 Chris Macdonald
Chris Macdonald- University of Cambridge, Cambridge, United Kingdom
Public speaking anxiety is a prevalent issue with significant negative impacts. While virtual reality exposure therapy is an effective treatment, it currently has significant limitations. This study outlines the design process of a new VR platform that seeks to make virtual reality exposure therapy more effective and more accessible. To increase accessibility, the platform is open access and accessible via multiple devices and operating systems. To increase efficacy, the concept of overexposure therapy was developed: training in extreme scenarios that one is unlikely to encounter in real life. For example, on the platform, users can practice public speaking in a highly distracting stadium environment to a virtual reality audience of 10,000 photorealistic spectators. A single-session experiment with 29 adolescents evaluated the platform’s impact on public speaking anxiety, confidence, and enjoyment. Results showed significant improvements in all three measures. These findings suggest that this novel approach holds promise. The paper concludes by exploring limitations and areas for future research.
Introduction
The fear of public speaking is widely cited as being the most common fear (Richmond and McCroskey, 1998; Furmark et al., 1999; Dwyer and Davidson, 2012; Grieve et al., 2021; Kahlon et al., 2023). Furthermore, there is evidence to suggest that the prevalence of social anxiety and a fear of public speaking are both on the rise (Dwyer and Davidson, 2012; Jefferies and Ungar, 2020; Ranta et al., 2024). This is concerning when one considers the range of known subsequent negative impacts on mental health, physical health, academic attainment, and career progression (Bardone et al., 1998; Greenberg et al., 1999; Sareen et al., 2005; Aarons et al., 2008; Ruscio et al., 2008; Russell and Shaw, 2009; Aderka et al., 2012; Poeschl, 2017; Grieve et al., 2021).
When looking specifically at students, multiple studies highlight the need and desire for a solution that helps students become more confident and skilled public speakers: When looking at students in the United Kingdom, it was found that c. 80% reported that presentations were associated with frequent anxiety (Russell and Topham, 2012); and when looking at students in the United States, it was found that c. 90% of students would like their educational institutions to provide classes that help them improve public speaking (Marinho et al., 2017).
Fortunately, with regard to public speaking anxiety, there is a range of known treatment options, including exposure therapy (ET). During ET, patients are encouraged to gradually confront fear-inducing stimuli (Abramowitz et al., 2019). Accordingly, it is “based on the well-validated theory that anxiety is maintained and worsened by avoiding feared stimuli” (Abramowitz et al., 2019). ET is a versatile treatment and can be adapted for a range of fears (Fedoroff and Taylor, 2001; Bradley et al., 2005; Rosa-Alcázar et al., 2008; Cahill et al., 2009; Sánchez-Meca et al., 2010). ET is frequently cited as the most evidenced and most effective way to treat fear (Marks, 1979; Ougrin, 2011; Sars and van Minnen, 2015); it has been reported that c. 90% of patients show a significant reduction in fear and avoidance after posttreatment followup (Ost, 1989; Barlow et al., 2000; Tolin, 2010; Kaplan and Tolin, 2011). Furthermore, ET has been shown to be more effective than medication in multiple studies (Barlow et al., 2000; Foa et al., 2005). Accordingly, ET is considered the gold-standard treatment option (Chowdhury and Khandoker, 2023).
Although in vivo ET is effective, it is underused: clinicians underuse it as a tool (Langthorne et al., 2023) and patients often refuse it due to the financial costs, time costs, and the apprehension of being placed into unpredictable social situations (Premkumar et al., 2021). Accordingly, virtual reality exposure therapy (VRET) is a promising alternative. VRET (example shown in Figure 1) can be easier to administer for the clinician and it can reduce time costs as well as provide a more predictable environment for the patient (Botella et al., 2017; Premkumar et al., 2021). As a result, VRET is a valuable mode of delivery to engage those currently left out. Importantly, VRET has been widely explored (Valmaggia et al., 2016; Carl et al., 2019), and it has been shown to be as effective as in vivo, with significant and enduring effects that generalise to real situations (Anderson et al., 2013; Owens and Beidel, 2015; Kampmann et al., 2016; Anderson et al., 2017; Horigome et al., 2020; Premkumar et al., 2021; Reeves et al., 2022; Chowdhury and Khandoker, 2023; Morina et al., 2023; Seuling et al., 2024). There are also reports of VRET being more effective than in vivo (Bouchard et al., 2017), and others have observed additional practical benefits of the delivery method such as it being more standardised and more confidential (Seuling et al., 2024).

Figure 1. Example of VRET (Lindner et al., 2020) from a prior study.
VRET can be delivered in a therapist-guided and/or self-guided format. While self-guided may appear an inherently lesser form, it has been shown to produce significant improvements for individuals reporting high levels of public speaking anxiety (Lindner et al., 2019). It is suggested that self-guided VRET is highly effective due to its perceived level of control (Premkumar et al., 2021). Control over treatment has been shown to increase compliance (Sirur et al., 2009; Alami et al., 2018) and facilitate the patient’s autonomy and the accelerated development of resilience (Evans and Fischer, 1992; Bhanji et al., 2016; Buchholz and Abramowitz, 2020; Premkumar et al., 2021).
This paper outlines the progress made thus far on an ongoing project that aims to make VRET more accessible and more effective. It details the design process and evaluation of a new VR platform that aims to help users become more skilled and confident public speakers.
Materials and methods
Virtual reality design process
Accessibility
Access to a therapist can be limited due to patient location, monetary costs, time costs, and lengthy waits (Punton et al., 2022). Accordingly, one of the first major design decisions was to make sure the offering was compatible for therapist-guided, self-guided, and hybrid forms of delivery. While self-guided delivery can greatly facilitate accessibility, as noted by others, there remains a significant accessibility issue associated with the cost of purchasing the necessary virtual reality headset (Sarpourian et al., 2022). As a result, I constructed the virtual reality environments in a manner that they could be accessed via both a conventional VR headset (e.g., Meta Quest) and/or a smartphone (e.g., Samsung Galaxy) inserted into a device mount. In the latter form, as the smartphone is providing the computing, screen, accelerometer, and gyroscope, and the device mount is merely holding the device in place, it is a viable low-cost solution. The required device mounts are widely available online (ranging from £5 to £30 depending on condition). Accordingly, a device mount could be thought of as a low-cost and non-destructive ‘smartphone conversion kit’ that transforms the technology that the user already owns into a functional VR headset.
It was considered important that a participant could use a smartphone running on either the Android and/or the iOS mobile operating system. This was a crucial step for accessibility as these operating systems have captured the global market share: worldwide they account for more than 99% of the market (StatCounter, 2024). Worldwide, Android is the current market leader with 71% of the market, however, in the United States, iOS is the current market leader with 57% of the market share (StatCounter, 2024). Accordingly, an offering that is not dual-compatible, could exclude the majority of smartphone users in a given area. To achieve dual compatibility, a custom VR player was built. To the extent of my knowledge, this is the only player of its kind that is dual-compatible.
To host the virtual reality player, associated course material, tutorials, and guidance, an online platform was built. To ensure this was also as accessible as possible, it was published with full open access and any remaining barriers to entry and friction points were removed: there are no requirements to sign up, register, log in, or pay any fees. To the extent of my knowledge, this is the only offering of its kind that is fully open access.
In summary, as multi-device and multi-operating system compatibility and open access were achieved, I was content that I had created a first-of-its-kind platform that had greatly increased accessibility of the treatment.
Efficacy
Prior researchers have noted that the efficacy of VRET could be improved with the option of more engaging, more photorealistic, and more challenging scenarios (Rapee and Heimberg, 1997; Fergus et al., 2009; Nazligul et al., 2017; Söyler et al., 2017; Premkumar et al., 2021). This led me to develop the concept of overexposure therapy (OT): training in extreme scenarios that one is unlikely to encounter in real life.
Conventionally, a student practices a presentation alone in their rooms. Accordingly, it can feel like a significant step up when they present in front of, even a very small class of students. By contrast, if a student were partaking in OT, they may have practiced in front of thousands of highly distracting spectators, and, as a result, when they present to their classmates, it could feel like a significant step down. In short, OT may be a powerful strategy to build extra confidence, adaptability, and resilience. It could be thought of as the psychological equivalent of ‘running with weights’ or ‘training at high altitude’.
To implement OT, I built a wide range of virtual reality training environments, starting with an empty classroom, and incrementally scaling all the way up to a stage inside of a highly-distracting stadium in front of 10,000 spectators. To the extent of my knowledge, this is the only offering of its kind that goes significantly beyond what an individual is likely to encounter in their lifetimes.
To make the audiences as realistic as possible, the audiences were animated, photorealistic, and accompanied by authentic sound effects. Natural audience movements such as head scratching and yawning were included to add further realism. Spontaneous distractions such as audience members arriving late or leaving and camera flashes were also included. I used a combination of live audience spherical video captures and computer-generated imagery to create the virtual reality training environments. Although, in theory, OT could be implemented in vivo (e.g., one could hire a stadium), it is significantly more feasible, scalable, and replicable with the use of virtual reality. The latter, virtual reality overexposure therapy (VROT) is what is explored in the reported experiment (example of VROT shown in Figure 2).

Figure 2. Example of VROT in the reported study.
In summary, as overexposure and dynamic photorealism were achieved, I was content that the platform had the potential to increase the efficacy of the treatment.
Prior to the experiment, multiple pre-tests were conducted. This culminated with a large-scale live stress testing exercise: during a 16-hour window, over 1,000 members of the public used the platform in a demo area at the University of Cambridge. This allowed me to stress test the platform at scale with a diverse pool of participants. The results confirmed that the available device mount hardware and platform architecture were robust. As a result, I progressed to the efficacy evaluation experiment stage.
Experiment
The reported experiment explores the efficacy of a single 30-minute session of VROT.
Hypotheses
H1 = Fewer students will describe themselves as anxious public speakers after VROT.
H2 = More students will describe themselves as confident public speakers after VROT.
H3 = More students will state that they enjoy public speaking after VROT.
Participants
29 students took part in the experiment. All students were from China and aged 13–15 (20 boys, 9 girls). The students were visiting Cambridge, United Kingdom, as part of a summer school programme. It was noted by the programme organiser that a session to help the students feel less anxious when speaking English would be beneficial as it would empower the students to make the most of their time in England.
Procedure
1 week prior to the 30-minute session, the students were asked to write and memorise a 1-minute script in English that introduces themselves (e.g., name, age, interests). At the beginning of the 30-minute session, the students were taught a relaxation technique known as 4–7–8. This technique involves breathing in through the nose for a count of 4, holding one’s breath for a count of 7, and exhaling from the mouth for a count of 8 (Aktaş and İlgin, 2023). The 30-minute session comprised of the six stages shown in Table 1.
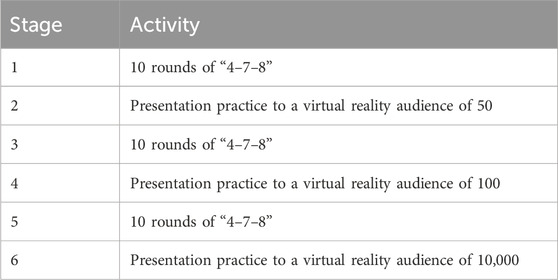
Table 1. 6-stage procedure.
After the 30-minute session, each student stood in front of the classroom and presented their presentation to the class. The classroom comprised of 35 people: 29 students and 6 members of staff. Therefore, each student presented to an audience of 34 which was significantly smaller than the virtual reality audiences in their practice sessions. Survey data was captured before the 30-minute session and after the presentations. Staff members were on hand to translate and/or clarify.
Results
When comparing the before and after survey results (shown in Table 2 and Figure 3), the data revealed a decrease of 45 percentage points in students who describe themselves as anxious public speakers (65% vs 20%), an increase of 48 percentage points in students who describe themselves as confident public speakers (31% vs 79%), and an increase of 52 percentage points in students who stated that they enjoy public speaking (34% vs 86%).

Table 2. Questions and responses.
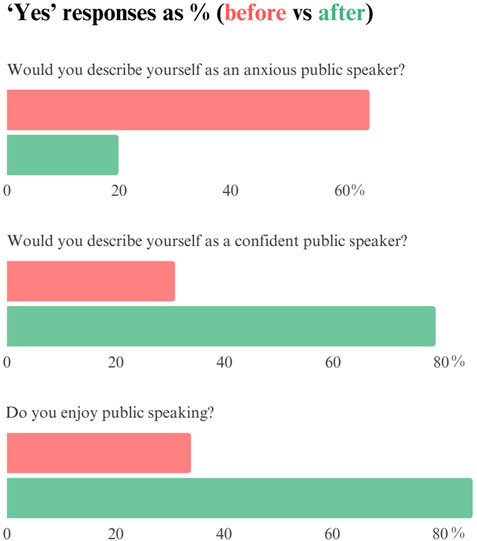
Figure 3. Bar graph of results.
H1
The responses required to assess the three hypotheses involve dichotomous variables from within-subjects. Accordingly, I used McNemar tests to assess for statistical significance. Hypothesis 1 was that fewer students would describe themselves as anxious public speakers after VROT. The data supports this hypothesis as there was a decrease of 45 percentage points in students who describe themselves as anxious public speakers (65% vs 20%). The H1 significance test revealed that there was a statistically significant difference when comparing the before and after data (χ2 (1) = 11.077, p = 0.0008), with a medium effect size (Cohen’s h = 0.474). Therefore, the null hypothesis is rejected and H1 holds.
H2
Hypothesis 2 was that more students will describe themselves as confident public speakers after VROT. The data supports this hypothesis as there was an increase of 48 percentage points in students who describe themselves as confident public speakers (31% vs 79%). The H2 significance test revealed that there was a statistically significant difference when comparing the before and after data (χ2 (1) = 12.071, p = 0.0005), with a medium effect size (Cohen’s h = 0.504). Therefore, the null hypothesis is rejected and H2 holds.
H3
Hypothesis 3 was that more students will state that they enjoy public speaking after VROT. The data supports this hypothesis as there was an increase of 52 percentage points in students who stated that they enjoyed public speaking (34% vs 86%). The H3 significance test revealed that there was a statistically significant difference when comparing the before and after data (χ2 (1) = 13.067, p = 0.0003), with a medium effect size (Cohen’s h = 0.565). Therefore, the null hypothesis is rejected and H3 holds.
Discussion
The fear of public speaking is pervasive and harmful (Richmond and McCroskey, 1998; Furmark et al., 1999; Dwyer and Davidson, 2012; Grieve et al., 2021; Kahlon et al., 2023). Accordingly, there is a need for a widely accessible and highly effective treatment option. The open access VR platform detailed in this paper seeks to achieve this goal. By enabling users to practice public speaking from any location to a range of audiences, for free, using their smartphones, it dismantles barriers to traditional exposure therapy such as cost, location, device type, and time constraints. The experiment results demonstrate significant improvements in self-reported anxiety, confidence, and enjoyment of public speaking after a single 30-minute session.
The concept of overexposure therapy opens up new avenues for building resilience and reducing anxiety in ways previously not feasible. When Joseph Wolpe was pioneering exposure therapy in the 1950s (Wolpe, 1954; Wolpe, 1958), he couldn't have predicted that the average citizen would someday have the ability to freely and instantly transport themselves into extreme fear-inducing scenarios, let alone into a virtual reality stadium with an audience of 10,000 photorealistic spectators. The ability to freely access and repeatedly train in such extreme scenarios presents a wealth of new and exciting opportunities.
The current research represents a starting point. It is important to acknowledge that the reported single-session single-arm experiment has limitations. Further investigation that incorporates control groups and explores long-term effects across diverse demographics are important next steps. It is also important to note that no conclusions regarding VROT vs. standard VRET can be drawn as the two are not directly compared in this study.
As this is a novel treatment option, it would also be valuable to seek to optimise the protocol. For example, the protocol in the experiment combined relaxation techniques with exposure to fear-inducing stimuli. This approach is a traditional systematic desensitisation form of exposure therapy that is based on Wolpe’s concept of reciprocal inhibition: e.g., “that an individual cannot be relaxed and anxious simultaneously” (Norwood and Ursano, 2002). The idea being that by pairing feared stimuli with relaxation techniques, it will “evoke a response incompatible with fear or anxiety” (Knowles and Olatunji, 2019). While this approach has been shown to be effective (Rachman, 1967), additional justifications to incorporate relaxation techniques into the reported experiment were based on the unparalleled scale of the virtual reality content (10,000 photorealistic spectators) and the fact that the participants did not construct or select the hierarchy of feared stimuli.
While there were valid justifications for this approach, multiple researchers have argued that the active ingredient in exposure therapy is not the use of relaxation techniques, or even gradation, but instead the mere repeated exposure to feared stimuli (Marks, 1972; Morganstern, 1973; Marks, 1975; Tryon, 2005; Craske et al., 2012; Knowles and Olatunji, 2019; Carona et al., 2023). Accordingly, foregoing or decreasing relaxation techniques and/or gradation may be a more efficient protocol with overexposure therapy. However, it is also important to note that an optimal approach needs to consider buy-in and acceptability in addition to efficiency; relaxation techniques may facilitate greater uptake and gradation may increase engagement through gamification and thus decreasing dropout rates. Furthermore, gradation may facilitate autonomy through a logical and agreed end-point to the treatment.
Future exploration should also consider setting. As noted by others (Chowdhury and Khandoker, 2023), there is a need for investigations exploring self-guided VR treatment in home settings. As increased scalability is a core component of this project, a priority for future research should include exploring VROT in a range of accessible settings including the patient’s home and a freely bookable space (e.g., at a higher education institution, community centre, public library).
It may also be valuable to explore alternative assessment methods. It has been noted that physiological measures are a suboptimal approach for the assessment of public speaking anxiety: e.g., “arousal is not necessarily the same as anxiety” (Gallego et al., 2022). By contrast, self-report measures are more typically used and have demonstrated both good reliability and validity (Gallego et al., 2022). Accordingly, a self-report measure was used in the reported experiment, however, due to time constraints with the participant cohort and potential language barriers, a simplified version was used. In future experiments, an established self-report measure—e.g., the Public Speaking Anxiety Scale (Bartholomay and Houlihan, 2016) or the Liebowitz Social Anxiety Scale (Liebowitz, 1987)—could be used to gain further insights and facilitate comparison of results with other studies. In addition to this, it would also be valuable to assess the user’s familiarity and openness to treatment technology; prior studies have indicated that both openness to treatment technology and general familiarity with digital technology may increase efficacy of digital treatments (Kothgassner et al., 2019; Hawajri et al., 2023).
The open access nature of the platform facilitates further exploration, replication, and collaboration. This is a great opportunity to empower individuals to overcome their fear of public speaking, ultimately enhancing not only their quality of life but also their capacity to become a driving force of positive change in the world.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by ROLVIC Global Education, chaired by Dr Xing Chen. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’; legal guardians/next of kin.
Author contributions
CM: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing–original draft, Writing–review and editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. Lucy Cavendish College, University of Cambridge provided funding for publication costs.
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The authors declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Aarons, G. A., Monn, A. R., Leslie, L. K., Garland, A. F., Lugo, L., Hough, R. L., et al. (2008). Association between mental and physical health problems in high-risk adolescents: a longitudinal study. J. Adolesc. Health 43 (3), 260–267. doi:10.1016/j.jadohealth.2008.01.013
Abramowitz, J. S., Deacon, B. J., and Whiteside, S. P. (2019). Exposure therapy for anxiety: principles and practice. 2nd ed. London: Guilford Publications.
Aderka, I. M., Hofmann, S. G., Nickerson, A., Hermesh, H., Gilboa-Schechtman, E., and Marom, S. (2012). Functional impairment in social anxiety disorder. J. Anxiety Disord. 26 (3), 393–400. doi:10.1016/j.janxdis.2012.01.003
Aktaş, G. K., and İlgin, V. E. (2023). The effect of deep breathing exercise and 4-7-8 breathing techniques applied to patients after bariatric surgery on anxiety and quality of life. Obes. Surg. 33 (3), 920–929. doi:10.1007/s11695-022-06405-1
Alami, S., Stieglitz, J., Kaplan, H., and Gurven, M. (2018). Low perceived control over health is associated with lower treatment uptake in a high mortality population of Bolivian forager-farmers. Soc. Sci. Med. 200, 156–165. doi:10.1016/j.socscimed.2018.01.017
Anderson, P. L., Edwards, S. M., and Goodnight, J. R. (2017). Virtual reality and exposure group therapy for social anxiety disorder: results from a 4–6 Year follow-up. Cogn. Ther. Res. 41 (2), 230–236. doi:10.1007/s10608-016-9820-y
Anderson, P. L., Price, M., Edwards, S. M., Obasaju, M. A., Schmertz, S. K., Zimand, E., et al. (2013). Virtual reality exposure therapy for social anxiety disorder: a randomized controlled trial. J. Consult Clin. Psychol. 81, 751–760. doi:10.1037/a0033559
Bardone, A. M., Moffitt, T. E., Caspi, A., Dickson, N., Stanton, W. R., and Silva, P. A. (1998). Adult physical health outcomes of adolescent girls with conduct disorder, depression, and anxiety. J. Am. Acad. Child. Adolesc. Psychiatry 37 (6), 594–601. doi:10.1097/00004583-199806000-00009
Barlow, D. H., Gorman, J. M., Shear, M. K., and Woods, S. W. (2000). Cognitive-behavioral therapy, imipramine, or their combination for panic disorder: a randomized controlled trial. JAMA 283 (19), 2529–2536. doi:10.1001/jama.283.19.2529
Bartholomay, E. M., and Houlihan, D. D. (2016). Public speaking anxiety scale: preliminary psychometric data and scale validation. Personal. Individ. Differ. 94, 211–215. doi:10.1016/j.paid.2016.01.026
Bhanji, J., Kim, E., and Delgado, M. (2016). Perceived control alters the effect of acute stress on persistence. J. Exp. Psychol. 145, 356–365. doi:10.1037/xge0000137
Botella, C., Fernández-Álvarez, J., Guillén, V., García-Palacio, A., and Baños, R. (2017). Recent progress in virtual reality exposure therapy for phobias: a systematic review. Curr. Psychiatry Rep. 19, 42. doi:10.1007/s11920-017-0788-4
Bouchard, S., Dumoulin, S., Robillard, G., Guitard, T., Klinger, E., Forget, H., et al. (2017). Virtual reality compared with in vivo exposure in the treatment of social anxiety disorder: a three-arm randomised controlled trial. Br. J. Psychiatry 210 (4), 276–283. doi:10.1192/bjp.bp.116.184234
Bradley, R., Greene, J., Russ, E., Dutra, L., and Westen, D. (2005). A multidimensional meta-analysis of psychotherapy for PTSD. Am. J. Psychiatry 162, 214–227. doi:10.1176/appi.ajp.162.2.214
Buchholz, J. L., and Abramowitz, J. S. (2020). The therapeutic alliance in exposure therapy for anxiety-related disorders: a critical review. J. Anxiety Disord. 70, 102194. doi:10.1016/j.janxdis.2020.102194
Cahill, S. P., Rothbaum, B. O., Rosick, P. A., and Folette, V. (2009). “Cognitive-behavioural therapy for adults,” in Effective treatments for PTSD. Editors E. B. Foa, T. M. Keane, M. J. Friedman, and J. A. Cohen (New York: The Guilford Press), 139–222.
Carl, E., Stein, A. T., Levihn-Coon, A., Pogue, J. R., Rothbaum, B., Emmelkamp, P., et al. (2019). Virtual reality exposure therapy for anxiety and related disorders: a meta-analysis of randomized controlled trials. J. Anxiety Disord. 61, 27–36. doi:10.1016/j.janxdis.2018.08.003
Carona, C., Ramos, K., and Salvador, C. (2023). Psychotherapy by Reciprocal Inhibition: Wolpe’s unique legacy to the evolution of cognitive–behavioural therapy. BJPsych Adv. 29 (3), 218–222. doi:10.1192/bja.2022.75
Chowdhury, N., and Khandoker, A. H. (2023). The gold-standard treatment for social anxiety disorder: a roadmap for the future. Front. Psychol. 13, 1070975. doi:10.3389/fpsyg.2022.1070975
Craske, M. G., Liao, B., and Vervliet, B. (2012). Role of inhibition in exposure therapy. J. Exp. Psychopathol. 3, 322–345. doi:10.5127/jep.026511
Dwyer, K. K., and Davidson, M. (2012). Is public speaking really more feared than death? Commun. Res. Rep. 29 (2), 99–107. doi:10.1080/08824096.2012.667772
Evans, B., and Fischer, D. (1992). A hierarchical model of participatory decision-making, job autonomy, and perceived control. Hum. Relat. 45, 1169–1189. doi:10.1177/001872679204501103
Fedoroff, I. C., and Taylor, S. (2001). Psychological and pharmacological treatments of social phobia: a meta-analysis. J. Clin. Psychopharmacol. 21 (3), 311–324. doi:10.1097/00004714-200106000-00011
Fergus, T. A., Valentiner, D. P., McGrath, P. B., Stephenson, K., Gier, S., and Jecius, S. (2009). The fear of positive evaluation scale: psychometric properties in a clinical sample. J. Anxiety Disord. 23, 1177–1183. doi:10.1016/j.janxdis.2009.07.024
Foa, E. B., Liebowitz, M. R., Kozak, M. J., Davies, S., Campeas, R., Franklin, M. E., et al. (2005). Randomized, placebo-controlled trial of exposure and ritual prevention, clomipramine, and their combination in the treatment of obsessive-compulsive disorder. Am. J. Psychiatry 162 (1), 151–161. doi:10.1176/appi.ajp.162.1.151
Furmark, T., Tillfors, M., Everz, P., Marteinsdottir, I., Gefvert, O., and Fredrikson, M. (1999). Social phobia in the general population: prevalence and sociodemographic profile. Soc. Psychiatry Psychiatr. Epidemiol. 34 (8), 416–424. doi:10.1007/s001270050163
Gallego, A., McHugh, L., Penttonen, M., and Lappalainen, R. (2022). Measuring public speaking anxiety: self-report, behavioral, and physiological. Behav. Modif. 46 (4), 782–798. doi:10.1177/0145445521994308
Greenberg, P. E., Sisitsky, T., Kessler, R. C., Finkelstein, S. N., Berndt, E. R., Davidson, J. R., et al. (1999). The economic burden of anxiety disorders in the 1990s. J. Clin. Psychiatry 60 (7), 427–435. doi:10.4088/jcp.v60n0702
Grieve, R., Woodley, J., Hunt, S. E., and McKay, A. (2021). Student fears of oral presentations and public speaking in higher education: a qualitative survey. J. Furth. High. Educ. 45 (9), 1281–1293. doi:10.1080/0309877X.2021.1948509
Hawajri, O., Lindberg, J., and Suominen, S. (2023). Virtual reality exposure therapy as a treatment method against anxiety disorders and depression-A structured literature review. Issues Ment. Health Nurs. 44 (4), 245–269. doi:10.1080/01612840.2023.2190051
Horigome, T., Kurokawa, S., Sawada, K., Kudo, S., Shiga, K., Mimura, M., et al. (2020). Virtual reality exposure therapy for social anxiety disorder: a systematic review and meta-analysis. Psychol. Med. 50, 2487–2497. doi:10.1017/S0033291720003785
Jefferies, P., and Ungar, M. (2020). Social anxiety in young people: a prevalence study in seven countries. PLoS ONE 15 (9), e0239133. doi:10.1371/journal.pone.0239133
Kahlon, S., Lindner, P., and Nordgreen, T. (2023). Gasified virtual reality exposure therapy for adolescents with public speaking anxiety: a four-armed randomized controlled trial. Front. Virtual Real. 4, 2673–4192. doi:10.3389/frvir.2023.1240778
Kampmann, I. L., Emmelkamp, P. M., and Morina, N. (2016). Meta-analysis of technology-assisted interventions for social anxiety disorder. J. Anxiety Disord. 42, 71–84. doi:10.1016/j.janxdis.2016.06.007
Kaplan, J. S., and Tolin, D. F. (2011). Exposure therapy for anxiety disorders. Psychiatr. Times 28 (9). Available at: https://www.psychiatrictimes.com/view/exposure-therapy-anxiety-disorders.
Knowles, K. A., and Olatunji, B. O. (2019). Enhancing inhibitory learning: the utility of variability in exposure. Cogn. Behav. Pract. 26 (1), 186–200. doi:10.1016/j.cbpra.2017.12.001
Kothgassner, O. D., Goreis, A., Kafka, J. X., Van Eickels, R. L., Plener, P. L., and Felnhofer, A. (2019). Virtual reality exposure therapy for posttraumatic stress disorder (PTSD): a meta-analysis. Eur. J. Psychotraumatology 10 (1), 1654782. doi:10.1080/20008198.2019.1654782
Langthorne, D., Beard, J., and Waller, G. (2023). Therapist factors associated with intent to use exposure therapy: a systematic review and meta-analysis. Cogn. Behav. Ther. 4, 347–379. doi:10.1080/16506073.2023.2191824
Liebowitz, M. R. (1987). Social phobia. Mod. Problems Pharmacopsychiatry 22, 141–173. doi:10.1159/000414022
Lindner, P., Dagöö, J., Hamilton, W., Miloff, A., Andersson, G., Schill, A., et al. (2020). Virtual Reality exposure therapy for public speaking anxiety in routine care: a single-subject effectiveness trial. Cogn. Behav. Ther. 50 (1), 67–87. doi:10.1080/16506073.2020.1795240
Lindner, P., Miloff, A., Fagernäs, S., Andersen, J., Sigeman, M., Andersson, G., et al. (2019). Therapist-led and self-led one-session virtual reality exposure therapy for public speaking anxiety with consumer hardware and software: a randomized controlled trial. J. Anxiety Disord. 61, 45–54. doi:10.1016/j.janxdis.2018.07.003
Marinho, A. C. F., Mesquita de Medeiros, A., Côrtes Gama, A. C., and Caldas Teixeira, L. (2017). Fear of public speaking: perception of College students and correlates. J. Voice 31 (1), 7–11. doi:10.1016/j.jvoice.2015.12.012
Marks, I. (1979). Cure and care of neurosis. I. Cure. Psychol. Med. 9 (4), 629–643. doi:10.1017/S0033291700033961
Marks, I. M. (1972). Perspective on flooding. Seminars Psychiatry 4, 129–138. Available at: https://pubmed.ncbi.nlm.nih.gov/4155532/.
Marks, I. M. (1975). Behavioral treatments of phobic and obsessive-compulsive disorders: a critical appraisal. Prog. Behav. Modification 1, 65–158. doi:10.1016/B978-0-12-535601-5.50010-X
Morganstern, K. P. (1973). Implosive therapy and flooding procedures: a critical review. Psychol. Bull. 79 (5), 318–334. doi:10.1037/h0034571
Morina, N., Kampmann, I., Emmelkamp, P., Barbui, C., and Hoppen, T. H. (2023). Meta-analysis of virtual reality exposure therapy for social anxiety disorder. Psychol. Med. 53, 2176–2178. doi:10.1017/S0033291721001690
Nazligul, M. D., Yilmaz, M., Gulec, U., Gozcu, M. A., O'Connor, R. V., and Clarke, P. M. (2017). “Overcoming public speaking anxiety of software engineers using virtual reality exposure therapy,” in Systems, software and services process improvement. EuroSPI. Communications in computer and information science. Vol. 748 (Cham: Springer), 191–202.
Norwood, A. E., and Ursano, R. J. (2002). “Posttraumatic stress disorder,” in Encyclopedia of psychotherapy. Editors M. Hersen,, and W. Sledge (Academic Press), 373–378. doi:10.1016/B0-12-343010-0/00166-5
Ost, L. G. (1989). One-session treatment for specific phobias. Behav. Res. Ther. 27 (1), 1–7. doi:10.1016/0005-7967(89)90113-7
Ougrin, D. (2011). Efficacy of exposure versus cognitive therapy in anxiety disorders: systematic review and meta-analysis. BMC Psychiatry 11, 200. doi:10.1186/1471-244X-11-200
Owens, M. E., and Beidel, D. C. (2015). Can virtual reality effectively elicit distress associated with social anxiety disorder? J. Psychopathol. Behav. Assess. 37, 296–305. doi:10.1007/s10862-014-9454-x
Poeschl, S. (2017). Virtual reality training for public speaking—a quest-vr Framework validation. Front. ICT 4, 13. doi:10.3389/fict.2017.00013
Premkumar, P., Heym, N., Brown, D. J., Battersby, S., Sumich, A., Huntington, B., et al. (2021). The effectiveness of self-guided virtual-reality exposure therapy for public-speaking anxiety. Front. Psychiatry 12, 694610. doi:10.3389/fpsyt.2021.694610
Punton, G., Dodd, A. L., and McNeill, A. (2022). ‘You’re on the waiting list’: an interpretive phenomenological analysis of young adults’ experiences of waiting lists within mental health services in the UK. PLoS ONE 17 (3), e0265542. doi:10.1371/journal.pone.0265542
Ranta, K., Aalto-Setälä, T., Heikkinen, T., and Kiviruusu, O. (2024). Social anxiety in Finnish adolescents from 2013 to 2021: change from pre-COVID-19 to COVID-19 era, and mid-pandemic correlates. Soc. Psychiatry Psychiatr. Epidemiol. 59, 121–136. doi:10.1007/s00127-023-02466-4
Rapee, R. M., and Heimberg, R. G. (1997). A cognitive-behavioral model of anxiety in social phobia. Behav. Res. Ther. 35, 741–756. doi:10.1016/S0005-7967(97)00022-3
Reeves, R., Curran, D., Gleeson, A., and Hanna, D. (2022). A meta-analysis of the efficacy of virtual reality and in vivo exposure therapy as psychological interventions for public speaking anxiety. Behav. Modif. 46, 937–965. doi:10.1177/0145445521991102
Richmond, V., and McCroskey, J. C. (1998). Communication: apprehension, avoidance, and effectiveness. 5th ed. Scottsdale, AZ: Gorsuch Scarisbrick.
Rosa-Alcázar, A. I., Sánchez-Meca, J., Gómez-Conesa, A., and Marín-Martínez, F. (2008). Psychological treatment of obsessive-compulsive disorder: a meta-analysis. Clin. Psychol. Rev. 28, 1310–1325. doi:10.1016/j.cpr.2008.07.001
Ruscio, A. M., Brown, T. A., Chiu, W. T., Sareen, J., Stein, M. B., and Kessler, R. C. (2008). Social fears and social phobia in the USA: results from the national comorbidity survey replication. Psychol. Med. 38 (1), 15–28. doi:10.1017/S0033291707001699
Russell, G., and Shaw, S. (2009). A study to investigate the prevalence of social anxiety in A sample of higher education students in the United Kingdom. J. Ment. Health 18 (3), 198–206. doi:10.1080/09638230802522494
Russell, G., and Topham, P. (2012). The impact of social anxiety on student learning and well-being in higher education. J. Ment. Health 21 (4), 375–385. doi:10.3109/09638237.2012.694505
Sánchez-Meca, J., Rosa-Alcázar, A. I., Marín-Martínez, F., and Gómez-Conesa, A. (2010). Psychological treatment of panic disorder with or without agoraphobia: a meta-analysis. Clin. Psychol. Rev. 30, 37–50. doi:10.1016/j.cpr.2009.08.011
Sareen, J., Cox, B. J., Clara, I., and Asmundson, G. J. (2005). The relationship between anxiety disorders and physical disorders in the U.S. National Comorbidity Survey. Depress Anxiety 21 (4), 193–202. doi:10.1002/da.20072
Sarpourian, F., Samad-Soltani, T., Moulaei, K., and Bahaadinbeigy, K. (2022). The effect of virtual reality therapy and counseling on students' public speaking anxiety. Health Sci. Rep. 20 (5), e816. doi:10.1002/hsr2.816
Sars, D., and van Minnen, A. (2015). On the use of exposure therapy in the treatment of anxiety disorders: a survey among cognitive behavioural therapists in The Netherlands. BMC Psychol. 3 (1), 26. doi:10.1186/s40359-015-0083-2
Seuling, P. D., Czernin, N. S., and Schiele, M. A. (2024). Virtual Reality exposure therapy in the treatment of public speaking anxiety and social anxiety disorder. Neurosci. Appl. 3, 104074. doi:10.1016/j.nsa.2024.104074
Sirur, R., Richardson, J., Wishart, L., and Hanna, S. (2009). The role of theory in increasing adherence to prescribed practice. Physiother. Can. 61, 68–77. doi:10.3138/physio.61.2.68
Söyler, E., Gunaratne, C., and Akbaş, M. I. (2017). “Towards a comprehensive simulator for public speaking anxiety treatment,” in Advances in applied digital human modeling and simulation. Advances in intelligent systems and computing (Cham: Springer), 195–205. doi:10.1007/978-3-319-41627-4_18
StatCounter (2024). Mobile operating system market share. Available at: https://gs.statcounter.com/os-market-share/mobile/worldwide#yearly-2009-2024 (Accessed August 10, 2024).
Tolin, D. F. (2010). Is cognitive-behavioral therapy more effective than other therapies? A meta-analytic review. Clin. Psychol. Rev. 30 (6), 710–720. doi:10.1016/j.cpr.2010.05.003
Tryon, W. W. (2005). Possible mechanisms for why desensitization and exposure therapy work. Clin. Psychol. Rev. 25 (1), 67–95. doi:10.1016/j.cpr.2004.08.005
Valmaggia, L. R., Latif, L., Kempton, M. J., and Rus-Calafell, M. (2016). Virtual reality in the psychological treatment for mental health problems: an systematic review of recent evidence. Psychiatry Res. 236, 189–195. doi:10.1016/j.psychres.2016.01.015
Wolpe, J. (1954). Reciprocal Inhibition as the main basis of psychotherapeutic effects. Achieves Neurology Psychiatry 72, 205–226. doi:10.1001/archneurpsyc.1954.02330020073007
Keywords: virtual reality exposure therapy, public speaking anxiety, fear of public speaking, overexposure therapy, VROT, VRET, reducing anxiety, anxiety
Citation: Macdonald C (2024) Improving virtual reality exposure therapy with open access and overexposure: a single 30-minute session of overexposure therapy reduces public speaking anxiety. Front. Virtual Real. 5:1506938. doi: 10.3389/frvir.2024.1506938
Received: 06 October 2024; Accepted: 30 November 2024;
Published: 16 December 2024.
Edited by:
Stephen Palmisano, University of Wollongong, AustraliaReviewed by:
Peter Eachus, University of Salford, United KingdomMatthew Coxon, York St John University, United Kingdom
Copyright © 2024 Macdonald. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chris Macdonald, Y20yMTUwQGNhbS5hYy51aw==