pit latrines with slab or composting toilets. It should be noted that shared or public-use sanitation facilities are not considered to be improved. Similarly, flush or pour-flush to elsewhere, pit latrines without slabs or open pits, bucket latrines, hanging latrines or open defecation are not considered to be improved sanitation (WHO, 2024).
Demographic characteristics of beneficiaries and adoption/utilization of water and sanitation interventions
Demographic characteristics and adoption/utilization of water interventions
A strong positive association between the sex of household heads and the adoption/utilization of improved water interventions was realized from the results and the chi-square test revealed that this association was statistically significant at (chi = 15.679, p = 0.000) (Table 3). More male-headed households (79.1%) adopted/utilized improved water interventions than female-headed households.
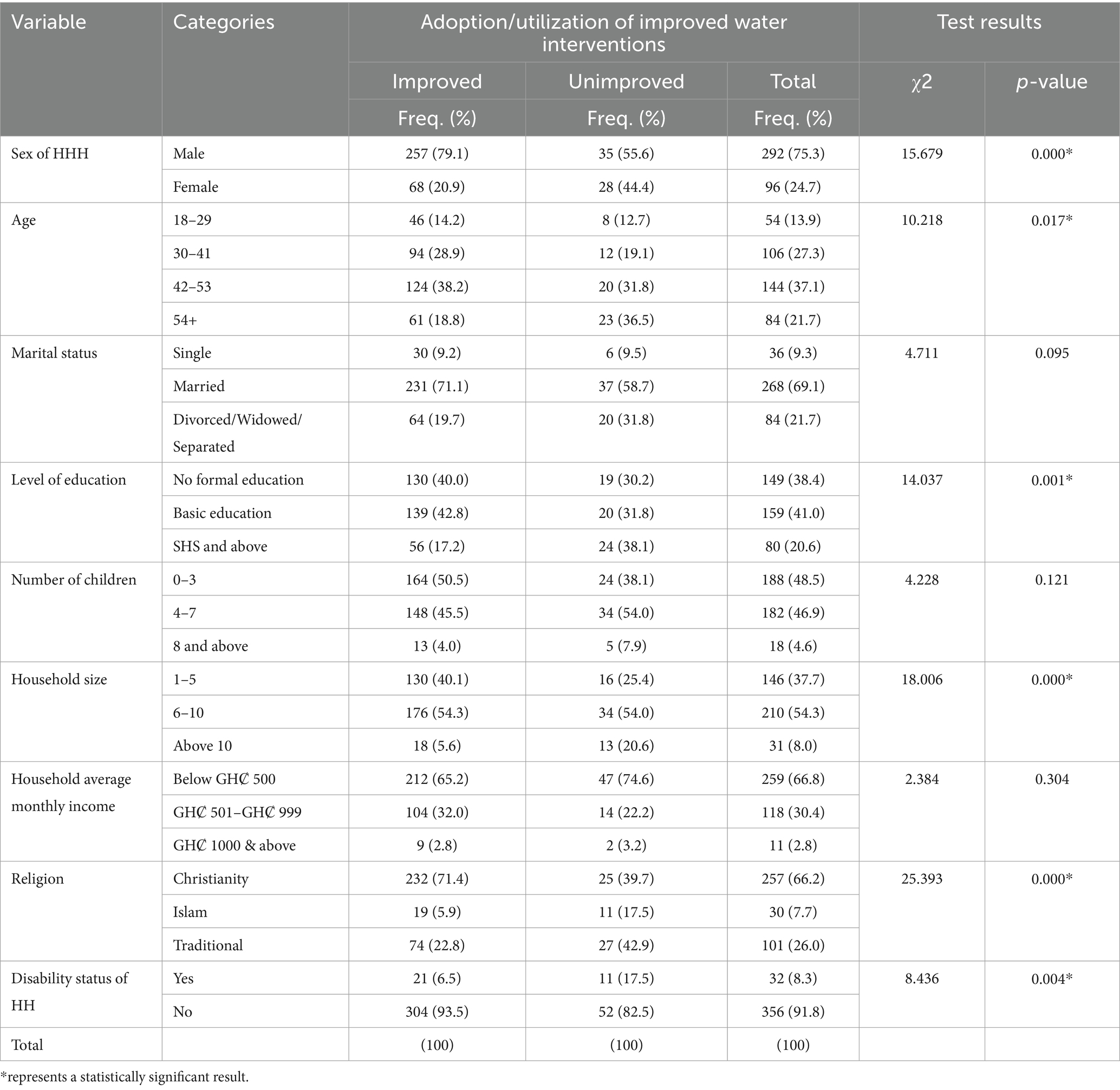
Table 3. Demographic characteristics and adoption/utilization of water interventions.
Similarly, a statistically significant association (chi = 10.218, p = 0.017) was found between the age category of household heads and their adoption/utilization of improved water interventions, thus, the results suggest that households headed by people within the age category of 42–53 years were more susceptible to adopt/utilize improved water interventions (38.15%) than households headed by people within the ages of 18–29 years, 30–41 years and 54+. In addition, the results further show that the level of education of household heads was statistically significantly associated with the adoption/utilization of improved water interventions (chi = 14.037, p = 0.001). The study results indicated that households whose heads had attained at basic education (42.8%) had adopted/utilized improved water interventions than those who had attained SHS and above or had no formal education at all.
Additionally, a strong statistically significant association was found to exist between household size and the adoption/utilization of improved water interventions (chi = 18.006, p = 0.000). The study results indicate that households with sizes ranging from 6 to 10 members adopted/utilized improved water interventions than those with 1–5 or above 10 members.
Again, the adoption/utilization of improved water interventions were found to be significantly associated with religion (chi = 25.393, p = 0.000) as well as the disability status of a household (chi = 8.436, p = 0.004). Households that reported being Christian (71.4%) were more inclined to adopt/utilize water interventions than the other religions whilst households with no known disability status adopted/utilized more improved water interventions than those with known disability status. These findings do not support those of Angoua et al. (2018). In their study on barriers to access to improved water and sanitation in poor peri-urban areas, they assert that household size, education and religion do not improve the adoption and utilization of water among households.
On the contrary, the adoption/utilization of improved water interventions was found not to show any association with the marital status of household heads (chi = 4.711, p = 0.095); the number of children in a household (chi = 4.228, p = 0.121) and household average monthly income (chi = 2.384, p = 0.304).
Demographic characteristics and adoption/utilization of sanitation (toilet) interventions
The findings revealed a strong significant association between the adoption/utilization of improved sanitation interventions and the sex of the household head (chi = 15.948, p = 0.000) and the level of education of the household head (chi = 23.879, p = 0.000) (Table 4). It was revealed that male-headed households adopted/utilized more improved sanitation interventions (79.4%) than female-headed households whilst households headed by people with the educational attainment of basic education adopted/utilized more improved sanitation interventions (43.8%) than households headed by people with SHS and above qualification or no formal education. Similarly, the results further revealed a strong significant association between the adoption/utilization of sanitation interventions and household size (chi = 14.867, p = 0.001) and religion (chi = 22.696, p = 0.000). The results suggest that the adoption/utilization of improved sanitation interventions was more among households with sizes between 6 and 10 members (54.7%). Likewise, the adoption/utilization of improved sanitation interventions were equally more among households that practised the Christian religion (71.3%). Furthermore, the study results also found a significant association between the disability status of households and the adoption/utilization of improved sanitation interventions (chi = 6.614, p = 0.010). This was found to be more among households without any known disability statuses (93.4%) than those with known disability statuses (6.6%). Adoption/utilization of sanitation interventions were equally found to be significantly associated with the household’s average monthly income at chi = 8.188, p = 0.017 and the marital status of household heads at chi = 7.360, p = 0.025.
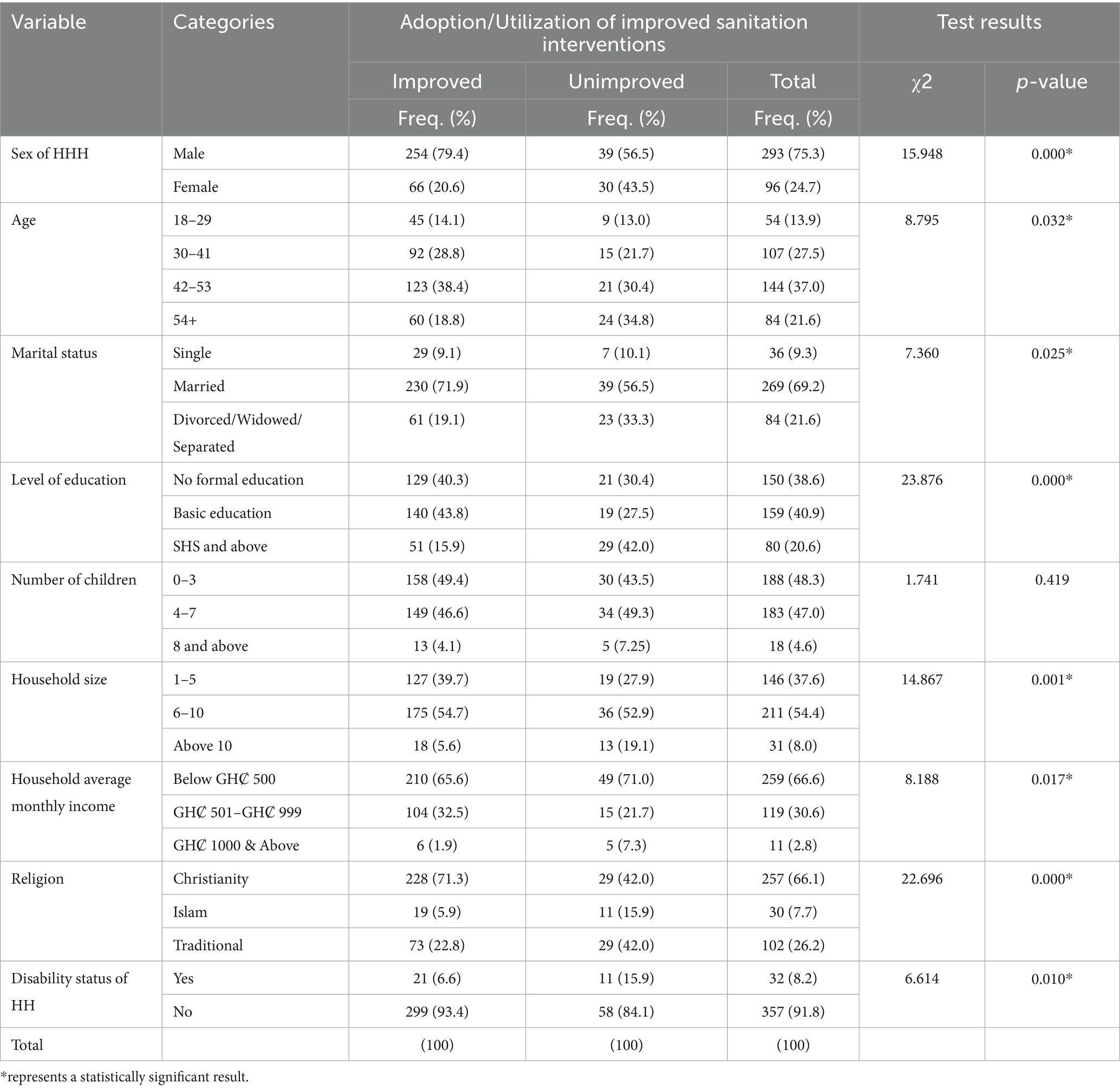
Table 4. Demographic characteristics and adoption/utilization of sanitation interventions.
On the other hand, the findings however did not find any association between the number of children in a household and the adoption/utilization of improved sanitation interventions (chi = 1.741, p = 0.419).
Factors affecting adoption/utilization of water and sanitation facilities
The results show that, among the many factors, knowledge of beneficiary households about derived benefits associated with the adoption/use of improved water (85.9%) and sanitation (86.9%) interventions was the most important factor affecting the adoption and utilization of these interventions (Figure 3).
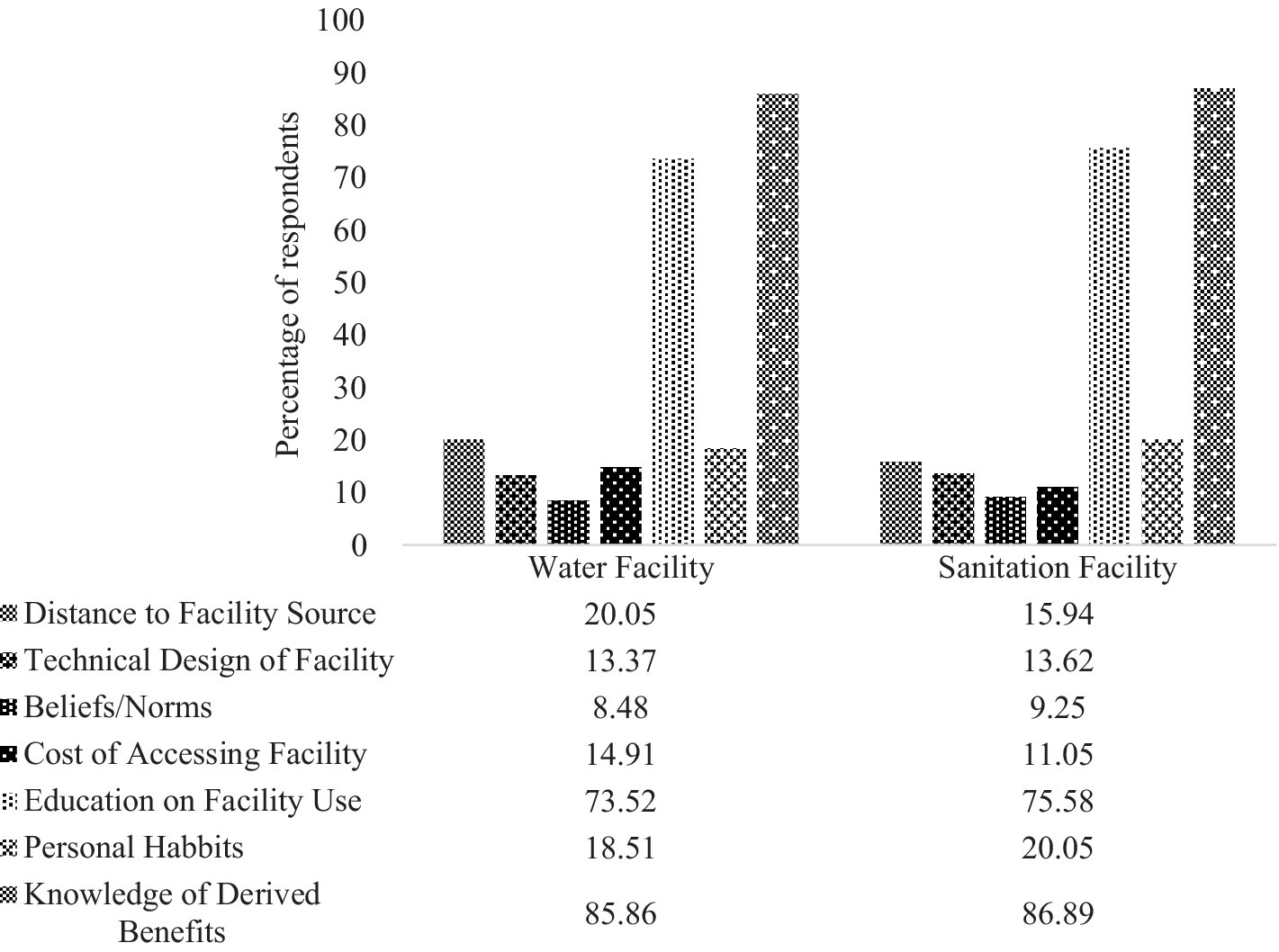
Figure 3. Factors affecting adoption/utilization of water and sanitation facilities.
The objective here assessed the factors that affect the adoption and utilization of water and sanitation facilities in the Bongo District. The results revealed that knowledge of beneficiary households about derived benefits associated with the adoption or use of improved sanitation interventions was the most important factor affecting the adoption and utilization of these interventions. It was further revealed that education on the use of water and sanitation facilities has a great effect on the adoption and utilization of these facilities. Similarly, factors such as distance to the facility source, the technical design of the facility, cost of accessing the facility, personal habits and beliefs/norms affect household adoption and utilization of both water and sanitation facilities.
In support of the quantitative results, a female discussant during a focus group discussion in Kodorogo-Gingirigo community had this to say regarding improved water interventions.
Before the improved facility came to this community, our children get to school late and even workers because they must go through the pain of standing in long queues and crowds before fetching water at the limited water sources. This is no more because it has helped everyone who goes to fetch water by saving time (FGD, female discussant, Kodorogo-Gingirigo, 16.08.2020).
A male discussant in Akunduo-Apeelinga community said.
The water source we had in this community was somehow salty and we got used to it because we had no option but since we were provided with the improved water facilities, we have known the difference in taste and we enjoy the water now especially when drinking it (FGD, male discussant, Akunduo-Apeelinga 15.08.2020).
In line with sanitation, a female discussant in Gorogo-Asalako community affirmed that.
There used to be stench all around the community because of open defecation, sitting here for this discussion would not have been possible at all before due to stench and flies but now we enjoy the good smell from plants and the community is much cleaner than before (FGD, female discussant, Gorogo-Asalako, 14.08.2020).
Another discussant reaffirmed that.
…. the fact that every household has a toilet facility and does not resort to open defecation, has reduced common illnesses like cholera, which was prevalent here. No one has been sick since we stopped open defecation (FGD, female discussant, Kodorogo-Gingirigo, 16.08.2020).
Moreover, the findings also reveal that education on the use of water and sanitation facilities also had a great effect on the adoption and utilization of the facilities. For instance, in both cases of adoption of water and sanitation interventions, 73.5 percent and 75.6 percent of beneficiary households, respectively, reported that education on the use of both facilities affected their adoption/utilization. This finding supports those of Mukadi (2016) who averred that education influences household adoption and utilization of water and sanitation facilities. The outcome of this study is also in line with the findings of Crocker et al. (2016) who reported that education and training led to increased time spent on community-led total sanitation by community members, increased latrine construction, and reduction in open defecation. Considering the reports by Osumanu et al. (2019) that over the years, lack of proper sanitation in most households in sub-Saharan Africa has led to an increase in open defecation from 204 million to 220 million resulting in severe environmentally endemic health problems, one can conclude that the reduction in open defecation as confirmed by the discussants is indication of improvement adoption and utilization of improved sanitation interventions. The following qualitative results in a focus group discussion confirm that of the quantitative results. For instance, a male discussant concerning improved water intervention had this to say.
They trained people to form an executive team on how to maintain the facility and educate households on facility usage. They further educated us on every household contributing financially every year, so we do not have to wait until the facility breakdown. Anyone who is up to the age of marriage and married is required to pay except for those who attend school (FGD, male discussant, Akunduo-Apeelinga 15.08.2020).
Another discussant said.
We were educated that children not more than 10 years should not be allowed to use the facility, clean the solar facility and contribute money so, in case of breakage, the facility can be fixed (FGD, female discussant, Kodorogo-Gingirigo, 16.08.2020).
In relation to sanitation, a discussant in Gorogo-Asalako community highlighted that.
We were educated to buy a certain chemical and use salt or ashes to reduce the rate at which the toilet holes get full. It’s better that way than to wait for the facility to fill up and leave it to dig another toilet facility (FGD, female discussant, Gorogo-Asalako, 14.08.2020).
A discussant further highlighted that.
Some people in the community were trained as artisans on how to build and maintain toilet facilities (FGD, male discussant, Akunduo-Apeelinga 15.08.2020).
Furthermore, less than 50 percent of beneficiary households reported that distance to the facility source, the technical design of the facility, beliefs/norms, cost of accessing the facility and personal habits affected their adoption and utilization of both water and sanitation interventions (see Tables 3, 4). In respect to the cost of accessing water and sanitation facilities, the findings support those of Armah et al. (2018) who averred that poor households in urban and rural areas do not afford the initial cost of water and sanitation facilities. It also confirms the findings of Bazaanah (2019), that open defecation is more widespread (70%) among the poorest rural household population in Ghana Also, 20.1 percent of beneficiary household admitted distance to the water facility source affected their adoption/utilization whilst 15.9 percent of beneficiary households reported that distance to the toilet facility affected their adoption and use. In support with the distance to facility sources, a discussant relating to the improved water facility in Gorogo-Asalako community had this to say.
We cannot all be close to the facility; some will have to always to get there first before others because the houses are not at the same location. However, since we do not carry water for long the facility location is good (FGD, female discussant, Gorogo-Asalako, 14.08.2020).
A discussant in Akunduo-Apeelinga community highlighted in relation to sanitation that.
The toilet facility in my house is spoiled and has not been fixed for a long time now so I pair with the nearby house (FGD, male discussant, Akunduo-Apeelinga 15.08.2020).
In the case of the technical design of the facility, the results reveal that 13.4 percent of beneficiary households said that affected their adoption/utilization whilst an equally similar result of 13.6 percent of beneficiary households also said that the technical design of the facility affected their adoption/use. For instance, female discussants concerning the technical design of improved water intervention had this to say.
The design of the gutters at the facility is not too good in that the narrow gutters make it difficult for water to flow out of the facility hence breeding mosquitoes (FGD, female discussant, Akunduo-Apeelinga 15.08.2020).
The design of the facility is not bad just that the polytank makes the water hot for me and sometimes dirty even though we clean it (FGD, male discussant, Kodorogo-Gingirigo, 16.08.2020).
The polytank stand is too tall making it fall whenever there is no water anytime there is wind. We have brought down the polytank three times to patch it. It will have been easier if the tank was down (FGD, male discussant, Gorogo-Asalako, 14.08.2020).
Regarding sanitation, a male and female discussant during the focus group discussion supported the statement that.
The design of some of the toilet facilities has become death traps because of poor design. Not all of us here had the money to buy cement to build our toilet facilities (FGD, male discussant, Kodorogo-Gingirigo, 16.08.2020).
The bucket bowl style that we use for our toilet is not suitable because it easily gets full and many of us here cannot afford the most suitable one (FGD, female discussant, Gorogo-Asalako, 14.08.2020).
In addition, 14.9 percent of the beneficiary households also admitted that the cost associated with accessing water interventions affected their adoption/use whilst 11.1 percent said the cost associated with the adoption/use of sanitation (toilet) interventions affected their adoption/use. In confirming the quantitative results, a female discussant in the Kodorogo-Gingirigo community had this to say regarding improved water interventions.
There is an irregularity in the payment of yearly fees among community members and sometimes when a member defaults he/she finds it, difficult to access the facility so they go elsewhere to fetch water (FGD, female discussant, Kodorogo-Gingirigo, 16.08.2020).
Another discussant in the Akunduo-Apeelinga community had this to say.
In accessing the water facility every member of each household except for school children, contributes financially yearly to take care of future maintenance of the facility as and when it breaks down (FGD, female discussant, Akunduo-Apeelinga 15.08.2020).
In line with sanitation, a male discussant in Gorogo-Asalako highlighted that.
Every house has its toilet facility built by the occupants themselves and it does not involve any cost that will affect accessing the facilities (FGD, male discussant, Gorogo-Asalako, 14.08.2020).
Personal habits were also another factor affecting the adoption/use of water and sanitation interventions. Whereas 18.5 percent of beneficiary households said personal habits in their households affected the adoption/use of water interventions, 20.1 percent reported that personal habits affected their adoption/use of sanitation (toilet) interventions. The following qualitative results in a focus group discussion confirm that of the quantitative results. For instance, a female discussant concerning improved water intervention had this to say.
Before we used to get water freely without thinking of paying any contribution for maintenance but now that the improved water facility is introduced into the community, we are compelled to develop the habit of contributing monthly or yearly (FGD, female discussant, Kodorogo-Gingirigo, 16.08.2020).
In relation to sanitation, a discussant in the Gorogo-Asalako community highlighted that.
From the beginning, it was very difficult for us to accept the pit latrines as a place for defecation, but its benefits have been seen all over making everyone healthy (FGD, male discussant, Gorogo-Asalako, 14.08.2020).
Another discussant further highlighted that.
I was much familiar to open defecation but with the toilet facility now, it is very warm and makes me sweat all time. This does not motivate me to use it (FGD, male discussant, Akunduo-Apeelinga 15.08.2020).
Beliefs and norms were the least among the factors reported to affect the utilization and adoption of water and sanitation interventions, thus only 8.5 percent and 9.3 percent of beneficiaries, respectively, reported that belief and norms affected their adoption and use of the improved water and sanitation interventions. This implies that beliefs and norms do not affect the adoption and utilization of water and sanitation at the community level. This disconfirms the findings of Alhassan (2019) who asserts that beliefs, norms and values are very critical factors that shape people’s lives and their utilization of water and sanitation. Similarly, a study employing a cluster-randomized controlled trial approach examined Community-Led Total Sanitation (CLTS) and reported that changes in factors such as social norms explain why participants construct latrines (Harter et al., 2020).
Level of community involvement in water and sanitation facilities’ interventions
The evidence shows that majority of households responded that their communities were not involved (54.8%) in deciding on the appropriateness of the water facility/intervention. Similar evidence exists for the sanitation intervention where most of the respondents also revealed that they were not involved (40.4%) in deciding the appropriateness of the sanitation facilities in the communities (Table 5).
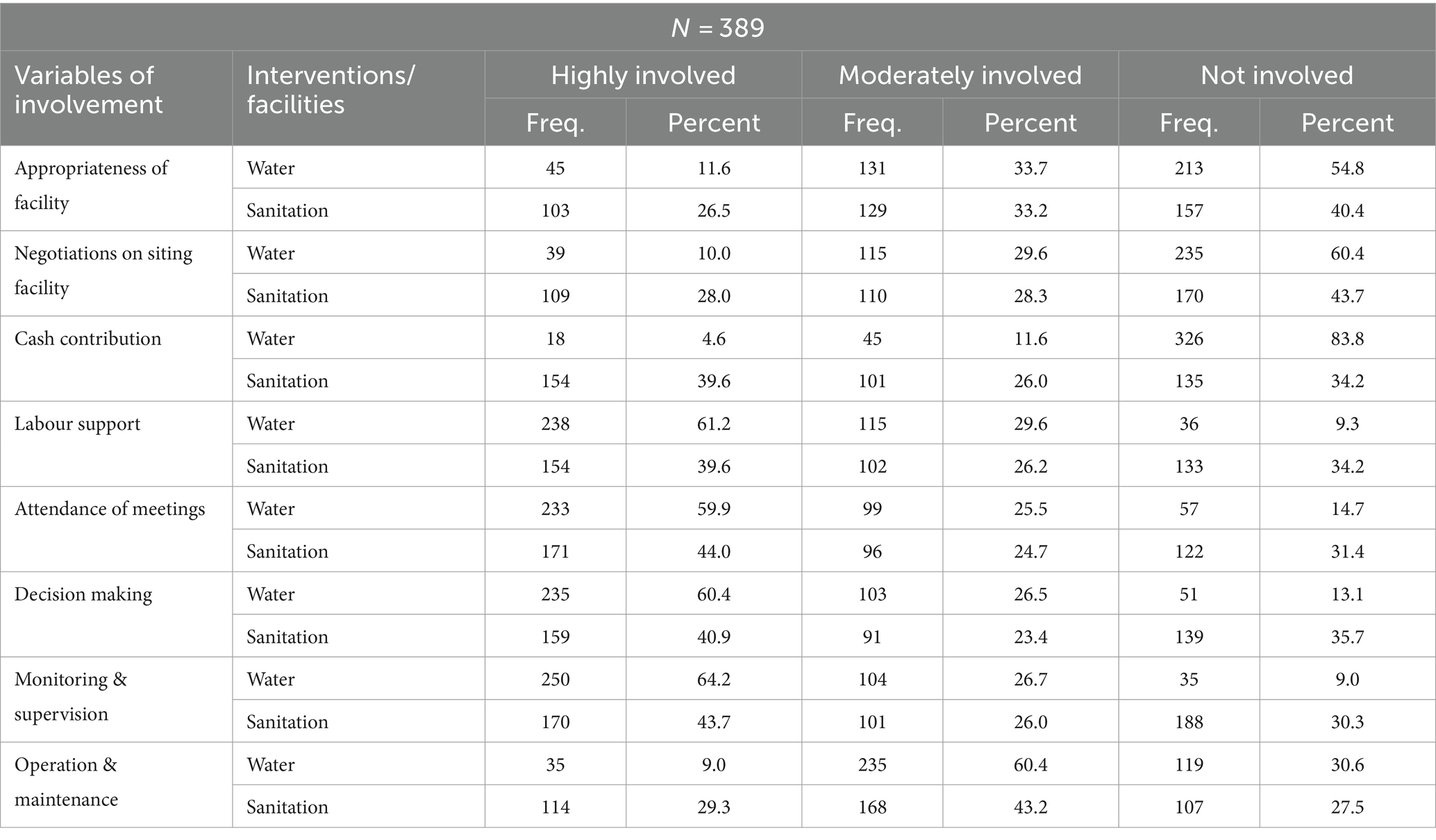
Table 5. Level of community involvement in water and sanitation facilities’ interventions.
The qualitative interviews conducted with key informants revealed mixed results on the level of community involvement in deciding the appropriateness of both water and sanitation interventions. As pointed out by some of the key informants, most of the water and sanitation interventions in the Bongo District are usually pre-determined by donor agencies before implementation, thereby leaving community members with little or no room to decide on whether these facilities are appropriate to their needs. One of the key informants had this to say when questioned on whether community members are often involved in deciding the appropriateness of water and sanitation facilities:
“Usually, interventions are pre-designed by donor or funding bodies after which community members are informed. However, sensitization and necessary education may be done after establishing the projects on how community members can sustain them” (KII, August 2020).
On the contrary, some of the persons interviewed acknowledged that communities are often core to decisions regarding the appropriateness of water and sanitation facilities for their benefit.
“Community members are deeply involved in deciding the appropriateness of water and sanitation interventions in the area. As a District Assembly, water and sanitation interventions are implemented on demand-driven not supply driven. We meet with the community members and explain to them the terms and conditions accompanied with facilities that are to be allocated to them upon demand” (KII, August 2020).
In addition, the majority of households admitted that their communities were equally not involved (60.4, 43.7%) in negotiating the siting of the water and sanitation facilities, respectively. The interviews conducted with key informants revealed a divergent position. Almost all the key informants strongly maintained that issues regarding the sitting of water and sanitation facilities are often discussed with community members through their leaders before the actual siting of the interventions. Some of them averred that:
“Traditional and opinion leaders are usually engaged, to ask for permission to use a particular piece of land or area and if the said piece of land is not available for use, they offer an alternative area for the facility to be sited” (KII, August 2020).
Another key informant said,
“Communities decide where any water and sanitation facility should be sited with technical assistance given to them by the DWST” (KII, August 2020).
With regards to cash contributions to water and sanitation facilities construction, the majority of beneficiary households reported that their communities were not involved (83.8%) in contributing cash towards the establishment of the water facility. The majority of households (39.6%) however, admitted that they were highly involved and thus contributed cash towards the establishment of the sanitation (toilet) facilities. The qualitative findings also amplified these results where key informants equally maintained that cost issues associated with the establishment of water facilities were borne solely by the donor or funding agencies whilst community members take up the cost of putting up pit latrines/toilets. Some of the key informants said that:
“With regards to donor-funded projects, communities do not contribute cash. However, when it comes to sanitation (toilet facilities specifically), community members take the initiative of household latrine construction through the community-led total sanitation (CLTS) approach” (KII, August 2020).
“Community members often do not contribute cash towards the construction of water facilities but for the toilet facilities; they use much of the available local materials in the construction of pit latrines” (KII, August 2020).
The results in Table 5 again showed that majority of households asserted that their communities were highly involved in terms of labour support towards the establishment of both the water (61.2%) and sanitation (39.6%) intervention/facilities. Some key informants reinforced these findings during the qualitative interviews with them. They maintained that labour was the bloodline for any water or sanitation intervention. As such, to ensure that community members owned water and sanitation facilities, they are often encouraged to actively engage in any labour works associated with the implementation of these facilities or delegate some community members who can better perform specific tasks related to projects. Some of them, therefore, narrated that.
“Community members do support in fetching water and sand during the construction of platforms around boreholes. With the household pit latrines, they take up the entire construction including labour” (KII, August 2020).
In all the water and sanitation interventions/facilities, there is always local content which is normally given to the community members to execute in the form of labourers” (KII, August 2020).
One of the key informants however said that; “although community members are highly involved in the construction of water and sanitation facilities through labour works, they are often compensated at the end and so do not do it for free” (KII, August 2020).
Similarly, the majority of the respondents (59.9, 44.0%) said their communities were equally highly involved in attending meetings relating to issues bothering the establishment of the water and sanitation interventions, respectively. Divergent evidence emerged from the qualitative interviews conducted with key informants on the attendance of meetings relating to water and sanitation interventions. Below are some quotes from key informants:
“Attendance to meetings at the community level is usually low, especially where there are no freebies or incentives to offer participants at the end of the meeting” (KII, August 2020).
Another had this to say.
Community members rarely attend meetings and even when they come; they are not always effective in contributing meaningfully to the issues before them” (KII, August 2020).
Again, the results further reveal that majority of the households and for that matter, the communities were highly involved in terms of decision-making for the water and sanitation projects/interventions (60.4 and 40.9% respectively). The qualitative evidence lends credence to these results as well where key informants generally maintained that community members were the major stakeholders in the interventions that they provide and so they are integral to decisions taken to ensure sustainable provision and utilization of water and sanitation facilities.
“Community members are highly involved in decision making through the establishment of certain structures such as community hygiene volunteers, water and sanitation management teams to manage facilities after they are constructed. It is the community’s sole responsibility to nominate people to occupy those structures and take up decisions regarding their sustainable management” (KII, August 2020).
With regards to monitoring and supervision of the water and sanitation projects in the communities, most respondents were again of the view that their involvement was high for both projects/interventions, thus 64.2 percent said they were highly involved in monitoring and supervising water facilities whilst 43.7 percent said they were involved in monitoring and supervising sanitation (toilet) interventions. Further corroborative evidence from the qualitative findings shows that communities were involved in the monitoring and supervision of water and sanitation projects/facilities through the leaders who constitute the various teams for these facilities. For instance, some key informants maintained that:
“In most instances, monitoring and supervision is done by the structures put in place by the community” (KII, August 2020).
Community members take part in the monitoring and supervision of WASH facilities during site meetings and inspection of projects” (KII, August 2020).
Finally, the findings also showed that the majority of households/communities were moderately involved in the operation and maintenance of both water and sanitation facilities (60.4 and 43.2% respectively). A key informant had this to say when asked about the extent to which community members were involved in the overall operation and maintenance of water and sanitation facilities in support of the moderate involvement of community members:
Operation of the facilities has greatly relied on the community members, but the maintenance of the facilities is however a shared responsibility between community members and the District Assembly” (KII, August 2020).
However, another key informant asserted that communities were highly involved in the operation and maintenance of water and sanitation facilities. He said:
“Water and sanitation facilities are operated on the community own management system as per the community water and sanitation Agency policies. So, the community members manage their water and sanitation systems” (KII, August 2020).
The level of community involvement in water and sanitation interventions was evaluated using the variables: appropriateness of facility, negotiations on siting facility, cash contribution, labour support, attendance of meetings, decision making, monitoring and supervision and operation and maintenance. The findings showed that households in their communities were highly involved in terms of labour support towards the establishment of both water and sanitation facilities, attending meetings relating to issues bothering the establishment of the water and sanitation interventions, decision making and monitoring and supervision of both water and sanitation interventions. Also, households were moderately involved in the operation and maintenance of both water and sanitation facilities/interventions. On the contrary, households in the communities were not involved in deciding the appropriateness of the water and sanitation interventions as well as negotiating the sitting of the water and sanitation facilities. Moreover, households were highly involved in cash contributions for the construction of the sanitation facilities but were not involved in the contribution of cash for the establishment of the water interventions/facilities.
The results above reveal the involvement of community members and households at every stage of the implementation of water and sanitation interventions. In addition, this brings about the sustainability of such water and sanitation facilities. These findings corroborate those of Issah-Bello (2011) who asserted that lack of community involvement at every stage of project implementation accounts for sustainability problems. In other words, involving beneficiaries at every stage of water and sanitation interventions brings about the sustainability of such facilities.
Determining the association between the demographic characteristics of beneficiaries and their adoption of water and sanitation interventions
In this objective, the association between the demographic characteristics of beneficiaries and their adoption of both water and sanitation interventions were determined. The demographic characteristics of beneficiaries have been concentrated on the sex of household heads, age of household heads, household size, educational status, religion, disability status, marital status, number of children and household average monthly income based on literature. The statistical data analysis revealed age, sex, education household size, religion and disability status were found statistically significant to households’ adoption and utilization of improved water interventions. On the contrary, the adoption and utilization of improved water interventions were not significantly associated with marital status, the number of children and household average monthly income. For sanitation, the findings revealed a significant association between the adoption of sanitation interventions with the sex of the household head, level of education, household size, religion and disability status. Similarly, the adoption of sanitation interventions was equally found significantly associated with household average monthly income and marital status of household heads. However, the number of children in a household and adoption of improved sanitation interventions were not significantly associated.
Conclusion
The study has shown that demographic characteristics of beneficiaries of water and sanitation interventions in the Bongo District in the Upper East Region of Ghana affect how improved water and sanitation are adopted and utilized. This implies that demographic characteristics play a critical role in determining how households in communities adopt and use improved water and sanitation in their communities. The study indicated that stakeholders consider certain factors to ensure household continuous adoption and utilization of improved water and sanitation facilities thereby sustaining such interventions. It can also be concluded from the study findings that the participation of beneficiaries in the implementation process of water and sanitation interventions is very crucial to the sustainability of such interventions. For this reason, households in the communities are involved at every stage of the interventions/project implementation to ensure the sustainability of water and sanitation facilities.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Graduate Studies Board, Institute of Local Government Studies, Tamale, Ghana. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
RA: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Resources, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. SA: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. EA: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Alfredo, K. A., Lawler, D. F., and Katz, L. E. (2014). Fluoride contamination in the Bongo District of Ghana, West Africa: geogenic fluoride contamination in the Bongo District of Ghana, West Africa: geogenic contamination and cultural complexities. Water Int. 39, 1–16. doi: 10.1080/02508060.2014.926234
Alhassan, H. (2019). Effects of WASH interventions on access to clean drinking water and sanitation practices in the Lawra and Nandom districts of the upper west region of Ghana. MPhil Thesis, Tamale, Ghana: University for Development Studies.
Angoua, E. L. E., Dongo, K., Templeton, M. R., Zinsstag, J., and Bonfoh, B. (2018). Barriers to access improved water and sanitation in poor peri-urban settlements of Abidjan, Côte d’Ivoire. PLoS One 13:e0202928. doi: 10.1371/journal.pone.0202928
Armah, F. A., Ekumah, B., Yawson, D. O., Odoi, J. O., Afitiri, A.-R., and Nyieku, F. E. (2018). Access to improved water and sanitation in sub-Saharan Africa in a quarter century. Heliyon 4, e00931–e00927. doi: 10.1016/j.heliyon.2018.e00931
Asiedu, B. A. (2015). Household access to water and sanitation facilities: a case study of the Offinso south municipality. Kumasi, Ghana: Kwame Nkrumah University of Science and Technology.
Awoke, Z. (2012). Assessment of challenges of sustainable rural water supply: Quarit woreda, Amhara region. New York, USA: A Project Paper Presented to the Faculty of the Graduate School of Cornell University in Partial Fulfillment of the Requirements for the Degree of Master of Professional Studies.
Bazaanah, P. (2019). Evaluating the effects of household’s socio-demographic elements on the determination of drinking water quality and quantity in rural. Int. J. Econ. Commer. Manag. 7:356.
Bonda . (2016). Bongo district assembly: medium term development plan. Bongo District Assembly, Ghana.
Braimah, I., Amponsah, O., and Asibey, O. M. (2016). The effectiveness of the local management systems of rural water facilities for sustainable service delivery: a case study of the Sekyere East District, Ghana. Sustain. Water Res. Manag. 2, 405–418. doi: 10.1007/s40899-016-0070-7
Brundtland Commission (2014). Defining sustainable development: The world commission on environment and development. London, UK: Earthscan/Routledge.
Community Water and Sanitation Agency – CWSA . (2015). Fact sheet: Rural and small towns water service. Ghana: Community Water and Sanitation Agency (CWSA).
Creswell, J. W. (2014). Research design: Qualitative, quantitative and mixed methods approaches (fourth Edi). California, USA: SAGE Publications.
Crocker, J., Abodoo, E., Asamani, D., Domapielle, W., Gyapong, B., and Bartram, J. (2016). Impact evaluation of training natural leaders during a community-led total sanitation intervention: a cluster-randomized field trial in Ghana. Environ. Sci. Technol. 50, 8867–8875. doi: 10.1021/acs.est.6b01557
Fielmua, N., Akudugu, A. M., and Dugle, G. (2019). Water, sanitation and rural livelihoods nexus: an exploratory study of Wogu in the upper west region of Ghana. Ghana J. Dev. Stud. 16, 199–219. doi: 10.4314/gjds.v16i2.10
Food and Agriculture Organization – FAO . (2017). Coping with water scarcity: challenge of the 21st century. Available at: http://www.fao.org/3/a-aq444e.pdf.
German Industry and Commerce in Ghana – GICG . (2018). Access to clean drinking water and water management in Ghana. Ghana Statistical Service.
Ghana Statistical Service . (2014). 2010 Population & Housing Census. District analytical report. Ghana Statistical Service.
Ghana Statistical Service – GSS . (2018). Ghana multiple indicator cluster survey; snapshots on key findings.
Harter, M., Inauen, J., and Mosler, H.-J. (2020). How does community-led Total sanitation (CLTS) promote latrine construction, and can it be improved? A cluster-randomized controlled trial in Ghana. Soc. Sci. Med. 245:112705. doi: 10.1016/j.socscimed.2019.112705
Hesse-Biber, S. N. (2010). Mixed methods research: Merging theory with practice. New York, USA: The Guilford Press.
Issah-Bello, S. (2011). An assessment of sustainability of water and sanitation interventions in northern region: A case study of Nanumba North District. Kumasi, Ghana: Kwame Nkrumah University of Science and Technology.
Kramer, A., and Pahl-Wostl, C. (2014). The global policy network behind integrated water resources management: is it an effective norm diffusor? Ecol. Soc. 19, 1–11.
Mukadi, L. N. (2016). Factors influencing adoption of water sanitation and hygiene practices in Kenya: a case of Shivanga location, Kakamega County. Nairobi, Kenya: University of Nairobi.
Nyanza, E. C., Jahanpour, O. L. A., Hatfield, J., Meer, F. V. A. N. D. E. R., and Allen-, L. (2018). Access and utilization of water and sanitation facilities and their determinants among pastoralists in the rural areas of northern Tanzania. Tanzan. J. Health Res. 20, 1–10. Available at: https://www.ajol.info/index.php/thrb/article/view/157792
Osahon, O. J., and Kingsley, O. (2016). Statistical approach to the link between internal service quality and employee job satisfaction: a case study. Am J Appl Math Stat 4, 178–184. doi: 10.12691/ajams-4-6-3
Osumanu, I. K. (2010). Community involvement in urban water and sanitation provision: the missing link in partnerships for improved service delivery in Ghana. J. Afr. Stud. Dev. 2, 208–215. Available at: http://www.academicjournlas.org/JASD
Osumanu, I. K., Kosoe, E. A., and Ategeeng, F. (2019). Determinants of open defecation in the Wa municipality of Ghana: empirical findings highlighting sociocultural and economic dynamics among households. J. Environ. Public Health 2019, 1–10. doi: 10.1155/2019/3075840
Smithson, J. (2008). “Focus groups” in The Sage handbook of social research methods. eds. P. Alasuutari, L. Bickman, and J. Brannen London, UK: SAGE Publications Ltd.), 356–371.
Solane, M., and Jouravlev, A. (2006). Water Governance for Development and Sustainability, CEPAL-SERIE Recursos Naturals e Infraestrutura No. 111. Santiago, Chile: United Nations.
Todaro, P. T., and Smith, C. M. (2014). Economic development (12th Edition). United Kingdom: Pearson.
UNICEFGhana Center for Democratic Development (CDD-Ghana)the Centre for Social Policy Studies (University of Ghana) . (2019). 2018 / 19 district league Table II with new perspectives and modified methodology. UNICEF, Ghana Center for Democratic Development (CDD-Ghana) and the Centre for Social Policy Studies (University of Ghana).
UNICEF/WHO . (2022). Africa to drastically accelerate progress on water, sanitation and hygiene. Available at: https://www.unicef.org/senegal/en/press-releases/africa-drastically-accelerate-progress-water-sanitation-and-hygiene-report.
United Nations . (2018). Our common future: towards sustainable development. Available at: http://www.un-documents.net/ocf-02.htm.
United Nations Economic and Social Council – UNESCO . (2017). Progress towards the sustainable development goals: report of the secretary-general. Available at: http://www.un.org/ga/search/view_doc.asp?symbol=E/2017/66&Lang=E.
WHO (2024). Improved sanitation facilities and drinking-water sources. Available at: https://www.who.int/data/nutrition/nlis/info/improved-sanitation-facilities-and-drinking-water-sources (Accessed May 27, 2024).
World Bank . (2018). Understanding poverty. Available at: http://www.worldbank.org/en/topic/poverty/overview.
Keywords: Ghana, Bongo District, demographic characteristics, household, communities, education, water and sanitation interventions, concurrent mixed method design
Citation: Atengdem RA, Abobi SM and Alhassan EH (2024) Evaluating community adoption and participation in water and sanitation interventions in the Bongo District, Ghana. Front. Water. 6:1349331. doi: 10.3389/frwa.2024.1349331
Edited by:
Henry Bikwibili Tantoh, University of South Africa, South AfricaReviewed by:
Anyway Katanha, Zimbabwe Open University, ZimbabweSammy Letema, Kenyatta University, Kenya
Copyright © 2024 Atengdem, Abobi and Alhassan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Seth Mensah Abobi, bWFib2JpQHVkcy5lZHUuZ2g=
†ORCID: Seth Mensah Abobi, http://orcid.org/0000-0001-5538-8573