 Nancy van Veelen1,2*
Nancy van Veelen1,2* Rudy C. Boonekamp3
Rudy C. Boonekamp3 Tjeerd A.J. Schoonderwoerd3
Tjeerd A.J. Schoonderwoerd3 Martijn L. van Emmerik3
Martijn L. van Emmerik3 Mirjam J. Nijdam2,4
Mirjam J. Nijdam2,4 Bastiaan Bruinsma5
Bastiaan Bruinsma5 Elbert Geuze5,6
Elbert Geuze5,6 Chelsea Jones1,7
Chelsea Jones1,7 Eric Vermetten1,2,8
Eric Vermetten1,2,8- 1Leiden University Medical Centre (LUMC), Psychiatry, Leiden, Netherlands
- 2ARQ Centrum’ 45, Oegstgeest, Netherlands
- 3Netherlands Organisation for Applied Scientific Research (TNO), Soesterberg, Netherlands
- 4Department of Psychiatry, Amsterdam University Medical Center, Amsterdam, Netherlands
- 5Brain Research and Innovation Centre, Ministry of Defence, Utrecht, Netherlands
- 6Department of Psychiatry, UMC Utrecht Brain Center, Utrecht, Netherlands
- 7Canadian Forces Health Services, Department of National Defense, Ottawa, ON, Canada
- 8Military Mental Health Care, Ministry of Defense, Utrecht, Netherlands
With the application of virtual reality (VR), tailored interventions can be created that mirror the traumatic experiences of veterans with post-traumatic stress disorder (PTSD). Visual elements can be mimicked, and auditory and other senses stimulated. In doing so, the degree of immersion can be adjusted to optimize the therapeutic process. Objectively measuring the sensory immersion is key to keep subjects within their personal window of tolerance. Based on this information the therapist can decide manipulate the sensory stimulation embedded in the treatment. The objectives of this article are to explore the different immersive design aspects of VRET that can be modified to influence the experienced presence in veterans with PTSD, and to discuss possible methods of measuring the emotional response facilitated by immersive design aspects and experienced presence. Four design aspects are discussed: system, sensory cues, narrative and challenge. We also report on a user experiment in three veterans that informed on quality and depth of immersion. Believability of the neutral virtual environment was important for maintaining the veterans’ presence within the VR experience. The immersive design aspects that were personalized and supportive in the narrative of the veteran such as music and self-selected images appeared to have a strong influence on recall and reliving of the traumatic events. Finally, in order to increase the therapeutic effect in veterans with PTSD, the highlighted design aspects should be recognized and tailored to maximize immersion in virtual reality exposure therapy.
Introduction
Veterans and military personnel are exposed to extreme situations and potentially traumatic experiences during their deployment. Afterwards, a significant number of veterans develop post-traumatic stress disorder (PTSD; e.g., life-time prevalence: US 2–17%, UK 4–6%, NL 5–8%) (Richardson et al., 2010; Reijnen et al., 2015). Treatment options currently available to address PTSD have proven to be less effective in military and veteran populations when compared to their civilian counterparts (Haagen et al., 2015). These traditional psychotherapies have important commonalities, such as emotion regulation and imaginal exposure (Schnyder et al., 2015).
It is hypothesized that reduced effectiveness in this specific population can be explained by means of avoidant coping strategies and limited emotional engagement, which can hinder optimal processing of the traumatic events (Eshuis et al., 2020). This warrants the exploration and utilization of novel interventions for these populations including the implementation of virtual reality (VR) within psychotherapeutic interventions. With virtual reality exposure therapy (VRET), it is possible to create an immersive, realistic, and safe environment where veterans can be exposed to trauma-related stimuli in a controlled setting (Rizzo and Shilling, 2017; Eshuis et al., 2020). These facilitators enable a customized and tailored psychotherapy experience for veterans with PTSD, which may be effective through enhanced emotional engagement and challenging classic symptoms of PTSD such as avoidance (Nijdam and Vermetten, 2018; van Gelderen et al., 2018).
Previous research on anxiety disorders and PTSD suggests that a person must feel “present” in the virtual environment to be able to activate and possibly modify the fear structure or traumatic memory trace (Vermetten et al., 2013; Diemer et al., 2015). For this paper, “presence” will be defined as a subjective psychological state where an individual’s experience of a virtual environment (VE) is perceived as if the technology was not involved (Schubert et al., 2001). The experienced presence is facilitated by immersive design aspects and the objective qualification of the VR equipment to convey an illusion of reality to the participant (Schubert et al., 2001). In this paper, “immersion” is defined as the combination of the experienced presence and the immersive design aspects. It is hypothesized that increased immersion will lead to a stronger emotional response during VRET which subsequently increases the efficacy of this intervention (Waterworth and Waterworth, 2003; Gromer et al., 2018). Adjustment of the immersion provides the opportunity to modify the dosage and depth of exposure to moderate the emotional responses a participant may experience. The VE can be tailored in several ways, such as a scenario of a traumatic event that is generic for a certain patient population or by adding personalized sensory cues related to the traumatic event (Rizzo and Shilling, 2017). The depth of the level of immersion and the type of simulation used during the therapy can be discussed with the patient and adjusted if needed. Shared decision making can contribute to achieving one’s optimal level of immersion. To appropriately and accurately adjust the immersion objective parameters to measure the emotional response during VRET are required. Therefore, the objectives of this article are to: 1) explore the different immersive design aspects of VRET that can be modified to influence the experienced presence in veterans with PTSD, and; 2) discuss possible methods of measuring the emotional response facilitated by immersive design aspects and experienced presence. This article presents a theoretical framework supported by a real-world contextualization with the user experiences of three veterans. This paper presents a unique perspective on tailored immersion of several domains of expertise, combining technical expertise, clinical expertise and expertise of academic and health care partners and the military context. The expertise of six centers (Applied Scientific Research (TNO), Leiden University Medical Center and Arq National Psychotrauma Center and two military centers Dutch Military Mental Health and Canadian Forces Health Service) were combined to augment the potential of VRET in veterans with PTSD.
Immersive Design Aspects
The environment where fear-related stimuli are presented can be enriched with immersive VR aspects that are designed to increase the feeling of presence in subjects (Figure 1). A reinforcing relationship between presence and emotional engagement has been demonstrated, however for trauma-related stimuli this relationship remains unclear. To understand the relevance of the immersive design aspects, comprehension of the cognitive foundation of the level of presence is necessary (Freeman et al., 2005; Jennett et al., 2008; Visch et al., 2010). There are three attention-based processes that are indicators of the experience of “being present” (Waterworth and Waterworth, 2003; Riva et al., 2011). First, the focus of attention is directed at the immediate VE within and around the body. It increases with concrete interaction in the VE and decreases with abstract reasoning, which moves attention towards absence (Waterworth and Waterworth, 2001). Next, the locus of attention, meaning the location that is attended to, is within the VE opposed to the external environment. Lastly, the sensus of attention, referring to the level of attentional arousal that is experienced, is elevated. When developing interactive environments with presence as an important goal, it is helpful to consider how particular immersive design aspects might direct, reinforce or attenuate the attention of presence in the user.
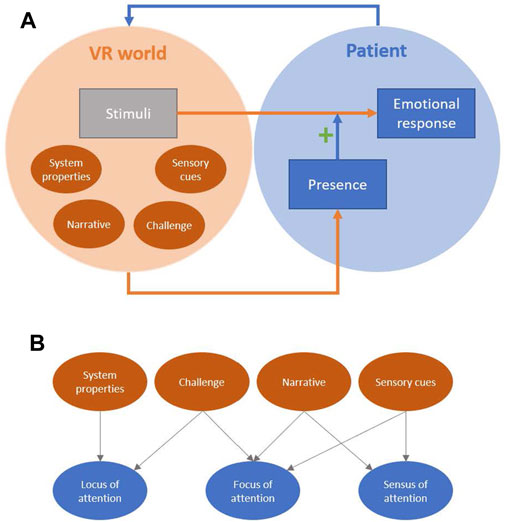
FIGURE 1. Schematic overview of virtual reality exposure therapy (VRET), in which trauma-relevant stimuli are presented in a VR environment that is enriched with immersive design aspects (dark orange circles) (A) These aspects can affect presence as experienced by the patient, which can moderate their emotional response to the stimuli (B) The design aspects influence presence through their effects on different attention-based processes.
Based on literature, four immersive design aspects were identified as potentially influencing the presence during exposure: the system presenting the VR, sensory cues, subject’s narrative, and challenge (Figure 1). These design aspects will be described in the next paragraph.
Design Aspect: System
First, the system utilized to deliver the VE is an important element of the VR context. The VR system can enhance presence by isolating a subject from the external physical environment through blocking out sensory information as well as presenting interactive experiences within the VE (Witmer and Singer, 1998; McMahan, 2013). Thus, the VR system can shift the locus of attention from the external physical environment to the VE (Figure 1). The type and number of sensory modalities that are used (visuals, sounds, haptics, scents, tastes), and their properties, such as display size, field of view, tracking fidelity, responsiveness, frame rate, and audio quality, are critical to the level of presence and context of the VR experience. While the VR system can be considered a technical design aspect as it concerns the presentation of the VE, the other three identified design aspects are related to the contents of the VR experience.
Design Aspect: Sensory Cues
The second design aspect is the use of multi-modal, sensory cues during VRET, which refers to all observable stimuli that are implemented in the VE. These stimuli precede a continuous stream of perceptions and have an important role in increasing the believability of the VE. Personalized trauma-related stimuli, such as scents and sounds, refer to the sensory cues the therapist asks about during regular exposure therapy. This type of stimuli is utilized to lead to an experience that is authentic and relevant to the traumatic experiences of the veteran, rather than achieving a high-fidelity simulation of real-world sensory information. Authentic sensory cues affect presence by masking the sensory information coming from the real world, directing the focus of attention (Ermi and Mäyrä, 2005; Gilbert, 2016) (Figure 1). Moreover, they facilitate a richer recollection of the traumatic experience, thereby increasing the sensus of attention (Tielman et al., 2015; Dibbets, 2020).
Design Aspect: Narrative
The third design aspect concerns contents of the subject’s narrative in the VE. Narrative typically refers to the story that is being told, including the plot, characters, and events. One of the goals of VRET is to enable subjects to tell their own story, rather than to create a new narrative. Treating the trauma-related memory as the narrative fulfills two prerequisites for the effect of narrative on presence: the subject is engaging in the story in the role of a character, and the story is accepted as reality (Riva et al., 2004; Adams and Rollings, 2006). The subject’s narrative influences presence by maintaining the focus of attention on trauma-relevant events, and by increasing the sensus of attention as a result of activating trauma-associated memories and experiences (Figure 1).
Design Aspect: Challenge
The fourth immersive design aspect for optimal presence is challenge. Facing challenging tasks that match one’s mental and/or sensorimotor capabilities often results in intense focus on the activity (Ermi and Mäyrä, 2005). Challenge affects presence by providing a sense of autonomy and agency (Riva et al., 2004). However, only sensorimotor challenges might be suitable for this purpose, as they actively stimulate perceptual processing and interaction with the environment (i.e., placing the locus of attention on the VR world) (Waterworth and Waterworth, 2001) (Figure 1). Cognitive challenges, on the other hand, are more likely to redirect attention from the VE towards the cognitive processes that are required to solve the task.
Tailoring of Immersion and Presence for VRET
Numerous studies have indicated that VRET can result in extreme emotional responses as the nervous system responds to traumatic experiences by engaging its physiological survival mode—fight, flight or freeze (Parsons and Rizzo, 2008). If the VE very closely corresponds with the traumatic experience itself, the person can be fully immersed in the trauma. This state is associated with being outside the window of tolerance in the case of PTSD. The window of tolerance is a zone of autonomic and emotional arousal that is optimal for well-being, effective functioning and receiving and integrating information from both internal and external environments (Siegel, 2020). The zone falls between the extremes of hyper- and hypoarousal. Like in other trauma-focused psychotherapies, optimal processing of the trauma takes place in VRET when the person stays within these boundaries and there is a need to regulate when the veteran is outside the window of tolerance (Corrigan et al., 2011). This underlines the need for tailored immersion within the therapeutic context; by controlling immersion, emotional responses can be moderated. A distinction can be made between offline (in preparation for the immersive therapy session) and online (during the immersive therapy session) adaptations. These adaptations can be categorized according to the four immersive design aspects, which will be discussed in the next paragraphs.
Design Aspect: System
The system refers to the devices that enable sensory cues for the subject. In the context of a VRrehabilitation environment, adaptive feedback has been based on the subject’s behavior in the VE by means of various modalities (i.e., visual or auditory) (Chen et al., 2011). Online tailored engagement of sensory feedback during therapy can be extended to the olfactory sense (scent dispensers) and somatosensory system (motion controllers or gesture control). The use and research of immersive simulation of the gustatory system during VRET is still in its infancy (Ranasinghe et al., 2013). The influence of olfactory sense on the experienced presence and levels of stress and relaxation in VE has not been supported by previous studies (Serrano et al., 2016; Narciso et al., 2019). However, for PTSD this might be different, since various studies described that olfaction might precipitate PTSD symptoms and suggested that it was an important component of re-experiencing (Vermetten and Bremner, 2003; Daniels and Vermetten, 2016).
Design Aspect: Sensory Cues
Presentation of sensory cues during the online exposure is a powerful method to elicit higher levels of presence and stronger emotional responses (Beck et al., 2007; Gamito et al., 2010; Rizzo and Shilling, 2017). There are two important characteristics related to using sensory cues for tailored immersion in VRET: authenticity and timing. First, to increase emotional engagement, it is important to choose cues that are authentic to the trauma-related memory and the expectations of patients, while leaving out irrelevant ones (Witvliet et al., 2001; Gilbert, 2016; Picard et al., 2017). Identification of such personal sensory cues may take place offline, in advance of therapy sessions (e.g., from a subject’s descriptions of the traumatic experience, by letting a subject select music that is relevant to the trauma or that is calming).
Next, sensory cues should be added or removed at the right moments during a VRET session based on the veteran’s responses. If the presented visual cue is a trauma-related image that leads to a mild emotional response, the response can for instance be enhanced by adding an olfactory or auditory cue at that moment. The timing and choice of cues might be best controlled by a therapist who guides the therapy (Rizzo and Shilling, 2017).
Design Aspects: Narrative
A distinction can be made between direct and indirect presentation of trauma-related stimuli and events that make up the subject’s trauma narrative. In the direct presentation of this narrative, the VE itself is used to reconstruct a complete environment that is authentic to the traumatic experiences of the subject (Rizzo and Shilling, 2017). Alternatively, VR can be used to create a safe environment (e.g., a cabin on a beach), in which trauma-related stimuli are gradually presented. For example, personal images can be collected offline, and used within the VE to assist in recalling associated memories that help shape the subject’s trauma narrative and increase the presence and engagement in his or her treatment (van Gelderen et al., 2018). To tailor the immersion online, the branching of the narrative may be directed towards exposure or reduction of tension depending on the subject’s response (Dibbets, 2020). Recall of the trauma narrative can be consolidated with active guidance of the therapist, for example by online creation of a written record of memories and associated feelings.
Design Aspect: Challenge
A person is fully engaged in the present moment if the level of challenge in the VE matches the skill level of that person (Sweetser and Wyeth, 2005). A level of challenge greater than the available skills may result in anxiety. Conversely, challenges requiring less skill than available may result in apathy (Johnson and Wiles, 2003). The optimal balance between these polarities is described as the “flow channel” (Csikszentmihalyi, 1990). To experience flow, one must be allowed to exercise control over one’s actions and be able to translate intentions into behaviour in the VE, giving a sense of agency (Stoffregen et al., 2003)). To tailor immersion, adaptive variables that influence the level and type of challenge and the sense of agency are worth consideration, such as cognitive difficulty level of the scenario, sensorimotor challenges, secondary task load and subject control (or agency) (Zahabi and Razak, 2020). The difficulty level of the task at hand, either in the main scenario or as a secondary task load, can be increased or decreased for the purpose of exposure or tension reduction. Subject control implies the ability to control factors within the VE such as an avatar, virtual objects, and other components that can influence therapeutic and performance outcomes. The real or perceive subject control can be utilized to increase the level of immersion (Sweetser and Wyeth, 2005).
Measuring Immersion, Presence and Emotional Response in Window of Tolerance
The discussed adaptations, framed as immersive design aspects, have the potential to influence the immersion and the emotional response of the subject. Knowledge of the level of immersion and emotional response during VR exposure, is required to monitor the effect of the online adaptations within a therapeutic session. This data may be gathered through subjective immersion questionnaires and objective physiological parameters and analyzed for the purpose of keeping emotional responses of the subject within the window of tolerance. Although validated questionnaires for the purpose of measuring immersion exist, issues with their theoretical underpinnings and psychometric properties have been identified. For example, pre-emptive exposure to the questionnaire prior to the VR experience could cause bias and disruption of the immersion at the moment itself in the VE (Slater, 1999). We identified one tool, the Self-Assessment Manikin (SAM), that is suitable to be embedded into the VE, to minimize the disruption of the immersion (Grübel et al., 2016). Besides this assessment tool, we argue that objective measures are preferred for assessing immersion.
Psychophysiological and Biobehavioral Monitoring
Although further validation is needed, a number of methods exist to indirectly measure and monitor presence and immersion by means of physiological indicators during VRET (Bradley et al., 2000). The most common parameter utilized within VR interventions is skin conductance to measure the indirect emotional response in psychophysiological studies (van Dooren et al., 2012). Another cluster of physiological indicators that are commonly utilized as indirect indicators of emotional response are measures of cardiorespiratory performance, such as heart rate, blood pressure, and respiratory rate. These parameters are related to emotional arousal of negative emotional affect (Bradley et al., 2000; Feldman et al., 2004). Respiratory rate, for instance, is associated with emotional states such as anger, joy, fear and sadness (Philippot et al., 2002). Furthermore, there is evidence that heart rate variability (HRV) correlates with emotion-specific blood flow in associated cerebral regions (Lane et al., 2009; Blase et al., 2016). Evidence further suggests that visuomotor indicators, such as eye blink rate and pupillary diameter, may also act as physiological indicators of emotional arousal in PTSD (Rubin et al., 2017). Besides the aforementioned physiological outputs that are commonly utilized to indirectly measure emotional responses, additional visuomotor parameters specific to the measurement of immersion have been utilized within a VE. These include eye movements or gaze fixation, which measures the number and duration of fixation (Toet, 2006; Jennett et al., 2008). Finally, eye tracking can be used to measure the focus of attention of the subject during the entire session (Toet, 2006; Jennett et al., 2008). By measuring the focus of attention, immediate information about the immersion of the subject in the VE can be obtained.
User Experiences
Participants
Three user experiences were described which explored the influence of immersive design aspects on the experienced presence and emotional response in a VE in healthy veterans with deployment experience. Three veterans within our professional network were approached, that profiled themselves as PTSD ambassadors and regularly participate as experience experts in treatment evaluations of PTSD. The participants agreed to participate by means of written informed consent. The participants had no psychiatric medical history based on self-report, and were not seeking treatment for PTSD. Approval of the ethics committee was not deemed necessary, since the report is a case series about experienced immersion in a VE in healthy participants.
Design
We selected three healthy veterans with deployment experience, to gather information about this specific population and to inform future application of tailoring the VE in a therapeutic context. The participants were asked to bring a neutral music song and pictures and music that reminded them of a mild traumatic experience during their employment, to the user experiment. The self-selected images and music were added as personal sensory cues to the VE. The participants were engaged in a multisensory VR environment (Sensiks Sensory Reality Pod www.sensiks.com). In the VE, the participants were asked to first interact with the radio in the VE, which would play the self-selected music associated with their deployment experience. After the music the participants were asked to open the virtual photo-album, which would display the self-selected picture. First the participants had to describe the picture, then the therapist asked about the story behind the picture and finally the emotions and bodily sensations the picture evoked at that moment were explored in the VE. After each image was discussed, the participant performed a cognitive task - Serial sevens - that taxes working memory (“challenge” design aspect).
The participants could interact with the virtual radio, photo-album and plush toy, facilitated by hand gesture recognition (Leap Motion Controller). A live connection with the therapist behind a webcam was projected on a monitor within the VE throughout the session with audio and video. Additionally, the therapist could add notes in the virtual photo-album, capturing parts of the participant’s recollection (“narrative” design aspect). In this setting, visuals are presented through a head mounted display (HTC Vive Pro Eye), while the Sensiks Pod can add olfactory, auditory and tactile stimuli (“system” design aspect). During the VRET session, respiratory rate was measured with a wireless sensor (VimScore FLOW chest band) and displayed on the therapist’ screen together with eye-tracking data (Figure 2). The VE (Infinity Labs BV, Netherlands) displayed a beach house on a tropical beach, (“indirect presentation” design aspect). During the VR experience, olfactory, temperature, and tactile sensory stimuli were presented to simulate ocean smells, Sun, and a breeze respectively (“sensory cues” design aspect).
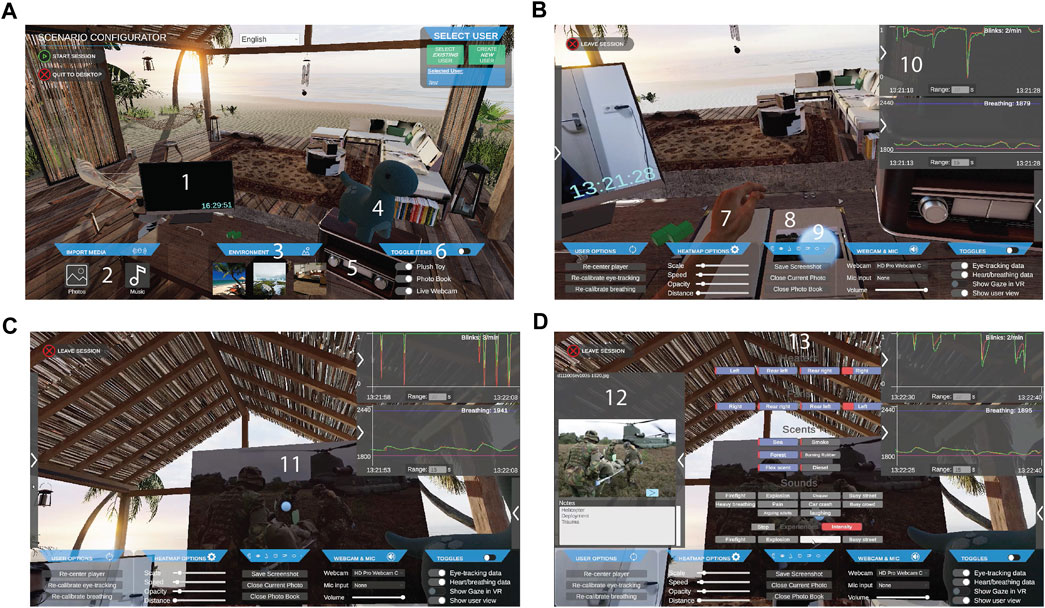
FIGURE 2. VR exposure application (A) Scenario configurator screen with view of the selected virtual environment for the session, in this case a beach cabin (B) Therapist view during a session. Participant can browse through virtual photo album with self-provided photographs (C) The selected photo can be enlarged by the participant for in-depth discussion. The Therapist can follow the participants’ gaze via eye-tracking measurements (D) The Therapist can add notes to the photo, that appear in the virtual photo book and immersive elements to the experience (heat, wind, scents and sounds) via a pop-up menu. 1: Interaction with the therapist in session occurs via a webcam, the therapist is displayed on this screen in the virtual environment. 2: In the scenario configurator, media such as photos and music can be selected. 3: One of three virtual environment can be selected for the session: a beach cabin (shown here), a cabin in the woods and a living room. 4: A plush toy with which the participant can virtually interact. 5: Self-provided music can be switched on, paused, and fast-forwarded via this virtual radio set. 6: Several virtual items can be added. 7: Participants interact with the virtual world through hand tracking. 8: The participant can browse through the self-provided photos in the virtual photo book. 9: The gaze of the participant as measured with eye-tracking. 10: Respiratory and eye-lid measurements are visible for the therapist. 11: Enlarged photo from the virtual photo book. 12: Therapist view of the photo book, the therapist can add notes. 13: Pop-up menu for adding immersive elements to the virtual experience.
Measurements
We collected qualitative information by interviewing the participants after the VR experience, to explore the influence of the design aspects on their experienced presence and emotional reactions in the VE, to identify the design components that were most strongly related to the level of immersion. The respiratory rate and eye-tracking data were not collected for further analysis, but solely used as feedback during the experience.
User Experience 1
Participant 1, male in his mid-fifties was wounded during his deployment in Bosnia in 1993. His self-selected image was composed after he was shot, depicting him lying on a stretcher while still in his uniform. He reported that this event caused major challenges for him with both positive and negative aspects and outcomes for his health and personal development.
Music and images: evoked memories leading to a re-experience of emotions from that moment in time.
Presence: felt immediately present in VE although it was not realistic, was disturbed by the airflow, the desynchronization of hand movements with his own hands and the motionless ocean and trees.
Additional comments: turning on the VR-radio made the object more realistic in the VE but turning the pages of the photo-album with a button did not have the same effect. Guidance of the therapist was very important to appoint the emotions attached to the images.
User Experience 2
Participant 2, a woman in her mid-forties was deployed to Afghanistan where she reported to have felt very vulnerable when she was irradiated by a targeting laser during a helicopter flight. In the picture she brought, the landscape from the helicopter perspective was shown and within it the person that had targeted the helicopter.
Music and images: immersed her within her deployment evoking contradictory feelings of being sad and being, “on the top of her game.”
Presence: increased when helicopter sound and airflow was added, but was disturbed by incorrect details depicted such as VR hands appearing male, absence of movement in the VE, olfactory stimulus that reminded her of a public toilet, incoherence of warmth of the Sun and the cool airflow.
Additional comments: she reported not to feel present, but kicked the cabin door several times, while stretching legs in the VE, and felt uncomfortable when the table in the VE was pushed up against her.
User Experience 3
Participant 3, male in his late fifties, was deployed in the last months while the genocide in Srebrennica took place. He brought a newspaper article that showed him sitting next to his wife, in his uniform holding his baby on his arm.
Music and images: took him immediately back in time to his deployment, with feelings of sadness and feeling powerless, he even smelled the odor of burning wood.
Presence: VE was a motionless picture but it felt pleasant and safe which helped to decrease the emotional tension. VR hands were dirty and without a wedding ring, which disturbed presence and airflow was mistaken as air conditioning. The limited interaction possibilities made the VE less interesting.
Additional comments: valued the guidance of the therapist and enjoyed the independence in the VE.
Summary of the User Experiences
The aforementioned design aspects were utilized in the user experience to influence immersion and afterwards reflected upon during the interview. In the user experiences, the system design aspects, including the olfactory stimuli and hand gesture recognition, disturbed the experienced presence, because they were not congruent with the VE. The sensory design aspects, which included music and images, were authentic and shifted the focus of attention within the VE, enhancing the presence. Conversely, the misaligned details of the sensory visual cues disrupted the presence, since the believability of the VE was disturbed by the misaligned details, such as the presented male hands in the visual field and the motionless ocean.
Timing of cues was utilized with one participant by adding auditory and haptic sensory stimuli. This resulted in an enhanced emotional response during the exposure. The images and guidance of the therapist supported the participant’s narrative in the indirect presentation, resulting in an increased focus and sensus of attention toward the VE. A limitation of the VE could be the level of difficulty which, at times, was not challenging enough with limitations regarding subject control. The presented secondary task, serials seven, was challenging but abstract, which also disrupted the presence by shifting the focus of attention to absence (Waterworth and Waterworth, 2001). During the VRET, the eye tracking data provided direct feedback about the focus of attention of the participant. The respiratory rate graphic was projected live on the therapist’s screen. During the exposure and serial sevens, observed changes of these parameters indicated changes in emotional arousal.
Discussion
The aim of this paper was to explore immersive design aspects of VRET that can be modified to influence presence in veterans with PTSD, and discuss possible methods of measuring the emotional response. Three user experiences of veterans provided real-life illustrations of VR adaptations and consequent changes in immersion. Four immersive design aspects: system, sensory cues, narrative and challenge, were identified as being essential to modify presence during exposure in treatment, to induce a necessary emotional response for processing of traumatic events (Rizzo et al., 2005; Botella et al., 2010; Rothbaum et al., 2014). To regulate the emotional response and stay within the window of tolerance, we believe it is necessary to measure the emotional response during VRET. Potential measures include physiological parameters, such as cardiorespiratory performance, pupillary diameter, eye blink rate and skin conductance.
These aforementioned design aspects can be utilized in various ways to modify the immersion, resulting in a spectrum of VE designs. At one end of the spectrum are the VEs that are very realistic representations of deployment scenarios (e.g., BRAVEMIND) (Rizzo et al., 2005) and, on the other end of the spectrum, augmented reality that can be positioned, adding virtual fear stimuli to the physical world surrounding the user (Eshuis et al., 2020). In the middle are the neutral VEs in which personalized details are inserted (e.g. 3MDR, EMMA’s world) (Botella et al., 2010; van Gelderen et al., 2020a). The presented VE in the user experience of the current study could also be placed in the middle of this spectrum. In comparison to other VRET approaches, novel aspects of this current approach are an explicit measurement of the emotional response, and the opportunity for the therapist to use this information to optimally adjust the treatment to the subject’s needs. The usage of personalized aspects in the VE is also utilized in 3MDR, this novel treatment hints towards a therapeutic effect in a population of veterans with PTSD (van Gelderen et al., 2020a; Bisson et al., 2020; van Gelderen et al., 2020b).
This overview serves to provide a theoretical basis for future VRET research, utilizing the different design aspects to attain the intended immersion and treatment effect. Utilizing the expertise of multiple domains was essential in creating this theoretical basis and we think that such collaborations are essential for the further development of tailored immersion. One of the deliverables we aim to create is a tool for the therapist that informs them of levels of immersion and emotional engagement by combining different objective measures. This enables the therapist to modify the exposure to stay within the window of tolerance, by adjustment of design aspects online and offline. We will conduct further to identify the parameters that can be utilized to measure or approximate the emotional response as closely as possible. Furthermore, there is also a need for future research to establish the relationships between different design aspects and their respective effects on the level of immersion. Finally, another investigative need concerns the effect of immersion on emotional responses. Clarity surrounding this relationship would be valuable for the future development of tailored immersion (Krijn et al., 2004; Visch et al., 2010; Gromer et al., 2018; van Gelderen et al., 2020c).
In conclusion, knowledge of the immersive design aspects within a VE can be utilized to optimize the presence and immersion as well as, evoke and maintain an emotional response within the window of tolerance. We see this study as a first step towards development of an evidence-based tool that can be utilized in VRET to measure the emotional response. From the user experience we conclude that the believability of the neutral VE is important to maintain presence within the VR experience. Contrarily, the personalized details, such as self-selected images and music, had a profound influence on how the veterans recalled and relived their traumatic events. This therapeutic approach bypasses the cognitive avoidance during exposure and can lead to a stronger emotional response, which is correlated with an increased therapeutic effect (Jaycox et al., 1998). Therefore, we expect that tailoring immersion and measuring the emotional response in VRET will increase the therapeutic effect in veterans with PTSD.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics Statement
Ethical approval was not provided for this study on human participants because the performed user experience does not belong to medical scientific research. It is a usability testing, and ethical approval was not needed. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author Contributions
NV, RB, BB, and EV carried out the experiment. NV, RB, TS, ME, wrote the manuscript with support from CJ, MN, BB and EG and MN helped supervise the project. NV, EV, and ME conceived the original idea. EV supervised the project.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors wish to acknowledge Fred Galstaun for expert consultation in the use of the Sensiks sensory pod.
References
Adams, E., and Rollings, A. (2006). Fundamentals of Game Design (Game Design and Development Series). Upper saddle River: Prentice-Hall.
Beck, J. G., Palyo, S. A., Winer, E. H., Schwagler, B. E., and Ang, E. J. (2007). Virtual Reality Exposure Therapy for PTSD Symptoms after a Road Accident: An Uncontrolled Case Series. Behav. Ther. 38 (1), 39–48. doi:10.1016/j.beth.2006.04.001
Bisson, J. I., Deursen, R., Hannigan, B., Kitchiner, N., Barawi, K., Jones, K., et al. (2020). Randomized Controlled Trial of Multi‐Modular Motion‐Assisted Memory Desensitization and Reconsolidation (3MDR) for Male Military Veterans with Treatment‐Resistant Post‐Traumatic Stress Disorder. Acta Psychiatr. Scand. 142 (2), 141–151. doi:10.1111/acps.13200
Blase, K. L., van Dijke, A., Cluitmans, P. J., and Vermetten, E. (2016). Efficacy of HRV-Biofeedback as Additional Treatment of Depression and PTSD. Tijdschr Psychiatr. 58 (4), 292–300.
Botella, C., García-Palacios, A., Guillen, V., Baños, R. M., Quero, S., and Alcaniz, M. (2010). An Adaptive Display for the Treatment of Diverse Trauma PTSD Victims. Cyberpsychology, Behav. Soc. Networking 13 (1), 67–71. doi:10.1089/cyber.2009.0353
Bradley, M. M., and Lang, P. J. (2000). “Measuring Emotion: Behavior, Feeling, and Physiology,” in Cognitive Neuroscience of Emotion. Series in Affective Science. Editors RD Lane, and L Nadel (New York, NY: Oxford University Press), 242–276.
Chen, Y., Baran, M., Sundaram, H., and Rikakis, T. (2011). “A Low Cost, Adaptive Mixed Reality System for home-based Stroke Rehabilitation,” in 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, USA (IEEE).
Corrigan, F., Fisher, J., and Nutt, D. (2011). Autonomic Dysregulation and the Window of Tolerance Model of the Effects of Complex Emotional Trauma. J. Psychopharmacol. 25 (1), 17–25. doi:10.1177/0269881109354930
Daniels, J. K., and Vermetten, E. (2016). Odor-Induced Recall of Emotional Memories in PTSD-Review and New Paradigm for Research. Exp. Neurol. 284, 168–180. doi:10.1016/j.expneurol.2016.08.001
Dibbets, P. (2020). A Novel Virtual Reality Paradigm: Predictors for Stress-Related Intrusions and Avoidance Behavior. J. Behav. Ther. Exp. Psychiatry 67, 101449. doi:10.1016/j.jbtep.2019.01.001
Diemer, J., Alpers, G. W., Peperkorn, H. M., Shiban, Y., and Muhlberger, A. (2015). The Impact of Perception and Presence on Emotional Reactions: A Review of Research in Virtual Reality. Front. Psychol. 6, 26. doi:10.3389/fpsyg.2015.00026
Ermi, L., and Mäyrä, F. (2005). “Fundamental Components of the Gameplay Experience: Analysing Immersion,” in Worlds in play: International perspectives on digital games research, New York, 37–53.
Eshuis, L., van Gelderen, M., van Zuiden, M., Nijdam, M., Vermetten, E., Olff, M., et al. (2020). Efficacy of Immersive PTSD Treatments: A Systematic Review of Virtual and Augmented Reality Exposure Therapy and a Meta-Analysis of Virtual Reality Exposure Therapy. J. Psychiatr. Res. S0022-3956 (20), 31089–X. doi:10.1016/j.jpsychires.2020.11.030
Feldman, P. J., Cohen, S., Hamrick, N., and Lepore, S. J. (2004). Psychological Stress, Appraisal, Emotion and Cardiovascular Response in a Public Speaking Task. Psychol. Health 19 (3), 353–368. doi:10.1080/0887044042000193497
Freeman, D., Garety, P. A., Bebbington, P., Slater, M., Kuipers, E., Fowler, D., et al. (2005). The Psychology of Persecutory Ideation II. J. nervous Ment. Dis. 193 (5), 309–315. doi:10.1097/01.nmd.0000161686.53245.70
Gamito, P., Oliveira, J., Rosa, P., Morais, D., Duarte, N., Oliveira, S., et al. (2010). PTSD Elderly War Veterans: A Clinical Controlled Pilot Study. Cyberpsychology, Behav. Soc. Networking 13 (1), 43–48. doi:10.1089/cyber.2009.0237
Gilbert, S. B. (2016). Perceived Realism of Virtual Environments Depends on Authenticity. Presence: Teleoperators and Virtual Environments 25 (4), 322–324. doi:10.1162/pres_a_00276
Gromer, D., Madeira, O., Gast, P., Nehfischer, M., Jost, M., Müller, M., et al. (2018). Height Simulation in a Virtual Reality CAVE System: Validity of Fear Responses and Effects of an Immersion Manipulation. Front. Hum. Neurosci. 12, 372. doi:10.3389/fnhum.2018.00372
Grübel, J., Weibel, R., Jiang, M. H., Hölscher, C., Hackman, D. A., and Schinazi, V. R. (2016). “EVE: A Framework for Experiments in Virtual Environments,” in Spatial Cognition X (Bremen: Springer), 159–176.
Haagen, J. F. G., Smid, G. E., Knipscheer, J. W., and Kleber, R. J. (2015). The Efficacy of Recommended Treatments for Veterans with PTSD: A Metaregression Analysis. Clin. Psychol. Rev. 40, 184–194. doi:10.1016/j.cpr.2015.06.008
Jaycox, L. H., Foa, E. B., and Morral, A. R. (1998). Influence of Emotional Engagement and Habituation on Exposure Therapy for PTSD. J. consulting Clin. Psychol. 66 (1), 185–192. doi:10.1037/0022-006x.66.1.185
Jennett, C., Cox, A. L., Cairns, P., Dhoparee, S., Epps, A., Tijs, T., et al. (2008). Measuring and Defining the Experience of Immersion in Games. Int. J. human-computer Stud. 66 (9), 641–661. doi:10.1016/j.ijhcs.2008.04.004
Johnson, D., and Wiles, J. (2003). Effective Affective User Interface Design in Games. Ergonomics 46 (13-14), 1332–1345. doi:10.1080/00140130310001610865
Krijn, M., Emmelkamp, P. M. G., Biemond, R., de Wilde de Ligny, C., Schuemie, M. J., and van der Mast, C. A. P. G. (2004). Treatment of Acrophobia in Virtual Reality: The Role of Immersion and Presence. Behav. Res. Ther. 42 (2), 229–239. doi:10.1016/s0005-7967(03)00139-6
Lane, R., McRae, K., Reiman, E., Chen, K., Ahern, G., and Thayer, J. (2009). Neural Correlates of Heart Rate Variability during Emotion. NeuroImage 44 (1), 213–222. doi:10.1016/j.neuroimage.2008.07.056
McMahan, A. (2013). “Immersion, Engagement, and Presence: A Method for Analyzing 3-D Video Games,” in The Video Game Theory Reader (London: Routledge), 89–108.
Narciso, D., Bessa, M., Melo, M., and Vasconcelos-Raposo, J. (2019). “Virtual Reality for Training-The Impact of Smell on Presence, Cybersickness, Fatigue, Stress and Knowledge Transfer,” in 2019 International Conference on Graphics and Interaction (ICGI), Faro, Portugal (IEEE).
Nijdam, M. J., and Vermetten, E. (2018). Moving Forward in Treatment of Posttraumatic Stress Disorder: Innovations to Exposure-Based Therapy. Eur. J. Psychotraumatology 9 (1), 1458568. doi:10.1080/20008198.2018.1458568
Parsons, T. D., and Rizzo, A. A. (2008). Affective Outcomes of Virtual Reality Exposure Therapy for Anxiety and Specific Phobias: A Meta-Analysis. J. Behav. Ther. Exp. Psychiatry 39 (3), 250–261. doi:10.1016/j.jbtep.2007.07.007
Philippot, P., Chapelle, G., and Blairy, S. (2002). Respiratory Feedback in the Generation of Emotion. Cogn. Emot. 16 (5), 605–627. doi:10.1080/02699930143000392
Picard, L., Abram, M., Orriols, E., and Piolino, P. (2017). Virtual Reality as an Ecologically Valid Tool for Assessing Multifaceted Episodic Memory in Children and Adolescents. Int. J. Behav. Develop. 41 (2), 211–219. doi:10.1177/0165025415616198
Ranasinghe, N., Cheok, A., Nakatsu, R., and Do, E. Y-L. (2013). “Simulating the Sensation of Taste for Immersive Experiences,” in Proceedings of the 2013 ACM international workshop on Immersive media experiences, New York, USA.
Reijnen, A., Rademaker, A. R., Vermetten, E., and Geuze, E. (2015). Prevalence of Mental Health Symptoms in Dutch Military Personnel Returning from Deployment to Afghanistan: A 2-Year Longitudinal Analysis. Eur. Psychiatr. 30 (2), 341–346. doi:10.1016/j.eurpsy.2014.05.003
Richardson, L. K., Frueh, B. C., and Acierno, R. (2010). Prevalence Estimates of Combat-Related Post-Traumatic Stress Disorder: Critical Review. Aust. N. Z. J. Psychiatry 44 (1), 4–19. doi:10.3109/00048670903393597
Riva, G., Waterworth, J. A., Waterworth, E. L., and Mantovani, F. (2011). From Intention to Action: The Role of Presence. New Ideas Psychol. 29 (1), 24–37. doi:10.1016/j.newideapsych.2009.11.002
Riva, G., Waterworth, J. A., and Waterworth, E. L. (2004). The Layers of Presence: A Bio-Cultural Approach to Understanding Presence in Natural and Mediated Environments. CyberPsychology Behav. 7 (4), 402–416. doi:10.1089/cpb.2004.7.402
Rizzo, A., Pair, J., McNerney, P. J., Eastlund, E., Manson, B., Gratch, J., et al. (2005). Development of a VR Therapy Application for Iraq War Military Personnel with PTSD. Stud. Health Technol. Inform. 111, 407–413.
Rizzo, A. S., and Shilling, R. (2017). Clinical Virtual Reality Tools to Advance the Prevention, Assessment, and Treatment of PTSD. Eur. J. Psychotraumatology 8 (Suppl. 5), 1414560. doi:10.1080/20008198.2017.1414560
Rothbaum, B. O., Price, M., Jovanovic, T., Norrholm, S. D., Gerardi, M., Dunlop, B., et al. (2014). A Randomized, Double-Blind Evaluation Ofd-Cycloserine or Alprazolam Combined with Virtual Reality Exposure Therapy for Posttraumatic Stress Disorder in Iraq and Afghanistan War Veterans. Am. J. Psychiatry 171 (6), 640–648. doi:10.1176/appi.ajp.2014.13121625
Rubin, M., Hien, D. A., Das, D., and Melara, R. D. (2017). Inhibitory Control under Threat: The Role of Spontaneous Eye Blinks in Post-Traumatic Stress Disorder. Brain Sci. 7 (2), 16. doi:10.3390/brainsci7020016
Schnyder, U., Ehlers, A., Elbert, T., Foa, E. B., Gersons, B. P. R., Resick, P. A., et al. (2015). Psychotherapies for PTSD: What Do They Have in Common. Eur. J. Psychotraumatology 6 (1), 28186. doi:10.3402/ejpt.v6.28186
Schubert, T., Friedmann, F., and Regenbrecht, H. (2001). The Experience of Presence: Factor Analytic Insights. Presence: Teleoperators & Virtual Environments 10 (3), 266–281. doi:10.1162/105474601300343603
Serrano, B., Baños, R. M., and Botella, C. (2016). Virtual Reality and Stimulation of Touch and Smell for Inducing Relaxation: A Randomized Controlled Trial. Comput. Hum. Behav. 55, 1–8. doi:10.1016/j.chb.2015.08.007
Siegel, D. J. (2020). The Developing Mind: How Relationships and the Brain Interact to Shape Who We Are. New York: Guilford Publications.
Slater, M. (1999). Measuring Presence: A Response to the Witmer and Singer Presence Questionnaire. Presence 8 (5), 560–565. doi:10.1162/105474699566477
Stoffregen, T., Pagulayan, R., Smart, L., and Bardy, B. (2003). “On the Nature and Evaluation of Fidelity in Virtual Environments,” in Virtual and Adaptive Environments: Applications, Implications, and Human Performance Issues, 111–128. (Mahwah: CRC Press). doi:10.1201/9781410608888.ch6
Sweetser, P., and Wyeth, P. (2005). GameFlow. Comput. Entertain. 3 (3), 3. doi:10.1145/1077246.1077253
Tielman, M., van Meggelen, M., Neerincx, M. A., and Brinkman, W-P. (2015). “An Ontology-Based Question System for a Virtual Coach Assisting in Trauma Recollection,” in International conference on intelligent virtual agents, Delft, The Netherlands (Springer).
Toet, A. (2006). Gaze Directed Displays as an Enabling Technology for Attention Aware Systems. Comput. Hum. Behav. 22 (4), 615–647. doi:10.1016/j.chb.2005.12.010
van Dooren, M., de Vries, J. J. G., and Janssen, J. H. (2012). Emotional Sweating across the Body: Comparing 16 Different Skin Conductance Measurement Locations. Physiol. Behav. 106 (2), 298–304. doi:10.1016/j.physbeh.2012.01.020
van Gelderen, M. J., Nijdam, M. J., Haagen, J. F. G., and Vermetten, E. (2020). Interactive Motion-Assisted Exposure Therapy for Veterans with Treatment-Resistant Posttraumatic Stress Disorder: A Randomized Controlled Trial. Psychother Psychosom 89 (4), 215–227. doi:10.1159/000505977
van Gelderen, M. J., Nijdam, M. J., de Vries, F., Meijer, O. C., and Vermetten, E. (2020). Exposure-related Cortisol Predicts Outcome of Psychotherapy in Veterans with Treatment-Resistant Posttraumatic Stress Disorder. J. Psychiatr. Res. 130, 387–393. doi:10.1016/j.jpsychires.2020.08.011
van Gelderen, M. J., Nijdam, M. J., Dubbink, G. E., Sleijpen, M., and Vermetten, E. (2020). Perceived Treatment Processes and Effects of Interactive Motion-Assisted Exposure Therapy for Veterans with Treatment-Resistant Posttraumatic Stress Disorder: a Mixed Methods Study. Eur. J. Psychotraumatology 11 (1), 1829400. doi:10.1080/20008198.2020.1829400
van Gelderen, M. J., Nijdam, M. J., and Vermetten, E. (2018). An Innovative Framework for Delivering Psychotherapy to Patients with Treatment-Resistant Posttraumatic Stress Disorder: Rationale for Interactive Motion-Assisted Therapy. Front. Psychiatry 9, 176. doi:10.3389/fpsyt.2018.00176
Vermetten, E., and Bremner, J. D. (2003). Olfaction as a Traumatic Reminder in Posttraumatic Stress Disorder: Case Reports and Review. J. Clin. Psychiatry 64, 202–207. doi:10.4088/jcp.v64n0214
Vermetten, E., Meijer, L., van der Wurff, P., and Mert, A. (2013). The Effect of Military Motion-Assisted Memory Desensitization and Reprocessing Treatment on the Symptoms of Combat-Related post Traumatic Stress Disorder: First Preliminary Results. Stud. Health Technol. Inform. 191, 125–127. doi:10.3233/978-1-61499-282-0-125
Visch, V. T., Tan, E. S., and Molenaar, D. (2010). The Emotional and Cognitive Effect of Immersion in Film Viewing. Cogn. Emot. 24 (8), 1439–1445. doi:10.1080/02699930903498186
Waterworth, E. L., and Waterworth, J. A. (2001). Focus, Locus, and Sensus: The Three Dimensions of Virtual Experience. CyberPsychology Behav. 4 (2), 203–213. doi:10.1089/109493101300117893
Waterworth, J. A., and Waterworth, E. (2003). The Core of Presence: Presence as Perceptual Illusion. Presence Connect. 3 (3), 1–11.
Witmer, B. G., and Singer, M. J. (1998). Measuring Presence in Virtual Environments: A Presence Questionnaire. Presence: Teleoperators & Virtual Environments 7 (3), 225–240. doi:10.1162/105474698565686
Witvliet, C. V. O., Ludwig, T. E., and Laan, K. L. V. (2001). Granting Forgiveness or Harboring Grudges: Implications for Emotion, Physiology, and Health. Psychol. Sci. 12 (2), 117–123. doi:10.1111/1467-9280.00320
Keywords: post-traumatic stress disorder, virtual reality, immersion, presence, veterans, user experiment, tailored therapy, exposure therapy
Citation: van Veelen N, Boonekamp RC, Schoonderwoerd TA, van Emmerik ML, Nijdam MJ, Bruinsma B, Geuze E, Jones C and Vermetten E (2021) Tailored Immersion: Implementing Personalized Components Into Virtual Reality for Veterans With Post-Traumatic Stress Disorder. Front. Virtual Real. 2:740795. doi: 10.3389/frvir.2021.740795
Received: 13 July 2021; Accepted: 20 September 2021;
Published: 30 September 2021.
Edited by:
Julie Gore, Birkbeck, University of London, United KingdomReviewed by:
Kelsey Sprang Jones, Emory University, United StatesRaúl Duron-Figueroa, National Autonomous University of Mexico, Mexico
Copyright © 2021 van Veelen, Boonekamp, Schoonderwoerd, van Emmerik, Nijdam, Bruinsma, Geuze, Jones and Vermetten. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nancy van Veelen, bi52YW5fdmVlbGVuQGx1bWMubmw=