
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Urol. , 28 March 2023
Sec. Neurourology, Behavioural Urology, and Urodynamics
Volume 3 - 2023 | https://doi.org/10.3389/fruro.2023.1158260
 Andrei Krassioukov1,2,3*
Andrei Krassioukov1,2,3* Blayne Welk4Desiree Vrijens5Sabrina Islamoska6Kim Bundvig Barken7Veronique Keppenne8Michel Wyndaele9
Blayne Welk4Desiree Vrijens5Sabrina Islamoska6Kim Bundvig Barken7Veronique Keppenne8Michel Wyndaele9 Matthias Walter1,10
Matthias Walter1,10The value of disposable, single-use catheters has come under scrutiny in recent years with a growing attention on environmental sustainability. Intermittent catheterization (IC) is a widely available and minimally invasive technique for management of lower urinary tract dysfunction. Effective IC for individuals with neurogenic lower urinary tract dysfunction can promote their independence and improve quality of life. Are there alternative options within IC that could minimize environmental impact without compromising the safety and effectiveness of single-use catheters? How does the future of IC look – environmentally friendly, biodegradable, disposable catheters may be complementary to certified reusable catheters? In the midst of this debate, it is important to emphasize that individuals have the right to choose the best evidence-based treatment available. Here we consider the current landscape for IC with a focus on chronic use in individuals with neurogenic lower urinary tract dysfunction.
A considerable number of individuals living with neurogenic lower urinary tract dysfunction (NLUTD) rely on intermittent catheterization (IC) for their bladder management. Currently, there is much debate over which type of catheter – single-use or reusable – provides the safest and most effective management solution, whilst minimizing cost and environmental impact. This article considers the current landscapes for single-use and reusable catheters.
NLUTD is a consequence of various neurological disorders, such as spinal cord injury (SCI), multiple sclerosis (MS), stroke, dementia, spina bifida (SB), and peripheral neuropathy, such as diabetes mellitus (1, 2). The extent of NLUTD depends on the location (e.g., brain region or spinal cord level) and severity of neurological impairment (3). Common symptoms of NLUTD include urinary incontinence, urinary retention, and/or changes in bladder and urethral sensations (3–5).
The overall global prevalence of neurourological disorders, such as NLUTD, is difficult to establish (6). Nevertheless, prevalence rates for the various underlying conditions alongside sporadic data on the frequency of neurourological symptoms in these populations can provide a useful indication of the potential scale of the problem (Table 1).
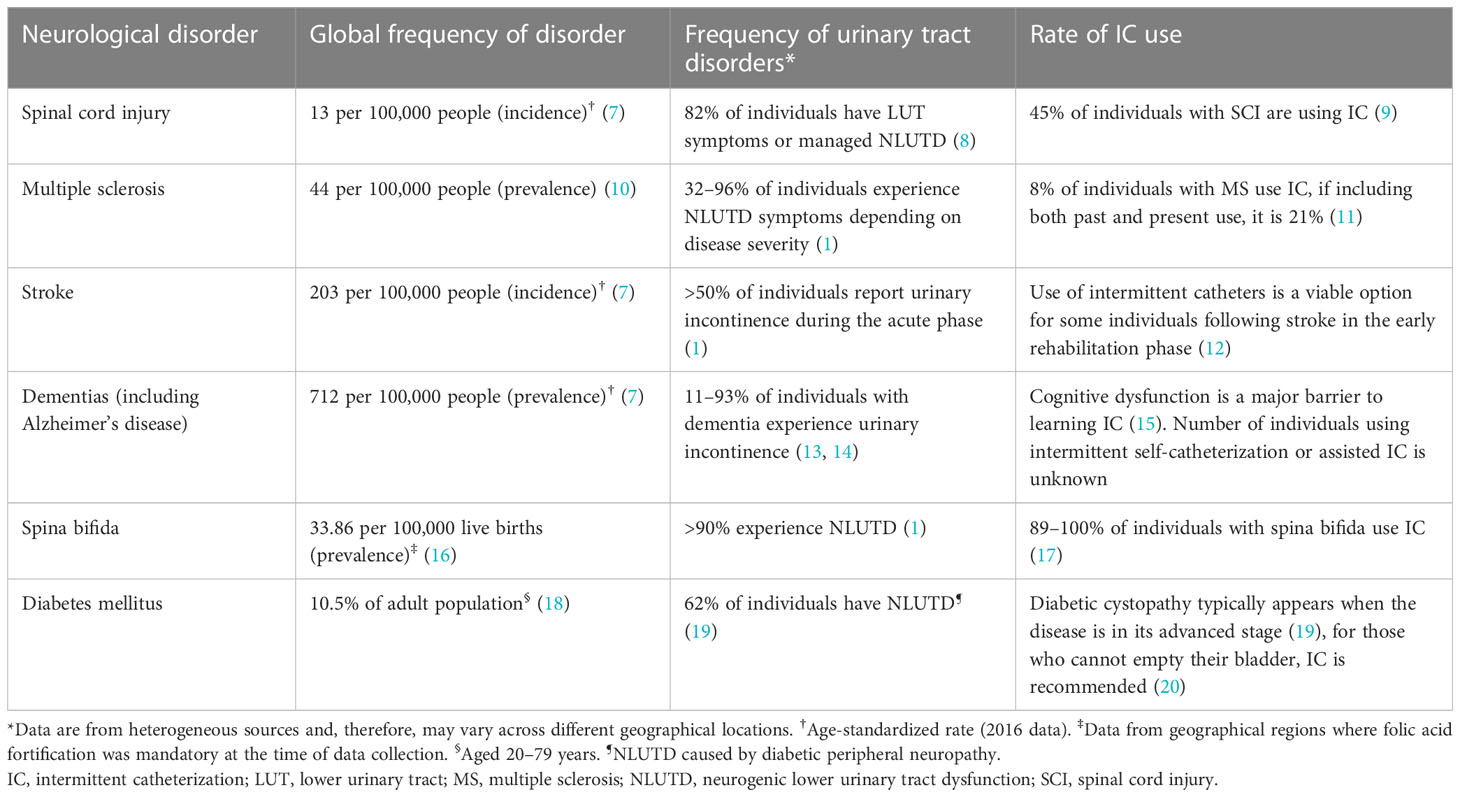
Table 1 Epidemiology of neurological conditions underlying urinary tract disorders.
The Global Burden of Disease study (2016 data) has shown that neurological disorders are the leading cause of disease burden on a global scale, with stroke being the largest contributing factor (7, 21). With an aging population and an increase in the number of individuals affected by neurological disorders, this global burden continues to grow, posing a challenge to healthcare systems, many of which are already overstretched (7). In addition, the added burden of NLUTD in individuals with neurological disorders places even more pressure on healthcare systems.
NLUTD has been shown to have a significant socio-economic burden (22), while also having a considerable negative impact on an individual’s health-related quality of life (HRQoL) (23–27). A Danish registry study has demonstrated a significantly greater number of total hospitalizations, outpatient visits and primary healthcare contacts, and longer inpatient stays during the first year after a diagnosis of NLUTD in individuals with SCI or MS versus controls from the general population (matched by age, gender, marital status, municipality, and education; all p<0.05) (5). The burden specifically due to lower urinary tract (LUT) and bowel complications was also significantly increased (5). These complications often required hospitalization and antibiotic therapy (5, 28). Furthermore, earned income was reduced by up to threefold versus matched controls, which was countered by an increase in income transfer payments, mainly in the form of disability pension and sick pay (5).
Neurological disorders and associated NLUTD can restrict many aspects of an affected individual’s life (29). For example, individuals with MS, SCI, or stroke who are experiencing NLUTD compared with neurologically intact individuals with normal independent bladder function, reported poorer HRQoL in terms of their physical, mental, and sexual health, and in other important aspects of life, such as socializing and travel (24). Improvements in HRQoL in these individuals can be achieved through effective management of NLUTD, with the goals of continence, voluntary bladder emptying (often with IC), preserved renal function, and a low risk of urinary tract infections (UTIs) (6, 30, 31). If not addressed, UTIs can escalate to urosepsis, a severe medical condition that can be life-threatening and can have considerable negative impacts on individuals and healthcare (32, 33). Crucially, for many individuals with NLUTD, effective management helps them to retain an element of independence in their everyday lives (34).
Approaches to the management of NLUTD vary between clinical settings and there is no evidence that any one particular solution is optimal for all (35). An appropriate intervention should be carefully considered and aligned with the individual’s profile (e.g., extent of NLUTD, potential previous LUT surgery, anatomical factors, dexterity, and general motor/cognitive ability) and personal preferences to promote the best chances of effective management for NLUTD (35). Effective management of NLUTD must be supported by appropriate training from multi-disciplinary teams (36).
Clinical guidelines recommend IC as the gold standard treatment for individuals with NLUTD with sufficient dexterity, who are unable to empty their bladder (6, 35, 37). IC is a widely available and minimally invasive technique that aims to promote an individual’s independence and improve their HRQoL (38).
Since the 1970s, IC has been performed using a ‘clean’ technique, which involves handwashing, regular genital hygiene, and catheter cleaning before reuse (35, 38). Over the years, the practice of IC has evolved from reusable to single-use catheters (38), due, in part, to a lack of evidence on appropriate storage and cleaning procedures, a perceived increased risk of UTIs for reusable catheters (39, 40), and a lack of certified and available reusable catheters in many countries. Currently, there is no conclusive evidence that reusable catheters are as safe as single-use (41). Longitudinal studies are necessary to establish the efficacy and safety profile of cleaning procedures for reusable catheters (42). Given the complexity of underlying conditions of individuals who require management for NLUTD, there is no single type of IC that is suitable for all. Based on the current evidence available, hydrophilic single-use catheters are considered to be the optimal choice for management of NLUTD due to a reduced risk of UTIs, improved HRQoL, and individual preference (31, 35, 40, 43–45). Individual preference is likely to improve compliance with IC which, in turn, ensures long-term successful management of NLUTD (44). However, depending on geographical location, access to specific types of catheters is limited by reimbursement policies, under-resourcing, and issues with funding (39). In the US, restrictions on the type of catheter available and on the quantities provided to users are important factors challenging the health and well-being of individuals with NLUTD (46). Many private insurers do not provide enough catheters per month to cover the number of catheterizations needed each day and, consequently, people resort to reusing single-use catheters, even though this is considered ‘off-label’ use (38). In Europe, only disposable single-use catheters are reimbursed (44, 47, 48). The situation is very different in developing countries where resources and funding are limited, which means that reusable or reuse of disposable catheters may be the only option available (3, 39).
Recently published reports highlight a growing concern over the environmental impact of nonbiodegradable plastic waste resulting from the use of disposable, single-use catheters (40, 47, 49), including the products, packaging, manufacturing processes, and transportation. It has been suggested that this environmental impact may be alleviated by using reusable catheters (40, 47, 49). Reusable catheters have also been advocated as a means of reducing the cost of managing NLUTD (41). There have been proposals that reusable catheters are more cost-effective than single-use options (41, 50); however, the available economic data do not consider the influence of individual preference for type of catheter, the individual variation in the daily frequency of catheterizations, the environmental and financial impact of catheter cleaning protocols, or the impact of downstream complications, such as UTIs. In countries where the cost can be covered by the healthcare system or individuals, single-use catheters should be considered as the preferred routine method of choice for the management of NLUTD (39).
In an era where sustainability is a key focus for developed countries, and limited funding/access to healthcare resources remains a problem for developing countries, the value of disposable, single-use catheters is firmly under the spotlight (51). Arguably, reusable catheters alleviate the environmental and economic pressures of catheterization, whereas single-use catheters address user comfort and the risk of UTIs (52); all of which are important considerations for individuals using IC (40). Presently the vast majority of IC are produced with single-use indication.
Reusing catheters requires appropriate, effective cleaning to reduce the risk of bacteria entering the bladder (53), and to avoid damaging the structural integrity of the catheter (42). Various catheter cleaning methods have been evaluated but, as yet, no uniform clinical recommendations on how to clean and reuse catheters exist (42, 44, 54). Evidence on the safety and efficacy of different cleaning methods must be established to help guide future clinical guidelines (42). Furthermore, the cleaning processes involved in using reusable catheters may not be achievable for all individuals with NLUTD, for example, individuals with cognitive impairment, restricted hand dexterity, or limited access to clean water, and may represent an additional burden for caregivers. Importantly, ‘off-label’ reuse of catheters that are intended and approved for single-use can, potentially, lead to unsafe practice, health risks, and other complications (55). It would also be prudent to consider the environmental impact of the cleaning fluids used in catheter reuse processes.
Whether the incidence of UTIs is affected by the type of catheter remains a matter of debate. Some studies suggest that the use of hydrophilic-coated catheters considerably lowers the risk of UTIs versus other catheters (31, 56, 57). Hydrophilic-coated catheters have also been reported to be cost-effective compared with uncoated catheters (58, 59). In contrast, a retrospective study of individuals with SCI in the US found that a shift from reusable to single-use catheters did not decrease hospitalizations for genitourinary symptoms, including UTIs (60). To date, however, no randomized controlled trial of sufficient sample size and adhering to an up-to-date UTI definition including catheter-associated UTIs has been conducted to evaluate the effectiveness of reusable versus single-use catheters (48, 61). The COMPaRE study (Netherlands) and the MultICath study (UK) are ongoing large-scale clinical trials designed, primarily, to determine if the incidence of UTIs is the same between reusable and single-use catheters (48, 62). A recent publication by Welk et al., 2022 reported a significantly higher risk of UTIs in individuals with neurogenic versus non-neurogenic conditions using IC (63). Therefore, considering the presence of an underlying neurological disorder in a mixed population of individuals with neurogenic and non-neurogenic conditions is key when interpreting data, as the treatment needs of these groups differ based on the underlying condition and its severity, course of disease, and IC dependency.
To consider the use of reusable catheters as a routine clinical practice, an appropriate framework for management, supported by evidence from adequate randomized clinical trials, which considers the individual’s disability and cognitive status, alongside any potential risks, must be available. In addition, training and educational resources for healthcare professionals should be implemented to ensure that individuals receive the support they require for effective management of NLUTD. Until there is scientific evidence that reusable catheters are not inferior to single-use with respect to long-term complications as mentioned previously, healthcare providers (HCPs) should continue to take a patient-centric approach to catheterization; choosing single-use or reusable catheters (once certified reusable catheters are available), or a combination of both, considering the specific requirements of each individual and their preferences for management of NLUTD. Different groups may require different recommendations, but they all require a simple and easy solution that is not associated with any major risks (safety or otherwise). It is the role of the HCP to ensure that individuals are well-informed of the benefits and risks before starting IC. Furthermore, the choice of catheter should not be based on financial aspects at the detriment of safety.
On the issue of sustainability, the responsibility of ensuring the safety of individuals using catheters (or any other medical device) for treatment purposes must be prioritized over minimizing environmental impact, without disregarding it. All medical devices should be optimally designed to deliver best performance on their intended purpose and manufactured using appropriate high-quality materials. This does not mean that sustainability should be compromised, but instead it should be considered at all steps in the process to achieve the same optimal outcome with the least environmental impact. It is important to consider ways in which the ‘catheter footprint’ could be reduced, for example, recycling used catheters or using biodegradable materials in catheter production (49). There have already been environmentally conscious moves toward reducing bulky packaging and manufacturing packaging from biodegradable and/or recyclable materials. Furthermore, reducing the need for additional lubricants could avoid the associated extra packaging waste. At present, catheters are treated as hazardous waste and have been excluded from recycling consideration (49). Therefore, the creation of facilities equipped to safely recycle used catheters would reduce the waste burden associated with IC (49). There have also been developments in the manufacturing of biodegradable catheters from materials such as water-soluble corn starch-based bioplastic and polyolefin-based elastomer, which have demonstrated better environmental performance compared with standard plastics used in catheter manufacturing (64, 65). It may be more prudent to explore environmentally friendly solutions rather than stopping the use of disposable catheters altogether. These solutions will not only require advances in technology but also changes in current legislation on medical devices to encompass sustainability as well.
Personal choice and access to the best care are important considerations for individuals when choosing treatment options for IC. Hydrophilic single-use catheters are, currently, regarded as the optimal choice for draining an individual’s bladder, whereas concerns remain over appropriate cleaning methods and infection risk for reusable catheters. Furthermore, from an individual perspective, switching from reusable catheters to single-use hydrophilic-coated catheters improved HRQoL and were the preferred choice among users (31). Acknowledging that sustainability is high on the current global agenda, the plastic waste (and carbon footprint) associated with disposable catheters is a critical issue. Therefore, individuals using plastic-based catheters may feel stigmatized. HCPs must be astute to the possibility of stigma to avoid consequences for mental health, which may already be impaired due to their LUT problems and associated symptom-driven behavior (e.g., frequent trips to the bathroom) (66, 67). Ultimately, HCPs are responsible for informing individuals of the most appropriate IC solution tailored to their individual needs and preferences to promote adherence.
Whilst the sustainability debate continues, it is important to remember that individuals must always have the right to choose the best evidence-based treatment available.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
The authors declare that this study received funding from Coloplast A/S. The funder had the following involvement with the study sponsoring medical writing assistance by CAMBRIDGE.
Writing and editorial assistance was provided by ‘Cambridge – a Prime Global Agency’, funded by Coloplast.
AK, BW, DV, VK, MiW and MaW are all part of the Global Expert Panel Advisory Board funded by Coloplast. KB and SI are employed by Coloplast.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Panicker JN. Neurogenic bladder: Epidemiology, diagnosis, and management. Semin Neurol (2020) 40:569–79. doi: 10.1055/s-0040-1713876
2. Agochukwu-Mmonu N, Pop-Busui R, Wessells H, Sarma AV. Autonomic neuropathy and urologic complications in diabetes. Auton Neurosci (2020) 229:102736. doi: 10.1016/j.autneu.2020.102736
3. Przydacz M, Denys P, Corcos J. What do we know about neurogenic bladder prevalence and management in developing countries and emerging regions of the world? Ann Phys Rehabil Med (2017) 60:341–46. doi: 10.1016/j.rehab.2017.02.008
4. Gajewski JB, Drake MJ. Neurological lower urinary tract dysfunction essential terminology. Neurourol Urodyn (2018) 37(S6):S25–31. doi: 10.1002/nau.23758
5. Buchter ML, Kjellberg J, Ibsen R, Sternhufvud C, Petersen B. Burden of illness the first year after diagnosed bladder dysfunction among people with spinal cord injury or multiple sclerosis – a Danish register study. Expert Rev Pharmacoecon Outcomes Res (2022) 22(6):919–26. doi: 10.1080/14737167.2022.2054804
6. Blok B, Castro-Diaz D, Del Popolo G, Hamid R, Karsenty G, Kessler TM, Pannek J. EAU guidelines on neuro-urology. Arnhem: EAU Guidelines Office (2022).
7. GBD 2016 Neurology Collaborators. Global, regional, and national burden of neurological disorders, 1990-2016: A systematic analysis for the global burden of disease study 2016. Lancet Neurol (2019) 18:459–80. doi: 10.1016/S1474-4422(18)30499-X
8. Anderson CE, Birkhäuser V, Jordan X, Liechti MD, Luca E, Möhr S, et al. Urological management at discharge from acute spinal cord injury rehabilitation: a descriptive analysis from a population-based prospective cohort. Eur Urol Open Sci (2022) 38:1–9. doi: 10.1016/j.euros.2022.01.005
9. Cameron AP, Wallner LP, Forchheimer MB, Clemens JQ, Dunn RL, Rodriguez G, et al. Medical and psychosocial complications associated with method of bladder management after traumatic spinal cord injury. Arch Phys Med Rehabil (2011) 92(3):449–56. doi: 10.1016/j.apmr.2010.06.028
10. Walton C, King R, Rechtman L, Kaye W, Leray E, Marrie RA, et al. Rising prevalence of multiple sclerosis worldwide: insights from the atlas of MS, third edition. Mult Scler (2020) 26(14):1816–21. doi: 10.1177/1352458520970841
11. Mahajan ST, Frasure HE, Marrie RA. The prevalence of urinary catheterization in women and men with multiple sclerosis. J Spinal Cord Med (2013) 36(6):632–7. doi: 10.1179/2045772312Y.0000000084
12. Holroyd S. Urinary incontinence after stroke. Br J Community Nurs (2019) 24(12):590–4. doi: 10.12968/bjcn.2019.24.12.590
13. Averbeck MA, Altaweel W, Manu-Marin A, Madersbacher H. Management of LUTS in patients with dementia and associated disorders. Neurourol Urodyn (2017) 36(2):245–52. doi: 10.1002/nau.22928
14. Sakakibara R, Uchiyama T, Yamanishi T, Kishi M. Dementia and lower urinary dysfunction: With a reference to anticholinergic use in elderly population. Int J Urol (2008) 15(9):778–88. doi: 10.1111/j.1442-2042.2008.02109.x
15. Balhi S, Arfaoui RB. Barriers affecting patient adherence to intermittent self-catheterisation. Br J Community Nurs (2021) 26(9):444–51. doi: 10.12968/bjcn.2021.26.9.444
16. Atta CAM, Fiest KM, Frolkis AD, Jette N, Pringsheim T, St Germaine-Smith C, et al. Global birth prevalence of spina bifida by folic acid fortification status: A systematic review and meta-analysis. Am J Public Health (2016) 106:e24–44. doi: 10.2105/AJPH.2015.302902
17. Faleiros F, Warschausky S, Käppler C, Schutt W, Cintra MM, Rabeh SAN, et al. Bladder self-management in the transition to adulthood with spina bifida in 3 countries: A comparative study. J Wound Ostomy Continence Nurs (2019) 46(4):321–6. doi: 10.1097/WON.0000000000000545
18. Sun H, Saeedi P, Karuranga S, Pinkepank M, Ogurtsova K, Duncan BB, et al. IDF diabetes atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract (2022) 183:109119. doi: 10.1016/j.diabres.2021.109119
19. Bolgeo T, Maconi A, Bertolotti M, Roveta A, Betti M, Gatti D, et al. Physiopathology of the diabetic bladder. Arch Ital Urol Androl (2020) 92(4):314–7. doi: 10.4081/aiua.2020.4.314
20. Nanigian DK, Keegan KA, Stone AR. Diabetic cystopathy. Curr Bladder Dysfunct Rep (2007) 2:197–202. doi: 10.1007/s11884-007-0020-1
21. Feigin VL, Vos T, Nichols E, Owolabi MO, Carroll WM, Dichgans M, et al. The global burden of neurological disorders: Translating evidence into policy. Lancet Neurol (2020) 19(3):255–65. doi: 10.1016/S1474-4422(19)30411-9
22. Palma-Zamora ID, Atiemo HO. Understanding the economic impact of neurogenic lower urinary tract dysfunction. Urol Clin North Am (2017) 44(3):333–43. doi: 10.1016/j.ucl.2017.04.001
23. Olesen JD, Kiddoo DA, Metcalfe PD. The association between urinary continence and quality of life in paediatric patients with spina bifida and tethered cord. Paediatr Child Health (2013) 18(7):e32–8. doi: 10.1093/pch/18.7.e32
24. Patel DP, Elliott SP, Stoffel JT, Brant WO, Hotaling JM, Myers JB. Patient reported outcomes measures in neurogenic bladder and bowel: A systematic review of the current literature. Neurourol Urodyn (2016) 35:8–14. doi: 10.1002/nau.22673
25. Nazari F, Shaygannejad V, Sichani MM, Mansourian M, Hajhashemi V. Quality of life among patients with multiple sclerosis and voiding dysfunction: A cross-sectional study. BMC Urol (2020) 20(1):62. doi: 10.1186/s12894-020-00590-w
26. Welk B. Quality of life in neurourology patients. Eur Urol Focus (2020) 6(3):531–3. doi: 10.1016/j.euf.2019.09.001
27. Moghalu O, Stoffel JT, Elliott S, Welk B, Lenherr S, Herrick J, et al. Psychosocial aspects of health-related quality of life and the association with patient-reported bladder symptoms and satisfaction after spinal cord injury. Spinal Cord (2021) 59(9):987–96. doi: 10.1038/s41393-020-00609-x
28. Gabbe BJ, Nunn A. Profile and costs of secondary conditions resulting in emergency department presentations and readmission to hospital following traumatic spinal cord injury. Injury (2016) 47:1847–55. doi: 10.1016/j.injury.2016.06.012
29. Browne C, Salmon N, Kehoe M. Bladder dysfunction and quality of life for people with multiple sclerosis. Disabil Rehabil (2015) 37:2350–8. doi: 10.3109/09638288.2015.1027007
30. Kessler TM, Ryu G, Burkhard FC. Clean intermittent self-catheterization: a burden for the patient? Neurourol Urodyn (2009) 28(1):18–21. doi: 10.1002/nau.20610
31. Newman DK, New PW, Heriseanu R, Petronis S, Håkansson J, Håkansson MÅ, et al. Intermittent catheterization with single- or multiple-reuse catheters: Clinical study on safety and impact on quality of life. Int Urol Nephrol (2020) 52:1443–51. doi: 10.1007/s11255-020-02435-9
32. McKibben MJ, Seed P, Ross SS, Borawski KM. Urinary tract infection and neurogenic bladder. Urol Clin North Am (2015) 42:527–36. doi: 10.1016/j.ucl.2015.05.006
33. Hajj J, Blaine N, Salavaci J, Jacoby D. The "Centrality of sepsis": A review on incidence, mortality, and cost of care. Healthcare (Basel) (2018) 6:90. doi: 10.3390/healthcare6030090
34. Goldstine J, Leece R, Samas S, Zonderland R. In their own words: Adults’ lived experiences with intermittent catheterization. J Wound Ostomy Continence Nurs (2019) 46:513–8. doi: 10.1097/WON.0000000000000591
35. Campeau L, Shamout S, Baverstock RJ, Carlson KV, Elterman DS, Hickling DR, et al. Canadian Urological Association best practice report: Catheter use. Can Urol Assoc J (2020) 14:E281–9. doi: 10.5489/cuaj.6697
36. Castel-Lacanal E, Gamé X, De Boissezon X, Guillotreau J, Braley-Berthoumieux E, Terracol C, et al. Impact of intermittent catheterization on the quality of life of multiple sclerosis patients. World J Urol (2013) 31:1445–50. doi: 10.1007/s00345-012-1017-8
37. Ginsberg DA, Boone TB, Cameron AP, Gousse A, Kaufman MR, Keays E, et al. The AUA/SUFU guideline on adult neurogenic lower urinary tract dysfunction: Treatment and follow-up. J Urol (2021) 206(5):1106–13. doi: 10.1097/JU.0000000000002239
38. Lamin E, Newman DK. Clean intermittent catheterization revisited. Int Urol Nephrol (2016) 48:931–9. doi: 10.1007/s11255-016-1236-9
39. New PW. The evidence supporting single-use intermittent catheters in people with spinal cord injury. Spinal Cord Ser cases (2020) 6:89. doi: 10.1038/s41394-020-00339-5
40. Avery M, Prieto J, Okamoto I, Cullen S, Clancy B, Moore KN, et al. Reuse of intermittent catheters: A qualitative study of IC users’ perspectives. BMJ Open (2018) 8:e021554. doi: 10.1136/bmjopen-2018-021554
41. Patel DN, Alabastro CG, Anger JT. Prevalence and cost of catheters to manage neurogenic bladder. Curr Bladder Dysfunct Rep (2018) 13:215–23. doi: 10.1007/s11884-018-0483-2
42. Grasdal M, Walter M, Krassioukov AV. The microbiological and physical properties of catheters for intermittent catheterization: A systematic review on the impact of reuse and cleaning. Spinal Cord (2022) 60:581–93. doi: 10.1038/s41393-021-00740-3
43. Gopalakrishnan K, Fabrin Nielsen N, Ramirez AL, Sørensen J, Walter M, Krassioukov AV. Time needed to perform intermittent catheterization in adults with spinal cord injury: A pilot randomized controlled cross-over trial. Continence Reports (2022) 2:100010. doi: 10.1101/2021.08.16.21253936
44. Håkansson MÅ. Reuse versus single-use catheters for intermittent catheterization: What is safe and preferred? Review of current status. Spinal Cord (2014) 52:511–6. doi: 10.1038/sc.2014.79
45. Barken KB, Vaabengaard R. A scoping review on the impact of hydrophilic versus non-hydrophilic intermittent catheters on UTI, QoL, satisfaction, preference, and other outcomes in neurogenic and non-neurogenic patients suffering from urinary retention. BMC Urol (2022) 22(1):153. doi: 10.1186/s12894-022-01102-8
46. Schladen MM, Rounds AK, McManus T, Bennewith A, Claypool H, Groah SL. Intermittent catheter reimbursement in the United States: The experience of nine stakeholders through the lens of actor-network theory. Qual Rep (2021) 26:443–64. doi: 10.46743/2160-3715/2021.4660
47. Berendsen SA, van Doorn T, Blok BFM. Trends in the use and costs of intermittent urinary catheters in the Netherlands from 1997 to 2018: A population-based observational study. Neurourol Urodyn (2021) 40:876–82. doi: 10.1002/nau.24643
48. van Doorn T, Berendsen SA, Scheepe JR, Blok BFM. Single use versus reusable catheters in intermittent catheterisation for treatment of urinary retention: A protocol for a multicentre, prospective, randomised controlled, non-inferiority trial (COMPaRE). BMJ Open (2022) 12:e056649. doi: 10.1136/bmjopen-2021-056649
49. Sun AJ, Comiter CV, Elliott CS. The cost of a catheter: an environmental perspective on single use clean intermittent catheterization. Neurourol Urodyn (2018) 37:2204–8. doi: 10.1002/nau.23562
50. Bermingham SL, Hodgkinson S, Wright S, Hayter E, Spinks J, Pellowe C. Intermittent self catheterisation with hydrophilic, gel reservoir, and non-coated catheters: A systematic review and cost effectiveness analysis. BMJ (2013) 346:e8639. doi: 10.1136/bmj.e8639
51. Del Popolo G, Antonucci L. Disability and sustainability: Reusable versus single-use catheters for persons with neurogenic bladder due to spinal cord injury. Spinal Cord Ser cases (2020) 6(1):90. doi: 10.1038/s41394-020-00340-y
52. Lavelle JP. Intermittent catheters: to reuse or not. Spinal Cord Ser cases (2020) 6:91. doi: 10.1038/s41394-020-00342-w
53. Heard L, Buhrer R. How do we prevent UTI in people who perform intermittent catheterisation? Rehabil Nur (2005) 30:44–5, 61. doi: 10.1002/j.2048-7940.2005.tb00358.x
54. Wilks SA, Morris NS, Thompson R, Prieto JA, Macaulay M, Moore KN, et al. An effective evidence-based cleaning method for the safe reuse of intermittent urinary catheters: In vitro testing. Neurourol Urodyn (2020) 39:907–15. doi: 10.1002/nau.24296
55. Walter M, Krassioukov AV. Single-use versus multi-use catheters: pro single-use catheters. Eur Urol Focus (2020) 6:807–8. doi: 10.1016/j.euf.2019.10.001
56. Christison K, Walter M, Wyndaele JJM, Kennelly M, Kessler TM, Noonan VK, et al. Intermittent catheterization: the devil is in the details. J Neurotrauma (2018) 35:985–9. doi: 10.1089/neu.2017.5413
57. Walter M, Wyndaele M, Keppenne V, Vrijens D, Averbeck MA, Konstantinidis C, et al. Intermittent catheterisation: the devil is still in the details. Continence (2022) 4:100566. doi: 10.1016/j.cont.2022.100566
58. Rognoni C, Tarricone R. Healthcare resource consumption for intermittent urinary catheterisation: Cost-effectiveness of hydrophilic catheters and budget impact analyses. BMJ Open (2017) 7:e012360. doi: 10.1136/bmjopen-2016-012360
59. Welk B, Isaranuwatchai W, Krassioukov A, Husted Torp L, Elterman D. Cost-effectiveness of hydrophilic-coated intermittent catheters compared with uncoated catheters in Canada: A public payer perspective. J Med Econ (2018) 21:639–48. doi: 10.1080/13696998.2018.1443112
60. Elliott CS, Dallas K, Shem K, Crew J. Adoption of single-use clean intermittent catheterization policies does not appear to affect genitourinary outcomes in a large spinal cord injury cohort. J Urol (2022) 208(5):1055–74. doi: 10.1097/JU.0000000000002836
61. Hooton TM, Bradley SF, Cardenas DD, Colgan R, Geerlings SE, Rice JC, et al. Diagnosis, prevention, and treatment of catheter-associated urinary tract infection in adults: 2009 international clinical practice guidelines from the Infectious Diseases Society of America. Clin Infect Dis (2010) 50(5):625–63. doi: 10.1086/650482
62. Buckley B, Archer M, Macaulay M, Fader M. The MultICath study: Creating an evidence base. Br J Nurs (2015) 24:S4–5. doi: 10.12968/bjon.2015.24.Sup18.S4
63. Welk B, Lenherr S, Santiago-Lastra Y, Norman HS, Keiser MG, Elliott CS. Differences in the incidence of urinary tract infections between neurogenic and non-neurogenic bladder dysfunction individuals performing intermittent catheterization. Neurourol Urodyn (2022) 41(4):1002–11. doi: 10.1002/nau.24914
64. Stripple H, Westman R, Holm D. Development and environmental improvements of plastics for hydrophilic catheters in medical care: An environmental evaluation. J Clean Prod (2008) 16(16):1764–76. doi: 10.1016/j.jclepro.2007.12.006
65. Emteva catheter. Available at: https://hunterurology.com/catheters/25-emteva-catheter.html (Accessed 14 September 2022).
66. Elstad EA, Taubenberger SP, Botelho EM, Tennstedt SL. Beyond incontinence: the stigma of other urinary symptoms. J Adv Nurs (2010) 66:2460–70. doi: 10.1111/j.1365-2648.2010.05422.x
Keywords: intermittent catheterization, neurogenic lower urinary tract dysfunction, neurourology, access to health care, patient safety
Citation: Krassioukov A, Welk B, Vrijens D, Islamoska S, Barken KB, Keppenne V, Wyndaele M and Walter M (2023) Intermittent catheterization: A patient-centric approach is key to optimal management of neurogenic lower urinary tract dysfunction. Front. Urol. 3:1158260. doi: 10.3389/fruro.2023.1158260
Received: 03 February 2023; Accepted: 27 February 2023;
Published: 28 March 2023.
Edited by:
Charles Hubscher, University of Louisville, United StatesReviewed by:
David Castro-Diaz, University of La Laguna, SpainCopyright © 2023 Krassioukov, Welk, Vrijens, Islamoska, Barken, Keppenne, Wyndaele and Walter. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrei Krassioukov, a3Jhc3Npb3Vrb3ZAaWNvcmQub3Jn; QW5kcmVpLktyYXNzaW91a292QHZjaC5jYQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.