
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Sustain. Cities , 05 March 2021
Sec. Health and Cities
Volume 3 - 2021 | https://doi.org/10.3389/frsc.2021.638278
This article is part of the Research Topic Supporting Wellbeing During and After COVID-19 in Cities View all 5 articles
 Akaninyene Otu1,2*
Akaninyene Otu1,2* Okey Okuzu3,4
Okey Okuzu3,4 Bassey Ebenso5
Bassey Ebenso5 Emmanuel Effa1,2
Emmanuel Effa1,2 Nrip Nihalani6
Nrip Nihalani6 Adebola Olayinka7Sanni Yaya8,9
Adebola Olayinka7Sanni Yaya8,9Mobile health (mhealth) tools delivered through wireless technology are emerging as effective strategies for delivering quality training, ensuring rapid clinical decision making, and monitoring implementation of simple and effective interventions in under-resourced settings. We share our early experience of developing and deploying the InStrat COVID-19 health worker training application (App) in Ogun State, Western Nigeria where the country's first COVID-19 case was reported. This App was designed to directly provide frontline health workers with accurate and up-to-date information about COVID-19; enable them to quickly identify, screen and manage COVID-19 suspects; provide guidance on specimen collection techniques and safety measures to observe within wards and quarantine centers dealing with COVID-19. The App was deployed in 271 primary health care facilities in Ogun state and a total of 311 health workers were trained to use it. Of the 123 health workers who completed knowledge pre- and post-tests, their average test score improved from 47.5 (±9.4) to 73.1(±10.0) %, P < 0.0001 after using the tutorial. Rapid adoption and uptake were driven largely by public-private sector involvement as well as certification of health workers with reported satisfaction levels of over 95% among those who completed pre- and post-test surveys. Challenges encountered included a lack of universal availability of android phones for frontline health workers, lack of internet access in remote areas and a need to incentivize the workers. The timely deployment of this App targeting primary health care workers, mostly in hard-to-reach areas, obviated the need for conventional didactic training with potential of savings in training costs and time and could be applied to similar contexts.
- Mobile health (mhealth) tools delivered through wireless technology are emerging as effective strategies for delivering quality training to health workers.
- Our rapid development and deployment of the InStrat COVID-19 health worker training application (App) in Ogun State, Western Nigeria addressed immediate response priorities and simultaneously strengthened the local health system.
- The timely deployment of this App mostly in hard-to-reach areas, obviated the need for conventional didactic training with the potential for savings in training costs and time.
- This App represents a user-friendly and low-cost approach to frontline health worker training that can be safely implemented any time during an outbreak, and could be applied to other diseases in similar contexts.
- Strong local leadership, collaborative efforts and built-in incentives such as certification of health workers can boost commitment, ownership, and sustainability of such digital technologies.
There had been widespread apprehension about Africa's capability to deal with the COVID-19 pandemic given her fragile health-care systems and scarcity of resources (Gilbert et al., 2020; Kapata et al., 2020). On Friday 28 February 2020, Nigeria, the continent's most populous country, announced sub-Saharan Africa's first confirmed case of COVID-19 identified in Ogun State, Western Nigeria (Ebenso and Otu, 2020). The rapidity of spread of COVID-19 and the ensuing social upheavals, constrained health systems across the globe, including Nigeria, from rolling out comprehensive educational programmes on COVID-19 for their frontline workers. Although the Nigeria Centre for Disease Control (NCDC) was quick to provide COVID-19 case definitions and guidelines for health workers, these materials had not been cascaded to the local level. In a bid to bridge the existing gap between the NCDC and frontline health workers, we sought to explore timely and efficient ways of disseminating credible information on COVID-19 to health workers in Ogun State Nigeria. These dissemination strategies would have to be delivered within the context of social distancing that had been adopted by the Nigerian government in response to the COVID-19 pandemic.
Health worker training remains a crucial step to controlling infectious disease pandemics such as COVID-19 as it empowers them to execute active surveillance, rapid assessment, isolation, and management of new cases. Their training needs to be synchronized with other key steps such as community engagement and contact tracing (Sacks et al., 2015). The rapidly evolving nature of pandemics is a complicating factor as transmission is constant and dynamic thereby presenting moving targets. Against this backdrop, real-time data becomes invaluable for influencing policy-making and guiding intervention development to control such pandemics. Mobile health (mHealth) has the potential to facilitate real-time patient monitoring and healthcare information delivery thereby improving heath intervention outcomes (Braun et al., 2013; Otu et al., 2016).
Advantages of using mHealth to deliver training include improved access to training materials by users in hard-to-access areas and affordability as the only requirements from the users is a smart phone and ongoing cost of internet (Otu et al., 2021). With these requirements in place, health workers could review accurate and current clinical information at their convenience on their mobile devices. Establishing mHealth interventions and infrastructure involve costs of initial software development and routine system trouble shooting but the incremental cost of cascading training to large groups of users remains minimal as these users just need to link into the existing training platform with their devices.
Numerous applications (Apps) are now available to assist health care practitioners with many important tasks, such as clinical decision-making, medical education, and training. mHealth innovations have been used to alleviate health system constraints such as limited access to training for health workers. Evidence from our setting suggest that mHealth can be effectively leveraged to bridge the gaps of distance and expertise and train frontline health workers especially during disease outbreaks.(Otu et al., 2016). Within days of the confirmation of Nigeria's index COVID-19 case in Ogun State Nigeria, InStrat Global Health Solutions (an indigenous technology company) worked with Plus91 Technologies to deploy an Android InStrat COVID-19 health worker training App in Ogun State. This App contained a tutorial for training health workers on the background, identification, and management of COVID-19 cases. The InStrat COVID-19 Mobile App was deployed in primary health care (PHC) facilities in Ogun State and ultimately to all clinical health workers in the State with high adoption rates (The Guardian, 2020). This article describes our experiences including the processes, challenges, and lessons learned during and following the deployment of the InStrat COVID-19 Mobile App in response to the pandemic in Ogun State Nigeria.
Ogun State is located in Southwestern part of Nigeria (Figure 1) and has a total population of 3,751,140 residents from the 2006 population census [National Population Commission (NPC). Federal Republic of Nigeria, 2006]. With a landmass of 16,980.55 km2 and a total of 1,520 health facilities across 20 local government areas (LGAs), the government was still grappling with the task of educating and equipping its frontline health workers with knowledge and skills to contain the outbreak when the index case was identified. Of the 1,520 health facilities in the state, 90% (1,373) are PHC facilities in remote locations, 144 are secondary health care facilities and 3 are tertiary health care facilities located in urban areas. Thus, majority of the health workers in Ogun State are based in difficult-to-reach locations which poses logistical challenges to the organization of didactic residential-type training courses.
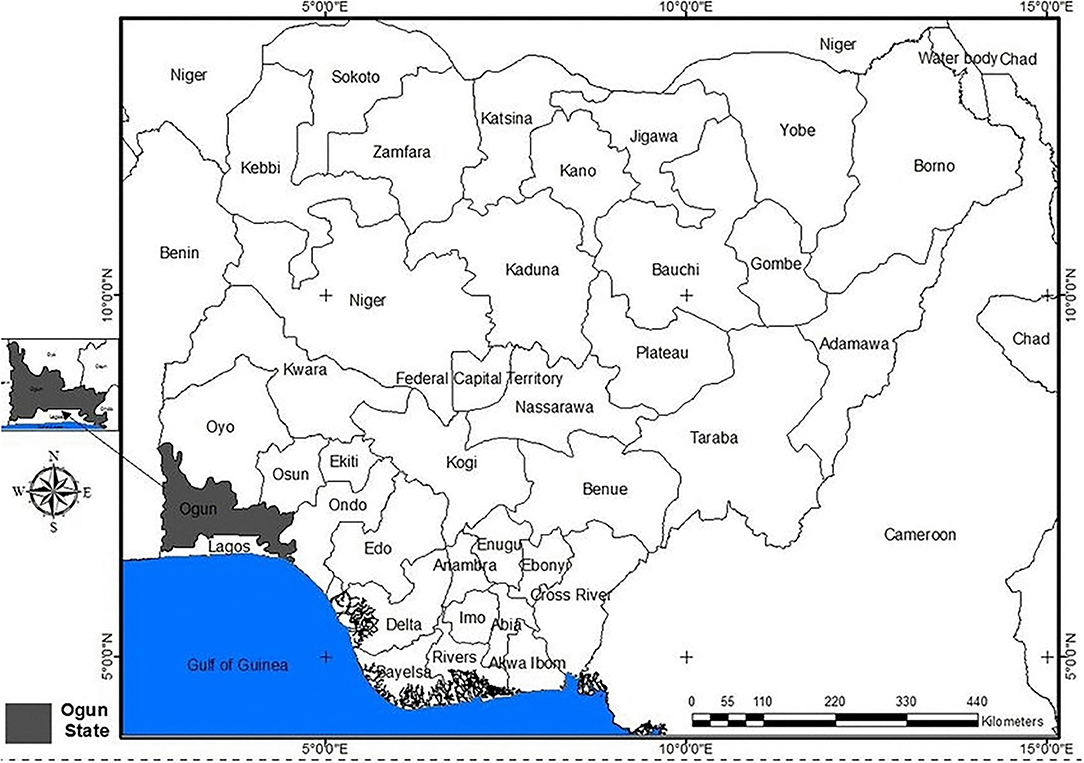
Figure 1. Map of Nigeria showing the boundary of Ogun State, other States and neighboring countries (Source: Ogun State, Ministry of Land and Housing, 2017).
Following confirmation of Nigeria's index COVID-19 Case in Ogun State, the State Government worked with InStrat and Plus91 Technologies to co-design and deploy the InStrat COVID-19 Mobile App (see Figure 2) between March 3 and April 12, 2020.

Figure 2. An android phone showing the homepage of the InStrat COVID-19 Mobile App.
The COVID-19 Mobile tutorial App was built using the MediXcel Lite health technology platform and was designed to:
• Directly provide health workers accurate and regularly updated information about the novel Coronavirus disease.
• Enable front line health workers, epidemic response officers, and strategic personnel to rapidly identify, screen, and manage persons suspected to have COVID-19.
• Train health workers on specimen collection techniques and safety measures to observe within wards and quarantine centers dealing with COVID-19.
Key features that informed deployment of the InStrat COVID-19 tutorial via the MediXcel Lite Health Technology platform were:
• Its ability to support rapid development and deployment of healthcare Apps.
• Its network independent nature which enabled deployment in regions without internet connectivity.
• Its integrated reporting portal promotes tracking, analysis, visualization, and reporting of App usage.
• Encryption of data interaction between the App and the reporting portal.
The App design was built to accommodate people with low literacy levels by incorporating user interaction prompts. MediXcel Lite Technology's web-based online, real-time reporting platform facilitated the generation, analysis, and reporting of data including gender of users; number of registered users; health worker cadre, the extent of App usage by workers and user satisfaction survey results.
The InStrat COVID-19 tutorial App was designed to run on an Android Operating System. Prior InStrat surveys revealed that every health facility in urban areas of Ogun State had three to five Android resident smart phones and that all health workers had access to Android devices.
InStrat worked with Foundation for Healthcare Innovation and Development (FHIND) to develop the tutorial content which was originally created in English and then translated to Nigeria's three major dialects: Hausa, Igbo, and Yoruba (see Figure 3). The COVID-19 content for the tutorial was drawn from the NCDC; the US Center for Disease Control; the World Health Organization (WHO); and Johns Hopkins University, United States of America. The content was reviewed and edited by Adebola Olayinka, a Professor of Clinical Microbiology and Technical Officer, WHO. Tutorial topics (see Figure 3) covered by the App included:
• Description and origin of the novel coronavirus.
• Signs and symptoms of COVID-19.
• Risk factors for contracting COVID-19.
• Precautions against COVID-19.
• Specimen collection and management guidelines.
• A WHO COVID-19 tutorial video to provide additional background information for health workers.
• Official NCDC daily COVID-19 updates and case summaries.
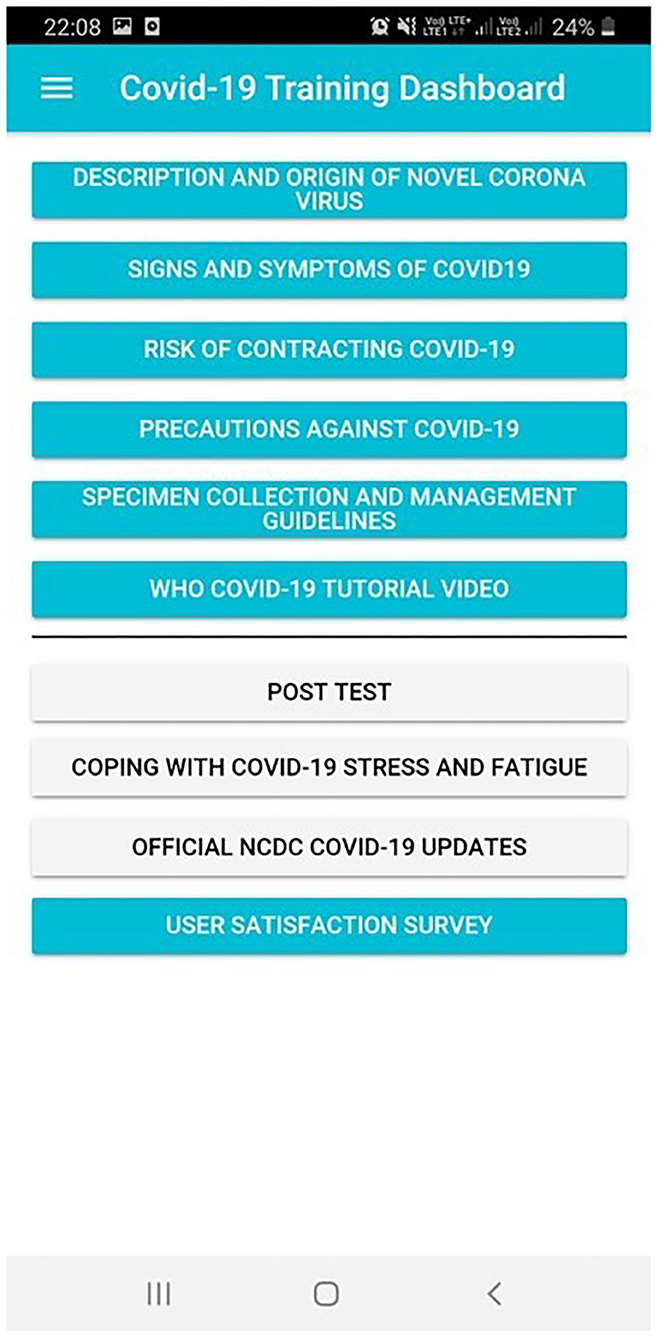
Figure 3. Screenshot showing the InStrat COVID-19 Mobile App® training dashboard.
Extensive user acceptance testing of the InStrat COVID-19 tutorial App was conducted among all levels of health workers in Ogun State prior to deployment.
Due to the rapidly evolving nature of the COVID-19 pandemic, the content within the App was regularly updated as MediXcel Lite's sync capability accommodated these updates. The official daily data updates from the NCDC were made available within the App in English and the local languages (see Figure 4). The training modules were also updated weekly in tune with the current guidelines from the WHO and the NCDC.
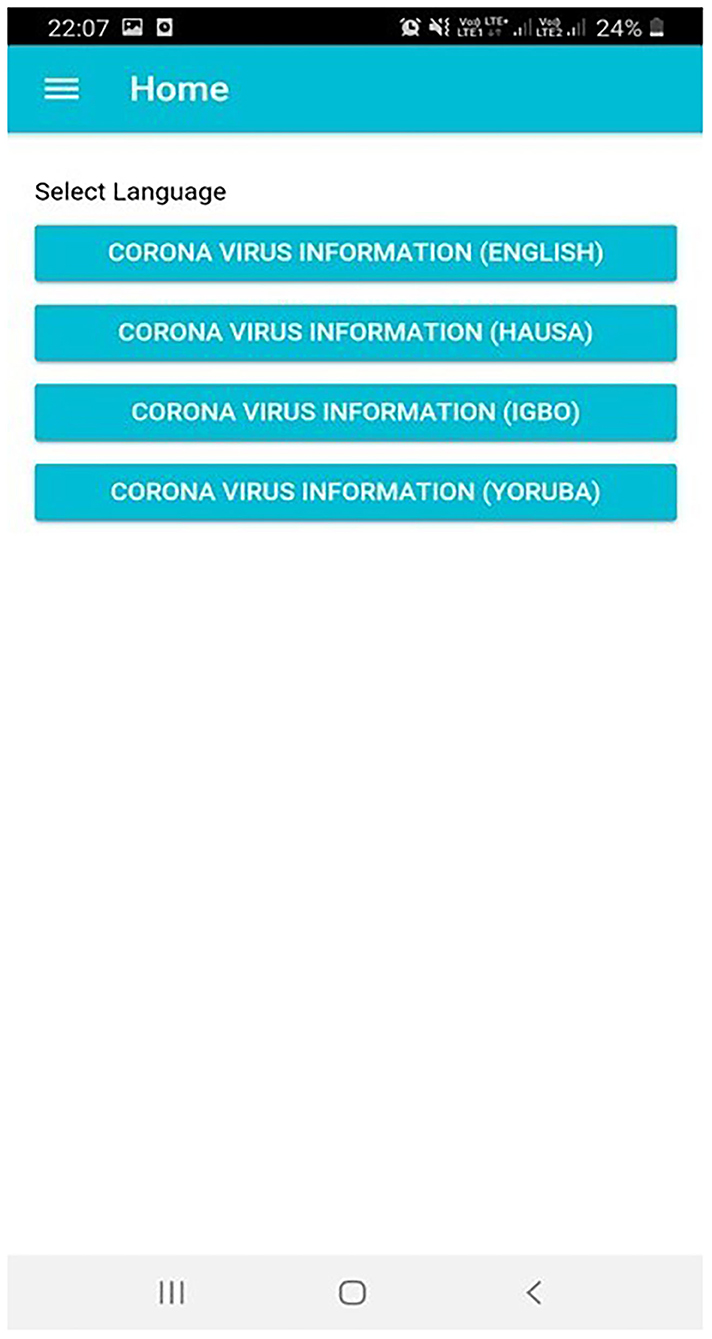
Figure 4. Screenshot of the InStrat COVID-19 Mobile App showing the various language options available.
Users of the tutorial were provided with login authorization to access the App. Users were encouraged to complete a multiple choice pre-and post-tutorial evaluation consisting of 10 questions to assess for changes in knowledge. The post-tutorial test (“post-test”) questions were the same as the pre-test questions. The deployment approach was as follows:
• InStrat provided a downloadable link for the App to Ogun State Primary Health Board (OSPHB) officers who maintain State health worker staff WhatsApp communication groups.
• The OSPHB officers sent the downloadable link for the App and use instructions to health workers through the WhatsApp groups.
• InStrat provided bi-weekly health worker registration details to OSPHB staff on user adoption.
• InStrat provided certificates of completion (co-signed by the Ogun State Commissioner for Health and InStrat Chief Executive Officer) to health workers that completed the tutorial.
Due to the expediency of the situation, formal sample size calculations were not applied when the App was initially deployed. The App was made available to health workers in the 21 PHCs in Ewekoro LGA, Ogun State where the index case presented. These health workers were provided with login links and they participated in the training via their mobile phones. Preliminary evaluation suggested that health workers preferred guidance on how to use the App to come from their State Government supervisors. In response to this, we worked closely with Ogun State Ministry of Health (SMOH) and OSPHB in subsequent deployments of the App to the workers. One week after the first deployment, and at the request of the Ogun SMOH, InStrat extended this App to an additional 250 PHCs in all 20 LGAs in Ogun State. We anticipated at least 1 health worker per facility would posses a mobile phone, so our minimum sample size was 250 persons, and we increased this to 300 health workers for both rural and urban LGAs to compensate for a 20% non-response rate.
All the data collected in this study remained completely anonymous and confidential. No unnecessary personal identifiers were recorded or requested from the users. Assurance was provided to all users that their data would remain anonymous and they were permitted to leave the study at any point.
Pre- and post-tests results were obtained from the users and analyzed using Stata 14. The Shapiro-Wilk test and Levene's test were used to test for normality and homogeneity of variance of the pre-test and post-test scores. The average pre-test and post-test scores were obtained and a paired t-test was conducted to identify statistically significant differences in the mean pre-and post-test scores.
A total of 29 health workers were trained across 21 PHCs in Ewekoro LGA on the use of this App. Twenty-four (82.8%) of the workers were female. The workers consisted of 19 (65.6%) Community Health Extension Workers (CHEWs); 5 (17.2%) nurses and 5 (17.2%) medical records officers. One week later, at the request of the Ogun SMOH, InStrat extended this App to an additional 250 PHCs in all 20 LGAs in Ogun State. A total of 282 health workers took the pre-test in the second phase of the rollout; of these 178 (63%) were female. Those trained in the second phase consisted of 206 (73%) CHEWs; 53 (18.8%) nurses; 12 (5.8%) medical records officers; 3 (1.4%) community health officers and 3 (1.4%) laboratory scientists. Five people (1.7%) did not provide their cadre.
The average pre-test score was 47.5(±9.4) % and the average post-test score was 73.1(±10.0) % with 95% confidence interval −27.9 to −23.3; a paired t-test was conducted on the pre-and post-test scores and the difference was extremely statistically significant with two-tailed P-value of < 0.0001.
An optional user satisfaction survey was conducted to obtain feedback from health workers on the App. This was a subjective assessment of user experience with the technical functioning and design elements of the App such as ease of installation, logins, accessing courses, completing tests, and receiving reports. The satisfaction extended to include the ease of navigation as the App was designed to prompt users on next action steps by presenting action selection options. The survey question and answer options were as follows:
“How Satisfied are you with the InStrat COVID-19 App (Select One): Very Satisfied; Satisfied; Neutral; Not so Satisfied; Very Unsatisfied”
A total of 72 users who completed the post-test took this satisfaction survey. Ninety-seven percentage of the 72 users expressed being satisfied or more with the App; 41 (58%) were very satisfied; 29 (40%) were satisfied; 1 was neutral; and 1 was very unsatisfied with the App. Satisfaction here referred to how well the App had been able to provide timely and reliable information on COVID-19 thus enabling rapid diagnosis and management of patients with the infection. Perceived benefits of App by government officials included.
• The rapid deployment of the App (within days of confirmation of the index case) which inspired health workers to take the novel Coronavirus disease seriously—even in the early stages.
• Easy access to government approved up-to-date information and guidelines on COVID-19.
Feedback from health workers highlighted the need for additional information on specific issues such as:
• Why COVID-19 is so easily transmissible.
• Why there is no therapeutic cure or vaccination for COVID-19.
• Lack of global coordination by world leaders—especially since the risk was obvious from the China experience.
• Reasons for ongoing low COVID-19 testing rates in Nigeria.
• Impact of the ensuing recession on the State, national, and global economies.
• Absence of proper sensitization channels especially for people in semi-rural and rural areas.
• Continued reluctance, resistance and apathy by some States in Nigeria to adopt this mHealth solution despite it being free for all users.
• Reasons for the minimal involvement of the private sector (laboratories especially) in COVID-19 testing.
This mHealth intervention has demonstrated the successful deployment of a COVID-19 tutorial App in 271 PHC care facilities in Ogun State for training of 311 frontline health workers. Statistically significant average knowledge test score improvements from 47.5(±9.4) to 73.1(±10.0) % were recorded among the 123 health workers who completed knowledge pre- and post-tests with reported satisfaction levels of over 95% We acknowledge that these improvements in the test score does not necessarily translate to improvement in skills of the health workers. Our intervention was not designed to evaluate improvement in skills of these workers. However, there is evidence to suggest that effective knowledge dissemination of right material to underpin policy, service, and practice can result in clinical practice and service improvements (Brownson et al., 2018; Eljiz et al., 2020). Healthcare worker training is a vital step in disease control but health workforce training is currently threatened by misinformation promoted by sources such as the internet and social media (Brennen et al., 2010). In the context of a fast-evolving pandemic such as COVID-19 where community spread is a key factor, an equally rapid response is essential for disease control especially at primary care level.
Mobile devices are reshaping healthcare in Africa, leading to rapid growth in the development of medical software Apps. The mobile phone subscription within Nigeria is projected to be as high as 180 million with phone penetration (tele density) being as high as 95% (Industry Statistics, 2021). With the estimated number of 25–40 million smartphone users in Nigeria (O'Dea, 2020), the potential to leverage smartphones for healthcare information delivery to remote locations is promising. The deployment of educational and clinical decision-making tools via mobile telephones can facilitate the efficient triage of suspects presenting at PHC facilities. Such a system can ensure that all assessed patients are directed to the right care first time. In the current COVID-19 pandemic, mHealth tools would facilitate the exclusion of more common medical conditions with overlapping symptoms (such as fever and cough) and provide actions to be taken if the case definition for COVID-19 is met.
This process revealed two important lessons for policy and practice. First, that regular training and continuous technical support are invaluable determinants of success of disease control and digital technological interventions. Second, that certification of health workers is a major driver of the adoption of training initiatives. At the beginning of the intervention, there was some apathy among the health workers toward the training. However, increased SMOH supervision and the issuance of certificates of completion appeared to be strong motivating factors. We witnessed a 30% increase in enrolment 24 h after the first batch of certificates were issued to health workers who completed the training. We also discovered that we were able to leverage existing relationships to cut through major bureaucratic red tape given InStrat's track record of dealing with similar outbreaks in Nigeria such as Ebola (Otu et al., 2016), Lassa fever and a methanol poisoning incident amongst others.
This intervention could be applied in other developing country settings where smart phone penetration is equally high. Africa is recording phenomenal growth in the smartphone space which appears to be largely driven by the huge influx of affordable models that have recently been launched in these markets. In 2019, smartphone sales in Africa constituted 6.6% of the global smartphone market, compared with 6.3% in 2018 and 5.9% in 2017, according to International Data Corporation (IDC) (FDI Intelligence, 2021). This holds promise for the use of an App such as ours to train frontline health workers in such settings. Extensive training and supportive supervision will be crucial especially for users who may not be so technologically inclined.
We identified several challenges in the process of rolling out this intervention. First, the App was exclusively available on Android OS as we were unable to make the App available on Google Play store. This was due to temporary delays as Google had prioritized critical services and temporarily reduced its staff strength in response the COVID-19 situation. Second, we found a lack of access to Android devices among some health workers in rural areas of Ogun State. InStrat is working with Plus91 to develop a new version of the App that will allow multiple user registrations on the COVID-19 App and enable health workers to share their devices and overcome this challenge. Third, there was a limited storage space to run the COVID-19 App on the mobile devices of some of the health workers. InStrat staff had to provide instructions to users on how to create space on their devices by deleting unused/seldom used Apps and old media files. Fourth, we found a dearth of internet facilities particularly in the more remote locations. InStrat staff tried to mitigate this by convening central training sessions, during which content (and updates) was transferred directly from laptops on to devices.
In conclusion, our intervention has demonstrated the utility of mHealth innovations that rely on private-public sector collaborations in supporting the response to complex disease outbreaks such as COVID-19. Investment in mHealth could improve health security in low-middle income country settings whilst facilitating outbreak response. Given the fragility of Nigeria's present health system, the COVID-19 training App presents an opportunity to cascade vital training to health workers and mitigate community transmission of COVID-19. Arising from our experiences, effective deployment of technology for disease surveillance and risk management requires strong local leadership. This needs to be combined with a comprehensive private public partnership approach to guarantee commitment, ownership, and sustainability.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation if required.
This intervention involving human participants was reviewed and received ethical approval from the National Health Research Ethics Committee of Nigeria (NHREC) number NHREC/01/01/2007. The participants provided written informed consent to participate in this project.
AO, OO, AdO, and EE conceived the project. AO, OO, NN, AdO, EE, and BE were involved in implementation of the project. AO, OO, EE, NN, BE, and SY were involved in the data analysis. All authors discussed the results and contributed to the final manuscript.
OO is employed by InStrat Limited Liability Company, Montclair, NJ USA. InStrat LLC, Montclair, NJ USA. NN is employed by Plus91 Technologies Pvt Ltd., Pune, India.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to acknowledge the invaluable contributions of following persons to the success of this intervention: Prince Dapo Abiodun MFR the Governor of Ogun State; Dr. Tomi Coker the Commissioner for Health Ogun State and Dr. A. E. Ogunsola, Executive Secretary Ogun State Primary Healthcare Board. Their support for our project and dedication to service of the Ogun State people was outstanding.
Braun, R., Catalani, C., Wimbush, J., and Israelski, D. (2013). Community health workers and mobile technology: a systematic review of the literature. PLoS ONE 8:e65772. doi: 10.1371/journal.pone.0065772
Brennen, S., Simon, F. M., Howard, P. N., and Nielsen, R. K. (2010). Types, Sources, and Claims of COVID-19 Misinformation. Reuters Institute for the Study of Journalism. Available online at: https://reutersinstitute.politics.ox.ac.uk/types-sources-and-claims-covid-19-misinformation (accessed 9 November, 2020).
Brownson, R. C., Eyler, A. A., Harris, J. K., Moore, J. B., and Tabak, R. G. (2018). Getting the word out: new approaches for disseminating public health science. J. Public Health Manage. Pract. (2018) 24, 102–111. doi: 10.1097/PHH.0000000000000673
Ebenso, B., and Otu, A. (2020). Can Nigeria contain the COVID-19 outbreak using lessons from recent epidemics? Lancet Glob. Health. 8:e770. doi: 10.1016/S2214-109X(20)30101-7
Eljiz, K., Greenfield, D., Hogden, A., Taylor, R., Siddiqui, N., Agaliotis, M., et al. (2020). Improving knowledge translation for increased engagement and impact in healthcare. BMJ Open Qual. 9:e000983. doi: 10.1136/bmjoq-2020-000983
FDI Intelligence (2021). Will Mobile Phone Penetration Maintain African Momentum? Available online at: https://www.fdiintelligence.com/article/76565 (accessed January 27, 2021)
Gilbert, M., Pullano, G., Pinotti, F., Valdano, E., Poletto, C, Boëll, P.-Y., et al. (2020). Preparedness and vulnerability of African countries against importations of COVID-19: a modelling study. Lancet 395, 871–877. doi: 10.1016/S0140-6736(20)30411-6
Industry Statistics (2021). Available online at: https://www.ncc.gov.ng/stakeholder/statistics-reports/industry-overview#view-graphs-tables (accessed January 27, 2021)
Kapata, N., Ihekweazu, C., Ntoumi, F., Raji, T., Chanda-Kapata, P., Mwaba, P., et al. (2020). Is Africa prepared for tackling the COVID-19 (SARS-CoV-2) epidemic. lessons from past outbreaks, ongoing Pan-African public health efforts, and implications for the future. Int. J. Infect. Dis. 93, 233–236. doi: 10.1016/j.ijid.2020.02.049
National Population Commission (NPC). Federal Republic of Nigeria (2006). Population and Housing Census, Priority Table Volume IV, Population Distribution by Age and Sex. Abuja: National Population Commission (NPC).
O'Dea, S. (2020). Number of smartphone users in Nigeria from 2014 to 2025 (in millions). Statistica. Available online at: https://www.statista.com/statistics/467187/forecast-of-smartphone-users-in-nigeria/. (accessed 9 November, 2020).
Otu, A., Ebenso, B., Okuzu, O., and Osifo-Dawodu, E. (2016). Using a mHealth tutorial application to change knowledge and attitude of frontline health workers to Ebola virus disease in Nigeria: a before-and-after study. Hum. Resour. Health 14:5. doi: 10.1186/s12960-016-0100-4
Otu, A., Ukpeh, I., Okuzu, O., and Yaya, S. (2021). Leveraging mobile health applications to improve sexual and reproductive health services in Nigeria: implications for practice and policy. Reprod. Health 18:21. doi: 10.1186/s12978-021-01069-z
Sacks, J. A., Zehe, E., Redick, C., Bah, A., Cowger, K., Camara, M., et al. (2015). Introduction of mobile health tools to support ebola surveillance and contact tracing in Guinea. Glob. Health Sci. Pract. 3, 646–659. doi: 10.9745/GHSP-D-15-00207
The Guardian (2020, March 4). Coronavirus. Ogun government launches mobile app for health workers. The Guardian [newspaper on the Internet]. Available online at: https://guardian.ng/news/coronavirus-ogungovernment-launches-mobile-app-for-health-workers/ (accessed November 9, 2020)
Keywords: mobile health, health workers, training, COVID-19, Ogun State
Citation: Otu A, Okuzu O, Ebenso B, Effa E, Nihalani N, Olayinka A and Yaya S (2021) Introduction of Mobile Health Tools to Support COVID-19 Training and Surveillance in Ogun State Nigeria. Front. Sustain. Cities 3:638278. doi: 10.3389/frsc.2021.638278
Received: 05 December 2020; Accepted: 05 February 2021;
Published: 05 March 2021.
Edited by:
Ruoyu Wang, University of Edinburgh, United KingdomReviewed by:
Dongsheng He, University of Cambridge, United KingdomCopyright © 2021 Otu, Okuzu, Ebenso, Effa, Nihalani, Olayinka and Yaya. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Akaninyene Otu, YWthbm90dUB5YWhvby5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.