 Sara A. Freedman1*
Sara A. Freedman1* Ehud Dayan2
Ehud Dayan2 Michal Senitsky1Elisheva Bellin1Yossi Attias1Tzvi Richman1Renana Eitan3Lucian Tatsa-Laur4
Michal Senitsky1Elisheva Bellin1Yossi Attias1Tzvi Richman1Renana Eitan3Lucian Tatsa-Laur4- 1School of Social Work, Bar Ilan University, Ramat Gan, Israel
- 2Sonarion Ltd, Jerusalem, Israel
- 3Tel Aviv Medical Center—Ichilov, Tel Aviv, Israel
- 4Health Department, Medical Corps, Israel Defense Forces, Tel Aviv, Israel
Posttraumatic stress disorder (PTSD) occurs in approximately 20% of individuals following exposure to a potentially traumatic event. Re-experiencing in the form of intrusive memories is a hallmark feature, and often includes sensory elements, including odor. A small body of studies have examined the relationship between PTSD and odor evoked memories. Patients avoid smells that remind them of their traumatic event, and odors are known triggers for intrusive memories and distress. PTSD is associated with higher ratings of odor intensity and unpleasantness however accuracy of odor detection is often impaired. It has been suggested that adding trauma-related odors will enhance treatment, however little data exists. This case study illustrates the addition of trauma specific olfaction in Virtual Reality (VR) enhanced exposure therapy for combat related PTSD. Treatment was successful, the patient no longer met criteria for PTSD at the end of treatment, and self-report symptoms scores indicated clinically significant reductions. The patient indicated at the end of treatment that he would not have been helped had the therapy not used VR, and the addition of odors helped him process the traumatic memories. Future research should assess the addition of olfaction in a systematic way, in order to assess its specific impact in the effectiveness of PTSD treatment.
Introduction
“Smell is a potent wizard that transports us across thousands of miles and all the years we have lived…. odors, instantaneous and fleeting, cause my heart to dilate joyously or contract with remembered grief”.
This quote from Helen Keller (Keller, 1910) expresses an experience that is common to us all: being taken back in time, vividly remembering a seemingly forgotten past event after encountering an odor. This is known as the Proust effect, following the example the writer Proust gave of the smell of biscuits that took him back to a lucid childhood memory (Proust and Sturrock, 2003).
Odor evoked memories are autobiographical memories, often from the first decade of life. Perceptual elements of memory include all sensory information: visual, tactile, auditory and olfactory. Studies have shown that olfactory memories are the most likely to be related to remembering emotionally laden events (Toffolo et al., 2012). Odor associated with a stressful situation has been shown in rats to lead to conditioned fear responses to the odor by itself (Bombail, 2019). These findings are also explained by the neuroanatomy of emotion and olfaction: the olfactory system and the limbic system have a direct interconnection (Kontaris et al., 2020).
Posttraumatic stress disorder (PTSD) occurs in approximately 20% of individuals following exposure to a potentially traumatic event (Kessler et al., 2017). Symptoms of PTSD include four constellations: re-experiencing of the traumatic event via flashbacks, nightmares and intrusive memories, avoidance of trauma cues, negative emotions and cognitions and hyperarousal (Schaal et al., 2015). Re-experiencing in the form of intrusive memories are suggested to be fear memories that have not extinguished and are a hallmark feature of the disorder (Duek et al., 2020).
A small body of studies that have examined the relationship between PTSD and odor evoked memories. Widespread anecdotal clinical experience exists regarding patients’ avoidance of smells that remind them of their traumatic event, and odors are known triggers for intrusive memories and distress. As described a century ago by a First World War poet and sufferer of PTSD: “… any unusual smell, even a sudden strong smell of flowers in a garden, was enough to send me trembling.” (Graves, 1960). An early research paper examining aspects of traumatic memories shows that they included odors 77% of the time (Van der Kolk and Fisler, 1995). A study of refugees showed that 45% experienced panic attacks triggered by odor, and many of these involved flashbacks to the traumatic event (Hinton et al., 2004). Between 4%–10% of assault victims with PTSD reported smells or tastes related to intrusions (Michael et al., 2005). A more recent paper describes three case studies that report olfactory triggers for traumatic memories (Vermetten and Bremner, 2003).
Experimental studies of combat related trauma survivors have shown that PTSD is associated with higher ratings of odor intensity and unpleasantness, and odors are more likely to act as triggers for posttraumatic symptoms (Dileo et al., 2008; Cortese et al., 2015; Tjalvin et al., 2017; Bedwell et al., 2018; Wilkerson et al., 2018). One study of PTSD following child maltreatment showed similar results (Croy et al., 2010). Similar to studies of other types of psychopathology such as depression, levels of odor detection in general are impaired in PTSD relative to healthy controls (Dileo et al., 2008; Cortese et al., 2015). Taken together these studies indicate that PTSD symptom levels are related to increased sensitivity to unpleasant trauma-related odors, which cause more distress, while at the same time showing decreased sensitivity to odors in general. These studies clearly point to the conclusion that olfactory memories may play an important role in PTSD.
PTSD is a chronic and costly disorder (Kessler, 2000) and current effective treatments help only between 60%–70% of people (Bisson et al., 2019). The most effective PTSD treatments involve interventions that target traumatic memories, with a goal of moving from a perceptual sensory memory to one that is more verbal (Foa and Kozak, 1986). These trauma-focused cognitive behavioural treatments (TF-CBT) often ask the patient to reconstruct the narrative of the traumatic event, telling this story repeatedly. It is important that the patient feels emotionally connected to this narrative, so the patient is requested to close their eyes, and use first person, present tense, in order to facilitate this. However, this key component of therapy can be challenging: some patients do not have clear memories of the event, while others find it hard to retell the narrative of these memories. Often, with events that involve atrocities or unusual elements, the patient finds it hard to find the appropriate language. Therefore, ways to embellish this type of therapy with agents that will enhance memory retrieval or reconsolidation such as D-cycloserine (Cukor et al., 2009; de Kleine et al., 2015) and intranasal oxytocin (Flanagan et al., 2018) have been examined.
The use of Virtual Reality (VR) to enhance this type of therapy is well established (e.g., (‘Skip’ and Shilling, 2017; Rizzo et al., 2009; Skip et al., 2010; Rothbaum et al., 2001)) and allows the patient to retell the narrative while inside a headset, experiencing scenes that are similar to the traumatic event. VR enhanced therapy is effective, and can overcome some barriers to treatment, such as avoidance, as well as allowing the patient easier access to emotions when retelling the narrative.
It has been suggested that adding odors that are related to the traumatic event will improve treatment outcomes, and this has been carried out both in hypnotherapy (Abramowitz and Lichtenberg, 2010) as well as in the context of Virtual Reality enhanced Exposure Therapy (Van Veelen et al., 2021; Lo and Hurley, 2022), This case study describes the treatment of combat related PTSD using VR enhanced exposure therapy with the addition of olfaction.
Case description
Patient Y
Y was a 25-year-old single man, with no history of psychiatric problems. He was an army veteran, who had served in compulsory service from the ages of 18–21. During the last year of his service he was serving as a combat medic during a month-long conflict, when he was exposed to several potentially traumatic events. Y developed symptoms of PTSD immediately following the conflict. During the next 4 years, his symptoms worsened but he did not seek help during this time. He self-referred for treatment 4 years later. Figure 1 illustrates the timeline of his history and treatment.
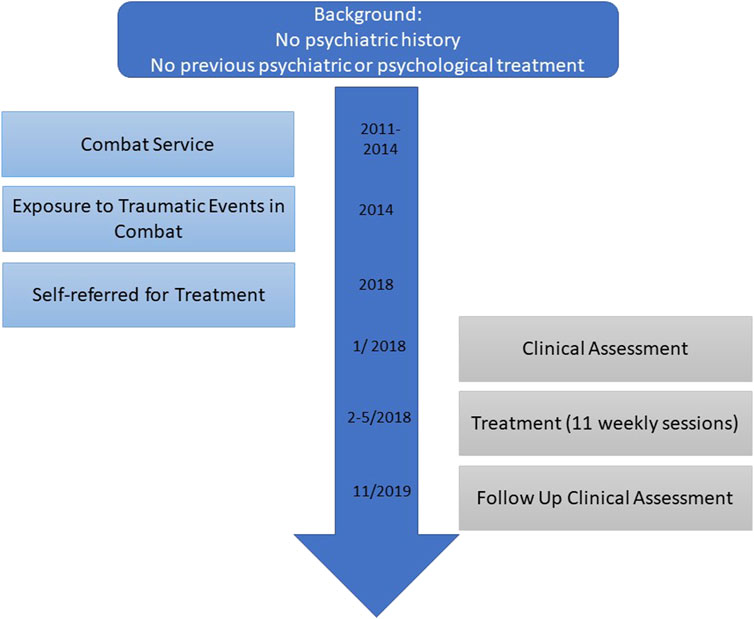
FIGURE 1. Timeline of treatment.
Current treatment
The treatment took place as part of an ongoing randomized clinical trial comparing Prolonged Exposure with Virtual Reality enhanced Exposure Therapy, for combat related PTSD. The study was approved by the Helsinki Committee, Jerusalem Mental Health Center and the Medical Unit, IDF (NCT-03000478). Participants were assessed pre and post treatment by an assessor blind to treatment condition.
Assessment measures
A clinical assessment was carried out by a trained clinician before and after treatment. This included self-report measures:
PTSD symptom levels were measured using the PCL5 (Blevins et al., 2015), a 20 item self-report questionnaire covering all PTSD symptoms.
Depression symptom levels were measured using the BDI (Beck et al., 1996) a 21 item self-report questionnaire.
Dissociation levels were measured using the DES (Sheehan et al., 1998) a 28 item self-report questionnaire.
In addition, clinical interviews were carried out: the MINI (Sheehan et al., 1998) o assess all current and past Axis I psychiatric disorders, and the CAPS5 (Weathers et al., 2013) to assess PTSD intensity and presence.
Instruments
The Virtual Reality system used Oculus Rift VR goggles with 110° diagonal fields of view per eye and 1080 by 120 pixels resolution per eye (90 hz). The goggles were plugged into a workstation with Intel Core i5 6500 (3.2 GHz) 8 GB Memory 1 TB HDD NVIDIA GeForce GTX 970 4 GB GDDR5. The software (Virtual Azza) was developed by Sonarion Ltd. using Unity and used urban fighting scenes. Some of the scenes contained soldiers, military vehicles and tank turrets. The OS was windows 10- home edition - 64 bit (Figure 2).
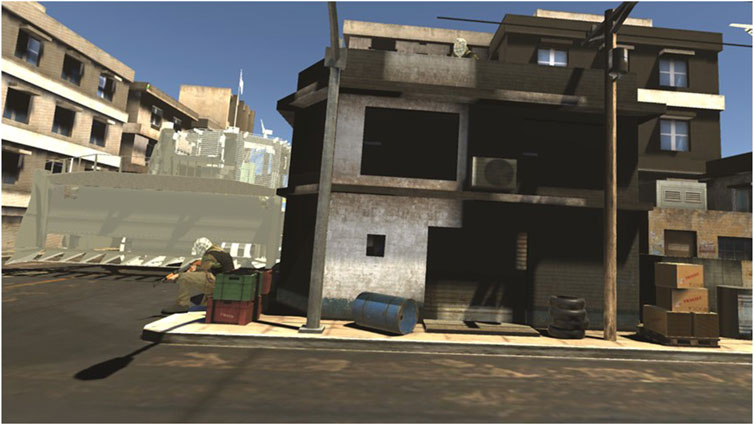
FIGURE 2. Scene from virtual Azza.
Olfaction System: The ScentMixer system designed by Sonarion Ltd. (http://sonarion.com) was used in this project (Figure 2). The system enables the therapist to dictate odor release manually or automatically. When using the auto mode, the odor intensity varies in relation to the position of the smell source in the VR scene. The odor flow releases short (few seconds) airbursts in ∼300 mHg pressure producing an airflow of 0.03LPM/s. As can be seen in Figure 3, the odor is released a few centimeters from the patient nose via a tube attached to the VR headset. The odor is then washed away by fresh air. Different scents can be added, dependent on the patient’s individual narrative; in the case presented here gun oil was used.
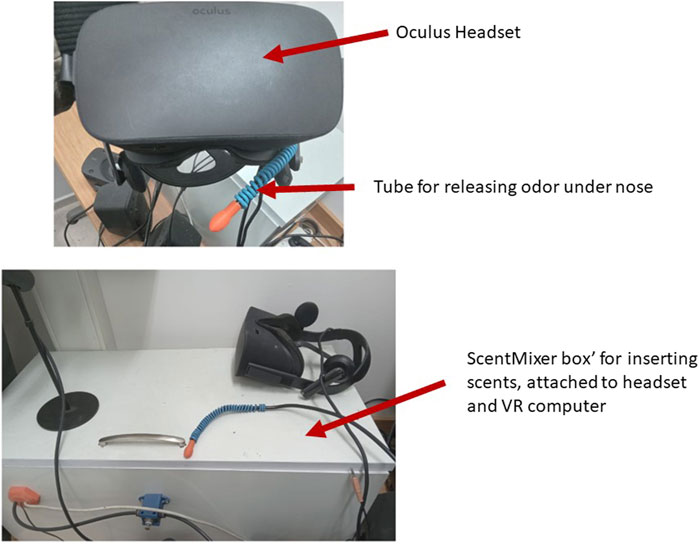
FIGURE 3. Scent mixer.
Procedure
All participants, including Y, signed written informed consent. Y also signed permission to publish details of his treatment. Y was randomized to receive Virtual Reality enhanced treatment. All therapists had received training in Cognitive Behavior Therapy, in Prolonged Exposure, in the use of VR and the VR enhanced exposure therapy protocol and received weekly supervision from SAF. Sessions were videoed and reviewed for the purpose of supervision.
Assessment
During the initial assessment, Y reported that he was single and not working. Apart from the combat related incidents, he also reported being exposed to a natural disaster. In the 4 years that had passed since the conflict, Y found it increasingly difficult to function. At the time of the assessment, he had not been working for several months. Y reported the main traumatic incident he had experienced was the recovery of several bodies of soldiers who had been killed. He had no recollection of where or when this had exactly taken place. Y had not talked about his experiences with anyone. As can be seen (Table 1), Y reported initial high levels of PTSD, dissociation and depression. He reported no other psychiatric diagnoses and no previous history of psychiatric problems or treatment.

TABLE 1. PTSD, depression and dissociation measures.
Treatment
Following the assessment, Y began weekly treatment, receiving 11 sessions of Virtual Reality Enhanced Treatment. The VR protocol follows the Prolonged Exposure (PE) protocol closely. The therapy includes weekly sessions of 90 min, and the patient is given exercises to complete between sessions. The first session includes psychoeducation about PTSD and breathing retraining. In session two, in vivo exposure is introduced, and a hierarchy of avoided situations is built. The patient begins this exposure as homework assignments, and each subsequent session this is discussed and further exposure assignments are agreed upon. From session three, imaginal exposure is begun. This consists of 45–60 min of the patient reliving the traumatic memory, telling the narrative in first person and present tense, over and over again. The patient is asked every 5 minutes to rate his Subjective Units of Distress (SUDS, from 0 to 100). Sessions are recorded, and the patient is requested to listen to the whole session once between sessions, and the imaginal exposure daily. The VR protocol differs from the PE protocol in one respect: the patient carries out the imaginal exposure whilst using the VR headset. Thus, Y received 11 weekly session, and began the narrative exposure with VR from session three, as per the PE protocol.
Treatment course
Y’s initial session concentrated on psychoeducation and breathing retraining. In the second session Y and the therapist focused on building in vivo exposure hierarchy. These exposures included listening to radio and television news, talking to friends from his army days and talking to his friends about his experiences.
In this session, Y was also introduced to the VR equipment, including a neutral scenario in VR. This is done to ensure that the patient has no negative side effects precluding the use of the VR, such as cybersickness. It also gives the patients an opportunity to become accustomed to the VR room, which looks different to a normal clinic room, before the session where imaginal exposure takes place.
In session three, Y was introduced to the rationale for imaginal exposure, and began the exposure while using the VR headset. The VR has five conflict-based scenarios, these are not hierarchical (i.e., one is not considered more anxiety provoking than another) but reflect different scenes the veteran may have encountered. The therapist and patient decide each session on which scenario to use, and can change between scenarios if this will help the patient feel more connected. In this session, within minutes of beginning to re-tell the traumatic incident, he began crying heavily. There were few details given, and at several points he said he could not continue. His SUDS remained high during these sessions.
During session four, Y reported during the processing that the imaginal exposure that it “was less hard this time” and he noticed a difference in how he saw the event. He was less shocked by the story and mentioned that the more he got used to the story, the more he was able to remember that he is no longer in the traumatic event.
By session five, Y was concentrating on hotspots during the imaginal exposure (specific points in the narrative that are associated with high distress), and his overall levels of distress were lower. Y noted in this session that he required fewer breaks when telling the story.
In session six, the importance of olfaction became more apparent. Y did not cry when discussing going through the pockets of the soldiers who died but reported how hard it was to manage the smells related to the incident. He reported experiencing olfactory flashbacks and was very distressed by these.
During sessions six to eight, Y concentrated on retelling the hotspots (the hardest parts of the narratives); when he reached the part of the narrative where he had reported difficulty regarding smell, the therapist added the smell of gun oil. The scent mixer is loaded with the scent (which is actual gun oil) before the start of the session, and the therapist presses a command on the desktop to release the smell. The smell was released each time the patient reached the part of the narrative when the odor was salient. In each subsequent session (after session 6), the smell was added during imaginal exposure.
By session 8, Y reported significantly lower SUDS, no higher than 30. In the last session, Y related the whole narrative, not just hotspots, and reported SUDS of 0.
Treatment outcome
As can be seen in Table 1, Y’s symptoms reduced drastically during the treatment, and the clinical assessment at the end of treatment showed that he no longer met criteria for PTSD.
Patient’s perspective
A qualitative interview was carried out following completion of therapy. The patient was interviewed by a research team member who had no knowledge of the treatment and its outcome.
Y explained that the VR component of the treatment was salient in its success. There were several components of the VR that he felt specifically contributed to the effectiveness of the treatment. Firstly, Y had never spoken of his experiences with anyone, and was reluctant to even tell his therapist. He felt that the VR enabled this, since he could not actually see the therapist during the imaginal exposure although he knew she was present. In this way, his story “went out” (in his words) without him needing to make eye contact. He would not, he felt, have been able to tell the narrative to a therapist without the VR, and likened it to the invisibility cloak in Harry Potter. Y knew he was not alone, and that the therapist was there, however the VR gave him privacy and control. He described sometimes closing his eyes when he needed to, adding to his feeling of control.
Secondly, Y felt the visual scenes of combat were very helpful. Y had no clear memory of some of the events he had experienced, and the VR allowed him to remember with more clarity. He was reassured that the scenes were clearly related to his combat experiences but were not so realistic that they would be hard to differentiate from reality.
Thirdly, Y described the addition of the odors as extremely important. During the therapy, Y began experiencing olfactory flashbacks. He felt, that the addition of an odor that was part of these flashbacks, that he smelt at the point of the narrative when he had encountered the odor during the traumatic event, was very important to his ability to process the event. This combination of the visual component with the olfactory within the VR was challenging for him, however he described that it allowed him to retrieve the traumatic memory, and learn to cope with it. Y had not talked about the events for the 4 years between their occurrence and the therapy partly because he had very unclear memories of the events. The VR enhanced therapy allowed him to remember in much better detail what he had experienced. He was sure that the visual and olfactory cues were essential in this process.
Discussion
Evidence based interventions for PTSD demonstrate effectiveness for the majority of patients (Forbes et al., 2020). However, many patients avoid therapy, dropout or remain symptomatic (van Minnen et al., 2002; Hoge et al., 2004) and therefore methods that can enhance treatment effects are important. This paper describes the use of Virtual Reality in Exposure Therapy treatment of a patient with combat related PTSD where treatment was enhanced using olfaction during imaginal exposure. As with most VR enhanced therapies, the content of the VR scenarios was similar to the narrative of the patients but does not correspond exactly. Although it has been suggested that individualized VR scenarios are important (see (Van Veelen et al., 2021), both very realistic although generic scenarios (Skip et al., 2010) as well as abstract scenarios (Botella et al., 2015) have been found to be effective and at the theory underlying exposure based treatment for PTSD places importance on the ability of the patient to emotionally process the traumatic memory (Foa and Kozak, 1986) and employs techniques to enhance this, for instance asking the patient to retell the narrative using first person, present tense. Since this process can be challenging for patients, methods to enhance prolonged exposure have been examined (e.g., (Flanagan et al., 2018). Using Virtual Reality, and adding sensory elements such as odor, are additional ways to increase emotional connections. It remains unclear to what degree VR in general, and odor in particular, contribute to this process. One study has shown that VR helped patients who had not responded to previous trauma-focused treatments, possibly indicating that the VR plays an important role in enhancing emotional processing (Difede et al., 2007). Moving from case studies to systematic randomized controlled trials that tease out different therapeutic techniques is necessary to answer this question, and future studies that address this are needed.
This case study does, however, show the way in which odor can be incorporated into VR enhanced PE. The addition of olfaction may add to the efficiency and depth to which a survivor is able to recall memories and engage in the imaginal exposure of the therapy in deeper ways. Further, the addition of olfaction can allow for a more holistic and full-body experience when trying to reimagine and recreate in one’s mind the events of the past: this need to be further explored.
val.
Limitations
Several limitations are noted in the context of this study. Firstly, as a case study, only one case is explored here. A larger sample size may increase generalizability of the case findings. Further, while qualitative data can offer an important perspective on the connection between olfaction deepening the imaginal exposure process, additional data is needed on the significant impact that olfaction can have on the process, comparing subjects where odor was used during treatment as compared to subjects who did not receive the addition of odor. These findings could strengthen the impact that odor has on the treatment.
Conclusion
This case study describes VR enhanced treatment for PTSD, with the addition of odor. While it is not possible to delineate the contribution of each element of the treatment to its success, the patient was confident that the VR and the odor were essential for treatment to be effective. Further studies should examine the addition of odor in treatment in a systematic manner.
Data availability statement
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Helsinki Committee, Jerusalem Mental Health Center and Helsinki Committee, Medical Unit, IDF. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article. Written informed consent was obtained from the participant/patient(s) for the publication of this case report.
Author contributions
SF: Conceptualization, Methodology, Writing–original draft. ED: Software, Writing–original draft. MS: Investigation, Writing–original draft. EB: Writing–original draft, Writing–review and editing. YA: Project administration, Writing–original draft. TR: Investigation, Writing–original draft. RE: Supervision, Writing–review and editing. LT-L: Resources, Supervision, Writing–original draft.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was funded by a grant from the IDF Medical Corps.
Conflict of interest
Author ED was employed by Sonarion Ltd.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Abramowitz, E. G., and Lichtenberg, P. (2010). A new hypnotic technique for treating combat-related posttraumatic stress disorder: a prospective open study. Int. J. Clin. Exp. Hypn. 58 (3), 316–328. doi:10.1080/00207141003760926
Beck, A. T., Steer, R. A., and Brown, G. K. (1996). BDI-II manual. San Antonio, TX: The Psychological Corporation.
Bedwell, J. S., Bohil, C. J., Neider, M. B., Gramlich, M. A., Neer, S. M., O’Donnell, J. P., et al. (2018). Neurophysiological response to olfactory stimuli in combat veterans with posttraumatic stress disorder. J. Nerv. Ment. Dis. 206 (6), 423–428. doi:10.1097/nmd.0000000000000818
Bisson, J. I., Berliner, L., Cloitre, M., Forbes, D., Jensen, D. K., Lewis, C., et al. (2019). The International society for traumatic stress studies new guidelines for the prevention and treatment of posttraumatic stress disorder: methodology and development process. J. Trauma. Stress 32 (4), 475–483. doi:10.1002/jts.22421
Blevins, C. A., Weathers, F. W., Davis, M. T., Witte, T. K., and Domino, J. L. (2015). The posttraumatic stress disorder checklist for DSM-5 (PCL-5): development and initial psychometric evaluation. J. Trauma. Stress 28, 489–498. doi:10.1002/jts.22059
Bombail, V. (2019). Perception and emotions: on the relationships between stress and olfaction. Appl. Animal Behav. Sci. 212 (February 2018), 98–108. doi:10.1016/j.applanim.2018.12.013
Botella, C., Serrano, B., Baños, R. M. G. P. A., and García-Palacios, A. (2015). Virtual reality exposure-based therapy for the treatment of post-traumatic stress disorder: a review of its efficacy, the adequacy of the treatment protocol, and its acceptability. Neuropsychiatr. Dis. Treat. 11, 2533–2545. doi:10.2147/ndt.s89542
Cortese, B. M., Leslie, K., and Uhde, T. W. (2015). Differential odor sensitivity in PTSD: implications for treatment and future research. J. Affect. Disord. 179 (2015), 23–30. doi:10.1016/j.jad.2015.03.026
Croy, I., Schellong, J., Joraschky, P., and Hummel, T. (2010). PTSD, but not childhood maltreatment, modifies responses to unpleasant odors. Int. J. Psychophysiol. 75 (3), 326–331. doi:10.1016/j.ijpsycho.2010.01.003
Cukor, J., Spitalnick, J., Difede, J. A., Rizzo, A., and Rothbaum, B. O. (2009). Emerging treatments for PTSD. Clin. Psychol. Rev. 29 (8), 715–726. doi:10.1016/j.cpr.2009.09.001
de Kleine, R. A., Smits, J. A. J., Hendriks, G.-J., Becker, E. S., and van Minnen, A. (2015). Extinction learning as a moderator of D-cycloserine efficacy for enhancing exposure therapy in posttraumatic stress disorder. J. Anxiety Disord. 34, 63–67. doi:10.1016/j.janxdis.2015.06.005
Difede, J., Cukor, J., Jayasinghe, N., Patt, I., Jedel, S., Spielman, L., et al. (2007). Virtual reality exposure therapy for the treatment of Posttraumatic stress disorder following September 11, 2001. J. Clin. Psychiatry 68, 1639–1647.
Dileo, J. F., Brewer, W. J., Hopwood, M., Anderson, V., and Creamer, M. (2008). Olfactory identification dysfunction, aggression and impulsivity in war veterans with post-traumatic stress disorder. Psychol. Med. 38 (4), 523–531. doi:10.1017/s0033291707001456
Duek, O., Raphael, T., Robert, S., Fried, E. I., and Harpaz-Rotem, I. (2020). Network analysis of PTSD and depressive symptoms in 158, 139 treatment - seeking veterans with PTSD. Depress. Anxiety 38 (October), 1–9. doi:10.1002/da.23112
Flanagan, J. C., Sippel, L. M., Wahlquist, A., Moran-Santa Maria, M. M., and Back, S. E. (2018). Augmenting Prolonged Exposure therapy for PTSD with intranasal oxytocin: a randomized, placebo-controlled pilot trial. J. Psychiatric Res. 98, 64–69. doi:10.1016/j.jpsychires.2017.12.014
Foa, E. B., and Kozak, M. J. (1986). Emotional processing of fear: exposure to corrective information. Psychol. Bull. 99 (1), 20–35. doi:10.1037//0033-2909.99.1.20
Forbes, D., Bisson, J. I., Monson, C. M., and Berliner, L. (2020), Effective treatments for PTSD: practice guidelines from the international society for traumatic stress studies. New York, NY, USA: Guilford.
Hinton, D., Pich, V., Chhean, D., and Pollack, M. (2004). Olfactory-triggered panic attacks among Khmer refugees: a contextual approach. Transcult. Psychiatry 41, 155–199. doi:10.1177/1363461504043564
Hoge, C. W., Castro, C. A., Messer, S. C., McGurk, D., Cotting, D. I., and Koffman, R. L. (2004). Combat duty in Iraq and Afghanistan, mental health problems, and barriers to care. N. Engl. J. Med. 351, 13–22. doi:10.1056/nejmoa040603
Kessler, R. C. (2000). Posttraumatic stress disorder: the burden to the individual and to society. J. Clin. Psychiatry 61 (Suppl. 5), 4–14.
Kessler, R. C., Aguilar-Gaxiola, S., Alonso, J., Benjet, C., Bromet, E. J., Cardoso, G., et al. (2017). Trauma and PTSD in the WHO World mental health surveys. Eur. J. Psychotraumatology 8 (Suppl. 5), 1353383. doi:10.1080/20008198.2017.1353383
Kontaris, I., East, B. S., and Wilson, D. A. (2020). Behavioral and neurobiological convergence of odor, mood and emotion: a review. Front. Behav. Neurosci. 14 (March), 35–15. doi:10.3389/fnbeh.2020.00035
Lo, W., and Hurley, R. A. (2022). Extended reality Technologies: expanding therapeutic approaches for PTSD. J. Neuropsychiatry Clin. Neurosci. 34, A4–A5. doi:10.1176/appi.neuropsych.21100244
Michael, T., Ehlers, A., Halligan, S. L., and Clark, D. M. (2005). Unwanted memories of assault: what intrusion characteristics are associated with PTSD? Behav. Res. Ther. 43 (5), 613–628. doi:10.1016/j.brat.2004.04.006
Rizzo, A., Newman, B., Parsons, T., Reger, G., Holloway, K., Gahm, G., et al. (2009). “Development and clinical results from the virtual Iraq exposure therapy application for PTSD,” in 2009 Virtual Rehabilitation International Conference, Haifa, Israel (IEEE), 8–15.cited 2023 Dec 14 Available from: http://ieeexplore.ieee.org/document/5174198/
Rothbaum, B. O. B. B. O., Hodges, L. F. L. F., Ready, D., Graap, K., Alarcon, R. D., Bo, R., et al. (2001). Virtual reality exposure therapy for Vietnam veterans with posttraumatic stress disorder. J. Clin. Psychiatry 62, 617–622. doi:10.4088/jcp.v62n0808
Schaal, S., Koebach, A., Hinkel, H., and Elbert, T. (2015). Posttraumatic stress disorder according to DSM-5 and DSM-IV diagnostic criteria: a comparison in a sample of congolese ex-combatants. Eur. J. Psychotraumatology 6, 24981–24988. doi:10.3402/ejpt.v6.24981
Sheehan, D. V., Lecrubier, Y., Sheehan, K. H., Amorim, P., Janavs, J., Weiller, E., et al. (1998). The Mini-International Neuropsychiatric Interview (M.I.N.I): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J. Clin. Psychiatry 59, 22–57.1998
Skip, R. A., Difede, J., Rothbaum, B. O., Reger, G., Spitalnick, J., Cukor, J., et al. (2010). Development and early evaluation of the Virtual Iraq/Afghanistan exposure therapy system for combat-related PTSD. Ann. N. Y. Acad. Sci. 1208 (1), 114–125. doi:10.1111/j.1749-6632.2010.05755.xOct
Skip, R. A., and Shilling, R. (2017). Clinical Virtual Reality tools to advance the prevention, assessment, and treatment of PTSD. Eur. J. Psychotraumatology 8 (Suppl. 5), 1414560. doi:10.1080/20008198.2017.1414560Oct 27
Tjalvin, G., Magerøy, N., Bråtveit, M., Lygre, S. H. L., Hollund, B. E., and Moen, B. (2017). Odour as a determinant of persistent symptoms after a chemical explosion, a longitudinal study. Ind. Health 55 (2), 127–137. doi:10.2486/indhealth.2016-0155
Toffolo, M. B. J., Smeets, M. A. M., and van den Hout, M. A. (2012). Proust revisited: odours as triggers of aversive memories. Cognition Emot. 26 (1), 83–92. doi:10.1080/02699931.2011.555475
Van der Kolk, B., and Fisler, R. (1995). Dissociation and the fragmentary nature of traumatic memories: overview and exploratory study. J. Trauma. stress 8 (4), 505–525. doi:10.1007/bf02102887
van Minnen, A., Arntz, A., and Keijsers, G. P. J. (2002). Prolonged exposure in patients with chronic PTSD: predictors of treatment outcome and dropout. Behav. Res. Ther. 40 (4), 439–457. doi:10.1016/s0005-7967(01)00024-9Apr
Van Veelen, N., Boonekamp, R. C., Schoonderwoerd, T. A. J., Van Emmerik, M. L., Nijdam, M. J., Bruinsma, B., et al. (2021). Tailored immersion: implementing personalized components into virtual reality for veterans with post-traumatic stress disorder. Front. Virtual Real 2, 740795. doi:10.3389/frvir.2021.740795Sep 30
Vermetten, E., and Bremner, J. D. (2003). Olfaction as a traumatic reminder in posttraumatic stress disorder: case reports and review. J. Clin. Psychiatry 64 (2), 202–207. doi:10.4088/jcp.v64n0214
Weathers, F. W., Blake, D. D., Schnurr, P. P., Kaloupek, D. G., Marx, B. P., and Keane, T. M. (2013). The clinician-administered PTSD scale for DSM-5 (CAPS-5). Available from: [Assessment] Available from
Keywords: PTSD, virtual reality, olfaction, exposure therapy, case report PTSD, case study
Citation: Freedman SA, Dayan E, Senitsky M, Bellin E, Attias Y, Richman T, Eitan R and Tatsa-Laur L (2024) Case report: the addition of olfaction to virtual reality enhanced exposure therapy for PTSD. Front. Virtual Real. 5:1284299. doi: 10.3389/frvir.2024.1284299
Received: 28 August 2023; Accepted: 26 February 2024;
Published: 13 March 2024.
Edited by:
Orestis Georgiou, Ultraleap Ltd., United KingdomReviewed by:
Justin Maximilian Mittelstädt, German Aerospace Center (DLR), GermanyTiago Henrique Falk, Université du Québec, Canada
Copyright © 2024 Freedman, Dayan, Senitsky, Bellin, Attias, Richman, Eitan and Tatsa-Laur. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sara A. Freedman, c2FyYS5mcmVlZG1hbkBiaXUuYWMuaWw=