 Benjamin Arnfred
Benjamin Arnfred Johanna Kvist Svendsen
Johanna Kvist Svendsen Ali Adjourlu
Ali Adjourlu Carsten Horthøj
Carsten Horthøj- 1Copenhagen Research Center for Mental Health—CORE, Mental Health Center Copenhagen, Copenhagen University Hospital, Hellerup, Denmark
- 2Multisensory Experience Lab, Aalborg University, Copenhagen, Denmark
- 3Department of Public Health, University of Copenhagen, Copenhagen, Denmark
Introduction: The use of virtual reality technology to deliver exposure therapy in the treatment of phobic anxiety (i.e., social anxiety disorder, agoraphobia, and specific phobia) has been proposed to be advantageous compared with in-vivo exposure therapy. These supposed advantages depend on the features of the virtual reality technology and how it is used therapeutically. Therefore, the aim of this study was to provide a comprehensive overview of the features of the hardware and software used in studies examining virtual reality exposure therapy studies for phobic anxiety disorders.
Methods: 70 studies using virtual reality exposure therapy to treat social anxiety disorder, agoraphobia and/or specific phobia, were systematically reviewed for 46 data points relating to these features.
Results: We found that studies generally did not utilize contemporary virtual reality technology and that hardware and software features were inconsistently delineated.
Discussion: The implications of these findings are that the use of modern virtual reality technology represents a relevant frontier in anxiety treatment and that a framework for reporting technical features of virtual reality exposure interventions would benefit the field.
Introduction
Social anxiety disorder (SAD), agoraphobia and specific phobia are characterized by pronounced fear and often extensive avoidance of specific situations and/or stimuli (American Psychiatric Association, 2013). Patients with SAD fear situations where they perceive a risk of negative evaluation from other people. Patients with agoraphobia fear situations in which escape is difficult or where help might not be available in the event of a panic attack, panic-like symptoms, or incapacitating symptoms such as loss of bladder and/or bowel control. Patients with specific phobia have extreme fear reactions to either specific animal types (e.g., dogs, spiders), natural environments (e.g., thunder, heights), injury (e.g., dentists, injections, blood) or situations (e.g., enclosed spaces, flying). Phobic disorders are associated with marked reduction in normal functioning capabilities, have an early onset, long duration and are highly prevalent, with estimates ranging from 4%–12% depending on the country (Kessler et al., 2005, 2012; Wang et al., 2005; Stein et al., 2017).
Cognitive Behavioral Therapy (CBT) has proven an effective intervention for SAD and agoraphobia and is the recommended first-line treatment in several clinical guidelines (National Institute for Health and Care Excellence, 2011a; National Institute for Health and Care Excellence, 2011b; National Institute for Health and Care Excellence, 2013; Sundhedsstyrelsen, 2016). An important element of CBT for phobic disorders is exposure therapy. In exposure therapy, the patient is systematically confronted with feared stimuli and the patient’s expectations of the likelihood and consequences of a feared outcome are challenged (Abramowitz et al., 2019). However, the application of exposure therapy is generally dependent on the disorder and the underlying theory that the clinician aligns with.
Thus, exposure therapy for specific phobia often involves probability estimations before/after exposures, long exposure exercises allowing the patient to gradually approach the feared object and minimal therapeutic work before and after exposure exercises (Öst, 2012).
Exposure therapy for agoraphobia often involves exposure to a combination of physiological sensations (e.g., dizziness, being out of breath, the urge to urinate/defecate/vomit) and the specific situations triggering these sensations, which is generally situations where escape or help is perceived to be unavailable (e.g., public transportation, elevators, driving alone, bridges) (Craske, 2002).
For SAD, exposure therapy is often combined with social skills training and attention training (i.e., shifting from an inward to an outward focus) and involves both public speaking exercises and one-on-one social interactions (Turk et al., 2008).
Beyond the disorder specific variations in exposure therapy, multiple explanations for the psychological mechanisms underlying exposure therapy have been proposed. Of these, two theories in particular have informed practice in recent decades: Emotional Processing Theory and Inhibitory Learning Theory.
In Emotional Processing Theory, between-session habituation (i.e., the lessening of an initial fear response during an exposure, between two exposure exercises) is thought to reflect progress in emotional processing and is therefore an important treatment goal and benchmark of progress (Foa and McLean, 2016).
In contrast, for Inhibitory Learning Theory, the primary goal of exposure exercises is to maximize the discrepancy between what the patient fears will happen and what actually happens during exposure. One strategy to maximize this discrepancy is to purposefully design exercises to be more challenging than how those actions are commonly performed (e.g., asking strangers for directions to nonsensical locations). Another strategy is to minimize or remove safety signals (i.e., a companion) and safety behaviors (i.e., rehearsing social interactions) (Craske, 2022).
Therefore, depending on the disorder and theoretical underpinnings, the execution of exposure therapy can vary and may thus also vary in logistical demands and aversiveness (Butler, 1985; Olatunji et al., 2009; Neudeck and Einsle, 2012; Pittig et al., 2019).
In virtual reality exposure therapy (VRET), the patient is exposed to feared stimuli via immersive Virtual Reality (VR) technology. The proposed benefits of VRET compared with in-vivo exposure therapy is flexibility, acceptability and decreased logistical demand because it allows patients to confront virtual, yet credible, feared situations from the therapist’s office or from home (Botella et al., 2017; Bouchard et al., 2017; Freeman et al., 2017). Immersive VR technology encompasses all technology that induces an illusion of actually being in a virtual environment, an experience termed presence (Lombard and Ditton, 1997).
VRET is commonly delivered via head-mounted displays (HMD). HMDs typically place one or two display optics in front of the user’s eyes, combined with a head tracking system and an input device for interacting with the virtual environment (e.g., a controller) (Cieślik et al., 2020). Meta-analysis has shown that the treatment effect of VRET for phobic anxiety, either as a stand-alone treatment or integrated into CBT, is not significantly different from active control conditions (Carl, 2018; Chesham et al., 2018). However, for SAD specifically, VRET has been found to result in significantly lower effect sizes compared to control groups that received equal amounts of in-vivo exposure (Wechsler et al., 2019). Considering the proposed benefits of VRET, what might explain these findings?
An important aspect of VRET, is that potential benefits are contingent on the characteristics of its hardware (e.g., quality of optical device, tracking capabilities) and software (e.g., interaction options, range of environments). For example, if a VRET ‘setup’ (i.e., it’s software and hardware) does not allow patients to converse, it might be inadequate for many patients with SAD (Emmelkamp et al., 2020). In addition, the cognitive and behavioral strategies available in VRET will depend on the VRET setup (Bouchard, 2012).
The patients experience of the virtual environments is also contingent on the quality of the hardware and software in a VRET setup. Sense of presence, has been found to be greater in high-immersion VR setups as compared to low-immersion VR setups (Cummings and Bailenson, 2016). Anxiety and presence seem to correlate (Ling et al., 2014; Diemer, 2015), which points to its importance, because exposure therapy is thought to rely on the patient experiencing a certain level of anxiety (Foa and McLean, 2016; Craske, 2022). Yet, findings relating to presence and treatment efficacy are inconclusive, especially for SAD (Price et al., 2011; Ling et al., 2014).
However, it stands to reason that the VRET setup must influence the quality of therapy, since it determines:
• Applicability (e.g., the range of virtual environments that are available)
• Acceptability (e.g., ease-of-use for patient and therapist)
• Accessibility (e.g., options for self-led VR-based therapy)
• The visual and auditory quality of the virtual environments
• The cognitive and behavioral strategies that are possible (e.g., the degree to which interaction is possible in the virtual environments)
One step towards a better understanding of the impact of a VRET setup on treatment efficacy is a systematic mapping of the hardware and software features in existing research. This should put researchers in a better position to interpret results and make informed decisions when developing new VRET interventions. Such a review could also serve as a framework that can assist researchers to systematically describe VRET interventions in future research.
Objectives
In this scoping review, we systematically describe and categorize the hardware and software features used in VRET research for phobic anxiety disorders. We were guided by the following research questions:
• What are the technical features of the hardware and software used in extant VRET research for phobic anxiety disorders?
• What are the salient features of the hardware and software used in VRET for phobic anxiety disorders and to what extent are they reported?
Methods
Eligibility criteria
To be included in the review, publications needed to:
• Use VRET in the treatment of SAD and/or agoraphobia and/or specific phobia
• Use HMDs as their method for delivering the visual stimuli in their VR setups
• Examine clinical populations, assessed with validated diagnostic instruments
• Have been published in 2005 or after, due to the fast pace of development in virtual reality technology in recent years
• Be peer-reviewed
• Be in English, Danish, Swedish or Norwegian
Information sources
To identify relevant studies the following bibliographic databases were searched on 31.03.2021 and on 13.04.2022: PubMED, PsycINFO and Web of Science. Additionally, appropriate reviews and meta-analysis were searched for relevant studies, which our search strategy might have missed (See Supplementary Material S1, for a list of the reviews and meta-analysis searched). Lastly, one author (BTA) asked peers for knowledge of newer studies our search strategy might have missed.
Search strategy
A three-step search strategy was employed. First, an initial search was conducted on the above-mentioned databases to identify the index terms, words in titles and abstracts, and keywords in the resulting studies. Second, the identified keywords and index terms were used to construct a search string used in all the databases. In addition, the following criteria were added to the search: Only peer-reviewed studies, only studies from 2005 or newer (See Supplementary Material S1, for the exact search string and criteria applied). The results of these searches were downloaded as.ris files and uploaded to Covidence, a web-based program specializing in streamlining the systematic review process (Veritas Health Innovation, 2022). Third, duplicates were removed by the built-in function on the website.
Selection of sources of evidence
Two authors selected the sources of evidence: BTA and JS. First, studies were screened by one author (BTA or JS) for eligibility by reading title and abstracts. If there was any doubt about eligibility, another author would be involved in the screening.
Second, studies that survived the first level of scrutiny were fully read by both authors to confirm eligibility. Disagreements on study selection and data extraction were resolved by discussion with a third author. See Figure 1 for a flowchart of the selection process.
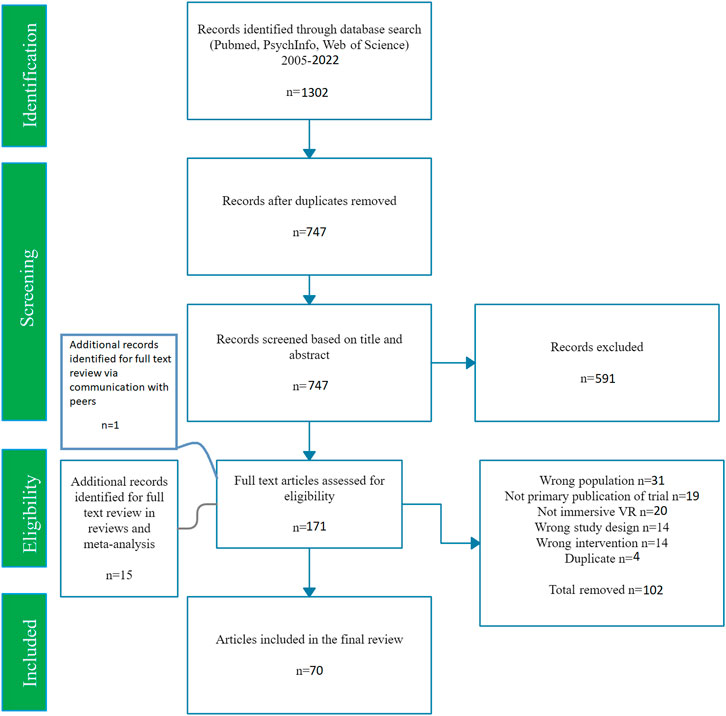
FIGURE 1. Flowchart of the study selection process.
Data charting process
A data-charting form was developed to determine relevant variables of interest. The development process was iterative as reviewers continuously discussed the variables and updated the form throughout the review. In choosing the variables of interest, it was decided to be as exhaustive as possible, since no consensus exists on what the salient features of a VR setup for exposure therapy are. Exhaustiveness was sought by including every variable in the data-charting form that was reported by any of the included studies, unless it was decided through discussion that a reported variable could have no salience for the conductance of the intervention (e.g., the model no. of a computer running the VR environments).
All publications were scrutinized for all data items in the final data-charting form. Data was gathered manually from the included publications, from webpages and from technical documents. When websites were not available or no longer provided relevant information, an earlier snapshot of the site would be found using the ‘Wayback Machine’ (the Internet Archive, 2022), based on the year of the relevant studies’ publication. See Supplementary Material S2, for the final data charting form.
Results
In the following section, data charted from the 70 included studies will be presented. Every data point will not be addressed in this section. However, Supplementary Material S2, contains all data points for all included studies. See Table 1 for an overview of included studies.

TABLE 1. Overview of included studies.
Software features
Social anxiety disorder
21 studies examining SAD were included. The virtual environments used were built around various performance situations (e.g., interviews, presentations), formal social interactions in public (e.g., shopping) and informal social interactions (e.g., eating with coworkers). Of the 21 studies included, three used 360-degree videos (Clemmensen et al., 2020; Zainal, 2021; Arnfred et al., 2022) and one used video-recorded actors superimposed onto a static 360-degree background (Lindner et al., 2019). The remaining studies used rendered environments or did not specify the type they used.
In four out of 21 studies examining SAD, conversation was simulated through the use of pre-recorded sentences and gestures (Herbelin, 2006; Hartanto, 2016; Kampmann et al., 2016; Bouchard et al., 2017). The remaining 17 studies focused on variations of public speaking tasks and situations requiring no conversation (e.g., riding a bus). Audiences in rendered public speaking environments could be made to look bored, interested, or neutral (e.g., Wallach et al., 2011; Anderson et al., 2013; Nazligul, 2017; Jeong et al., 2021). Beyond this, most VR setups had the option of adjusting difficulty by changing the number of avatars, their gender, and their attitude (e.g., Geraets et al., 2019; Kim et al., 2020; krijin and Emmelkamp, 2007). Lastly, for SAD, five studies used VRET at least partially as a self-led therapy tool (Hartanto, 2016; Lindner et al., 2019; Kim et al., 2020; Trahan et al., 2021; Zainal, 2021).
Agoraphobia
Ten studies examining agoraphobia were included. The virtual environments were based on confined spaces where it might be difficult to escape/get help (e.g., elevators, subway, cars, planes) and open spaces where it might be difficult to escape/get help (e.g., empty country, malls, town squares). One study also had an environment designed to induce sensations for interoceptive exposure (Pelissolo, 2012). Of the ten studies, three used 360-degree videos (Lundin, 2021; Shin et al., 2021; Arnfred et al., 2022), while the remaining seven used rendered environments.
The difficulty of the environments could be adjusted by manipulating the number of anxiogenic cues (e.g., the number of avatars), triggering feared outcomes (e.g., turbulence) and manipulating the length of the exercise (e.g., the amount of time needed to stand in line). Additionally, some VR setups allowed the therapist to overlay the environments with cues for feared bodily symptoms (e.g., palpitations and blurred vision) (Botella, 2007; Pérez-Ara et al., 2010; Malbos et al., 2013).
In some VR setups, patients could move and interact with the environment, by using a separate input device (Choi et al., 2005; Botella, 2007; Pérez-Ara et al., 2010; Malbos et al., 2013; Meyerbroeker et al., 2013). Interaction options beyond movement were opening doors, driving, pushing buttons, picking up objects and paying for goods while shopping. Lastly, for agoraphobia, one study used VRET as a therapist independent self-led treatment tool (Shin et al., 2021).
Specific phobia
41 studies examining variations of specific phobia were included. For the 14 studies examining aviophobia, environments were all rendered and consisted of bedrooms (i.e., getting ready to depart), airports, boarding and airplane rides, including lift-offs and landings. Difficulty was in some studies manipulated prior to immersions by changing the weather, amount of turbulence and whether a seatbelt was required (Tortella-Feliu et al., 2011; Meyerbroeker et al., 2012; Rus-Calafell et al., 2013; Botella, 2014). In three studies, patients could pack suitcases, obtain boarding passes, and read magazines before flying (Tortella-Feliu et al., 2011; Rus-Calafell et al., 2013; Botella, 2014). In four studies, patients used VRET while sitting in real airplane chairs with seatbelts and a powerful bass system installed that could vibrate to simulate lift-off and turbulence (Rothbaum et al., 2006; Meyerbroeker et al., 2012; Breuer, 2017; Meyerbröker et al., 2018).
For the 11 studies examining arachnophobia, environments were all rendered and consisted of indoor (e.g., living room) or outdoor (e.g., garden) localities with spiders. Difficulty was graduated by changing the size, amount, behavior, proximity, and realism of the spiders. In two studies, the patient could kill spiders by stepping on them (Bouchard et al., 2006) or swatting them with a magazine (Cote and Bouchard, 2005). Two studies used a gamification principles, in that the patient was required to interact in various ways with spiders to progress in the treatment (Miloff, 2019; Lindner et al., 2020). In one study, treatment was also self-led (Lindner et al., 2020). Lastly, one study draped the HMD wearing patient with a black cloth to block ambient light (Michaliszyn et al., 2010).
For the eight studies examining acrophobia, environments were all rendered and consisted of terraces, balconies, open elevators, and bridges. In three studies, six-degrees of freedom tracking allowed patients to move within a small area and hold on to a physical railing which was also represented virtually (Krijn et al., 2004; Whitney, 2005; Meyerbröker et al., 2018). In some studies, difficulty could be manipulated by increasing the height and/or perceived safety of the situation (Coelho et al., 2006; Graske and Barlow, 2008; de Quervain et al., 2011).
For the three dental phobia studies, the environments were 360-degree videos and consisted of a dental operatory with a dentist (Gujjar et al., 2017; Gujjar et al., 2018, 2019). In challenging difficulties, the dentist would carry various dental tools towards the patient. The patient received the therapy while seated in an actual dental chair and a body representing the patient’s body was visible in the virtual dentist’s chair. Lastly, dental operatory odor was simulated by placing cottons soaked in clove oil near the patient.
For the two hemophobia studies, environments were 360-degree videos and consisted of a blood draw performed in a doctor’s office (Meindl et al., 2019) and various procedures performed by health professionals in hospital and dental settings (Jiang et al., 2020). In one study, the virtual needle prick was timed with a physical prick from a pencil to simulate needle insertion and the therapy room was also made to look almost identical to the virtual doctor’s room (Meindl et al., 2019). In the other study both rendered, and 360-degree video environments were used. In the rendered environments, the patient could experience the procedure either as an observer or as the patient (Jiang et al., 2020).
For the one study examining cynophobia, the environment was 360-degree videos of dogs of different breeds presented in the same office room where therapy took place (Farrell et al., 2021). Difficulty was graduated by changing the breed of the dog, the proximity of the dog, the presence of an owner and the whether the dog was leashed or not.
For the one study examining squalophobia, environments were rendered and consisted of swimming in a pool, a lake and a sea-cove (Malbos et al., 2020). The patient could move using a handheld controller, including swimming and diving. The body of the patient was represented, and arms could be seen doing breaststrokes while swimming. Animals in the environments would react to the presence of the patient by swimming away and the patient could pick up objects, examine them and throw them. The therapist controlled the appearance and movement of a great white shark and used this to challenge the patient.
For the one study nyctophobia, the environment was a rendered house with five distinct rooms (Servera et al., 2020). The therapy was gamified so that the patient was rewarded with tokens for exploring the rooms and remaining in darkness. During VRET, the patient interacts with a virtual helper, while the therapist can control light levels, rain intensity, insert helpful phrases and teleport the patient to the various rooms.
In general, software characteristics were inconsistently reported. More than half of all included studies did not delineate:
• Interaction options within virtual environments.
• What the therapist could see during VRET (e.g., casting or mirrored rendering).
• If the therapist could manipulate the virtual environments during VRET (e.g., changing the facial expressions of avatars during a presentation).
• If the participant had a representation of themselves within the environments and/or whether their body was tracked.
See Table 2 for an overview of the software feature present in the included studies.

TABLE 2. Overview of the software feature present in the included studies.
Hardware features
The HMD models used in the included studies were varied, with 25 different models being used across 57 studies (the remaining 13 studies did not disclose HMD model). The most commonly used HMD was a Samsung Gear with a smartphone, being used in seven studies. For standalone HMDs, the most common model was the eMagin z800. HMDs with high resolution displays (>800 × 600 pr. eye) and high field of view (>90° diagonally) were used in 23 studies, which includes seven studies using smartphone-based HMDs. See Table 3 for an overview of the HMDs used in included studies.
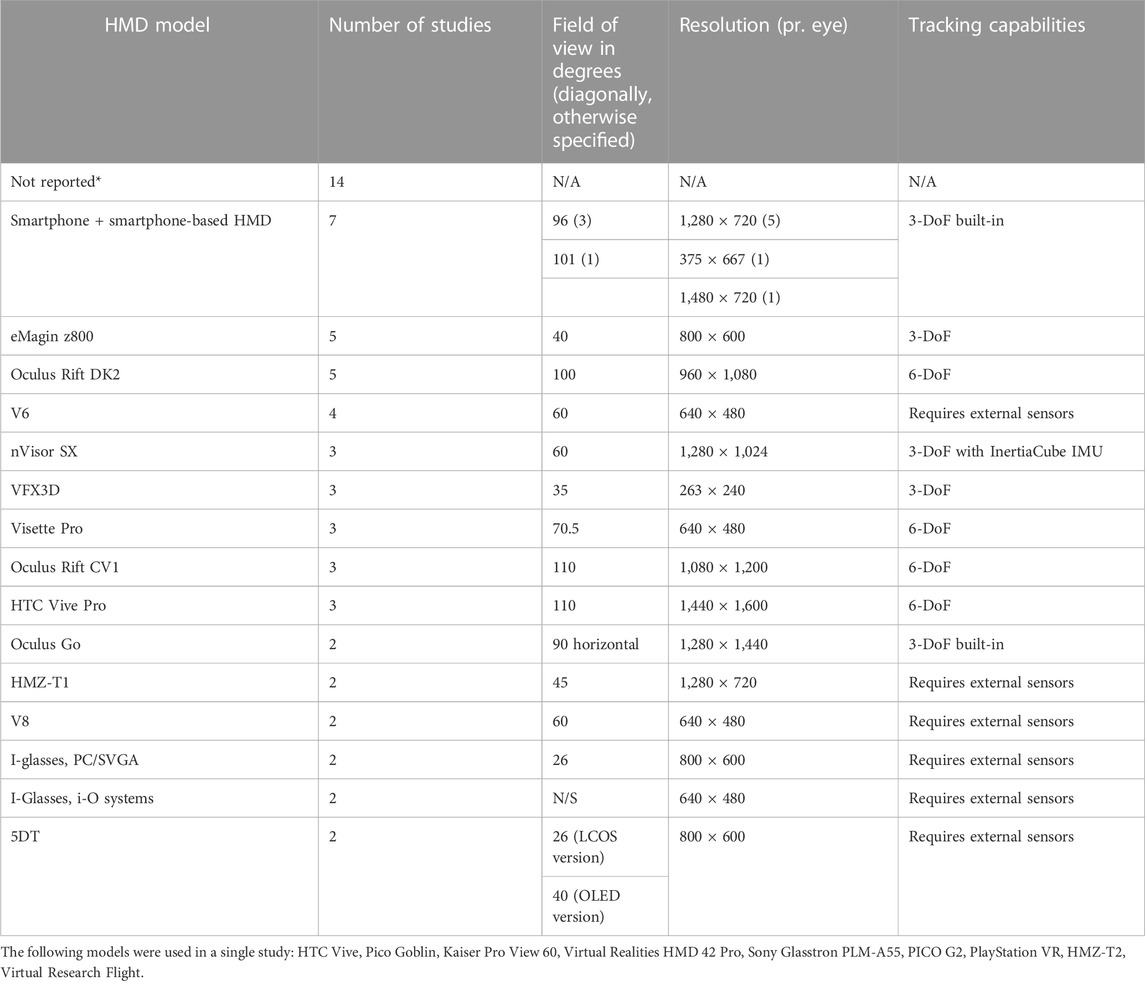
TABLE 3. Overview of the HMDs used in included studies.
It was often unclear what kind of tracking a study used, either because it was not reported or because it was unclear if the software and therapeutic procedures took advantage of any tracking capabilities. Three studies explicitly used six degrees of freedom tracking (Krijn et al., 2004; Whitney, 2005; Meyerbröker et al., 2018). The remaining 67 studies either did not report their tracking or used three degrees of freedom tracking.
Audio delivery system was widely undescribed, though several studies implied that they used the built-in audio system of the HMDs. Directional sound (i.e., sound that discernably matches the location from which it is heard in the virtual environments) was reported in one study (Meyerbröker et al., 2018), and noise cancellation (i.e., headsets that block or mitigate sound from the external environment) was reported in one study (Arnfred et al., 2022).
As has been mentioned, hardware features were generally inconsistently reported. More than half of all included studies did not delineate:
• Tracking capabilities (e.g., degrees of freedom)
• The Interaction method (e.g., controller)
• Audio delivery system, including features related to it (e.g., noise cancellation)
Discussion
In this scoping review, 70 studies were included that use HMD-based VRET to treat SAD, agoraphobia and/or specific phobia. All included studies were reviewed for 46 data points relating to the features of the hardware and software used in VRET. A strength of scoping reviews is that they can identify gaps in existing literature and propose avenues for future research (Arksey and O’Malley, 2005; Pham et al., 2014). As such, the discussion will address the state of extant VR setups vs. contemporary VR technology, as well as the inconsistent reporting of VR features in the included studies.
Gaps between examined VR setups and contemporary VR technology
How large is the gap between existing VR setups and contemporary VR technology? And to what extend might this gap affect relevant clinical variables, such as symptom reduction, acceptability, and attrition?
First, the HMDs used generally had poor specifications compared with widely available and affordable current-generation HMDs (i.e., the Oculus Quest 2). This is especially true for SAD and agoraphobia, where no studies reported their tracking to be six degrees of freedom. Several studies did use HMDs that were capable of six degrees of freedom tracking, but it was never stated that the software utilized took advantage of these capabilities.
Second, the movement and interaction within virtual environments were generally limited. Only four studies utilized the actual physical movement of the patient in therapy (Krijn et al., 2004; Whitney, 2005; Meyerbröker et al., 2018; Reitmaier et al., 2022) and the method for interacting was also generally outdated, with no studies utilizing body tracking. Similarly, there were only two studies utilizing haptic feedback (Meindl et al., 2019; Jiang et al., 2020) and three studies utilizing olfactory feedback (Gujjar et al., 2017; Gujjar et al., 2018, 2019). Notably, all the above-referenced studies examined specific phobia.
Third, no studies reported using any multi-user functions (i.e., two or more users using a shared virtual environment) within virtual environments. Though one study used a program where it was possible (Geraets et al., 2019).
Lastly, though seven studies examined self-led VR-based therapy (Hartanto, 2016; Lindner et al., 2019, 2020; Kim et al., 2020; Shin et al., 2021; Trahan et al., 2021; Zainal, 2021), no studies utilized online multi-user VR-based therapy (i.e., multiple users meeting online in the same virtual environment). One trial, not included in the present review, is currently in progress examining online multi-user VR-based group therapy for depression (Dilgul et al., 2021).
It seems fair to summarize that VR setups for phobic anxiety, and especially SAD and agoraphobia, has yet to take full advantage of contemporary VR technology. However, it is unclear how important this gap is for clinical outcomes. On the one hand, studies have found display factors (i.e., resolution, field of view, refresh rate), audio factors (e.g., directional sound), tracking, and framerate (i.e., the number of pictures displayed pr. second) to be related to a higher degree of presence (Youngblut, 2003; Cummings and Bailenson, 2016; Felton and Jackson, 2022), engagement (Sylaiou, 2010; Brade, 2017) and embodiment (i.e., the experience of owning a body within VR) (Slater, 2018) as well as a lower degree of cybersickness (i.e., motion sickness-like symptoms caused by prolonged HMD use) (Chang, 2020; Saredakis et al., 2020).
On the other hand, several studies have failed to find significant associations between presence and treatment efficacy (Krijn et al., 2004; Price and Anderson, 2007; Meyerbröker et al., 2011). Though contradictory evidence does exist (Price et al., 2011). Similarly, it remains unclear if presence is necessary to generalize learning achieved in virtual environments to real-life, with studies producing contradicting results (Makransky et al., 2019; Grassini et al., 2020).
The concept of presence has generally been difficult to study due to a plethora of competing definitions and measurement methods (Lombard, 2015; Grassini and Laumann, 2020). Even so, presence has been consistently found to be correlated to anxiety in virtual environments (Bouchard et al., 2008; Gorini et al., 2011; Ling et al., 2014; Peperkorn et al., 2015; Peperkorn et al., 2016) and is thus still considered an important aspect of VRET (Diemer et al., 2014; Morina, 2015).
Nevertheless, software and hardware features directly affect the range, customizability and interactability of virtual environments and thus influence therapists’ ability to manipulate the presentation of conditional stimuli (central in all exposure therapy), and therefore also the ability to manipulate exposure exercises for graduation of difficulty, habituation, and expectancy violation.
For example, using 360-degree video environments (e.g., Zainal, 2021) which at best allow limited interaction, may not be optimal for exposing patients to social interactions and/or training social skills. On the other hand, using virtual environments to access extremely challenging or otherwise unethical exposure exercises (e.g., Cote and Bouchard, 2005; Arnfred et al., 2022) may be a useful way to maximize expectancy violation, especially when testing expectancies regarding internal states (e.g., “I’ll clam up if I ever get into a conflict with my boss”).
Further, utilizing multi-user virtual environments could provide a method for engaging patients in a wide variety of social interaction, which may otherwise be difficult to simulate (Emmelkamp et al., 2020). Roleplaying with a therapist in multi-user virtual environments has been used successfully in the treatment of social anxiety in patients with psychosis (Pot-Kolder et al., 2018), but was not utilized in any of the studies included in this review.
For treating certain types of specific phobia, the use of six degrees of freedom tracking allowing patients to physically approach feared objects (e.g., Reitmaier et al., 2022) may be an important feature. Further, any measures to increase comfort and reduce cybersickness would allow patients to stay in the environments for extended periods, mimicking the gold standard treatments (Öst, 2012). As such, these features may be especially important when treating specific phobia using VRET.
For agoraphobia, three studies incorporated cues in an attempt induce fear of bodily sensations (Botella, 2007; Pérez-Ara et al., 2010; Malbos et al., 2013). This could be combined with classic interoceptive exposure exercises, such as spinning to induce dizziness, hyperventilating to induce tingling/dissociation, or drinking water to induce a need to urinate. However, no included studies stated they did so. As with the other phobic disorders, VR also allows access to useful but otherwise unethical situations, such as having your car break down on a heavily trafficked bridge (Arnfred et al., 2022).
Meta-analysis has already shown promising results for VRET in the treatment of phobic anxiety (Carl, 2018; Wechsler et al., 2019; Morina, 2021), but superiority to active control conditions has not yet been established. As such, the development of contemporary VR setups that fully capitalize on the advantages of the technology according to the specific disorder and an underlying empirically based theory, may be an important avenue for future clinical research.
Inconsistent reporting
In general, the data of interest for the present review was rarely reported consistently. The data charting form in this review was exhaustive and thus it was expected that some study designs and publication types (e.g., brief reports) would not provide information on every datapoint. Nevertheless, certain salient datapoints were expected in every publication or its referenced material because they directly impact the therapeutic procedure. These were:
• A description of how VR was used in therapy (e.g., presence of a therapist) and how much VRET was administered.
• A description of the hardware used, including: visual output device, auditory output device, interaction device, and tracking.
• A description of the software used, including: The virtual environments (or screenshots/video links), interaction elements, customizability (during and/or before immersion), movement and any auxiliary software that the therapist used during exposure (e.g., casting a live view of the patient’s point of view to a monitor).
• A description of further measures taken to improve or alter the experience of the VRET, including the use of: Olfactory feedback, haptic feedback, and/or miscellaneous measures (e.g., placing cloth over a participant’s head to block light).
Only three studies reported all of the above information, either in-text or through references (Malbos et al., 2013; Kampmann et al., 2016; Zainal, 2021). For an additional eight studies, the above information was found in-text, through referenced studies and through online searches (Whitney, 2005; Botella, 2007; Miloff, 2019; Lindner et al., 2020; Servera et al., 2020; Lundin, 2021; Shin et al., 2021; Arnfred et al., 2022). For the remaining 59 studies, all the information could not be found in English. This presents the reader of these 59 studies with two problems: First, is the problem of interpreting the results of a study in which you do not have an adequate understanding of the intervention. Second, is the problem of re-creating or adapting a treatment that is not thoroughly described (Boutron, 2009; Guidi et al., 2018). The latter is perhaps especially true in the quickly developing field of VR-based treatment for mental health disorders.
A framework for reporting VR setups
A reporting framework may be a useful way to increase transparency of VR-based interventions. Two challenges to clear dissemination were repeatedly observed:
1. Referring to websites which were no longer active, or which no longer contained any relevant information pertaining to the study in question.
2. Reporting unimportant features, such as the components of the computer rendering the virtual environments (e.g., graphics processing unit, central processing unit), while omitting to describe salient features (e.g., tracking, HMD model).
Because it is unfeasible to report all technical features of a VR setup, the information that is the most pertinent to the hypothesis of the study should be prioritized. In studies investigating VRET-based treatment, the salient features are those that impact the therapeutic procedure. For example, information about the processing power of the computer rendering the virtual environments is less important compared to the effect it has on the experience of the virtual environments, that is, preferably producing a high and stable framerate.
Case in point, low framerate has been associated with increased risk of cybersickness (Jones et al., 2004), while high framerate has been associated with a greater sense of presence (Meehan et al., 2002; Meehan, 2003). Yet, of the included studies, only one mentioned the framerate of their virtual environments (Meyerbroeker et al., 2012), while 37 studies reported at least one component of the computers running their virtual environments. A framework for reporting VR setups in VRET studies may be a useful way to counteract these challenges in future studies. Such a framework should contain information that gives the reader a clear idea of the participants experiences of the virtual environments and the therapeutic procedures possible within them. Lastly, such a framework should be accompanied by media (e.g., videos or photos) of the virtual environments, since media can give the viewer an immediate idea of the quality and content (e.g., the number of conditioned stimuli available) of the environments.
Examining which exact features should be included in such a framework and how the ultimate quality of a therapeutic VR setup should be evaluated is beyond the scope of the current study but would be useful areas of future research. A preliminary framework based on the data charting form used in this review, can be found in Supplementary Material S3.
Limitations
There were two primary limitations in conducting the present study. First, when extracting the data of the included studies, we considered it appropriate to derive some data indirectly. This was often the case with the audio hardware used, which was rarely directly stated to be the built-in headset/speakers of the HMD but was often indirectly stated. In such cases, it was discussed between the authors if it was appropriate to include it in the study. Data was only included when it was deemed by all involved authors to be accurate. Individual data-points which were not directly reported, has been marked as such in the data chart (See Supplementary Material S2).
Second, there was a general challenge in interpreting the interplay between the software and the hardware used in the VR setups of the included studies. Using a powerful HMD with contemporary visual specifications and tracking is inconsequential if the software run on it does not take advantage of the hardware. Conversely, the quality of high-fidelity virtual environments can be severely negatively impacted by being presented on older or low-end HMDs. This interaction was not accounted for in this study and may thus represent a source of bias in the interpretation of the findings.
Conclusion
Research has yet to examine VRET for phobic anxiety delivered with top-of-the-line hardware and software. Thus, to the extent that technical features affect important variables such as accessibility (e.g., access for homebound patients), acceptability (e.g., ease-of-use, minimal cybersickness), applicability (e.g., a range of environments for a general clinical population) and treatment effect (e.g., presence induced, availability of therapeutic procedures), the development of contemporary VR setups may represent an important Frontier in the field.
Despite the seeming importance of the hardware and software used for VRET, existing publications inconsistently report the technical aspects of their intervention. Thus, pertinent questions in the field are difficult to approach and extant research is difficult to build upon. A framework for delineating the salient technical features of a VR setup for VRET may increase transparency in future studies. A preliminary framework is proposed.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Author contributions
BA initiated the review. Wrote the protocol, determined the search strategy and drafted the initial data charting form. BA performed approximately 50% of the work assosciated with evidence selection and data charting process. BA wrote the initial draft for the manuscript and all further revisions. JS performed approximately 50% of the work assosciated with evidence selection and data charting process. JS also calculated and edited tables. CH criticially examined the review methodology. AA critically examined the technical terminology, the phrasing of the data charting form and provided general technical expertise. All authors contributed to the article and approved the submitted version.
Funding
This study was conducted as part of a PhD programme, embedded into the SoREAL trial (Can be found online at https://clinicaltrials.gov/ct2/show/NCT03845101). The SoREAL trial was funded by the Novo Nordisk Foundation [NNF17OC0027780] and by TrygFonden [ID: 146169]. The study is entirely independent of the Novo Nordisk Foundation and TrygFonden and therefore, the funding bodies plays no role in the design of the study, the review process, the analysis, and interpretation of data, in writing the manuscript, or the decision to submit it for publication.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frvir.2023.952741/full#supplementary-material
References
Abramowitz, J. S., Deacon, B. J., and Whiteside, S. P. H. (2019). Exposure therapy for anxiety: Principles and practice. 2nd edn New York, NY, US: The Guilford Press.
American Psychiatric Association (2013). Diagnostic and statistical manual of mental disorders. 5th edn Washington.
Anderson, P. L., Price, M., Edwards, S. M., Obasaju, M. A., Schmertz, S. K., Zimand, E., et al. (2013). Virtual reality exposure therapy for social anxiety disorder: A randomized controlled trial. J. Consult. Clin. Psychol. 81 (5), 751–760. doi:10.1037/a0033559
Arksey, H., and O’Malley, L. (2005). Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. Theory Pract. 8 (1), 19–32. doi:10.1080/1364557032000119616
Arnfred, B., Bang, P., Hjorthøj, C., Christensen, C. W., Stengaard Moeller, K., Hvenegaard, M., et al. (2022). Group cognitive behavioural therapy with virtual reality exposure versus group cognitive behavioural therapy with in vivo exposure for social anxiety disorder and agoraphobia: A protocol for a randomised clinical trial. BMJ Open 12 (2), e051147. doi:10.1136/bmjopen-2021-051147
Botella, C., Fernández-Álvarez, J., Guillén, V., García-Palacios, A., and Baños, R. (2017). Recent progress in virtual reality exposure therapy for phobias: A systematic review. Curr. PSYCHIATRY Rep. 19 (7), 42. doi:10.1007/s11920-017-0788-4
Botella, C. (2014). Treatment of flying phobia using virtual reality exposure with or without cognitive restructuring: PARTICIPANTS’ PREFERENCES/tratamiento de la fobia a volar usando la exposición de realidad virtual con o sin reestructuración cognitiva: Preferencias de los. Rev. Psicopatología Psicol. Clinica 19 (3), 157–169. doi:10.5944/rppc.vol.19.num.3.2014.13898
Botella, C. (2007). Virtual reality exposure in the treatment of panic disorder and agoraphobia: A controlled study’, clinical Psychology and psychotherapy. Bognor Regis 14 (3), 164. doi:10.1002/cpp.524
Bouchard, S., Côté, S., St-Jacques, J., Robillard, G., and Renaud, P. (2006)., 14. Netherlands, 19–27. doi:10.3233/thc-2006-14103Effectiveness of virtual reality exposure in the treatment of arachnophobia using 3D gamesTechnol. Health Care
Bouchard, S., Dumoulin, S., Robillard, G., Guitard, T., Klinger, É., Forget, H., et al. (2017). Virtual reality compared with in vivo exposure in the treatment of social anxiety disorder: A three-arm randomised controlled trial. Br. J. psychiatry J. Ment. Sci. Engl. 210 (4), 276–283. doi:10.1192/bjp.bp.116.184234
Bouchard, S., St-Jacques, J., Robillard, G., and Renaud, P. (2008). Anxiety increases the feeling of presence in virtual reality. Presence Teleoperators Virtual Environ. 17 (4), 376–391. doi:10.1162/pres.17.4.376
Bouchard, S. (2012). ‘Description of a treatment manual for in virtuo exposure with specific phobia’, Virtual reality in psychological. Med. pedagogical Appl. 22, 81–108. doi:10.5772/46417
Boutron, I. (2009). Extending the CONSORT statement to randomized trials of nonpharmacologic treatment: Explanation and elaboration. J. Chin. Integr. Med. 7 (7), 690–699.
Brade, J. (2017) ‘Being there again – presence in real and virtual environments and its relation to usability and user experience using a mobile navigation task’, Int. J. Hum. Comput. Stud., 101p. 76–87. doi:10.1016/j.ijhcs.2017.01.004
Breuer, T. A. (2017) Effects of values clarification intervention on treatment adherence and homework compliance during exposure therapy protocol for aviophobia, Dissertation.
Butler, G. (1985). Exposure as a treatment for social phobia: Some instructive difficulties. Behav. Res. Ther. 23 (6), 651–657. doi:10.1016/0005-7967(85)90060-9
Carl, E. (2018). Virtual reality exposure therapy for anxiety and related disorders: A meta-analysis of randomized controlled trials, Journal of anxiety disorders. Elsevier Ltd. Amsterdam, Netherlands, doi:10.1016/j.janxdis.2018.08.003
Chang, E. (2020). Virtual reality sickness: A review of causes and measurements virtual reality sickness: A review of causes and measurements. Int. J. Human–Computer Interact. 36 (17), 1658–1682. doi:10.1080/10447318.2020.1778351
Chesham, R. K., Malouff, J. M., and Schutte, N. S. (2018). “Meta-analysis of the efficacy of virtual reality exposure therapy for social anxiety,” in Behaviour change (Chennai, Tamil Nadu: Cambridge University of press), 1–15. doi:10.1017/bec.2018.15
Choi, Y.-H., Vincelli, F., Riva, G., Wiederhold, B. K., Lee, J. H., and Park, K. H. (2005). Effects of group experiential cognitive therapy for the treatment of panic disorder with agoraphobia.’, cyberpsychology & behavior: The impact of the Internet, multimedia and virtual reality on behavior and society U. S. U. S. 8 (4), 387–393. doi:10.1089/cpb.2005.8.387
Cieślik, B., Mazurek, J., Rutkowski, S., Kiper, P., Turolla, A., and Szczepańska-Gieracha, J. (2020). Virtual reality in psychiatric disorders: A systematic review of reviews. Complementary Ther. Med. 52, 102480. doi:10.1016/j.ctim.2020.102480
Clemmensen, L., Bouchard, S., Rasmussen, J., Holmberg, T. T., Nielsen, J. H., Jepsen, J. R. M., et al. (2020). Study protocol: EXPOSURE in virtual reality for social anxiety DISORDER-a randomized controlled superiority trial comparing cognitive behavioral therapy with virtual reality based exposure to cognitive behavioral therapy with in vivo exposure. BMC PSYCHIATRY 20 (1), 32. doi:10.1186/s12888-020-2453-4
Coelho, C. M., Santos, J. A., Silvério, J., and Silva, C. F. (2006). Virtual reality and acrophobia: One-year follow-up and case study. ’, Cyberpsychol Behav. U. S. 9, 336–341. doi:10.1089/cpb.2006.9.336
Cote, S., and Bouchard, S. (2005). Documenting the efficacy of virtual reality exposure with psychophysiological and information processing measures. Appl. Psychophysiol. biofeedback. Ger. 30 (3), 217–232. doi:10.1007/s10484-005-6379-x
Craske, M. G. (2022). Optimizing exposure therapy with an inhibitory retrieval approach and the OptEx nexus’, behaviour research and therapy. Amsterdam, Netherlands: Elsevier Ltd. doi:10.1016/j.brat.2022.104069
Cummings, J. J., and Bailenson, J. N. (2016). How immersive is enough ? A meta-analysis of the effect of immersive technology on user presence how immersive is enough. Media Psycology 19, 3269. doi:10.1080/15213269.2015.1015740
de Quervain, D. J.-F., Bentz, D., Michael, T., Bolt, O. C., Wiederhold, B. K., Margraf, J., et al. (2011). Glucocorticoids enhance extinction-based psychotherapy. Proc. Natl. Acad. Sci. United States of America. U. S. 108 (16), 6621–6625. doi:10.1073/pnas.1018214108
Diemer, J., Mühlberger, A., Pauli, P., and Zwanzger, P. (2014). Virtual reality exposure in anxiety disorders: Impact on psychophysiological reactivity. World J. Biol. Psychiatry 15 (6), 427–442. doi:10.3109/15622975.2014.892632
Diemer, J. (2015). The impact of perception and presence on emotional reactions: A review of research in virtual reality. Front. Psychol. 6, 26. doi:10.3389/fpsyg.2015.00026
Dilgul, M., Hickling, L. M., Antonie, D., Priebe, S., and Bird, V. J. (2021). Virtual reality group therapy for the treatment of depression: A qualitative study on stakeholder perspectives. Front. Virtual Real. 1, 1–14. doi:10.3389/frvir.2020.609545
Emmelkamp, P. M. G., Meyerbröker, K., and Morina, N. (2020). Virtual reality therapy in social anxiety disorder’, current psychiatry reports. Curr. Psychiatry Rep. 22 (7), 32. doi:10.1007/s11920-020-01156-1
Farrell, L. J., Miyamoto, T., Donovan, C. L., Waters, A. M., Krisch, K. A., and Ollendick, T. H. (2021). Virtual reality one-session treatment of child-specific phobia of dogs: A controlled, multiple baseline case series’, behavior therapy. Elsevier Ltd. 52 (2), 478–491. doi:10.1016/j.beth.2020.06.003
Felton, W. M., and Jackson, R. E. (2022). Presence: A review’, international Journal of human-computer interaction. Taylor Francis 38 (1), 1–18. doi:10.1080/10447318.2021.1921368
Foa, E. B., and McLean, C. P. (2016). The efficacy of exposure therapy for anxiety-related disorders and its underlying mechanisms: The case of OCD and PTSD. Annu. Rev. Clin. Psychol. 12, 1–28. doi:10.1146/annurev-clinpsy-021815-093533
Freeman, D., Reeve, S., Robinson, A., Ehlers, A., Clark, D., Spanlang, B., et al. (2017). Virtual reality in the assessment, understanding, and treatment of mental health disorders. Psychol. Med. 47 (14), 2393–2400. doi:10.1017/S003329171700040X
Geraets, C. N. W., Veling, W., Witlox, M., Staring, A. B., Matthijssen, S. J., and Cath, D. (2019). Virtual reality-based cognitive behavioural therapy for patients with generalized social anxiety disorder: A pilot study. Behav. COGNITIVE PSYCHOTHERAPY 47 (6), 745–750. doi:10.1017/S1352465819000225
Gorini, A., Capideville, C. S., De Leo, G., Mantovani, F., and Riva, G. (2011). The role of immersion and narrative in mediated presence: The virtual hospital experience’, cyberpsychology, behavior, and social networking. Mary Ann. Liebert Inc. 14 (3), 99–105. doi:10.1089/cyber.2010.0100
Graske, M. G., and Barlow, D. H. (2008). “Panic disorder and agoraphobia,” in Clin handb psychol disord. Editor D. H. Barlow (New York: The Guilford Press), 1–65.
Grassini, S., and Laumann, K. (2020). Questionnaire measures and physiological correlates of presence: A systematic review. Front. Psychol. 11, 349. doi:10.3389/fpsyg.2020.00349
Grassini, S., Laumann, K., and Rasmussen Skogstad, M. (2020). The use of virtual reality alone does not promote training performance (but sense of presence does). Front. Psychol. 11, 1743. doi:10.3389/fpsyg.2020.01743
Guidi, J., Brakemeier, E. L., Bockting, C., Cosci, F., Cuijpers, P., Jarrett, R., et al. (2018). Methodological recommendations for trials of psychological interventions. Psychotherapy Psychosomatics 87 (5), 276–284. doi:10.1159/000490574
Gujjar, K. R., Sharma, R., and De Jongh, A. (2017). Virtual reality exposure therapy for treatment of dental phobia. Dent. Update 44 (5), 423–435. doi:10.12968/denu.2017.44.5.423
Gujjar, K. R., van Wijk, A., Kumar, R., and de Jongh, A. (2019). Efficacy of virtual reality exposure therapy for the treatment of dental phobia in adults: A randomized controlled trial. J. ANXIETY Disord. 62, 100–108. doi:10.1016/j.janxdis.2018.12.001
Gujjar, K. R., van Wijk, A., Sharma, R., and de Jongh, A. (2018). Virtual reality exposure therapy for the treatment of dental phobia: A controlled feasibility study’, Behavioural and cognitive psychotherapy. U. S. 46 (3), 367–373. doi:10.1017/S1352465817000534
Hartanto, D. (2016). “Home-based virtual reality exposure therapy with virtual health agent support,” in Pervasive computing paradigms for mental health (mindcare 2015). (Communications in computer and information science). Editors S. Serino, A. Matic, D. Giakoumis, G. Lopez, and P. Cipresso (Berlin, Germany: Springer), 85–98. doi:10.1007/978-3-319-32270-4\_9
Herbelin, B. (2006). Virtual reality as a therapeutic tool in the confines of social anxiety disorder treatment. Int. J. Disabil. Hum. Dev. 5 (3), 243–250. doi:10.1515/IJDHD.2006.5.3.243
Jeong, H. S., Lee, J. H., Kim, H. E., and Kim, J. J. (2021). Appropriate number of treatment sessions in virtual reality-based individual cognitive behavioral therapy for social anxiety disorder. J. Clin. Med. 10 (5), 915. doi:10.3390/jcm10050915
Jiang, M. Y. W., Upton, E., and Newby, J. M. (2020). A randomised wait-list controlled pilot trial of one-session virtual reality exposure therapy for blood-injection-injury phobias. J. Affect. Disord. 276, 636–645. doi:10.1016/j.jad.2020.07.076
Jones, M. B., Kennedy, R. S., and Stanney, K. M. (2004). Toward systematic control of cybersickness. Presence Teleoperators Virtual Environ. 13 (5), 589–600. doi:10.1162/1054746042545247
Kampmann, I. L., Emmelkamp, P. M., Hartanto, D., Brinkman, W. P., Zijlstra, B. J., and Morina, N. (2016). Exposure to virtual social interactions in the treatment of social anxiety disorder: A randomized controlled trialBehav. Res. Ther., 77. England, 147 -156 doi:10.1016/j.brat.2015.12.016
Kessler, R. C., Chiu, W. T., Demler, O., and Walters, E. E. (2005). Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the national comorbidity survey replication. Archives General Psychiatry 62 (6), 617–627. doi:10.1001/archpsyc.62.6.617
Kessler, R. C., Petukhova, M., Sampson, N. A., Zaslavsky, A. M., and Wittchen, H. U. (2012). Twelve-month and lifetime prevalence and lifetime morbid risk of anxiety and mood disorders in the United States. Int. J. Methods Psychiatr. Res. 21, 169–184. doi:10.1002/mpr.1359
Kim, H. J., Lee, S., Jung, D., Hur, J. W., Lee, H. J., Lee, S., et al. (2020). Effectiveness of a participatory and interactive virtual reality intervention in patients with social anxiety disorder: Longitudinal questionnaire study. J. Med. Internet Res. 22 (10). doi:10.2196/23024
Krijn, M., Emmelkamp, P. M. G., Ólafsson, R., Schuemie, M. J., and Van Der Mast, C. A. (2007). Do self-statements enhance the effectiveness of virtual reality exposure therapy? A comparative evaluation in acrophobia.’, cyberpsychology & behavior: The impact of the Internet, multimedia and virtual reality on behavior and society U. S. 10 (3), 362–370. doi:10.1089/cpb.2006.9943
Krijn, M., Emmelkamp, P. M., Biemond, R., de Wilde de Ligny, C., Schuemie, M. J., and van der Mast, C. A. (2004). Treatment of acrophobia in virtual reality: The role of immersion and presence.’, Behaviour research and therapy England 42 (2), 229–239. doi:10.1016/S0005-7967(03)00139-6
Lindner, P., Miloff, A., Bergman, C., Andersson, G., Hamilton, W., and Carlbring, P. (2020). Gamified, automated virtual reality exposure therapy for fear of spiders: A single-subject trial under simulated real-world conditions. Front. PSYCHIATRY 11, 116. doi:10.3389/fpsyt.2020.00116
Lindner, P., Miloff, A., Fagernäs, S., Andersen, J., Sigeman, M., Andersson, G., et al. (2019) ‘Therapist-led and self-led one-session virtual reality exposure therapy for public speaking anxiety with consumer hardware and software: A randomized controlled trial’, J. Anxiety Disord., 61, 45–54. doi:10.1016/j.janxdis.2018.07.003
Ling, Y., Nefs, H. T., Morina, N., Heynderickx, I., and Brinkman, W. P. (2014). A meta-analysis on the relationship between self-reported presence and anxiety in virtual reality exposure therapy for anxiety disorders. PloS One. U. S. 9 (5), e96144. doi:10.1371/journal.pone.0096144
Lombard, M., and Ditton, T. (1997). At the heart of it all: The concept of presence. J. Computer-Mediated Commun. 3 (2), 0. doi:10.1111/j.1083-6101.1997.tb00072.x
Lombard, M. (2015). Immersed in media: Telepresence theory. Berlin, Germany: Springer. doi:10.1007/978-3-319-10190-3
Lundin, J. (2021). Using 360-degree videos for virtual reality exposure in CBT for panic disorder with agoraphobia: A feasibility study. Behav. Cognitive Psychotherapy 22, 1–13. doi:10.1017/S1352465821000473
Makransky, G., Terkildsen, T. S., and Mayer, R. E. (2019). Adding immersive virtual reality to a science lab simulation causes more presence but less learning. Learn. Instr. 60, 225–236. doi:10.1016/j.learninstruc.2017.12.007
Malbos, E., Burgess, G. H., and Lancon, C. (2020). Virtual reality and fear of shark attack: A case study for the treatment of squalophobia. Clin. CASE Stud. 19 (5), 339–354. doi:10.1177/1534650120940014
Malbos, E., Rapee, R. M., and Kavakli, M. (2013). A controlled study of agoraphobia and the independent effect of virtual reality exposure therapy. Aust. N. Z. J. Psychiatry 47 (2), 160–168. doi:10.1177/0004867412453626
Meehan, M. (2003). “Effect of latency on presence in stressful virtual environments,” in Proceedings - IEEE Virtual Reality, Los Angeles, CA, USA, 22-26 March 2003, 141–148. doi:10.1109/VR.2003.1191132
Meehan, M., Insko, B., Whitton, M., and Brooks, F. P. (2002). Physiological measures of presence in stressful virtual environments. ACM Trans. Graph. 21 (3), 645–652. doi:10.1145/566654.566630
Meindl, J. N., Saba, S., Gray, M., Stuebing, L., and Jarvis, A. (2019). Reducing blood draw phobia in an adult with autism spectrum disorder using low-cost virtual reality exposure therapy. J. Appl. Res. Intellect. Disabil. 32 (6), 1446–1452. doi:10.1111/jar.12637
Meyerbroeker, K., Morina, N., Kerkhof, G., and Emmelkamp, P. (2013). Virtual reality exposure therapy does not provide any additional value in agoraphobic patients: A randomized controlled trial. Psychotherapy psychosomatics. Switz. 82 (3), 170–176. doi:10.1159/000342715
Meyerbroeker, K., Powers, M. B., van Stegeren, A., and Emmelkamp, P. M. (2012). Does yohimbine hydrochloride facilitate fear extinction in virtual reality treatment of fear of flying? A randomized placebo-controlled trial. Psychotherapy psychosomatics 81 (1), 29–37. doi:10.1159/000329454
Meyerbröker, K., Morina, N., and Emmelkamp, P. M. G. (2018). Enhancement of exposure therapy in participants with specific phobia: A randomized controlled trial comparing yohimbine, propranolol and placebo. J. Anxiety Disord. 57, 48–56. doi:10.1016/j.janxdis.2018.05.001
Meyerbröker, K., Morina, N., Kerkhof, G., and Emmelkamp, P. M. G. (2011). Virtual reality exposure treatment of agoraphobia: A comparison of computer automatic virtual environment and head-mounted display. Stud. health Technol. Inf. 167, 51–56.
Michaliszyn, D., Marchand, A., Bouchard, S., Martel, M. O., and Poirier-Bisson, J. (2010). A randomized, controlled clinical trial of in virtuo and in vivo exposure for spider phobia.’, Cyberpsychology, behavior and social networking\ U. S. 13 (6), 689–695. doi:10.1089/cyber.2009.0277
Miloff, A. (2019) ‘Automated virtual reality exposure therapy for spider phobia vs. in-vivo one-session treatment: A randomized non-inferiority trial’, Behav. Res. Ther., 118, 130–140. doi:10.1016/j.brat.2019.04.004
Moldovan, R., and David, D. (2014). One session treatmet of cognitive and behavioral therapy and virtual reality for social and specific phobias. Preliminary results from a randomized clinical trial. J. Cognitive Behav. Psychotherapies 14 (1), 67–83.
Morina, N. (2015). Can virtual reality exposure therapy gains be generalized to real-life? A meta-analysis of studies applying behavioral assessments. Behav. Res. Ther. 74, 18. doi:10.1016/j.brat.2015.08.010
Morina, N. (2021). Meta-analysis of virtual reality exposure therapy for social anxiety disorder. Psychol. Med. 53, 1–3. doi:10.1017/S0033291721001690
National Institute for Health and Care Excellence (2011a). Common mental health problems: Identification and pathways to care (CG123). Available at: https://www.nice.org.uk/terms-and-.
National Institute for Health and Care Excellence (2011b). Generalised anxiety disorder and panic disorder in adults: Management. United kingdom: National Institute for Health and Clinical Excellence.
National Institute for Health and Care Excellence (2013). NICE guidelines: Social anxiety disorder: Assessment and treatment. United kingdom: National Institute for Health and Care Excellence. doi:10.1002/9781118775349.ch47
Nazligul, M. D. (2017). Overcoming public speaking anxiety of software engineers using virtual reality exposure therapy, 191–202. doi:10.1007/978-3-319-64218-5
Neudeck, P., and Einsle, F. (2012). “Dissemination of exposure therapy in clinical practice: How to handle the barriers?,” in Exposure therapy rethinking the model - refining the method. Editors P. Neudeck, and H. U. Wittchen (London: Springer), 23–34.
Olatunji, B. O., Deacon, B. J., and Abramowitz, J. S. (2009). The cruelest cure? Ethical issues in the implementation of exposure-based treatments’, Cognitive and behavioral practice. Elsevier B.V. 16 (2), 172–180. doi:10.1016/j.cbpra.2008.07.003
Öst, L.-G. (2012). “One-session treatment: Principles and procedures with adults,” in Intensive one-session treatment of specific phobias. Editors T. E. DavisIII, L.-G. Öst, and T. H. Ollendick (Berlin, Germany: Springer), 59–97. doi:10.1007/978-1-4614-3253-1
Pelissolo, A. (2012). Virtual reality exposure therapy versus cognitive behavior therapy for panic disorder with agoraphobia: A randomized comparison study.’, Journal of Cybertherapy and rehabilitation. Pelissolo, antoine: Service de Psychiatrie adulte, hopital pitie-salpetrieie, paris, France, 75651, cedex 13,YW50b2luZS5wZWxpc3NvbG9AdXBtYy5mcg==Virtual Real. Med. Inst. BVBA 5 (1), 35–43.
,+antoine.pelissolo@upmc.fr&btnG=">Google Scholar
Peperkorn, H. M., Diemer, J. E., Alpers, G. W., and Mühlberger, A. (2016)., 7. Switzerland, 268. doi:10.3389/fpsyg.2016.00268Representation of patients’ hand modulates fear reactions of patients with spider phobia in virtual realityFront. Psychol.
Peperkorn, H. M., Diemer, J., and Mühlberger, A. (2015). Temporal dynamics in the relation between presence and fear in virtual reality. Comput. Hum. Behav. 48, 542–547. doi:10.1016/j.chb.2015.02.028
Pérez-Ara, M. A., Quero, S., Botella, C., Baños, R., Andreu-Mateu, S., García-Palacios, A., et al. (2010). Virtual reality interoceptive exposure for the treatment of panic disorder and agoraphobia. Stud. Health Technol. Inf. 154, 77–81. PG-77-81). doi:10.3233/978-1-60750-561-7-77
Pham, M. T., Rajić, A., Greig, J. D., Sargeant, J. M., Papadopoulos, A., and McEwen, S. A. (2014). A scoping review of scoping reviews: Advancing the approach and enhancing the consistency. Res. Synthesis Methods 5 (4), 371–385. doi:10.1002/jrsm.1123
Pittig, A., Kotter, R., and Hoyer, J. (2019). The struggle of behavioral therapists with exposure: Self-reported practicability, negative beliefs, and therapist distress about exposure-based interventions’, behavior therapy. Elsevier Ltd. 50 (2), 353–366. doi:10.1016/j.beth.2018.07.003
Pot-Kolder, R. M. C. A. C. A., Geraets, C. N. W., Veling, W., van Beilen, M., Staring, A. B. P., Gijsman, H. J., et al. (2018). Virtual-reality-based cognitive behavioural therapy versus waiting list control for paranoid ideation and social avoidance in patients with psychotic disorders: A single-blind randomised controlled trial. Lancet Psychiatry 5 (3), 217–226. doi:10.1016/S2215-0366(18)30053-1
Price, M., and Anderson, P. (2007). The role of presence in virtual reality exposure therapy. J. anxiety Disord. 21 (5), 742–751. doi:10.1016/j.janxdis.2006.11.002
Price, M., Mehta, N., Tone, E. B., and Anderson, P. L. (2011). Does engagement with exposure yield better outcomes? Components of presence as a predictor of treatment response for virtual reality exposure therapy for social phobia. J. anxiety Disord. 25 (6), 763–770. doi:10.1016/j.janxdis.2011.03.004
Reitmaier, J., Schiller, A., Mühlberger, A., Pfaller, M., Meyer, M., and Shiban, Y. (2022). Effects of rhythmic eye movements during a virtual reality exposure paradigm for spider-phobic patients. Psychol. Psychotherapy Theory, Res. Pract. 95 (1), 57–78. doi:10.1111/papt.12363
Rothbaum, B. O., Anderson, P., Zimand, E., Hodges, L., Lang, D., and Wilson, J. (2006). Virtual reality exposure therapy and standard (in vivo) exposure therapy in the treatment of fear of flying. Behav. Ther. 37 (1), 80–90. doi:10.1016/j.beth.2005.04.004
Rus-Calafell, M., Gutiérrez-Maldonado, J., Botella, C., and Baños, R. M. (2013). Virtual reality exposure and imaginal exposure in the treatment of fear of flying: A pilot study. Behav. Modif. 37 (4), 568–590. doi:10.1177/0145445513482969
Saredakis, D., Szpak, A., Birckhead, B., Keage, H. A. D., Rizzo, A., and Loetscher, T. (2020). Factors associated with virtual reality sickness in head-mounted displays: A systematic review and meta-analysis. Front. Hum. Neurosci. 14, 96. doi:10.3389/fnhum.2020.00096
Servera, M., Saez, B., and Mir, J. M. G. (2020). Feasibility of a virtual reality program to treat children with fear of darkness with nonexpert therapists. Rev. De. Psicol. Clin. CON NINOS Y Adolesc. 7 (2), 16–21. doi:10.21134/rpcna.2020.07.2.2
Shin, B., Oh, J., Kim, B. H., Kim, H. E., Kim, H., Kim, S., et al. (2021). Effectiveness of self-guided virtual reality-based cognitive behavioral therapy for panic disorder: Randomized controlled trial. JMIR Ment. Health 8 (11). doi:10.2196/30590
Slater, M. (2018). Immersion and the illusion of presence in virtual reality. Br. J. Psychol. 109 (3), 431–433. doi:10.1111/bjop.12305
Stein, D. J., Lim, C. C. W., Roest, A. M., de Jonge, P., Aguilar-Gaxiola, S., Al-Hamzawi, A., et al. (2017). The cross-national epidemiology of social anxiety disorder: Data from the world mental health survey initiative’, BMC medicine. BMC Med. 15 (1), 143–221. doi:10.1186/s12916-017-0889-2
Sundhedsstyrelsen, (2016). National klinisk retningslinje for behandling af angst hos børn og unge. Available at: https://www.sst.dk/da/udgivelser/2016/∼/media/7637E5A2ED0746FBA1E45245F8C1E430.ashx.
Sylaiou, S. (2010). Exploring the relationship between presence and enjoyment in a virtual museum. Int. J. Hum. Comput. Stud. 68 (5), 243–253. doi:10.1016/j.ijhcs.2009.11.002
Tortella-Feliu, M., Botella, C., Llabrés, J., Bretón-López, J. M., del Amo, A. R., Baños, R. M., et al. (2011). Virtual reality versus computer-aided exposure treatments for fear of flying.’, Behavior modification U. S. 35 (1), 3–30. doi:10.1177/0145445510390801
Trahan, M. H., Morley, R. H., Nason, E. E., Rodrigues, N., Huerta, L., and Metsis, V. (2021). Virtual reality exposure simulation for student veteran social anxiety and ptsd: A case study. Clin. Soc. WORK J. 49, 220–230. doi:10.1007/s10615-020-00784-7
Turk, C. L., Heimberg, R. G., and Magee, L. (2008). “Social anxiety disorder,” in Clin handb psychol disord a step-by-step treat man. Editor D. H. Barlow (London: Guilford Press), 123–163.
Veritas Health Innovation, (2022). Covidence systematic review software. Available at: www.covidence.org.
Wallach, H. S., Safir, M. P., and Bar-Zvi, M. (2011). Virtual reality exposure versus cognitive restructuring for treatment of public speaking anxiety: A pilot study. ISRAEL J. PSYCHIATRY Relat. Sci. 48 (2), 91–97.
Wang, P. S., Lane, M., Olfson, M., Pincus, H. A., Wells, K. B., and Kessler, R. C. (2005). Twelve-Month use of mental health services in the United States. Archives General Psychiatry 62 (6), 629. doi:10.1001/archpsyc.62.6.629
Wechsler, T. F., Mühlberger, A., and Kümpers, F. (2019). Inferiority or even superiority of virtual reality exposure therapy in phobias? - a systematic review and quantitative meta-analysis on randomized controlled trials specifically comparing the efficacy of virtual reality exposure to gold standard in vivo e. Front. Psychol. 10, 1758. doi:10.3389/fpsyg.2019.01758
Whitney, S. L. (2005) ‘Acrophobia and pathological height vertigo: Indications for vestibular physical therapy?’, Phys. Ther., 85, 443–458. doi:10.1093/ptj/85.5.443
Keywords: virtual reality exposure therapy, social anxiety disorder, agoraphobia, specific phobia, virtual reality technology, scoping review
Citation: Arnfred B, Svendsen JK, Adjourlu A and Horthøj C (2023) Scoping review of the hardware and software features of virtual reality exposure therapy for social anxiety disorder, agoraphobia, and specific phobia. Front. Virtual Real. 4:952741. doi: 10.3389/frvir.2023.952741
Received: 25 May 2022; Accepted: 08 May 2023;
Published: 06 June 2023.
Edited by:
Hai-Ning Liang, Xi’an Jiaotong-Liverpool University, ChinaReviewed by:
Asle Hoffart, Modum Bad Psychiatric Center, NorwayTomasz Kupka, Polish Dental Association, Poland
Copyright © 2023 Arnfred, Svendsen, Adjourlu and Horthøj. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Benjamin Arnfred, YmVuamFtaW4uYWxleGFuZGVyLnRob3J1cC5hcm5mcmVkQHJlZ2lvbmguZGs=