 Hélène Buche
Hélène Buche Aude Michel
Aude Michel Nathalie Blanc
Nathalie Blanc- 1Univ Paul Valéry Montpellier 3, Epsylon Ea 4556, Montpellier, France
- 2Montpellier Institut Du Sein, Clinique Clémentville, Montpellier, France
Over the past 20 years, virtual reality (VR) has been the subject of growing interest in oncology. More and more researchers are studying the effects of virtual environments to contribute to current thinking on technologies likely to support patients undergoing oncological treatment. Recent research highlights how VR can divert attention while reducing anxiety in stressful healthcare situations through its multisensory and participative nature. VR appears to be a promising tool capable of reducing cancer-related anxiety symptoms, improving treatment adherence, and increasing satisfaction with oncology care. While the literature reports these positive effects in the therapeutic management of cancer, few studies have focused on theoretical models capable of explaining the psychological benefits of virtual immersion. This literature review provides a theoretical framework combining results from all relevant empirical work in oncology. The review can help researchers identify the optimal conditions for using VR in oncology and bridge the gap between divergent devices, modalities, and practices (e.g., headmounted displays, environments, interactivity, immersion time).
1 Introduction
For the past 30 years, the number of new cancer cases has been steadily increasing. The National Cancer Institute (Institut National du Cancer, 2019) reported 328,000 diagnoses in metropolitan France in 2018 compared to 320,000 in 2005. The most common cancers in men were prostate cancer (48,427 new cases in 2013), followed by lung (32,500 cases) and colorectal (24,000 cases). In women, breast cancer was the most frequent (59,000 cases), followed by colon-rectal cancer (21,000 cases) and lung cancer (17,000 cases) (Defossez et al., 2019). Many stress factors have been identified at different times in cancer management, including diagnosis, treatment, and long-term management of the disease (Chirico et al., 2015). Among patients treated for cancer, 55% met clinical criteria for an anxiety disorder (O’Connor et al., 2010), with an increase to 77% in patients who received chemotherapy (Nikbakhsh et al., 2014). In addition, the prevalence of cancer-related pain was 39.3% in patients who received curative treatment, increasing to 55% in patients undergoing cancer treatment and reaching 71% in advanced or metastatic cancer (Van den Beuken-van Everdingen et al., 2016; Alawneh et al., 2017). Many stress agents and physical symptoms can cause increased emotional distress (Arrieta et al., 2013).
In this context, virtual reality (VR) is the object of interest and curiosity in cancerology. More and more researchers are studying the effects of VR to improve the conditions of oncological treatments (Pittara et al., 2020). Most studies have highlighted the benefits of VR, which, thanks to its distraction power, can divert attention while reducing the anxiety and pain of patients facing particularly distressing care situations (Chirico et al., 2016; Ahmad et al., 2020). Although the literature focuses on the positive effects of this tool in the context of cancer treatment, few studies have focused on the theoretical models of cognitive science that explain and try to understand the benefits of VR. Rather than viewing it as a technical medium, in-depth research based on an appropriate theoretical framework is needed to explore the complexity of virtual environments (de Loor and Tisseau, 2011). Only these foundations can give scientific legitimacy to this technological revolution (de Loor and Tisseau, 2011) and provide us with elements of knowledge on the mechanisms that promote patients’ emotional wellbeing. Let us note that beyond understanding the mechanisms, these foundations could be used as support to design specialized interfaces adapted to different clinical situations.
VR became more accessible for consumer use after 2016 (Tsaï, 2016). It is “the application that allows the user to navigate and interact in real-time with a three-dimensional environment generated by a computer” (Pratt et al., 1995). This artificial environment is usually made possible using a computer screen that responds to the individual’s head movements by providing synthetic sensory stimuli such as images of real or imaginary landscapes, spatialized sounds, and sometimes tactile or olfactory feedback (Chirico et al., 2016; Chirico et al., 2019). VR equipment also includes devices that allow action in the virtual world, such as a mouse, keyboard, or more sophisticated game controllers (Pittara et al., 2020; Indovina et al., 2018). In other words, different systems offer users different sensations and levels of involvement.
The development of high-performance virtual reality devices accelerates innovation focused on health to facilitate the realization of cancer care by offering a quality immersive device allowing patients to escape from their distress and painful medical situations (Pittara et al., 2020; Ahmad et al., 2020). Immersion in a virtual environment is considered both as a distractor (reducing anxiety and pain) (Chirico et al., 2019; Bani Mohammad and Ahmad, 2018; Ahmadpour et al., 2020) and as a tool for emotional regulation (reducing negative emotions, inducing positive emotions), allowing improvement in care tolerance (Pizzoli et al., 2019).
The benefits of VR were first observed in oncology during chemotherapy sessions. The results were encouraging (Oyama et al., 1999; Schneider and Workman, 1999), promoting a decrease in anxiety, an improvement in mood as well as an underestimation of care time (Schneider and Workman, 1999; Schneider et al., 2003), (Schneider et al., 2004; Schneider and Hood, 2007). Today, the distractive power of VR is of interest in a range of oncology situations ranging from palliative care (Niki et al., 2019; Johnson et al., 2020) to the support of hospitalized patients during various medical procedures (Pittara et al., 2020; Ahmad et al., 2020; Zeng et al., 2019).
Although several studies have emphasized the effectiveness of VR distraction in oncology, the virtual reality devices used are wildly divergent in terms of content, intervention strategies, and technological qualities. It is thus necessary to go beyond the wonder and attractiveness that VR arouses to resist this technological hype toward rethinking and resituating its use within our knowledge of the human. This literature review aims to take stock of the benefits of using VR as a distraction tool for anxiety and pain management in oncology. To this end, the results known to date are listed, and their analysis is considered according to the methodology used. This literature review aims to bring out the points of consensus and the methodological divergences in the research while emphasizing that few interventional studies are theoretically anchored. Based on this review of the available literature, recommendations will be made to enable the research community to move towards common methodological choices and thus improve clinical practice. Another aim of this literature review is to leverage the theoretical foundations identified toward a theoretical model that will allow us to think about the contributions of VR in oncology, especially the cognitive and emotional processes involved.
2 Method
2.1 Data source and search method
Based on the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) method, we proceeded stepwise using six computerized databases: Google Scholar, PubMed, PsychInfo, Academic Search Premier, Ebsco, and Sciencedirect to search for relevant studies. We limited the search to 10 years (2011–2021). In each database, we used the same search terms: virtual reality and cancer, virtual reality and oncology, virtual reality and anxiety, virtual reality and cancer and anxiety, virtual reality and pain, virtual reality and cancer and pain. We also manually searched bibliographic references of included studies and previously published systematic reviews.
2.2 Study selection
Our inclusion criteria incorporated studies explicitly examining the effectiveness of VR as a distraction tool in oncology. In this sense, we excluded all studies that were unrelated to cancer and all research conducted with cancer populations whose purpose was not associated with distraction to improve emotional state and decrease pain.
2.3 Data collection
To collect the data, we extracted all relevant information from the selected articles into an Excel file: characteristics of the study population sample, type of cancer, psychological variables, VR equipment, environments, immersive tasks, methodology, objectives of the studies, medical context, stated theoretical frameworks and main results, as well as current limitations of VR and its future direction.
2.4 Data analysis
The selected articles were subjected to a literature review to exploit and classify the results according to recurrent characteristics that allowed the different studies to be compared. The selected characteristics included VR equipment, immersive modalities, environments, effectiveness of VR in oncology, theoretical basis for the benefits of VR, limitations, and future direction of VR distraction to decrease pain intensity and anxiety in clinical situations.
3 Results
3.1 State of the art presentation
3.1.1 Characteristics of the studies
3.1.1.1 Population
Nearly three-quarters of the selected studies evaluating the intervention of VR during the management of cancer patients (1,153 participants aged 6–85 years) were conducted with adults (72, 73%, 16/22 studies) (Chirico et al., 2019; Bani Mohammad and Ahmad, 2018; Pizzoli et al., 2019; Niki et al., 2019; Johnson et al., 2020; Schneider et al., 2011; Espinoza et al., 2012; Baños et al., 2013; Li et al., 2016; Glennon et al., 2018; Gupta and Hande, 2019; Higgins et al., 2019; Garrett et al., 2020; Gerçeker et al., 2020; Scates et al., 2020; Buche et al., 2021). The remaining studies were conducted in pediatric oncology (27, 27%, 6/22 studies) (Li et al., 2011; Atzori et al., 2018; Birnie et al., 2018; Semerci et al., 2020; Sharifpour et al., 2020; Tennant et al., 2020).
3.1.1.2 Type of cancer in which virtual reality has been proposed
The qualitative analysis of these studies reveals a clear diversity in the medical context for evaluating the effects of VR according to the type of cancer. As shown in Figure 1, more than a third of the studies were performed during the treatment of breast cancer (36.36%) (Chirico et al., 2019; Bani Mohammad and Ahmad, 2018; Pizzoli et al., 2019; Schneider et al., 2011; Espinoza et al., 2012; Gupta and Hande, 2019; Garrett et al., 2020; Buche et al., 2021) and almost a third during the management of blood cancer (e.g., leukemia) and/or lymphatic system (e.g., lymphoma) (27.27%) (Glennon et al., 2018; Garrett et al., 2020; Li et al., 2011; Atzori et al., 2018; Birnie et al., 2018; Tennant et al., 2020). A few studies have examined the effects of VR during treatment of lung cancer (Niki et al., 2019; Schneider et al., 2011; Espinoza et al., 2012; Garrett et al., 2020), bone cancer and brain tumors (Li et al., 2011; Birnie et al., 2018; Sharifpour et al., 2020; Tennant et al., 2020) (18.18% each). Few studies included patients with germ cell tumors (13.64%) (Li et al., 2011; Sharifpour et al., 2020; Tennant et al., 2020), skin cancer (9.09%) (Higgins et al., 2019; Tennant et al., 2020), or kidney cancer (9.09%) (Niki et al., 2019; Garrett et al., 2020), while some types of cancer were invoked only once in VR applicability (4.55% each) (see Figure 1: Type of cancer in which VR has been proposed) (Niki et al., 2019; Schneider et al., 2011; Espinoza et al., 2012; Baños et al., 2013; Garrett et al., 2020; Sharifpour et al., 2020).
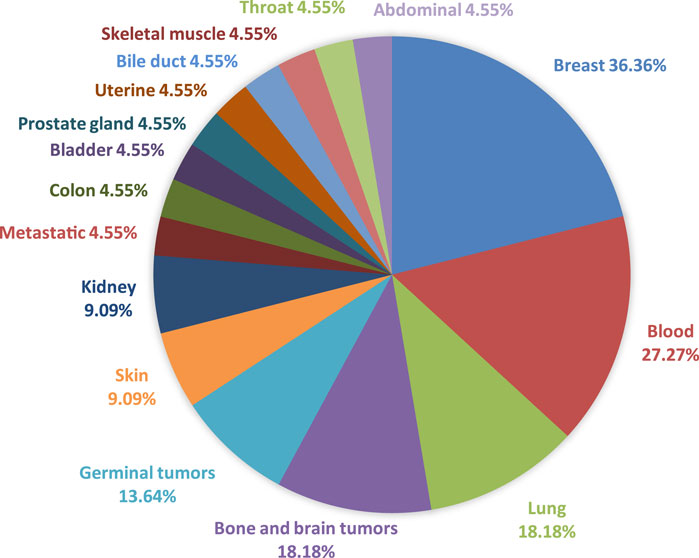
FIGURE 1. Type of cancer in which VR has been proposed.
3.1.2 Context of virtual reality intervention in oncology
In addition to the types of cancer, studies have evaluated the benefits of VR according to the context of VR use (see Figure 2: Contexts of Use). In the context of long-term hospitalization, VR is used as a distraction tool to promote emotional and physical well-being (31.81%, 7/22 studies) (Bani Mohammad and Ahmad, 2018; Espinoza et al., 2012; Baños et al., 2013; Gupta and Hande, 2019; Higgins et al., 2019; Li et al., 2011; Tennant et al., 2020). In the context of day hospitalization, it is proposed in particular when patients have to undergo a painful medical procedure (i.e., catheter port placement, venipuncture, IV station, bone marrow aspiration and biopsy) to reduce acute pain (27.27%, 6/22 studies) (Glennon et al., 2018; Gerçeker et al., 2020; Scates et al., 2020; Atzori et al., 2018; Birnie et al., 2018; Semerci et al., 2020). Its application in oncology is no longer limited to chemotherapy sessions (13.64%, 3/22 studies) (Chirico et al., 2019; Schneider et al., 2011; Sharifpour et al., 2020). Distraction under VR is now used in palliative care (9.09%, 2/22 studies) to relieve symptoms in terminally ill patients (Niki et al., 2019; Johnson et al., 2020) and at home (9.09%, 2/22 studies) to manage patients’ chronic pain (Garrett et al., 2020), alleviate symptoms of psychological distress and promote patient empowerment (Li et al., 2016). In physiotherapy, this distraction strategy has recently been proposed during post-mastectomy scar massage sessions by comparing participative and contemplative distraction (4.55%, 1/22 studies) (Buche et al., 2021). Finally, only one study went outside the medical context to test the first virtual laboratory experiment measuring the effects of VR associated with two different relaxation techniques (i.e., breath control vs. Body Scanning Procedure) on breast cancer patients (4.55%, 1/22 studies) (Pizzoli et al., 2019).
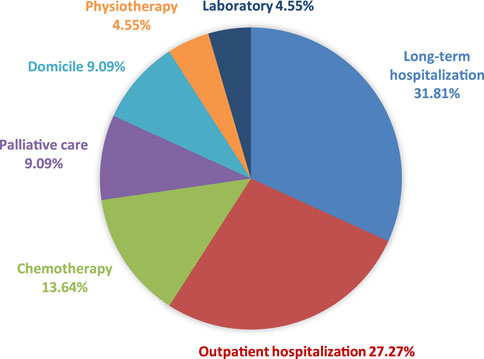
FIGURE 2. Context of VR intervention in oncology.
3.1.3 Benefits of virtual reality in oncology
Distraction is a non-pharmacological technique increasingly used by healthcare professionals to alleviate anxiety and pain related to medical procedures (Bani Mohammad and Ahmad, 2018; Gold et al., 2007). The underlying mechanism of the power of distraction relies on the limited cognitive resources of an individual’s attention (Arane et al., 2017). An engaging and attractive distractor diverts the patients’ attention and hinders their ability to process external negative stimuli, decreasing anxiety, and pain (Gold et al., 2007; Kleiber and McCarthy, 2006). Two forms of distraction can be distinguished: a passive form (e.g., watching television, listening to music) and an active form (e.g., electronic games) (Arane et al., 2017; Koller and Goldman, 2012). Thus, using a distractor is a cognitive strategy that can passively redirect the patients’ attention or actively involve them in a task (Gold et al., 2007; Kleiber and Harper, 1999). VR is a powerful distractor as it can offer several degrees of involvement by immersing the patient in a contemplative or participative environment that mobilizes several senses (Chirico et al., 2019; Ahmadpour et al., 2020; Buche et al., 2021). The multimodal aspect of VR induces a subjective feeling of being present in the environment (Chirico et al., 2019).
On the one hand, the effectiveness of VR lies in the intensity of this multisensory immersion called the sense of presence (Tennant et al., 2020), that is, the subjective experience of being in another place than the one where the individual is physically located (Witmer and Singer, 1998). On the other hand, its effectiveness depends on the patients’ sensory, cognitive, and emotional involvement as well as the level of acceptability of this tool (Garrett et al., 2020). The degree of engagement and interactivity are closely related to the sense of presence and increased attention to distraction, leading to an increase in the positive effects of VR (Birnie et al., 2018).
3.1.3.1 Anxiety/stress
The benefits of VR have been shown to affect anxiety in cancer patients (Chirico et al., 2019; Bani Mohammad and Ahmad, 2018; Pizzoli et al., 2019; Niki et al., 2019; Espinoza et al., 2012; Baños et al., 2013; Gupta and Hande, 2019; Higgins et al., 2019; Garrett et al., 2020; Gerçeker et al., 2020; Scates et al., 2020; Li et al., 2011; Tennant et al., 2020; Buche et al., 2021). Two-thirds of the selected studies focused on anxiety relief (14/22 studies, see Figure 3: Percentage of studies evaluating the effects of VR in oncology) (Chirico et al., 2019; Bani Mohammad and Ahmad, 2018; Niki et al., 2019; Johnson et al., 2020; Schneider et al., 2011; Li et al., 2016; Glennon et al., 2018; Gupta and Hande, 2019; Higgins et al., 2019; Gerçeker et al., 2020; Scates et al., 2020; Li et al., 2011; Tennant et al., 2020; Buche et al., 2021). In most cases, the application of VR as a distraction tool promotes a significant decrease in anxiety during chemotherapy sessions (Chirico et al., 2019), during hospitalization (Bani Mohammad and Ahmad, 2018; Niki et al., 2019; Gupta and Hande, 2019; Higgins et al., 2019; Tennant et al., 2020), during painful procedures (Gerçeker et al., 2020; Scates et al., 2020) and physiotherapy rehabilitation (Buche et al., 2021). Participative VR seems to be a more effective distractive strategy than music for improving emotional wellbeing (Chirico et al., 2019). Distraction is defined by Lazarus and Folkman’s (1984) stress and coping model (Lazarus et al., 1984) as a coping strategy, namely the set of cognitive and behavioral efforts intended to control, reduce, or tolerate an aversive situation (Chirico et al., 2019). Distraction under VR regulates patients’ emotional responses related to distressing medical procedures through selective attention that focuses attention on pleasant stimuli in the virtual environment. Thus, using participative VR is an active “vigilant” strategy, while listening to music is a distractive strategy that requires only passive attentional engagement on the part of patients.
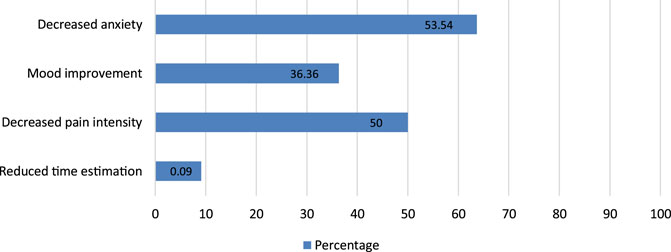
FIGURE 3. Percentage of studies evaluating the effects of VR in oncology.
Moreover, immersion in a natural environment significantly enhances the power of distraction by, among other things, leading to increased feelings of peace and relaxation in patients (Scates et al., 2020). Scates et al. (2020) support Kaplan and Kaplan’s (1989) (Kaplan and Kaplan, 1989) attention restoration theory that natural environments can refocus attention but also Ulrich et al.'s (1991) psychophysiological stress recovery theory (Ulrich et al., 1991) where positive distractions involving natural elements (e.g., trees, flowers, streams, etc.) help individuals combat stress. Beyond natural content, (Niki et al., 2019) speculate that retrieval of episodic memories involving the medial temporal lobe may promote decreased anxiety and depression (Ramirez et al., 2015). Thus, they suggest that the hippocampal region is particularly involved in the biological mechanisms by which a VR simulating a pleasant place already visited by the individual in the real world would alleviate anxiety and depression.
3.1.3.2 Mood improvement
As for the studies focused on mood improvement (8/22 studies), they generally show that VR can promote the emotional wellbeing of patients (Pizzoli et al., 2019; Niki et al., 2019; Buche et al., 2021; Li et al., 2011) by increasing positive emotions such as joy or happiness and decreasing negative emotions such as fear (Gerçeker et al., 2020), sadness (Espinoza et al., 2012; Baños et al., 2013) and anger (Tennant et al., 2020). Baños et al. (2013) refer to the broaden-and-build theory proposed by Fredrickson et al. (2001), which is based on positive psychology. According to this theory, the promotion and experience of positive emotions expand individuals’ momentary repertoires of thought-action. The ability to experience positive emotions can create and strengthen lasting personal resources that are useful for coping with difficult times during cancer management.
3.1.3.3 Perception of pain
Half of the studies presented in Table 1 focused on the reduction of pain intensity in oncology (11/22 studies) (Bani Mohammad and Ahmad, 2018; Niki et al., 2019; Johnson et al., 2020; Glennon et al., 2018; Garrett et al., 2020; Gerçeker et al., 2020; Atzori et al., 2018; Birnie et al., 2018; Semerci et al., 2020; Sharifpour et al., 2020; Tennant et al., 2020). The different results show that immersion in an artificial world is associated with an analgesic effect (Bani Mohammad and Ahmad, 2018; Niki et al., 2019; Garrett et al., 2020; Gerçeker et al., 2020; Atzori et al., 2018; Birnie et al., 2018; Semerci et al., 2020; Sharifpour et al., 2020; Tennant et al., 2020). VR is a pleasant and effective distraction strategy used to reduce pain during medical procedures that can be painful for patients, such as venipuncture (Atzori et al., 2018) or veinous port access (Gerçeker et al., 2020; Birnie et al., 2018; Semerci et al., 2020). The immersive and participative experience can significantly reduce the acute pain associated with treatments (Bani Mohammad and Ahmad, 2018; Birnie et al., 2018; Sharifpour et al., 2020; Tennant et al., 2020) and reduce chronic pain (Niki et al., 2019; Garrett et al., 2020). According to Eccleston and Crombez’s (1999) Attention Pain Theory (Eccleston and Crombez, 1999), the illusion of being in an artificial world and the patients’ interaction with objects in the virtual environment may reduce the amount of attention available to deal with painful stimuli, thus decreasing the perception of conscious pain (Atzori et al., 2018). Within the theory of Melzack and Wall (1960) (Melzack and Wall, 1996) entitled “Gate Control Theory of Pain,” the nervous system contains a neurological gateway controlled by the cortex that could either block the ascending and descending pain signals or allow their transmission to the brain to continue (Sharifpour et al., 2020). For example, attention and negative emotions such as fear and sadness can open this gateway, increasing pain perception. In contrast, distraction and positive emotions such as joy and calmness can close this gateway, decreasing pain perception. When the gateway is open, nociceptive messages are allowed to reach the brain; when it is closed, nociceptive messages are inhibited. Based on this model, distraction under VR can alleviate pain by decreasing negative emotions and favoring positive emotions, thus inducing a decrease in pain perception. In other words, virtual reality generates a slower reaction to pain reporting by acting on attention, emotion, and in a broader sense, cognition (Gold et al., 2007), (Arane et al., 2017).
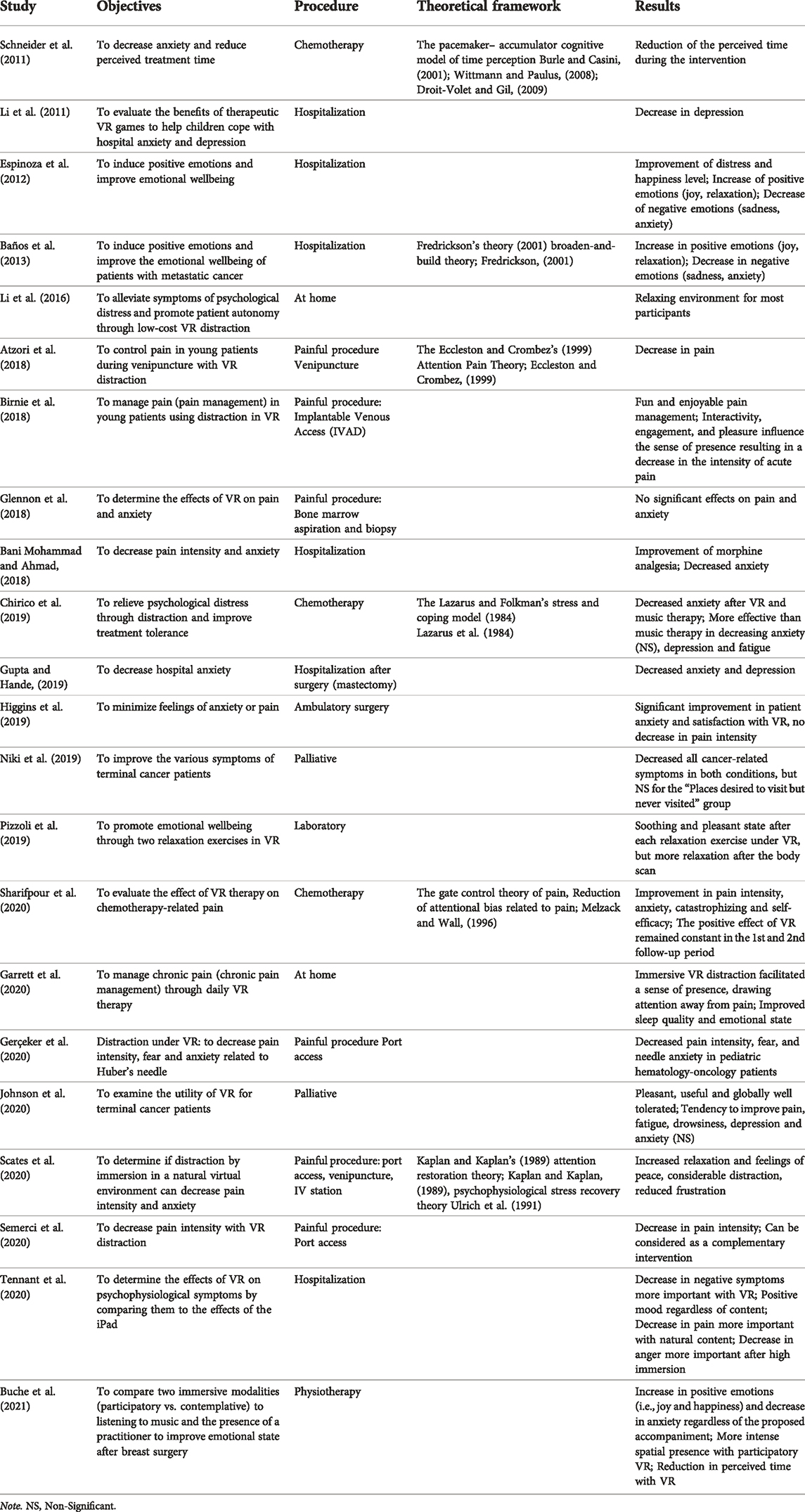
TABLE 1. Studies on the benefits of virtual reality.
3.1.3.4 Temporal perception
In the past 10 years, few studies have addressed the issue of time perception in oncology (Schneider et al., 2003; Schneider et al., 2004), (Schneider and Hood, 2007). One study (Schneider et al., 2011), based on the simulation-accumulation cognitive model (Burle and Casini, 2001; Wittmann and Paulus, 2008; Droit-Volet and Gil, 2009), explains the effects of distraction intervention on the perception of time. It seems that time spent under virtual immersion passes more quickly due to the decrease in heart rate and negative stimuli of the stressful context, thus diverting attention from processing temporal information.
3.1.4 Technological diversity
Although the literature has identified the advantages of distraction under VR in oncology (Michel et al., 2019a), the variety of the tools and methods used should be highlighted to define the optimal conditions for using VR and propose interfaces adapted to support cancer patients.
3.1.4.1 Hardware used
The vast majority of studies examined in this literature review take advantage of fully immersive devices through an HMD headset (86.36%, 19/22 studies) (Chirico et al., 2019; Bani Mohammad and Ahmad, 2018; Pizzoli et al., 2019; Niki et al., 2019; Johnson et al., 2020; Schneider et al., 2011; Li et al., 2016; Glennon et al., 2018; Gupta and Hande, 2019; Higgins et al., 2019; Garrett et al., 2020; Gerçeker et al., 2020; Scates et al., 2020; Buche et al., 2021; Atzori et al., 2018; Birnie et al., 2018; Semerci et al., 2020; Sharifpour et al., 2020; Tennant et al., 2020), while a minority (9.09%, 2/22 studies) use a device that researchers describe as “non-immersive” virtual reality for clinical purposes in oncology via a 32-inch LCD television screen connected to a computer, keyboard, mouse, and headset (Espinoza et al., 2012; Baños et al., 2013). Overall, the immersive devices used are smartphone VR headsets with the distinction of being low-cost systems (68.42%, 13/19 studies) (Chirico et al., 2019; Bani Mohammad and Ahmad, 2018; Pizzoli et al., 2019; Johnson et al., 2020; Li et al., 2016; Gupta and Hande, 2019; Higgins et al., 2019; Gerçeker et al., 2020; Scates et al., 2020; Buche et al., 2021; Semerci et al., 2020; Sharifpour et al., 2020; Tennant et al., 2020). In some cases, smartphones VR headsets are accompanied by headphone (Bani Mohammad and Ahmad, 2018; Birnie et al., 2018), or earphones (Pizzoli et al., 2019; Atzori et al., 2018), and joysticks (hand controllers) (Li et al., 2016; Birnie et al., 2018). Few researchers opt for systems as high-tech as the HCT VIVE headset (Niki et al., 2019; Higgins et al., 2019; Garrett et al., 2020), ez Vision X4 (Gupta and Hande, 2019) or Oculus Go (Buche et al., 2021) (26.31%, 5/19 studies). One study exploited a particular VR system (PlayMotion) (4.55%, 1/22 studies) in a playroom of a pediatric oncology department. This system has the particularity of increasing the immersive space by transforming the room into a totally intuitive and participative virtual environment since it does not require a headset or a controller. The software responds to patients’ actions by analyzing the shadows of moving limbs projected on the walls thanks to sensors.
3.1.4.2 Immersive environments
Regarding the content of virtual environments, a consensus emerges around natural relaxing environments (90.91% or 20/22 studies) (Chirico et al., 2019; Bani Mohammad and Ahmad, 2018; Pizzoli et al., 2019; Niki et al., 2019; Johnson et al., 2020; Schneider et al., 2011; Espinoza et al., 2012; Baños et al., 2013; Li et al., 2016; Glennon et al., 2018; Higgins et al., 2019; Garrett et al., 2020; Gerçeker et al., 2020; Scates et al., 2020; Atzori et al., 2018; Birnie et al., 2018; Semerci et al., 2020; Sharifpour et al., 2020; Tennant et al., 2020; Buche et al., 2021) rather than urban ones (13.64%, or 3/22 studies) (Espinoza et al., 2012; Baños et al., 2013), (Li et al., 2011). Thanks to the extent of research, we now have a range of natural environments that correspond to the demand of patients (Michel et al., 2019b). On the one hand, the environments are built with synthetic images such as sea worlds (Schneider et al., 2011; Glennon et al., 2018; Higgins et al., 2019; Gerçeker et al., 2020; Buche et al., 2021; Birnie et al., 2018; Sharifpour et al., 2020), forests (Pizzoli et al., 2019; Espinoza et al., 2012; Baños et al., 2013; Garrett et al., 2020; Gerçeker et al., 2020; Buche et al., 2021) paradise islands (Chirico et al., 2019; Bani Mohammad and Ahmad, 2018; Sharifpour et al., 2020; Buche et al., 2021) and mountains (Chirico et al., 2019) with waterfalls (Pizzoli et al., 2019), and on the other hand, the environments are created with images captured in 360° of real world destinations (Niki et al., 2019; Johnson et al., 2020; Gerçeker et al., 2020; Tennant et al., 2020). For some of them, this natural component is complemented by playful content (50%, 11/22 studies) which includes, for example, roller coaster simulations (Johnson et al., 2020; Gerçeker et al., 2020; Semerci et al., 2020) or space travel (Johnson et al., 2020; Garrett et al., 2020). Some studies include educational (Bani Mohammad and Ahmad, 2018; Gerçeker et al., 2020), enigmatic (Schneider et al., 2011; Garrett et al., 2020), creative (Higgins et al., 2019; Li et al., 2011), cultural (Schneider et al., 2011; Tennant et al., 2020), musical (Garrett et al., 2020), or sports games (Li et al., 2011) environments. Some studies are not standardized and vary accordingly to content by integrating mixed environments (i.e., playful and relaxing) (18.18%, 4/22 studies) (Johnson et al., 2020; Higgins et al., 2019; Garrett et al., 2020; Gerçeker et al., 2020) with still images while others involve videos (Johnson et al., 2020).
3.1.4.3 Interactivity
The diversity of the devices also concerns the levels of sensorimotor interactivity. Contemplative VR inviting patients to observe the virtual environment (45.45%, 10/22 studies) (Pizzoli et al., 2019; Niki et al., 2019; Espinoza et al., 2012; Baños et al., 2013; Glennon et al., 2018; Garrett et al., 2020; Buche et al., 2021; Semerci et al., 2020; Sharifpour et al., 2020; Tennant et al., 2020), is opposed to participative VR, called participative VR, which offers patients the possibility to act as an actor in the virtual world (27.27%, 6/22 studies) (Chirico et al., 2019; Li et al., 2016; Buche et al., 2021; Li et al., 2011; Atzori et al., 2018; Birnie et al., 2018). Almost a third of the studies do not control for this participative variable that involves patients to different degrees in immersive experiences (27.27%, 6/22 studies) (Bani Mohammad and Ahmad, 2018; Johnson et al., 2020; Schneider et al., 2011; Higgins et al., 2019; Garrett et al., 2020; Gerçeker et al., 2020) or do not report on the sensorimotor interaction between patients and the virtual device (4.55%, 1/22 studies) (Gupta and Hande, 2019). Contemplative immersions consist of passive observation of virtual environments (Bani Mohammad and Ahmad, 2018; Glennon et al., 2018) with sometimes the possibility of navigating (Espinoza et al., 2012; Baños et al., 2013; Buche et al., 2021; Tennant et al., 2020) or performing meditation (Johnson et al., 2020; Garrett et al., 2020) and relaxation exercises such as the control of breathing frequencies (Espinoza et al., 2012; Baños et al., 2013) or the focusing of attention on physical sensations to improve emotional wellbeing (Pizzoli et al., 2019). Participatory immersions offer multiple possibilities of actions such as participative explorations by body limb movements (Chirico et al., 2019; Bani Mohammad and Ahmad, 2018; Gerçeker et al., 2020; Buche et al., 2021; Li et al., 2011) or educational ones by information retrieval (Bani Mohammad and Ahmad, 2018; Li et al., 2011). Explorations require solving mysteries by strategically choosing different options to advance in the scenario (Schneider et al., 2011; Garrett et al., 2020). Others consist in modifying objects in the environment (Li et al., 2016; Buche et al., 2021) or in painting one’s environment in three dimensions (Higgins et al., 2019; Li et al., 2011). Finally, target games allow the patient to aim at characters or objects present in the environment by pointing with the use of game controllers (Johnson et al., 2020; Birnie et al., 2018) or a computer mouse and keyboard (Atzori et al., 2018).
3.1.4.4 Audio and sound
Apart from the visual contents and their participative potentialities, there is a form of consensus on the need to solicit the auditory sensory modality (Bani Mohammad and Ahmad, 2018; Pizzoli et al., 2019; Johnson et al., 2020; Espinoza et al., 2012; Baños et al., 2013; Li et al., 2016; Glennon et al., 2018; Garrett et al., 2020; Gerçeker et al., 2020; Scates et al., 2020; Buche et al., 2021; Semerci et al., 2020; Sharifpour et al., 2020). This auditory component is thought to favor the immersive experience that increases the intensity of the sense of presence in the virtual world. However, we notice a certain heterogeneity regarding the aural characteristics of the proposed devices. Some immersions are enhanced by a background sound related to the virtual environment (e.g., nature sounds, sound feedback, educational narration) (Bani Mohammad and Ahmad, 2018; Gerçeker et al., 2020; Scates et al., 2020; Buche et al., 2021; Sharifpour et al., 2020), whereas others are accompanied by soothing musical stimuli (Li et al., 2016; Glennon et al., 2018; Garrett et al., 2020; Buche et al., 2021; Semerci et al., 2020) associated with guided relaxation (Johnson et al., 2020; Espinoza et al., 2012; Baños et al., 2013) with the help of a qualified yoga and mindfulness instructor (Pizzoli et al., 2019).
3.1.5 Methodological diversity
3.1.5.1 Experimental design
Beyond the technological diversity, there are differences in the scientific methodologies used. These differences can be observed in terms of the comparison of experimental methods. Almost half of the studies do not compare distraction under VR to a control group or to another form of distraction (40.91%, 9/22 studies) (Pizzoli et al., 2019; Niki et al., 2019; Johnson et al., 2020; Espinoza et al., 2012; Baños et al., 2013; Li et al., 2016; Gupta and Hande, 2019; Higgins et al., 2019; Birnie et al., 2018). As for the control groups, they consist of apprehending the medical act without distraction (50%) (Chirico et al., 2019; Bani Mohammad and Ahmad, 2018; Niki et al., 2019; Schneider et al., 2011; Glennon et al., 2018; Gerçeker et al., 2020; Scates et al., 2020; Buche et al., 2021; Atzori et al., 2018; Semerci et al., 2020; Sharifpour et al., 2020). Thus, the difference between the groups could be due to using a distractive device rather than the specific use of VR. Only 22.73% of the research (5/22 studies) compared the virtual device to another distractive mode, either by presenting the same content through another medium (i.e., computer, television, or tablet: 13.64%) (Glennon et al., 2018; Garrett et al., 2020; Tennant et al., 2020) or by comparing VR to music (9.09%) (Chirico et al., 2019; Buche et al., 2021). According to the reported results, VR was more conducive to reducing negative symptoms with a greater decrease in anger levels after more intense immersion (Tennant et al., 2020). A gender effect was found with a higher increase in positive mood with VR than with iPad in young females (Tennant et al., 2020). Therefore, VR may be a more powerful form of distraction than tablet games by facilitating a sense of presence in a new environment diverting attention from pain (Garrett et al., 2020). Similarly, VR has been shown to be more effective than music therapy in relieving depression and fatigue (Chirico et al., 2019). VR was also more effective than listening to classical music in reducing estimated care time regardless of whether the immersion was participative or passive (Buche et al., 2021).
3.1.5.2 Familiarization
Only six out of twenty-two studies implemented a familiarization phase before starting the real immersive experience (27.27%), (Chirico et al., 2019; Johnson et al., 2020; Gupta and Hande, 2019; Gerçeker et al., 2020; Atzori et al., 2018; Scates et al., 2020). The studies that implemented this familiarization phase in their research protocol showed significant results in reducing anger, pain, and anxiety (83.33%, 5/6 studies). This step might be necessary to decrease the surprise effect and the naive attractiveness of the patients to obtain a more accurate measure of their emotional states associated with the virtual immersion (Buche et al., 2021). These familiarization phases nevertheless present methodological differences. The most frequent method consists of the experimenter accompanying the patients to guide them during their first manipulations (50%, 3/6 studies), (Chirico et al., 2019; Johnson et al., 2020; Atzori et al., 2018). In comparison, others consist in viewing a handholding video during which the patient can practice (16.66%, 1/6 studies) (Tennant et al., 2020) or start the immersion a few minutes before the medical procedure (16.66%, 1/6 studies) (Gerçeker et al., 2020). In daily VR exposures, this familiarization phase can result in a short immersion of 10 min on the first day of experimentation with a progressive increase in immersion time going up to 30 min per day (16.66%, 1/6 studies) (Gupta and Hande, 2019).
3.1.5.3 Duration of immersion
The duration varies mainly according to the duration of the medical act. For short painful procedures such as catheter insertion or venipuncture, immersion varies from 3 to 18 min (Glennon et al., 2018; Buche et al., 2021; Scates et al., 2020; Atzori et al., 2018; Birnie et al., 2018; Semerci et al., 2020). When the context allows for a longer immersion, as is the case in chemotherapy, during long-term hospitalization or on return home, VR is proposed between 10 and 63 min (Schneider et al., 2011; Higgins et al., 2019; Tennant et al., 2020; Buche et al., 2021), although in 60% of cases (i.e., 9/15 studies), the immersion time mainly applied by the experimenters corresponds to 30 min (Niki et al., 2019; Johnson et al., 2020; Espinoza et al., 2012; Baños et al., 2013; Li et al., 2016; Gupta and Hande, 2019; Garrett et al., 2020; Li et al., 2011; Sharifpour et al., 2020). Most virtual immersions lasting 30 min reported positive effects (88.88%, 8/9 studies) (Niki et al., 2019; Espinoza et al., 2012; Baños et al., 2013; Li et al., 2016; Gupta and Hande, 2019; Garrett et al., 2020; Li et al., 2011; Sharifpour et al., 2020). According to the diversity of the medical act in which VR is proposed, there is no strong consensus on the most favorable duration of immersion.
In terms of measurement tools (See Table 2: Nature of measures and instruments in studies evaluating the effects of VR in oncology), most studies collected quantitative data (21/22, 95.45%). Only one study used a qualitative inductive approach using the interpretive description method to explore participants’ experiences (Garrett et al., 2020). Seven studies collected qualitative data (31.82%) (Baños et al., 2013; Li et al., 2016; Higgins et al., 2019; Scates et al., 2020; Buche et al., 2021; Birnie et al., 2018; Sharifpour et al., 2020). Only two studies (9.09%) collected physiological data such as blood pressure, pulse rate, respiration, temperature, and percent oxygen saturation using an oximeter (Glennon et al., 2018; Tennant et al., 2020).
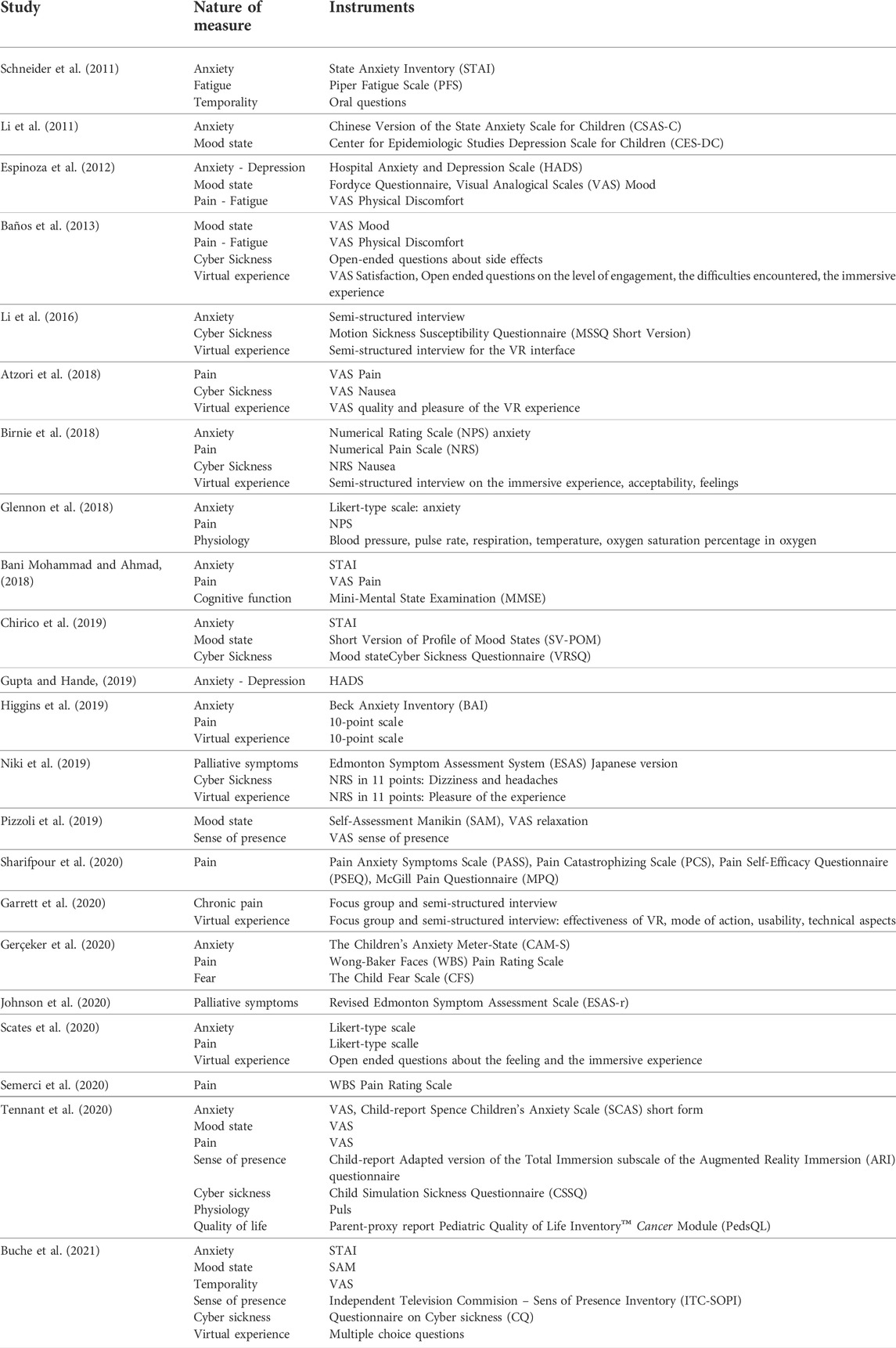
TABLE 2. Nature of measure and instruments in studies evaluating the effects of virtual reality in oncology.
Regarding measures reflecting emotional state, anxiety was mainly measured using the State Anxiety Inventory (STAI) (Chirico et al., 2019; Bani Mohammad and Ahmad, 2018; Schneider et al., 2011; Buche et al., 2021) and depression using the Hospital Anxiety Depression Scales (HADS). Mood states were most often assessed using the Visual Analogical Scales (VAS) (Pizzoli et al., 2019; Espinoza et al., 2012; Baños et al., 2013; Tennant et al., 2020) and the Self-Assessment Manikin (SAM) (Pizzoli et al., 2019; Buche et al., 2021). Concerning pain, most researchers have opted for scales (see Table 2: Nature and measurement tools in studies evaluating the effects of VR in oncology) (Bani Mohammad and Ahmad, 2018; Espinoza et al., 2012; Baños et al., 2013; Glennon et al., 2018; Higgins et al., 2019; Scates et al., 2020; Atzori et al., 2018; Birnie et al., 2018; Semerci et al., 2020; Tennant et al., 2020), while others have used specific questionnaires to measure several components of pain such as pain anxiety, catastrophizing, self-efficacy and intensity (Sharifpour et al., 2020). In addition, the Edmonton Symptom Assessment System (ESAS) questionnaire has been used to assess the various symptoms of palliative cancer (Niki et al., 2019; Johnson et al., 2020). The question of temporality was asked orally (Schneider et al., 2011) or by using a VAS from 0 to 40 min with a 5-min interval (Buche et al., 2021).
Semi-structured interviews (Li et al., 2016; Garrett et al., 2020; Birnie et al., 2018) accompanied by various scales (Higgins et al., 2019) (Baños et al., 2013) and supplemented by open-ended (Baños et al., 2013; Scates et al., 2020) or multiple-choice questions (Buche et al., 2021) were conducted to examine the virtual experience with patients. Discomfort that could be caused by the virtual device was monitored through different questionnaires (Chirico et al., 2019; Li et al., 2016; Tennant et al., 2020; Buche et al., 2021), scales (Niki et al., 2019; Birnie et al., 2018; Atzori et al., 2018) and open-ended questions (Baños et al., 2013). Only three studies (13.64%) assessed the subjective feeling of presence in the virtual world using questionnaires (Tennant et al., 2020; Buche et al., 2021) or a VAS (Pizzoli et al., 2019).
In addition, uncommon measures in VR in oncology were collected: one study assessed cognitive function to screen for cognitive impairment in hospitalized adults and determine patients’ ability to manipulate the virtual device (Bani Mohammad and Ahmad, 2018). Another assessed quality of life in young patients (Tennant et al., 2020).
3.2 Research recommendations
Based on the twenty-two studies selected, this third part aims to optimize the methodological choices made in the studies by encouraging the use of practices that are comparable from one study to another for a more rigorous comparison of the reported effects. From a strictly methodological point of view, it seems promising to continue the reflection already initiated at several levels: the degree of interactivity of the devices to be proposed to the patients; the contents to be preferred; the duration of the distractive session; the context of use.
Given the literature, it seems that having access to dynamic feedback from our actions in the virtual environment is a primary criterion for giving patients the feeling of being immersed inside this environment (Chirico et al., 2019; Buche et al., 2021). Participatory immersion can provide better experiential quality than contemplative immersion by actively engaging patients (Garrett et al., 2020). Future studies should evaluate the links between immersive quality and distraction power benefits under VR to leverage this finding. It is worth noting that the auditory component contributes to the immersion of patients in the virtual world (Michel et al., 2019b) as this is notably the case of natural environments enhanced with background sound, relaxing music, or guided relaxation. These results are more convincing when the technology allows a qualitative VR experience. Devices with high technological quality promote the feeling of presence (Cummings and Bailenson, 2016) and the quality of the distraction. In summary, the better the technical quality, the more intense the transport into the virtual environment.
If there is a consensus on the need to present patients with natural and high-definition sound content, developing new and constantly renewed content is essential to overcome the phenomenon of habituation. A regularly updated system could preserve the awe of this innovative device and continue to captivate patients even after repeated immersions. The exploitation of future software should further engage the patient in the immersive task mobilizing his cognitive resources at different levels ranging from distraction to concentration or skill reinforcement (Ahmadpour et al., 2020).
Although VR is a promising technology, there are still some limitations to applying this distractive tool in oncology. To date, it is difficult to recommend an immersive duration most conducive to patients’ emotional comfort. It would be interesting to evaluate the differential effects of time immersed in the virtual environment (Tennant et al., 2020). Immersion time seems to be determined by the nature and duration of medical procedures and not by the relaxation/distraction needs of the patient. Thus, devices that adapt the duration of immersion to individual patient needs and preferences would be a considerable asset to enhance the benefits of distraction.
The context of VR use essentially conditions the duration of immersion. However, specific methodological recommendations can be retained. Given the observed results, an extended hospitalization allows a progressive increase in immersion time, allowing the patients to become a little more familiar with the virtual device each day (Gupta and Hande, 2019). To ensure the benefits of VR, it would be preferable that the virtual experience not exceed 30 min per day during a long-term hospitalization (Niki et al., 2019; Johnson et al., 2020; Espinoza et al., 2012; Baños et al., 2013; Gupta and Hande, 2019; Li et al., 2011). During an outpatient hospitalization involving short, painful procedures such as port access or venipuncture, it would seem appropriate that the immersion starts 2–5 min before the medical act (familiarization phase) and continues until the end of the procedure (experimental phase) (Buche et al., 2021; Atzori et al., 2018). In chemotherapy, following Chirico et al. (2019), a familiarization phase of 5–10 min could be introduced to optimize the effects of the virtual experience. As for the duration of the immersive experience during the administration of chemotherapy, there is currently no consensus in the literature to propose a recommendation (Chirico et al., 2019; Schneider et al., 2011; Sharifpour et al., 2020).
When examining the benefits using VR in oncology, it is regrettable to note the absence of a control condition in nearly half of the studies (Pizzoli et al., 2019; Niki et al., 2019; Johnson et al., 2020; Espinoza et al., 2012; Baños et al., 2013; Li et al., 2016; Gupta and Hande, 2019; Higgins et al., 2019; Birnie et al., 2018). In the future, researchers should design randomized controlled studies that compare medical care using VR for distraction with the same care without using distraction (i.e., a control condition) as well as this same care using other distractive strategies (i.e., different conditions) to reveal in a more rigorous comparison setting the true effectiveness of virtual immersion in oncology.
In addition, some measurement tools are not systematically used. Assessing the risk of side effects from virtual devices is helpful to ensure that VR is well tolerated by patients. This also allows us to distinguish between the physical discomfort of treatment and those that VR may cause. Future studies evaluating the effects of VR through physiological variables such as heart rate, oxygenation rate, or skin conductance could refine the assessment of patients’ emotional states (Chirico et al., 2019). The measurement of the subjective sense of presence in the virtual environment should be systematized in oncology, knowing that this feeling is closely linked to the sensation of escape (Tennant et al., 2020; Witmer and Singer, 1998).
Furthermore, the effectiveness of VR depends on personal acceptance (Garrett et al., 2020) and patient interest in the device (Lessiter et al., 2001). It may be that the positive results reported in the literature are partly a result of the acceptance rate at recruitment and the predisposition of patients to the virtual experience. Patients who prefer to maintain control and observe the routine of care may be more likely to decline the experience, while patients who are more open to the device may already be in a favorable emotional state to use VR. Future research should not neglect to assess patient enjoyment and motivation to engage in the immersive experience to consider their level of involvement in the immersion. Like (Bani Mohammad and Ahmad, 2018), future studies would benefit from considering the patient’s ability to process sensorimotor information from VR through the measurement of cognitive impairments to ensure an optimal relaxing experience.
Finally, this device is considered an effective distractive strategy when it fulfills certain conditions according to the medical context, but even more so according to the patient’s needs at the time. As we have seen in the study by Buche et al. (2021), VR can be used not only to distract from anxiety-provoking or painful experiences during treatment but also to compensate for the monotonous nature of the treatments. It can also be used when the practitioners are unavailable, for instance, if they have other things to manage than the patient relationship.
3.3 Theoretical model
The richness of the available scientific literature and the exploitation of the state of the art allow us to think of an integrative theoretical model that considers the effects of VR on both the cognitive and emotional levels. Articulating the cognitive and emotional sides will enable us to envisage a valid and robust schematic representation aligned with the benefits reported in oncology and the theories mentioned (see Table 1: Studies of the Benefits of VR). Based on this careful exploitation of the current state of knowledge and the methodological and theoretical choices made by the community, we propose an explanatory model of the effects of exposure to VR (see Figure 4: Model of the mechanisms involved in VR distractive experience and underlying its benefits) to contribute to the understanding of the processes leading to the emergence of the positive effects of virtual immersion with cancer patients during medical interventions. This model is based on an ideal situation where the use of VR as a distractive tool has been preceded by a familiarization phase (i.e., when the handling of the device is no longer likely to hinder the relaxing experience).
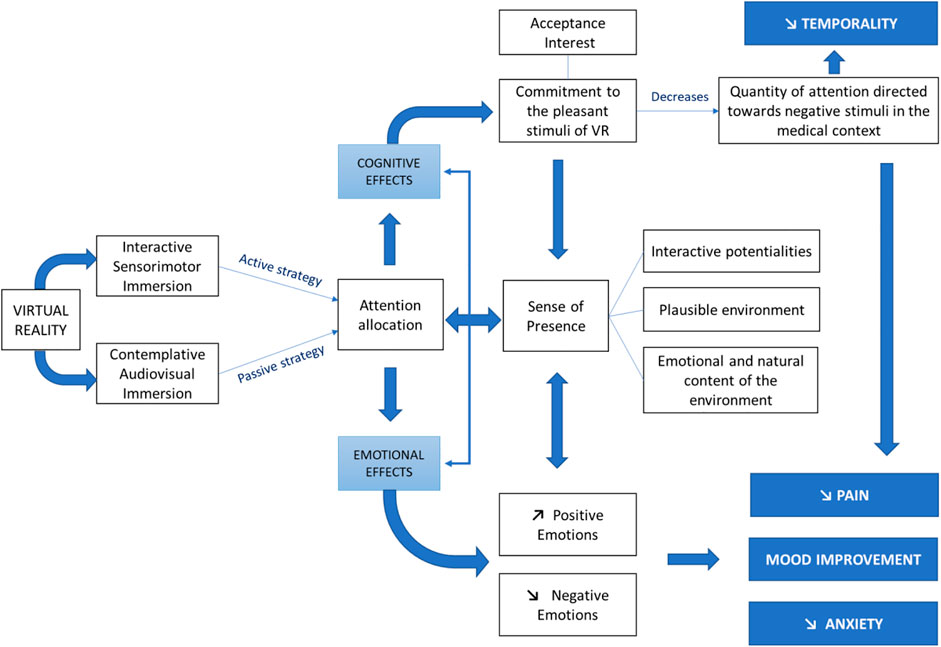
FIGURE 4. Model of the mechanisms involved in VR distractive experience and underlying its benefits.
The theoretical basis of our model is mainly based on the allocation of attentional resources related to the limited cognitive capacities of human beings (Arane et al., 2017). As stated above, we consider that VR can offer several levels of immersion involving different senses simultaneously (Chirico et al., 2019). The immersive technologies employed can mobilize active or passive cognitive strategies that aim to reduce attention to the physical environment. The first effect of multimodal immersion is to spontaneously draw attention to pleasurable VR stimuli by passively or actively engaging the patient in the virtual experience. Engagement or involvement is a state of strong concentration in which the patient no longer directs their conscious attention towards external negative stimuli and forgets the medical context in which they are situated. This results in a feeling of presence, that is, the impression that the patient is escaping into a world other than their real-world (Witmer and Singer, 1998). According to the presence model (Lessiter et al., 2001), the immersive task depends mainly on the individual’s interest in the experience. However, these authors underline that the device’s immersive qualities and participative potentialities are likely to awaken or hinder the interest in VR.
It should be noted that the immersive qualities determine the credibility of the experience by recreating the perceptive attributes (e.g., tracking level, stereoscopy, and field of view) that a person can find in physical reality (Cummings and Bailenson, 2016). Thus, the level of engagement, interactivity, and plausible environment influence the prevalence of presence which focuses attention on immersion. Since fantasy environments can also benefit patients (Pourmand et al., 2018), most oncology studies used believable natural environments. In addition to inducing a sense of presence, the cognitive resources mobilized modify the perception of temporality by giving the impression that time is passing more rapidly within the virtual environment. Furthermore, the attentional engagement in the immersive task affects the cognitive evaluation of pain by reducing the amount of attention available to process the painful information, thus attenuating the pain felt (Eccleston and Crombez, 1999; Atzori et al., 2018).
Moreover, the cognitive effects maintain a virtuous circle with the emotional effects generated by this distractive strategy. VR is a medium capable of increasing positive emotions and decreasing negative emotions thanks to immersion in a natural environment (Scates et al., 2020), which carries positive emotions (Baños et al., 2013). Riva et al. (2007) have demonstrated the bidirectional relationship between emotions and presence: A relaxing environment generates a higher sense of presence than a neutral environment, and once the sense of presence is established, positive emotions are felt more intensely (Bouvier, 2009). This emotional induction not only decreases anxiety and improves mood by inducing joy and calmness but also influences pain perception. Attention focused on positive emotions inhibits the nociceptive message conveyed by the nervous system, which leads to a decrease in the intensity of the pain felt (Sharifpour et al., 2020; Melzack and Wall, 1996).
4 Discussion
Based on the accumulated results, which primarily convey a positive image of VR, there is no doubt today that the use of this technology is of major interest. However, the beneficial effects regularly reported must be understood in terms of the characteristics of the technology used and according to the particularities of the patients and their immersion preferences.
The objective of this article is twofold, given the converging and diverging points highlighted in this literature review. The first is identifying avenues for harmonizing the procedures and tools used in future research. This analysis of the current state of practice in measuring the effects of VR in oncology synthesizes the data accumulated over the past decade on the distractive power of VR in oncology. Based on this analysis, the scientific community has the means to move towards a more substantial consensus to encourage more rigorous reflection by clarifying methodological regularities. Secondly, this article invites the scientific community to consider more systematically the need for a theoretical foundation that contributes to consolidating the understanding of the processes at work in the results reported in the scientific literature used in this article. While some authors have attempted to explain the psychological phenomena that underlie the benefits of VR, few of them have articulated their approach to theoretical models of reference. The theoretical model proposed in this article considers the available knowledge and provides a promising framework for future studies that aim to deepen the cognitive and emotional processes at stake during the use of VR. Our framework describes the broader impact of VR benefits concerning cognitive and emotional regulation. The medical context (cancer) from which our theoretical model has emerged could be applied broadly where pain and anxiety reduction are critical (e.g., child dental care (Du et al., 2022), wound care and rehabilitation after burns (Czech et al., 20221028), skin prick testing (Stassart and Giebels, 2022). Also, other sectors beyond healthcare can substantially contribute to testing the validity of our theoretical framework. Indeed, there is no doubt that the potentialities offered by our framework would benefit from being considered outside the medical context to ensure the robustness and generalizability of its articulation between emotion and cognition.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding authors.
Author contributions
All authors listed have made a substantial direct and intellectual contribution to the workand approved it for publication.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Ahmad, M., Bani Mohammad, E., and Anshasi, H. A. (2020). Virtual reality technology for pain and anxiety management among patients with cancer: A systematic review. Pain Manag. Nurs. doi:10.1016/j.pmn.04.002
Ahmadpour, N., Keep, M., Janssen, A., Rouf, A. S., and Marthick, M. (2020). Design strategies for virtual reality interventions for managing pain and anxiety in children and adolescents: Scoping review. JMIR Serious Games 8 (RM), e14565. doi:10.2196/14565
Alawneh, A., Anshasi, H., Khirfan, G., Yaseen, H., and Quran, A. (2017). Symptom prevalence of patients with cancer in a tertiary cancer center in Jordan. Gulf J. Oncol. 1, 37–43.
Arane, K., Behboudi, A., and Goldman, Ran. D. (2017). Virtual reality for pain and anxiety management in children. Can. Fam. Physician 63, 932–934.
Arrieta, O., Angulo, L., Núnez-Valencia, C., Dorantes-Gallareta, Y., Macedo, E., Martínez-Lopez, D., et al. (2013). As-sociation of depression and anxiety on quality of life, treatment adherence, and prognosis in patients with advanced non-small cell lung cancer. Ann. Surg. Oncol. 20, 1941–1948. doi:10.1245/s10434-012-2793-5
Atzori, B., Hoffman, H. G., Vagnoli, L., Patterson, D. R., Alhalabi, W., Messeri, A., et al. (2018). Virtual reality analgesia during venipuncture in pediatric patients with onco-hematological diseases. Front. Psychol. 9, 2508. doi:10.3389/fpsyg.2018.02508
Bani Mohammad, E., and Ahmad, M. (2018). Virtual reality as a distraction technique for pain and anxiety among patients with breast cancer: A randomized control trial. Palliat. Support. Care 17, 29–34. doi:10.1017/s1478951518000639
Baños, R. M., Espinoza, M., García-Palacios, A., Cervera, J. M., Esquerdo, G., Barrajón, E., et al. (2013). A positive psychological intervention using virtual reality for patients with advanced cancer in a hospital setting: A pilot study to assess feasibility. Support. Care Cancer 21, 263–270. doi:10.1007/s00520-012-1520-x
Birnie, K. A., Kulandaivelu, Y., Jibb, L., Hroch, P., Positano, K., Robertson, S., et al. (2018). Usability testing of an interactive virtual reality distraction intervention to reduce procedural pain in children and adolescents with cancer. J. Pediatr. Oncol. Nurs. 35, 406–416. doi:10.1177/1043454218782138
Bouvier, P. (2009). La présence en réalité virtuelle, une approche centrée utilisateur. Thèse de 699 doctorat en informatique. Paris: Université de Paris-Est.
Buche, H., Michel, A., Piccoli, C., and Blanc, N. (2021). Contemplating or acting? Which immersive modes should Be favored in virtual reality during physiotherapy for breast cancer rehabilitation. Front. Psychol. 12, 631186. doi:10.3389/fpsyg.2021.631186
Burle, B., and Casini, L. (2001). Dissociation between activation and attention effects in time estimation: Implications for internal clock models. J. Exp. Psychol. Hum. Percept. Perform. 27, 195–205. doi:10.1037/0096-1523.27.1.195
Chirico, A., Lucidi, F., De Laurentiis, M., Milanese, C., Napoli, A., Giordano, A., et al. (2016). Virtual reality in health system: Beyond entertainment. A mini‐review on the efficacy of VR during cancer treatment. J. Cell. Physiol. 231, 275–287. doi:10.1002/jcp.25117
Chirico, A., Lucidi, F., Mallia, L., D'Aiuto, M., and Merluzzi, T. V. (2015). Indicators of distress in newly diagnosed breast cancer patients. PeerJ 3, 1107. doi:10.7717/peerj.1107
Chirico, A., Maiorano, P., Indovina, P., Milanese, C., Giordano, G. G., Alivernini, F., et al. (2019). Virtual reality and music therapy as distraction interventions to alleviate anxiety and improve mood states in breast cancer patients during chemotherapy. J. Cell. Physiol. 235, 5353–5362. doi:10.1002/jcp.29422
Cummings, J. J., and Bailenson, J. N. (2016). How immersive is enough? A meta-analysis of the effect of immersive technology on user presence. Media Psychol. 19 (2), 272–309. doi:10.1080/15213269.2015.1015740
Czech, O., Wrzeciono, A., Baťalík, B., Szczepańska-Gieracha, S. G., Malicka, I., Rutkowski, S., et al. (202210283). Virtual reality intervention as a support method during wound care and rehabilitation after burns: A systematic review and meta-analysis. Complementary Ther. Med. 68. doi:10.1016/j.ctim.2022.102837
de Loor, P., and Tisseau, J. (2011). Réalité Virtuelle et énaction. J. de l’Association Française de Réalité Virtuelle 3. ffhal-00603993f.
Defossez, G., Le Guyader-Peyrou, S., Uhry, Z., Grosclaude, P., Colonna, M., Dantony, E., et al. (2019). Estimations nationales de l’incidence et de la mortalité par cancer en France métropolitaine 35 entre 1990 et 2018. Volume 1 – tumeurs solides. Saint-Maurice (Fra). Saint-Maurice: Santé publique France, 372.
Droit-Volet, S., and Gil, S. (2009). The time–emotion paradox. Phil. Trans. R. Soc. B 364, 1943–1953. doi:10.1098/rstb.2009.0013
Du, Q., Ma, X., Wang, S., Zhou, S., Luo, C., Tian, K., et al. (2022). A digital intervention using virtual reality helmets to reduce dental anxiety of children under local anesthesia and primary teeth extraction: A randomized clinical trial. Brain Behav. 12, e2600. doi:10.1002/brb3.2600
Eccleston, C., and Crombez, G. (1999). Pain demands attention: A cognitive– affective model of the interruptive function of pain. Psychol. Bull. 125, 356–366. doi:10.1037/0033-2909.125.3.356
Espinoza, M., Baños, R. M., Garcia-Palacios, A., Cervera, J. M., Esquerdo, G., Barrajon, E., et al. (2012). Promotion of emotional wellbeing in oncology inpatients using VR. Stud. Health Technol. Inf. 181, 53–57.
Fredrickson, B. (2001). The role of positive emotions in positive psychology. The broaden-and-build theory of positive emotions. Am. Psychol. 56, 218–226. doi:10.1037/0003-066x.56.3.218
Garrett, B. M., Tao, G., Taverner, T., Cordingley, E., and Sun, C. (2020). Patients perceptions of virtual reality therapy in the management of chronic cancer pain. Heliyon 6, e03916. doi:10.1016/j.heliyon.2020.e03916
Gerçeker, G. Ö., Bektaş, M., Aydınok, Y., Ören, H., Ellidokuz, H., Olgun, N., et al. (2020). The effect of virtual reality on pain, fear, and anxiety during access of a port with huber needle in pediatric hematology-oncology patients: Randomized controlled trial. Eur. J. Oncol. Nurs. 50, 101886. doi:10.1016/j.ejon.2020.101886
Glennon, C., McElroy, S., Connelly, L., MischeLawson, L., Bretches, A., Gard, A., et al. (2018). Use of virtual reality to distract from pain and anxiety. Oncol. Nurs. Forum 45, 545–552. doi:10.1188/18.onf.545-552
Gold, J. I., Belmont, K. A., and Thomas, D. A. (2007). The neurobiology of virtual reality pain attenuation. CyberPsychol. Behav. 10, 536–544. doi:10.1089/cpb.2007.9993
Gupta, N., and Hande, D. (2019). Is virtual reality program is effective in reducing anxiety in post mastectomy among breast cancer patient? Int. J. Multidiscip. Res. Dev. 6, 32–35.
Higgins, S., Feinstein, S., Hawkins, M., Cockburn, M., and Wysong, A. (2019). Virtual reality to improve the experience of the mohs patient-A prospective interventional study. Dermatol. Surg. doi:10.1097/DSS.000000000000001854
Indovina, P., Barone, D., Gallo, L., Chirico, A., De Pietro, G., Giordano, A., et al. (2018). Virtual reality as a distraction intervention to relieve pain and distress during medical procedures. Clin. J. Pain 34, 858–877. doi:10.1097/ajp.0000000000000599
Institut National du Cancer (2019). Les cancers en France : l’essentiel des faits et des chiffres. https://www.oncorif.fr/wpcontent/uploads/2019/02/Cancers_en_FranceEssentiel_Faits_et_chiffres-2018.pdf.
Johnson, T., Bauler, L., Vos, D., Hifko, A., Garg, P., Ahmed, M., et al. (2020). Virtual reality use for symptom management in palliative care: A pilot study to assess user perceptions. J. Palliat. Med. 23, 1233–1238. doi:10.1089/jpm.2019.0411
Kaplan, R., and Kaplan, S. (1989). The experience of nature: A psychological perspective. Cambridge University Press.
Kleiber, C., and Harper, D. C. (1999). Effects of distraction on children's pain and distress during medical procedures: A metaanalysis. Nurs. Res. 48, 44–49. doi:10.1097/00006199-199901000-00007
Kleiber, C., and McCarthy, A. M. (2006). Evaluating instruments for a study on children's responses to a painful procedure when parents are distraction coaches. J. Pediatr. Nurs. 21, 99–107. doi:10.1016/j.pedn.2005.06.008
Koller, D., and Goldman, R. D. (2012). Distraction techniques for children undergoing procedures: A critical review of pediatric research. J. Pediatr. Nurs. 27, 652–681. doi:10.1016/j.pedn.2011.08.001
Lazarus, R. S., and Folkman, S. (1984). “Stress, appraisal, and coping,” in Behaviour research and therapy. Editor S. P. Company. doi:10.1016/0005.7967(85)90087.7
Lessiter, J., Freeman, J., Keogh, E., and Davidoff, J. (2001). A cross-media presence questionnaire: The ITC-Sense of Presence Inventory. Presence. (Camb). 10, 282–297. doi:10.1162/105474601300343612
Li, W. H., Chung, J. O., and Ho, E. K. (2011). The effectiveness of therapeutic play, using virtual reality computer games, in promoting the psychological wellbeing of children hospitalised with cancer. J. Clin. Nurs. 20, 2135–2143. doi:10.1111/j.1365-2702.2011.03733.x
Li, Z., Han, X. G., Sheng, J., and Ma, S. J. (2016). Virtual reality for improving balance in patients after stroke: A systematic review and metaanalysis. Clin. Rehabil. 30, 432–440. doi:10.1177/0269215515593611
Melzack, R., and Wall, P. D. (1996). Pain mechanisms: A new theory. Pain Forum 5, 3–11. doi:10.1016/s1082-3174(96)80062-6
Michel, A., Brigaud, E., Cousson-Gélie, F., Vidal, J., and Blanc, N. (2019). La réalité virtuelle chez les femmes âgées suivies pour un cancer du sein : Intérêts et attentes. Geriatr. Psychol. Neuropsychiatr. Vieil. 17, 415–422. doi:10.1684/pnv.2019.0832
Michel, A., Vidal, J., Brigaud, E., Sokratous, K., and Blanc, N. (2019). Dessine-moi une réalité plus belle : La réalité virtuelle vue par les patientes atteintes d’un cancer du sein. Psycho-Oncol. 13, 69–78. doi:10.3166/pson-2019-0087
Nikbakhsh, N., Moudi, S., Abbasian, S., and Khafri, S. (2014). Prevalence of depression and anxiety among cancer patients. Casp. J. Intern. Med. 5, 167–170. doi:10.1016/j.jpainsymman.2015.12.340
Niki, K., Okamoto, Y., Maeda, I., Mori, I., Ishii, R., Matsuda, Y., et al. (2019). A novel palliative care approach using virtual reality for improving various symptoms of terminal cancer patients: A preliminary prospective, multicenter study. J. Palliat. Med. 22, 702–707. doi:10.1089/jpm.2018.0527
O’Connor, M., White, K., Kristjanson, L., Cousins, K., and Wilkes, L. (2010). The prevalence of anxiety and depression in palliative care patients with cancer in Western Australia and New South Wales. Med. J. Aust. 193, S44–S47. doi:10.5694/j.1326-5377.2010.tb03927.x
Oyama, H., Ohsuga, M., Tatsuno, Y., and Katsumata, N. (1999). Evaluation of the psycho-oncological effectiveness of the bedside wellness system. CyberPsychol. Behav. 2, 81–84. doi:10.1089/cpb.1999.2.81
Pittara, M., Matsangidou, M., Stylianides, K., Petkov, N., and Pattichis, C. S. (2020). Virtual reality for pain management in cancer : A comprehensive review. IEEE Access 8, 225475–225489. doi:10.1109/access.2020.3044233
Pizzoli, S. F. M., Mazzocco, K., Triberti, S., Monzani, D., Alcañiz Raya, M. L., Pravettoni, G., et al. (2019). User-centered virtual reality for promoting relaxation: An innovative approach. Front. Psychol. 10, 479. doi:10.3389/fpsyg.2019.00479
Pourmand, A., Davis, S., Marchak, A., Whiteside, T., and Sikka, N. (2018). Virtual reality as a clinical tool for pain management. Curr. Pain Headache Rep. 22 (8), 53. doi:10.1007/s11916-018-0708-2
Pratt, D. R., Zyda, M., and Kelleher, K. (1995). Virtual reality: In the mind of the beholder. IEEE Comput. 28, 17–19.
Ramirez, S., Liu, X., MacDonald, C. J., Moffa, A., Zhou, J., Redondo, R. L., et al. (2015). Activating positive memory engrams suppresses depression-like behaviour. Nature 522, 335–339. doi:10.1038/nature14514
Riva, G., Mantovani, F., Capideville, C. S., Preziosa, A., Morganti, F., Villani, D., et al. (2007). Affective interactions using virtual reality: The link between presence and emotionsectiveinteractions using virtual reality : The link between presence and emotions. CyberPsychol. Behav. 10, 45–56. doi:10.1089/cpb.2006.9993
Scates, D., Dickinson, J. I., Sullivan, K., Cline, H., and Balaraman, R. (2020). Using nature-inspired virtual reality as a distraction to reduce stress and pain among cancer patients. Environ. Behav. 58, 895–918. doi:10.1177/0013916520916259
Schneider, S. M., Ellis, M., Coombs, W. T., Shonkwiler, E. L., and Folsom, L. C. (2003). Virtual reality intervention for older women with breast cancer. Cyberpsychol. Behav. 6, 301–307. doi:10.1089/109493103322011605
Schneider, S. M., and Hood, L. E. (2007). Virtual reality: A distraction intervention for chemotherapy. Oncol. Nurs. Forum 34 (1), 39–46. doi:10.1188/07.ONF.39-46
Schneider, S. M., Kisby, C. K., and Flint, E. P, (2011). Effect of virtual reality on time perception in patients receiving chemotherapy. Support. Care Cancer 19, 555–564. doi:10.1007/s00520-010-0852-7
Schneider, S. M., Prince-Paul, M., JoAllen, M., Silverman, P., and Talaba, D. (2004). Virtual reality as a distraction intervention for women receiving chemotherapy. Oncol. Nurs. Forum 31, 81–88. doi:10.1188/04.onf.81-88
Schneider, S. M., and Workman, M. L. (1999). Effects of virtual reality on symptom distress in children receiving chemotherapy. CyberPsychology Behav. 2, 125–134. doi:10.1089/cpb.1999.2.125
Semerci, R., Akgün Kostak, M., Eren, T., and Avci, G. (2020). Effects of virtual reality on pain during venous port access in pediatric oncology patients: A randomized controlled study. J. Pediatr. Oncol. Nurs. 38, 142–151. doi:10.1177/1043454220975702
Sharifpour, S., Manshaee, G., and Sajjadian, I. (2020). Effects of virtual reality therapy on perceived pain intensity, anxiety, catastrophising and self-efficacy among adolescents with cancer. Couns. Psychother. Res. 21, 218–226. doi:10.1002/capr.12311
Stassart, C., and Giebels, K. (2022). Effectiveness of virtual reality for pediatric pain and anxiety management during skin prick testing. Open J. Med. Psychol. 11 (03), 89–102. doi:10.4236/ojmp.2022.113007
Tennant, M., Youssef, G. J., McGillivray, J. A., Clark, T.-J., McMillan, L., McCarthy, M. C., et al. (2020). Exploring the use of immersive virtual reality to enhance psychological wellbeing in pediatric oncology: A pilot randomized controlled trial. Eur. J. Oncol. Nurs. 48, 101804. doi:10.1016/j.ejon.2020.101804
Tsaï, F. (2016). La réalité virtuelle, un outil pour renouer avec la sensorialité. Hermes (Wiesb). 74, 188. doi:10.3917/herm.074.0188
Ulrich, R. S., Simons, R. F., Losito, B. D., Fiorito, E., Miles, M. A., Zelson, M., et al. (1991). Stress recovery during exposure to natural and urban environments. J. Environ. Psychol. 11, 201–230. doi:10.1016/s0272-4944(05)80184-7
Van den Beuken-van Everdingen, M. H. J., Hochstenbach, L. M. J., Joosten, E. A. J., Tjan-Heijnen, V. C. G., and Janssen, D. J. A. (2016). J. Pain Symptom Manage. 51 (6), 1070–1090.e9. e9. doi:10.1016/j.jpainsymman.2015.12.340
Witmer, B. G., and Singer, M. J. (1998). Measuring presence in virtual environments: A presence questionnaire. Presence. (Camb). 7, 225–240. doi:10.1162/105474698565686
Wittmann, M., and Paulus, M. P. (2008). Decision making, impulsivity and time perception. Trends Cogn. Sci. 12, 7–12. doi:10.1016/j.tics.2007.10.004
Keywords: cancer, anxiety, pain, immersion, presence, interaction, equipment
Citation: Buche H, Michel A and Blanc N (2022) Use of virtual reality in oncology: From the state of the art to an integrative model. Front. Virtual Real. 3:894162. doi: 10.3389/frvir.2022.894162
Received: 14 April 2022; Accepted: 06 July 2022;
Published: 04 August 2022.
Edited by:
Marientina Gotsis, University of Southern California, United StatesReviewed by:
Andrea Chirico, Sapienza University of Rome, ItalyAli Fardinpour, Wise Realities Institute for Healthcare Emerging Technologies Research, Australia
Copyright © 2022 Buche, Michel and Blanc. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hélène Buche, buchehelene@gmail.com; Aude Michel, aude.michel@univ-montp3.fr