 Christopher Tacca
Christopher Tacca Barbara A. Kerr
Barbara A. Kerr Christopher McLamb2
Christopher McLamb2- 1Bioengineering Graduate Program, University of Kansas, Lawrence, KS, United States
- 2Counseling Psychology, Department of Educational Psychology, University of Kansas, Lawrence, KS, United States
- 3Department of Mechanical Engineering, University of Kansas, Lawrence, KS, United States
More than 40% of the U.S. population have experienced mental health disorders since the COVID-19 pandemic. 40% of this group received no treatment for their mental illness. Barriers to treatment include stigma, prohibitive cost, and a belief that treatment is inaccessible, particularly in isolated or rural communities. A novel remote, EEG-enhanced VR psychotherapy system was assessed for its presence and restorativeness, and therapeutic efficacy in improving mood with a single session positive solution-focused session. Thirty adults experiencing depressive symptoms were randomly assigned to either a single session Positive Solutions Focused counseling treatment via Zoom videoconferencing, or the EEG enabled VR psychotherapy system. Participants rated the environment in the VR-EEG therapy as more restorative than Zoom counseling, t = 2.928, p < .004, Cohen’s d = .259, and comparable to the Zoom session in presence. The VR-EEG system performed comparably to Zoom online counseling in clients’ session ratings of depth and smoothness and client reactions, positivity, and arousal. For a treatment to be considered empirically supported, and therefore valid for use in psychotherapy, it must have equal or greater efficacy than a standard treatment or format. VR-EEG, therefore, has promise as a positive, solution-focused, brief therapy for isolated clients with depressive symptoms.
Introduction
Since the COVID-19 pandemic, mental illnesses have affected more than 40% of the population in the United States (SAMHSA, 2021). Rural, psychologically isolated, and poorer communities receive mental health services at a lower rate than other populations (Hartley, 2004; SAMHSA, 2021). Some major reasons for this disparity include lack of resources in rural communities and increased physical distance for the nearest counseling office, stigma and anxiety towards attending counseling sessions in person, and the inability to afford counseling sessions (Möller-Leimkühler, 2002; Kelly et al., 2007; Cohn and Tsai, 2020; Gulliver et al., 2010);. With the COVID-19 pandemic making in person psychotherapy sessions impossible, counselors turned to telepsychology to reach their clients. Since 2020, 98% of mental healthcare professionals have used some form of telepsychology in their practice. Giovanetti et al. (2022) found in their meta-analysis of online vs face-to-face therapy for depression that online therapy was as efficacious as face-to-face treatment.
Remote technologies are effective alternatives to in person therapy because they provide an accessible option for treatment for those who live far from the nearest counseling center that meets their needs (rural or geographically isolated), those who find the idea of getting out of bed in the morning and meeting their counselors in person impossible (psychologically isolated), and those concerned with the stigma of attending in person counseling sessions (Weightman, 2020). Current technologies for telepsychology include online videoconferencing services and phone or text-based therapy. For many, these technologies have provided a valuable lifeline during the pandemic and a valuable alternative to in person therapy independently of the pandemic (Sampaio et al., 2021). For some, however, the shift to remote counseling has meant therapists and clients have had to adjust to this new form of treatment. In remote counseling where the face and body are not clearly visible, it can become more difficult for counselors to recognize nonverbal cues. In addition, the client’s environment may not be suitable for therapeutic healing, and the face to face nature of videoconferencing therapy can still cause too much anxiety for clients (Simpson and Reid, 2014; Simpson et al., 2021).
For these isolated clients, new technologies could provide a solution. A therapy system that uses virtual reality (VR) technology and electroencephalography (EEG) could provide the potential tools for counselors to address both factors. VR can immerse users into the virtual environment and build presence, or the feeling of truly being there in the space. Fodor et al. (2018) confirmed the potential of VR based psychotherapies in a meta-analysis on the use of VR in the treatment of anxiety and depression. These therapies were more effective than controls for anxiety depression, but not for treatment attrition. They found too few studies of VR therapy for depression for more detailed analyses of its effectiveness compared to other treatments. Dellazizzo et al. (2020) conducted a meta -meta-analysis of VR treatments for psychiatric disorders and found that VR therapies were equal to other evidence based treatments in successful outcomes of therapy, but performed better than control groups. In addition, VR has been most successfully used to treat anxiety and phobias through VR exposure therapy (VRET), with moderate effect sizes. VR therapy has also been used to foster self-compassion and mitigate self-criticism (Falconer et al., 2014; 2016) and treat depression with positive psychotherapy (Hwang et al., 2017) and cognitive behavioral therapy (Banos et al., 2002). This technology has also been used to teach or enhance empathy by simulating realistic interactions (Seinfeld et al., 2022. A bibliometric analysis by Jingli et al. (2023) concluded that the use of VR in treating anxiety and depression is burgeoning, especially since the pandemic. In addition, they found that VR was much more common in the treatment of anxiety than depression. A wide variety of psychotherapies were used across these studies, with cognitive behavior therapy most common for depression. Although rare before 2020, applications that combine VR and EEG monitoring have increased in psychotherapy studies. Weber et al. (2021) attribute this not only to the increased use of technology after the pandemic, but also the ease of use of commercial VR and EEG headsets, and recommended improvements to testing of quality of signals. Kosonogov, V.V., Efimov, Rakhmankulova, and Zyabreva (2023) found ten examples of combinations of VR and EEG technology in therapies for the relief of stress; however, the EEG monitoring was used as a measure of reduction of stress rather than as a part of psychotherapy. One of the few studies showing the efficacy of the use of EEG in psychotherapy showed that EEG monitoring combined with positive psychotherapy assisted the therapist in identifying relaxed and mindfulness states (Hwang et al., 2017).
Common factors
In order to develop an effective psychotherapy for depression in isolated clients while using an EEG-enabled VR system, it is necessary to understand how each component of psychological healing works. Effective healing consists of three components: natural factors, specific factors or common (or contextual) factors (Walmpold and Flückinger, 2023). Specific factors refer to the actual treatment used to help the client with specific disorders, such as cognitive behavioral theory for depression or exposure therapy for phobias. Common factors are those factors which are the context of all healing therapies. Although there are many conceptualizations of common factors, the original common factors proposed by Frank and Frank (1993) are a strong relationship with the healer, called the therapeutic alliance; healing environment; a rationale or explanation of the problem that makes sense to the client; and a “ritual,” a set of specific procedures for healing. Interestingly, most studies of specific factors and common factors find that specific factors account for less of the variance in outcome than common factors (Wampold and Imel, 2008). Of all the common factors, the relationship, or therapeutic alliance, is repeatedly found to explain the largest proportion of the variance in outcome. Therapeutic alliance is defined as “a positive emotional bond between therapist and client, and their mutual agreement on the goals and tasks of the treatment” (Bordin, 1994, p.362). Alliance is important in predicting the outcome of traditional face-to-face psychotherapy (Norcross, 2011). The therapeutic alliance is dependent upon the therapist being able to read and respond to client emotions accurately. Understanding client emotions is essential for counselors to build an empathetic alliance with their clients, recognize moments when clients are anxious when responding to something the counselor said, and build a working relationship with their clients (Castonguay et al., 1996). Monitoring electroencephalographic data (EEG) assists the counselor in recognizing client’s emotions in real time (Li and Lu, 2009; Bashivan et al., 2016; Peining et al., 2017). EEG may also make it possible to solve one of the major problems of VR therapy, the ability to observe client emotions. Adding EEG monitoring to VR therapy essentially makes emotions visible, by allowing the counselor to view the client’s level of arousal and the EEG bands associated with relaxation, anxiety or excitement, creative flow, and insight. In this way, EEG-enabled VR therapy has the potential to enhance the therapeutic alliance, the most important common factor.
The second common factor that must be addressed by this therapy system is a special healing setting (Frank and Frank, 1993.) Although neglected and deemed less important as a contextual variable in healing by psychotherapy researchers (Pressley and Heesacker, 2001), scholars in healthcare, design, and environmental science took up the study of the physical environment’s impact on health and wellbeing with enthusiasm. Gesler (2003) proposed that healing places had natural, built, social, and symbolic aspects that could all be managed to improve health. Ecotherapists found that natural environments could be restorative, reducing stress and increasing positive feelings (Joye and van den Berg, 2018). Li et al. (2021) successfully incorporated restorative, natural elements into VR environments, and used EEG monitoring to show how virtual, natural environments assisted emotional positivity and cognitive recovery from anxiety and depression. Therefore, VR technologies for remote psychotherapy may be designed to address environmental factors to bring an effective and accessible therapy solution to isolated populations (Tacca et al., 2022).
The other two common factors underlying effective therapy are a rationale, that is a theory of change that is explained to the client, and a “ritual,” that is, a series of techniques that engage the client in thinking and acting on the problem.
Specific factor: positive solution focused brief therapy
The particular therapy used, or the specific factor, should be an evidence-based therapy that has a strong rationale and a set of meaningful activities that contribute to the client’s goals. Positive solution-focused theory and procedures have been successfully used in the brief, online therapy with college students (Novella et al., 2022). The theories underlying the counseling approach chosen for this treatment were Positive Psychology and Single Session Solution Focused Therapy, an integration described by Bannick and Jackson (2011). Solution-focused therapy is a brief, evidence-based treatment that is used widely across social work and counseling. As a social constructivist therapy, solution-focused therapy assumes that the client is continually creating the self, and that in co-constructing a solution to the client’s problem, the therapist helps the client to gain greater self-compassion and self-efficacy (DeShazer et al., 2021 A key aspect of positive psychology interventions is focusing on strengths in order to build self-compassion and motivation for change, which according to Shapira and Mongrain (2011) are critical to treatments for depression. Gingerich and Peterson, (2013) claim that the addition of positive psychology to solution-focused therapy is a powerful combination for the treatment of depression by increasing the positivity of the client. Positive, solution-focused counseling encourages the client to find strengths in the efforts they are already making to get well. For example, counselors in positive solution-focused counseling often ask “What made it possible for you to get up this morning?” to emphasize that getting out of bed on time for counseling when depressed is indeed a strength and a reason for self-compassion. Another important component of a positive solution focused therapy is the inclusion of the Miracle Question, which states that, “if you woke up in the morning and the problem that you were struggling with was suddenly completely resolved by some miracle, describe what you would be like and what you would do.” (Corcoran and Pillai, 2009; Macdonald, 2011; Palmer, 2015). Gingerich and Peterson (2013) conducted a systematic, qualitative review of controlled experimental studies of solution-focused brief therapy (SFBT) and concluded that across studies, this therapy was effective, with Positive SFBT leading to greater emotional improvement and cognitive recovery in individuals with mild-to-moderate anxiety and depression.
It seems, therefore, that a positive, solution-focused brief treatment delivered through an EEG-enabled Virtual Reality system might fulfill all four of Frank and Frank’s (1993) common factors for therapeutic effectiveness: a virtual healing environment; an empathic counseling alliance; a rationale; and a set of procedures that allow the client to engage, in one session, in meaningful construction of a positive self and effective problem-solving. Together, these techniques might be effective in reducing depressed mood and increasing positivity. A laboratory test of VR and Zoom based SFBT seems appropriate not only because SFBT was found to be effective in treating depression, but also because single session analog studies preceding field clinical trials are considered the “bedrock” of therapeutic outcome studies (Scheel et al., 2011).
Research questions
In this study, a VR-EEG positive SFBT session will be compared to a standard Zoom videoconferencing positive SFBT session in order to compare the systems’ ability to foster a sense of presence and restorativeness in clients, its ability to facilitate an counseling alliance of depth and comfort, and its ability to enhance mood and increase positivity.
The research questions for this study are as follows:
1. Is the VR-EEG therapy system as useful and functional in fostering restorativeness and a sense of presence as Zoom online counseling?
2. Is the VR-EEG therapy system as efficacious as Zoom online counseling in creating clients’ positive assessment of the therapeutic alliance, in improving client mood-related symptoms of depression, increasing positivity, and producing positive client reactions to the counseling?
Methods
Participants and criteria for inclusion
The study included 30 participants recruited through social media from the local community in Lawrence, Kansas and the surrounding areas (Figure 1). The criteria for inclusion were as follows: 1. Participants were 18 years or older, 2. Currently experiencing depressive symptoms, and 3. Actively seeking counseling. Participants were also asked to travel in person to a counseling laboratory where they could anonymously and remotely complete a session with a counselor. Table 1 shows the demographics for sample, which was representative of the regional demographics in gender, ethnicity, and income.
Figure 1. An example of the posted flyer on Instagram with examples of VR environments.
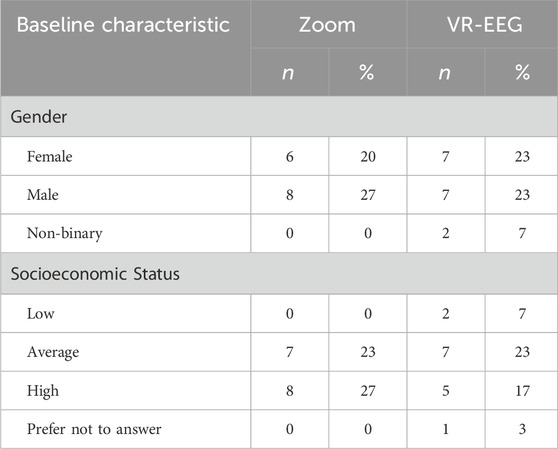
Table 1. Demographics.
Recruitment
Participants were recruited for the study in accordance with the guidelines by the Institutional Review Board. An example of recruitment flyer is in Figure 1 The recruitment process for this study included advertising the study in the local student newspaper (offering a free VR counseling session or demonstration and a referral for further counseling), putting flyers up in academic buildings, and posting advertisements on social media including posts on Reddit in local subreddits and on the local newspaper’s Instagram. The majority of participants heard of this study through posts on Reddit. Demographics are presented in Table 1.
Procedure
Participants were randomly assigned to VR-EEG or Zoom teleconferencing groups. Participants did not meet with their counselor before the counseling session, nor see them in person during the session. In the remote EEG-enabled VR psychotherapy system, the counseling session occurred in a virtual natural forest environment with a counselor represented by a therapist avatar (see Figure 1). The avatars were designed by an author of the study to be appropriate healer figures. The therapist avatar was either resembled male sage or a woman healer, and was voiced by the appropriate gender. The Zoom group was given a remote counseling session using Zoom videoconferencing with a male or female counselor. Participants were taken to their counseling room and joined a video Zoom call with a counselor in a separate room. Counseling sessions for both groups followed the same positive, solution-focused counseling script. Both groups received pre and post tests before and after their session. Online groups were also given an opportunity to try out the VR system after their post-tests.
A brief description of an example study protocol:
1. The client was greeted by a secretary at the counseling laboratory and given a brief introduction to the activities for the session.
2. The client was then asked to read and sign a consent form explaining the procedure as a participant and the potential risks involved.
3. The client was then asked to complete a brief surveys on demographic information and two pre-test scales of mood and arousal.
4. The client was then taken to their counseling room by a secretary and instructed on how to conduct their counseling sessions.
5. Once set up with their telepsychology system, the client was connected with their counselor online.
6. The client then experienced a 45–60 min positive, solution focused counseling session.
7. Immediately following the counseling session, the client was administered four post-test measures.
8. Once finished with the post assessment and demonstration, the client debriefed by the experimenter, and was offered a referral to the positive psychology clinic if needing further help as well as given contact information of their counselor.
Counseling script
The counseling script used for this study was developed by counseling psychology Ph.D. students, two of whom were authors for this study. The goal for the script was to create a guideline for counselors to conduct the sessions using the technology at their disposal and to give clients practical help and actionable changes after a single counseling session. Counselors using the VR psychotherapy system were instructed to use the neurofeedback to reflect emotions as called for in the script. For example, if they noticed a moment where clients had a spike in their EEG, they could ask their client about what they noticed. Counselors could use the feedback either passively or bring up the EEG data directly with clients at various times throughout the session, for example, saying, “Your EEG seems to show that you have relaxed quite a bit. What is helping you to be more comfortable?” Online counselors used the nonverbal expressions they were able to see in order to reflect emotions, e.g., saying “I notice from your expression that you seem to be anxious now.” An effective Solutions Focused Counseling session leaves clients with positive mood and increased desire for action and agency and with techniques to address their concerns, as well as specific action plans to take for immediate change.
Instruments
Two assessments were taken by participants before the session and four were taken immediately following their respective counseling sessions.
Pre-session demographic survey
The demographic survey asked participants for their age, self-identified gender, and self-identified socioeconomic privilege. The demographic survey also asked the participant where they heard about the study.
Perceived restorativeness scale
The Perceived Restorativeness Scale (PRS) is used to assess the environment of the counseling session (Hartig et al., 1997). Across four studies, the internal consistency for each subscale measured was determined to be sufficient with Cronbach’s α > .60 (Hartig et al., 1996). The construct validity measures for each subscale were determined to be sufficient when the measure was compared with the Küller Semantic Scale and Zuckerman Inventory of Personal Reactions with positive correlations to positive constructs on each and negative correlations to negative constructions on each (Hartig et al., 1996). When using the instrument, clients rate how suitable an environment is for therapeutic healing including their comfort level in the environment, excitement, and ability to focus on the counselor. Clients were asked to consider both the physical and virtual environment when completing the survey.
Presence questionnaire
The Presence Questionnaire (PQ) is used to analyze the immersiveness of a VR experience. The VR technology is assessed based on presence or immersion, interactivity, and users opinion of the overall quality of the VR (Witmer et al., 2005). The instrument uses 32 questions with each pertaining to one of four factors. Internal consistency was measured across three studies with the Cronbach’s α = .91, and the reliability coefficients were also determined to be α = .57 for the interface quality factor, α = .89 for the involvement factor, α = .84 for the sensory fidelity factor, α = .80 for the sensory fidelity factor (Witmer et al., 2005).
Pre-session and post-session session evaluation questionnaire
The Session Evaluation Questionnaire (SEQ) is a common measure to assess the quality of a counseling session and client mood (Stiles et al., 1994). The SEQ is a semantic differential instrument consisting of four subscales: Depth, Smoothness, Positivity, and Arousal. The internal consistency reliability alpha for each of these subscales was determined as to be .90 for depth, .93 for smoothness, .90 for positivity, and .81 for arousal (Reynolds et al., 1996). The Depth and Smoothness subscales evaluate the therapeutic alliance, and the Positivity and Arousal subscales evaluate the client positive feelings and mood. The Depth and Smoothness subscales were administered to the client following the counseling session. The Positivity and Arousal subscales were administered to the client both before and after the counseling session to assess the change in mood and positivity across one session (Tryon, 1990; Stiles et al., 1994). These subscales are useful in measuring changes in depression symptoms of low energy and low positivity. Positivity included items such as “Happy-----Sad” and “Friendly-----Unfriendly.” The Arousal scale included items such as “Aroused-----Quiet,” “Excited -----Calm, “and “Fast-----Slow.”
Client reactions system
The Client Reactions System (CRS) is used to give a basic understanding of the client’s perception of the quality of the counseling session (Hill, 1992). Face and content validity were established by comparing scores to previous literature with positive correlations found between reported helpfulness ratings and reactions of counselors (Hill, 1992). No reliability data has been given for the instrument as Hill (1992) argued that memory would prevent accurate retesting (Hill et al., 2001). They are asked to assess the quality of the session and give information about their current feelings (Hill et al., 2001). In this study, the CRS is used as a check for positive or negative reactions that might affect the validity or generalizability of the study.
Statistics and analysis
To test the functionality of the VR-EEG compared to Zoom online technology, scores on the Perceived Restorativeness Scale and the Presence Questionnaire were analyzed with a two-sample t-tests to compare the means of the two groups after counseling.
Scores on the SEQ mood subscales (Positivity and Arousal) were analyzed with a 2 × 2 repeated measures Analysis of Variance (ANOVA) test with type of treatment (VR-EEG treatment vs Zoom counseling) and time (pre- and post-) as the independent variables. The SEQ: Session Evaluation (Depth and Smoothness) subscales were scored and analyzed with a two-sample t-tests to compare the score of the control and experimental groups after counseling.
Results
Overall, the goal of the VR-EEG therapy study was twofold: 1. To assess how a VR-EEG counseling session compared to an Online Zoom therapy session in the sense of presence and restorativeness 2. To assess VR-EEG therapy compared to Zoom therapy in the client’s arousal, positivity, therapeutic alliance, and perception of overall counseling effectiveness.
Presence questionnaire results
The PQ was scored on a scale from 1 to 5 with a neutral score of 3. No significant difference between the control group and the experimental group was found. Clients rated the immersiveness of the VR technology neutrally (Table 2). It was comparable to the Zoom group in presence.
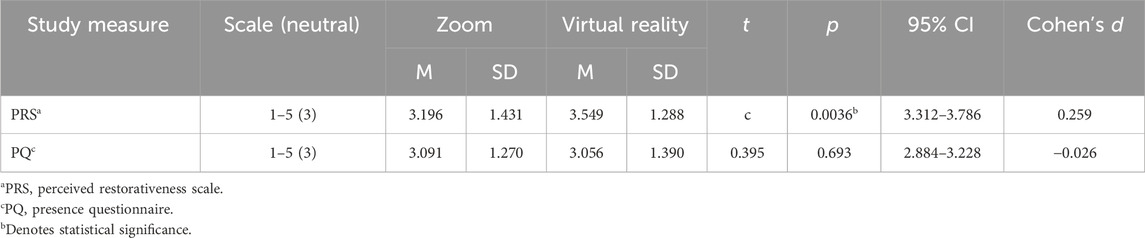
Table 2. Summary of the results for perceived restorativeness and presence.
Perceived restorativeness scale results
The PRS was scored on a scale from 1 to 5 with a neutral score of 3. The mean score of the Zoom Therapy was 3.196 and the mean score for the VR Therapy was 3.549. Both groups rated the restorativeness of the environment as above the neutral score (Table 2), with the VR-EEG group scoring significantly higher than the Zoom group, t = 2.928, p < .004, Cohen’s d = .259.
SEQ: depth and smoothness
The Depth score was scored on a scale from 1 to 7 with a neutral score of 4. Depth was calculated based on averaging the scores of the five questions in the SEQ related to depth. Both groups scored the depth of the session as positively compared to the neutral score. No significant difference was found between scores for Zoom therapy and VR-EEG (Table 3).
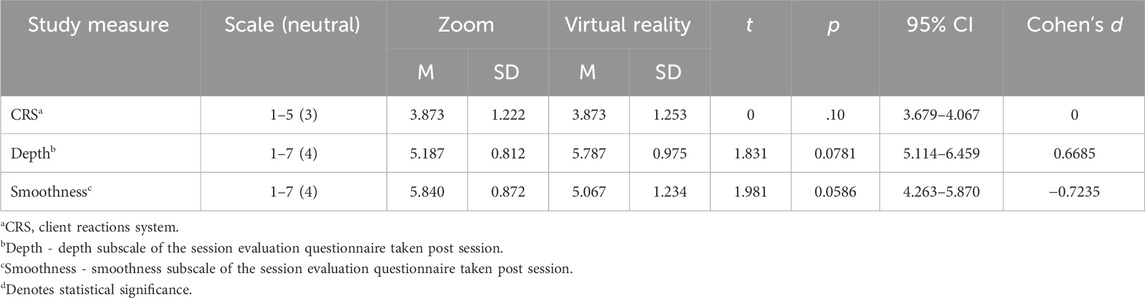
Table 3. Summary of the results for counselor rating, counseling depth, and counseling smoothness.
The Smoothness score was scored on a scale from 1 to 7 with a neutral score of 4. Smoothness was calculated based on averaging the scores of the five questions in the SEQ related to smoothness. No significant difference was found in scores for Zoom and VR-EEG (Table 3).
Session evaluation questionnaire: positivity results
The Positivity was scored both pre- and post-session from 1 to 7 with a neutral score of 4. Positivity score was calculated by averaging the scores of the five questions related to positivity. The mean positivity score of the control group increased by 1.20 between pre- and post-session and the mean positivity score of the experimental group increased by 1.00 between pre- and post-session. No significant difference was found between the effects of the Zoom and the VR-EEG therapies. However, the overall main effects between pre- and post-session showed a significant positive difference across all groups, F (1, 28) = 29.824, p < .001, partial η2 = .51 (Table 3).
SEQ: arousal results
The Arousal scale was scored both pre- and post-session from 1 to 7 with a neutral score of 4. Arousal score was calculated by averaging the scores of the five questions related to arousal. No significant main or interaction effects were found (Table 4). Both groups had low to moderate arousal before and after the session.
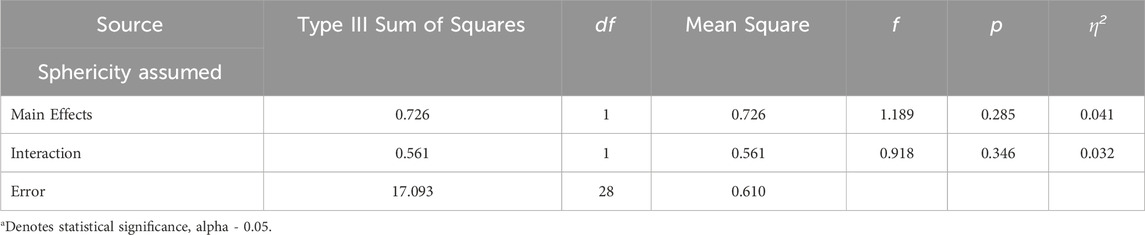
Table 4. Session Evaluation Questionnaire: Arousal results from the 2 × 2 Repeated Measures ANOVA.
Counseling reaction system
The CRS was scored on a scale from 1 to 5 with a neutral score of 3. No significant difference between the control group and the experimental group was found. However, clients in both the control and experimental groups rated their immediate reactions towards the counseling session as positive in comparison to the neutral score (Table 3).
Discussion
All thirty clients were respondents to a social media post recruiting volunteers who were experiencing symptoms of depression and who were seeking counseling. Fifteen participants were randomly assigned to a single Positive Solutions Focused Therapy remote counseling session using Zoom Videoconferencing and fifteen participants were assigned to a remote counseling session using the VR-EEG psychotherapy system. Pre- and post-tests of depth and smoothness of therapeutic alliance, and arousal and positivity were given. Post-tests of perceptions of presence and restorativeness of Zoom or VR-EEG environments were also given to clients.
Overall, this study provided support for the idea that the VR-EEG counseling is as efficacious as Zoom online counseling for the brief treatment of depressive symptoms, and superior to Zoom online counseling in restorativeness of the environment. Clients saw the VR environment as more pleasant, calming, and beautiful than the online counseling environment they could see on Zoom, which was a counselor in a standard counseling interview room. This was unexpected, because with the prototype, the criterion for success was for the VR therapy system to perform relatively equal to the Zoom session. However, clients rated their environment more positively in VR. Responding to critiques of the conventional interview room, Kim et al., (2009) explored the use of forest environments with cognitive behavioral therapy clients and found them to be more conducive than offices to therapeutic change. This study shows that even VR forest environments can feel more restorative to clients than standard office environments. Li et al. (2021) found that VR forest environments (without therapy) were effective in mood recovery from depression. Wang et al. (2022) included interactive components with a guide and found positive effects of VR interactive forest environments. They recommended more comprehensive treatments that included therapy, such as the current study.
Scores on the Session Rating Scale indicated that VR-EEG therapies and Zoom therapies both indicated the establishment of a therapeutic alliance. With therapeutic alliance being a strong predictor of successful outcome, this was a promising finding (Norcross, 2011).
The VR-EEG therapies and the Zoom therapies both resulted in increases in positivity in mood. This subscale of the SEQ is a measure frequently used to indicate relief of depression symptoms, because the five items all pertain to mood (Stiles et al., 1994). The Positivity subscale pertains to feelings of happiness, friendliness, confidence, sureness, and pleasure and is considered to be inversely related to depression symptoms. McClintock et al., (2015) suggested that the boost to the client’s mood from the positivity of therapeutic experience could, in turn, counteract depressed affect and could initiate a cascading effect leading to improvements in functioning and quality of life. Like previous studies of positive SFBT, the emphasis on strengths may have had a greater impact on positive feelings than solution-focused counseling alone (Bannick and Jackson, 2011). The treatments were equally neutral on arousal, with clients at about the same level of arousal before and after therapy. Although arousal scores were the same before and after therapy, this can be expected, with a general pattern on VR EEG’s seen to be lower arousal before therapy, variations in high and low arousal during therapy, and return to lower arousal after therapy. The Arousal scale can show excessive excitement and anxiety, often co-morbid with depression. Both groups were low to moderate in arousal both before and after. The comparability of these two forms of treatment is important, given that a psychotherapy is considered empirically supported when it performs as well or better than a standard treatment in a standard format. Solution-focused therapy in an online format is considered a standard, empirically supported treatment for depression (Kim, 2008). The increases observed in positivity suggest that both sessions reduced depression. The equally high ratings of VR-EEG solution-focused counseling and Zoom solution-focused counseling mean that VR-EEG therapy has potential as an empirically supported therapy, recognized by the American Psychological Association and most healthcare providers (Tolin, 2015). Finally, although VR forest environments have been found to be restorative in previous studies (Li et al., 2021; Joye and van den Berg, 2018), we thought it important to provide all four common factors associated with positive outcome so that these clients would have the experience of a therapeutic alliance as a foundation for further therapy, and so that they would have actionable solutions to their presenting problems as a benefit of their volunteering for the study.
Although qualitative analysis was not done for this study, the Client Reactions System allows for general feelings and thoughts to be expressed. No negative reactions were observed, and participants were overall positive about the counseling session. Students were also free to comment and make observations during the de-briefing session. Experimenters noted that clients looked noticeably more positive and talkative following the sessions with many of them wanting to connect further with their counselors. One client directly noted the influence of EEG, because their counselor seemed to continuously pick up things that they were feeling but did not know how to express. This client said that it was a validating experience, and that their counselor understood them. The feedback from counselors was also positive. Many of the counselors were initially nervous about conducting counseling sessions with the VR therapy system. However, after completing their first session, they were excited and confident that they were able to conduct quality sessions.
Limitations
It has long been noted that compared to medical studies in which the control group is offered a placebo or sham treatment, psychotherapy studies cannot ethically or practically create a control group (Klein, 1997). Instead, one treatment can only be compared to one or more other treatments. This study would have benefitted from the addition of one or two more conditions involving another empirically supported treatment in VR-EEG and online formats. In addition, clients needed to come to a lab setting in order to receive “remote” counseling–that is, whether they were seen on Zoom or through VR and were not in the same room with the counselor. This improved standardization but came with limitations. The cost and time needed for mailing headsets for both VR and Zoom to thirty clients was prohibitive, given the funding available. In the field, it would be expected that this expense, about $250.00 usd, would need to be included in the fee for therapy or sent for a lending fee and returned. This is how many leading VR therapy companies manage the process (XR, 2020; Society for Virtual Reality, 2023). It is still possible that results might not be generalizable to actual remote counseling where the client does not leave home. The laboratory setting may have differed in terms of difficulty of getting there, having to meet the person acting as receptionist, and having to go into an interview room for either session. The laboratory setting requires that the treatments be labeled as “efficacious” rather than “effective,” until proven out in the field (Lutz, 2003). The long-term impact of these interventions remains unknown. The next step in this research should be to take the system into the field, to increase numbers of sessions, and to track outcome over an extended period.
In addition, although power analysis indicated that 30 participants were sufficient for our design, more participants would have increased the power to detect significant differences, particularly where resulting probabilities approached significance.
Another limited factor is the possibility of cybersickness. One client had to remove the VR headset and complete the session via audio because of cybersickness, a known problem for some people using VR, so that an audio-assigned client had to take the place of a VR client. Some improvements could be made to the presence in the VR to help mitigate the cybersickness and a guide for using the VR in intervals and resting in between could help counselors navigate this problem.
Finally, as noted earlier, this prototype was a very basic VR environment that could be much improved by professional VR developers, possibly creating more presence and even higher restorativeness.
Conclusion
Untreated mental illness is often the result of geographical remoteness, psychological isolation and poverty. Remote psychotherapy systems have been developed to address the need for an alternative to in person therapy for populations where it is inaccessible, particularly during the COVID-19 pandemic. A novel VR-EEG remote psychotherapy system was developed to address some of the limitations in the current remote psychotherapy options including fostering the therapeutic alliance over distance and bringing a restorative environment into the client’s home. This system was compared to Zoom videoconferencing. The sessions were rated positively overall, with VR-EEG creating greater restorativeness of the environment. In both systems, participants perceived themselves to have experienced a positive working alliance. In both systems, this positive solution-focused brief session increased positivity, and maintained low to neutral arousal. All of this suggests that quality counseling sessions are able to be conducted through the VR psychotherapy system and that it could provide a necessary alternative for those in which the current options are not suitable. Future research could investigate the impact of further immersion aspects into the VR such as in world interactivity and haptic feedback, improvements in EEG and real time alerts, and the implementation of further restorative environments and therapist avatars. While this study increases the possibility that one remote session of a positive solution-focused treatment for depression that focuses on client strengths holds promise, further field-based studies that include more sessions and follow-up would strengthen the case for VR-EEG therapy.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Human Subjects Research Protection University of Kansas #STUDY00148535. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
CT: Conceptualization, Investigation, Software, Visualization, Writing–original draft. BK: Conceptualization, Data curation, Investigation, Methodology, Supervision, Writing–review and editing. CM: Conceptualization, Data curation, Investigation, Writing–review and editing. KR: Conceptualization, Data curation, Investigation, Writing–review and editing. EF: Conceptualization, Supervision, Writing–review and editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. University of Kansas Endowment Self Doctoral Fellowship and University of Kansas Endowment Williamson Family Distinguished Professor Fund.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Bannink, F., and Jackson, P. Z. (2011). Positive psychology and solution focus–looking at similarities and differences. InterAction-The J. Solut. Focus Organ. 3 (1), 8–20.
Banos, R. M., Botella, C., Perpina, C., Alcaniz, M., Lozano, J. A., Osma, J., et al. (2002). Virtual reality treatment of flying phobia. IEEE Trans. Inf. Technol. Biomed. 6 (3), 206–212. doi:10.1109/TITB.2002.802380
Bashivan, P., Rish, I., and Heisig, S. (2016). Mental state recognition via Wearable EEG. arXiv. arXiv:1602.00985). doi:10.48550/arXiv.1602.00985
Bordin, E. S. (1994). “Theory and research on the therapeutic working alliance,” in The working alliance: theory, research, and practice. Editors A. O. Horvath, and L. S. Greenberg, 13–37. doi:10.1192/s0007125000065351
Botella, C., Fernández-Álvarez, J., Guillén, V., García-Palacios, A., and Baños, R. (2017). Recent progress in virtual reality exposure therapy for phobias: a systematic review. Curr. Psychiatry Rep. 19 (7), 42. doi:10.1007/s11920-017-0788-4
Castonguay, L. G., Goldfried, M. R., Wiser, S., Raue, P. J., and Hayes, A. M. (1996). Predicting the effect of cognitive therapy for depression: a study of unique and common factors. J. Consult. Clin. Psychol. 64 (3), 497–504. doi:10.1037//0022-006x.64.3.497
Cohn, T. J., and Tsai, P.-C. (2020). “Providing psychotherapy in rural areas,” in Bringing psychotherapy to the underserved: challenges and strategies (Oxford University Press), 208–228. doi:10.1093/med-psych/9780190912727.003.0010
Corcoran, J., and Pillai, V. (2009). A review of the research on solution-focused therapy. Br. J. Soc. Work 39 (2), 234–242. doi:10.1093/bjsw/bcm098
Dellazizzo, L., Potvin, S., Luigi, M., and Dumais, A. (2020). Evidence on virtual reality–based therapies for psychiatric disorders: meta-review of meta-analyses. J. Med. Internet Res. 22 (8), e20889. doi:10.2196/20889
De Shazer, S., Dolan, Y., Korman, H., Trepper, T., McCollum, E., and Berg, I. K. (2021). More than miracles: the state of the art of solution-focused brief therapy. Abington, UK: Routledge. doi:10.4324/9781003125600
Dilgul, M., Hickling, L. M., Antonie, D., Priebe, S., and Bird, V. J. (2021). Virtual reality group therapy for the treatment of depression: a qualitative study on stakeholder perspectives. Front. Virtual Real. 1. doi:10.3389/frvir.2020.609545
Falconer, C. J., Rovira, A., King, J. A., Gilbert, P., Antley, A., Fearon, P., et al. (2016). Embodying self-compassion within virtual reality and its effects on patients with depression. BJPsych Open 2 (1), 74–80. doi:10.1192/bjpo.bp.115.002147
Falconer, C. J., Slater, M., Rovira, A., King, J. A., Gilbert, P., Antley, A., et al. (2014). Embodying compassion: a virtual reality paradigm for overcoming excessive self-criticism. PLOS ONE 9 (11), e111933. doi:10.1371/journal.pone.0111933
Flückiger, C., Rubel, J., Del Re, A. C., Horvath, A. O., Wampold, B. E., Crits-Christoph, P., et al. (2020). The reciprocal relationship between alliance and early treatment symptoms: a two-stage individual participant data meta-analysis. J. Consult. Clin. Psychol. 88 (9), 829–843. doi:10.1037/ccp0000594
Fodor, L. A., Coteț, C. D., Cuijpers, P., Szamoskozi, Ș., David, D., and Cristea, I. A. (2018). The effectiveness of virtual reality based interventions for symptoms of anxiety and depression: a meta-analysis. Sci. Rep. 8 (1), 10323. doi:10.1038/s41598-018-28113-6
Frank, J. D., and Frank, J. B. (1993). Persuasion and healing: a comparative study of psychotherapy. Baltimore, MD: JHU Press. doi:10.1097/00005053-199308000-00022
Gingerich, W. J., and Peterson, L. T. (2013). Effectiveness of solution-focused brief therapy: a systematic qualitative review of controlled outcome studies. Res. Soc. Work Pract. 23 (3), 266–283. doi:10.1177/1049731512470859
Giovanetti, A. K., Punt, S. E., Nelson, E. L., and Ilardi, S. S. (2022). Teletherapy versus in-person psychotherapy for depression: a meta-analysis of randomized controlled trials. Telemedicine e-Health 28 (8), 1077–1089. doi:10.1089/tmj.2021.0294
Gonçalves, R., Pedrozo, A. L., Coutinho, E. S. F., Figueira, I., and Ventura, P. (2012). Efficacy of virtual reality exposure therapy in the treatment of ptsd: a systematic review. PLOS ONE 7 (12), e48469. doi:10.1371/journal.pone.0048469
Gulliver, A., Griffiths, K. M., and Christensen, H. (2010). Perceived barriers and facilitators to mental health help-seeking in young people: a systematic review. BMC Psychiatry 10 (1), 113. doi:10.1186/1471-244X-10-113
Hartig, T., Korpela, K., Evans, G. W., and Gärling, T. (1996). Validation of a measure of perceived environmental restorativeness. Goteborg Psychol. Rep. 26 (7). doi:10.1080/02815739708730435
Hartig, T., Korpela, K., Evans, G. W., and Gärling, T. (1997). A measure of restorative quality in environments. Scand. Hous. Plan. Res. 14 (4), 175–194. doi:10.1080/02815739708730435
Hartley, D. (2004). Rural health disparities, population health, and rural culture. Am. J. Public Health 94 (10), 1675–1678. doi:10.2105/AJPH.94.10.1675
Hill, C. E. (1992). An overview of four measures developed to test the hill process model: therapist intentions, therapist response modes, client reactions, and client behaviors. J. Couns. Dev. 70 (6), 728–739. doi:10.1002/j.1556-6676.1992.tb02156.x
Hill, C. E., Helms, J. E., Spiegel, S. B., and Tichenor, V. (2001). Development of a system for categorizing client reactions to therapist interventions. American Psychological Association, 60. doi:10.1037/10412-003
Hwang, K., Kwon, A., and Hong, C. (2017). A preliminary study of new positive psychology interventions: neurofeedback-aided meditation therapy and modified positive psychotherapy. Curr. Psychol. 36, 683–695. doi:10.1007/s12144-016-9538-8
Imel, Z. E., and Wampold, B. E. (2008). The importance of treatment and the science of common factors in psychotherapy. Handb. Couns. Psychol. 4, 249–266.
Jingili, N., Oyelere, S. S., Ojwang, F., Agbo, F. J., and Nyström, M. B. T. (2023). Virtual reality for addressing depression and anxiety: a bibliometric analysis. Int. J. Environ. Res. Public Health 20, 5621. doi:10.3390/ijerph20095621
Kelly, B., Kay-Lambkin, F. J., and Kavanagh, D. J. (2007). “Rurally isolated populations and co-existing mental health and drug and alcohol problems,” in Clinical handbook of Co-existing mental health and drug and alcohol problems (Abington, UK: Routledge).
Kim, J. S. (2008). Examining the effectiveness of solution-focused brief therapy: a meta-analysis. Res. Soc. Work Pract. 18 (2), 107–116. doi:10.1177/1049731507307807
Kim, W., Lim, S. K., Chung, E. J., and Woo, J. M. (2009). The effect of cognitive behavior therapy-based psychotherapy applied in a forest environment on physiological changes and remission of major depressive disorder. Psychiatry investig. 6 (4), 245. doi:10.4306/pi.2009.6.4.245
Klein, D. F. (1997). Control groups in pharmacotherapy and psychotherapy evaluations. Treatment 1 (1), 1a. doi:10.1037/1522-3736.1.1.11a
Li, H., Dong, W., Wang, Z., Chen, N., Wu, J., Wang, G., et al. (2021). Effect of a virtual reality-based restorative environment on the emotional and cognitive recovery of individuals with mild-to-moderate anxiety and depression. Int. J. Environ. Res. Public Health 18 (17), 9053. doi:10.3390/ijerph18179053
Li, M., and Lu, B.-L. (2009). “Emotion classification based on gamma-band EEG,” in 2009 annual international conference of the. IEEE Engineering in Medicine and Biology Society, 1223–1226. doi:10.1109/IEMBS.2009.5334139
Lindner, P. (2021). Better, virtually: the past, present, and future of virtual reality cognitive behavior therapy. Int. J. Cognitive Ther. 14 (1), 23–46. doi:10.1007/s41811-020-00090-7
Lutz, W. (2003). Efficacy, effectiveness, and expected treatment response in psychotherapy. J. Clin. Psychol. 59 (7), 745–750. doi:10.1002/jclp.10169
Macdonald, A. (2011). Solution-focused therapy: theory, research & practice. Thousand Oaks, CA: SAGE. doi:10.4135/9781446288764
Mallinckrodt, B. (1993). Session impact, working alliance, and treatment outcome in brief counseling. J. Couns. Psychol. 40, 25–32. doi:10.1037/0022-0167.40.1.25
McClintock, A. S., Anderson, T., and Petrarca, A. (2015). Treatment expectations, alliance, session positivity, and outcome: an investigation of a three-path mediation model. J. Clin. Psychol. 71 (1), 41–49. doi:10.1002/jclp.22119
Möller-Leimkühler, A. M. (2002). Barriers to help-seeking by men: a review of sociocultural and clinical literature with particular reference to depression. J. Affect. Disord. 71 (1), 1–9. doi:10.1016/S0165-0327(01)00379-2
Novella, J. K., Ng, K. M., and Samuolis, J. (2022). A comparison of online and in-person counseling outcomes using solution-focused brief therapy for college students with anxiety. J. Am. Coll. Health 70 (4), 1161–1168. doi:10.1080/07448481.2020.1786101
Palmer, S. (2015). The beginner’s guide to counselling & psychotherapy. The Beginner’s Guide to Counselling & Psychotherapy, 1–480. doi:10.4135/9781473918061
Peining, P., Tan, G., Aung, A., and Phyo wai, A. aung (2017). Evaluation of consumer grade EEG headsets for BCI drone control. Biopolis, SG: Unpublished manuscript.
Pressly, P. K., and Heesacker, M. (2001). The physical environment and counseling: a review of theory and research. J. Couns. Dev. 79 (2), 148–160. doi:10.1002/j.1556-6676.2001.tb01954.x
Reynolds, S., Stiles, W. B., Barkham, M., Shapiro, D. A., Hardy, G. E., and Rees, A. (1996). Acceleration of changes in session impact during contrasting time-limited psychotherapies. J. Consult. Clin. Psychol. 64 (3), 577–586. doi:10.1037/0022-006x.64.3.577
Sakallaris, B. R., Macallister, L., Voss, M., Smith, K., and Jonas, W. B. (2015). Optimal healing environments. Glob. Adv. health Med. 4 (3), 40–45. doi:10.7453/gahmj.2015.043
SAMHSA (2021). Key substance use and mental health indicators in the United States: results from the 2020 national survey on drug use and health, 156. Available at: https://www.samhsa.gov/data/report/2020-nsduh-annual-national-report.
Sampaio, M., Navarro Haro, M. V., De Sousa, B., Vieira Melo, W., and Hoffman, H. G. (2021). Therapists make the switch to telepsychology to safely continue treating their patients during the COVID-19 pandemic. Virtual reality telepsychology may Be next. Front. Virtual Real. 1, 576421. doi:10.3389/frvir.2020.576421
Scheel, M. J., Berman, M., Friedlander, M. L., Conoley, C. W., Duan, C., and Whiston, S. C. (2011). Counseling-related research in counseling psychology: creating bricks, not edifices. Couns. Psychol. 39 (5), 719–734. doi:10.1177/0011000011410894
Seinfeld, S., Hasler, B. S., Banakou, D., and Levy, J. (2022). Editorial: virtual reality and empathy. Front. Psychol. 13, 1089006. doi:10.3389/fpsyg.2022.1089006
Simpson, S., Richardson, L., Pietrabissa, G., Castelnuovo, G., and Reid, C. (2021). Videotherapy and therapeutic alliance in the age of COVID-19. Clin. Psychol. Psychotherapy 28 (2), 409–421. doi:10.1002/cpp.2521
Simpson, S. G., and Reid, C. L. (2014). Therapeutic alliance in videoconferencing psychotherapy: a review. Aust. J. Rural Health 22 (6), 280–299. doi:10.1111/ajr.12149
Slater, M., Banakou, D., Beacco, A., Gallego, J., Macia-Varela, F., and Oliva, R. (2022). A separate reality: an update on place illusion and plausibility in virtual reality. Front. Virtual Real. 3, 914392. doi:10.3389/frvir.2022.914392
Society for Virtual Reality (2023). Cost analysis. Available at: https://www.svrt.org/vr-therapy-cost-analysis.
Stiles, W. B., Reynolds, S., Hardy, G. E., Rees, A., Barkham, M., and Shapiro, D. A. (1994). Evaluation and description of psychotherapy sessions by clients using the session evaluation questionnaire and the session impacts scale. J. Couns. Psychol. 41, 175–185. doi:10.1037/0022-0167.41.2.175
Tacca, C., Kerr, B., and Friis, E. (2022). “The development of a common factors based virtual reality therapy system for remote psychotherapy applications,” in 2022 IEEE conference on virtual reality and 3D user interfaces abstracts and workshops (VRW) (IEEE), 454–458.
Tryon, G. S. (1990). Session depth and smoothness in relation to the concept of engagement in counseling. J. Couns. Psychol. 37, 248–253. doi:10.1037/0022-0167.37.3.248
Wang, Z., Li, Y., An, J., Dong, W., Li, H., Ma, H., et al. (2022). Effects of restorative environment and presence on anxiety and depression based on interactive virtual reality scenarios. Int. J. Environ. Res. Public Health 19 (13), 7878. doi:10.3390/ijerph19137878
Weber, D., Hertweck, S., Alwanni, H., Fiederer, L. D., Wang, X., Unruh, F., et al. (2021). A structured approach to test the signal quality of electroencephalography measurements during use of head-mounted displays for virtual reality applications. Front. Neurosci. 15, 733673. doi:10.3389/fnins.2021.733673
Weightman, M. (2020). Digital psychotherapy as an effective and timely treatment option for depression and anxiety disorders: implications for rural and remote practice. J. Int. Med. Res. 48 (6), 030006052092868. doi:10.1177/0300060520928686
Witmer, B. G., Jerome, C. J., and Singer, M. J. (2005). The factor structure of the presence questionnaire. Presence Teleoperators Virtual Environ. 14 (3), 298–312. doi:10.1162/105474605323384654
XR health (2020). Pricing. Available at: https://www.xr.health/pricing/.
Keywords: virtual reality, EEG, remote psychotherapy, positive psychology, solution-focused
Citation: Tacca C, Kerr BA, McLamb C, Ridgway KL and Friis EA (2024) Efficacy of a remote virtual reality and EEG enabled psychotherapy system for the treatment of depressive symptoms. Front. Virtual Real. 5:1281017. doi: 10.3389/frvir.2024.1281017
Received: 21 August 2023; Accepted: 22 April 2024;
Published: 24 May 2024.
Edited by:
Avinash Kumar Singh, University of Technology Sydney, AustraliaReviewed by:
Ane Wilhelmsen-Langeland, Haukeland University Hospital, NorwayRaquel Simões de Almeida, Polytechnic of Porto, Portugal
Copyright © 2024 Tacca, Kerr, McLamb, Ridgway and Friis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Barbara A. Kerr, YmtlcnJAa3UuZWR1