
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Transplant. , 27 October 2023
Sec. Transplantation Immunology
Volume 2 - 2023 | https://doi.org/10.3389/frtra.2023.1264903
 Wolfgang Arns1*
Wolfgang Arns1* Aurélie Philippe2,3Vanessa Ditt4Ingeborg A. Hauser5
Aurélie Philippe2,3Vanessa Ditt4Ingeborg A. Hauser5 Friedrich Thaiss6Claudia Sommerer7
Friedrich Thaiss6Claudia Sommerer7 Barbara Suwelack8Duska Dragun9Jan Hillen10Christiane Schiedel10Anja Elsässer10
Barbara Suwelack8Duska Dragun9Jan Hillen10Christiane Schiedel10Anja Elsässer10 Björn Nashan11,12*
Björn Nashan11,12*
Background: Studies prospectively monitoring de novo donor-specific antibodies (dnDSAs) and their clinical impact are sparse. This substudy of ATHENA was initiated to evaluate the effect of everolimus (EVR) or mycophenolic acid (MPA) in combination with reduced calcineurin inhibitor (CNI, tacrolimus [TAC] or cyclosporine [CsA]) on the formation of human leukocyte antibodies (HLA), including dnDSA, and the impact on clinical outcomes in kidney transplant (KTx) recipients.
Methods: All eligible patients were randomized 1:1:1 to receive either EVR + TAC, EVR + CsA or MPA + TAC, with basiliximab induction plus steroids after transplantation up to Month 12. The incidence of dnDSA by treatment group and the association with clinical events were evaluated descriptively as an exploratory objective in the intent-to-treat (ITT) and per-protocol (PP) populations with at least one antibody assessment.
Results: Overall, none of the patients in the EVR + TAC group had either dnDSA or antibody mediated rejection (PP or ITT population) and only one patient with dnDSA in the TAC + MPA group had antibody mediated rejection.
Conclusion: The EVR regimen was comparable to MPA regimen with an extremely low incidence of dnDSA over 1 year of treatment.
The development of de novo donor-specific human leukocyte antigen (HLA) antibodies (dnDSA) is a major risk factor for acute and chronic antibody-mediated rejection (AMR) and graft loss after kidney transplantation (KTx) (1). Single center studies report that acute AMR was more common in KTx recipients with dnDSA vs. without dnDSA (18.8% vs. 0%, respectively; P < 0.001) (2) and probability of graft survival was lower (79% vs. 94%, respectively; P = 0.05) (3). In a case-control study, dnDSA were more common in patients with graft failure vs. controls without graft failure (54% vs. 16%, respectively; P < 0.001), and chronic active AMR was significantly more common in patients with dnDSA compared to those without dnDSA (61% vs. 12%, P < 0.001) (4). The prevalence of dnDSAs is generally between 5% and 10% at 1-year post KTx and slowly increases thereafter to 20% at 5 years (5). Risk factors for dnDSA development include a high number of HLA mismatches (especially DQ mismatches), and inadequate immunosuppression and non-adherence (1). Since dnDSA development has been associated with worse outcomes, it is important to avoid this undesirable alloimmune response and understand the effects of different immunosuppressive agent combinations on dnDSA formation. Although B cells and plasma cells produce antibodies, T cells also play role in the development of dnDSA, and effective T-cell suppression is required to prevent dnDSA formation (6).
Everolimus (EVR), an inhibitor of mammalian target of rapamycin (mTORi), permits reduced calcineurin inhibitor (CNI) exposure after KTx (7). CNIs affect humoral immune response by acting on T cells, whereas mTORis, such as EVR, affect both T cells and B cells (6). Previous studies with CNI-free EVR-based regimens in KTx patients demonstrated increased formation of dnDSA and transplant rejection compared with CNI (8–10). Also, Liefeldt and colleagues reported an increased risk for dnDSA after conversion to CNI-free therapy with EVR, though another reason could be that a high percentage of patients were also steroid-free, and CNI- plus steroid-free regimen may have led to rejection (11). These CNI elimination immunosuppression regimens may result in inadequate immunosuppression, possibly contributing to DSA development and subsequent graft failure.
An alternative strategy using EVR with reduced CNI exposure was investigated in the ATHENA study, a large, randomized trial involving 612 de novo kidney transplant recipients (ClinicalTrials.gov identifier: NCT01843348; EudraCT number: 2011–005238–21) (7). ATHENA compared EVR + tacrolimus (TAC) or EVR + cyclosporine A (CsA) vs. a standard-of-care regimen of mycophenolic acid (MPA) + TAC; all patients received steroids. The 12-month results of the ATHENA study revealed a comparable efficacy of EVR + TAC or EVR + CsA to MPA + TAC and though non-inferiority of renal function with EVR + TAC/CsA was not achieved, an increase in renal function from Month 1 to 12 was comparable in both EVR and MPA groups (7). Given the paucity of data with regards to the development of dnDSA with EVR + reduced CNI-therapy in de novo kidney transplant recipients, this substudy of ATHENA was initiated to evaluate the effect of EVR or MPA in combination with reduced CNI on the formation of HLA antibodies, including dnDSA, and the impact on clinical outcomes over 1 year.
ATHENA was a 12-month, prospective, multicenter, randomized, controlled, parallel-group, open-label study in de novo kidney transplant recipients (who received a first kidney transplant). The study was conducted from December 27, 2012 through March 23, 2016 in Germany and France. Details of the ATHENA study, including complete inclusion/exclusion criteria, the immunosuppression regimen, and patient stratification have been described previously (7).
In brief, patients with preformed HLA antibodies not directed against the donor and with <20% panel reactivity at the time of transplant were included in the study (12). Patients with a current panel reactive antibody level of >20% (within 4 months before enrollment) were excluded from the study.
Patients were randomized 1:1:1 to receive either, EVR + TAC, EVR + CsA, or MPA + TAC. EVR was maintained at target trough concentration of 3–8 ng/mL throughout the study period. The target trough concentration of TAC in the EVR + TAC and MPA + TAC arms was 4–8 ng/mL until the end of Month 2 and 3–5 ng/mL thereafter. In the EVR + CsA arm, the target trough concentration of CsA was 75–125 ng/mL until the end of Month 2 and 50–100 ng/mL thereafter. MPA was used either as enteric coated mycophenolate sodium (1.44 g/day) or mycophenolate mofetil (2 g/day). All patients received basiliximab 20-mg induction therapy on Day 0 and 4, and steroids (≥5 mg/day) until Month 12 (Supplementary Figure S1). The study was conducted in accordance with the Declaration of Helsinki and the International Conference on Harmonization Guidelines for Good Clinical Practice. The study was approved by all competent Ethics Committees and regulatory authorities. Informed consent was obtained by investigators from all patients enrolled into the study.
The primary objective of the ATHENA study was to demonstrate non-inferiority of renal function [as assessed by estimated glomerular filtration rate (eGFR), Nankivell formula] with EVR + TAC and/or EVR + CsA vs. MPA + TAC at Month 12 after transplantation (7). This substudy was performed with the objective to evaluate the incidence of HLA antibodies, including DSA, by treatment group and the association with acute rejection within 1 year post de novo KTx (12). Blood samples (5 ml) for all patients were collected at baseline, Month 6, and Month 12. The presence and evolution of HLA antibodies and DSA antibodies in serum at baseline and Month 12 were evaluated using Luminex® LABScreenTM Single Antigen Bead assays (One Lambda, CA, USA) according to the manufacturer's instructions (13). This method used color-coded microbeads coated with purified HLA-A, -B, -C, -DR and -DQ, and major-histocompatibility-complex (MHC) class I–related chain A (MICA) antigens. The beads were analyzed using Luminex xMAP multiplex technology. In principle, the presence of HLA antibodies was detected using a goat anti-human IgG coupled with phycoerythrin, and fluorescence of each bead was detected by the reader and recorded as mean fluorescent intensity (MFI) as described previously by our group (14). A cut-off of 500 MFI was selected based on the literature (15).
Patients who received at least one dose of the study drug were considered in the intent-to-treat (ITT) population and all ITT patients without any major protocol deviation were considered in the per-protocol (PP) population. This post hoc analysis included a statistical analysis plan that was developed after the database lock for analyses of preformed HLA antibodies and dnDSA. The analysis set included all transplanted patients with at least one antibody assessment (either HLA and/or non-HLA). The analysis of HLA antibodies was carried out descriptively. Demographic variables were analyzed using F-test for continuous variables and Fisher's exact test for categorical variables. The embedded subgroups of HLA antibodies were defined as preformed HLA: respective HLA class/loci detected at baseline (MFI ≥ 500) independent of mismatch; respective preformed critical HLA: HLA class/loci detected at baseline (MFI ≥ 500) although being a mismatch; and dnDSA: HLA class/loci detected: respective HLA class/loci increased from negative or <500 MFI at baseline to MFI ≥ 500 at endpoint and the HLA was specified as mismatch.
Of 655 patients randomized to treatment in ATHENA, 612 patients who received at least one dose of the study drug were included in the ITT population and 338 in the PP population (7). Of these, 606 (206 in EVR + TAC, 198 in EVR + CsA, and 202 in MPA + TAC) and 337 (110 in EVR + TAC, 80 in EVR + CsA, and 147 in MPA + TAC) patients, respectively, had at least one antibody assessment and were included in the ITT and PP analysis populations described herein for the HLA analyses. We limited the main analyses to the PP population since this population comprised patients who were on the assigned treatment regimen throughout the study without major protocol deviations and would better represent the effect of continuous immunosuppression. Results in the ITT population were comparable to those reported for the PP population and are presented in the Supplementary Tables S1–S3.
In general, baseline demographic and clinical characteristics of patients were well balanced between treatment groups except a numerically higher proportion of patients with 2 human leukocyte antigen-DR mismatches in the EVR + TAC and EVR + CsA groups compared with MPA + TAC group (Table 1 [PP population with HLA data] and Supplementary Table S1 [ITT population]). This finding was consistent to that reported for the ITT population in the primary ATHENA study (7).

Table 1. Baseline demographics and characteristics of patients in ATHENA HLA substudy cohort (PP population with HLA data at baseline).
At baseline, HLA data were available for 294/337 patients in the PP population (97 in EVR + TAC, 68 in EVR + CsA, and 129 in MPA + TAC; Table 2). Data for 535/606 patients in the ITT population with HLA data available are shown in Supplementary Table S2. A total of 130 patients (44.2%) in the PP population had preformed HLA antibodies at baseline (EVR + TAC, 46.4%; EVR + CsA, 41.2%; and MPA + TAC, 44.2%; MFI ≥ 500 independent of mismatch) (Table 2).
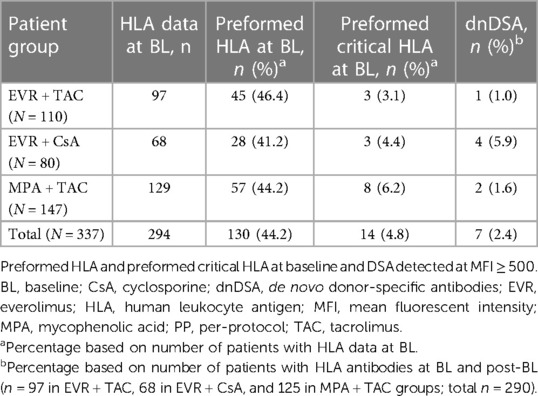
Table 2. Patients in ATHENA HLA substudy cohort with preformed HLA and dnDSA antibody data (PP population).
Overall, 8/130 (6.2%) patients from the PP population with preformed HLA had clinical events (EVR + TAC, 6.7%, EVR + CsA, 7.1%, and MPA + TAC, 5.3%) (Table 3). These clinical events were all biopsy-proven acute rejection (BPAR): 1 patient in the EVR + TAC group had evidence of AMR and the other 7 patients had no evidence of AMR. No patients experienced graft loss or death. Corresponding data for the ITT population are shown in Supplementary Table S3. In the PP population, the change in renal function (eGFR, Nankivell) from baseline to Month 12 was comparable between patients with or without preformed HLA at baseline treated with EVR + TAC (3.9 and 3.5 mL/min/1.73 m2, respectively) or MPA + TAC (8.5 and 7.7 mL/min/1.73 m2, respectively) (Figure 1).
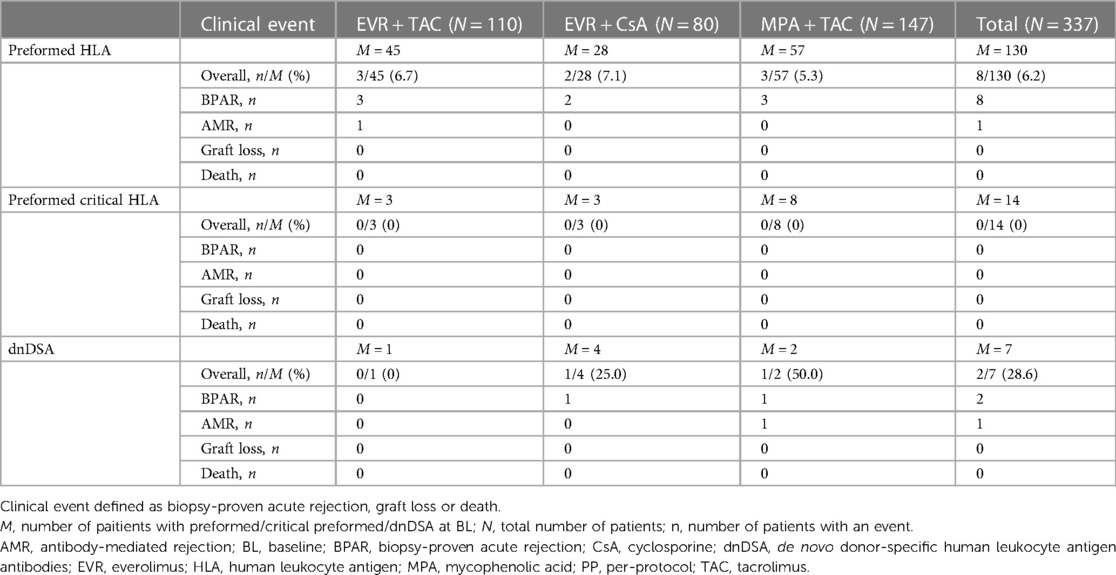
Table 3. Clinical outcome of patients with preformed HLA and dnDSA (PP population).
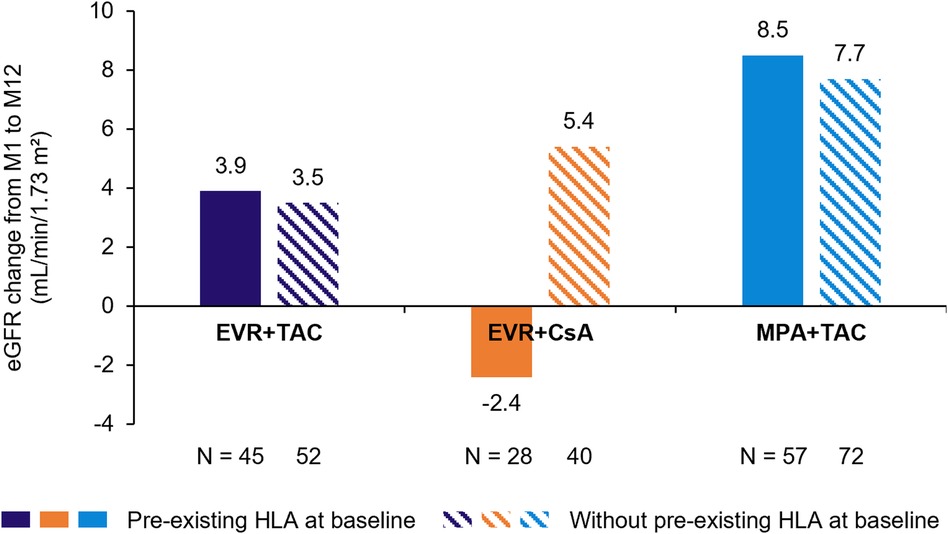
Figure 1. Change in renal function (eGFR, Nankivell) over 12 months in patients with vs. without preformed HLA antibodies (PP population). N is patients with eGFR data at Month 12. CsA, cyclosporine; eGFR, estimated glomerular filtration rate; EVR, everolimus; HLA, human leukocyte antigen; MPA, mycophenolic acid; PP, per-protocol; TAC, tacrolimus.
In the PP population, 14 patients had preformed critical HLA antibodies at baseline (MFI ≥ 500 although being a mismatch): EVR + TAC, 3.1%; EVR + CsA, 4.4%; and MPA + TAC, 6.2% (Table 2). None of these patients had a clinical event over Month 12 (BPAR, graft loss, or death; Table 3). Corresponding data for the ITT population are shown in Supplementary Table S3.
Across the 3 immunosuppressive regimens, only 7 patients in the PP population developed dnDSA (MFI ≥ 500) within 1 year after KTx. Similar rates of dnDSA development were observed in the EVR + CsA [1 patient (1%)] and MPA + TAC [2 patients (1.6%)] groups (Table 2). In the EVR + CsA group, 4 (5.9%) patients developed dnDSA. Of these 7 patients with dnDSA, 2 patients had clinical events: 1 patient in the EVR + CsA and MPA + TAC groups, respectively, both of whom experienced BPAR (Table 3). The patient in the EVR + CsA group had no evidence of AMR, whereas only 1 patient in the MPA + TAC group had evidence of AMR. No graft loss or death occurred in any patient with dnDSA in the PP population. Corresponding data for the ITT population is shown in Supplementary Table S3. Of note, neither in the PP nor in the ITT population dnDSA were observed in the EVR + TAC group.
Primary results of the ATHENA study showed that EVR + reduced CNI was efficient and safe in de novo patients (7). The study showed that renal function was comparable between the EVR arms and standard-of-care regimen (MPA + TAC), and that immunosuppressive efficacy was similar in the EVR + TAC and MPA + TAC groups. In addition, both EVR-based arms had significantly fewer cytomegalovirus infections compared with the MPA + TAC regimen. This prospective substudy of ATHENA showed that EVR + reduced CNI was also very effective against formation of dnDSA. More importantly, after 12 months there was no substantial difference between the 3 immunosuppression regimens on the development of dnDSA, suggesting EVR does not increase the risk for dnDSA development.
Overall, the incidence of dnDSA was extremely low under conditions of a controlled clinical trial and dnDSA, at least in this setting, did not appear to adversely affect clinical outcomes. Our findings confirmed that AMR is not necessarily related to the development of dnDSA per se. Although the substudy was designed to investigate the impact of immunosuppressive regimens on the development of dnDSA, it was interesting to observe that the presence of preformed HLA antibodies (MFI ≥ 500 at baseline, independent of mismatch) and critical HLA antibodies (MFI ≥ 500 at baseline, although being a mismatch) had no influence on clinical outcome, irrespective of EVR or MPA exposure.
Previous preclinical studies involving kidney and heart allotransplantation models have demonstrated an inferior immunosuppressive ability with EVR vs. CNI exposure, indicating that CNI-free regimens present an immunological risk (16, 17). Also, clinical studies have suggested that CNI-free and CNI-sparing regimens may be associated with an increased risk of acute rejection (18, 19). Plus, in addition to acute rejection as an indicator of under-immunosuppression, the CNI-sparing regimen with EVR vs. MPA has been said to lead to the development of DSAs and AMR. Yet, on the contrary, other studies investigating CNI-minimizing regimens have not been associated with an increased incidence of acute rejection/immunological risk in de novo KTx patients (20–23), which goes well with the findings of this substudy. Here, we have presented an ideal platform to prospectively analyze the formation of DSAs in the ATHENA study and to determine if immunosuppression is adequate in controlling the emergence of DSAs and AMR.
In line with our findings, results from several randomized, controlled trials in de novo KTx patients have shown that EVR with reduced-exposure CNI is not associated with a higher incidence of dnDSA compared to standard-exposure CNI (24–26). Moreover, no difference in the incidence of acute rejection between groups was reported. In addition, our findings were comparable with another observational study in patients treated with MPA plus TAC, either once or twice daily over 2 years (incidence of DSA: 3.6% and 1.2% and AMR: 4.8% and 2.7%, respectively, with twice- and once-daily TAC) (27). Hence, these findings, in combination with our results, which both exhibited no increased risk for dnDSAs in patients receiving EVR with reduced CNI, strongly oppose results of other studies that suggest dnDSA may be more frequent in patients given EVR in a CNI-free regimen (8–10), likely reflecting inadequate immunosuppression with CNI-free regimens.
The role of induction therapy in preventing de novo DSA is also worth discussion. Studies have reported that induction with basiliximab is associated with lower incidence of de novo DSA in kidney transplant recipients compared with anti-depleting agent, alemtuzumab or rabbit antithymocyte globulin (rATG) (28). Bath NM et al. (2020) also reported that patients who received induction with basiliximab had lower incidence of de novo DSA than alemtuzumab, which could be because of elevated B-cell activating factor levels in patients treated with alemtuzumab (29). In our study, basiliximab was given as induction therapy in all treatment arms, all of which showed an extremely low incidence of DSA over 1 year treatment. Results from the TRANSFORM study in which majority of patients received induction with basiliximab (83%) showed comparable low incidence of de novo DSA on treatment with EVR + reduced CNI vs. MPA + standard CNI over 12 months (10.2% vs. 13.6%, P = 0.508) and 24 months (22.4% vs. 17.7%, P = 0.508) (24, 26). A retrospective analysis of a randomized trial reported comparable incidence of de novo DSA over 12 months in patients who received r-ATG + EVR + TAC [5/78 (6.4%)] vs. basiliximab + EVR + TAC [3/87 (3.4%)] vs. basiliximab + MPS + TAC [5/90 (5.5%)] (25). A multicenter analysis of 24 patients who were enrolled to 2-year, randomized phase-3 study (RAD001A1202 study) and treated with basiliximab + EVR + reduced CsA vs. basiliximab + MMF + standard CsA showed comparable rates of de novo DSA (15.4% vs. 18.3%) over 10 years (30).
The favorable effects observed in this study with the mTORi, EVR-based regimen, can be explained. The mTOR signaling plays an important role in the pathomechanism of HLA antibody-mediated endothelial cell activation and proliferation, which lead to rejection and vasculopathies. The HLA antibodies stimulate the activation of mTOR, as well as the downstream targets extracellular-signal regulated kinase (ERK), S6 kinase (S6K), and S6 ribosomal protein (S6RP) [the latter stimulating intercellular adhesion molecule 1 (ICAM-1) expression and clustering], and favor monocyte adhesion to the endothelium (31). In an in vitro model, mTOR inhibition suppressed Ezrin/Radixin/Moesin (ERM) phosphorylation, ICAM-1 clustering and monocyte adhesion to HLA antibody-activated endothelium (32). Another in vitro study showed that mTOR inhibition prevented endothelial cell proliferation by downregulating interleukin-8 (IL-8), monocyte chemoattractant protein-1 (MCP-1), transforming growth factor-β1 (TGF-β1) and von Willebrand factor (vWF) (33). A recently reported cohort study in hypersensitized kidney transplant recipients (calculated panel reactive antibody ≥50%) showed better results in patients treated with EVR vs. MPA, both in combination with CNI and steroids. The risk of BPAR-free survival over 1 year was lower in the EVR group (hazard ratio: 0.32, confidence interval: 0.11–0.90, P = 0.031) with numerically lower incidence of dnDSA (4/33 [12.1%] vs. 6/38 [18.2%], P = 0.408) (34).
The low number of dnDSAs and events at 12 months in the PP population clearly indicate that close follow-up and monitoring of patients following transplantation play a major role in preventing the development of DSAs. In our study, it is possible that we did not observe any difference in dnDSA development between the 3 immunosuppressive regimens because CNIs were included in all study arms. Moreover, non-adherence increases the likelihood of dnDSA production (1). Similar to other controlled studies, the ATHENA trial conditions were likely to support medication adherence, leading to effective immunosuppression. Although there were high rates of study drug discontinuation and withdrawal in the ATHENA study (7), our primary analysis was based on the PP population. Thus, the treatment effect was estimated among adherent patients, which may have led to the observed comparable rate of dnDSA development across the 3 immunosuppressive regimens. However, it should be noted that similarly low rates of dnDSA development were observed across treatment groups in the ITT population, which included both adherent and non-adherent patients.
There are few limitations which are worth consideration. A follow-up to Month 12 after transplantation does not encompass the long-term effects of the treatment regimens on development of DSA or AMR. Further long-term results, ideally 5- or 10-year data, from prospective studies are required to fully understand the risk of these immunosuppressive regimens on dnDSA and AMR. Nevertheless, late graft loss tends to be related to recurrence of previous disease and adherence to the therapy protocol rather than to the initial immunosuppressive protocol (35). Finally, the substudy was not powered to detect statistical significant differences in clinical outcomes. Thus, the lack of differences in dnDSAs between the groups may be due to the small sample size. The strength of the analysis includes the prospective nature of data sampling, and as such, the data are embedded in a broad analysis of primary and secondary endpoints conducted as part of the primary ATHENA study (7). In the ATHENA study, kidneys were allocated within Eurotransplant according to the standard allocation process (36).
The non-HLA antibodies may also play an important role in transplant rejection and patients with both HLA and non-HLA antibodies have been reported to have poor outcomes and lower graft survival (37–39). A separate substudy of ATHENA evaluated the effect of EVR in combination with CNI on the formation of non-HLA antibodies and graft outcome in KTx patients (40). The results showed that EVR + TAC group had a higher incidence of patients negative for angiotensin II type 1 receptor (AT1R) and endothelin-1 type A receptor (ETAR) antibodies (82.2% and 76.7%, respectively) compared to MPA + TAC group (71.9% and 65.3%, respectively) over Month 12. Similar to findings found for HLA, non-HLA antibodies had no influence on clinical outcomes and no death was reported in patients.
In conclusion, findings from the ATHENA substudy showed that immunosuppression with EVR or MPA in combination with reduced CNI did not increase the risk for dnDSA development. Interestingly, the overall incidence of dnDSA was extremely low and did not directly influence clinical outcome in the first 12 months after KTx. Preformed HLA antibodies (MFI ≥ 500 at baseline, independent of mismatch) and critical HLA antibodies (MFI ≥ 500 at baseline, although being a mismatch) had no influence on clinical outcome, irrespective of EVR or MPA exposure. Clinical outcomes are in line with previous results of ATHENA trial (7).
Anonymized patient-level data from clinical trials may be shared by Novartis in a consortium called ClinicalStudyDataRequest.com (CSDR) in accordance with Novartis’ policy for sharing clinical trial data. Requests to access the datasets should be directed to https://www.clinicalstudydatarequest.com/Study-Sponsors/Study-Sponsors-Novartis.aspx.
The studies involving humans were approved by Ärztekammer Hamburg, Geschäftsstelle der Ethik-Kommission, Weidestr. 122b, 22083 Hamburg. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
WA: Writing – original draft, Writing – review & editing. AP: Writing – original draft, Writing – review & editing. VD: Writing – original draft, Writing – review & editing. IH: Writing – original draft, Writing – review & editing, Investigation. FT: Writing – original draft, Writing – review & editing. CS: Writing – original draft, Writing – review & editing, Investigation. BS: Writing – original draft, Writing – review & editing. DD: Writing – original draft, Writing – review & editing. JH: Writing – original draft, Writing – review & editing. CS: Writing – original draft, Writing – review & editing, Methodology. AE: Writing – original draft, Writing – review & editing. BN: Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, and/or publication of this article.
This study was funded by Novartis Pharma GmbH, Nuremberg, Germany.
In memoriam DD, our dear friend and always inspiring colleague, who passed away much too early. The authors thank the participating patients and clinicians involved in the trial. The authors would also like to thank Sarabjeet Kaur, PhD, of Novartis Healthcare Pvt Ltd, for medical writing support and Elizabeth Grünewald from Winicker Norimed GmbH for performing the statistical analysis.
WA received consulting honoraria from Novartis. IAH was in the advisory board of Novartis and received honoraria for lectures from Takeda, Biotest, MSD, CareDx, Novartis, Astellas, Bayer, and Astra Zeneca. FT has received study honoraria from Novartis, Sanofi, Astellas, Alexion, Hexal, Chiesi, and Pfizer. BS received study honoraria and was in the advisory board of Novartis. JH, CS, and AE are employees of Novartis. BN was in the advisory board and received funding from Novartis.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frtra.2023.1264903/full#supplementary-material
1. Zhang R. Donor-specific antibodies in kidney transplant recipients. Clin J Am Soc Nephrol. (2018) 13(1):182–92. doi: 10.2215/CJN.00700117
2. Jung HY, Kim SH, Seo MY, Cho SY, Yang Y, Choi JY, et al. Characteristics and clinical significance of de novo donor-specific anti-HLA antibodies after kidney transplantation. J Korean Med Sci. (2018) 33(34):e217. doi: 10.3346/jkms.2018.33.e217
3. Lachmann N, Terasaki PI, Budde K, Liefeldt L, Kahl A, Reinke P, et al. Anti-human leukocyte antigen and donor-specific antibodies detected by luminex posttransplant serve as biomarkers for chronic rejection of renal allografts. Transplantation. (2009) 87(10):1505–13. doi: 10.1097/TP.0b013e3181a44206
4. Castro A, Malheiro J, Tafulo S, Dias L, Martins LS, Fonseca I, et al. Role of de novo donor-specific anti-HLA antibodies in kidney graft failure: a case-control study. HLA. (2017) 90(5):267–75. doi: 10.1111/tan.13111
5. Thaunat O, Koenig A, Leibler C, Grimbert P. Effect of immunosuppressive drugs on humoral allosensitization after kidney transplant. J Am Soc Nephrol. (2016) 27(7):1890–900. doi: 10.1681/ASN.2015070781
6. O'Leary JG, Samaniego M, Barrio MC, Potena L, Zeevi A, Djamali A, et al. The influence of immunosuppressive agents on the risk of de novo donor-specific HLA antibody production in solid organ transplant recipients. Transplantation. (2016) 100(1):39–53. doi: 10.1097/TP.0000000000000869
7. Sommerer C, Suwelack B, Dragun D, Schenker P, Hauser IA, Witzke O, et al. An open-label, randomized trial indicates that everolimus with tacrolimus or cyclosporine is comparable to standard immunosuppression in de novo kidney transplant patients. Kidney Int. (2019) 96(1):231–44. doi: 10.1016/j.kint.2019.01.041
8. de Fijter JW, Holdaas H, Øyen O, Sanders JS, Sundar S, Bemelman FJ, et al. Early conversion from calcineurin inhibitor- to everolimus-based therapy following kidney transplantation: results of the randomized ELEVATE trial. Am J Transplant. (2017) 17(7):1853–67. doi: 10.1111/ajt.14186
9. Kamar N, Del Bello A, Congy-Jolivet N, Guilbeau-Frugier C, Cardeau-Desangles I, Fort M, et al. Incidence of donor-specific antibodies in kidney transplant patients following conversion to an everolimus-based calcineurin inhibitor-free regimen. Clin Transplant. (2013) 27(3):455–62. doi: 10.1111/ctr.12127
10. Liefeldt L, Brakemeier S, Glander P, Waiser J, Lachmann N, Schönemann C, et al. Donor-specific HLA antibodies in a cohort comparing everolimus with cyclosporine after kidney transplantation. Am J Transplant. (2012) 12(5):1192–8. doi: 10.1111/j.1600-6143.2011.03961.x
11. Pascual J, Arns W. Does everolimus increase donor-specific HLA antibodies in kidney transplant recipients? Am J Transplant. (2012) 12(9):2561–2; author reply 3. doi: 10.1111/j.1600-6143.2012.04159.x
12. Sommerer C, Suwelack B, Dragun D, Schenker P, Hauser IA, Nashan B, et al. Design and rationale of the ATHENA study--A 12-month, multicentre, prospective study evaluating the outcomes of a de novo everolimus-based regimen in combination with reduced cyclosporine or tacrolimus versus a standard regimen in kidney transplant patients: study protocol for a randomised controlled trial. Trials. (2016) 17:92. doi: 10.1186/s13063-016-1220-9
13. One Lambda. Antibody Monitoring. (2022). Available at: https://www.thermofisher.com/onelambda/wo/en/post-transplant/antibody-monitoring.html
14. Dieplinger G, Ditt V, Arns W, Huppertz A, Kisner T, Hellmich M, et al. Impact of de novo donor-specific HLA antibodies detected by Luminex solid-phase assay after transplantation in a group of 88 consecutive living-donor renal transplantations. Transpl Int. (2014) 27(1):60–8. doi: 10.1111/tri.12207
15. Wisse WB, Kamburova EG, Joosten I, Allebes WA, van der Meer A, Hilbrands LB, et al. Toward a sensible single-antigen bead cutoff based on kidney graft survival. Transplantation. (2019) 103:789–97. doi: 10.1097/TP.0000000000002357
16. Schuler W, Sedrani R, Cottens S, Häberlin B, Schulz M, Schuurman HJ, et al. SDZ RAD, a new rapamycin derivative: pharmacological properties in vitro and in vivo. Transplantation. (1997) 64(1):36–42. doi: 10.1097/00007890-199707150-00008
17. Schuurman HJ, Cottens S, Fuchs S, Joergensen J, Meerloo T, Sedrani R, et al. SDZ RAD, a new rapamycin derivative: synergism with cyclosporine. Transplantation. (1997) 64(1):32–5. doi: 10.1097/00007890-199707150-00007
18. Ekberg H, Grinyó J, Nashan B, Vanrenterghem Y, Vincenti F, Voulgari A, et al. Cyclosporine sparing with mycophenolate mofetil, daclizumab and corticosteroids in renal allograft recipients: the CAESAR study. Am J Transplant. (2007) 7(3):560–70. doi: 10.1111/j.1600-6143.2006.01645.x
19. Vincenti F, Ramos E, Brattstrom C, Cho S, Ekberg H, Grinyo J, et al. Multicenter trial exploring calcineurin inhibitors avoidance in renal transplantation. Transplantation. (2001) 71(9):1282–7. doi: 10.1097/00007890-200105150-00017
20. Lorber MI, Mulgaonkar S, Butt KM, Elkhammas E, Mendez R, Rajagopalan PR, et al. Everolimus versus mycophenolate mofetil in the prevention of rejection in de novo renal transplant recipients: a 3-year randomized, multicenter, phase III study. Transplantation. (2005) 80(2):244–52. doi: 10.1097/01.TP.0000164352.65613.24
21. Nashan B. Induction therapy and mTOR inhibition: minimizing calcineurin inhibitor exposure in de novo renal transplant patients. Clin Transplant. (2013) 27(Suppl 25):16–29. doi: 10.1111/ctr.12156
22. Nashan B, Curtis J, Ponticelli C, Mourad G, Jaffe J, Haas T. Everolimus and reduced-exposure cyclosporine in de novo renal-transplant recipients: a three-year phase II, randomized, multicenter, open-label study. Transplantation. (2004) 78(9):1332–40. doi: 10.1097/01.TP.0000140486.97461.49
23. Vitko S, Tedesco H, Eris J, Pascual J, Whelchel J, Magee JC, et al. Everolimus with optimized cyclosporine dosing in renal transplant recipients: 6-month safety and efficacy results of two randomized studies. Am J Transplant. (2004) 4(4):626–35. doi: 10.1111/j.1600-6143.2004.00389.x
24. Berger SP, Sommerer C, Witzke O, Tedesco H, Chadban S, Mulgaonkar S, et al. Two-year outcomes in de novo renal transplant recipients receiving everolimus-facilitated calcineurin inhibitor reduction regimen from the TRANSFORM study. Am J Transplant. (2019) 19(11):3018–34. doi: 10.1111/ajt.15480
25. Ferreira A, Felipe C, Cristelli M, Viana L, Basso G, Stopa S, et al. Donor-specific anti-human leukocyte antigens antibodies, acute rejection, renal function, and histology in kidney transplant recipients receiving tacrolimus and everolimus. Am J Nephrol. (2017) 45(6):497–508. doi: 10.1159/000475888
26. Pascual J, Berger SP, Witzke O, Tedesco H, Mulgaonkar S, Qazi Y, et al. Everolimus with reduced calcineurin inhibitor exposure in renal transplantation. J Am Soc Nephrol. (2018) 29(7):1979–91. doi: 10.1681/ASN.2018010009
27. Hage V, Ferrandiz I, Béllière J, Esposito L, Hebral AL, Cointault O, et al. Incidence of donor-specific anti-HLA antibodies in non-HLA-sensitized patients given tacrolimus once or twice daily during the first 2 years after kidney transplant. Exp Clin Transplant. (2019) 17(3):313–9. doi: 10.6002/ect.2018.0043
28. Jarmi T, Abdelmoneim Y, Li Z, Jebrini A, Elrefaei M. Basiliximab is associated with a lower incidence of De novo donor-specific HLA antibodies in kidney transplant recipients: a single-center experience. Transpl Immunol. (2023) 77:101778. doi: 10.1016/j.trim.2022.101778
29. Bath NM, Djamali A, Parajuli S, Mandelbrot D, Leverson G, Hidalgo L, et al. Induction and donor specific antibodies in low immunologic risk kidney transplant recipients. Kidney 360. (2020) 1(12):1407–18. doi: 10.34067/KID.0000122020
30. Narumi S, Watarai Y, Goto N, Hiramitsu T, Tsujita M, Okada M, et al. Everolimus-based immunosuppression possibly suppresses mean fluorescence intensity values of de novo donor-specific antibodies after primary kidney transplantation. Transplant Proc. (2019) 51(5):1378–81. doi: 10.1016/j.transproceed.2019.03.019
31. Louis K, Loupy A, Lefaucheur C. mTOR signaling cascade: novel clinical implications in HLA and non-HLA antibody-mediated vasculopathies? Kidney Int. (2022) 101(3):451–4. doi: 10.1016/j.kint.2021.12.008
32. Salehi S, Sosa RA, Jin YP, Kageyama S, Fishbein MC, Rozengurt E, et al. Outside-in HLA class I signaling regulates ICAM-1 clustering and endothelial cell-monocyte interactions via mTOR in transplant antibody-mediated rejection. Am J Transplant. (2018) 18(5):1096–109. doi: 10.1111/ajt.14544
33. Eleftheriadis T, Pissas G, Crespo M, Filippidis G, Antoniadis N, Liakopoulos V, et al. The effect of antiHLA class I antibodies on the immunological properties of human glomerular endothelial cells and their modification by mTOR inhibition or GCN2 kinase activation. Mol Med Rep. (2021) 23(5):355–65. doi: 10.3892/mmr.2021.11994
34. Cucchiari D, Molina-Andujar A, Montagud-Marrahi E, Revuelta I, Rovira J, Ventura-Aguiar P, et al. Use of de novo mTOR inhibitors in hypersensitized kidney transplant recipients: experience from clinical practice. Transplantation. (2020) 104(8):1686–94. doi: 10.1097/TP.0000000000003021
35. Hassanein M, Augustine JJ. Chronic kidney transplant rejection. StatPearls. Treasure Island, FL: StatPearls Publishing Copyright © 2022, StatPearls Publishing LLC. (2022).
36. Eurotransplant. Available at: https://www.eurotransplant.org/allocation/allocation-of-organs/ (Cited 26 July 2022).
37. Giral M, Foucher Y, Dufay A, Duong Van Huyen JP, Renaudin K, Moreau A, et al. Pretransplant sensitization against angiotensin II type 1 receptor is a risk factor for acute rejection and graft loss. Am J Transplant. (2013) 13(10):2567–76. doi: 10.1111/ajt.12397
38. Lefaucheur C, Viglietti D, Bouatou Y, Philippe A, Pievani D, Aubert O, et al. Non-HLA agonistic anti-angiotensin II type 1 receptor antibodies induce a distinctive phenotype of antibody-mediated rejection in kidney transplant recipients. Kidney Int. (2019) 96(1):189–201. doi: 10.1016/j.kint.2019.01.030
39. Taniguchi M, Rebellato LM, Cai J, Hopfield J, Briley KP, Haisch CE, et al. Higher risk of kidney graft failure in the presence of anti-angiotensin II type-1 receptor antibodies. Am J Transplant. (2013) 13(10):2577–89. doi: 10.1111/ajt.12395
Keywords: everolimus, HLA antibodies, kidney transplant, DSA, reduced calcineurin inhibitor
Citation: Arns W, Philippe A, Ditt V, Hauser IA, Thaiss F, Sommerer C, Suwelack B, Dragun D, Hillen J, Schiedel C, Elsässer A and Nashan B (2023) Everolimus plus reduced calcineurin inhibitor prevents de novo anti-HLA antibodies and humoral rejection in kidney transplant recipients: 12-month results from the ATHENA study. Front. Transplant. 2:1264903. doi: 10.3389/frtra.2023.1264903
Received: 21 July 2023; Accepted: 5 October 2023;
Published: 27 October 2023.
Edited by:
Alessandro Alessandrini, Harvard Medical School, United StatesReviewed by:
Paul Schroder, University of Wisconsin Health, United States© 2023 Arns, Philippe, Ditt, Hauser, Thaiss, Sommerer, Suwelack, Dragun, Hillen, Schiedel, Elsässer and Nashan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wolfgang Arns d29sZmdhbmcuYXJuc0B1bmkta29lbG4uZGU= Björn Nashan YmpvZXJuLm5hc2hhbkBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.