 Ramona Nicolau-Raducu
Ramona Nicolau-Raducu Gaetano Ciancio
Gaetano Ciancio Yehuda Raveh
Yehuda Raveh
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Transplant. , 25 June 2024
Sec. Abdominal Transplantation
Volume 3 - 2024 | https://doi.org/10.3389/frtra.2024.1412391
Background: Kidney transplantation is the therapy of choice for end-stage kidney disease, and a fast-growing transplant procedure worldwide. Diverse clinical practices for recipients and donors' selection and management between transplant centers hinder the creation and dissemination of an anesthesia-surgical checklist.
Methods: Components of the anesthesia-surgical checklist were selected after a review of the English literature using PubMed search for donor, recipient and graft protocols and outcomes of existing practices in the field of kidney transplantation. Key elements of the most relevant articles were combined with our own center's experience and formulated into the proposed checklist. The checklist is intended to be used perioperatively, once patient receives an offer.
Results: The perioperative checklist centers primarily on the following donor and recipient's factors: (i) Review of the pretransplant candidate workup; (ii) Assessment of donor/graft status; (iii) Hypothermic machine perfusion parameters; (iv) Operating room management; (v) Sign out. The proposed kidney transplant checklist was designed to ensure consistency and completeness of diverse tasks and facilitates team communication and coordination.
Conclusion: We present a novel standardized combined anesthesia-surgical checklist framework for kidney transplant aimed at increasing perioperative safety and streamline the perioperative care of recipients. Future validation studies will determine its clinical feasibility and post-implementation efficacy.
Kidney transplantation (KT) is the therapy of choice for patients with end-stage kidney disease, and a fast-growing transplant procedure worldwide. The World Health Organization launched The World Alliance for Patient Safety in 2004, and in 2008 the second Global Patient Safety Challenge was formulated and aims to improve surgical safety. The compilation of a procedure checklist for use in the operating room is one of the four tenets of the initiative (1). Proven benefits of surgical checklists include enhanced team communication, procedural consistency, and ultimately significant reduction in related medical errors and surgical complications (2). Within the scope of urology checklists were successfully implemented in transurethral resection of a bladder tumor, robotic nephrectomy, and radical nephrectomy with tumor thrombectomy (3–5).
To expand the ever-limited donors pool, high-volume transplant centers are generally more inclined to consider expanded criteria donors who are older (≥75 years), hypertensive, or stroke-stricken (6). However, the increased comorbidities of aging donors or donation after circulatory death are associated with poorer graft and recipient's outcomes (7, 8). Perioperative fluid and hemodynamic management determine renal allograft function and, consequently, perioperative adverse cardiac events of recipients (9). As such, it is increasingly important to optimize modifiable risk-factors and improve short- and long-term outcomes in KT recipients. In addition to the surgical technique itself, optimal outcomes of KT also require careful matching of the donor and recipient, adequate machine perfusion of graft, immunosuppression, and a set of perioperative hemodynamic and fluid goals. Notwithstanding its complexity, a universal checklist for KT is strikingly lacking. Presumably, diverse clinical practices for recipients and donors’ selection and management between transplant centers hinder the creation and dissemination of such a checklist.
This study aims to fill this gap. We propose a combined anesthetic-surgical perioperative checklist framework aiming at improving the perioperative care of patients undergoing KT.
Components of the anesthesia-surgical checklist were selected after a review of the English literature using PubMed search for donor, recipient and graft protocols and outcomes of existing practices in the field of KT. Key elements of most relevant articles were combined with our own center's experience and formulated into the proposed checklist, see Table 1. The KT checklist is intended to be used perioperatively once the patient receives an offer.
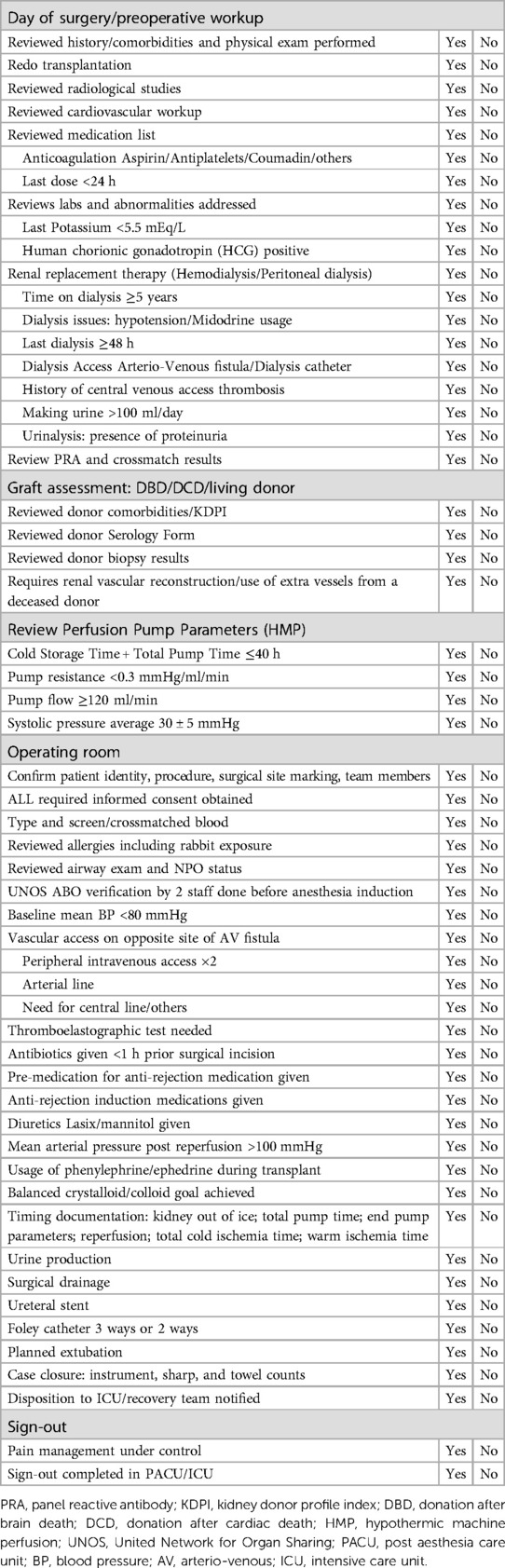
Table 1 Checklist for the performance of kidney transplantation.
The perioperative checklist centers primarily on the following donor and recipient's factors:
(i) Review of the pretransplant candidate workup
(ii) Assessment of donor/graft status
(iii) Hypothermic machine perfusion parameters
(iv) Operating room management
(v) Sign out
(i) Review of the workup of the recipient
A thorough review of recipient's history, medication, physical examination, recent laboratory radiological results is mandatory. Issues which may preclude transplantation should be sought after and addressed.
Patients with a cardiovascular or respiratory disease, limited functional status, or prior hospitalization should be identified, and attainment of patient's optimal medical status prior to KT should be ascertained. Cardiovascular complications continue to be the leading cause of mortality after KT. While KT is categorized as an intermediate risk surgery by the American College of Cardiology and the American Heart Association, is associated with a 1.1% perioperative cardiovascular mortality, compared to 0.7% mortality reported after major abdominal surgery (10). Preoperative referral for cardiology consultation should be guided by cardiac risk assessment of the KT candidate (11).
The recently updated Kidney Disease: Improving Global Outcomes guidelines (12) recommended the referral of potential kidney transplant candidates for evaluation at least 6–12 months before anticipated dialysis initiation in order to facilitate the identification and workup of living donors and to plan for possible pre-emptive transplantation. The reason is that the time spent on dialysis before transplantation appears to have a directly proportional negative effect on patient and/or graft survival (13). Symptomatic hypotension is a common complication in patients with end-stage renal disease (14). Midodrine users were more likely to have a longer duration of dialysis dependence, and higher levels of sensitization compared to non-users (15). In addition, they are at increased risks of developing delayed graft function (DGF), graft failure and death in the 1st year post transplant (15). Details regarding dialysis access, when last dialysis was done, amount of urine making are important in regard of intraoperative venous/arterial access, potassium level and the size of the bladder, respectively. Occurrence of proteinuria, (≥0.5 g/day), first post-transplant year, is significantly linked to graft/patient survival and usage of older donors (≥60 years), which appear more sensitive to proteinuric injuries (16). The first consideration in evaluating post-transplant proteinuria is whether it originates from the native kidneys or may be due to various allograft pathologies, and/or may be a side effect of immunosuppressive medications (17). Patients not on dialysis before transplantation may have proteinuria due to their native kidney disease (17).
Human leukocyte antigens (HLAs) are the primary determinants of alloimmunity (18). A crossmatch test is a test that determines the immunologic risk and can be done by mixing patient serum and donor cell (logistically challenging) or virtually, which is analyzing the results of 2 independently done physical laboratory tests—patient anti-HLA antibody and donor HLA typing (18). Exposure to nonself HLA antigens can lead to formation of anti-HLA antibodies, a process known as sensitization (19). This occurs primarily via three types of exposure: blood transfusions, pregnancy, and solid organ transplant (19). Panel reactive antibody (PRA) is a test that identifies sensitized patients and estimate their likelihood of finding a crossmatch-compatible donor (18). The calculated PRA (cPRA), mandated in the United States since 2009 to assess immune sensitization status (18). To improve transplant rates among highly sensitized patients, the Organ Procurement and Transplantation Network implemented key changes to the kidney allocation system in December 2014 by awarding points based on cPRA level (19). Desensitization involves the use of treatment regimens that decrease the preformed antibody levels directed toward the potential donor (19). Typically, the goal of therapy is to reduce the antibody level, so the flow cytometric crossmatch is negative or lower than a predetermined cutoff (19). Many different protocols used with varying success; most combine plasmapheresis, Intravenous immunoglobulin, rituximab, bortezomib, and early initiation of maintenance immunosuppression several weeks before the transplant (19).
(ii) Assessment of donor/graft status
There are different types of donor allograft kidneys: deceased vs. living donor. Deceased brain death (DBD) organs can come from standard criteria donors or from expanded criteria donors (ECD) (20), donation after cardiac death (DCD) (21), double kidney transplant (dual) (22) or donor with increased risk social behavior (23). Living donor can be direct or non-direct (altruistic) donation vs. pair donation or pair exchange (24).
The growing gap between demand and supply for kidney transplants has led to worldwide renewed interest in the use of ECD to increase the donor pool. Although most studies confirm lower allograft survival rates and, generally, worse outcomes than standard criteria donor kidneys, recipients of expanded donor criteria kidneys generally have improved survival compared with wait-listed dialysis patients (20, 25). The Kidney Donor Profile Index (KDPI) was introduced in the United States in 2014 to guide the decision making of clinicians with respect to accepting or declining a donated kidney. The KDPI is a more refined metric for assessing expected longevity of grafted kidneys, since it considers 10 donor factors, compared to ECD which only considers four (age, creatinine, history of hypertension, and cause of death). In addition, the ECD criterion is limited since it is a binary assessment of donor quality, while KDPI estimates donor quality on a continuous scale. The KDPI measures the quality of deceased kidney and assigns a percentage score. The KDPI is derived by calculating the Kidney Donor Risk Index (KDRI)—a numerical measure of the quality of deceased donor kidney that combines 10 donor factors, including clinical parameters and demographics. The KDRI is an estimate of the relative risk of post-operative kidney graft failure (in an average adult recipient) from a particular deceased donor compared to a reference donor. The ability of KDPI to capture only some but not all donor factors that are predictive to graft outcome, and the absence of relevant recipient variables as well as factors related to the transplant procedure are amongst its important limitations (26).
Donation after circulatory death kidney transplantation has been introduced also to address organ shortage. Two recent systematic review and meta-analysis showed that long-term DCD kidney transplant outcomes are like DBD despite a higher risk of primary non function, DGF and graft loss in the first year after transplantation (27, 28).
The concept of “increased risk” (previously referred to as “high risk”) donors was created to identify a population of deceased or living donors potentially at risk for recent acquisition of human immunodeficiency virus, or viral hepatitis (29). This period between infection and the development of antibodies is called the “serological window period.” Nucleic Acid Testing, which has been used with increasing frequency over the last decade, is now required by the Organ Procurement and Transplantation Network Policy (for hepatitis C virus and human immunodeficiency virus) for all increased risk donors (29). Even with the increased sensitivity offered by nucleic acid testing, this testing may not detect a human immunodeficiency virus, hepatitis B or C virus exposure that occurred within the three to five days prior to testing (29). In communicating the risk of donor-derived infection from any donor including those associated with donors bearing the behavioral factors, it is important to consider the risks to the potential recipient of not accepting that organ and continuing to wait for another offer (29). Further, recipients who receive organs from donors bearing these characteristics should be informed that they will be monitored post-transplant for infection with human immunodeficiency virus, or hepatitis B or C virus (29).
Procurement kidney biopsies are used to assess a deceased organ donor's kidney for organ damage and potential kidney function (30). Over the years, kidney biopsies have become more widely used, but their usage varies greatly across the country (30). Recently, Organ Procurement and Transplantation Network policy proposed minimum adult kidney donor criteria which require biopsy such us: urine output of less than 100 ml in 24 h; donor has received hemodialysis or other renal replacement therapy either during most recent hospital admission or in the course of donor management; history of diabetes, including a hemoglobin A1c of 6.5 or greater during donor evaluation and management; KDPI greater than 85%; donor age 60 years old or greater; donor age 50–59, and meets at least two of the following criteria: history of hypertension; manner of death: cerebrovascular accident; terminal creatinine of 1.5 mg/dl or greater (31). However, many transplant centers don't see this as a tool to decrease the number of unnecessary biopsies, thus increasing kidney utilization (31). Reasons behind are: (i) the donor selection criteria for biopsy are too wide; (ii) no standardized approach to the biopsy process (who recovers the sample, how it is processed, read and reported); (iii) donor hospitals do not have enough infrastructure to accommodate the proposed changes; (iv) no transplant center accountability, particularly if a biopsy is not required and the center performs their own after acceptance, leading to a turn down, (v) current data shows that renal biopsy does not significantly improve long term graft success/failure (31, 32).
(iii) Hypothermic machine perfusion parameters
Kidney grafts are often preserved initially in static cold storage and subsequently on hypothermic machine perfusion (MP). Cannon et al. demonstrated the decreased incidence of DGF but no difference in graft survival by MP when compared with cold storage alone (33). In current practice in the United States, it is common that MP is used only for a small part of the entire preservation period, potentially explaining the lack of any survival benefit in the analyses (34). Similar to our center's protocol, a kidney graft may be preserved by MP only after the graft is transferred to a local organ recovery agency; a kidney may also be preserved by MP only for a short period of time (e.g., 4 h) just to assess the quality of the graft by perfusion parameters such us: pump resistance and flow and average systolic pressure (34, 35). Prolonged cold storage time (particularly ≥6 h) before MP has a negative impact on DGF occurrence in DCD kidney transplantation (34). Long MP time (≥36 h) (and thus cold ischemia time ≥42 h) detrimentally affects DGF occurrence in both DCD and DBD kidney transplant recipients even when the grafts were mainly preserved by MP (34).
(iv) Operating room
The routine verification of recipient identity, all required consents, no per os status, allergies and type and screen/cross is followed by United Network for Organ Sharing (UNOS) ABO verification. When the transplant surgery must begin before the organ arrives in the operating room, a pre-transplant verification must take place: two licensed healthcare professionals (does not have to be the surgeon); must occur before induction of general anesthesia (unless patient is receiving continuous sedation prior to arriving the operating room; then prior to first incision). Verification MUST include: UNOS donor identification expected from the UNOS match run; expected organ AND laterality (if applicable); expected donor blood type from UNOS documentation; verify recipient in room is intended recipient; intended recipient's blood type from medical record; verification that donor and recipient are ABO compatible.
Thymoglobulin, an IgG fraction purified from the serum of rabbits immunized against human thymocytes, is commonly used as immunosuppressant in kidney transplantation (36). While there are rare reports of anaphylactic reaction to thymoglobulin due to rabbit protein allergy, this can be avoided if rabbit exposure is ruled out during preoperative evaluation (36).
Due to inability of the allograft to auto regulate blood pressure, both low and high blood pressure perioperatively could be detrimental. Chronic hypotension remained a major predictive factor for DGF development with lower graft survival if kidney transplant was done from >50 years old donor (37). On the other hand, early hypertension is common after renal transplantation, however early blood pressure control has the potential to influence the risk of allograft rejection and DGF (38). In general, during anesthesia, we aim to keep blood pressure at baseline ±20%. Transplant surgeons often are asking for a mean blood pressure of 100 mmHg at the time of reperfusion. A higher than traditional normal is linked to the need of the newly grafted kidney for optimal perfusion pressure (35). Treating hypotension can be challenging in kidney transplant because vasoconstrictor drugs such as: phenylephrine (35) and/or ephedrine (39) were linked with DGF. Phenylephrine was linked to delayed graft function especially in patients who had a drop of 30 mmHg or more in blood pressure 30 min after reperfusion (35). However, it's unlikely that phenylephrine-induced vasoconstriction is the culprit, since the effect of a bolus dose is brief, and the phenylephrine was administered before reperfusion in more than half of the recipients (35). Plausibly, intraoperative phenylephrine use is a surrogate of an unmeasured hemodynamic variable, e.g., postoperative allograft perfusion, or another clinical parameter that influences the outcome (35).
A recent published Consensus Statement of the Committee of Transplant Anesthesia of the American Society of Anesthesiologists, systematic review of the literature addressed the fluid management in kidney transplantation: types of fluids, quantity, and volume status assessment (9). Regarding the amount of fluids and monitoring volume status during kidney transplantation the Consensus Statement found that we have weak recommendation for instance: low quality evidence for larger volume fluid administration targeting higher central venous pressure during KT; use of central venous pressure as a guide to fluid administration is weakly supported; weak evidence of accelerated fluid administration during graft ischemia rather than constant infusion will lead to improved graft function; although not specific to fluid volume, avoidance of intraoperative hypotension with different thresholds support improved graft function; reports of stroke volume variation or esophageal Doppler to guide fluid administration are promising but limited (9). Regarding colloids and type of crystalloids the Consensus Statement also found weak recommendations to the use of albumin over crystalloids alone discourages the use of starches which were linked to worse outcomes. However, there is strong evidence that supports the use of balanced solutions over normal saline and (9, 40).
Enhanced recovery after surgery protocols is not limited to a specific surgical intervention, allowing for wider implementation, including in kidney transplantation. Enhanced recovery after surgery protocol, modified to address kidney transplantation unique issues, is feasible and renders low morbidity and reasonable readmission rates (41).
(v) Sign out
A brief operative note should be completed prior to patient transport to ensure accurate communication to teams in the post-operative recovery area or intensive care unit. At the time of patient handoff, the surgeon and anesthesia should speak directly with the receiving team to ensure continuity of care.
The proposed checklist may appear vague without any workup specifics or cutoff, since each transplant center has its own selection criteria.
The proposed checklist is geared towards ensured consistency and completeness of miscellaneous tasks. The checklist also facilitates team communication and coordination. This manuscript did not aim to address perioperative management; therefore, specifics of perioperative management were omitted.
We present a novel standardized combined anesthesia-surgical checklist framework for kidney transplant aimed at increasing perioperative safety and streamline the perioperative care of recipients. Future validation studies will determine its clinical feasibility and post-implementation efficacy.
RN-R: Writing – original draft. GC: Conceptualization, Writing – review & editing. YR: Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. World Alliance for Patient Safety. WHO guidelines for safe surgery (2008). Available online at: http://www.who.int/patientsafety/safesurgery/knowledge_base/SSSL_Brochure_finalJun08.pdf
2. Haynes AB, Weiser TG, Berry WR, Lipsitz SR, Breizat AH, Dellinger EP, et al. A surgical safety checklist to reduce morbidity and mortality in a global population. N Engl J Med. (2009) 360(5):491–9. doi: 10.1056/NEJMsa0810119
3. Joshi S, Gorin MA, Ayyathurai R, Ciancio G. Development of a surgical safety checklist for the performance of radical nephrectomy and tumor thrombectomy. Patient Saf Surg. (2012) 6(1):27. doi: 10.1186/1754-9493-6-27
4. Nepple KG, Sandhu GS, Rogers CG, Allaf ME, Kaouk JH, Figenshau RS, et al. Description of a multicenter safety checklist for intraoperative hemorrhage control while clamped during robotic partial nephrectomy. Patient Saf Surg. (2012) 6(1):8. doi: 10.1186/1754-9493-6-8
5. Pan D, Soloway MS. The importance of transurethral resection in managing patients with urothelial cancer in the bladder: proposal for a transurethral resection of bladder tumor checklist. Eur Urol. (2012) 61(6):1199–203. doi: 10.1016/j.eururo.2012.03.018
6. Wall A, Lee GH, Maldonado J, Magnus D. Medical contraindications to transplant listing in the USA: a survey of adult and pediatric heart, kidney, liver, and lung programs. World J Surg. (2019) 43(9):2300–8. doi: 10.1007/s00268-019-05030-x
7. Faravardeh A, Eickhoff M, Jackson S, Spong R, Kukla A, Issa N, et al. Predictors of graft failure and death in elderly kidney transplant recipients. Transplantation. (2013) 96(12):1089–96. doi: 10.1097/TP.0b013e3182a688e5
8. Muller AK, Breuer E, Hubel K, Lehmann K, Cippa P, Schachtner T, et al. Long-term outcomes of transplant kidneys donated after circulatory death. Nephrol Dial Transplant. (2022) 37(6):1181–7. doi: 10.1093/ndt/gfab358
9. Wagener G, Bezinover D, Wang C, Kroepfl E, Diaz G, Giordano C, et al. Fluid management during kidney transplantation: a consensus statement of the committee on transplant anesthesia of the American Society of Anesthesiologists. Transplantation. (2021) 105(8):1677–84. doi: 10.1097/TP.0000000000003581
10. Boersma E, Kertai MD, Schouten O, Bax JJ, Noordzij P, Steyerberg EW, et al. Perioperative cardiovascular mortality in noncardiac surgery: validation of the lee cardiac risk index. Am J Med. (2005) 118(10):1134–41. doi: 10.1016/j.amjmed.2005.01.064
11. Nimmo A, Forsyth JL, Oniscu GC, Robb M, Watson C, Fotheringham J, et al. A propensity score-matched analysis indicates screening for asymptomatic coronary artery disease does not predict cardiac events in kidney transplant recipients. Kidney Int. (2021) 99(2):431–42. doi: 10.1016/j.kint.2020.10.019
12. Chadban SJ, Ahn C, Axelrod DA, Foster BJ, Kasiske BL, Kher V, et al. Summary of the kidney disease: improving global outcomes (KDIGO) clinical practice guideline on the evaluation and management of candidates for kidney transplantation. Transplantation. (2020) 104(4):708–14. doi: 10.1097/TP.0000000000003137
13. Dirix M, Philipse E, Vleut R, Hartman V, Bracke B, Chapelle T, et al. Timing of the pre-transplant workup for renal transplantation: is there room for improvement? Clin Kidney J. (2022) 15(6):1100–8. doi: 10.1093/ckj/sfac006
14. Sands JJ, Usvyat LA, Sullivan T, Segal JH, Zabetakis P, Kotanko P, et al. Intradialytic hypotension: frequency, sources of variation and correlation with clinical outcome. Hemodial Int. (2014) 18(2):415–22. doi: 10.1111/hdi.12138
15. Alhamad T, Brennan DC, Brifkani Z, Xiao H, Schnitzler MA, Dharnidharka VR, et al. Pretransplant midodrine use: a newly identified risk marker for complications after kidney transplantation. Transplantation. (2016) 100(5):1086–93. doi: 10.1097/TP.0000000000001113
16. Diena D, Messina M, De Biase C, Fop F, Scardino E, Rossetti MM, et al. Relationship between early proteinuria and long term outcome of kidney transplanted patients from different decades of donor age. BMC Nephrol. (2019) 20(1):443. doi: 10.1186/s12882-019-1635-0
17. Amer H, Cosio FG. Significance and management of proteinuria in kidney transplant recipients. J Am Soc Nephrol. (2009) 20(12):2490–2. doi: 10.1681/ASN.2008091005
18. Bhaskaran MC, Heidt S, Muthukumar T. Principles of virtual crossmatch testing for kidney transplantation. Kidney Int Rep. (2022) 7(6):1179–88. doi: 10.1016/j.ekir.2022.03.006
19. Keith DS, Vranic GM. Approach to the highly sensitized kidney transplant candidate. Clin J Am Soc Nephrol. (2016) 11(4):684–93. doi: 10.2215/CJN.05930615
20. Filiopoulos V, Boletis JN. Renal transplantation with expanded criteria donors: which is the optimal immunosuppression? World J Transplant. (2016) 6(1):103–14. doi: 10.5500/wjt.v6.i1.103
21. Gill J, Rose C, Lesage J, Joffres Y, Gill J, O'Connor K. Use and outcomes of kidneys from donation after circulatory death donors in the United States. J Am Soc Nephrol. (2017) 28(12):3647–57. doi: 10.1681/ASN.2017030238
22. Dafoe DC, Alfrey EJ. Dual renal grafts: expansion of the donor pool from an overlooked source. Transpl Int. (1998) 11(3):164–8. doi: 10.1111/j.1432-2277.1998.tb00797.x
23. Reese PP, Tehrani T, Lim MA, Asch DA, Blumberg EA, Simon MK, et al. Determinants of the decision to accept a kidney from a donor at increased risk for blood-borne viral infection. Clin J Am Soc Nephrol. (2010) 5(5):917–23. doi: 10.2215/CJN.08251109
24. United Network for Organ Sharing. Kidney paired donation—KPD (2022). Available online at: https://unos.org/transplant/kidney-paired-donation/ (Accessed April 04, 2024).
25. Merion RM, Ashby VB, Wolfe RA, Distant DA, Hulbert-Shearon TE, Metzger RA, et al. Deceased-donor characteristics and the survival benefit of kidney transplantation. JAMA. (2005) 294(21):2726–33. doi: 10.1001/jama.294.21.2726
26. Health Resources and Services Administration. A Guide to Calculating and Interpreting the Kidney Donor Profle Index (KDPI). Available online at: https://optn.transplant.hrsa.gov/media/1512/guide_to_calculating_interpreting_kdpi.pdf (Accessed June 06, 2024).
27. Gavriilidis P, Inston NG. Recipient and allograft survival following donation after circulatory death versus donation after brain death for renal transplantation: a systematic review and meta-analysis. Transplant Rev (Orlando). (2020) 34(4):100563. doi: 10.1016/j.trre.2020.100563
28. Rijkse E, Ceuppens S, Qi H, IJzermans JNM, Hesselink DA, Minnee RC. Implementation of donation after circulatory death kidney transplantation can safely enlarge the donor pool: a systematic review and meta-analysis. Int J Surg. (2021) 92:106021. doi: 10.1016/j.ijsu.2021.106021
29. OPTN/UNOS. Guidance on explaining Risk Related to Use of U.S. PHS Increased Risk Donor Organs When Considering Organ Offers: Juner 2017 (2017). Available online at: https://optn.transplant.hrsa.gov/media/2116/guidance_increased_risk_organ_offers_20170327.pdf (Accessed April 04, 2024).
30. Lentine KL, Fleetwood VA, Caliskan Y, Randall H, Wellen JR, Lichtenberger M, et al. Deceased donor procurement biopsy practices, interpretation, and histology-based decision-making: a survey of US kidney transplant centers. Kidney Int Rep. (2022) 7(6):1268–77. doi: 10.1016/j.ekir.2022.03.021
31. Temple K. Establish Minimum Kidney Donor Criteria to Require Biopsy: Organ Procurement & Transplantation Network (2022). Available online at: https://optn.transplant.hrsa.gov/media/pgngir2n/establish-minimum-kidney-donor-criteria-to-require-biopsy_winter-2022-pc.pdf (Accessed April 04, 2024).
32. Wang CJ, Wetmore JB, Crary GS, Kasiske BL. The donor kidney biopsy and its implications in predicting graft outcomes: a systematic review. Am J Transplant. (2015) 15(7):1903–14. doi: 10.1111/ajt.13213
33. Cannon RM, Brock GN, Garrison RN, Smith JW, Marvin MR, Franklin GA. To pump or not to pump: a comparison of machine perfusion vs cold storage for deceased donor kidney transplantation. J Am Coll Surg. (2013) 216(4):625–33. discussion 33–4. doi: 10.1016/j.jamcollsurg.2012.12.025
34. Paloyo S, Sageshima J, Gaynor JJ, Chen L, Ciancio G, Burke GW. Negative impact of prolonged cold storage time before machine perfusion preservation in donation after circulatory death kidney transplantation. Transpl Int. (2016) 29(10):1117–25. doi: 10.1111/tri.12818
35. Mendez NV, Raveh Y, Livingstone JJ, Ciancio G, Guerra G, Burke Iii GW, et al. Perioperative risk factors associated with delayed graft function following deceased donor kidney transplantation: a retrospective, single center study. World J Transplant. (2021) 11(4):114–28. doi: 10.5500/wjt.v11.i4.114
36. Brabant S, Facon A, Provot F, Labalette M, Wallaert B, Chenivesse C. An avoidable cause of thymoglobulin anaphylaxis. Allergy Asthma Clin Immunol. (2017) 13:13. doi: 10.1186/s13223-017-0186-9
37. Dolla C, Mella A, Vigilante G, Fop F, Allesina A, Presta R, et al. Recipient pre-existing chronic hypotension is associated with delayed graft function and inferior graft survival in kidney transplantation from elderly donors. PLoS One. (2021) 16(4):e0249552. doi: 10.1371/journal.pone.0249552
38. Berber I, Aydin C, Yigit B, Kara VM, Yildar M, Duzyol C, et al. Blood pressure and graft outcome in renal transplantation. Transplant Proc. (2005) 37(2):997–8. doi: 10.1016/j.transproceed.2005.01.021
39. Efune GE, Zerillo J, Zhou G, Mazzeffi MA, Demaria S, Wang C. Society for the advancement of transplant anesthesia research committee writing G. intravenous fluid management practices in kidney transplant patients: a multicenter observational cohort pilot study. Semin Cardiothorac Vasc Anesth. (2020) 24(3):256–64. doi: 10.1177/1089253220901665
40. Kolodzie K, Cakmakkaya OS, Boparai ES, Tavakol M, Feiner JR, Kim MO, et al. Perioperative normal saline administration and delayed graft function in patients undergoing kidney transplantation: a retrospective cohort study. Anesthesiology. (2021) 135(4):621–32. doi: 10.1097/ALN.0000000000003887
Keywords: checklist, kidney transplantation, perioperative, anesthesia, surgery
Citation: Nicolau-Raducu R, Ciancio G and Raveh Y (2024) Development of a checklist framework for kidney transplantation. Front. Transplant. 3:1412391. doi: 10.3389/frtra.2024.1412391
Received: 4 April 2024; Accepted: 13 June 2024;
Published: 25 June 2024.
Edited by:
Abdolreza Haririan, University of Maryland, United StatesReviewed by:
Duilio Pagano, Mediterranean Institute for Transplantation and Highly Specialized Therapies (ISMETT), Italy© 2024 Nicolau-Raducu, Ciancio and Raveh. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ramona Nicolau-Raducu, cnhuMjU2QG1pYW1pLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.