 Kamilla Bergsnev
Kamilla Bergsnev Ana Luisa Sánchez Laws
Ana Luisa Sánchez Laws
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Virtual Real. , 29 April 2022
Sec. Virtual Reality and Human Behaviour
Volume 3 - 2022 | https://doi.org/10.3389/frvir.2022.834004
This article is part of the Research Topic Immersive Reality and Personalized User Experiences View all 7 articles
This mini review presents the current state of the art in studies on the personalization of virtual reality for basic research and treatment of fear-related disorders. Of particular interest to the review are the choice of self-report measures and manipulations of contextual factors that researchers are using in their virtual reality procedures. As this mini review will show, work is starting to emerge on the area of the interaction between context and individual differences, yet this topic remains a current gap in the literature on fear learning mechanisms and therapies for fear-related disorders. Studies in this review conclude that virtual reality environments offer many advantages, as they can be adjusted to model different contexts with great precision and control of the experimental context. Virtual reality is also seen by researchers as an opportunity to decrease the translational gap that exists between the research laboratories and the practical use for therapy treatments in clinics. However, the heterogeneity of methodological approaches that have created replicability as well as comparability issues in the field of fear learning is also a concern in studies using virtual reality. Thus, another, albeit secondary, aim of this mini review will be to point out some of the methodological challenges that should be addressed in future research aimed at the personalization of virtual reality for the research and treatment of fear-related disorders. Factors that will be addressed are 1) the use of self-report measures, and 2) interactivity aspects of contextual factor design in the virtual reality environment.
Global statistics of persons affected by fear-related disorders show that the development of new research and treatment tools for these disorders should be a high priority. In 2019, the prevalence of anxiety and fear-related disorders was about 300 million persons, amounting to around 4% of the total world population (Global Burden of Disease Collaborative Network, 2019). Anxiety and fear-related disorders refer to a collection of disorders that produce excessive responses either to imminent threat or to anticipated threats (real or perceived). Fear-related disorders are associated with excessive fight or flight reactions and concern the alarm system for imminent danger. Anxiety-related disorders are more often characterized by mood disorders leading to avoidance behaviour, and triggered by the expectation of future danger (Craske et al., 2011; American Psychiatric Association, 2013). These disorders include amongst others Post-traumatic Stress Disorder (PTSD), Obsessive-Compulsive Disorder (OCD), General Anxiety Disorder (GAD), Social Anxiety Disorder (SAD), panic disorder, agoraphobia, selective mutism and other specific phobias, as described in Diagnostic and statistical manual of mental disorders, 5th edition (DSM-V) for current classification of fear and anxiety disorders (World Health Organization, 2019; American Psychiatric Association, 2013; Kogan et al., 2016). Specific phobias are the most common type of anxiety disorders and are marked by fear or anxiety about a specific object or situation, such as fear of flying, fear of heights, of animals, of taking a vaccine and seeing blood (American Psychiatric Association, 2013). Situations in which fear-related cues are present are usually avoided, which in turn can contribute to a reinforced behavioral pattern restricting one’s quality of life. Finding new ways to understand and treat fear-related disorders is important because these disorders often come with a high physical and emotional burden, as well as high economical costs for society and for individuals themselves.
Treatments for anxiety and fear-related disorders involve mainly exposure-based therapies such as cognitive behavioral therapy (CBT), in vivo exposure therapy, imaginal therapy, and virtual reality exposure therapy (VRET). Some challenges of exposure therapies are related to the need to expose patients to what they fear most. This can be one of the reasons why many patients either avoid treatment in the first place, fail to complete the whole treatment, or experience relapse over time (Bouton, 2002; Craske et al., 2006; Hermans et al., 2006; Phelps et al., 2010; Davis, 2011; Otte, 2011; Schiller & Phelps, 2011; Milad et al., 2014; Grillon et al., 2019). Drug-based treatments are used as alternatives to exposure-based therapies, or may be used in conjunction with them, and involve the use of anxiolytic or antidepressants drugs (Bandelow et al., 2017; Gomez et al., 2018).
Exposure therapies work in many cases, but not in all (Bouton, 2002; Craske et al., 2006; Hermans et al., 2006; Phelps et al., 2010; Davis, 2011; Otte, 2011; Schiller and Phelps, 2011; Milad et al., 2014; Grillon et al., 2019). Two main lines of thought on how to address this problem have so far dominated the field of fear-learning research and treatment. The first line prioritizes understanding the role of contextual factors in fear learning, because deficient processing of contextual information (Baas et al., 2004) and problems with separating cue and context (Baas, 2013) may be main factors behind the development of these disorders. The second line argues that the solution to improve the efficacy of exposure therapies lies in understanding the interaction between individual experiential, biological and temperamental differences (Lonsdorf and Merz, 2017). This is because fear may be thought of as primarily an individual subjective state (LeDoux and Pine, 2016).
The fact that these disorders can range from a specific stimulus (as in specific phobia) to more complex or broad situations (as in social phobia), highlights the need for personalized understanding and treatment. Virtual reality has emerged as a suitable paradigm to combine these two lines of thought and investigate the effect of individual differences and of context in fear learning, both separately and in their interaction. Such research is targeting the personalization potential of virtual reality technologies, for example via the use of individual baseline measures to dynamically adjust contextual factors (Freeman et al., 2018; Kritikos et al., 2020; Kritikos et al., 2021). To achieve this, such systems combine virtual reality with electromyography (EMG), fear potentiated startle, functional magnetic resonance (fMRI), electroencephalography (EEG), skin-conductance response (SCR) and other behavioral and biological measures. This third line of thought prioritizes interactivity. This line of thought is built on the idea that even if context may strongly condition possibilities for action, people will still have agency, that is, their interaction with the context will be key in developing either maladaptive or adequate fear responses.
This mini review presents the current state of the art in studies on the personalization of virtual reality for basic research and treatment of fear-related disorders. As this mini review will show, work is starting to emerge on the area of the interaction between context and individual differences, yet this topic remains a current gap in the literature. In addition, research on methodological harmonization is also lagging. The heterogeneity of methodological approaches that have created replicability as well as comparability issues in the field of fear learning (Lonsdorf and Merz, 2017) is also a concern in studies using virtual reality. Thus, a secondary aim of this mini review is to point out some of these methodological challenges. Factors that will be addressed are the use of self-report measures and interactivity aspects of contextual factor design in the virtual reality environment.
The review was conducted using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews, PRISMA-ScR (Tricco et al., 2018).
Studies using virtual reality to investigate individual differences and/or context in fear learning mechanisms were selected. The search was conducted for studies published in the last ten years, from 2011 until November 2021. The review was conducted in November 2021 and submitted in the first week of December 2021. The following databases were searched: PsycINFO (OVID), Web of Science, and Medline (OVID) as recommended by the librarian specializing in systematic reviews in this specific field at the Department of Psychology, UiT The Arctic University of Norway. Search criteria were developed in collaboration with the librarian, who recommended a strategy using controlled terms in PsycINFO. We built a thesaurus for term selection (see Supplementary Materials). From this term selection, we performed a stepwise controlled search (instead of single string search) in the relevant databases, which allowed us to assess the contribution of each search term to the results, as a quality control measure. Articles that dealt with genetics or pharmacology were excluded, as reviewing those aspects was beyond the scope of this paper. Review articles were excluded. Animal studies were excluded. Non-peer reviewed publications, case studies, study protocols, conference papers and dissertations were also excluded. Upon review, the anonymous reviewer suggested an additional set of eight relevant papers. These were screened for suitability. None of these papers was included in our final set. Papers were excluded because they did not deal with either context and/or individual differences (n = 5), because they were case reports or study protocols (n = 2), or because they had serious inconsistencies in the reported methods (n = 1). Both authors were involved in reviewing the articles and deciding which ones to keep.
In PsycINFO and Medline, the search was conducted using a controlled search procedure with the explode function and mapping of terms to the database thesaurus. The search terms used were individual differences, individual, individual differen*; context, contextual factors; fear, fear learning, conditioned fear; and virtual reality, VR, virtual reality exposure therapy, respectively.
The process for filtering results is represented in the following PRISMA-ScR Flow Diagram:

FIGURE 1. PRISMA-ScR Flow Diagram.
The list of selected studies with their corresponding IDs is provided at the end of the paper.
Data from the included records (n = 20) were extracted and coded to form the coding matrix. The coding matrix included ID, author, title, year of the record, study type, study design, sample characteristics (including age and number of participants), inclusion/exclusion criteria, covariates, self-report measures, behavioural measures in the virtual reality procedure, physiological measures, individual difference studied, VR setup (including equipment used), interactivity level, type of fear-related disorder studied, and key findings. Every record was assigned with a unique identification number (ID column).
Results are reported for the columns of interest for this review, which are self-report measures and contextual factor measures in the virtual reality procedure. These two types of measures are considered as the clearest indicators of the types of individual differences studied and the types of context manipulations performed in the studies.
Studies used a wide variety of self-report measures: in total, 42 different self-report measures were used, of which 30 were validated questionnaires, while 12 were unvalidated custom rating scales developed for the specific experiment. Eleven studies from four different distinct groups of researchers involved use of a version and part of the State Trait Anxiety Inventory (STAI, STAI-Y, and STAI-DY2). Six studies from a single research laboratory involved administration of the Positive and Negative Affect Schedule (PANAS). STAI (State-Trait Anxiety Index, an instrument with 20 items for assessing trait anxiety and 20 for state anxiety, rated on a 4-point scale from 1—almost never to 4- almost always) and PANAS (Possitive and Negative Affect Schedule, an instrument with 10 items for assessing positive and negative affect, rated on a 5-point scale from 1—not at all to 5- very much) were the two most used self-report measures, but STAI was used by a wider number of research laboratories. For readers interested in more detailed explanations of the different measures, we refer them to the methods sections of the articles included in our review.
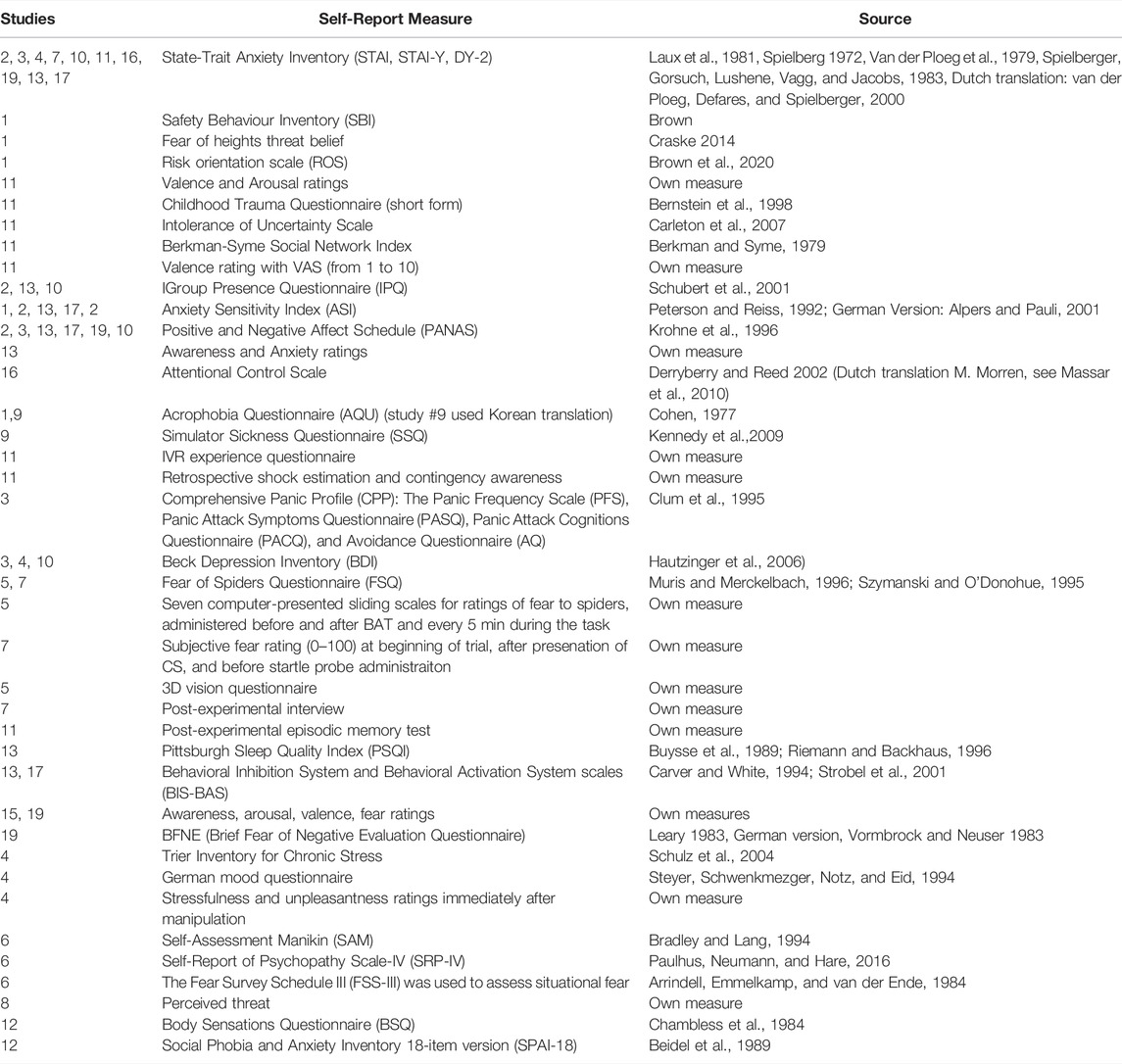
TABLE 1. Self-report measures.
Studies investigating therapeutical applications showed comprehensive use of self-report measure results. For example, one study looking at the use of virtual reality for the treatment of fear of heights (McInerney et al. (2021), study ID = 1) made an extensive analysis involving linear mixed effects models of manipulation efficacy accounting for individual baseline Acrophobia Questionnaire (AQU) score. The study also presented individual linear regressions of individual baseline predictors on post-conviction and pre-conviction of estimated fear of heights, as a measure to identify the extent to which beliefs moderated the effectiveness of the virtual reality intervention. A thorough consideration of the validity of the four self-report measures selected for the experiment and a solid rationale for the combination of these measures with other behavioral and physiological measures in the study were provided.
In studies on basic mechanisms of fear learning, there was either 1) no reporting of the results, 2) reporting that the results of self-measures were not significant, or 3) self-report measure scores were used to stratify participants into different analysis groups. For example, Andreatta et al. (2020) (study ID = 2) reported administering the State Trait Anxiety Inventory (STAI) but made no use of score results in the analysis of results. Another study using healthy young adults as participants (Kroes et al. (2017), study ID = 11) found no evidence of moderation of EMG scores by scores from the Trait section of the State Trait Anxiety Inventory (STAI-T), Intolerance of Uncertainty Scale (IUS), or Childhood Trauma Questionnaire, and explained this finding by pointing out that self-report measures scores for the healthy young adult population tend to be low and homogeneous. A third study (Neueder et al. (2019), study ID = 3) used several measures of anxiety and fear related disorders to confirm the difference between a group of participants clinically diagnosed with panic attack disorder and healthy controls. The study found differences in terms of contextual fear conditioning between these two groups, where the panic attack group was more prone to generalize fear across contexts.
Measures addressing the role of context included the design of the interaction with and appearance of the virtual environment. In what concerns interaction with the virtual environment, 15 studies (study ID = 2, 4, 5, 7, 8, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20) used passive virtual reality procedures: participants were either exposed to stimuli and asked not to move during exposure, or they were guided passively around a set of virtual rooms. Three studies (study ID = 1, 9, 6) used interactive tasks as part of the virtual reality procedure, asking the participants to either walk around, grab, or use objects in the virtual environment. Two studies (study ID = 3, 10) allowed participants to explore the virtual environment prior to the experiment to make participants acquainted with the environment. However, these two studied did not allow interactivity during the experimental phase. In addition, five studies (study ID = 2, 5, 7, 12, 15) used virtual reality to manipulate cue conditioning, nine studies (study ID = 3, 9, 10, 11, 13, 14, 17, 18, 19) used virtual reality to manipulate context, and six studies (study ID = 1, 4, 6, 8, 16, 20) used virtual reality for both cue and context manipulation.
Studies on therapeutical applications coupled changes in the appearance of the virtual context with requests for increasing interaction with the environment to overcome specific fears. For example, one study on fear of heights (study ID = 1) asked participants to first tell a virtual therapist to gradually lower a balcony barrier. On the first floor, the barrier was a solid color, whereas on subsequent floors, the barrier was glasslike. When the barrier was fully lowered, participants were asked to pick up colored balls from a bucket and throw them over the edge.
While studies on fear learning mechanisms tended to use static scenarios, there were also examples of studies using interactivity to alter context appearance. One study (study ID = 6) used an interactive horror video scenario (“A Chair in a Room”) where the participant had the ability to turn on and off a rechargeable flashlight by clicking the mouse button.
Only one study in the review (study ID = 7) investigated whether virtual reality would be better or equal than other types of exposure therapy. This involved a comparison between film and virtual reality. The conclusion of this study was that virtual reality was more effective than film, but more research was needed to support this claim. No studies in the current set made a comparison between the virtual reality treatment and in vivo exposure.
This review uses self-report measures as an index for individual differences studied. On this aspect, the review revealed that a wide variety of self-report measures were in use, at times without a good explanation of why these specific measures were collected. For example, several studies reported collecting measures from STAI, but these measures had consistently little impact on study results. STAI scores were not significant, and therefore not used to explain variation in fear learning responses. This is likely explained by the fact that most to the participants were healthy young people. Also, what was seen in the results was that the self-report measures were applied without presenting an adequate rationale for continued use: a single laboratory kept using the same self-report measures across all experiments, even when these self-report measures had proved unhelpful to explain variation in the data in previous experiments. Often, the self-report measures used were not critically assessed in the experiments. Many studies used measures that were developed in the 1970s, ‘80s and ‘90s. This is not necessarily a problem, but few studies provided an indication of whether newer research on the continued validity and reliability of these measures was considered before these were adopted for the study. In sum, we see that many researchers in the papers we reviewed expose informants to a long battery of measures. This can create fatigue, which in turn may diminish the quality of the results.
Our recommendation for researchers is to use self-report measures only to the extent to which these are directly connected to the variables studied. For example, if the study in question is looking at issues related to personality differences, it would be appropriate to integrate a measure such as the STAI, since it assesses anxiety both as a transitory and as a personality related state. In another example, if the variable related to individual differences or context has to do with mood as a moderator of fear, then it is appropriate to use a measure such as PANAS-SF, because this measure is about capturing an individual’s positive or negative mood. However, it is irrelevant to use either one of these measures when the variables in question do not have directly to do with any assumptions about the relationship between a subject’s personality or mood and fear learning mechanisms.
We take as example of best practice study 1 in our set (McInerney et al., 2021). In this study, the researchers administered the Risk orientation scale (Brown 2020) because one of the issues being studied was the willingness of subjects to take a risk and do increasingly harder “fear-defeating” tasks. Another measure was the Fear of heights threat belief (Craske 2014), which was appropriate since the scenarios used were floors in a high-rise building. Variables of interest included the extent to which subjects would be willing to go to increasingly higher floor heights, or willing to gaze down. What matters then is not only that the self-report measures used are robust and reliable as well as sufficiently validated, but also that they are relevant to the variables studied.
In what concerns the study of context, many researchers in the field of fear learning are currently searching for new ways to improve the control of contextual factors in their experiments. Studies in this review have concluded that virtual reality environments offer many advantages, as they can be adjusted to model different contexts with great precision and control of the experimental design. Virtual reality is also seen by researchers as an opportunity to decrease the translational gap that exists between the research laboratories and the practical use for therapy treatments in clinics.
Virtual reality offers the possibility to adjust individual differences to better respond to treatment settings. This may be achieved through interaction inside the virtual reality system, and dynamic response to this interaction. However, only a small number of studies in this review (n = 3) have made full use of the interactive capabilities of virtual reality. The review found that studies using virtual reality to understand the basic mechanisms of fear learning have mostly employed passive procedures. In contrast, the studies focusing on therapeutical applications of virtual reality have incorporated interactivity. Some studies harnessed more fully the potential of VR, since they required participants to not only focus on audiovisual cues, but also use touch (the feeling of grabbing something in the environment) or proprioception (for example, “walking towards one’s fear”). This shows that the possibilities of VR extend beyond visual or auditory cues. We expect that future versions of these technologies will also make more accessible the implementation of smell and/or flavor cues.
One must also consider that different types of learning mechanisms may be involved in studies where subjects are passive versus studies where interactivity is required. Studies in our set were based on a Pavlovian classical conditioning fear learning paradigm. This paradigm focuses on learning that occurs as a result of instinctive responses. One can hypothesize that studies using the operant conditioning paradigm, which is about learning that is related to the subject’s willful actions, would have more often included interactivity as part of the virtual reality procedure. Two experiments on basic learning mechanisms included in this review used an avoidance behavior paradigm, which is closer to operant conditioning (instrumental phase). These studies included interactivity, though not as part of the virtual reality procedure itself. Also, these studies did not refer to the operant conditioning literature explicitly. A specific search for studies on basic fear learning mechanisms from within an operant conditioning paradigm could be conducted as a follow up, to assess the extent to which the researchers apply interactivity as part of the virtual reality procedure.
In what concerns drawbacks of using virtual reality, for researchers, the most obvious drawback is that the technology changes very rapidly and this will create consistency, comparability and therefore replicability problems. Even within the same laboratory, procedures and programs may have to be redone very often to keep up with the changes in device design. For patients, some applications may cause discomfort, purely because of design choices that increase the likelihood of producing motion sickness. Likewise, even when not feeling this kind of discomfort, it may be undesirable for patients to wear a device that “locks them out” of their surroundings, even when this is one of the reasons why the therapy may be more efficient. In our experience, at least in the beginning stages of using VR, one may experience a certain loss of control when wearing the device. Thus, instead of having a calming effect, using VR may produce even more fear and anxiety in patients. Some of these issues are being addressed in newer devices (for instance, new devices allow for modes of operation that let users quickly shift to an infrared camera that shows the surroundings). For clinicians, not being able to correctly “read” the reactions of patients during a treatment session may also be a problem since there is loss of eye contact and other facial expression cues.
Finally, the diversity of study designs and statistical analytic approaches in this review reveals that the field of fear learning has some challenges to overcome when in relation to producing replicable results. As shown by the review, there is a vast amount of variation in procedures and measures in use, even in such a small set of studies as this. If the field is to become more robust, guidelines to increase the compatibility of approaches must be agreed upon, made available, and followed by researchers.
KB: Conceptualization, Methodology, Investigation, Validation, Writing–Original Draft. AS: Conceptualization, Investigation, Validation, Writing–Reviewing and Editing.
UiT The Arctic University of Norway provided the funding for open access publication fees.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The authors would like to thank Torstein Låg, Senior Academic Librarian and subject librarian for psychology, psychiatry and philosophy at UiT The Arctic University of Norway, for his assistance in the preliminary stages of this scoping review process. Låg provided expert feedback on strategies to find the terms for the glossary and for conducting the controlled search in PsycINFO.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frvir.2022.834004/full#supplementary-material
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders : DSM-5. 5th ed. American Psychiatric Association. doi:10.1176/appi.books.9780890425596
Andreatta, M., Genheimer, H., Wieser, M. J., and Pauli, P. (2020). Context-dependent Generalization of Conditioned Responses to Threat and Safety Signals. Int. J. Psychophysiology 155, 140–151. doi:10.1016/j.ijpsycho.2020.06.006
Baas, J. M., Nugent, M., Lissek, S., Pine, D. S., and Grillon, C. (2004). Fear Conditioning in Virtual Reality Contexts: a New Tool for the Study of Anxiety. Biol. Psychiatry 55 (11), 1056–1060. doi:10.1016/j.biopsych.2004.02.024
Baas, J. M. P. (2013). Individual Differences in Predicting Aversive Events and Modulating Contextual Anxiety in a Context and Cue Conditioning Paradigm. Biol. Psychol. 92 (1), 17–25. doi:10.1016/j.biopsycho.2012.02.001
Bandelow, B., Michaelis, S., and Wedekind, D. (2017). Treatment of Anxiety Disorders. Dialogues Clin. Neurosci. 19 (2), 93–107. doi:10.31887/DCNS.2017.19.2/bbandelow
Bouton, M. E. (2002). Context, Ambiguity, and Unlearning: Sources of Relapse after Behavioral Extinction. Biol. Psychiatry 52 (10), 976–986. doi:10.1016/S0006-3223(02)01546-9
Craske, M. G., Hermans, D. E., and Vansteenwegen, D. E. (2006). Fear and Learning: From Basic Processes to Clinical Implications. American Psychological Association.
Craske, M. G., Rauch, S. L., Ursano, R., Prenoveau, J., Pine, D. S., and Zinbarg, R. E. (2011). What Is an Anxiety Disorder? Foc 9 (3), 369–388. doi:10.1176/foc.9.3.foc369
Davis, M. (2011). NMDA Receptors and Fear Extinction: Implications for Cognitive Behavioral Therapy. Dialogues Clin. Neurosci. 13 (4), 463–474.
Freeman, D., Haselton, P., Freeman, J., Spanlang, B., Kishore, S., Albery, E., et al. (2018). Automated Psychological Therapy Using Immersive Virtual Reality for Treatment of Fear of Heights: a Single-Blind, Parallel-Group, Randomised Controlled Trial. The Lancet Psychiatry 5 (8), 625–632. doi:10.1016/S2215-0366(18)30226-8
Global Burden of Disease Collaborative Network, (2019). Global Burden of Disease Study 2019 (GBD 2019) Reference Life Table. Seattle, United States of America: Institute for Health Metrics and Evaluation. doi:10.6069/1D4Y-YQ37
Gomez, A. F., Barthel, A. L., and Hofmann, S. G. (2018). Comparing the Efficacy of Benzodiazepines and Serotonergic Anti-depressants for Adults with Generalized Anxiety Disorder: a Meta-Analytic Review. Expert Opin. Pharmacother. 19 (8), 883–894. doi:10.1080/14656566.2018.1472767
Grillon, C., Robinson, O. J., Cornwell, B., and Ernst, M. (2019). Modeling Anxiety in Healthy Humans: a Key Intermediate Bridge between Basic and Clinical Sciences. Neuropsychopharmacol. 44 (12), 1999–2010. doi:10.1038/s41386-019-0445-1
Hermans, D., Vansteenwegen, D., and Craske, M. G. (2006). Fear and Learning : From Basic Processes to Clinical Implications. American Psychological Association.
Kogan, C. S., Stein, D. J., Maj, M., First, M. B., Emmelkamp, P. M. G., and Reed, G. M. (2016). The Classification of Anxiety and Fear-Related Disorders in the ICD-11. Depress. Anxiety 33 (12), 1141–1154. doi:10.1002/da.22530
Kritikos, J., Alevizopoulos, G., and Koutsouris, D. (2021). Personalized Virtual Reality Human-Computer Interaction for Psychiatric and Neurological Illnesses: A Dynamically Adaptive Virtual Reality Environment that Changes According to Real-Time Feedback from Electrophysiological Signal Responses. Front. Hum. Neurosci. 15 (23), 596980. Article 596980. doi:10.3389/fnhum.2021.596980
Kritikos, J., Zoitaki, C., Tzannetos, G., Mehmeti, A., Douloudi, M., Nikolaou, G., et al. (2020). Comparison between Full Body Motion Recognition Camera Interaction and Hand Controllers Interaction Used in Virtual Reality Exposure Therapy for Acrophobia. Sensors 20 (5), 1244. Article 1244. doi:10.3390/s20051244
Kroes, M. C. W., Dunsmoor, J. E., Mackey, W. E., McClay, M., and Phelps, E. A. (2017). Context Conditioning in Humans Using Commercially Available Immersive Virtual Reality. Sci. Rep. 7 (14), 8640. Article 8640. doi:10.1038/s41598-017-08184-7
LeDoux, J. E., and Pine, D. S. (2016). Using Neuroscience to Help Understand Fear and Anxiety: A Two-System Framework. Am. J. Psychiatry 173 (11), 1083–1093. doi:10.1176/appi.ajp.2016.16030353
Lonsdorf, T. B., and Merz, C. J. (2017). More Than Just Noise: Inter-individual Differences in Fear Acquisition, Extinction and Return of Fear in Humans - Biological, Experiential, Temperamental Factors, and Methodological Pitfalls. Neurosci. Biobehavioral Rev. 80, 703–728. doi:10.1016/j.neubiorev.2017.07.007
McInerney, J., Brown, P., Bird, J. C., Nickless, A., Brown, G., and Freeman, D. (2021). Does Raising Heart Rate Prior to a Behavioural Test Enhance Learning in Cognitive Therapy for Anxiety? an Experimental Test for the Treatment of Fear of Heights Using Virtual Reality. Behav. Res. Ther. 144 (6), 103928. doi:10.1016/j.brat.2021.103928
Milad, M. R., Rosenbaum, B. L., and Simon, N. M. (2014). Neuroscience of Fear Extinction: Implications for Assessment and Treatment of Fear-Based and Anxiety Related Disorders. Behav. Res. Ther. 62, 17–23. doi:10.1016/j.brat.2014.08.006
Neueder, D., Andreatta, M., and Pauli, P. (2019). Contextual Fear Conditioning and Fear Generalization in Individuals with Panic Attacks. Front. Behav. Neurosci. 13 (10), 152. Article 152. doi:10.3389/fnbeh.2019.00152
Otte, C. (2011). Cognitive Behavioral Therapy in Anxiety Disorders: Current State of the Evidence. Dialogues Clin. Neurosci. 13 (4), 413–421.
Schiller, D., Monfils, M.-H., Raio, C. M., Johnson, D. C., LeDoux, J. E., and Phelps, E. A. (2010). Preventing the Return of Fear in Humans Using Reconsolidation Update Mechanisms. Nature 463 (7277), 49–53. doi:10.1038/nature08637
Schiller, D., and Phelps, E. A. (2011). Does Reconsolidation Occur in Humans? Front. Behav. Neurosci. 5, 24. doi:10.3389/fnbeh.2011.00024
Tricco, A. C., Lillie, E., Zarin, W., O'Brien, K. K., Colquhoun, H., Levac, D., et al. (2018). PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 169 (7), 467–473. doi:10.7326/m18-0850
World Health Organization, (2019). ICD-11: International classification of diseases (11th revision). Geneva: World Health Organization. Available at: https://icd.who.int/.
Keywords: fear-related disorders, fear learning, virtual reality, individual differences, contextual factors, exposure therapy, self-report measures
Citation: Bergsnev K and Sánchez Laws AL (2022) Personalizing Virtual Reality for the Research and Treatment of Fear-Related Disorders: A Mini Review. Front. Virtual Real. 3:834004. doi: 10.3389/frvir.2022.834004
Received: 12 December 2021; Accepted: 24 March 2022;
Published: 29 April 2022.
Edited by:
Simon Richir, Arts et Métiers ParisTech, FranceReviewed by:
Abdelmajid Kadri, Arts et Métiers ParisTech, FranceCopyright © 2022 Bergsnev and Sánchez Laws. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kamilla Bergsnev, a2FtaWxsYS5iZXJnc25ldkB1aXQubm8=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.