
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Urol., 03 November 2022
Sec. Endourology
Volume 2 - 2022 | https://doi.org/10.3389/fruro.2022.917195
This article is part of the Research TopicChallenging Dogma: Evolution in Endourological Techniques and ManagementView all 6 articles
 Meera B. Ganesh1†
Meera B. Ganesh1† Matthew S. Lee2*†
Matthew S. Lee2*† Joshua G. Han1
Joshua G. Han1 Mark A. Assmus3Nicholas Dean1Jessica W. Helon1Amy E. Krambeck1
Mark A. Assmus3Nicholas Dean1Jessica W. Helon1Amy E. Krambeck1Introduction: The use of 5-alpha reductase inhibitors (5-ARIs) has been shown to improve lower urinary tract symptoms (LUTS) and decrease prostate size in men with benign prostate hyperplasia (BPH). 5-ARI therapy could increase prostate tissue density through increased collagen deposition and contraction of stromal/epithelial components. Increased tissue density could prolong morcellation times, but the effects of preoperative 5-ARI exposure on morcellation efficiency during Holmium Laser Enucleation of the Prostate (HoLEP) are not well described. Herein, we examine outcomes after HoLEP of patients on pre-operative 5-ARIs.
Methods: A retrospective review of patients undergoing HoLEP by an expert surgeon from Jan – Oct 2021 was performed. Student t-tests and chi-square tests were performed for continuous and categorical variables, respectively. Matched-pair analysis was performed using SPSS v28 (IBM, 2022). A p-value <0.05 was determined statistically significant. All other statistical analyses were performed using SAS v9.4 (SAS, 2019).
Results: A total of 322 patients underwent HoLEP during the study period and 84 patients had pre-operative 5-ARI exposure. Patients in the 5-ARI group had larger preoperative prostate size (p = 0.016). Morcellation time was longer (p=0.01), specimen weight was higher (p=0.02), and morcellation efficiency (p=0.02) was lower in the 5-ARI group. After matching, there were 67 patients in each chort (total 134) and these associations for size, morcellation time, specimen weight, and morcellation efficiency were no longer seen (p=0.8, 0.6, 0.5, and 0.7, respectively). Furthermore, no associations between 5-ARI and post-operative admissions or ED visits were noted.
Conclusion: In this retrospective study, preoperative use of 5-ARIs did not affect enucleation or morcellation efficiency. Thus, preoperative 5-ARI therapy does not appear to alter outcomes after HoLEP.
Benign prostatic hypertrophy (BPH) is one of the most common medical conditions in elderly men. The prevalence of lower urinary tract symptoms (LUTS) attributed to BPH increases as men age. Approximately 50% of men over the age of 50 and up to 80% of men over the age of 80 experience LUTS (1). Medical management of BPH and LUTS includes selective and nonselective alpha-adrenergic antagonists, 5-alpha reductase inhibitors (5-ARIs), phosphodiesterase type 5 inhibitors (PDE5-I), and combination therapy (5-ARIs and alpha-blockers) (2). 5-ARIs inactivate 5 alpha-reductase, an enzyme that converts testosterone into dihydrotestosterone (DHT) (3). DHT is the primary androgen involved in prostatic growth (4). Thus, 5-ARIs reduce prostate volume through induction of prostate atrophy and cell shrinkage (5). In a gerbil prostate model, Finasteride, a selective 5-ARI, increased: fibroblast density in prostatic stroma, secretion of extracellular matrix components, and collagen deposition (6).
Holmium Laser Enucleation of the Prostate (HoLEP) is a size-independent surgical treatment for BPH (7). Indications for BPH surgery include: renal insufficiency, recurrent UTI, bladder stones, recurrent gross hematuria, or symptoms refractory to medical management (2). Thus, some men who undergo HoLEP may have had preoperative 5-ARI exposure if they failed combination therapy. The limited available evidence on perioperative outcomes of 5-ARIs prior to HoLEP suggests there are no effects on blood loss (8), enucleation time or morcellation time (9, 10). We hypothesized that because 5-ARIs reduce prostate volume by ~20% (11) and increase collagen deposition, increased tissue density could result in prolonged morcellation.
To our knowledge, only one study has evaluated morcellation efficiency in patients undergoing HoLEP with prior 5-ARI therapy and found 5-ARIs had no effect on morcellation. However, this study was an abstract and never peer-reviewed (12). Herein, we aimed to evaluate perioperative outcomes of patients undergoing HoLEP with prior 5-ARI therapy. Our primary outcome was to identify if there were any differences in morcellation efficiency due to increased tissue density.
A retrospective review was performed of all patients who underwent HoLEP from January 2021 – October 2021 at our institution. Patients were consented to have their data stored in a prospective REDCap database, which was approved by the Northwestern University Institutional Review Board. Patients were categorized into two categories: those with 5-ARI use prior to HoLEP and those without any 5-ARI therapy (control). 5-ARI therapy was self-reported, but the patient medication list in the medical record was used to confirm 5-ARI exposure. Those with prior non-5-ARI medical therapy were also included in the control group e.g. alpha-blocker therapy. Unfortunately, our database did not contain information on duration of 5-ARI therapy, but since the majority of our patients are referrals for surgical treatment, presumably they had been on maximum medical therapy i.e. chronic 5-ARI therapy and failed. We excluded patients undergoing concurrent procedures during HoLEP. Our technique for HoLEP has previously been published (13) and the Wolf® Piranha™ Morcellator was utilized for morcellation. Morcellation is performed through an extra-long nephroscope. The morcellator is positioned away from the bladder mucosa and above the trigone or in the prostatic fossa. The suction pedal is used to engage enucleated tissue and then the morcellator is activated. We utilize the 3L canister, which requires changing when it is full.
Demographic variables included: age and body mass index (BMI). Preoperative variables included American Society of Anesthesiology (ASA) score, use of anticoagulation therapy (which is routinely held prior to HoLEP after conferring with the prescribing physician), prostate size, PSA level, and history of urinary retention or other prior BPH surgeries. Perioperative characteristics included total procedure time, enucleation time, morcellation time, total energy, and specimen weight. Postoperative characteristics included outpatient status, presence of hematuria 1-week post-procedure (all patients receive a follow-up phone call at 1 week), and 30-day Emergency Department visits. We did not collect patient reported outcomes such as urinary incontinence or voiding symptom scores for this study since the study’s focus was on morcellation efficiency.
The primary outcome was to determine if patients on prior 5-ARI therapy have decreased morcellation efficiency. Enucleation and morcellation efficiency were calculated by dividing the specimen weight by enucleation or morcellation time, respectively (g/min). Chi-square tests were conducted to detect associations for categorical variables and student t-tests were conducted to determine the differences between the two groups for continuous variables. We then performed a matched-pair analysis for size between the two cohorts. After matching, logistic regression was also performed to compare variables that were significantly different on univariate analysis. All tests were two-sided and a p-value of <0.05 was pre-determined to be significant. Statistical analyses were conducted using SAS v9.4 (SAS, 2019). Matching was performed using SPSS v28 (IBM, 2022).
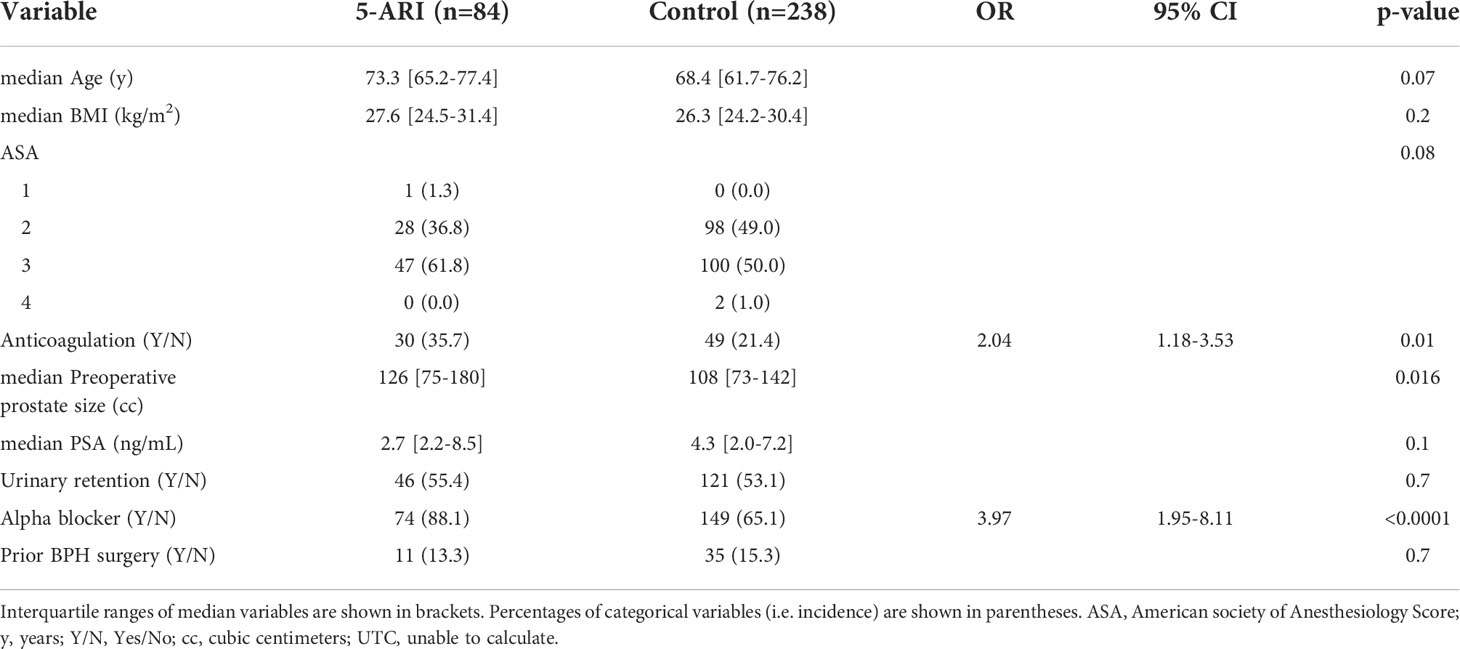
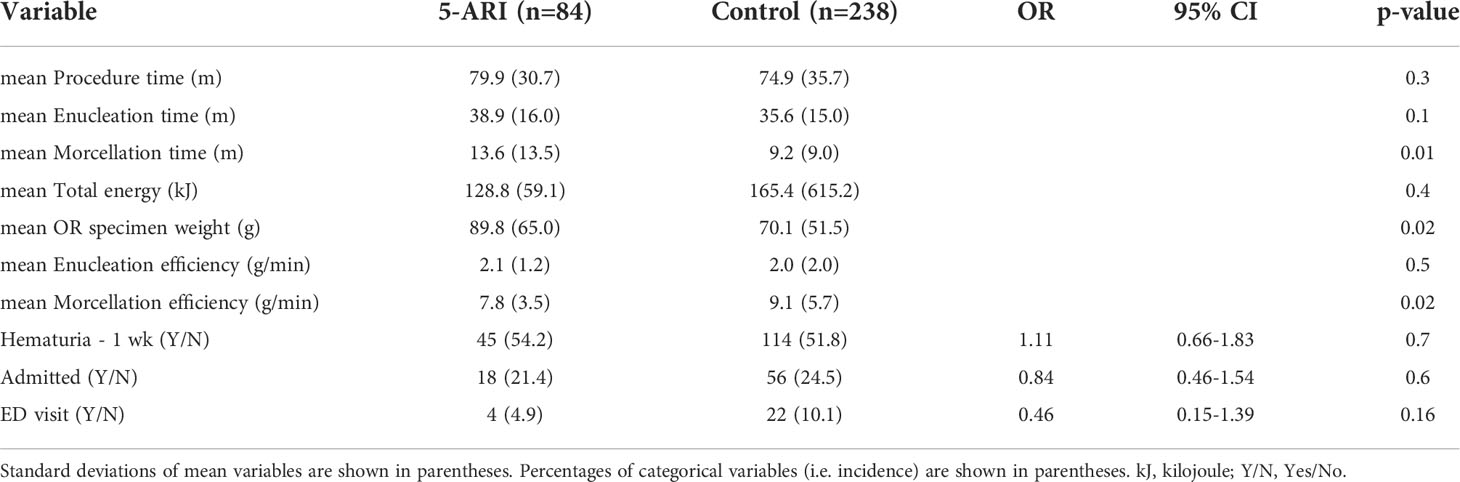
A total of 322 patients underwent HoLEP by one fellowship trained surgeon. There were 84 patients in the 5-ARI group and 238 patients in the control group. There were no significant differences for BMI, history of urinary retention, or history of prior BPH surgery (p=0.2, p=0.7 and p=0.7, respectively. Table 1A). Patients in the 5-ARI group tended to be older (p=0.07) and have a lower preoperative PSA (p=0.1), but these associations were not significant. More patients in the 5-ARI group were on anticoagulation therapy (35.7% vs. 21.4%, p=0.01) and alpha-blocker therapy (88.1 vs. 65.1%, p<0.0001, Table 1). Median preoperative prostate volume was larger in the 5-ARI group (126 vs. 108 cc, p=0.016, Table 1A). There was no significant difference in total mean procedure time (p=0.3, Table 2A). Mean morcellation time was longer in the 5-ARI group (13.6 vs. 9.2 min, p=0.01). Mean OR specimen weight was also significantly higher in the 5-ARI group (89.8 vs. 70.1 g, p=0.02, Table 2A). No difference was seen in enucleation efficiency (p=0.5), but morcellation efficiency was slower (7.8 vs. 9.1 g/min, p=0.02, Table 2A).
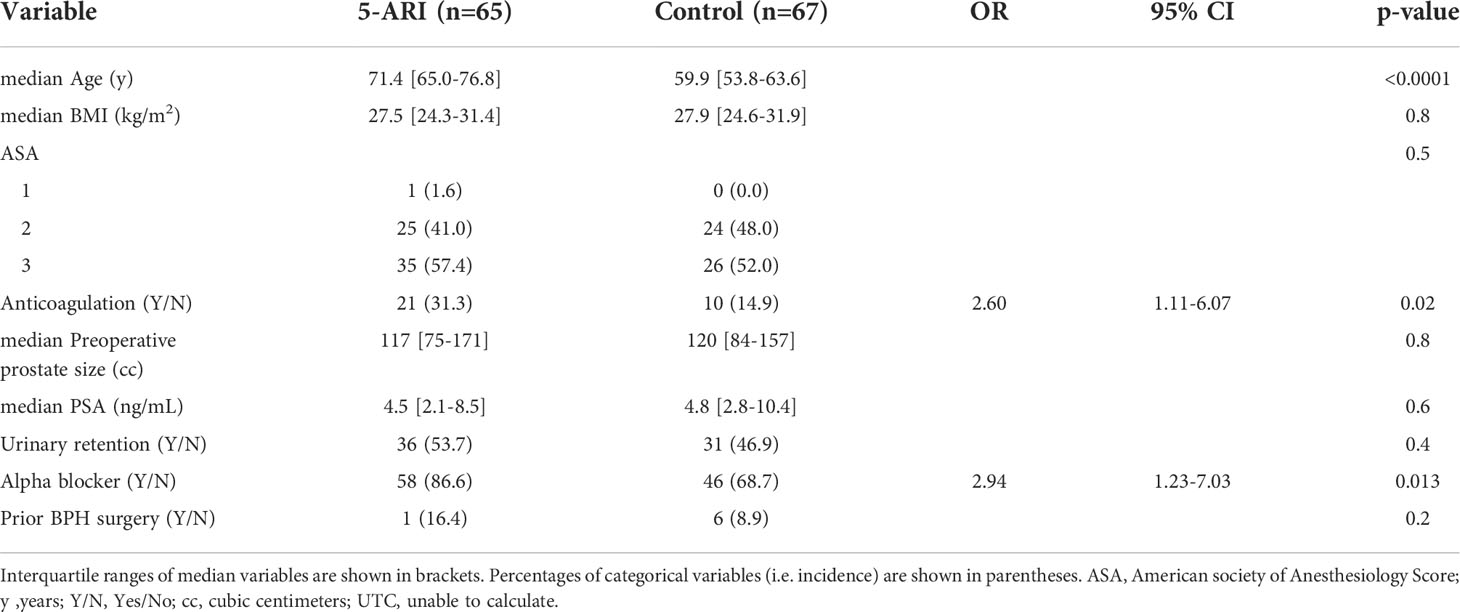
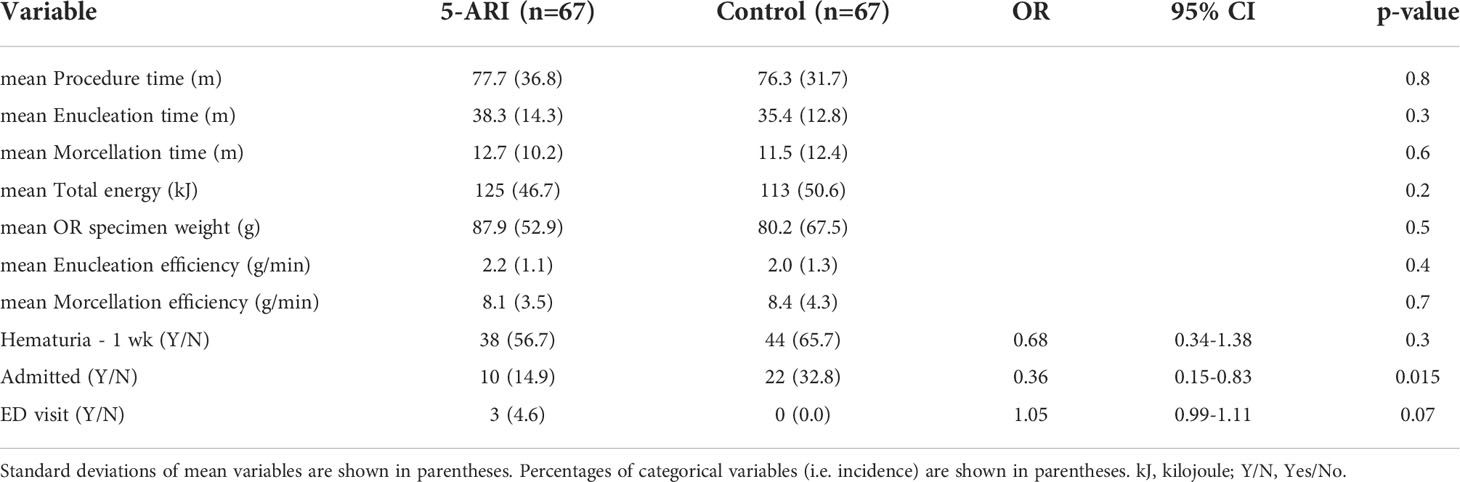
We then performed a matched-pair analysis for prostate size. After matching there was a total of 134 patients (67 in each group). Patients in the 5-ARI group were older (71.4 vs. 59.9 y, p=<0.0001, Table 3B) and more were on anticoagulation (31.3% vs 14.9%, p=0.02) and alpha-blocker therapy (p=0.013). After matching, prostate size was no longer significantly different (117 vs 120 cc, p=0.8, Table 3B). Interestingly, after matching, there were no further differences in morcellation time (p=0.6), OR specimen weight (p=0.5), or morcellation efficiency (p=0.7, Table 2B).
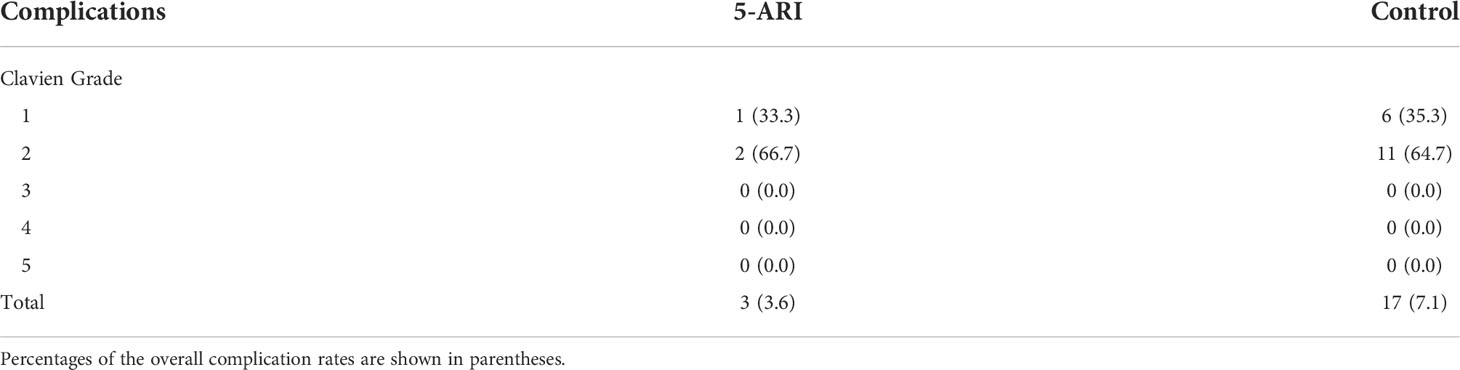
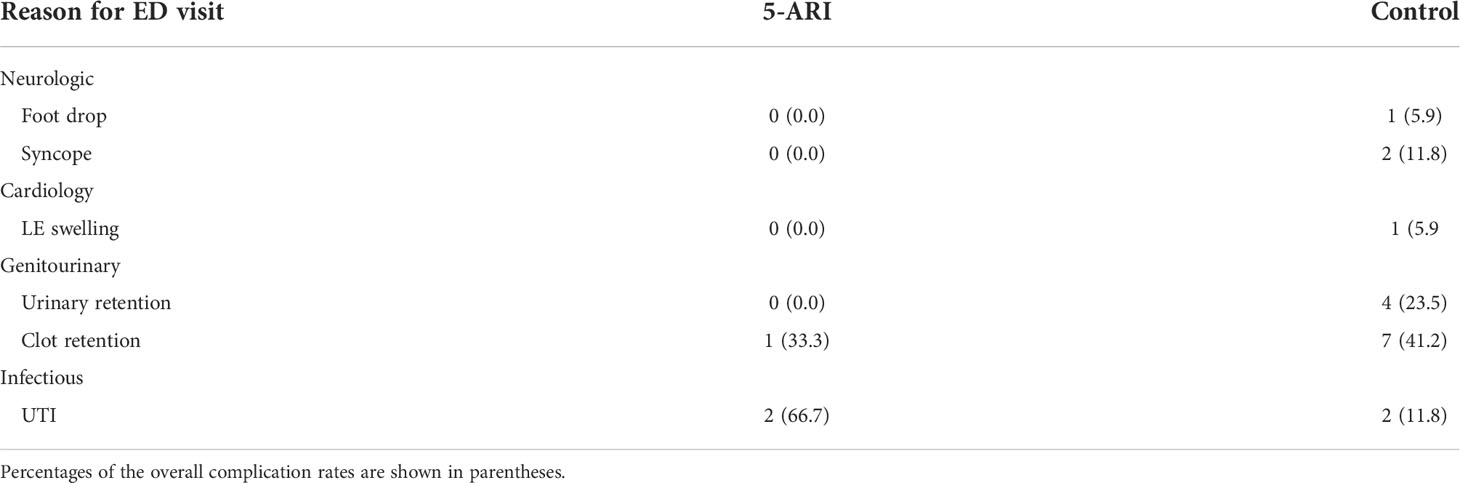
At our institution, we perform same day discharge after HoLEP. After matching, there were more patients who were admitted in the control group (14.9% vs. 32.8%, p=0.015, Table 2B). At the 1-week follow-up, similar rates of patients in both cohorts reported persistent hematuria (56.7% vs 65.7%, p=0.3, Table 2B). On a multivariate logistic regression analyzing associations between age, admission, and 5-ARI use, only age remained significant (p<0.0001, results not shown) and the association for admission was no longer significant (p=0.4, results not shown). Lastly, no significant difference in rates of ED visits were noted before or after matching (Table 2). Complications leading to ED visits were graded by Clavien classification (Table 3A) and are shown in Table 3B. The most common reason for ED visit was UTI for the 5-ARI group and clot retention for the control group.
This study is a contemporary evaluation of morcellation efficiency in patients undergoing HoLEP with preoperative 5-ARI exposure. Prior to matching, morcellation time was longer and specimen weight was higher in the 5-ARI group. Morcellation efficiency was then calculated, and we found that morcellation efficiency was decreased in the 5-ARI group. However, after matching for size, the associations for morcellation time, specimen weight, and morcellation efficiency were no longer significant (p=0.6, p=0.5, and p=0.7, respectively, Table 2B).
Patients in the 5-ARI group were older (p<0.0001, Table 3B). Intuitively, this makes sense as referring urologists may have been trying to maximize medical management for these older patients. The 5-ARI group prior to matching had a larger preoperative prostate size (126 vs. 108 cc, p=0.016). Since 5-ARIs are used to reduce prostate size and are most effective in prostates that are ≥30 g (14) this is not surprising. The fact that prostate size was no longer significant after matching, demonstrated that the process was successful (117 vs 120 cc, p=0.8, Table 3B).
Prior studies have explored whether HoLEP might be more difficult in patients with preoperative 5-ARI treatment. Sato et al. examined whether preoperative dutasteride exposure was associated with increased difficulty in identifying and maintaining the correct surgical plane (9). The authors had three surgeons (blinded to preoperative dutasteride exposure) evaluate surgical videos of 116 patients undergoing HoLEP to grade the level of enucleation difficulty. They found that dutasteride exposure was the only variable associated with increasing enucleation difficulty (9). Interestingly, the authors found that enucleation efficiency was not different between the two groups (0.6 vs 0.6 g/min, p>0.05), which they speculated was due to the experience level of the surgeon who was able to progress through the surgery despite the increased subjective difficulty (9). The authors hypothesized that the increased enucleation difficulty was due to inflammation and adhesions that occur as a result of glandular epithelial atrophy with 5-ARI treatment. In a prospective, double-blinded, placebo-controlled trial of pre-HoLEP dutasteride, Busetto et al. found the surgeon also reported subjective difficulty in finding the enucleation plane and this resulted in the 5-ARI group having a lower enucleation efficiency (1.09 vs. 1.32 g/min, p<0.05). However, in a multi-institutional, retrospective study, Warner et al. compared 176 patients undergoing HoLEP with prior 5-ARI treatment (n=70) against those without (n=106), and found enucleation efficiency was actually faster in the 5-ARI group (0.63 vs 0.81 g/min, p=0.01) (15). We found no difference in enucleation efficiency for the unmatched or matched groups (p=0.5 and 0.4, respectively), which could be due to the experience level of this study’s senior author (who is past the learning curve).
Others have speculated that increased tissue density and collagen deposition in patients on 5-ARIs could result in fibrous and rubbery tissue that is more difficult to morcellate and could prolong morcellation time (10, 12, 15). El Tayeb et al. examined the effect of 5-ARIs on enucleation and morcellation efficiency in a retrospective abstract of 714 patients undergoing HoLEP (5-ARI group, n=222) and found that only prostate size was associated with enucleation and morcellation time on univariate and multivariate analysis. Furthermore, there was no difference in morcellation efficiency between the 5-ARI and control groups on univariate analysis (5.6 vs 5.5 g/min, p=0.8, respectively). However, to our knowledge, this study was never published in a peer-reviewed journal. Warner et al. also reported no difference in the morcellation efficiency for the 5-ARI vs. control groups (4.54 vs. 4.90 g/min, p=0.384, respectively) (15). However, both the El Tayeb and Warner studies did not report which morcellators were utilized. Busetto et al. used the VersaCut™ morcellator and also reported no difference in morcellation efficiency for the 5-ARI group (5.34 vs. 5.65 g/min, p=0.44, respectively) (8).
In our study, we identified that morcellation efficiency was reduced in the unmatched 5-ARI group (7.8 vs. 9.1 g/min, p=0.02) suggesting that increased tissue density could be decreasing the morcellation efficiency. Another consideration was that more bleeding in the 5-ARI group could lead to worse visibility which might prolong morcellation given that there were more patients on anticoagulation in the 5-ARI group (p=0.01). However, we obtain excellent hemostasis before and after morcellation to achieve same-day discharge after HoLEP. Given that HoLEP can be performed for patients on active anticoagulation (14), it is unlikely that poorer visualization in the 5-ARI group contributed to longer morcellation times. Furthermore, all HoLEPs were performed with the Lumenis® Moses™ 2.0 laser, which has also been shown to decrease hemostasis time (16). Indeed, in the matched-pair analysis, neither morcellation time or morcellation efficiency were significantly different. Thus, even though morcellation efficiency takes specimen weight into account, the association seen between 5-ARI use and morcellation efficiency in the unmatched cohort, was likely primarily driven by prostate size. For example, larger prostates might have required more “three-lobe” incisions instead of “two-lobe” incisions, which could have resulted in decreased morcellation efficiency due to time lost in re-targeting the morcellator towards a new lobe or waiting for cannister changes. These are nuances that would be lost in the calculation for morcellation efficiency (specimen weight/morcellation time).
The morcellation efficiency we reported of 7.8-9.1 g/min is faster than the 4.5-5.65 g/min reported by other authors (8, 12, 15). The Piranha™ Morcellator was used in our study, but it is unknown which morcellators were utilized in the other studies. Thus, this difference could be due to differences in morcellators. Indeed, in a recent ex-vivo comparison of several morcellators, we identified the Piranha™ was able to morcellate bull testicle tissue (which was very soft) the fastest, but there were no significant differences when morcellating cooked chicken breast (which was very firm) (17). Furthermore, Elshal et al. noted that the VersaCut™ had a higher rate of “beachball” tissue formation than the Piranha™, which could also account for the slower morcellation efficiency reported by the other studies (18).
Some investigators have also explored if 5-ARIs reduce bleeding risk after HoLEP. Busetto et al. performed microvascular density and VEGF expression analyses in the HoLEP specimens and identified that the 5-ARI group had lower microvascular density and VEGF expression. Interestingly, they found no difference in hemoglobin or hematocrit between the two groups pre and postoperatively. Warner et al. noted a trend towards less hemoglobin drop after HoLEP in the 5-ARI group, but this was not statistically significant (p=0.089) (15). They also noted no difference in postoperative complication rates between the cohorts (15). Although we did not measure postoperative hemoglobin changes, there was no significant difference in the proportion of patients reporting hematuria at 1 week follow up for the unmatched and matched cohorts (p=0.7 and 0.3, respectively). Interestingly, the unmatched cohort had no difference in ability to be discharged the same day (p=0.6), but the matched cohort had more patients in the control group being admitted (14.9 vs. 32.8%, respectively, p=0.015, Table 2B). However, on logistic regression analysis, this association for admission was no longer seen (p=0.4, results not shown) and only age remained a significant association (p<0.0001, results not shown).
Limitations to our study include that it is retrospective and based at a single institution. However, we attempted to adjust for the retrospective nature of the study by performing a matched-pair analysis. As a single institution study, our results may not be applicable to institutions that do not utilize the Piranha™ morcellator or to surgeons who are not past the learning curve (the senior author on this study is past the learning curve of > 50 HoLEPs). Nevertheless, our results add to the current body of literature that suggest there are no differences in morcellation or enucleation efficiency with preoperative 5-ARI therapy. Lastly, patients in the 5-ARI group were self-reported, so we are unable to comment on duration of therapy prior to HoLEP or medication adherence. However, since most patients were referred to our center for surgical management, it is reasonable to assume they had been on prolonged 5-ARI therapy and failed.
In this retrospective study, we demonstrate that preoperative 5-ARI therapy did not decrease morcellation efficiency during HoLEP. This adds to a growing body of literature that suggest that 5-ARI use prior to HoLEP does not result in decreased enucleation or morcellation efficiency or increased complication rates.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Northwestern University Institutional review board. The patients/participants provided their written informed consent to participate in this study.
MG: Conceptualization, validation, investigation, writing: original draft, review & editing, project administration. ML Conceptualization, methodology, validation, formal analysis, investigation, writing: original draft, review & editing, visualization, project administration. JHa - validation, investigation, project administration MA: Supervision, methodology, review & editing, validation, project administration AK: Conceptualization, methodology, validation, formal analysis, investigation, writing: original draft, review & editing, visualization, project administration. ND: validation, writing, review & Editing. JHe: validation, writing, review & editing, project administration. All authors contributed to the article and approved the submitted version.
This work was supported by internal institutional funds.
ML is a consultant for Lumenis. AK is a consultant for Ambu, Boston Scientific, Lumenis, and karl Storz. She is on the data safety monitoring board for Sonomotion and Uropriene
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be constructed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Parsons JK BM, Dahm P, Gahndi MC, Kaplan SA, Kohler TS Lerner LB, Roehrborn CG, et al. Benign prostatic hyperplasia: Surgical management of benign prostatic Hyperplasia/Lower urinary tract symptoms. AUA Guidelines (2019).
2. Kim EH, Larson JA, Andriole GL. Management of benign prostatic hyperplasia. Annu Rev Med (2016) 67:137–51. doi: 10.1146/annurev-med-063014-123902
3. Abreu-Mendes P, Silva J, Cruz F. Pharmacology of the lower urinary tract: update on LUTS treatment. Ther Adv Urol (2020) 12:1756287220922425. doi: 10.1177/1756287220922425
4. Pejčić T, Tosti T, Tešić Ž, Milković B, Dragičević D, Kozomara M, et al. Testosterone and dihydrotestosterone levels in the transition zone correlate with prostate volume. Prostate (2017) 77(10):1082–92. doi: 10.1002/pros.23365
5. Iczkowski KA, Qiu J, Qian J, Somerville MC, Rittmaster RS, Andriole GL, et al. The dual 5-alpha-reductase inhibitor dutasteride induces atrophic changes and decreases relative cancer volume in human prostate. Urol Jan (2005) 65(1):76–82. doi: 10.1016/j.urology.2004.08.042
6. Corradi LS, Goes RM, Carvalho HF, Taboga SR. Inhibition of 5-alpha-reductase activity induces stromal remodeling and smooth muscle de-differentiation in adult gerbil ventral prostate. Differentiation (2004) 72(5):198–208. doi: 10.1111/j.1432-0436.2004.07205004.x
7. Lerner LB, McVary KT, Barry MJ, Bixler BR, Dahm P, Das AR, et al. Management of lower urinary tract symptoms attributed to benign prostatic hyperplasia: AUA GUIDELINE PART II-surgical evaluation and treatment. J Urol (2021) 206(4):818–26. doi: 10.1097/JU.0000000000002184
8. Busetto GM, Del Giudice F, Maggi M, Antonini G, D'Agostino D, Romagnoli D, et al. Surgical blood loss during holmium laser enucleation of the prostate (HoLEP) is not affected by short-term pretreatment with dutasteride: a double-blind placebo-controlled trial on prostate vascularity. Aging (Albany NY). (2020) 12(5):4337–47. doi: 10.18632/aging.102883
9. Sato R, Sadaoka Y, Nishio K, Kobori Y, Yagi H, Arai G, et al. Effects of preoperative dutasteride treatment in holmium laser enucleation of the prostate. Int J Urol (2015) 22(4):385–8. doi: 10.1111/iju.12703
10. Dimopoulos P, Christopoulos P, Kampantais S. A focused review on the effects of preoperative 5alpha-reductase inhibitors treatment in patients undergoing holmium laser enucleation of the prostate: What do we know so far? J Endourol (2018) 32(2):79–83. doi: 10.1089/end.2017.0734
11. Theoret MR, Ning Y-M, Zhang JJ, Justice R, Keegan P, Pazdur R. The risks and benefits of 5α-reductase inhibitors for prostate-cancer prevention. New Engl J Med (2011) 365(2):97–9. doi: 10.1056/NEJMp1106783
12. El Tayeb MM, Bhojani N, Mandeville JA, Boris RS, Rawlings LD, Smoot KJ, et al. Pd26-03 impact of 5-alpha reductase inhibitors on enucleation and morcellation efficiency during holmium laser enucleation of the prostate. J urol (2014) 191(4):e759–9. doi: 10.1016/j.juro.2014.02.2090
13. Agarwal DK, Large T, Tong Y, Stoughton CL, Damler EM, Nottingham CU, et al. Same day discharge is a successful approach for the majority of patients undergoing holmium laser enucleation of the prostate. Eur Urol Focus (2021) 4:228–34. doi: 10.1016/j.euf.2020.12.018
14. Lerner LB MK, Barry MJ, Das AK, Gandhi MC, Kaplan SA, Kohler TS, et al. Management of lower urinary tract symptoms attributed to benign prostatic hyperplasia: AUA guideline part I, initial work-up and medical management. J Urol (2021) 206:806. doi: 10.1097/JU.0000000000002183
15. Warner JN, Nunez RN, Tyson MD, Viprakasit DP, Miller NL, Humphreys MR. A multiinstitutional study of the effects of medical therapy for lower urinary symptoms on the perioperative outcomes of holmium laser enucleation of the prostate. Urology (2011) 78(6):1385–90. doi: 10.1016/j.urology.2011.03.039
16. Kavoussi NL, Nimmagadda N, Robles J, Forbes C, Wang A, Stone B, et al. MOSES(TM) technology for holmium laser enucleation of the prostate: A prospective double-blind randomized controlled trial. J Urol (2021) 206(1):104–8. doi: 10.1097/ju.0000000000001693
17. Lee MS, Assmus M, Cooley LF, Li E, Large T, Krambeck A. Ex vivo comparison of efficiency, safety, and surgeon satisfaction in four commercial morcellators. J Endourol (2021) 514–21. doi: 10.1089/end.2021.0573
Keywords: HoLEP, 5-ARI, morcellation efficiency, morcellation time, enucleation time, Piranha Morcellator
Citation: Ganesh MB, Lee MS, Han JG, Assmus MA, Dean N, Helon JW and Krambeck AE (2022) Effects of 5-alpha reductase inhibitors prior to Holmium Laser Enucleation of the prostate: Does increased adenoma density result in prolonged morcellation times? Front. Urol. 2:917195. doi: 10.3389/fruro.2022.917195
Received: 10 April 2022; Accepted: 18 October 2022;
Published: 03 November 2022.
Edited by:
Saum Ghodoussipour, Rutgers Cancer Institute of New Jersey, Rutgers, The State University of New Jersey, United StatesReviewed by:
Shinsuke Okada, Gyotoku General Hospital, JapanCopyright © 2022 Ganesh, Lee, Han, Assmus, Dean, Helon and Krambeck. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Matthew S. Lee, bWF0dGhldy5sZWVAb3N1bWMuZWR1
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.