
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CURRICULUM, INSTRUCTION, AND PEDAGOGY article
Front. Urol. , 03 June 2022
Sec. Male Urology
Volume 2 - 2022 | https://doi.org/10.3389/fruro.2022.904484
This article is part of the Research Topic Current Perspectives in Urology Education View all 5 articles
 Amelia A. Khoei1
Amelia A. Khoei1 Blair T. Stocks2Jerry Zhuo2Wesley A. Mayer2Michael Coburn2
Blair T. Stocks2Jerry Zhuo2Wesley A. Mayer2Michael Coburn2 Caroline Hubbard2
Caroline Hubbard2 Jennifer M. Taylor2*
Jennifer M. Taylor2*Objective: To offer learning opportunities to medical students during the pandemic and address technical challenges for operating room involvement, the Scott Department of Urology at the Baylor College of Medicine designed and evaluated a 2-week virtual elective course.
Materials and Methods: A manual for a virtual sub-internship was created by members of the Society of Academic Urologists, structured around core competencies. Our curriculum incorporated the manual to design a virtual experience. The course combined live surgical case streaming, one-on-one didactics, and virtual participation during in-person clinic sessions. The surgical streaming was enabled through a nominal investment of $150 for equipment. A post-course evaluation was distributed to participating students.
Results: The course evaluation received a 91% response rate from 11 enrolled fourth-year medical students. There was a very high level of satisfaction with the quality of the educational experience (M=5.8 +/-0.4). Open comments on course strengths highlighted the surgical streaming aspect of the experience, and 80% of evaluation respondents reported that one-on-one time with physicians was a strength of the virtual format.
Conclusions: Our curriculum effectively engaged medical students during a 2-week virtual urology elective. The surgical video streaming format is unique even among virtual rotations nationwide and may be adapted for any learners within or beyond an institution. Our curriculum provides an example for programs to incorporate these inexpensive streaming techniques and for students to gain exposure in their surgical areas of interest.
The current novel coronavirus (COVID-19) pandemic is an unprecedented global crisis which has had significant ramifications upon worldwide economies and healthcare burdens (1). The pandemic has consequently affected education for medical students, residents, and fellows (2–4). In March 2020, both the Association of American Colleges (AAMC) and Liaison Committee of Medical Education (LCME) issued recommendations to limit direct patient care for medical students in clinical learning environments (5). The recommendations were made for the purpose of reducing personal protective equipment usage (PPE) and reducing risk of coronavirus transmission (6). Overnight, students pivoted to alternative learning modalities.
In addition, the LCME discouraged in-person clerkships, and the Accreditation Council for Graduate Medical Education (ACGME) discouraged visiting student rotations (5, 7). This recommendation disrupted many fourth-year medical students’ clinical experience and curricular plans. In many specialties, students rely on the visiting sub-internship as a component of their residency applications (8). For surgical specialties such as Urology, the visiting sub-internship is an important component for both the applicants and the resident program. Visiting sub-internships are a critical opportunity for medical students to learn and demonstrate clinical knowledge and skills, network with institutions throughout the country, and explore their fields of interest. The rotations further generate useful feedback regarding an applicant’s candidacy in the field. The visiting rotation may provide invaluable clinical education and specific access to a subspecialty like Urology (9–12).
In response to the pandemic and travel restrictions, The Society of Academic Urologists (SAU), a national society of chairs and program directors, quickly assembled a taskforce to develop a manual to help institutions implement a virtual sub-internship in Urology (13). Our residency program created a 2-week virtual elective curriculum that utilized Zoom™ to facilitate didactic sessions, simulated patient modules, journal clubs, virtual conferences, virtual participation in live clinic visits, livestreaming of surgical cases, and inpatient census discussion with resident teams.
To our knowledge, a virtual elective with the extensive technical aspects of the Scott Department of Urology at the Baylor College of Medicine’s (BCMSDU) offering has not been previously described. While a few urology programs also executed virtual electives, many experienced technical challenges and limited virtual operating room experiences (14). Our program targeted these challenges and designed a technologically innovative solution for virtual student engagement in the operating room. Our hypothesis was that our virtual urology elective could sufficiently represent the breadth of an in-person urology rotation, showcasing the surgical experience in particular.
Due to the recommendations of professional medical organizations, BCM suspended all in-person clinical rotations in March 2020. Two faculty (WAM and MC) members from BCMSDU worked on the SAU curricular taskforces and helped design the SAU manual with content areas based on the ACGME Core Competencies and Milestones for Urology. Table 1 provides a reference for the intersection between the ACGME Core Competencies and the course components. There were novel opportunities in the virtual format to include more of the core competencies explicitly in the course structure.
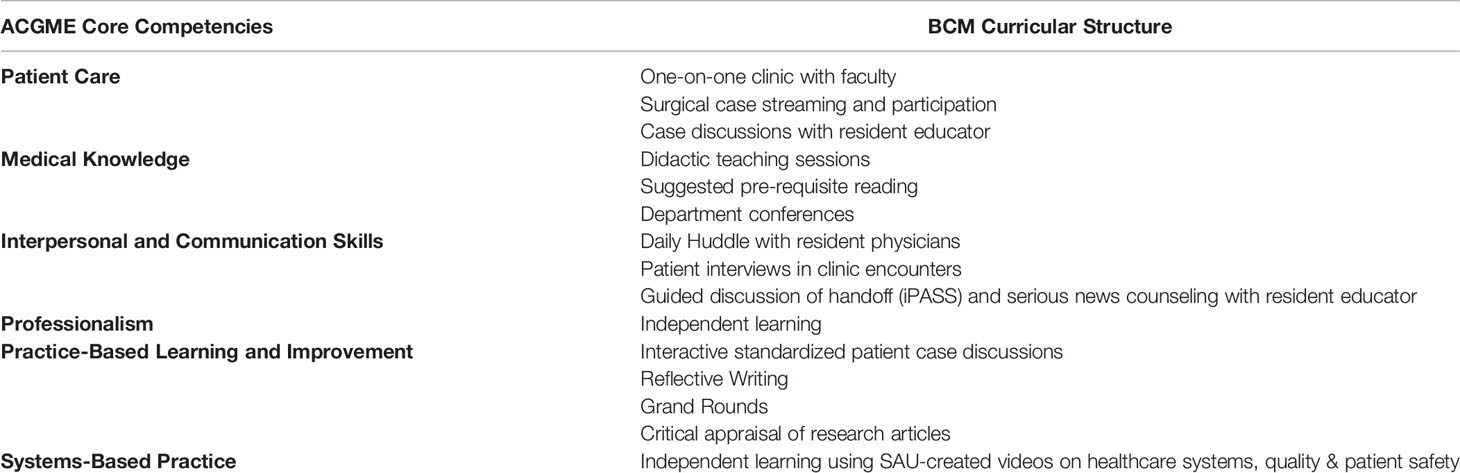
Table 1 Curricular elements which met ACGME core competencies.
The BCMSDU course director (JMT) and program director (WAM) met with key stakeholders within the urology department, at each clinical site, the Office of the Registrar, and the Curriculum Committee to determine necessary steps and components for a Non-Clinical Advanced Elective. Following course approval, we designed specific daily activities considering varying capabilities at each clinical site to integrate students virtually in clinical activities. As the students were registered as visiting students at our institution, their activities were protected under medical education policies. Our institutional license of Zoom, utilized for transmission of clinical activities, is fully compliant with federal HIPAA policies and Texas state privacy laws. Orientation for the students enrolled in the virtual elective included standard required trainings, including privacy modules, for visiting students at our institution. Multiple residents and faculty members within the department committed to scheduled didactic sessions during each 2-week rotation. The reduced clinical activity and volume due to pandemic restrictions allowed for greater educator availability, and residents fulfilled alternative educational plans by participating in the course design and implementation. At least one clinical site acquired new equipment to implement the virtual format at a relatively nominal cost of $150 USD.
The course availability was advertised through multiple channels including the SAU website, the BCMSDU website, our Twitter account, and a website created by current fourth-year students applying into Urology (uroresidency.com). Students applied via the Visiting Student Application System (VSAS) to the 2-week virtual elective in Urology. Accepted Virtual Away Students (VASs) participated in scheduled content from Monday to Friday over the 2-week experience. VASs spent one dedicated week at one of our public hospital practice sites and one dedicated week at one of our private hospital practice sites. Public practice sites included the Michael E. DeBakey Veterans Administration Medical Center (MEDVAMC) and Ben Taub Hospital (BTH). The private practice sites included Baylor St. Luke’s Medical Center (BSLMC) and Texas Children’s’ Hospital (TCH).
This weekly structure mirrored previous years’ in-person visiting sub-internship with exposure and experience spanning across our many residency training sites. The proportion of time at each site was determined by logistics of virtual connectivity and clinical volume, with some sites experiencing reductions in clinic and case volume due to the pandemic surge. All students were enrolled as visiting students at BCM, and most students received course credit via their home institutions. Prerequisite resources needed by learners included a personal computer with audio/video conferencing capabilities, installation of Zoom™ Video Communications software (San Jose, California), and a dedicated high-speed internet connection. Facilitators included BCMSDU faculty and residents with access to similar technology.
The learning objectives were approved with assessment measures as follows:
1) Objective: Student will demonstrate knowledge of common conditions in Urology and their management.
Assessment Method: Didactics; Student Assessment Form.
2) Objective: Student will describe indications, anatomy, basic technical steps, and potential complications for common urological surgeries.
Assessment Method: Didactics, Surgical case review; Student Assessment Form.
3) Objective: Student will locate, appraise, and assimilate evidence from scientific studies related to patients’ urologic problems.
Assessment Method: Reflective Writing Assessment Tool.
Each morning, VASs logged into secure Zoom™ video meetings and proceeded to interact with faculty and residents throughout the day. After a one-hour orientation session at the start of the two-week rotation, typical sessions included the following:
1) Surgical Case streaming: Real-time participation in surgical cases.
As described in detail in the next section, VASs interacted with faculty and residents via live audio/video feeds of ongoing urologic surgeries.
2) Clinic Encounters: Dedicated one-on-one clinic time with faculty.
In these sessions, faculty members would include VASs in live clinic encounters via audio/video conference enabled laptops. The VAS was allowed to interview the patient individually and then present to the attending physician and accompany the attending physician for further discussion, or the student was connected live while the attending interviewed and examined the patient.
3) Didactic teaching sessions with department educators: Small-group didactic sessions scheduled with BCMSDU faculty, chief resident, or fellow on a variety of topics, including guidelines and clinical management of common conditions.
4) Interactive case discussions: Small-group standardized patient scenarios moderated by residents.
Cases were adapted from the SAU Virtual Sub-Internship manual and included the evaluation and surgical management of patients presenting with conditions such as testicular torsion, male factor infertility, gross hematuria, and metabolic stone disease.
5) Critical Appraisal of Literature: Small group journal clubs with residents and faculty.
VASs presented and critically evaluated peer-reviewed journal articles focusing on clinical topics.
6) Daily huddle with residents: Each VAS would have time at the end of the clinical day with residents at one site to discuss the inpatient census, consults, and cases. This also provided time to ask questions informally.
7) Independent learning: Scheduled blocks in which the VASs could prepare for the above sessions as well review assigned online content, including quality improvement, patient safety, interprofessional communication, and the business of medicine. This online content was adapted from the SAU Virtual Sub-Internship manual.
8) Reflective writing: Each VAS was given an assignment and the writing was reviewed with a faculty member in an individual virtual session.
9) Department conferences: Participation in weekly Grand Rounds, Resident Educational Conference, Preoperative Case Conference, and/or site-specific Tumor Board.
ACGME Core Competencies are also referenced in the short course description: “This course will engage the student in observation and participation in clinical scenarios specific to Urologic practice, with a distribution of experiences across ACGME core competencies (in parentheses). Through this 2-week rotation, the student will participate in virtual experiences to include: group didactics with an attending physician (Medical Knowledge), critical appraisal of sentinel literature (Evidence-Based Medicine), facilitated case discussion with residents (Medical Knowledge, Practice-Based Learning), self-directed learning through reading and video assignments (Practice-Based Learning), surgical case review and discussion (Patient Care and Procedural Skills), and self-reflection (Professionalism, Practice-Based Learning)” (Table 1).
At the conclusion of the two-week course, VASs attended a wrap-up session with the course director and residency program director. VASs were also invited to participate in an open forum with BCMSDU residents pertaining to resident life, living in Houston, the interview process, or any topic of their choosing.
Feedback was formative and provided face-to-face by the attending physician. Each student had a performance assessment form completed by the Course Director, based on compiling feedback from the faculty and resident educators, that was submitted to their home institution. All students were graded Pass/Fail given the Non-Clinical structure of the course.
Critical to the success of the BCMSDU Virtual Elective Student Rotation was the integration of live video and audio streams from within our surgical suites. Streamed surgical cases included robotic, laparoscopic, percutaneous, endoscopic, and microsurgical cases.
For the MEDVAMC rotation, faculty and residents worked closely with onsite system engineers from Karl Storz Endoscopy-America, Inc (El Segundo, California) to leverage the Karl Storz StreamConnect software platform, which already provided internal streaming of video input from several operating rooms. As a result, we were able to stream live video and audio content from the DaVinci Si/Xi Surgical System (Intuitive, Sunnyvale, California) or the endoscopic suite to secure Zoom™ Video meetings attended by VASs.
At BSLMC, we partnered with surgical and IT staff to stream live video and audio from operating rooms not equipped with this integrated software. Specifically, we created a mobile and cost-effective solution for other surgical programs and/or subspecialities wishing to creative a virtual operating room experience. Both the Intuitive DaVinci Surgical System and Karl Storz Endoscopic surgical platforms transmit high-definition video via uncompressed Digital Visual Interface (DVI) connections. Accordingly, we utilized an available “DVI Video Out” connection on these platforms to capture live robotic or endoscopic video feeds. For our needs, we purchased a 10-foot long male DVI to male High-Definition Multimedia Interface (HMDI) cable (~$10 - Figure 1A). However, as most personal computers do not have a graphics card with dedicated video input, an external video capture card was required. We utilized a female HDMI to male USB HMDI Video Capture Card (~$20 – Figure 1B). Ultimately, the set up was as follows: Female DVI-OUT (as found on the robotic console or endoscopic tower) to our male DVI/male HDMI cable, to our female HDMI/male USB video capture card, to a personal laptop or desktop computer in the operating room, which was logged into Zoom™ with a high-speed internet connection. Once connected, facilitators were able select “USB Camera” as a video input source that the Zoom™ Software streamed to VASs in high definition. Students were able to communicate with the surgical team through a two-way audio-video stream. In some cases, the attending physician wore a Bluetooth-enabled headset to allow discussion that was less intrusive to the case.

Figure 1 Video Equipment used for Virtual Away Student Live OR Streaming Experience. (A) Male DVI to Male HDMI cable ($~10 – preferably 10 feet or longer). (B) Female HDMI to Male USB external video capture card (~$20). (C) Smartphone gooseneck stand (~$20). (D) Bluetooth enabled noise-reducing audio conferencing speakerphone (~$90).
To augment the live operating room experience to show both the video image and the operating room interior perspective, we installed “gooseneck” smartphone stands (~$20 - Figure 1C) within the operating room to provide a bird’s eye view of the operating surgeons and patients. A facilitator placed a Zoom™ -enabled smartphone in the stand with camera pointed over the operating table. Additionally, we paired a Bluetooth enabled audio-conferencing speakerphone with noise-reducing technology (~$90 – Figure 1D) to the smartphone in order to dampen OR cacophony, which provided surgeons and VASs clear communication.
At the conclusion of the virtual elective, our program requested students to complete a course evaluation in a deidentified fashion. The electronic questionnaires were designed in SurveyHero (Zurich, Switzerland) to evaluate satisfaction with the course, effectiveness of faculty and resident teaching in the virtual format, satisfaction with learning opportunities, and success in achieving learning objectives. The evaluation also solicited qualitative feedback. Outcomes were measured on a 6-point Likert scale (1=strongly disagree, 6=strongly agree).
Our curriculum was implemented as a virtual elective for 11 virtual fourth-year medical students. We hosted a total of 5 rotation blocks, which ran consecutively from August 3, 2020, to October 9, 2020. Participants were 36% female and attended medical schools from the following geographic regions: Mid-Atlantic, Southeast, Southwest, Midwest, and West. Evaluation responses were collected from 10 of the 11 participants using the electronic questionnaire via SurveyHero.
In the course evaluation (Table 2), students reported a high level of satisfaction with the quality of the educational experience provided by the virtual elective (M=5.8 out of 6, SD=0.4). Students felt the elective was well organized (M=6, SD=0.0). With regards to learning, students felt that the elective provided sufficient opportunities to meet the stated knowledge objectives (M=5.7, SD=0.45), attending physicians provided effective teaching during the rotation (M=5.7, SD=0.64), and residents and fellows provided effective teaching during the rotation (M=5.9, SD=0.3).

Table 2 Course evaluation components and results.
The majority of respondents (80%) reported that a major strength of the virtual format was one-on-one time with residents and attendings. Within the comments, students highlighted that they experienced more meaningful and dedicated discussions with faculty through the scheduled virtual format than they would have experienced in-person. One student noted, “I felt the biggest strength of this elective was having one-on-one sessions with faculty and residents. This allowed for an uninterrupted learning experience that was valuable in learning more about urology and the program in general. I was able to ask any questions I wanted in a non-hostile setting.” Another student noted, “This is dedicated time that likely would not be possible in an in-person away rotation, and this is what made the rotation so special.”
Many students (40%) also noted the virtual urology clinic component as a strength, as they were able to follow patients through the electronic medical record, complete a history and physical exam, and present an assessment and plan to their attending physician. A couple of students also noted as a strength that our institution was equipped with streaming and recording equipment prior to the start of the pandemic. One student noted, “I loved having time in the operating room, [especially] streaming in the operating room when headphones were attached to the attending physician.” Other strengths noted include the research/journal club assignments (40%) and faculty mentorship (100%).
When asked about potential improvements to the virtual rotation, two respondents (20%) noted that differences in time-zones made evening sign-out difficult to attend. One respondent noted a desire for more educational information on in-patient hospital management of urology patients. This student recommended the option of following a hospital patient via electronic medical record with virtual discussion of the patient’s hospital course with the team. Other recommendations include purchasing headsets with longer battery life for operation streams, including more institution-specific educational videos, and more scheduled time at the affiliated county hospital, BTH.
Our curriculum was successful in providing a virtual format for a 2-week rotation in urology. Students were highly satisfied with the rotation. Strengths of the program included video streaming capabilities in the operating room, dedicated time in the urology clinic with attending physicians, one-on-one time with residents and faculty, and journal club assignments. Given the positive evaluation feedback, we believe that our curricular structure in a virtual format can be adapted to multiple institutions and specialties.
A major goal of our rotation included addressing the challenge of student integration into operating room experiences while in a virtual format. While other virtual urology rotations existed, a unique strength of our institution’s adaptation was inexpensive video streaming capabilities. Prior examples of virtual rotations in surgical subspecialties have been shorter (15, 16) or do not incorporate virtual operating room experiences (14). For the cost of roughly $150, our partnering institutions became equipped to integrate our virtual students directly into the operating room.
Although this rotation was designed for off-site away-rotation students, the procedural video streaming format is largely unique and may be further adapted for any interested learners in any setting. In addition, the standardized virtual one-on-one didactic sessions allowed residents and faculty to measure and comparatively evaluate students’ knowledge and participation. This presents an opportunity for virtual surgical rotations to continue even after the COVID-19 pandemic subsides, as the option may offer more personal and dedicated time with faculty than an in-person rotation. In addition, the virtual rotation can create availability for students who were not selected for in-person rotations.
Benefits of this virtual rotation included efficiency for students to be involved with patients and faculty at multiple hospital sites in the span of a single day and reduced cost for students participating in away-rotations. The urology match cost a median of $9,725 for applicants in 2020 (17). The mean estimated cost to participate in an in-person away rotation prior to the COVID-19 pandemic was $958 per rotation (18). In comparison, the cost for students who participated in our rotation only included the Visiting Student Application Service (VSAS) application fee, which is $15 per application. The virtual option will further allow programs to market their strengths and weaknesses for interested students who may not have direct access. Many leaders in medical education note the cost of traveling for in-person rotations bring potential disparities in opportunities for students to light (18). Providing a meaningful and educational experience in a virtual format may create opportunities for students from a spectrum of geographic and socioeconomic backgrounds.
There is an additional concern over the loss of in-person exposure to a student translating to a decreased ability to evaluate a student’s performance. A clear disadvantage of the virtual rotation is the inability to assess a student’s collaborative efforts on the inpatient team or perform a direct observation of the student’s skills with patient examination or surgical techniques. However, standardizing the virtual curriculum ensured a consistency to the rotation and provided more objective experiences by which to evaluate students comparatively. The virtual format presented opportunities to develop content in core competencies, such as Interpersonal and Communication Skills, Problem Based Learning, and Improvement. It is notable that one of the students who participated in the virtual elective matched to our program for residency, signaling an experience that gave the student familiarity with the program and its strengths.
A limitation of this report is the lack of pre- versus post-measures assessing the impact on participants’ subjective knowledge, attitudes, and/or behavior changes. Future iterations of this rotation may include pre- and post-session evaluations to assess participants’ planned behaviors. In addition, while our program explored the novel technological facets of a virtual operating room, and this contributed to overall user satisfaction scores, the evaluation design did not specifically track technological satisfaction. These results may not be generalizable to all medical schools or hospital sites in the US as this iteration included 11 students rotating at several clinical sites at a single institution.
In terms of future directions, the video-based teaching strategies may be applied for in-person students participating at various clinic sites with the addition of active narration. In addition, the unique one-on-one didactic sessions may be further adapted for in-person and on-site medical students; we utilized the format already this year for synchronous learning activities with several students at various clinical sites. Furthermore, this virtual curriculum lends to more standardized learning opportunities for all participating students.
Our curriculum is effective and feasible for integrating medical students virtually into a surgical visiting elective rotation. Our curriculum offers other medical institutions and specialties a model for operating room integration, didactic education, and medical student mentoring in a virtual format. We hope that our promising results inspire education leadership to incorporate technological equipment to design future successful virtual electives in surgical specialties.
The virtual program was made possible by significant time investments from BCMSDU residency program faculty and trainees during COVID-19 restrictions, and the resource of time may be difficult to secure in traditional, non-restricted schedules. When considering a virtual rotation in subsequent years, it was challenging to reproduce the availability of the teaching faculty and teaching residents; the unique context of the pandemic created additional time for teaching, which was not as easily secured in the standard non-pandemic context.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical review and approval was not required for the study on human participants, in accordance with the local legislation and institutional requirements.
Study conception and design, JT, WM, MC, CH, BS, and JZ. Acquisition of data, AK, JT, and WM. Analysis and interpretation of data, AK, JT, and WM. Drafting of manuscript, AK, JT, WM, MC, CH, BS, and JZ. Critical revision, AK, JT, WM, MC, CH, BS, and JZ. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We acknowledge the contributions of other valued members of the intervention implementation teams, including the case discussion resident educator leaders and faculty volunteers. Our team also formally acknowledges the SAU taskforce for creating the manual, and Lee Richstone, MD who chaired the effort nationally.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fruro.2022.904484/full#supplementary-material
1. Sohrabi C, Alsafi Z, O'Neill N, Khan M, Kerwan A, Al-Jabir A. World Health Organization Declares Global Emergency: A Review of the 2019 Novel Coronavirus (COVID-19). Int J Surg (2020) 76:71–6. doi: 10.1016/j.ijsu.2020.02.034
2. Rose S. Medical Student Education in the Time of COVID-19. JAMA (2020) 323(21):2131. doi: 10.1001/jama.2020.5227
3. Akers A, Blough C, Iyer MS. COVID-19 Implications on Clinical Clerkships and the Residency Application Process for Medical Students. Cureus (2020) 12(4):525e–57e. doi: 10.7759/cureus.7800
4. Donohue JM, Miller E. COVID-19 and School Closures. JAMA (2020) 324(9):845. doi: 10.1001/jama.2020.13092
5. Barzansky B, Catanese VM. LCME Update on Medical Students, Patients, and COVID-19: Approaches to the Clinical Curriculum (2020). Available at: https://lcme.org/wp-content/uploads/filebase/March-20-2020-LCME-Approaches-to-Clinical-Curriculum.pdf (Accessed May 23, 2021).
6. Whelan A, Prescott J, Young G, Catanese VM, McKinney R. Guidance on Medical Students’ Participation in Direct In-Person Patient Contact Activities (2020). Available at: https://www.aamc.org/system/files/2020-08/meded-August-14-Guidance-on-Medical-Students-on-Clinical-Rotations.pdf.
7. The Coalition for Physician Accountability’s Work Group on Medical Students in the Class of 2021 Moving Across Institutions for Post Graduate Training. Final Report and Recommendations for Medical Education Institutions of LCME-Accredited, U.S. Osteopathic, and Non-U.S. Medical School Applicants. Available at: https://www.aamc.org/system/files/2020-05/covid19_Final_Recommendations_Executive%20Summary_Final_05112020.pdf (Accessed May 23, 2021).
8. Nikonow TN, Lyon TD, Jackman SV, Averch TD. Survey of Applicant Experience and Cost in the Urology Match: Opportunities for Reform. J Urol (2015) 194(4):1063–7. doi: 10.1016/j.juro.2015.04.074
9. Viers BR. COVID-19 Adjustments Impact Urology Residency Training, in: Mayo Clinic (2020). Available at: https://www.mayoclinic.org/medical-professionals/urology/news/covid-19-adjustments-impact-urology-residency-training/mqc-20504203 (Accessed May 23, 2021).
10. Theoret C, Ming X. Our Education, Our Concerns: The Impact on Medical Student Education of COVID-19. Med Educ (2020) 54(7):591–2. doi: 10.1111/medu.14181
11. Williams C, Familusi OO, Ziemba J, Lee D, Mittal S, Mucksavage P. Adapting to the Educational Challenges of a Pandemic: Development of a Novel Virtual Urology Subinternship During the Time of COVID-19. Urology (2021) 148:70–6. doi: 10.1016/j.urology.2020.08.071
12. Kenigsberg AP, Khouri RK, Kuprasertkul A, Wong D, Ganesan V, Lemack GE. Urology Residency Applications in the COVID-19 Era. Urology (2020) 143:55–61. doi: 10.1016/j.urology.2020.05.072
13. Mikhail D, Margolin EJ, Sfakianos J, Clifton M, Sorensen M, Thavaseelan S. Changing the Status Quo: Developing a Virtual Sub-Internship in the Era of COVID-19. J Surg Educ (2021) 78(5):1544–55. doi: 10.1016/j.jsurg.2021.03.007
14. Margolin EJ, Gordon RJ, Anderson CB, Badalato GM. Reimagining the Away Rotation: A 4-Week Virtual Subinternship in Urology. J Surg Educ (2021) 78(5):1563–73. doi: 10.1016/j.jsurg.2021.01.008
15. Farlow JL, Marchiano EJ, Fischer IP, Moyer JS, Thorne MC, Bohm LA. Addressing the Impact of COVID-19 on the Residency Application Process Through a Virtual Subinternship. Otolaryngol Head Neck Surg (2020) 163(5):926–8. doi: 10.1177/0194599820934775
16. Dean RA, Reghunathan M, Hauch A, Reid CM, Gosman AA, Lance SH. Establishing a Virtual Curriculum for Surgical Subinternships. Plast Reconstr Surg (2020) 146(4):525e–57e. doi: 10.1097/prs.0000000000007267
17. Tabakin AL, Srivastava A, Polotti CF, Gupta NK. The Financial Burden of Applying to Urology Residency in 2020. Urology (2021) 154:62–7. doi: 10.1016/j.urology.2021.01.013
Keywords: urology, medical students, COVID-19, undergraduate medical education (UME), distance education
Citation: Khoei AA, Stocks BT, Zhuo J, Mayer WA, Coburn M, Hubbard C and Taylor JM (2022) Design and Evaluation of a Virtual Urology Sub-Internship During the COVID-19 Pandemic. Front. Urol. 2:904484. doi: 10.3389/fruro.2022.904484
Received: 25 March 2022; Accepted: 10 May 2022;
Published: 03 June 2022.
Edited by:
Christopher Jaeger, Boston Children’s Hospital and Harvard Medical School, United StatesReviewed by:
Tomokazu Kimura, University of Tsukuba Hospital, JapanCopyright © 2022 Khoei, Stocks, Zhuo, Mayer, Coburn, Hubbard and Taylor. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jennifer M. Taylor, amVubmlmZXIudGF5bG9yQGJjbS5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.