
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Virtual Real., 02 September 2021
Sec. Virtual Reality in Medicine
Volume 2 - 2021 | https://doi.org/10.3389/frvir.2021.720523
This article is part of the Research TopicVirtual Reality Applications in Military and Veteran Medicine and HealthcareView all 8 articles
 Lora Appel1,2*
Lora Appel1,2* Eva Appel2
Eva Appel2 Erika Kisonas2
Erika Kisonas2 Zain Pasat1
Zain Pasat1 Khrystyna Mozeson1
Khrystyna Mozeson1 Jaydev Vemulakonda1
Jaydev Vemulakonda1 Lacey (Qing) Sheng3
Lacey (Qing) Sheng3Background: Many veterans with dementia placed in long term care exhibit responsive behaviours such as physical and verbal responsiveness (e.g., shouting, hitting, biting, grabbing). Responsive behaviours lead to negative clinical outcomes, staff burnout, contribute to absenteeism, low engagement, and an elevated risk of abuse or neglect. Virtual Reality (VR) has shown great promise in relieving stress and improving quality of life in frail older adults and has been increasingly explored as a non-pharmacological therapy for people with dementia. Ongoing studies are evaluating the clinical outcomes of VR-therapy for this population, but the challenges and learnings of the healthcare providers who administer VR-therapy remain under-reported.
Objective: Capture the experiences of Recreational Therapists (RTs) who conducted study sessions and administered VR-therapy to residents with dementia as part of a clinical trial that took place at the Perley and Rideau Veterans’ Health Centre. We collected: RTs’ feedback on the process of conducting research, specifically with respect to technical, environmental and personal challenges, learnings, and recommendations.
Methods: In-depth interviews were conducted with all seven RTs who administered VR-therapy and collected data for a trial that took place from January-December 2019. Interviews were audio-recorded, transcribed, anonymized, and imported into the NVivo analysis tool, where two independent researchers coded the interviews into themes.
Results: RTs reported ease in learning to use the VR-technology, main challenges were unfamiliarity with, and insufficient time allocated to, conducting research. Scheduled VR-therapy sessions were physically and emotionally easier for the RTs to administer. Despite RTs hesitations to place the VR-equipment on frail individuals in distress, RTs reported positive impacts on managing responsive behaviours during these few targeted sessions, especially for participants for whom the trigger was related to physical pain rather than emotional distress. Staff have continued to offer scheduled VR-therapy sessions beyond the duration of the study.
Conclusion: The experience of using VR in the veteran resident population is generally positive. Areas for improvements including better support to the RTs regarding to novel interventions and research method. Feedback received from RTs in this study provides critical information to support successful, sustainable implementation of VR-therapy, both for further evaluation and as a regular activity program. Failure to consider the experiences of these vital stakeholders when developing novel interventions contributes to the gap between efficacy in research and effectiveness in practice.
A large proportion of veterans suffer from post-traumatic stress disorder (PTSD) and older individuals with this condition have a twofold increased risk of dementia (Yaffe et al., 2010). In addition to the association of PTSD with accelerated brain aging, other common factors within the veteran population, such as the occurrence of depression, head injury, or medical comorbidities, further increase the likelihood of developing dementia (Yaffe et al., 2010). At the Perley and Rideau Veteran’s Health Centre (Perley Rideau), 67% of veterans have a diagnosis of dementia (Canadian Institute for Health Information, 2019). Most people diagnosed with dementia will exhibit behavioural and psychological symptoms of dementia (BPSD), and some of the responsive behaviours, such as physical and verbal responsiveness (e.g., shouting, hitting, biting, grabbing) are more often exhibited by veterans with dementia, than the general population with dementia (Dunt et al., 2012; Charles, 2020). Physical responsiveness was observed in 17.3% of the total veteran population. Moreover, 21% of veteran residents were recorded with previously mental health history (Canadian Institute for Health Information, 2019).
In addition to negatively impacting clinical outcomes for people with dementia, BPSDs are a main source of psychological distress for caregivers (Song and Oh, 2015) – both informal caregivers (i.e., family, friends, etc.) in community settings and formal caregivers (i.e., nurses, personal support workers, etc.) in institutional settings. Numerous studies show that care staff experience difficulties, feelings of guilt, and distress when dealing with aberrant thoughts or vocally disruptive behaviour (Bourbonnais and Ducharme, 2010; Hertogh et al., 2004). Morgan et al. (2012) reported that the frequency of disruptive behaviour increases distress on formal caregivers and can lead to staff burnout, contribute to absenteeism, low engagement, and elevated risk of patient abuse or neglect (Song and Oh, 2015; Islam et al., 2017). A negative cycle can then occur, where patients increasingly react negatively and exhibit responsive behaviours in response to burnt-out caregivers, leading to situations that are even more difficult for caregivers to manage (Miyamoto et al., 2010; Song and Oh, 2015). In fact, previous studies have reported that the prevalence of BPSD is higher in nursing homes (91–96%) than in the community setting (56–98%), and that the severity of BPSD in nursing home residents is more serious than those in the community (Cerejeira et al., 2012; Song and Oh, 2015; Charles, 2020). In general, being placed in a long-term care (LTC) facility is correlated with the progression of dementia and worsening symptoms (Fuh, 2006; University of South Australia, 2007; Charles, 2020).
For many, the progression of dementia in the veteran population results in placement in LTC facilities. As of March 31, 2018, Veterans Affairs Canada (VAC) was supporting 5,110 veterans in approximately 1,318 nursing homes and other LTC facilities across Canada (Veterans Affairs Canada, 2019). The physical and emotional challenges associated with caring for residents at these institutions results in high turnover of nursing staff, difficulty in securing staff, and chronic staff shortages (Tanaka et al., 2015). This is a serious concern, especially as the population ages; statistics indicate that a growing number of people will develop dementia and will need care in the coming years (Tanaka et al., 2015; Canadian Institute for Health Information, 2018).
As such, there is urgency to develop interventions that help formal caregivers manage BPSDs, improve quality of life (QoL) and care for people with dementia, but also in order to reduce the burden and burnout among caregivers. Currently, antipsychotic medications are still frequently used as the first line treatment for BPSDs, despite evidence of only limited efficacy and their association with cognitive and physical decline (University of South Australia, 2007). Clinicians have turned their attention to various non-pharmacological therapies as first line treatment recommendations. Among non-pharmacological interventions, recent evidence provides support for the efficacy of familiar music, light therapy, reminiscence, and changes to the physical environment (Dyer et al., 2017; Scales et al., 2018). Following in their footsteps, Virtual Reality (VR) has shown great promise in relieving stress and improving QoL in frail older adults, and is increasingly explored as a potential non-pharmacological therapy to manage BPSDs.
Since the release of mobile immersive VR head mounted displays (HMDs) in 2014, there has been an explosion of research and applications of VR. In older adult populations, VR has been explored as a means to conduct cognitive training, activities of daily living (ADL) exercises, physical rehabilitation exercises, falls prevention exercises, screen for mild cognitive impairment, as well as engage, relieve stress, and improve QoL (Snowdon, 1997; Beason-Held et al., 2013; D’Cunha et al., 2019; Liu et al., 2019; Phu et al., 2019; Appel et al., 2020; Clay et al., 2020; Matsangidou et al., 2020). More recently, VR has been suggested as a means to manage BPSDs in people with dementia, with some early studies showing promising results (Appel et al., 2020; Appel et al., 2021).
Clinicians and researchers hypothesize that VR-therapy may help manage instances of distress through distraction, a technique used often in pain-management (Carr and Goudas, 1999; Makris et al., 2014). There is substantial research supporting the use of VR for the attenuation of acute pain during medical procedures (Li et al., 2011). VR systems may be particularly well suited to distract individuals because of the level of immersion; stimulating multiple senses (e.g., visual and auditory) simultaneously, while occluding the user’s view of the real environment, generates a feeling of presence of “being there” in the virtual environment. Moreover, modern VR headsets are increasingly lightweight, easier to operate, simpler to disinfect, and more affordable, making the technology a valuable addition to a recreational therapist’s (RT) toolkit.
A growing body of research is evaluating the clinical outcomes and collects information about experiences with VR-therapy for people with dementia, However, the challenges and learnings of the healthcare-providers/therapists who conduct the sessions and administer VR-therapy remain under-reported. Although this is not unique to VR-therapy, it remains a serious oversight that can have detrimental consequences. Failure to consider the experiences of these vital stakeholders when developing novel interventions contributes to the gap between efficacy in research and effectiveness in practice, and can have a negative impact on the success of deploying and sustaining the initiatives.
Our team conducted a clinical trial to evaluate the impact of VR-therapy on managing responsive behaviours in veterans and community residents of the Perley and Rideau Veteran’s Health Centre, the outcomes of which are documented in a separate manuscript. The current article reports on the results of a complementary study conducted with the Recreational Therapist’s (RTs) responsible for administering the VR-therapy intervention to veterans at the centre.
Our primary objective was to capture the experiences of the seven RTs who conducted the study sessions and administered VR-therapy to residents with dementia in a research study at Perley Rideau. We were interested in RT’s feedback on the process of conducting the study, specifically with respect to technical, environmental, and personal challenges. We were also interested in RT’s learnings, recommendations, and perspectives on what they considered successful elements of the intervention.
This is a complementary study to a clinical trial conducted at Perley Rideau. This complementary study used in-depth interviews with RTs from Perley Rideau to gather information related to their experiences administering VR-therapy to residents and conducting the clinical trial. The interviewed participants (RTs) were assigned and subsequently referred to by de-identified study numbers. Verbal informed consent to participate in the complementary study was provided by each participant at the beginning of their interview before audio-recording began. Research ethics board approval was provided by York University (Ethics Protocol reference #2756).
The Perley and Rideau Veteran’s Health Centre is one of the largest and most progressive long-term care (LTC) homes in Ontario. The Perley Rideau campus includes 450 long-term care beds, a Seniors Village with 139 independent-living apartments for seniors and many clinical, therapeutic and recreational services available on-site. The Centre of Excellence in Frailty-Informed Care (CoE), established at Perley Rideau in 2019, conducts applied research, and identifies, develops, and shares best practices in the care of frail older adults.
The Perley Rideau Therapeutic Recreation and Creative Arts team is experienced in supporting veterans with dementia and responsive behaviours. At the time of this study, this team included 3 recreation therapists (RTs), approximately 12 recreation programmers and many others. The recreation therapists oversee the coordination of activities and resident plan of care, while the recreation programmers are in charge of program deliveries. Due to a shortage of funding, there are limited recreation therapist positions in LTC. Many of the recreation programmers employed in the sector are also qualified as recreation therapists. All 7 staff involved in this study are trained recreation professionals, therefore generally referred to as RTs regardless of their position at the Perley Rideau.
The Resident Assessment Instrument-Minimum Data Set (RAI-MDS) data from 2019 fourth quarter indicated that 66.7% of veteran residents at Perley Rideau had a diagnosis of dementia. Physical responsiveness was observed in 17.3% of the total veteran population. Moreover, 21% of veteran residents were recorded with previous mental health history. (Canadian Institute for Health Information, 2019).
Similar to other LTC homes, the Perley Rideau faces challenges with burnout in the workforce. According to a single question survey administered at the Perley Rideau in March 2020, 83 percent of Registered Practical Nurses and 63 percent of Personal Support Workers reported some symptoms of burnout.
During the months of January to December 2019, veterans and community residents residing in a dementia ward at Perley Rideau, who were exhibiting responsive behaviours, were recruited to participate in a clinical study, and assigned to one of two groups in the study: Group A received “scheduled VR sessions” akin to other recreational activities, at a mutually convenient time during the day; Group B received “targeted VR sessions” occurring just before or during events known to trigger responsive behaviours (e.g., before bathing). A total of 111 VR-therapy sessions took place, of which 88% (98/111) were scheduled and 12% (13/111) were targeted. Residents in both groups received the same VR-therapy intervention, which consisted of watching 360° VR video footage (also known as ‘VR experiences’ of natural and social scenes, using an Oculus Go head-mounted-display (HMD) (Oculus Go, n.d.). The VR experiences used in the study at Perley Rideau consist of a collection of short 360° VR recordings of various nature scenes (e.g., rocky lakeshore, sunny forest, dense forest, floating icebergs, and sunny beach), nature-themed YouTube videos, or Google street-view walk-throughs. These VR experiences were specifically created or selected from existing sources, in consultation with experts in the field of multisensory Integration and Aging to mitigate the effects of motion and simulator sickness, while maintaining passively interactive characteristics that support adequate stimulation for individuals with Alzheimer’s/dementia. For the study sessions, RTs were asking participating residents about their preferences regarding VR films themes, or they would start the session with a popular video among other participants.
The RTs were the main contact points with participating residents. The RTs explained the technology to participants and conducted the sessions, also collected observation data from these sessions. HCPs were also study participants in the clinical trial, recruited by RTs. They were only involved in targeted sessions. The HCPs provide care to the resident participants with responsive behaviour. The HCPs did not conduct any Virtual Reality therapy sessions. They participated in the clinical trial study by observing the impact of VR during targeted events that involves them.
Figure 1 depicts an RT helping a senior try on the VR HMD. RTs from the Perley Rideau were trained to provide the therapy and collect study data in the form of participant feedback and structured observations. In addition, baseline clinical data and progress notes were extracted from the electronic patient record system.

FIGURE 1. Recreational therapist from the Perley Rideau helps a senior experience VR through an Oculus Go HMD.
Seven RTs who participated in the clinical trial at the Perley Rideau and conducted the VR-therapy study sessions with residents were recruited to be interviewed. A separate interview was conducted with each RT by one or two interviewers. Interviews took place after the completion of the clinical trial in December 2019, at a time convenient for the RT, using audio-conferencing software. Interviews were semi-structured, followed a predefined script (see Supplementary Material S1), and lasted on average 1 h. The researchers who conducted the interviews followed principles of good qualitative interviews, which, according to Dörnyei (2007), have two key features: 1) to flow naturally and 2) be rich in detail. To attain this, the researchers were encouraged to ‘listen’ not just speak (Dörnyei, 2007). Moreover, as per Richards (2003) ‘golden advice’, interviewers aimed not only to be neutral, but also “always seek the particular” (p. 53). Interviews were audio-recorded, transcribed using NVivo Transcription tool, and manually reviewed for accuracy and corrected where necessary by a member of the research team.
Transcribed interviews were imported into the NVivo qualitative data analysis software tool and analyzed using the grounded theory approach, an inductive process whereby researchers construct theory from data, systematically obtained and analyzed using comparative analysis (Charmaz and Belgrave, 2012; Chun Tie et al., 2019). Two researchers (LA and EA) independently reviewed the interview deemed richest in content and detail. Based on this interview, using an open coding approach, the researchers proposed a coding structure which was consolidated into an initial framework of high-level clusters (parent themes) and sub-categories (child themes) (Khandkar, 2021). This framework was intended to comprehensively capture and categorize as much of the interview content as possible, with the assumption that some codes and themes would be further revised in greater detail.
Subsequently, four research assistants (KM, JV, ZP, EK) coded the interviews. Two research assistants independently coded each transcript. Then, an NVivo coding comparison query was conducted to measure inter-coder reliability test, determining the degree of agreement between the coding done by two coders (statistically measured using the Kappa coefficient). When the Kappa coefficient did not meet the minimum acceptable value of 0.4 (indicating moderate agreement in qualitative research), the research team traced those discrepancies, reviewed and resolved the discrepancies, and revised the coding framework accordingly (McHugh, 2012). Two researchers (LA and EA) then used the constant comparison method, a data-analytic process whereby each finding is compared with existing findings as they emerge from the data analysis, to further categorize and refine the interview themes into narrower topics (Lewis-Beck et al., 2004).
Finally, the aggregated responses for each coded theme were analyzed and, based on the reported impact on the overall success of the project, classified into one of three categories: “positive factors”, “negative factors”, and “suggestions for improvement”. The characteristic was considered a “positive” factor if it was reported as contributor to the success of the project, relating to any of the elements under consideration by this study (e.g., conducting research, administering VR intervention, RTs personal/professional growth); it was a “negative” factor if it was identified as a barrier to, or negatively impacting the success of the project, whereas thoughts and ideas proposed as possible improvements were grouped as “suggestions” for improvement. The grouping of results into positive and negative, although not always bearing a well-defined delineation, was meant to help with the analysis, discussion, and together with the suggestions for improvement, ultimately helped formulate recommendations and future directions for this study.
The high-level clusters identified by qualitatively analyzing the transcribed interviews, were: 1) Conducting the Research, 2) Using the Technology, and 3) Administering the Therapy. Details about the frequency of coded themes and topics, with the relevant quotes from the interviews listed by study participant number, are provided in Supplementary Material S2.
The sections below summarize the results obtained from the qualitative analysis of the interviews, presented by cluster, grouped by positive factors, negative factors, and participant suggestions. In some cases, select quotes from the interviews are presented.
The following aspects were reported as beneficial for the research study: the opportunity to purchase VR technology for the veteran’s health centre, the conditions made available for RTs to try VR with the residents (which would not have occurred without the study), and the experience of participating in a research study (which resulted in personal/professional growth and satisfaction for the staff involved). Moreover, due to their familiarity with and knowledge of the residents living at the centre, RTs felt very confident in their ability to accurately determine the reactions and feelings of residents receiving VR-therapy through subjective observation, even though resident’s eyes were covered by the HMD. Some RTs stated that even without personal familiarity with an individual, they would be able to deduce, at least in part, the effect of VR on the participant.
“Yes, I could tell right away if they (were) enjoying it or not even if they were not telling me. I would be able to see if he enjoys that because I have seen (…) I feel when you work so close with specific people you kind of know if they like something or not” (P1).
“Yes, I feel comfortable, just based on my history and experiences working with these types of residents that have dementia whether it is early stages or late stages. I can just tell if someone is kind of like rigid or stiffening up or not even moving their head or just by seeing their mouth even, because everything is covered up. I think, even if I would not know the resident, I think I would still be pretty confident in being able to tell if they’re getting anything out of it or if it is a negative response or a positive one” (P5).
Several drawbacks and challenges were reported to have negatively impacted the study, hampering the opportunity to introduce VR as a therapy to residents with dementia at the Perley Rideau.
Insufficient time allocated to conducting the study was the number one challenge raised by participants (mentioned explicitly by all seven RTs) which impacted the ability of staff to delivery VR-therapy during the study sessions. Although there were a number of backfilled shifts scheduled to support staff to participate in the study, given that the majority of sessions are conducted within the normal worked hours, it proved to be an insufficient amount of time to carry out the requirements of the study, as well as fulfil regular duties throughout the shift.
“For the most part my difficulty that I found was timing. We did not really have protected time to do this project. It was kind of we doing our daily job and as well trying to fit this in” (P4).
The lack of previous experience conducting research was another frequently reported challenge. Many RTs working in long-term care are not exposed to research as part of their normal scope of work, and therefore may not have understood the importance of adhering to the study protocol. This led to inconsistencies in data collection which may have impacted the validity of the outcomes.
“…so even though at every beginning we had the training session and there is research fellow. I do not think it hit the home what research was, there could be more knowledge thrown at the beginning” (P6).
Finally, another significant challenge expressed by RTs, was the difficulty in recruiting and consenting HCPs. As per the original study protocol, HCPs were required to be study participants in order to conduct the “targeted” VR sessions with residents. Recruiting HCPs was difficult for a variety of reasons, predominantly due to the expressed lack of time to participate in additional activities beyond their required workload (feeling they were already being overworked and understaffed). Another reason for HCPs unwillingness to join the study was their reluctance or refusal to allow their (human resources) data to be collected.
“Targeted it was just I guess a lot more time. I find it really, we all, kind of struggle to find staff that wanted to agree to do it. A lot of people were really iffy “Oh, I do not want them to see my hours” or whatever, even if it’s anonymous” (P1).
“Getting the nursing staff on the board - that was challenging ... I think I was surprised at how hard it was to get suitable residents for it and definitely with the staff. I was shocked at how many people did not want to participate” (P5).
Some RTs mentioned that having a personal relationship with HCPs made recruitment slightly easier. However, even for those who agreed to participate, it was difficult to schedule time to conduct sessions.
This cluster focuses on the usability of the VR system (equipment), both for the RTs when administering the VR-therapy, and for the residents receiving VR-therapy. For the most part, the off-the-shelf devices: Oculus HMD, iPad tablet, and Samsung 360 Camera were reported to be acceptable, but it was felt that some specific alterations could make the equipment far more effective for administering VR-therapy to this frail, older adult population.
Positive factors included the ease of use by staff and the overall comfort expressed by residents. Most staff found the VR HMD easy to get used to, taking at most a few weeks of experimentation with the device. Qualitative feedback from RTs demonstrated that they were able to add films from the internet (i.e., YouTube VR) and films that staff had recorded themselves using the Samsung camera to the device library.
“Yes, I was pretty comfortable with using it (HMD) on my own right away” (P4).
“I am not (tech) savvy but maybe at the same time I figured it (the VR system) out” (P6).
RTs completed an adapted version of the Systems Usability Scale, which is a validated tool that quantitatively measures usability of new technology/devices, and was adapted to refer to VR system specifically (Brooke, 1996). Table 1 reports the mean score of each question and the total weighted score. The mean of the total weighted scores was 72.5, equating to a score of “B”, meaning “Good” usability.
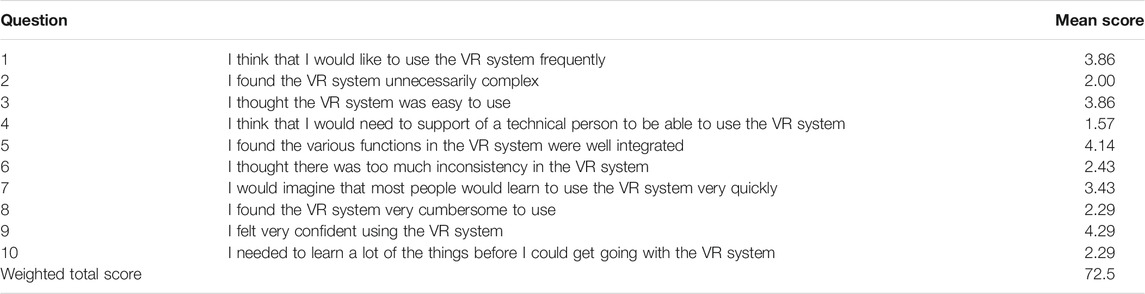
TABLE 1. SUS Results for VR System (Oculus Go HMD).
In terms of the quality of experience for the residents (acceptability of the visuals and the audio), the RTs reported positive experiences with few minor complaints. The headset was used with and without eyeglasses with no correlation to focus or quality of image. While some residents had to be prompted to look left and right with the headset on, RTs reported that the HMD was intuitive for others, who would explore the virtual environment on their own.
“No, I found it quite easy actually, the residents that I had done it with were very, again other than the one, were really open to it and I had no problem putting it on. And one gentleman he really enjoyed turning his head completely and everything was very (easy). He was even able to take it off and on himself” (P2).
Negative factors included problems with the HMD (straps used to secure the device, and the weight), as well as poor connectivity with the internet and the paired device.
Many RTs raised issues with the soft elastic straps used to secure the headset on the resident’s head. Straps were problematic for residents because they sometimes added to distress by increasing pressure on the head, and sometimes they would pull on their hair.
“Twenty percent were strapped on, and eighty percent not. The care ones yes it was always strapped on so maybe little bit more than that. So the care one was always strap on but if I would do just scheduled most of them were (…) they were holding it or I would” (P1).
A number of residents also expressed that the weight of the headset was challenging, although the RTs that were able to compare the Oculus Go used in this study to other VR HMDs, used for different projects at the Perley Rideau, found that the Oculus Go was the most light-weight.
“No, just the one I had mentioned that was heavy, that’s why I think there was lots of residents we had to physically hold on. Because their frailty we just had to hold it. But not as far as discomfort, no” (P2).
“I’ve tried other ones - where I am doing internship at the hospital – it’s a heavier set I do not know the name of it. But it is way heavier than Oculus one. Even when I try that at the other place I felt “wow this is good the guys were part of this study have the lighter one” … I do not remember which other one I was trying” (P5).
Internet connectivity was briefly mentioned by some as an issue when wanting to watch videos from YouTube, but the cause of this issue was unclear; the solution of downloading films to the device prior to the session was readily available. Pairing the iPad to the VR headset presented unique challenges. Screen mirroring using a secondary device (i.e., iPad) was useful for the RTs, allowing them to see what the residents were viewing in real time to provide prompts or assist navigation. Screen mirroring was also used so that a second person (i.e., family member) could jointly experience the VR environment alongside the resident. Screen mirroring was difficult due to the need to use Bluetooth, but also, once the devices were successfully paired, a red dot would appear in the HMD while the resident was viewing a film. Although this was a design feature (intended to make the viewer aware that an external person is watching the same VR experience simultaneously), this red dot was confusing and distracting for the residents with dementia that participated in the study.
“The only thing is that streaming or pairing to the tablet. It is not that I am not uncomfortable with it. It is frustrating when it disconnects in the middle of the session with a resident and you can no longer can see what they are looking at” (P2).
“No, I remember though when we first started with the first headset that we got - whenever you connected the iPad there would be red dot in the headset. I remember a few of them actually were like: “what’s the red dot? what’s the red dot?” but that is the only thing that I can remember about like, an unfortunate visual thing” (P4).
This cluster shows the RTs feedback regarding their experiences and perceived outcomes of administering VR-therapy to the residents, keeping in mind that the objective of the interviews with the RTs was not to collect outcomes of the VR-therapy, but rather to capture a detailed account and recollection of the sessions and gain a deeper understanding of RT’s experiences, challenges, and perceived usefulness of VR as a therapy.
Several positive experiences reported by the RTs suggest that VR-therapy can help improve resident’s mood, encourage reminiscence, and boost alertness, especially for participants in the scheduled sessions.
“I had one recently the other day that I can recall. There is gentleman, at the time I went to visit him I went with the purpose of doing some VR. I went to his room and he was kind of sleepy, kind of in and out of doziness. So I had pulled up on the VR his old house where he raised his kids. And showed him that and he perks right up and he was pointing out the garden and saying: “oh it is not quite how I left it (interviewer chuckle), I remember planting a certain tree”. I found out after the session he was much more alert” (P4).
For residents participating in targeted sessions VR-therapy was reported to result in better management of symptoms, such as aggressiveness, particularly when responsive behaviours were caused by physical pain (e.g., removal of leg braces) rather than emotional distress (e.g., calling out for their family). These effects were directly observed by the RTs throughout the study, but were also reflected in RTs documentation of the HCP’s reactions, if they were present during targeted sessions.
“Oh, yes that leg one for example … I do remember … The health care aide, she - I did not know that gentlemen that well I work sometimes but definitely not at night when he goes to bed or when he gets his leg braces off - but she told me and I remember writing this down and she was like “wow, wow that’s just so much better than every other night of the week that I put him to bed, he was so calm” that was definitely positive” (P5).
“And I showed him this video when he was getting his brace removed. He was just engaged with it like he was like … there was snow everywhere in the video. He loved it (laugh). Okay, it got to the point where I was like “I got to take the video off now okay?” (P7).
Negative factors included confusion about the VR-therapy and unpredictable reactions from residents. The targeted sessions were far more challenging to conduct than the scheduled sessions for a number of reasons. First, although triggered behaviours were assumed to be predictable, they did not always occur at expected and consistent times, making the planning of these sessions rather difficult. Secondly, when a trigger event did occur, or was anticipated to occur in the near future, bringing together sufficient staff (HCPs) to provide the care and administer VR-therapy was incredibly difficult.
Finally, targeted sessions were challenging and conducted far less frequently than planned because of emotional reactions that RTs experienced towards residents in distress. About half of the RTs (43%, 3/7) reported feeling hesitant to place the VR HMD on residents who exhibited any signs of distress and feeling concerned about aggravating (rather than decreasing) responsive behaviours.
“But trying it when she was in a real agitated state - just sort of not forcing the elastic band over her head - but I just felt like “I am doing more harm than good?” but we try it anyways … She did not take to it, I think I got it on no more than 5 s before I took off. The whole experience to putting on and off it was no more than 10 s, I stopped right away. But I just kind of felt I do not how morally correct this is” (P7).
“I did not really agree with it during when someone was having responsive behaviours. Some of the lashing out, kicking out, it seems kind of awkward to walk towards them with a headset and kind of do that” (P4).
Along with reporting their challenges with the VR-therapy clinical study, RTs provided suggestions which they expected that, if adopted in the future, could benefit various aspects of the Research, the Technology, and the VR-Therapy areas. To improve the research quality, 29% (2/7) of RTs recommended to allocate more protected time for the research team to conduct the study, to equip them with substantial research training, and have more frequent check-ins through a “community of practice” where RTs using the technology could help troubleshoot common problems and share useful tips.
Suggestions addressing issues with the technology included providing formal training for the staff accompanied by aids and tools (e.g., explanatory videos) that could be revisited at any time later into the study. In addition, one (14%, 1/7) RT suggested setting up a common account to sync all devices at a given time, so the same updated version of software is available on every HMD used for the study.
Finally, all RTs had recommendations for how VR could be administered more effectively and broadly across the Perley Rideau. Many (43%, 3/7) suggested that physical frailty and mental alertness/engagement were stronger indicators of challenges with administering VR-therapy, than age or cognitive ability (proxy for severity of dementia). Some RTs (29%, 2/7) reflected that those with dementia that are lower functioning were less likely to engage with the VR experiences, and therefore may benefit from this intervention to a lesser degree. RTs observed that residents that enjoyed being active and were more curious, seemed to be better candidates; some (29%, 2/7) RTs mentioned the trait of being “open-minded” being common amongst good candidates for VR-therapy. Others indicated that this intervention could aid residents that are more introverted and do not usually participate in group activities, and could therefore benefit from taking part in more diverse experiences. Staff expressed the value of leveraging family members to understand resident’s preferences and personal backgrounds to meaningfully customize the content for each resident.
Familiarity with the resident would help determine the best time of day to administer the VR-therapy (e.g., schedule of predictable responsive behaviours, time of day when resident is most lucid, etc.). Some RTs thought it would be better to task the permanent staff with administering VR-therapy, rather than the new or casual/temporary staff who were not sufficiently familiar with the residents. Overall feedback showed that conducting VR-therapy in a room with other residents present was an effective way to generate interest amongst residents and stimulate conversation, with the caveat that this could make hearing the audio more difficult than during a session in a private, quieter room.
Regarding the difficulty of assembling staff for conducting the VR-therapy targeted sessions, one RT suggested providing a pager to the staff members responsible for administering VR-therapy, so that they could be alerted to bring the VR system when a trigger for responsive behaviours was about to occur.
The primary objective of this qualitative study was to capture the experiences of the RTs who administered VR-therapy to residents with dementia, as part of an interventional clinical trial at the Perley and Rideau Veteran’s Health Centre. The information gained from interviewing all seven participating RTs is crucial for several reasons. Firstly, understanding the challenges with conducting research involving veterans with dementia at a long-term care institution can help:
1) Design future studies with protocols and methods that are feasible for this population in this setting.
2) Allocate the necessary resources to conduct similar studies.
3) Provide adequate training and regular check-ins with staff who are conducting the study.
Secondly, through these interviews we uncovered valuable insights that will help with designing instruments for studies evaluating VR for populations with dementia, which present significant challenges in gathering participant feedback.
Despite the support system in place, the main challenges faced by the RTs in conducting the clinical trial were the unfamiliarity with conducting research studies and insufficient time allocated to conduct this research; both of these may have negatively impacted the rigor of the study and adherence to the study protocol. The RTs reported difficulties recruiting HCPs into the study, obtaining informed consent for the residents, coordinating study sessions with other health-care providers within the regular workflow at the centre, and collecting data.
An important objective of the VR-therapy clinical trial was to evaluate the impact of VR-therapy in scenarios where responsive behaviours were triggered based on a predictable event (operationalized through “targeted” VR-therapy sessions). Unfortunately, only a limited number of targeted sessions were conducted due to the aforementioned reasons. It was highly challenging to assemble the required staff (nurses and RTs) to be present, on short notice, to administer and evaluate VR-therapy while providing the necessary care during a triggered event.
An unexpected finding that needs to be accounted for in future studies, was RT’s personal emotional reactions, such as hesitancy, around placing the VR HMD on frail individuals in distress. Hesitancy often affected the RT’s ability to administer VR-therapy; this also contributed to the small number of targeted sessions. This barrier may be alleviated with additional evidence of success in these instances, provided through training.
It was reassuring to validate, based on strong feedback, that RT’s were very confident in the accuracy of their perceptions of resident’s reactions and mood changes during the VR-therapy study sessions. This confidence was present when resident’s eyes were occluded by the HMD and/or when residents were unable to express or communicate how they felt in VR. Some RT’s stated that even without personal familiarity with an individual they would be able to deduce, at least in part, the effect of VR-therapy on the participant.
There seemed to be a consensus that scheduled VR-therapy sessions (when participants were not in an acute moment of panic or distress), were physically and emotionally easier for the RT’s to administer. However, even with the relatively small number of targeted VR-therapy sessions, RT’s reported positive impacts on managing responsive behaviours, especially for participants for whom the responsive behaviour trigger was related to physical pain rather than emotional distress. A common opinion shared by all RTs was that familiarity with the resident (i.e., knowing the person and understanding their preferences) was an important factor for success. They concluded that there is no “one right way” but that each resident should be treated as an individual with their own distinct therapy plan.
All RTs reported ease in learning to use the VR technology, and that having dedicated time to experiment or “try-out” the VR devices prior to starting the sessions was helpful. Overall, the off-the-shelf VR equipment (hardware and software) was acceptable with only few issues, that if addressed (mostly by the manufacturers), would greatly improve the experience for those administering the VR-therapy as well as for those receiving it. Important improvements include finding a better method to affix the headset (replacing the straps), developing lighter-weight headsets, and accommodating populations with visual and auditory impairments (e.g., no inference with hearing aids and image focus options for users with/without glasses). Another important element to consider, especially for the population with cognitive impairment, is designing a simpler way to connect to a secondary device (i.e., screen mirroring) so that another person can simultaneously view the VR experience.
Feedback suggested that VR-therapy can be an effective tool in targeted sessions by employing distraction techniques, and in scheduled sessions as conversation aid/prompting tool. Although conducting research provided staff at the Perley Rideau unique opportunities, the research experience had many drawbacks; the challenges were thought to have overall negatively impacted opportunities to provide VR-therapy to residents.
The authors feel the interviews accurately reflected the experiences of RTs, as all (seven) of the study RTs participated, showed convergence between their description of events, and saturation on the topics covered was reached.
Using the results of this study, we provide a set of recommendations that include evidence-based advice and suggestions for 1) the institutions launching similar research studies, and 2) the personnel that administer VR-therapy to residents with dementia.
At the institutional, management or research department level, it is recommended that similar initiatives dedicate sufficient resources, such as more protected time for the participating staff conducting the study, and a stronger focus around research training. Research training should take into consideration RT’s previous familiarity with research, ensure that objectives of the study are understood and the importance of following the study protocol is known and acknowledged. Also reference tools should be made available for staff to refresh their memories. If possible, more research team members tasked with conducting study sessions and collecting data should be involved early in the study design process to ensure the protocol is feasible in terms of staffing, timing, and workflow at the institution. At the protocol design stage, this study only engaged with two of the seven RT’s who were tasked later with conducting the study; they did not anticipate the challenges faced with the targeted approach. Frequent check-ins with the study team should be introduced to provide staff with the opportunity to ask questions, share experiences, elaborate on challenges, and collectively agree upon courses of action should the protocol need to be revised. This research team conducted team meetings every other week, which focuses on discussions and questions around the research protocols. A common computer account should be created for all VR-systems used for a specific VR initiative, enabling synchronization of the video libraries across all devices. This way, all devices are interchangeable between staff and all the videos are available in the same place on each device, making navigation smooth and predictable.
Below are specific recommendations for the staff that administer VR-therapy, either within a research project or as a regular therapy/activity program at an institution:
• Prepare for the session by turning the VR headset on before approaching the resident.
• Ensure that the direction of focus is set up properly for the position the resident is in (lying in a bed, sitting in a chair).
• Try giving the resident “control” - by having them touch/feel/hold up the headset prior to turning on the films.
• If this is the first session, try to demonstrate VR without using the head straps. Have the resident hold the headset up to their own eyes if they are able; then, once the resident is more familiar and comfortable, introduce head straps (or wait with this for the follow-up sessions).
• Consider resident preferences, and if unknown, start with the most popular film (e.g., the beach scene).
• Create opportunities for “choice” – such as the type/subject of VR experiences, the preferred location for the resident, and the time of day.
• Have a series of “cue” questions ready to prompt the resident to engage in the virtual environments.
• After a session, headsets should always be charged so that they are ready for the next session.
The study was based on interviews, which inherently carry some amount of bias, as well as other drawbacks: “what people say in an interview will indeed be shaped, to some degree, by the questions they are asked; the conventions about what can be spoken about; (...)…by what they think the interviewer wants; by what they believe he/she would approve or disapprove of” (Hammersley and Gomm, 2008). To mitigate some of these limitations, the research team made an effort to design guided interviews and conduct them as soon as possible (at most 2 weeks) after the completion of the clinical trial (to keep memories fresh). The interview script included impartial questions to encourage responses about both positive and negative experiences, as well as open-ended questions to allow participants to express thoughts on topics not covered by the script. The researchers who conducted the interviews were not working directly with the participant RTs, so participants were comfortable sharing honest feedback about their experiences without fear of repercussions (e.g., opinions towards the work environment). Additionally, while reliability is notoriously scrutinized in interview-based research, our team attempted to remove bias by ensuring that two independent reviewers coded each transcript into relevant themes using similar methods.
While the RT’s responses from the interviews reflect experiences at the Perley Rideau, the conclusions and recommendations derived from their experiences may not be generalizable to other long-term-care institutions, which may vary in levels of available resources and background knowledge on conducting research or how to administer VR-therapy.
The feedback collected from RT’s in this study provided critical information to help with successful, sustainable implementation of VR-therapy evaluation efforts or activity programs. Despite the difficulties RT’s encountered while conducting research, the overwhelming response regarding the introduction of VR-therapy for veterans with dementia was positive. Staff at the Perley Rideau have added VR-therapy to their toolkit of recreational activities and continued to provide VR-therapy as scheduled sessions beyond the duration of the study. We strongly recommend further research to examine the impact of VR-therapy on triggered responsive behaviours, with re-designed study protocols that address the challenges reported by RT’s in this study. While no definitive conclusions could be drawn from the small sample of residents that participated in targeted VR-sessions, feedback from RT’s suggest that there is potential for VR-therapy to be beneficial in the management of responsive behaviours, especially for pain-related triggers.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by The Office of Research Ethics, York University. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
LA and EA contributed to conception and design of the study. LS organized the onsite data collection. EA and LA designed the coding structure. EK, ZP, JV, and KM performed the data cleaning and qualitative coding. LA, EA, and EK wrote the first draft of the manuscript. All authors contributed to manuscript revision, read, and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to thank the Centre for Brain Health and Innovation for their generous support. We are grateful to Codrin Talaba for working with our research team to film, edit, and provide the VR experiences for this study. Finally, we would like to acknowledge the Perley Rideau Therapeutic Recreation and Creative Arts Program as well as the Perley Rideau Centre of Excellence for cooperating and collaborating with the research team on this study.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frvir.2021.720523/full#supplementary-material
Appel, L., Appel, E., Bogler, O., Wiseman, M., Cohen, L., Ein, N., et al. (2020). Older Adults with Cognitive And/or Physical Impairments Can Benefit from Immersive Virtual Reality Experiences: A Feasibility Study. Front. Med. 6. doi:10.3389/fmed.2019.00329
Appel, L., Kisonas, E., Appel, E., Klein, J., Bartlett, D., Rosenberg, J., et al. (2020). Introducing Virtual Reality Therapy for Inpatients with Dementia Admitted to an Acute Care Hospital: Learnings from a Pilot to Pave the Way to a Randomized Controlled Trial. Pilot Feasibility Stud. 6. doi:10.1186/s40814-020-00708-9
Appel, L., Kisonas, E., Appel, E., Klein, J., Bartlett, D., Rosenberg, J., et al. (2021). Administering Virtual Reality Therapy to Manage Behavioral and Psychological Symptoms in Patients with Dementia Admitted to an Acute Care Hospital: Results of a Pilot Study. JMIR Form Res. 5, e22406. doi:10.2196/22406
Beason-Held, L. L., Goh, J. O., An, Y., Kraut, M. A., O'Brien, R. J., Ferrucci, L., et al. (2013). Changes in Brain Function Occur Years before the Onset of Cognitive Impairment. J. Neurosci. 33, 18008–18014. doi:10.1523/jneurosci.1402-13.2013
Bourbonnais, A., and Ducharme, F. (2010). The Meanings of Screams in Older People Living with Dementia in a Nursing home. Int. Psychogeriatr. 22, 1172–1184. doi:10.1017/s1041610209991670
Brooke, J. (1996). SUS: A Quick and Dirty Usability Scale. Usability Evaluation in Industry Editors P. W. Jordan, I. McClelland, and B. Weerdmeester (Taylor and Francis), 207–212. doi:10.1201/9781498710411-35
Canadian Institute for Health Information (2018). Dementia in Canada: Summary. Ottawa: Canadian Institute for Health Information. Available at: https://www.cihi.ca/en/dementia-in-canada/dementia-in-canada-summary (Accessed May 5, 2021).
Canadian Institute for Health Information (2019). Internal RAI-MDS Report. [Unpublished Manuscript].
Carr, D. B., and Goudas, L. C. (1999). Acute Pain. The Lancet 353, 2051–2058. doi:10.1016/s0140-6736(99)03313-9
Cerejeira, J., Lagarto, L., and Mukaetova-Ladinska, E. B. (2012). Behavioral and Psychological Symptoms of Dementia. Front. Neur. 3. doi:10.3389/fneur.2012.00073
Charles, J. (2020). Innovative Care for Veterans with Dementia. Hospital News. Available at: https://hospitalnews.com/innovative-care-for-veterans-with-dementia/(Accessed April 14, 2021).
Charmaz, K., and Belgrave, L. L. (2012). Qualitative Interviewing and Grounded Theory Analysis. The SAGE Handbook Interview Research: The Complexity of the Craft Editors J. F. Gubrium, J. Holstein, A. B. Marvasti, and K. McKinney (Sage), 347–366. doi:10.4135/9781452218403.n25
Chun Tie, Y., Birks, M., and Francis, K. (2019). Grounded Theory Research: A Design Framework for Novice Researchers. SAGE Open Med. 7, 205031211882292. doi:10.1177/2050312118822927
Clay, F., Howett, D., Fitzgerald, J., Fletcher, P., Chan, D., and Price, A. (2020). Use of Immersive Virtual Reality in the Assessment and Treatment of Alzheimer's Disease: A Systematic Review. Jad 75, 23–43. doi:10.3233/jad-191218
D'Cunha, N. M., Nguyen, D., Naumovski, N., McKune, A. J., Kellett, J., Georgousopoulou, E. N., et al. (2019). A Mini-Review of Virtual Reality-Based Interventions to Promote Well-Being for People Living with Dementia and Mild Cognitive Impairment. Gerontology 65 (4), 430–440. doi:10.1159/000500040
Dörnyei, Z. (2007). Research Methods in Applied Linguistics: Quantitative, Qualitative, and Mixed Methodologies. Oxford: Oxford University Press, 140.
Dunt, D., Doyle, C., MacFarlane, A., Morris, P., Hunter, C., and Day, S. (2012). The Impact of War Experiences on Dementia in Veterans. Australian Government Department of Veterans' Affairs. Available at: https://www.dva.gov.au/documents-and-publications/impact-war-experiences-dementia-veterans-2012 (Accessed May 5, 2021).
Dyer, S. M., Harrison, S. L., Laver, K., Whitehead, C., and Crotty, M. (2017). An Overview of Systematic Reviews of Pharmacological and Non-pharmacological Interventions for the Treatment of Behavioral and Psychological Symptoms of Dementia. Int. Psychogeriatr. 30, 295–309. doi:10.1017/s1041610217002344
Fuh, J. L. (2006). Study of Behavioral and Psychological Symptoms of Dementia in Taiwan. Acta Neurol. Taiwan 15, 154–160.
Hammersley, M., and Gomm, R. (2008). Questioning Qualitative Inquiry: Critical Essays. Thousand Oaks: Sage Publications, 89–100. doi:10.4135/9780857024565.d7
Hertogh, C. M. P. M., Anne Mei The, B., Miesen, B. M. L., and Eefsting, J. A. (2004). Truth Telling and Truthfulness in the Care for Patients with Advanced Dementia: an Ethnographic Study in Dutch Nursing Homes. Soc. Sci. Med. 59, 1685–1693. doi:10.1016/j.socscimed.2004.02.015
Islam, M. S., Baker, C., Huxley, P., Russell, I. T., and Dennis, M. S. (2017). The Nature, Characteristics and Associations of Care home Staff Stress and Wellbeing: a National Survey. BMC Nurs. 16. doi:10.1186/s12912-017-0216-4
Khandkar, S. H. (2021). Open Coding. Available at: http://pages.cpsc.ucalgary.ca/∼saul/wiki/uploads/CPSC681/open-coding.pdf (Accessed May 5, 2021). doi:10.3390/ifou2018-05936
Lewis-Beck, M., Bryman, A., and Futing Liao, T. (2004). The SAGE Encyclopedia of Social Science Research Methods. doi:10.4135/9781412950589
Li, A., Montaño, Z., Chen, V. J., and Gold, J. I. (2011). Virtual Reality and Pain Management: Current Trends and Future Directions. Pain Manag. 1, 147–157. doi:10.2217/pmt.10.15
Liu, Y., Tan, W., Chen, C., Liu, C., Yang, J., and Zhang, Y. (2019). A Review of the Application of Virtual Reality Technology in the Diagnosis and Treatment of Cognitive Impairment. Front. Aging Neurosci. 11. doi:10.3389/fnagi.2019.00280
Makris, U. E., Abrams, R. C., Gurland, B., and Reidundefined, M. C. (2014). Management of Persistent Pain in the Older Patient. JAMA 312, 825. doi:10.1001/jama.2014.9405
Matsangidou, M., Schiza, E., Hadjiaros, M., Neokleous, K. C., Avraamides, M., Papayianni, E., et al. (2020). Dementia: I Am Physically Fading. Can Virtual Reality Help? Physical Training for People with Dementia in Confined Mental Health Units. Lecture Notes in Computer Science Universal Access in Human-Computer Interaction. Des. Approaches Supporting Tech. 12188, 366–382. doi:10.1007/978-3-030-49282-3_26
McHugh, M. L. (2012). Interrater Reliability: the Kappa Statistic. Biochem. Med. 22, 276–282. doi:10.11613/bm.2012.031
Miyamoto, Y., Tachimori, H., and Ito, H. (2010). Formal Caregiver Burden in Dementia: Impact of Behavioral and Psychological Symptoms of Dementia and Activities of Daily Living. Geriatr. Nurs. 31, 246–253. doi:10.1016/j.gerinurse.2010.01.002
Morgan, D. G., Cammer, A., Stewart, N. J., Crossley, M., D'Arcy, C., Forbes, D. A., et al. (2012). Nursing Aide Reports of Combative Behavior by Residents with Dementia: Results from a Detailed Prospective Incident Diary. J. Am. Med. Directors Assoc. 13, 220–227. doi:10.1016/j.jamda.2011.07.003
Oculus Go (n.d.). Experience The Next Level of Wireless VR. Available at: https://www.oculus.com/go/(Accessed April 15, 2021).
Phu, S., Vogrin, S., Al Saedi, A., and Duque, G. (2019). Balance Training Using Virtual Reality Improves Balance and Physical Performance in Older Adults at High Risk of Falls. Cia 14, 1567–1577. doi:10.2147/cia.s220890
Richards, K. (2003). Qualitative Inquiry in TESOL. Basingstoke: Palgrave Macmillan. doi:10.1057/9780230505056
Scales, K., Zimmerman, S., and Miller, S. J. (2018). Evidence-Based Nonpharmacological Practices to Address Behavioral and Psychological Symptoms of Dementia. The Gerontologist 58, S88–S102. doi:10.1093/geront/gnx167
Snowdon, D. A. (1997). Aging and Alzheimer's Disease: Lessons from the Nun Study. The Gerontologist 37, 150–156. doi:10.1093/geront/37.2.150
Song, J.-A., and Oh, Y. (2015). The Association between the Burden on Formal Caregivers and Behavioral and Psychological Symptoms of Dementia (BPSD) in Korean Elderly in Nursing Homes. Arch. Psychiatr. Nurs. 29, 346–354. doi:10.1016/j.apnu.2015.06.004
Tanaka, K., Iso, N., Sagari, A., Tokunaga, A., Iwanaga, R., Honda, S., et al. (2015). Burnout of Long-Term Care Facility Employees: Relationship with Employees' Expressed Emotion toward Patients. Int. J. Gerontol. 9, 161–165. doi:10.1016/j.ijge.2015.04.001
University of South Australia (2007). Antipsychotics in Dementia. Veterans' MATES. Available at: https://www.veteransmates.net.au/topic-12-therapeutic-brief (Accessed March 31, 2021).
Veterans Affairs Canada (2019). Introduction - Veterans Affairs Canada. 1.0 Introduction. Available at: https://www.veterans.gc.ca/eng/about-vac/publications-reports/reports/departmental-audit-evaluation/2019-evaluation-long-term-care/1-0 (Accessed April 15, 2021).
Keywords: virtual reality, long term care, non-pharmacologic, recreational therapist, recreational therapy/activities, dementia, behavioural and psychiatric symptoms of dementia, responsive behaviour
Citation: Appel L, Appel E, Kisonas E, Pasat Z, Mozeson K, Vemulakonda J and Sheng L( (2021) Virtual Reality for Veteran Relaxation (VR2) – Introducing VR-Therapy for Veterans With Dementia – Challenges and Rewards of the Therapists Behind the Scenes. Front. Virtual Real. 2:720523. doi: 10.3389/frvir.2021.720523
Received: 04 June 2021; Accepted: 22 July 2021;
Published: 02 September 2021.
Edited by:
Julie Gore, University of Bath, United KingdomReviewed by:
Laura E. Watkins, Emory University, United StatesCopyright © 2021 Appel, Appel, Kisonas, Pasat, Mozeson, Vemulakonda and Sheng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lora Appel, bG9yYS5hcHBlbEB1aG4uY2E=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.