
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Virtual Real., 12 May 2023
Sec. Technologies for VR
Volume 4 - 2023 | https://doi.org/10.3389/frvir.2023.1059278
 Chen Li*Pui Yin Yip
Chen Li*Pui Yin YipMotivated by the unique experience of creating three-dimensional artworks in virtual reality (VR) and the need for teletherapy due to the global pandemic, we conducted this pilot case study to explore the feasibility and effectiveness of using a custom-designed collaborative virtual environment (CVE) to enable remote arts therapy. Three participants (two females and one male) experiencing moderate to high stress as measured by the Perceived Stress Scale (PSS) joined this study. Each participant had eight 45-minute one-on-one sessions with the therapist for eight consecutive weeks. These eight sessions covered eight art creation themes and were delivered following pre-designed protocols. The CVE was the only medium to facilitate the sessions, during which the therapist and the participants were physically separated into two rooms. The quantitative and qualitative results suggested that the CVE-enabled approach was generally feasible and was welcomed by both the participants and the therapist. However, more evidence of the approach’s effectiveness in enhancing the participants’ mental wellbeing is needed because the results of the pilot case study were affected by the pandemic. The advantages and disadvantages of this approach and the CVE were investigated from practicality and technological affordance perspectives. Potential improvements to the CVE are also proposed to better facilitate the practice of remote arts therapy in CVE. We encourage future studies to cautiously investigate CVE-enabled remote arts therapy in clinical settings and collect more evidence regarding its effectiveness in addressing clinically diagnosed mental disorders and other complications.
Arts therapy is a term that umbrellas the psychotherapeutic use of various art forms (e.g., painting, music, dance, drama, etc.) by therapists to improve clients’ psychological wellbeing (Malchiodi, 2011; Zubala et al., 2021). The practice of arts therapy is mainly based on the idea that creative processing can facilitate the non-verbal communication of feelings and thoughts (Malchiodi, 2011). Under the umbrella of arts therapy, psychoeducational, humanistic, and systemic approaches are commonly employed in practice (Malchiodi, 2011; Rubin, 2012). Although technology-assisted psychotherapy practices are getting increasingly popular, there are some concerns about the practice of arts therapy purely in the technology-assisted format (Robledo Yamamoto et al., 2021). Among these concerns, the most prominent one is the challenge of translating and maintaining the unique triangular therapeutic relationship between the therapist, the client, and the artworks in the digital world, which could be crucial to the success of arts therapy (Gussak and Rosal, 2015).
Motivated by the unique experience of creating three-dimensional artworks in virtual reality (VR), a few pilot studies have been conducted to investigate the feasibility of using off-the-shelf VR applications to enable arts therapy. For example, Haeyen et al. (2021) invited five art therapists and two psychomotor therapists to experiment with Tilt Brush1 in their clinical practice. Kaimal et al. (2020) conducted a similar study to collect qualitative feedback from participants with more diverse backgrounds outside the clinical setting regarding the use of Tilt Brush1 and Kodon2 for art making. In both studies, the VR applications were considered as a promising medium for enabling arts therapy and were generally welcomed by the participants. However, because these off-the-shelf VR applications were designed to provide single-user experiences, therapists could only observe the art creation process on computer monitors without actual participation. Hence, it is unclear whether the unique triangular therapeutic relationship could be facilitated. It is also largely unknown how the therapeutic approaches should be adapted when such a new medium is used to enable arts therapy.
This paper reports a pilot case study that aimed to explore the feasibility and effectiveness of using a custom-designed collaborative virtual environment (CVE) to enable remote arts therapy. To address the most prominent concern of practising remote arts therapy, the CVE was designed to translate and maintain the triangular therapeutic relationship between the therapist, the client, and the artworks in the purely virtual space, so that the conventional therapeutic approaches could be easily practised remotely with minimal adaptation. Instead of tackling mental disorders in the clinical setting, which might lead to ethical concerns over using this utterly new approach, this study focused on improving youth’s mental wellbeing and reducing perceived stress. Compared to previous studies on using VR for enabling arts therapy, this pilot case study significantly contributes to this area of research in the following aspects. First, this study pioneers the use of CVE to deliver remote arts therapy following pre-designed protocols, which aligned with well-defined psychotherapeutic objectives; During all psychotherapeutic sessions, the participants and the therapist were always separated physically, and they could only communicate in the virtual space via self-avatars. As far as we know, this approach had never been employed in prior studies. Second, the mixed-methods approach helped us collect both quantitative and qualitative evidence on the feasibility and effectiveness; Our findings suggested that using CVE to enable remote arts therapy was generally feasible and was welcomed by both the participants and the therapist. However, more evidence of the approach’s effectiveness in enhancing the participants’ mental wellbeing is needed in future studies because the results of the pilot case study were affected by the pandemic. Finally, based on the feedback from the participants and the therapist, the advantages and disadvantages of our approach are discussed here from the perspectives of practicality and technological affordance. The discussion leads to potential improvements to the CVE that can better facilitate the practice of remote arts therapy in CVE.
CVE is a networked environment in which multiple users share the same set of virtual scenes and virtual worlds and participate in collaborative tasks or simply socialising via their own enabling devices, such as Head-mounted Displays (HMDs) (Benford et al., 2001). Compared to conventional means of technology-enabled communication, CVE can induce a better sense of copresence [i.e., the sense of being there with someone else (Biocca et al., 2003)], because it can offer a wide set of verbal and non-verbal social cues with high fidelity and immersion (Short et al., 1976; Biocca and Levy, 2013; Jung et al., 2021). Prior studies have demonstrated the importance of non-verbal social cues in interpersonal communication (Riggio and Friedman, 1986; Slater and Steed, 2002; Won et al., 2014). In CVEs, non-verbal social cues are commonly presented as gestures and facial expressions of avatars that are driven by users’ gestures and facial expressions in the physical world. These non-verbal social cues have been found to affect the perception of social experiences in CVEs. For example, Slater and Steed found that participants who received negative non-verbal feedback from their interaction partners in the CVE experienced higher levels of anxiety compared to those who received positive or neutral non-verbal feedback (Slater and Steed, 2002). Moreover, Herrera et al. found that the behavioural realism of avatars afforded to users in the CVE could also affect their non-verbal behaviours in the physical world (Herrera et al., 2020).
The CVE’s ability to offer a wide set of verbal and non-verbal social cues during avatar-mediated communications makes it a promising medium to deliver psychotherapeutic sessions remotely; besides connecting therapists and clients who might be in different physical locations, the medium can support social interactions that are close to the face-to-face experience while keeping the privacy of clients protected if they desire to do so. As the global pandemic stays, there is an increasing interest and demand in using CVE to deliver psychotherapy remotely and connect therapists with clients during this challenging time. For example, in a pilot study, Gumilar et al. (2021) designed a CVE for online counselling. The study found that non-verbal social cues (e.g., eye gazes) represented in the CVE could affect the feeling of connectedness as suggested by the participants’ neural activities collected during social interactions in the CVE. However, the feasibility and effectiveness of practising psychotherapy in CVEs are still underexplored and need to be further investigated.
The term VR was first coined in the 1980s by Jaron Lanier to describe a computer-generated virtual world. Since then, the scope of the term has been greatly expanded, covering both the enabling technologies and the human experience. Steuer suggested that “the key to defining VR in terms of human experience rather than technological hardware is the concept of presence” (p. 75) and defining VR solely by the technological capabilities was lacking in providing insights on the processes or effects of using VR (Steuer, 1992). The concept of presence, which might be interpreted slightly differently in various contexts but shares the similar idea of the sense of being there, is now widely regarded as the desired design outcome of VR experiences, thus a metric for measuring the quality of the experiences (Skarbez et al., 2017; Slater et al., 2022). Slater further developed the concept of presence by introducing place illusion (PI) and plausibility illusion (Psi) (Slater, 2009); The former was defined as “the qualia of having a sensation of being in a real place” (p. 3549)—A similar concept to the sense of being there and the latter referred to “the illusion that the scenario being depicted is actually occurring” (p. 3549). Slater also suggested that PI and Psi could lead to the participants’ realistic behaviours in virtual environments (Slater, 2009).
The aforementioned perceptual illusions during VR exposure and their potential impacts on human behaviours had inspired and supported the practice of psychotherapy in VR; Prior studies have provided strong evidence regarding the effectiveness of VR in the treatment of anxiety disorders (Opriş et al., 2012; Dellazizzo et al., 2020), depression (Fodor et al., 2018), and posttraumatic stress disorder (PTSD) (Deng et al., 2019). The most common psychotherapeutic approach that has been practised in VR is cognitive behavioural therapy (CBT)—A talking therapy that can help manage mental disorders by changing the way patients think and thus behave. VR environments are highly controllable and safe but also interactive and realistic, which can reduce the reliance on imaginative and abstract thinking skills during CBT (Scozzari and Gamberini, 2011).
In contrast, the experiment of arts therapy in VR has just started recently with off-the-shelf VR applications. For example, Haeyen et al. (2021) invited five art therapists and two psychomotor therapists to experiment with Tilt Brush1 in their clinical practice using the Lean Startup Method. The qualitative results showed that the therapists viewed Tilt Brush1 as an application with much potential in the clinical practice. The study also suggested that existing methodologies might need to be adapted for practising arts therapy in VR (Kaimal et al., 2020). Conducted a similar study to collect qualitative feedback from participants with more diverse backgrounds outside the clinical setting regarding the use of Tilt Brush1 and Kodon2 for art making. The results suggested that the medium had its uniqueness that could be more engaging and attractive than conventional media for art making; also, VR-enabled arts therapy could be more helpful for certain groups of participants (e.g., participants in the immune-compromised environment and participants with deficits in fine motor control). However, the authors also adverted that the off-the-shelf applications they tested did not allow multiple individuals to be in the same virtual space simultaneously, limiting the therapists’ viewing and interpretation of the artworks and communications with the clients. To address such limitations might need to either adapt existing psychotherapeutic methodologies significantly, as suggested by Haeyen et al. (2021), or transform existing single-user VR applications into multi-user CVEs so that the unique triangular therapeutic relationship between the therapist, the client, and the artworks could be translated and maintained.
To fill the knowledge gaps, this pilot trial study was scoped to investigate two important research questions by using a custom-designed CVE for remote arts therapy. The first research question is whether the CVE-enabled approach is feasible, given the concern about translating and maintaining the triangular relationship between the therapist, the client, and the artworks in the virtual world (Gussak and Rosal, 2015). Previous studies [e.g., (Kaimal et al., 2020; Haeyen et al., 2021)] have never delivered a complete intervention involving multiple psychotherapeutic sessions in a purely digital format. Hence, our pilot case study will be the first to tackle this question regarding the feasibility of VR-enabled arts therapy and, more importantly, CVE-enabled remote arts therapy. The second research question is whether the CVE-enabled approach is effective in enhancing youth’s mental wellbeing and reducing perceived stress. On top of these two research questions, we also investigated the advantages and disadvantages of the custom-designed CVE in delivering remote arts therapy from the perspectives of practicality and technological affordances. Potential improvements to the CVE will also be proposed to better facilitate the practice of remote arts therapy in CVEs.
The study was designed to be a case study that employed the mixed-method approach. Although conducting a case study is very time-consuming, we still chose to do so mainly because of the nature of arts therapy, which tends to be highly personal and expressive (Gussak and Rosal, 2015). This study design allowed us to study each subject more profoundly and reduced the potential of diluting the results due to between-subject differences, such as psychotherapeutic needs and art creation skills and experiences. The mixed-method approach was adopted to help us collect not only quantitative data but also qualitative evidence on the feasibility and effectiveness, which should be as valuable given the pioneering nature of this study.
The protocols of the psychotherapeutic sessions (see Section 4.7) were designed to enhancing the participants’ mental wellbeing and perceived stress. Instead of targeting clinically diagnosed mental disorders, focusing on mental wellbeing and perceived stress could help the results benefit a broader population and address the ethical concerns over conducting clinical trials using an utterly new approach.
The ethics application of this study was approved by the Institutional Review Board of The Hong Kong Polytechnic University. Three participants were recruited for the pilot case study via on-campus flyers. The participants were all experiencing a moderate or high level of stress as measured using the Perceived Stress Scale (PSS) (see Section 4.3.2), but none of them had a clinical diagnosis of mental disorders. The detailed demographics of the three participants are as follows.
• Participant 1– a female participant in her early twenties with no colour vision deficits or epilepsy. The participant had minimal experience with VR and never participated in art creation activities. Before joining any arts therapy sessions, her PSS score was 17, considered moderate perceived stress. She rated her stress level as 3 out of 5. During the phone call with the experimenter (see Section 4.6), she said her stress was mainly due to her study and worrying about her future.
• Participant 2– a female participant in her mid-twenties with no colour vision deficits or epilepsy. The participant had recently joined a VR technologies workshop and sometimes drew during her leisure time. Before joining any arts therapy sessions, her PSS score was 35, considered high perceived stress. She rated her stress level as 3 out of 5. During the phone call, the experimenter knew that her stress was due to challenges in her private life and study.
• Participant 3– a male participant in his mid-twenties with no colour vision deficits or epilepsy. The participant played some VR games before and rarely participated in art creation activities. Before joining any arts therapy sessions, his PSS score was 25, considered moderate perceived stress. He rated his stress level as 4 out of 5. During the phone call with the experimenter, he said his stress mainly came from his professional development, which was quite demanding for him.
The Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS) (Tennant et al., 2007) was used to measure the participants’ mental wellbeing. The scale has 14 positively worded statements covering feeling and functioning aspects of mental wellbeing. Each item is on a 5-point Likert-type scale anchored with “none of the time” (1) and “all the time” (5). The minimum score is 14 and the maximum is 70, with higher scores indicating better mental wellbeing.
The Perceived Stress Scale (PSS) (Cohen et al., 1983) was used to measure the participants’ perceived stress in the most recent month. The scale has ten items on a 5-point Likert-type scale ranging from “never” (0) to “very often” (4). The scores can range from 0 to 40 with higher scores indicating higher perceived stress.
Roger’s Happy/Sad Face Scale (Rogers, 1981) was also used to quickly assess the participants’ mental wellbeing before and after each session so that the longitudinal changes could be observed (see Section 4.6). The pictorial scale can be used to quickly assess mood, anxiety, and pain on a scale of 0–4, indicating no symptoms and worst possible symptoms respectively. The scale is often used as a convenient instrument to assess the outcomes of arts therapy [e.g., (Gallagher and Steele, 2002; Shella, 2018)].
The System Usability Scale (SUS) (Brooke, 1996) was used to measure the usability of our custom-designed CVE. The scale is one of the most widely used instrument to conduct subjective assessments of usability. It has ten items on a 5-point Likert-type scale ranging from “strongly disagree” (1) to “strongly agree” (5).
The same approach adopted in (Nowak and Biocca, 2003) was employed to measure copresence by considering its dual nature. Specifically, 12 items were used to measure the interaction partner’s (i.e., the therapist’s) copresence perceived by the participants and six items were used to measure the participants’ self-reported copresence. Each item is on a 5-point Likert-type scale anchored with “strongly disagree” (1) and “strongly agree” (5).
The CVE we used for this pilot study was designed to afford avatar-mediated communications, including real-time bidirectional voice chat, in addition to collaborative art creations. Regarding avatar-mediated communications in the CVE, the participants and the therapist could use the browser-based interface3 to customise their self-avatars in the CVE (see Figure 1). To avoid the technical complexity and to induce greater copresence as suggested by Herrera et al. (2020), instead of supporting full-body avatars, only half-body avatars with head and hands tracking were presented in the CVE. Regarding functionality related to collaborative art creations, we developed a simple user interface which was inspired by the interface design of Tilt Brush1 (see Figure 2). This simple user interface always followed the position and orientation of the VR controller in the participant’s non-dominant hand. The other controller, the controller in the participant’s dominant hand, could either be used to draw or to interact with the user interface by pointing and pressing the trigger button using the index finger. For example, the participant could pick a colour from the colour palette or a brush style from the pre-defined set by using the controller in his/her dominant hand to point at a desired colour or brush style then press the trigger button. The user interface also supported basic file operations (e.g., save and load) for managing the artworks created in the CVE by following the same interaction logic. The saved files contained all necessary information to replay the entire art creation processes when loaded into the system.

FIGURE 1. The self-avatars used by the participants and the therapist in the CVE.
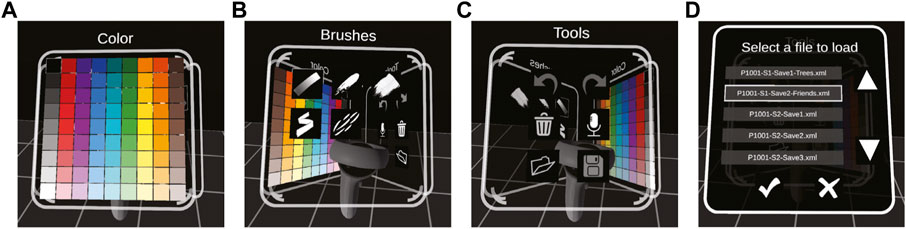
FIGURE 2. The user interface for collaborative arts creation in the CVE. (A) The colour palette; (B) The user interface for picking a brush style; (C) The user interface for using different tools and settings; (D) Basic file operations for managing the artworks.
Regarding the software implementation, the typical client-server software architecture was employed, and the software was developed using Unity4. Photon for Unity (PUN) network framework5 was used to ease the network programming and enable a reliable low-latency voice chat. The avatars’ movements were transported directly via the framework. To bidirectionally synchronise the drawings on both the participant side and the therapist side, the drawing process was decomposed into a series of pre-defined remote procedure calls (RPCs). The RPCs initialised by either of the two clients would be propagated to both clients. This design ensured reliable synchronisations between the two clients and provided the architectural flexibility needed to support more than two clients. The software architecture is illustrated in Figure 3.

FIGURE 3. The client-server architecture enables bidirectional synchronisation of the drawings. The blue lines show that client A requested an RPC to the PUN server, and the server propagates the RPC to all connected clients. The red lines show the same process being initialised by client B The architecture can be easily expanded to support more than two clients.
The ownership of the components of the virtual artworks is maintained during the presence of the participant and the therapist. Specifically, the therapist can only delete or modify those components added to the artworks by herself. The same rule is also applied to the participant. However, if one of the pairs leaves the CVE, the ownership will be transferred to the other, even if the therapist leaves the CVE. In addition, the file operations are designed to be available only to the therapist.
The therapist and the participants were provided two sets of the same hardware to access the CVE. Each set included one HMD with controllers, one desktop computer, and one WiFi router. Although the software was designed to be cross-platform, we chose to use Oculus Quest 2 HMD and its Air Link feature because the wireless connection between the HMD and the computer was highly desirable for safety reasons. The computer was equipped with an Intel Core i7-10700K processor, 32GB RAM, and NVIDIA RTX 3080 graphics card; it was connected to the WiFi router via a wired connection, and the HMD was connected to its router wirelessly, which followed the recommended network configuration for enabling the Air Link feature. We chose to use the HMD in this particular configuration rather than as a standalone device to enhance the overall system stability and ease the experimenter’s observation of the sessions through the computer monitor. The connections are illustrated in Figure 4. The HMD’s built-in microphone and speakers were used to enable the real-time bidirectional voice chat feature of the CVE. During the psychotherapeutic sessions, the therapist and the participant were physically separated into two rooms, and there was one set of the hardware mentioned above in each room. Hence, using the voice chat feature of the CVE was the only way for them to talk to each other (see Figure 5). The therapist’s room was 2 m by 3 m, while the participants enjoyed a larger 4 m by 4 m space in our laboratory. OBS Studio6 was used on the two computers to take screen recordings during each session. The recordings were used by the therapist to take session notes. Regarding the system performance, the headset was constantly working at its 90 Hz maximum refresh rate; The latency of the connection to the PUN server located in Singapore was always below 60 ms during the sessions, according to the software system logs.
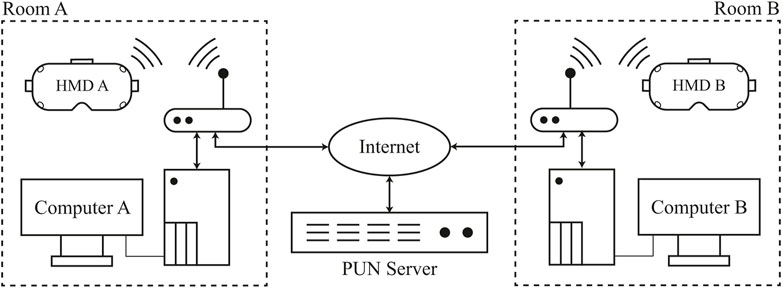
FIGURE 4. The hardware and the system connections for this pilot case study.
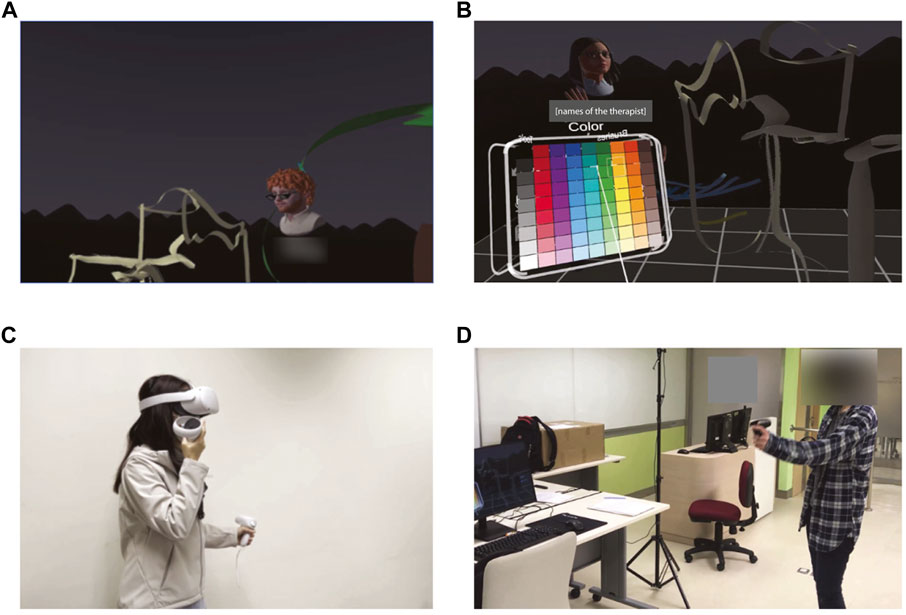
FIGURE 5. The overall setup of the apparatus. (A) The view of the therapist in VR; (B) The view of the participant in VR; (C) The therapist in her room; (D) The participant in our laboratory.
The experimenter first called each recruited participant before he/she joined the first session. During the phone call, he/she was briefed about the study procedure and interviewed to ensure his/her eligibility for participation. The experimenter would also ask about his/her stress level based on the self-rating. The time of the eight consecutive sessions was confirmed with the participant as well.
Upon the participant’s arrival for the first time, he/she was briefed about the procedure of the study again and was asked if he/she had any questions regarding the study. Then, he/she was asked to read the consent carefully and sign the consent. He/she also received the information sheet covering the experiment procedure, safety, privacy disclaims, and contacts of the project team. The pre-assessment, which included PSS and WEMWBS, was administered via a desktop computer in our laboratory. After finishing the pre-assessment, the participant was asked to customise his/her self-avatar in the web browser and choose a name to be displayed alongside the self-avatar in the CVE. The experimenter then demonstrated how to use the enabling software and hardware. The demonstration followed pre-drafted scripts. Specifically, the experimenter first introduced the volume control and sleep button on the HMD and showed the participant how to adjust the straps. The experimenter then showed the use of the two controllers in the CVE and introduced the functions of the user interface. Lastly, the experimenter demonstrated how to take off the HMD; The participant was reminded that if he/she felt uncomfortable using the HMD, he/she should quickly take off the HMD and let the experimenter know, which was covered in the consent and information sheet. When the participant felt ready, he/she was asked to complete Roger’s Happy/Sad Face Scale, after which he/she could formally start the first session with the therapist.
A total of eight sessions were delivered in the CVE to each participant. Every session lasted for around 45 min and covered two or three of the four psychotherapeutic objectives following pre-defined protocols (see Table 1). Upon finishing each of the sessions in the CVE, the participant was asked to complete Roger’s Happy/Sad Face Scale. The experimenter then reminded the participant to avoid driving or operating heavy machinery within 1 hour after the session. If it was the eighth session, the participant was also asked to complete the post-assessment, which included PSS, WEMWBS, SUS, and items for measuring copresence. The post-assessment was also completed on the desktop computer in our laboratory. The semi-structured interview was then conducted with the participant. The semi-structured interview covered three aspects, including 1) the participant’s recent feelings and emotions, 2) thoughts and suggestions towards the CVE and collaborative art creation in the CVE, and 3) his/her relationship with the therapist. Specifically, the experimenter asked the participant six questions in total. The first and second questions were “are there any observable changes in yourself, when compared with the time before joining the sessions?” and “can you describe your feelings about the changes in you?” These two questions were about the participant’s recent feelings and emotions. Next, the experimenter asked the third and fourth questions—“What are your thoughts towards art creation in VR?” and “is there any discovery during the art creation process?” These two questions aimed to collect the participant’s thoughts and suggestions towards the CVE and collaborative art creation in the CVE. The experimenter then moved on to the question about the participant’s relationship with the therapist by asking “can you describe your feeling towards the therapist and the relationship between you two?” For the first five questions, the experimenter may ask the participant to further elaborate his/her answers by asking additional follow-up questions. Finally, the experimenter asked the last open-ended question about his/her thoughts and suggestions about the entire experience. The semi-structured interview lasted between 15 and 20 min. After the interview, the participant was told that the study had been completed. Supermarket coupons worth HK$400 (equivalent to US$51.1) were given to the participant to thank him/her for the participation. The procedures of all eight sessions are summarised in Figure 6.
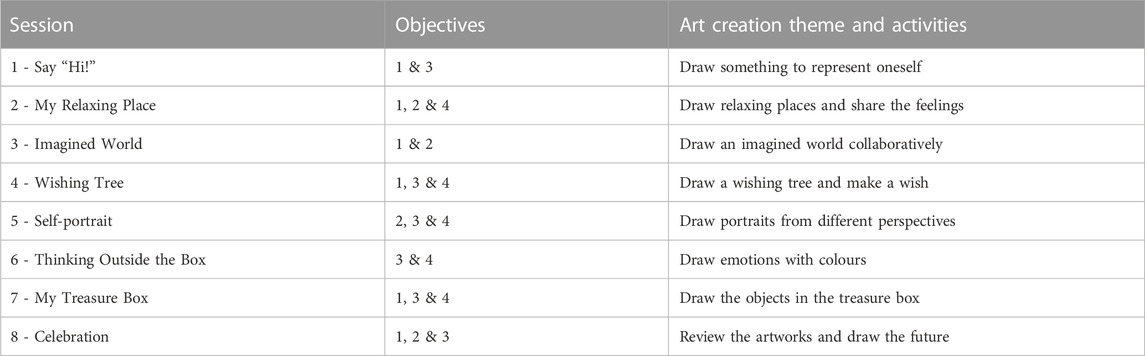
TABLE 1. The objectives and the art creation themes and activities of the eight sessions.
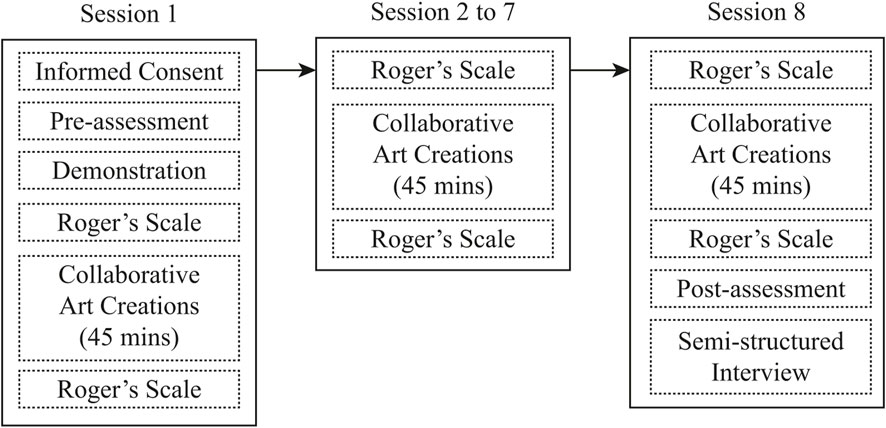
FIGURE 6. The procedures of the entire study.
The protocols of the sessions were designed with clear objectives to enhance the participants’ mental wellbeing and reduce their perceived stress. Specifically, the objectives were 1) to build a trusting relationship with the therapist and to provide a channel for the participants to express themselves, 2) to foster a caring, safe, and supportive space for personal growth and exploration, 3) to enhance self-awareness and recap the positive inner strength of the participants, and 4) to have stress relief and gain a sense of fun.
Each session’s art creation theme and activities were designed to be different, but they were all aligned to two or three of the four objectives (see Table 1). Specifically, in the first session, the participant was asked to draw something to represent him/herself, and the therapist would also draw something to represent herself. The activity was designed to help avoid embarrassment, build a trusting relationship between the participant and the therapist, and enhance the participant’s self-awareness. In the second and third sessions, the participant was asked to draw relaxing places and an imagined world with the therapist, which should bring fun and foster a caring, supportive, and willing-to-share atmosphere. As the sessions progressed and the trust relationship had been established, the participant was asked to share his/her feelings while drawing a wishing tree in the fourth session. The wishing tree was supposed to bring some encouragement and positive feelings. The fifth session was about better understanding oneself by drawing self-portraits from different perspectives. In the sixth session, the therapist would work with the participant directly on emotions using colours as a medium. The psychotherapy then progressed to the seventh and eighth sessions, which were designed to bring positive inner strength and a sense of hope to the participant. During the eighth session, besides drawing an imagined future, the therapist would also use the load and replay function of the system to review selected artworks they created collaboratively during previous sessions (see Figure 7).
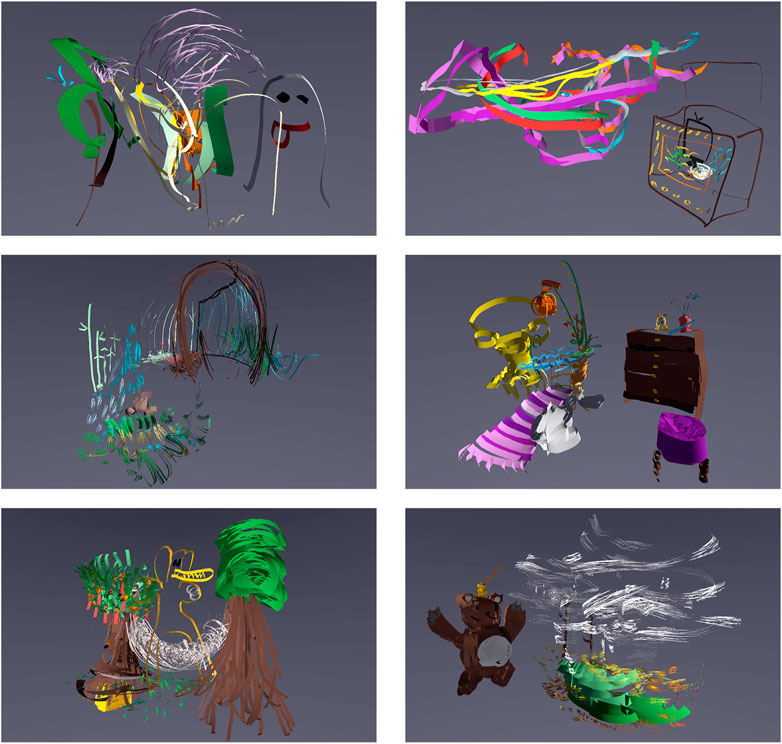
FIGURE 7. Selected artworks created collaboratively by the participants and the therapist.
All three participants completed the art creation sessions in eight consecutive weeks with the therapist. Besides reporting the quantitative results, the qualitative signs of progress and the semi-structured interviews are also summarised here based on the session notes taken by the therapist and the video recordings.
In the pre-test, the participant’s PSS score was 17, indicating moderate perceived stress. Her WEMWBS score was 40. In the post-assessment, her PSS score raised to 26, but still indicating a moderate level of perceived stress. Her WEMWBS score raised to 49. Regarding the SUS score, the participant rated the CVE 80 out of 100, indicating good system usability as perceived by the participant. The mean score of her self-reported copresence was 3.17, and the mean score of the interaction partner’s copresence perceived by her was 4.58. The participants’ mood, anxiety, and pain before and after each session are shown in Figure 8.
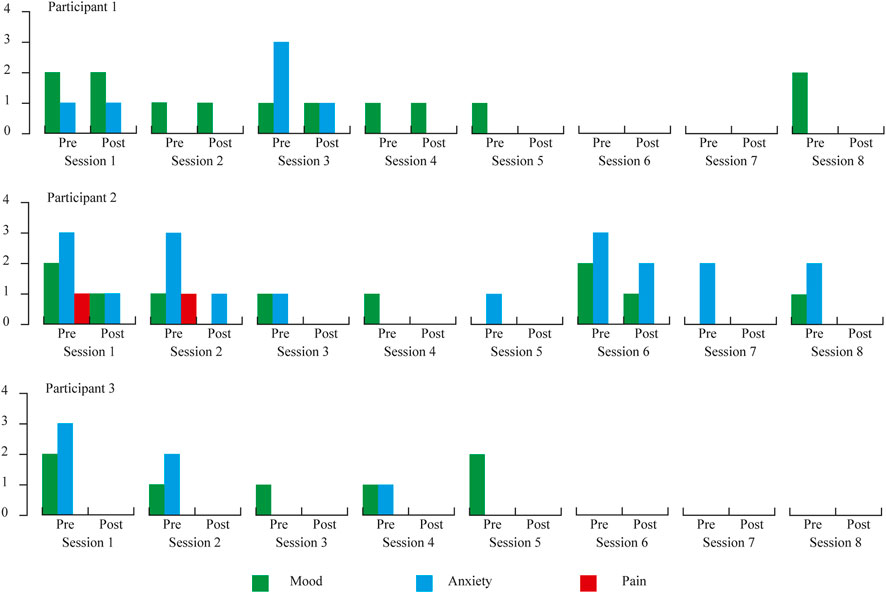
FIGURE 8. The participants’ mood, anxiety, and pain before and after each session as measured by Roger’s Happy/Sad Face Scale (Rogers, 1981).
In the first session, the participant drew an ant in a garden to represent herself. She said the ant, just like herself, was regarded as “a tiny but diligent and productive” individual. When asked if she wanted to invite someone to the garden she had just drawn, the participant thought and drew an anonymous figure that looked quite similar to a cartoon-style ghost. The participant then explained that the figure could be anyone, and she would like to share the virtual garden with anyone besides her friends.
In the second session, the participant was observed to be quiet but showed more body movements when drawing. The session started with a virtual door drawn by the therapist, and the therapist then asked the participant to imagine a relaxing place where the virtual door could lead. The participant drew four snow mountains and a forest in blue with zigzag lines. While drawing, she also shared that sometimes when her opinion was different from the majority in daily life, she felt stress and suffered from pressure. The snow mountains could be an ideal place for her to “filter out the comments from the majority” and to have her stress relief. The therapist asked if the participant wanted to have someone join the snow mountains with her; the participant then drew a similar figure she drew during the first session and said that she did not mind “sharing the space with someone who might also need a relaxing space.”
In the third session, the therapist and the participant collaboratively drew some coral and seaweed to kick off the session. The participant then added a shark to the drawing, and the therapist added a golden fish. The therapist asked if she wanted to be any plants or animals underwater; the participant said she wanted to be the seaweed because she thought that “being the seaweed can stay there and doing nothing.” The therapist then asked if the participant wanted to be somewhere else. The participant then drew the sky with white clouds and an aeroplane. The therapist then added some birds. During the conversation, the participant said she had no strong intention to be in the sky or take the aeroplane; she believed “even the same place could be experienced differently.” Following this conversation, the participant also commented that although drawing in the CVE was interesting and in the previous sessions, she and the therapist had drawn different places, the thing that impressed her was not about these imagined places but “the time shared with you [the therapist] during the sessions.” Her comments suggested that the bonding with the therapist was getting stronger.
The fourth session started by drawing a tree collaboratively. After drawing the tree trunk and leaves, the participant suggested that “no fruits should be added to the tree because it is wintertime.” The therapist asked her if there was anything she wanted to add. The participant then drew some fences around the tree, and she said that “this is the area for the tree to grow.” She associated her experience in local parks and said that “the fence is a way to protect the tree too.”
The theme of the fifth session was about drawing a self-portrait. The participant drew a relaxing self sitting on the sofa and watching television. After that, the therapist asked her to draw herself from other persons’ views. The participant then drew a person in red with strong emotion. She commented that both were herself and in different situations facing different persons, she might also be looked at as an individual that “cares about nothing and is always relaxing.”
In the sixth session, the therapist asked the participant to draw the things that were currently occupying her mind and pay attention to the use of colours. The participant drew a computer in grey, some special equipment in orange and dark grey, a fish in blue, and some bones in grey. When asked to explain what she had just drawn, she said that those were all related to her final year project, and she felt quite frustrated and stressed; Although she had been striving hard, she could not see the chance of achieving the expected result in her final year project. The therapist asked her to think about something based on her previous experience that could help her think out of the box. The participant thought for a while and drew a clock. She then explained that the clock represented time, and she would rather let the time pass so the troubles could go away.
In the seventh session, the participant drew a treasure box with things she liked. She drew a television and several books in the treasure box and said that she liked “watching television and reading books but could not have enough time to do these things to get relaxed.” Besides the television and books, she also drew some humanoid figures in the treasure box, representing her family and friends.
In the last session, the therapist and the participant reviewed some of the artworks created during the previous sessions. The participant said that the artworks in the three-dimensional space were fascinating when being reviewed from various angles. She also said she had a strong sense of freedom when drawing in three-dimensional space.
During the semi-structured interview, she first shared her thoughts on the CVE and the CVE-enabled arts creation. She said she liked using this “digital and three-dimensional medium” to draw, although she felt she needed “some time to get used to the medium and the user interface.” She also suggested that if the CVE could allow her to adjust the lighting, it would be easier for her to understand the spatial relationship between herself and the artwork. She said she did not perceive significant changes in her feelings and emotions, but she felt the sessions served as “outlets of her stress and negative emotions.” Moreover, the collaborative art creation process helped her better understand herself; the drawing themes proposed by the therapist helped her to think and reflect, which she rarely did before joining the sessions. Regarding the relationship with the therapist, the participant said she felt her “interaction with the therapist” during the sessions in CVE was “very inspiring and relaxing.” She also shared that the avatar-mediated communications, compared to face-to-face socialisation, was “less stressful and more relaxing” to her.
In the pre-test, the participant’s PSS score was 35, indicating high perceived stress. Her WEMWBS score was 34. In the post-assessment, her PSS score dropped to 31, still indicating a high level of perceived stress. Her WEMWBS score was slightly raised to 35. Regarding the SUS score, the participant rated the CVE 90 out of 100, indicating sound system usability. The mean score of her self-reported copresence was 4.33, and the mean score of the interaction partner’s copresence perceived by her was 4.00. The participants’ mood, anxiety, and pain before and after each session are shown in Figure 8.
In the first session, the participant drew a pumpkin to represent herself. She then enclosed the pumpkin by drawing a cosy bedroom. She drew a flower and a clock with great details on a shelf. Then she also added a purple chair and a carpet to the bedroom. The therapist asked the participant whether she could also draw someone or a buddy in the bedroom. The participant drew a cat. She was generally quiet during the entire process and only spoke very softly.
In the second session, the participant actively explored the three-dimensional space and the different brush styles. She drew a tree and a cat with a pair of yellow eyes to represent where she could feel relaxed. During this session, the participants started to speak more with the therapist but still only spoke very softly.
The participant drew some imagined mountain ranges covered in snow in the third session. At the foot of a mountain, she added a campfire with an igloo nearby. The therapist also drew a snowman near the igloo. During this session, it was observed by the therapist that the participant started to talk more about her thought during the art creation process. For example, she shared her experience of seeing mountain ranges covered in snow when travelling. The participant also explored the three-dimensional space more. She tried to hide in the igloo and said “it would be interesting to play hide-and-seek” in the CVE.
In the fourth session, since the participant had already drawn a tree during the second session, the therapist asked her to express her wishes by drawing. The participant began by drawing some white clouds in the sky. She then added two spaceships with fine details to the drawing. On one of the clouds, she drew a house which looked like a castle. She later explained that she wanted to have “a nice place to chill and relax”. She drew a mountain beside the river and a boat resting at the pier. She shared that she would like to live on the boat. The participant did not talk too much but was observed to be quite engaged in the art creation process.
In the fifth session, the participant drew lots of random lines to represent herself and drew a tree to represent herself in others’ eyes. She said her life was “somewhat messy”, but she preferred to “keep the messiness away from others.” Hence, she drew the tree because, to her, the tree was a “symbol of peacefulness and acceptance.”
In the sixth session, the therapist asked the participant to draw the things that were currently occupying her mind and pay attention to the use of colours. The participant drew a box in brown with white human figures and a piece of paper inside. She explained that her study and assignments occupied her mind; also, because some of the assignments were group assignments and she did not like collaborating with others, she felt pretty stressed recently. Moreover, she mentioned that she always felt uncomfortable if she needed to interact with others. While saying so, the participant drew some random lines in red around herself. The therapist asked her to think about something based on her previous experience that could help her think out of the box. The participant drew a cat and wrote “ZOOM” alongside the cat. She then explained that she preferred to attend classes online because she did not need to have face-to-face interactions with others.
The therapist asked the participant to draw something in her treasure box in the seventh session. She shared her favourite foods and drew a shopping mall where she could get the foods. Then she drew a flat with human figures inside. Each human figure was slightly different from the others, and according to the participant, the figures were people whom she interacted most with. She also said that she “treasures all the people who leave a mark” on her life journey.
In the last session, when asked to draw the future, the participant chose to draw a shelter. She drew a campsite with plants and tents under the highways and shared that she would like to “hide there to escape from the noise and chaos of the city.”
The participant first shared her thoughts on the CVE and the CVE-enabled arts creation during the semi-structured interview. She shared that she had joined conventional arts therapy in non-clinical settings before. Compared to conventional arts therapy, the CVE-enabled art therapy to her was “more immersive and engaging.” She liked “getting fully immersed in the artworks and even walking into the artworks.” However, she missed the opportunities to preserve and share the artworks with others as the CVE-enabled approach was “purely digital”, and the artworks were intangible. She was looking forward to joining the sessions and hoped the sessions could continue. Regarding her feelings and emotions, she said she had “a sense of fulfilment” after completing the sessions. She also felt “more positive, uplifting, and relaxed” after each session. She also mentioned that she was sensitive to different colours; in the CVE, she could forget about reality and try to use “bright and cheerful colours” when drawing. The drawing themes proposed by the therapist also helped her to “think about the past and the future.” Lastly, the participant said she felt the collaborative art creation process in the CVE helped build a trusting and caring relationship with the therapist.
In the pre-test, the participant’s PSS score was 25, indicating moderate to high perceived stress. His WEMWBS score was 52. In the post-assessment, his PSS score dropped to 19, indicating a low to moderate level of perceived stress. His WEMWBS score slightly dropped to 47. Regarding the SUS score, the participant rated the CVE 75 out of 100, indicating good system usability as perceived by the participant. The mean score of her self-reported copresence was 4.17, and the mean score of the interaction partner’s copresence perceived by her was 3.25. The participants’ mood, anxiety, and pain before and after each session are shown in Figure 8.
In the first session, the participant tried to draw a duck to represent himself and shared that people called him a duck when he was young because of his walking postures. He then added some clouds, a red Sun, and raindrops to the drawing. The session had to stop prematurely because the participant’s HMD was out of battery.
The participant drew a mid-night forest as his relaxing place in the second session. He then added several grey figures in the forest and said those were his imagined “family of ghosts in the forest.” The participant seemed relaxed and liked making jokes during his conversation with the therapist.
In the third session, the therapist and the participant decided to draw an underwater world together. The participant first drew some seaweeds in green, coral in pink and fishes in various colours. After that, the therapist asked the participant to use his imagination to add something to the scene. The participant then very patiently drew a sea turtle with lots of details. He shared that this was inspired by his grandpa, who lived in his old village for a very long time; the turtle might also spend a very long time in this underwater world.
In the fourth session, the participant first drew a tree and then introduced some red pockets hanging on the tree. He said this was the wishing tree he once saw, and he also added some oranges to the tree, which means good luck in Chinese culture. The participant was very engaged during the art creation and thus did not talk too much. However, before the end of the session, he said he felt “thrilled” when he saw the artwork was finished.
In the fifth session, the participant first drew a figure playing basketball and football. He then shared that he always wanted to try new things. However, he sometimes felt there might be too many things in his mind, and “the chaos could also lead to loneliness.” He chose not to draw himself in others’ eyes but shared that his friend should perceive him as a funny person who always makes jokes.
In the sixth session, the therapist first asked the participant to draw what stuck in his mind. He drew a video game controller in grey and several pieces of paper, which represented the games he played recently and his assignments. The participant then shared that he had “some issues in time management recently” because his friends kept inviting him to play video games together, but he had lots of assignments and his practicum as a nursing student was also very demanding. The therapist asked him to think about something based on his previous experience that could help him think out of the box. He first shared that he had to learn how to refuse his friends’ invitations and then started to draw the food he liked (e.g., sushi). He explained that eating might help him relax and redirect his focus.
In the seventh session, the participant drew a treasure box with his unforgettable memories. He drew his dog and his granddad, who had sadly passed away. Then he moved on to share his happy time with his friends by drawing a scene of people playing mahjong and his romantic time with her girlfriend by drawing the places they visited during a trip to Korea and the fireworks he saw during that trip. He later said that at first, he “could not think of anything to draw”, but soon there were many memories came to his mind once he started. He enjoyed the process very much, and he felt connected with the therapist by sharing his life experience.
In the eighth session, the participant drew a portrait of himself-to-be in the future. He drew a human figure running out from a black box first, and then he spent quite a while adding colourful lines outside the black box. He shared that sometimes he might be stuck in the black box in daily life, but he would try to find a way out via drawing to express his emotions and feelings.
The participant first shared his thoughts on the CVE and the CVE-enabled arts creation during the semi-structured interview. He said the CVE-enabled arts creation was “new and novel” to him since he had never had such experience before joining the sessions. He also never thought it would be that easy to draw and create something in the three-dimensional space. Regarding his feelings and emotions, he said the sessions helped him pay more attention to his thoughts and emotions. The sessions also helped him to “get calm and focused”, and he found the art creation process was an excellent way to expel his anxiety and other negative emotions. He also liked the idea of drawing the past and the future, which helped him to “reflect and reorganize the thoughts and ideas about the future.” Regarding the relationship with the therapist, the participant said he found the collaborative art creation was a helpful way to build his trust in the therapist. He also appraised the design of the first session, during which both the therapist and the participant used drawings to quickly know each other, which helped to “increase the sense of trust and caring.” He could feel that the therapist listened to him every time he tried to explain his artwork.
Since the feasibility of using CVE to enable remote arts therapy was largely unexplored, our pilot case study focused on whether CVE could be the medium to ease the translation and maintenance of the unique triangular therapeutic relationship between the therapist, the client, and the artworks in the remote setting, which was widely considered as the most prominent challenge in prior studies. Our results suggested that the trust and binding between the therapist and the participants could be established effectively in the first few sessions. The participants all became more willing to share their feelings and thoughts after the relationship had been established, which was very similar to the practice of face-to-face arts therapy in the clinical setting. The therapist, who got used to delivering conventional psychotherapeutic sessions through video conferencing platforms during the global pandemic, also suggested that compared to video conferencing, the avatar-mediated communications seemed more relaxing for both the therapist and the participants. Thus, the medium was considered very effective in building the trust and binding between the therapist and the participants. Meanwhile, the collaborative art creation process brought new opportunities to the therapeutic process and provided a way for improvisational art creation. During conventional face-to-face sessions, it could be very challenging to have the therapist and the clients working on the same artwork simultaneously due to the constraints of the physical world. However, during our CVE-enabled sessions, the therapist and the participants could easily work on the same artwork simultaneously, promoting the attunement between the participants and therapist through the collaborative art creation activities. The therapist could encourage the client to mirror the line drawings or any kinesthetic activities in the CVE to self-soothe and stimulate energy, depending on the needs of the participants. Moreover, as mentioned by the participants during the semi-structured interview, this collaborative process could be an excellent way to build a trusting relationship with the therapist and was inspiring and relaxing; the participants, in general, enjoyed the reflection and sharing process together with the therapist during the CVE-enabled sessions.
Regarding the system usability, all participants gave high SUS scores to our system. The design idea of the user interfaces and the interaction logic was borrowed from the design of Tilt Brush1, which the participants in prior studies well received [e.g., (Kaimal et al., 2020; Haeyen et al., 2021)]. Our system’s design could be considered a simplified version with only the essential functions, aiming to serve potential users who might have a limited understanding of three-dimensional computer graphics and the digital representation of colours. For example, to use the colour picker in Tilt Brush1, users might need to understand the HSV or RGB colour model to pick the desired colour quickly. In our implementation, users only need to pick a colour from the nine-by-nine colour palette, which shares the same interaction logic of selecting other system functions. Meanwhile, future studies could address several things to enhance the system’s usability. First, the participants could not see their self-avatars in the current design. This limitation originated from the user interface design; As the user interface for art creations and accessing various system functions was permanently attached to the controllers, the user interface might easily overlap with the hands of the self-avatars. Avoiding this issue required redesigning the entire user interface and deviating from the original user interaction design philosophy. It is unclear whether this issue negatively affected the sense of copresence in the CVE. We will continue investigating this issue and seeking other user interface designs that could be more suitable for enabling avatar-mediated communications and collaborative art creations in CVEs. Moreover, a suitable locomotion technique should be implemented in the CVE. The most widely implemented locomotion technique in single-user VR applications is “teleportation” due to its advantage in introducing less motion sickness (Bozgeyikli et al., 2016; Rahimi et al., 2018). However, a direct copy of this technique in the CVE was not well received during our internal testing because the interaction partner perceived the lack of a smoothly-animated translation of the avatar during teleportation as “random jumps” in the virtual space, which was quite confusing. Thus, the locomotion technique was disabled during the sessions to avoid such issues. In some cases, this caused difficulties in the collaborative art creation process since the therapist, who shared a smaller physical space than the participants, could not move to desirable locations to draw. This issue could become more prominent if there were more significant differences in the size of physical spaces used by different interaction partners. Addressing this issue would be beyond the scope of this pilot case study. However, we encourage future studies to design and test new locomotion techniques, such as the ones proposed by Freiwald et al. (2022), which could be more suitable for avatar-mediated communications and collaborations in CVEs.
The quantitative measures provided some interesting results regarding the effectiveness of CVE-enabled remote arts therapy. Specifically, the perceived stress of participants 2 and 3, as measured using PSS, was lowered after finishing the eight sessions. Meanwhile, the PPS score of participant 1 raised from 17 before the sessions to 26 after the sessions. Participant 3’s mental wellbeing, as measured by WEMWBS, was slightly lower in the post-assessment than in the pre-assessment, while both participants 1 and 2’s WEMWBS scores raised slightly. The quick assessment of the participants’ mental wellbeing via Roger’s Happy/Sad Face Scale showed very consistent results; generally, their mood, anxiety, and pain were reduced after each session in the CVE. Moreover, as the psychotherapy in the CVE progressed, their mood, anxiety, and pain were generally lowered in the inter-session comparison, except for participant 2’s sudden spike in the sixth session. As the sessions spanned 8 weeks, many factors could be attributed to the results. For example, in her sixth session, participant 2 mentioned to the therapist that the spike in her mood and anxiety, as reported on Roger’s Happy/Sad Face Scale, was affected by the quick deterioration of the COVID-19 pandemic situation in Hong Kong. In short, the quantitative data showed mixed results regarding the approach’s effectiveness in enhancing the participants’ mental wellbeing and reducing their perceived stress. Besides the psychotherapeutic sessions in CVE, we suspect other factors might have affected the results.
At the same time, the qualitative data we collected also shed light on the effectiveness of CVE-enabled remote arts therapy. The participants generally liked the sessions and the medium, which allowed them to express themselves and expel stress. All participants appraised the novelty and attractiveness of the CVE during the semi-structured interviews. They all felt that the therapist was kind, caring, and trustful, even though they only met virtually with the therapist in the CVE - the qualitative feedback aligned with the quantitative data on copresence. During the interview, participant 3 also said that through his participation, he realised that art creation could be beneficial in stress management, and he started drawing on paper when he wanted to get calm and focused. It shows that the approach could potentially lead to a long-term positive change in the participants’ mental wellbeing. From the therapist’s perspective, building a trusting relationship with the participants could be sensed as the sessions progressed—All participants started to talk more about themselves and their daily lives in the second or third session. The participants’ sources of stress were discussed during the sessions, which indicated a trust relationship had been established, just like what could be achieved in conventional arts therapy.
There were three significant advantages of using CVE for remote arts therapy, as we discovered during this pilot case study. First, the avatar-mediated communications in the CVE could protect the participants’ identity and privacy, hypothetically making the practice of arts therapy easier to accept by individuals who might be hesitate to seek psychotherapeutic interventions. At the same time, there was no evidence suggesting that our avatar-mediated approach hindered the psychotherapeutic interventions compared to the conventional face-to-face approaches. Second, the practice of collaborative arts creations was much easier in the CVE than in the physical world. The CVE broke the constraints of the physical world. Each interaction partner in the CVE could find the desired locations in this unlimited virtual space to participate in the collaborative arts creations. Currently, the collaborative experience is synchronised in real-time, but the medium does support asynchronous experiences if a few technical and design challenges could be addressed in future works (Chow et al., 2019; Wang et al., 2019; Pidel and Ackermann, 2020). Supporting both synchronised and asynchronous experiences will bring more possibilities for remote arts therapy in CVEs. Third, the digital nature of the artworks provided new ways for the therapist and the participants to review their collaborative art creation process. Each step during the process was stored digitally and could be loaded and replayed effortlessly in the three-dimensional space. During the eighth sessions, the therapist and the participants used this feature to review their collaborative art creation processes during the previous seven sessions; This would be very difficult to achieve with the conventional media for arts therapy but had been seen by the therapist as a useful way to talk about changes with the participants as the sessions progressed.
The medium also has several disadvantages, as found in this study. First, the conventional approaches for arts therapy often involve multisensory stimulation, which could not be easily enabled in CVEs. Like many off-the-shelf VR applications, the CVE-enabled remote arts therapy mainly relied on vision and hearing senses. It would be interesting to see how touch and smell senses could also be enabled in CVEs to deliver more immersive and engaging arts creation experiences. Second, at the current stage, the behavioural realism of the self-avatars was limited by the access to special hardware. Most off-the-shelf HMDs can only enable head and hand tracking, limiting the behavioural realism of the self-avatars in CVEs. Although Herrera et al. (2020) suggested that half-body self-avatars with head and hands tracking could induce great copresence, it would be interesting to know whether the facial expression of the self-avatars would better facilitate the avatar-mediated communications and bring even higher levels of copresence. There is hardware (e.g., VIVE Facial Tracker7) that can track users’ facial expressions while wearing HMDs. However, the avatar models might need to be modified to support the realistic and natural mapping of the tracked facial expressions using a standardised coding system [e.g., the Facial Action Coding System (Ekman and Friesen, 1978; Gutiérrez-Maldonado et al., 2014)]. We hope the hardware can become more accessible, and more software libraries could help the development of CVEs that support higher levels of behavioural realism so that we can further investigate the effects of behavioural realism on remote art therapy in CVEs. Lastly, we should admit that the technological and digital nature of CVE-enabled remote arts therapy could hinder its accessibility. In our pilot case study, the participants, who were well-educated and experienced in using digital technologies, had no issues interacting with the system. However, it might not be practical for people who might not be familiar with digital technologies to join the CVE-enabled sessions in remote locations without on-site technical support.
First, all participants were determined to complete all the sessions with the therapist. None of the participants missed a session, even during the quick deterioration of the COVID-19 pandemic in Hong Kong. When strict social-distancing rules were imposed in Hong Kong in the middle of this study, all participants communicated with the experimenter proactively regarding the arrangement of the psychotherapeutic sessions. This demonstrated the participants’ commitment to the sessions and their sense of engagement and enjoyment from another perspective. Second, as the sessions progressed, all participants started to draw enclosed geometries in the three-dimensional space, compared to strokes on two-dimensional canvases in the first and second sessions. Although the idea of creating three-dimensional artworks in VR is interesting, we found that it took some time for the participants to think and create in a truly three-dimensional manner. During the first and second sessions, the participants treated the three-dimensional space more like two-dimensional canvases from relatively fixed points of view. As the sessions progressed, they all started to dynamically observe the strokes from different points of view by moving around in the three-dimensional space. Lastly, the participants encountered no difficulties using the enabling software and hardware, even in the first session. All three participants of this study quickly learned how to use the system after watching the demonstration given by the experimenter. Making the CVE easy to use and avoiding a steep learning curve that leads to expressive art creations is vital if more participants with more diverse backgrounds are supposed to use the same software and hardware for remote arts therapy.
The major limitation of this study is the less than ideal diversity in the backgrounds of the participants, which may hinder the generalisation of the results to a more diverse population who need psychotherapeutic interventions. Specifically, because using CVE to deliver remote arts therapy is largely unexplored territory, to address ethical concerns on applying this entirely new approach in the clinical setting, our study investigated the feasibility and effectiveness of the approach with the three participants who did not have clinical diagnoses of mental disorders. Hence, the design of the protocols and art creation activities mainly focused on enhancing mental wellbeing instead of addressing mental disorders and other complications. The protocols and CVE-enabled art creation activities could be easily adapted to address specific mental disorders, such as generalised anxiety disorder (GAS), of which the psychotherapeutic approaches may share similar components. However, working with more complicated and less stable cases in the clinical setting may require the deep customisation of the protocols based on the needs of clients and the physical presence of another therapist, who can intervene immediately on-site if needed. Nevertheless, our study can serve as a solid foundation for future studying of CVE-enabled arts therapy in the clinical setting on a large scale, and we hope it can, to some degree, address the ethical concerns.
Motivated by prior studies that explored the use of off-the-shelf VR applications to enable arts therapy and the increasing demand for teletherapy due to the global pandemic, a CVE was designed and built specifically to enable remote arts therapy. Although the quantitative data regarding the approach’s effectiveness are mixed and inconclusive, the qualitative feedback and comments from the participants and the therapist were highly encouraging. The therapist and the participants also provided valuable insights regarding this approach’s advantages and disadvantages. We will further improve the usability of the CVE and study the effects of self-avatars on copresence as well as the psychotherapeutic process in general. Meanwhile, we encourage future studies to investigate CVE-enabled remote arts therapy in the clinical setting cautiously and collect more evidence regarding its effectiveness in addressing clinically diagnosed mental disorders and other complications.
The raw data supporting the conclusion of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by the Institutional Review Board of The Hong Kong Polytechnic University (application no.: HSEARS20220517004). The participants provided their written informed consent to participate in this study.
CL and PYY both contributed to conception and design of the study and wrote the draft of the manuscript. PYY, who is a registered expressive arts therapist, delivered the collaborative arts creation sessions. CL developed the collaborative virtual environment, transcribed the session recordings, and collected the quantitative data. All authors contributed to manuscript revision, read, and approved the submitted version.
Financial support was received from The Hong Kong Polytechnic University (project no: P0035264).
We want to thank Honglin Li and Yu Liu of The Hong Kong Polytechnic University for their assistance in the sessions.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frvir.2023.1059278/full#supplementary-material
3https://vr.readyplayer.me/avatar.
5https://www.photonengine.com/pun.
7https://www.vive.com/accessory/facial-tracker/.
Benford, S., Greenhalgh, C., Rodden, T., and Pycock, J. (2001). Collaborative virtual environments. Commun. ACM 44, 79–85. doi:10.1145/379300.379322
Biocca, F., Harms, C., and Burgoon, J. K. (2003). Toward a more robust theory and measure of social presence: Review and suggested criteria. Presence Teleoperators virtual Environ. 12, 456–480. doi:10.1162/105474603322761270
Biocca, F., and Levy, M. R. (2013). Communication in the age of virtual reality. Oxfordshire, England, UK: Routledge).
Bozgeyikli, E., Raij, A., Katkoori, S., and Dubey, R. (2016). “Point & teleport locomotion technique for virtual reality,” in Proceedings of the 2016 annual symposium on computer-human interaction in play, 205–216. doi:10.1145/2967934.2968105
Chow, K., Coyiuto, C., Nguyen, C., and Yoon, D. (2019). Challenges and design considerations for multimodal asynchronous collaboration in vr. Proc. ACM Human-Computer Interact. 3, 1–24. doi:10.1145/3359142
Cohen, S., Kamarck, T., and Mermelstein, R. (1983). A global measure of perceived stress. J. health Soc. Behav. 385, 385–396. doi:10.2307/2136404
Dellazizzo, L., Potvin, S., Luigi, M., and Dumais, A. (2020). Evidence on virtual reality–based therapies for psychiatric disorders: meta-review of meta-analyses. J. Med. Internet Res. 22, e20889. doi:10.2196/20889
Deng, W., Hu, D., Xu, S., Liu, X., Zhao, J., Chen, Q., et al. (2019). The efficacy of virtual reality exposure therapy for ptsd symptoms: A systematic review and meta-analysis. J. Affect. Disord. 257, 698–709. doi:10.1016/j.jad.2019.07.086
Ekman, P., and Friesen, W. V. (1978). Facial action coding system. Environ. Psychol. Nonverbal Behav. doi:10.1037/t27734-000
Fodor, L. A., Cotet, C. D., Cuijpers, P., Szamoskozi, S., David, D., and Cristea, I. A. (2018). The effectiveness of virtual reality based interventions for symptoms of anxiety and depression: A meta-analysis. Sci. Rep. 8, 10323. doi:10.1038/s41598-018-28113-6
Freiwald, J. P., Schmidt, S., Riecke, B. E., and Steinicke, F. (2022). The continuity of locomotion: Rethinking conventions for locomotion and its visualization in shared virtual reality spaces. ACM Trans. Graph. (TOG) 41, 1–14. doi:10.1145/3550454.3555522
Gallagher, L. M., and Steele, A. L. (2002). Music therapy with offenders in a substance abuse/mental illness treatment program. Music Ther. Perspect. 20, 117–122. doi:10.1093/mtp/20.2.117
Gumilar, I., Barde, A., Hayati, A. F., Billinghurst, M., and Singh, S. (2021). “Eye-gaze, inter-brain synchrony, and collaborative vr in conjunction with online counselling: A pilot study,” in 2021 IEEE international symposium on mixed and augmented reality adjunct (ISMAR-Adjunct) (IEEE), 57–62. doi:10.1109/ISMAR-Adjunct54149.2021.00021
Gussak, D. E., and Rosal, M. L. (2015). The Wiley handbook of art therapy. New Jersey, United States: John Wiley & Sons.
Gutiérrez-Maldonado, J., Rus-Calafell, M., and González-Conde, J. (2014). Creation of a new set of dynamic virtual reality faces for the assessment and training of facial emotion recognition ability. Virtual Real. 18, 61–71. doi:10.1007/s10055-013-0236-7
Haeyen, S., Jans, N., and Heijman, J. (2021). The use of vr tilt brush in art and psychomotor therapy: An innovative perspective. Arts Psychotherapy 76, 101855. doi:10.1016/j.aip.2021.101855
Herrera, F., Oh, S. Y., and Bailenson, J. N. (2020). Effect of behavioral realism on social interactions inside collaborative virtual environments. Presence 27, 163–182. doi:10.1162/pres_a_00324
Jung, S., Karki, N., Slutter, M., and Lindeman, R. W. (2021). On the use of multi-sensory cues in symmetric and asymmetric shared collaborative virtual spaces. Proc. ACM Human-Computer Interact. 5, 1–25. doi:10.1145/3449146
Kaimal, G., Carroll-Haskins, K., Berberian, M., Dougherty, A., Carlton, N., and Ramakrishnan, A. (2020). Virtual reality in art therapy: A pilot qualitative study of the novel medium and implications for practice. Art. Ther. 37, 16–24. doi:10.1080/07421656.2019.1659662
Nowak, K. L., and Biocca, F. (2003). The effect of the agency and anthropomorphism on users’ sense of telepresence, copresence, and social presence in virtual environments. Presence Teleoperators Virtual Environ. 12, 481–494. doi:10.1162/105474603322761289
Opriş, D., Pintea, S., García-Palacios, A., Botella, C., Szamosközi, Ş., and David, D. (2012). Virtual reality exposure therapy in anxiety disorders: A quantitative meta-analysis. Depress. anxiety 29, 85–93. doi:10.1002/da.20910
Pidel, C., and Ackermann, P. (2020). “Collaboration in virtual and augmented reality: A systematic overview,” in International conference on augmented reality, virtual reality and computer graphics (Springer), 141–156. doi:10.1007/978-3-030-58465-8_10
Rahimi, K., Banigan, C., and Ragan, E. D. (2018). Scene transitions and teleportation in virtual reality and the implications for spatial awareness and sickness. IEEE Trans. Vis. Comput. Graph. 26, 2273–2287. doi:10.1109/TVCG.2018.2884468
Riggio, R. E., and Friedman, H. S. (1986). Impression formation: The role of expressive behavior. J. personality Soc. Psychol. 50, 421–427. doi:10.1037/0022-3514.50.2.421
Robledo Yamamoto, F., Voida, A., and Voida, S. (2021). From therapy to teletherapy: Relocating mental health services online. Proc. ACM Human-Computer Interact. 5, 1–30. doi:10.1145/3479508
Rogers, A. (1981). Third world congress on pain of the international association for the study of pain. Pain, 319.
Rubin, J. A. (2012). Approaches to art therapy: Theory and technique. Oxfordshire, England, UK: Routledge.
Scozzari, S., and Gamberini, L. (2011). Virtual reality as a tool for cognitive behavioral therapy: A review. Adv. Comput. Intell. paradigms Healthc. 6. Virtual Real. psychotherapy, rehabilitation, Assess. 63, 63–108. doi:10.1007/978-3-642-17824-5_5
Shella, T. A. (2018). Art therapy improves mood, and reduces pain and anxiety when offered at bedside during acute hospital treatment. Arts Psychotherapy 57, 59–64. doi:10.1016/j.aip.2017.10.003
Short, J., Williams, E., and Christie, B. (1976). The social psychology of telecommunications. London: Wiley.
Skarbez, R., Brooks, F. P., and Whitton, M. C. (2017). A survey of presence and related concepts. ACM Comput. Surv. (CSUR) 50, 1–39. doi:10.1145/3134301
Slater, M., Banakou, D., Beacco, A., Gallego Vila, J., Macia-Varela, F., and Oliva, R. (2022). A separate reality: An update on place illusion and plausibility in virtual reality. Front. Virtual Real. 3, 914392. doi:10.3389/frvir.2022.914392
Slater, M. (2009). Place illusion and plausibility can lead to realistic behaviour in immersive virtual environments. Philosophical Trans. R. Soc. B Biol. Sci. 364, 3549–3557. doi:10.1098/rstb.2009.0138
Slater, M., and Steed, A. (2002). “Meeting people virtually: Experiments in shared virtual environments,” in The social life of avatars (London: Springer), 146–171. doi:10.1007/978-1-4471-0277-9_9
Steuer, J. (1992). Defining virtual reality: Dimensions determining telepresence. J. Commun. 42, 73–93. doi:10.1111/j.1460-2466.1992.tb00812.x
Tennant, R., Hiller, L., Fishwick, R., Platt, S., Joseph, S., Weich, S., et al. (2007). The warwick-edinburgh mental well-being scale (wemwbs): Development and UK validation. Health Qual. life Outcomes 5, 63–13. doi:10.1186/1477-7525-5-63
Wang, C. Y., Drumm, L., Troup, C., Ding, Y., and Won, A. S. (2019). “Vr-replay: Capturing and replaying avatars in vr for asynchronous 3d collaborative design,” in 2019 IEEE conference on virtual reality and 3D user interfaces (VR) (IEEE), 1215–1216. doi:10.1109/VR.2019.8797789
Won, A. S., Bailenson, J. N., Stathatos, S. C., and Dai, W. (2014). Automatically detected nonverbal behavior predicts creativity in collaborating dyads. J. Nonverbal Behav. 38, 389–408. doi:10.1007/s10919-014-0186-0
Keywords: virtual reality, collaborative virtual environment, arts therapy, teletherapy, mental wellbeing, COVID-19
Citation: Li C and Yip PY (2023) Remote arts therapy in collaborative virtual environment: A pilot case study. Front. Virtual Real. 4:1059278. doi: 10.3389/frvir.2023.1059278
Received: 01 October 2022; Accepted: 20 March 2023;
Published: 12 May 2023.
Edited by:
Nadia Magnenat Thalmann, University of Geneva, SwitzerlandReviewed by:
Byung-Hoon Kim, Yonsei University, Republic of KoreaCopyright © 2023 Li and Yip. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chen Li, richard-chen.li@polyu.edu.hk
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.