 Manisha Gupta
Manisha Gupta Souvik Bandyopadhyay
Souvik Bandyopadhyay- 1Independent Systematic Reviewer - Transport, New Delhi, India
- 2GlaxoSmithKline Asia Pvt. Ltd., Bangalore, India
Low- and middle-income countries have the highest proportions of road accident fatalities among vulnerable road users. This review established the effectiveness of road engineering and the enforcement of traffic laws, and regulation interventions to prevent injury (fatal and non-fatal) to vulnerable road users from low- and middle-income countries. We searched the following databases up to Jan 04, 2018: PubMed; OvidSP Medline, OvidSP Embase, OvidSP Transport, Cochrane Injuries Group Specialized Register, Cochrane Central Register of Controlled Trials, and Proquest ERIC database. In addition, road safety organizations' databases and conference proceedings were hand searched to Jan 2018. Twenty-eight studies were matched to the study inclusion criteria of which we did not analyze six studies assessed as C grade for risk-of-bias. We estimated the effect-size of 18 studies. Four of the studies presented a unique outcome or a study design; it was not possible to calculate a standardized effect-size. The risk-of-bias rating of the studies included for effect-size analysis ranged between A and B grade. There was no evidence that road engineering interventions were effective for road traffic death counts, the number of injuries, and road accident casualty outcomes. While the enforcement of mandatory helmet law was ineffective in reducing road traffic death counts, intervention efforts proved effective in decreasing injuries. Enforcement of mandatory helmet law, automated-enforcement-system (camera), and pedestrian signal interventions were effective in increasing road users' compliance with road safety laws. Daytime running-headlight intervention reduced the number of road accident casualties. The quality of evidence for outcomes was ranked very low. Further research is needed to examine the effects of road engineering interventions on injury severity outcomes. Even though the evidence was of very low quality, traffic laws, and regulation interventions when combined with enforcement initiatives or with, other approaches proved effective in changing drivers' behaviors. Research on road engineering interventions combined with automated-enforcement-systems must be explored in an Low- and Middle-Income Country (LMIC) setting. The review found evidence gaps on the effects of segregation of vulnerable road users from motorized vehicles, changes in intersections, and bicycle infrastructure interventions.
Introduction
The UN Decade of Action for Road Safety 2011–2020 Sustainable Development Goals aimed to reduce road traffic deaths by 50% by 2020. While it has made some progress, the number of road traffic deaths and injuries remains high (World Health Organization, 2018). About half of the world's road traffic deaths occur among motorcyclists (23%), pedestrians (22%), and cyclists (5%) also known as “vulnerable road users” (World Health Organization, 2018). Road traffic deaths among vulnerable road users are a major public health problem in low- and middle-income countries (LMICs) where walking, cycling, and motorcycling are predominant transport modes. Pedestrians and cyclists were the largest group of victims of road fatalities in Bangladesh, at 44% (World Health Organization, 2013). In India, 78 and 53% of those killed on the roads in Mumbai and Delhi respectively were pedestrians (Mohan et al., 2009). Some studies have placed pedestrian fatalities in Mexico as high as 48% (Bartels et al., 2010). In Nairobi, Kenya, vulnerable road users accounted for 54% of all road fatalities (Kim and Dumitrescu, 2010). Pedestrians accounted for 43% of all road traffic fatalities in Ghana (World Health Organization, 2013).
Research has shown that traffic speed measures are essential to prevent road injuries among vulnerable road users (Elvik, 2001; Allsop, 2010; Wilson et al., 2010). Bicycle infrastructure reduces injury risks (Reynolds et al., 2009; Lusk et al., 2011; Harris et al., 2013), while regulatory and legislative interventions play a significant role in lessening the severity of injuries (Redelmeirier et al., 2003; Chisholm, 2008; Blanco et al., 2017). Although many LMICs have implemented road safety strategies, compliance and law enforcement are often limited. The common challenges for preventing road traffic injuries among vulnerable road users in LMICs include mixed road conditions, negative perceptions of road safety among non-motorized road users, non-use of helmets or use of non-standard helmets, alcohol, and speed (Vasconcellos, 2001; Nantulya and Reich, 2003). The new regulatory approach called the safe system approach, which focuses on the institutional level deployment of large-scale safety interventions, had a positive effect on road safety in high-income countries. Political will, leadership, active public sector participation, and full support of the private sector and civil societies are considered vital to move in the direction of a safe system approach (ITRAC, 2008; Wegman, 2017). From a public health perspective, the safe system approach framework has several benefits for examining key risk factors for vulnerable road users in LMICs. For instance, two-wheelers are used as the primary mode of transport in many LMICs. Research (International Transport Forum, 2015) shows that the mean age of motorcycle crash victims in LMICs is 25. Other studies have found that the chances of young motorcycle crash victims in the 17–19 years age group from a lower-income group is 2.5 times greater than their peers in higher socioeconomic groups (Huang and Lai, 2011; de Vasconcellos, 2013; International Transport Forum, 2015). The loss of life or disability causes a big economic burden on individuals and households from poorer backgrounds and has a direct negative effect on the national economy.
Nevertheless, institutional level reforms for road safety have received little attention in LMICs. Major barriers include under-reporting of road crash data as well as limited amount of disaggregated data on road crash fatalities, injuries and intermediate outcomes in crash databases, a lack of technical expertise, and a lack of coordination between agencies responsible for road safety management and amongst different levels of governments (International Transport Forum, 2016).
In the light of increasing road traffic deaths and low levels of public investments in road safety measures, international agencies began getting involved in improving road safety conditions in LMICs during the 1990's. World Bank's Global Road Safety Partnership (1999), World Bank's Global Road Safety Facility (2006), Bloomberg Philanthropies “Road Safety in 10 Countries Project—RS-10” (2009), and the United Nations General Assembly Resolution “Decade of Action for Road Safety (2011 to 2020)” (2011) aimed to implement road safety measures in collaboration with national stakeholders, non-governmental organizations, and academic institutions of LMICs. Because of increased sensitization of local and civic organizations, the establishment of national coordinating committees and road safety programs, and some improvements in systems for data collection and analysis, successful road safety intervention implementation practices have emerged (Bishai and Hyder, 2006; Esperato et al., 2012; Commission for Global Road Safety, 2013).
Published reviews on the effects of road infrastructure interventions have focused on interventions for road users in high-income settings (Perel et al., 2007). The lack of studies on road safety from LMICs in systematic reviews could be because of the focus on stand-alone road infrastructure interventions and inclusion criteria to include high-quality study designs only. Furthermore, many of the interventions examined in high-income settings are developed after considerable research and testing. In LMICs, the challenge is to transfer the knowledge gained in developed countries in a fraction of the time. In addition, the interventions need to be tested for cost and design effectiveness as well as the legal system for implementing road infrastructure interventions need to be developed to similar standards practiced in developed countries. LMICs should avoid repeating studies showing the effectiveness of road safety measures in high-income country settings because of contextual differences (Wegman, 2017).
In this context, a review of the evidence of road infrastructure interventions was conducted to provide a quantification of the effects of road safety interventions in LMICs. The review focused on the LMIC context, not the sophistication of the intervention. The findings of this review provide valuable, and contextually relevant, data for road safety policy making in LMIC settings.
The purpose of this review was to measure the effects of road engineering and enforcement of traffic laws and regulation interventions for the prevention of injury (fatal and non-fatal) to vulnerable (non-motorized and motorized two-wheel) road users in low- and middle-income countries. This review included randomized controlled trials and non-randomized study designs and the comparator was no intervention.
Methods
We reported this systematic review under the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) Statement (Moher et al., 2009) (Table S1). The protocol of the review was published in the Cochrane Database of Systematic Reviews (Gupta et al., 2015).
Types of Studies
The review included randomized-controlled-trials (RCT) and non-randomized study designs: controlled before-and-after, uncontrolled before-and-after, interrupted time-series (ITS), and case-control.
Included studies compared changes in outcomes before and after the intervention implementation with or without a control group. For ITS, studies had a defined point in time when the intervention occurred and included data at least three time-points before and three time-points after the intervention. The intervention implementation was at the population level or the individual level, or both. Participants' selection was by the outcome; hence, outcome reporting was at the individual level.
This review did not include black spot identification studies and modeling studies.
Types of Participants
In this review, “vulnerable road users” included all vulnerable road users —pedestrians, those using non-motorized means of transport (NMT), and those using motorized two-wheelers (motorcycles, mopeds, and light mopeds) inclusive of all ages in LMICs. The World Bank definition of NMT (World Bank, 1993) defines “vulnerable road user” by the amount of protection they have from other motorized traffic. Pedestrians, cyclists, and riders of two-wheelers are unprotected; hence, they are referred to as “vulnerable.”
The World Bank definition of LMICs was used to classify low- and middle-income countries. As of July 1, 2018, low-income economies are those with a GNI per capita of $1005 or less; middle-income economies are those with a GNI per capita of more than $1006 but < $3,995.
Types of Interventions
Three broad categories of interventions, road engineering, enforcement of traffic laws and regulation, and a combination of road engineering, and regulatory and legislative interventions were included. Alongside this, a combination of one or more of these interventions as well as with other approaches were considered.
Road engineering interventions are preventive measures involving engineering or structural changes to the road design that affect road user behavior. Road engineering interventions covered in the review comprise three sub-categories: (1) measures for reduction in vehicle-speed, (2) changes in intersections, and (3) segregation of non-motorized road users from motorized vehicles.
Enforcement of traffic laws and regulation interventions refers to setting up road safety rules and ensuring compliance from road users through legal enforcement. Regulation interventions focused on regulatory approaches that can affect large populations through law enforcement such as speed cameras, speed limits, speed zones, red-light enforcement cameras, use of daytime running-lights for two-wheelers, mandatory helmet law, traffic signal regulation, and stop signs.
A combination of road engineering and regulatory interventions includes segregated or on-road marked bicycle lanes involving specific road changes at junctions and intersections, bus rapid transit system with motorcycle lanes, pedestrian crossing, rumble strips on bus rapid transit system, and speed limit enforcement with speed reduction measures.
Comparisons: Comparison of intervention vs. no intervention.
Types of Outcome Measures
This review studies reporting data on at least one of the following primary or secondary outcomes.
Primary Outcomes
(1) Road traffic death counts; (2) Road traffic death rates expressed as rate per 100,000 inhabitants or rate per kilometer of road year; (3) Number or proportion of severe injuries (Injury Severity Score (ISS) > 17, Glasgow Coma Scale (GCS) 9 to 12) and moderate injuries (ISS 8 to 16, GCS 3 to 8); (4) Number or proportion of road accident casualty1; and, (5) Number or proportion of disabilities (severe [Glasgow Outcome Scale (GOS) = 4) and moderate (GOS = 3)].
Secondary Outcomes
(1) Compliance; (2) Number or proportion of head-on collisions; (3) Number or proportion of rollovers; (4) Mean-vehicular-speed; and, (5) Mean cost of road crashes.
Outcome data on adverse impacts were extracted from all included studies, if available.
Search Methods for Identification of Studies
Terms describing population and interventions were combined in the final search strategy. The final draft search strategy for bibliographic databases consisted of the following combinations: “Population and Intervention,” “Population and Study type,” and “Population and Outcomes.” The search strategy was adapted for each database; for details, see search strategies for bibliographic databases (Appendix 1).
We searched the following bibliographic databases: PubMed; Ovid MEDLINE (1966–2018); EMBASE (1980–2018); ERIC (1966–2018); Cochrane Injuries Group Specialized Register; the Cochrane Central Register of Controlled Trials; TRANSPORT database [(combines records from Transport Research Information Service, International Road Research Documentation, and TRANSDOC(1980–2018)]; World Bank Impact Evaluation Working Paper Series; Poverty Impact Evaluation database; Development Impact Evaluation (DIME) Database; JOLIS Library catalog; Latin-American and Caribbean Center on Health Sciences Information (LILACS) database; global Transport Knowledge Practice (gTKP); The Institute of Transportation Studies at the University of California; Monash University Accident Research Centre; TRANweb database; and Google Scholar.
In addition, we searched the following road safety organizations' databases: Transport Research Laboratory (TRL), Australian Road Research Board (ARRB), AMEND, African Development Bank (AfDB), Asian Development Bank (ADB), The African Community Access Program (AFCAP), Crash Modification Factors Clearing House, Central Road Research Institute (CRRI), Department for International Development (DFID), International Road Assessment Program (iRAP), International Road Federation (IRF), Global Road Safety Facility (GRSF), Global Road Safety Partnership (GRSP), EMBARQ -The World Resource Institute Center for Sustainable Transport (EMBARQ), Sub-Saharan Africa Transport Policy Program (SSATP), Transport Research and Injury Prevention Program (TRIPP), Organization of Economic Cooperation and Development (OECD), Road Engineering Association of Asia and Australia (REAAA), Road Traffic Injury Research Network (RTIRN).
Further to this, we checked reference lists of selected papers and we hand-searched conference proceedings. We have considered 1990 as a cut-off for the identification of studies analyzing road infrastructure interventions.
Data Collection and Analysis
A team of two authors have screened the titles and abstracts and identified eligible studies independently. The full text of all eligible studies was obtained. Based on the study inclusion criteria, two authors conducted a full-text review for eligibility independently, and study inclusion differences were reconciled by a discussion between the two authors.
Full text of studies was screened in detail, and data from each study were extracted by one review author and checked by a second review author. Disagreements were resolved by discussion.
Where data were missing; we attempted to obtain the data from the authors. If we were unable to obtain missing data, we analyzed only the available data.
Assessment of Risk of Bias in Included Studies
The quality of all studies (RCTs and non-randomized studies) were assessed using the Hamilton Assessment Tool (HAT) (Thomas, 1998). We proposed some modifications under the “Confounding” domain of the HAT tool to ensure that it is appropriate for studies of road infrastructure interventions. Please see the Hamilton Assessment Tool (Appendix 2).
Two independent review authors assessed the quality of all studies using the HAT tool. Each component was first assigned a global rating (Strong = 1, Moderate = 2, Weak = 3) indicating the overall potential for bias in each component. Each study was assigned an overall risk of bias assessment rating. The criteria for an overall risk of bias assessment rating of a study were as follows: studies with no weak ratings were assessed as A grade, studies with one or two weak ratings were assessed as B grade. And, studies having very serious (more than two weak ratings) on study design, confounders, and data collection methods used were excluded as C grade studies. Intervention integrity and analysis domain were not included in the assessment of the overall risk of bias ratings. Disagreements in the assessment of bias were resolved through discussion between the two review authors.
Based on the HAT tool, studies assessed with low risk of bias (that is two or more studies with an overall grade of A or B) were quantitatively synthesized using meta-analysis. We excluded C grade studies from meta-analysis and narrative synthesis.
Measures of Treatment Effect
For uncontrolled before-and-after studies, we presented the dichotomous outcome data2 using Odds Ratio (OR) with 95% confidence intervals (CI). For controlled before-and-after studies, we extracted the dichotomous outcome data for treatment and control sites and calculated the ratio of the differences in event rates before and after intervention in the treatment site by a corresponding difference in the control site.
For uncontrolled before-and-after studies, we presented the continuous outcome data3 by calculating the mean difference with 95% CI. For continuous outcome data in controlled before-and-after studies, we calculated the difference in outcome data before and after intervention in the intervention site by the corresponding difference in the control site. We used mean differences (MDs) with 95% CI when the same scale was used and standardized mean differences (SMDs) with 95% CI when a different scale was used in studies. For time-series studies, we extracted the outcome data for calculating risk ratios (RR) using R software. The studies considered in this meta-analysis have road traffic death count or accident casualties as an outcome. The outcome being a count, a Poisson regression model was used to estimate the effects of intervention after adjusting for a linear trend in time.
We assessed statistical heterogeneity using the Chi2 and I2 statistics. A meta-analysis of effect sizes was conducted using a random-effects model.
Unit of Analysis
Road engineering and legislative interventions were implemented to individual roads meeting pre-specified criteria or to all roads within a targeted community or a geographical area. However, the reporting of outcomes was done at individual levels. In cases where a study had multiple intervention groups, data from all relevant intervention groups of the study were combined into a single group, and data from all relevant control groups were combined into a single control group.
Data Synthesis
For data synthesis, studies were grouped by intervention categories: road engineering, enforcement of traffic laws and regulations, and a combination of road engineering and enforcement of traffic laws and regulations. Under these categories, studies were grouped by randomized and non-randomized study designs. The data from randomized and non-randomized studies were presented by (1) primary outcomes: road traffic death counts, number of injuries (moderate and severe), and number of road accident casualty; and (2) secondary outcome: compliance.
We did not synthesize data from road infrastructure and enforcement of traffic laws and regulations intervention categories together. We reported meta-analysis results of randomized control trials and non-randomized studies separately.
If there was extreme heterogeneity, we presented the effect sizes of those studies graphically using forest plots, and a narrative synthesis of the data were presented according to the ESRC guidance (Popay et al., 2006). All the data to be synthesized were predominantly quantitative; we found vote counting and developing a common rubric the most relevant for the synthesis at hand. The vote counting and a common rubric were developed by using two approaches: (1) using a tick mark where the effect of the intervention was positive and overall statistical significance, and (2) analyzing absolute measure of effect. Two software packages were used for meta-analysis. The RevMan was used for uncontrolled before-and-after and controlled before-and-after studies. Effect sizes for time-series studies were computed using R Statistical Software (Appendix 3) because RevMan is not suitable for meta-analyzing data for time-series studies.
Sensitivity Analysis
Before making decisions about which studies should be included in the final syntheses, a sensitivity analysis was conducted to examine variation in reported effects by study characteristics. The key study characteristics used for sensitivity analysis were: in between-study heterogeneity, missing data, and the overall study quality grade assigned.
We considered a sensitivity analysis about the influence of small study effects on the result of the meta-analysis when there was evidence of between-study heterogeneity. We compared the fixed and random-effects estimates of the intervention effect. We performed a sensitivity analysis by excluding studies of the lowest quality.
We examined funnel plots and cumulative meta-analysis to assess the potential for publication bias in the included studies.
GRADE and summary of findings tables
A team of two authors was involved in conducting GRADE assessments. GRADE domains, risk-of-bias, indirectness, inconsistency, imprecision of results were primarily considered for assessing the quality of evidence.
Patient and Public Involvement
The review did not involve any patients or the public.
Results
Results of Search
The systematic search was conducted in January 2018. We identified 30,030 study records through database searching. Twenty-eight studies matched the study inclusion criteria; the search flow chart (Figure 1) details the search process.
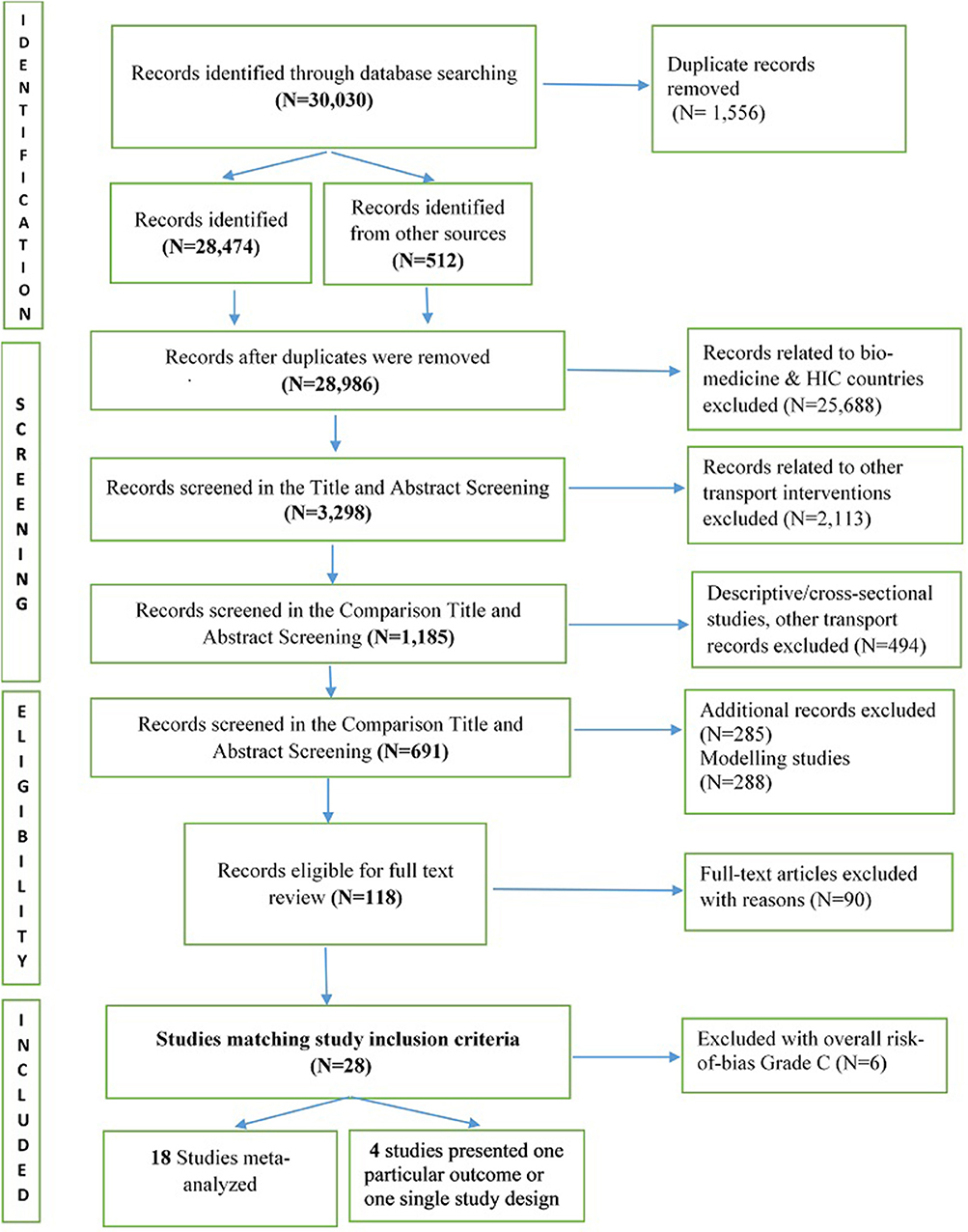
Figure 1. Search flow chart.
Included Studies
Twenty-eight studies matching study inclusion criteria were identified. Twenty-two studies were included for analysis and six studies were not analyzed because the outcome data did not qualify for analysis (Figure 1).
Study Characteristics
Notably, 21 studies belonged to middle-income countries and one study belonged to low-income countries.
Study designs included one cluster randomized-control-trial (Sumner et al., 2014), one case-control (Quistberg et al., 2014), one controlled before-and-after (Liu et al., 2011), five time-series (Radin Umar et al., 1995a,b; Radin Umar, 2005; Espitia-Hardeman et al., 2008; Nadesan-Reddy and Knight, 2013) and 14 uncontrolled before-and-after studies (Panichaphongse et al., 1995; Chiu et al., 2000; Liberatti et al., 2001; Afukaar, 2003; Ichikawa et al., 2003; Bastos et al., 2005; Hoque et al., 2005; Bhatti et al., 2011; Antic et al., 2013; Lipovac et al., 2013; Nguyen Ha et al., 2013; Allyana et al., 2014; Van der Horst et al., 2016; Nhan et al., 2017).
There were seven studies on the impact of road engineering interventions (Radin Umar et al., 1995b; Afukaar, 2003; Hoque et al., 2005; Liu et al., 2011; Antic et al., 2013; Nadesan-Reddy and Knight, 2013; Van der Horst et al., 2016). Fourteen studies reported the impact of enforcement of traffic laws and regulation interventions (Panichaphongse et al., 1995; Radin Umar et al., 1995a; Chiu et al., 2000; Liberatti et al., 2001; Ichikawa et al., 2003; Bastos et al., 2005; Radin Umar, 2005; Espitia-Hardeman et al., 2008; Bhatti et al., 2011; Lipovac et al., 2013; Nguyen Ha et al., 2013; Allyana et al., 2014; Sumner et al., 2014; Nhan et al., 2017).
In addition, one study (Quistberg et al., 2014) included a combination of regulatory and road engineering interventions.
All studies examined one or more of the primary or secondary outcomes. Some studies reported only primary outcome measures: road traffic death counts, the number of injuries (moderate and severe), and the number of road accident casualty. Some studies reported only secondary outcome measures: compliance and mean-vehicular-speed.
One study (Allyana et al., 2014) presented outcome data for two sub-categories of enforcement of traffic laws and regulation interventions separately. Outcome data were extracted and assessed as they related to the sub-category automated-enforcement-system (camera)—red-light regulation into one group, and as they related to the sub-category automated-enforcement-system (camera)—speed limit into another group.
One study (Hoque et al., 2005) evaluated controlled before-and-after analysis of safety improvements at three black spots, and before-and-after analysis of road engineering safety measures at two different site segments. Outcome data were extracted and assessed for the before-and-after analysis of road engineering safety measures only.
Included studies did not report the following primary and secondary outcome measures: moderate and severe disabilities (primary outcomes), the number, or proportion of rollovers, and mean cost of road crashes (secondary outcomes).
One study (Espitia-Hardeman et al., 2008) reported the outcome, the number of road traffic death rates expressed as the rate per 100,000 inhabitants. One before-and-after study (Afukaar, 2003), one case-control study (Quistberg et al., 2014), and one time-series study (Radin Umar et al., 1995b) reported the number of head-on collisions. One study (Nadesan-Reddy and Knight, 2013) reported pre-specified adverse outcome, increase in the collision between motor vehicles because of traffic calming measure speed humps. Because of an insufficient number of studies, we did not meta-analyze these outcome results.
For characteristics and the role of the funding source of studies analyzed, see the summary table of characteristics of studies included for meta-analysis (Table 1).
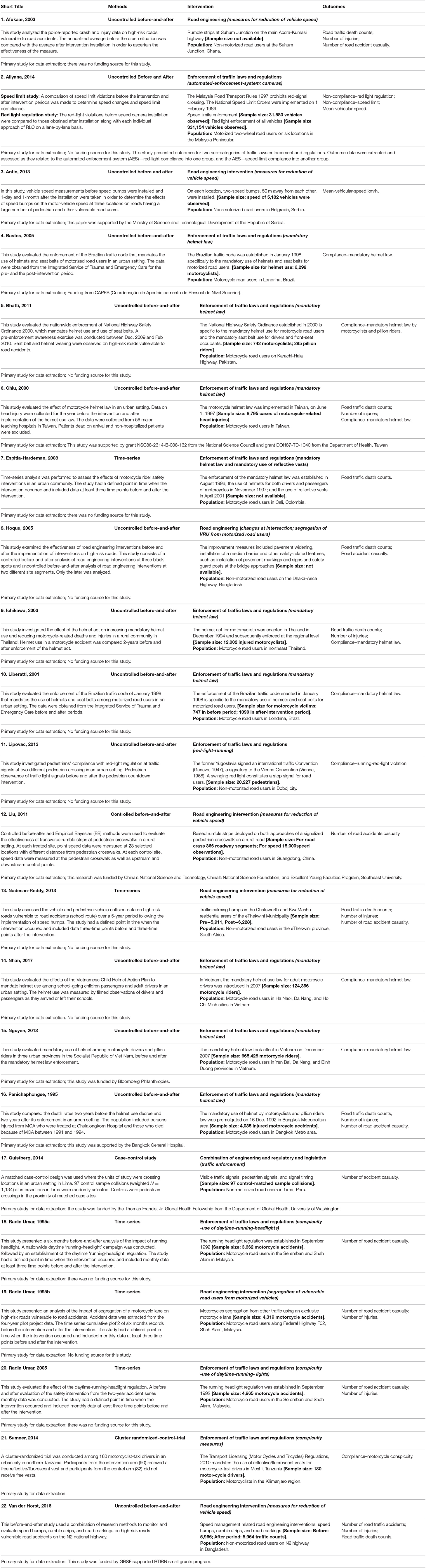
Table 1. Characteristics of studies included for meta-analysis.
Risk-of-Bias Assessment
The majority of the studies included in this review are observational and therefore subject to risk-of-bias in terms of making a causal inference of the effect of road safety interventions.
Selection Bias
Intervention sites in almost all studies were somewhat or most likely to represent the target population. Based on HAT ratings, studies ranked between strong and moderate for selection bias.
Study Design
Based on HAT ratings for study design criteria, one cluster RCT was rated strong for study design. Seven studies having time-series, controlled before-and-after, and case-control study designs were rated moderate. Time-series studies were short period time-series studies using monthly data extending at the most 1 year before and 1 year after the intervention. The controlled before-and-after study reported controlling for confounders by matching treatment and comparison sites on geographic characteristics of roads/location and the same period. The case-control study observed a short time-period for pedestrian and vehicle-flow, but the collision dates and data collection did not happen contemporaneously. However, the study explored the impact on the time difference and found no significant changes.
Confounders
All before-and-after studies adequately controlled for some essential confounders related to road infrastructure interventions such as exposure effect (in traffic volume, area type, geometric design, and type of intersection) before and after the intervention implementation and outcome ascertainment (outcome reporting for non-motorized road users or having road traffic injuries only). For road engineering interventions, almost all studies were coded as at risk for regression-to-the-mean confounder, given that the selection of treatment sites for road improvement interventions is influenced by the high accident rates (Elvik, 2002).
Data Collection
All studies described proper data collection methods. Overall, tools for primary and secondary outcome data were valid and reliable. All studies reported outcomes at the individual levels. Traffic laws enforcement intervention studies on motorized two-wheel road users reported outcomes for motorized two-wheel road users only.
Overall Risk-of-Bias
The overall risk-of-bias using the HAT ratings for one cluster RCT (Sumner et al., 2014), five time-series studies (Radin Umar et al., 1995a,b; Radin Umar, 2005; Espitia-Hardeman et al., 2008; Nadesan-Reddy and Knight, 2013), one controlled before-and after-study (Liu et al., 2011), and one case-control study (Quistberg et al., 2014) provided the strongest assessment of the safety effects of road engineering and enforcement interventions compared to the rest of the included studies.
There were 14 studies (Panichaphongse et al., 1995; Chiu et al., 2000; Liberatti et al., 2001; Afukaar, 2003; Ichikawa et al., 2003; Bastos et al., 2005; Hoque et al., 2005; Bhatti et al., 2011; Antic et al., 2013; Lipovac et al., 2013; Nguyen Ha et al., 2013; Allyana et al., 2014; Van der Horst et al., 2016; Nhan et al., 2017) with a moderate risk-of-bias assessment. These studies used an uncontrolled before-and-after study design. In some uncontrolled before-and-after studies, the post-intervention period started soon after the intervention and included just one period before and one period after; therefore, studies controlled for general changes and change of traffic volume confounding variables.
We have excluded six studies that have overall risk-of-bias grade C because the outcome data did not qualify for analysis because of high risk-of-bias around study design, data collection, and confounders (Mutto et al., 2002; Passmore et al., 2010; Yuan et al., 2012; Wu et al., 2013; Yuan and Chen, 2013; Mousa et al., 2014).
Table 2 provides an assessment of risk-of-bias and the overall risk-of-bias grade of A, B, and C.
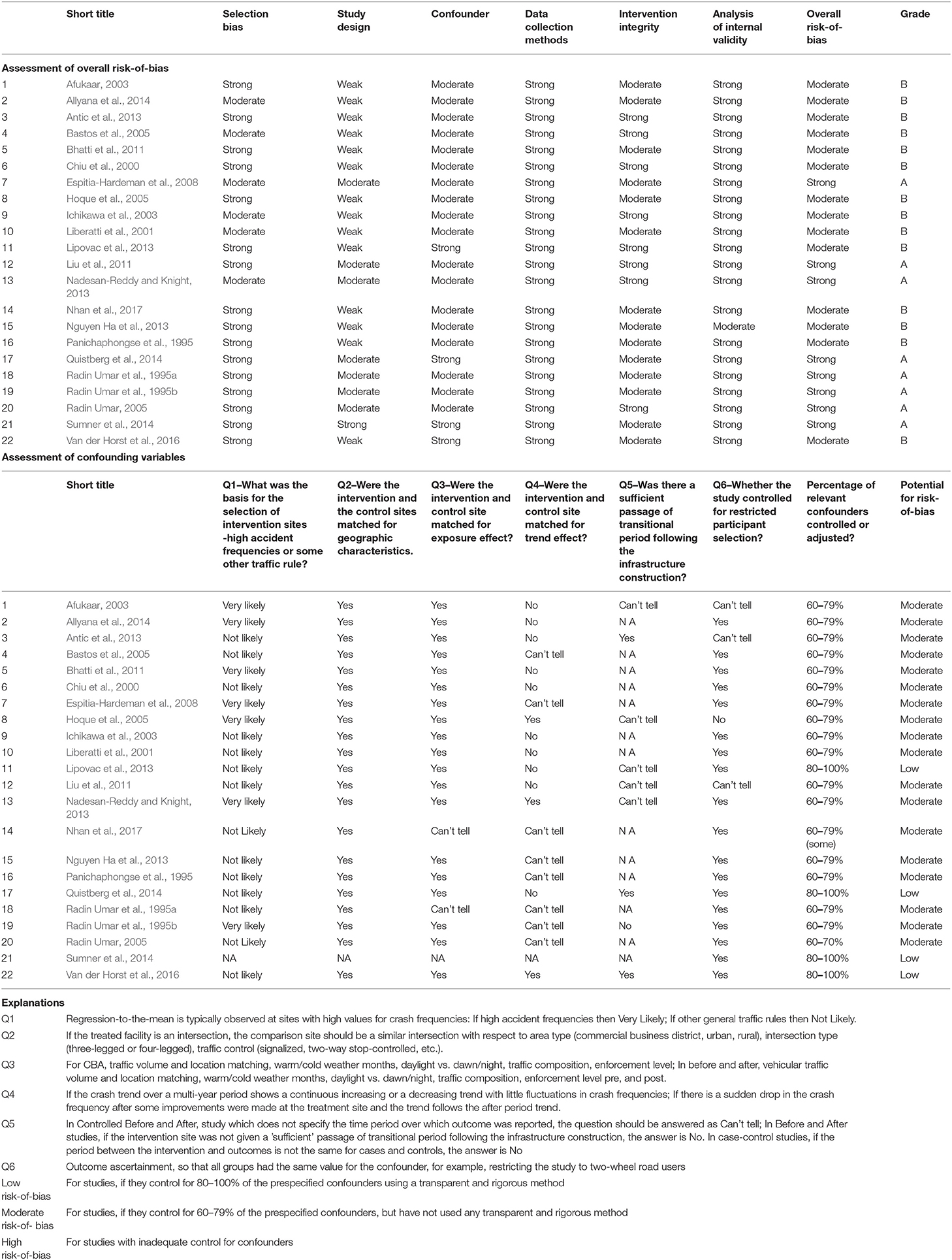
Table 2. Assessment of risk-of-bias of studies included for analysis based on HAT.
Effects of Interventions
Effect sizes were computed for 18 studies. Four studies (Liu et al., 2011; Antic et al., 2013; Quistberg et al., 2014; Sumner et al., 2014) presented one particular outcome or one single study design. The number of studies was not sufficient to calculate a standardized effect size.
Road Engineering Intervention Compared to No Intervention
Uncontrolled before-and-after studies
Three uncontrolled before-and-after studies assessed primary outcomes: road traffic death counts, the number of injuries (moderate and severe), and the number of road accident casualty before and after road engineering interventions.
Primary outcomes. Three studies (Afukaar, 2003; Hoque et al., 2005; Van der Horst et al., 2016) assessed road traffic death counts before and after road engineering interventions. There was no evidence that road engineering interventions were effective (OR 1.63; 95% CI 1.01–2.63; I2 = 0%) based on data from 948 people. Results were analyzed using a random-effects model, and the outcome was downgraded to very low quality. See forest plot, primary outcome: changes in “road traffic death counts”after road engineering interventions (Figure 2). Three studies (Afukaar, 2003; Hoque et al., 2005; Van der Horst et al., 2016) assessed the number of injuries and found no difference in the odds of occurrence of injuries before and after road engineering interventions (OR 0.76, 95% CI 0.47–1.23; I2 = 36%) based on data from 948 people. The results were analyzed using a random-effects model, and the outcome was downgraded to very low quality. See forest plot, primary outcome: changes in the number of “injuries” after road engineering interventions (Figure 3).
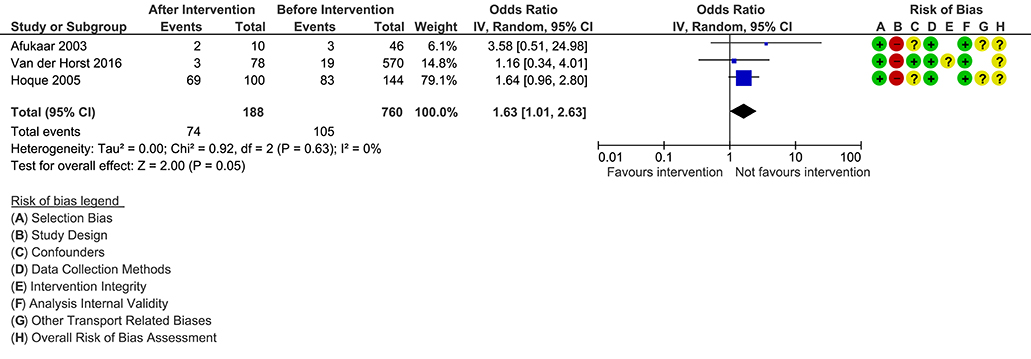
Figure 2. Primary outcome: changes in ‘road traffic death counts’ after road engineering interventions.
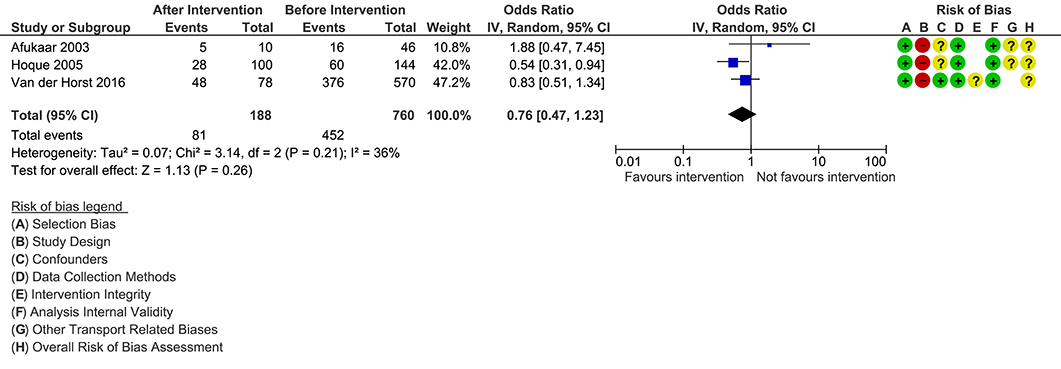
Figure 3. Primary outcome: changes in the number of ‘injuries’ after road engineering interventions.
Two studies (Afukaar, 2003; Van der Horst et al., 2016) assessed the number of road accident casualties before and after road engineering interventions. There was no evidence that road engineering interventions were effective after a road treatment (OR, 2.31; 95% CI 0.57–9.35; I2 = 77%) based on data from 718 people. Results were analyzed using a random-effects model, and the outcome was downgraded to very low quality because heterogeneity was significant. See forest plot, primary outcome: changes in the number of “road accident casualty” after road engineering interventions (Figure 4).
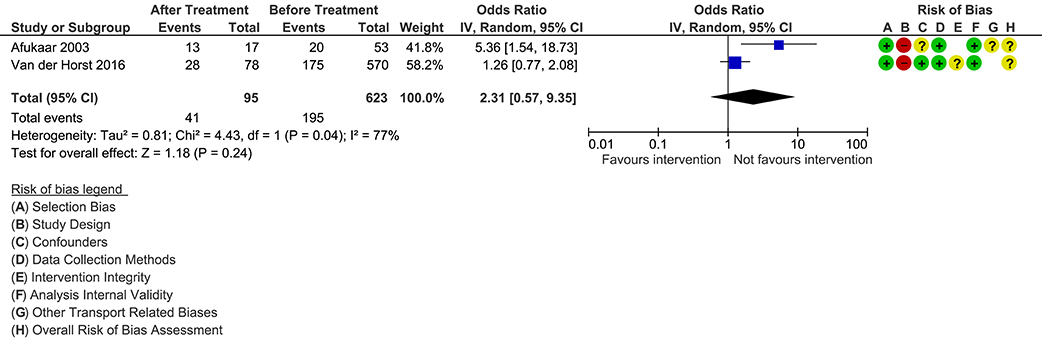
Figure 4. Primary outcome: changes in the number of ‘road accident casualty’ after road engineering interventions.
Secondary outcomes. We assessed no secondary outcomes for road engineering interventions in before-and-after studies.
Time-series studies
Two time-series studies were used to assess primary outcomes, road traffic death counts, and the number of road accident casualty before and after road engineering interventions.
Primary outcomes. One study (Nadesan-Reddy and Knight, 2013) reported road traffic death counts. However, because of an insufficient number of studies the outcome data for road traffic death counts were not assessed.
Two studies (Radin Umar et al., 1995b; Nadesan-Reddy and Knight, 2013) assessed the number of road accident casualty in percent change (-26.62, 95% CI−149.58 - 35.75;−111.80, 95% CI−492.97 - 24.34) based on data from 14,404 people involved in accidents after road engineering interventions. There was no difference in the occurrence of road accident casualty outcome before and after road engineering interventions. The outcome was downgraded as very low quality because of the high presence of heterogeneity. See forest plot, primary outcome: percent change in the number of “road accident casualty” after road engineering interventions (Figure 5).
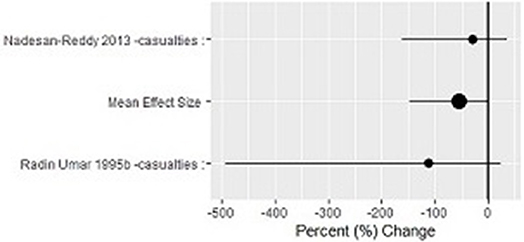
Figure 5. Primary outcome: percent change in the number of ‘road accident casualty’ after road engineering interventions.
Secondary outcomes. We assessed no secondary outcomes for road engineering interventions in time-series studies.
Vote counting and common rubric. We could not develop the vote counting and common rubric for time-series studies.
Enforcement of Traffic Laws and Regulation Interventions Compared to no Intervention
Uncontrolled before-and-after studies
Ten uncontrolled before-and-after studies assessed primary outcomes: road traffic death counts and the number of injuries (moderate and severe) and, secondary outcome, compliance before and after enforcement of traffic laws and regulation interventions.
Primary outcomes. Three studies (Panichaphongse et al., 1995; Chiu et al., 2000; Ichikawa et al., 2003) assessed road traffic death counts of motorcycle riders' road accidents before and after mandatory helmet law enforcement. There was no evidence that the mandatory helmet law enforcement was effective (OR 0.94, 95% CI 0.72–1.23; I2 = 68%) based on data from 35,710 people. Results were analyzed using a random-effects model, and the outcome was downgraded to very low quality. Moderate heterogeneity was present. See forest plot, primary outcome: changes in “road traffic death counts” after mandatory helmet law enforcement (Figure 6).
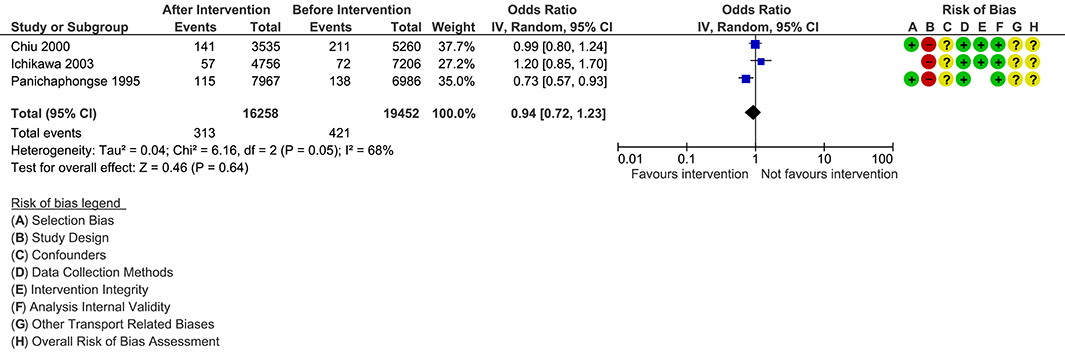
Figure 6. Primary outcome: changes in ‘road traffic death counts’ after mandatory helmet law enforcement.
Three studies (Panichaphongse et al., 1995; Chiu et al., 2000; Ichikawa et al., 2003) assessed the number of injuries before and after motorcycle riders' road accidents. The number of injuries decreased after the mandatory helmet law enforcement (OR, 0.74; 95% CI 0.61–0.89; I2 = 85%) based on data from 35,710 people. Results were analyzed using a random-effects model, and the outcome was downgraded to very low quality. The presence of statistically significant heterogeneity was observed. See forest plot, primary outcome: changes in the number of “injuries” after mandatory helmet law enforcement (Figure 7).
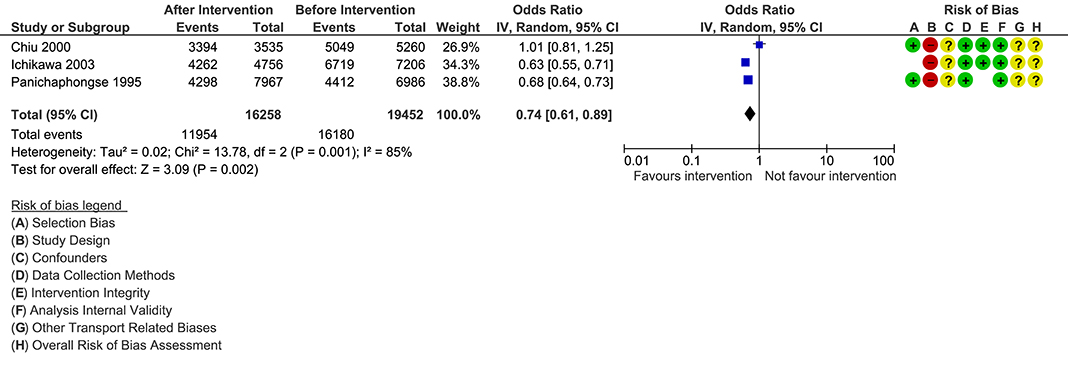
Figure 7. Primary outcome: changes in the number of ‘injuries’ after mandatory helmet law enforcement.
Two studies (Panichaphongse et al., 1995; Chiu et al., 2000) assessed the number of severe and moderate injuries of motorcycle riders before and after motorcycle road accidents. There was no evidence that the helmet law enforcement was effective for severe injuries (OR, 0.91; 95% CI 0.82–1.01; I2 = 32%) and moderate injuries (OR 0.83, 95% CI 0.64–1.07; I2 = 91%) based on data from 23,748 people.
The presence of heterogeneity for overall and moderate injuries was significant, and we developed the vote counting and common rubric.
Vote counting and common rubric. The mandatory helmet law enforcement did not have any effect on the absolute risk for road traffic death counts among motorcyclists. In two studies (Panichaphongse et al., 1995; Ichikawa et al., 2003), the absolute risk for the number of injuries among motorcyclists wearing helmets reduced by 4% and 9%, which was statistically significant. The number of moderate injury outcome for one study (Panichaphongse et al., 1995) stands out from other studies. This study showed a positive impact of the intervention; the absolute risk for the number of moderate injuries among motorcyclists wearing a helmet reduced by 8% and was statistically significant. For details, see vote counting and the common rubric of enforcement of traffic laws and regulations (Table 3).
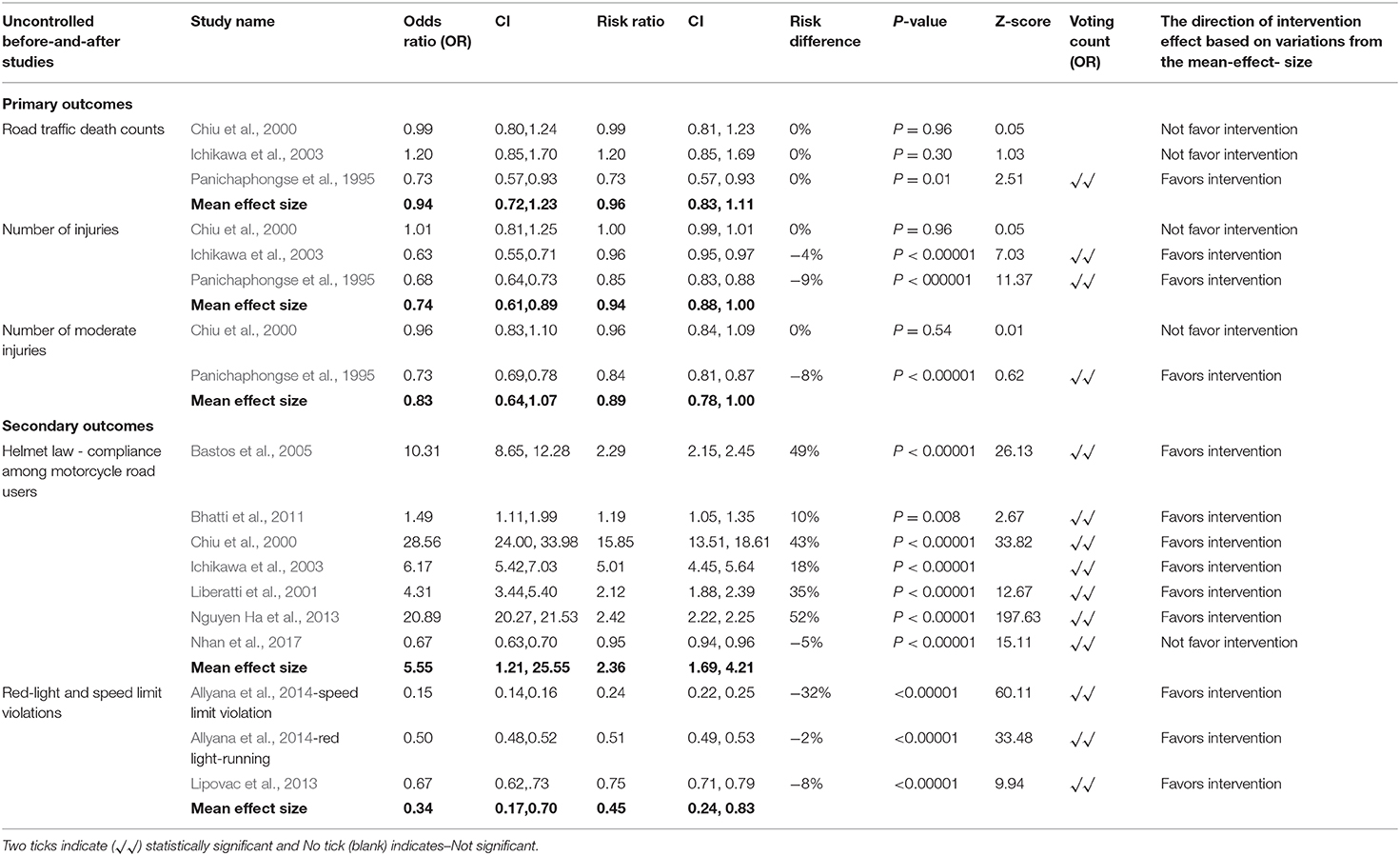
Table 3. Vote counting and the common rubric of enforcement of traffic laws and regulations.
Secondary outcomes. Seven studies (Chiu et al., 2000; Liberatti et al., 2001; Ichikawa et al., 2003; Bastos et al., 2005; Bhatti et al., 2011; Nguyen Ha et al., 2013; Nhan et al., 2017) assessed motorcycle road users' compliance with mandatory helmet law, and two studies assessed effects of automated-enforcement-system (camera) and pedestrian signal (Lipovac et al., 2013; Allyana et al., 2014).
Seven studies (Chiu et al., 2000; Liberatti et al., 2001; Ichikawa et al., 2003; Bastos et al., 2005; Bhatti et al., 2011; Nguyen Ha et al., 2013; Nhan et al., 2017) assessed motorcycle drivers compliance with helmet use after the mandatory helmet law enforcement (OR 5.55, 95% CI 1.21–25.55; I2 = 100%) based on data from 2,47,599 people. In places where a mandatory helmet law was enforced, there was five times more compliance among motorcyclists compared with when there was no mandatory helmet law enforcement. Results were analyzed using a random-effects model, and the outcome was downgraded to very low quality. The presence of a considerable heterogeneity between the effect sizes for the seven studies included in the meta-analysis was statistically significant (P=0.00001). See forest plot, secondary outcome: changes in helmet use “compliance” after mandatory helmet law enforcement (Figure 8).
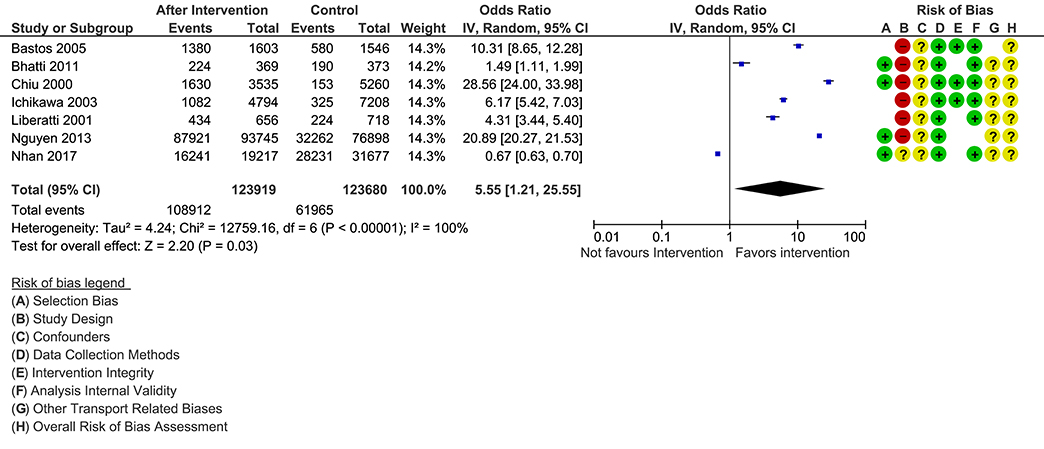
Figure 8. Secondary outcome: changes in helmet use ‘compliance’ after mandatory helmet law enforcement.
Two studies (Lipovac et al., 2013; Allyana et al., 2014) reported speed limit and red-light-running non-compliance (OR 0.37, 95% CI 0.16–0.86; I2 = 100%) based on 3,76,368 traffic volume and found that speed limit and red-light-running violations reduced by 63%. Results were analyzed using a random-effects model, and the outcome was downgraded to very low quality. See forest plot, secondary outcome: changes in “red light and speed limit non-compliance” after enforcement of traffic laws and regulations (Figure 9). Due to the presence of statistically significant heterogeneity (I2 = 100%), the vote counting and common rubric were also developed.
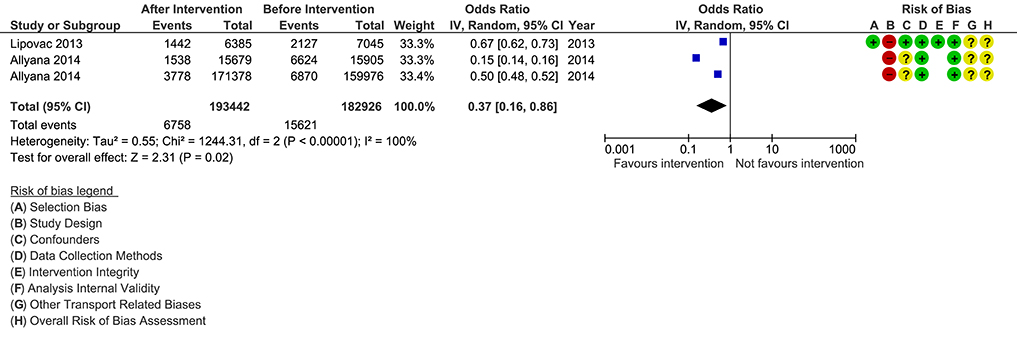
Figure 9. Secondary outcome: changes in ‘red light and speed limit non-compliance’ after enforcement of traffic laws and regulations.
Vote counting and common rubric. Mandatory helmet law compliance among motorcyclists after the intervention period showed a statistically significant increase across individual studies. It was observed that compliance for helmet use among motorcyclists increased between 10 and 52%, in absolute terms. In one study (Nhan et al., 2017) however, compliance among motorcycle drivers decreased by 5% in absolute terms. The impact of traffic law enforcement on the speed limit and red-light-running violations showed positive and statistically significant effects across individual studies (p < 0.00001). The absolute risk for violations against speed limit decreased by 32% (Allyana et al., 2014), and red-light-running decreased by 2% (Allyana et al., 2014), and 8% (Lipovac et al., 2013). For details, see vote counting and the common rubric of enforcement of traffic laws and regulations (Table 3).
Time-series studies
Three time-series studies assessed primary outcomes, road traffic death counts and the number of road accident casualty before and after enforcement of traffic laws and regulation interventions.
Primary outcomes. One study (Espitia-Hardeman et al., 2008) reported road traffic death-counts. Due to an insufficient number of studies, the outcome data for road traffic death counts were not assessed.
Two studies (Radin Umar et al., 1995a; Radin Umar, 2005) reported the number of road accident casualties in percent change (percent-change−51.06; 95% CI−228.64–30.56; percent-change −68.37; 95% CI−227.40–13.40) based on data from 5,083 people involved in accidents after the daytime running-headlight law enforcement. The mean effect size in percent change for road accident casualties declined by 38% after the law enforcement. The outcome was downgraded to low quality. See forest plot, primary outcome: percent change in the number of “road accident casualty” after daytime running-headlight regulation (Figure 10).
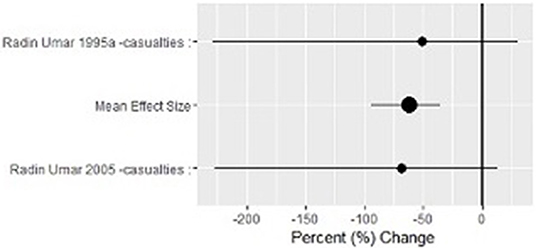
Figure 10. Primary outcome: percent change in the number of ‘road accident casualty’ after daytime running-headlight regulation.
Secondary outcomes. We assessed no secondary outcomes for enforcement of traffic laws and regulation interventions in time-series studies.
Vote counting and common rubric. We could not develop the vote counting and common rubric for time-series studies.
Sensitivity Analysis
We compared the fixed and random effects' estimates of interventions after which we found that the overall estimates were slightly larger with the random-effects model, but the confidence intervals were identical for fixed and random effects. The overall effect was calculated using a random-effects model. The heterogeneity of studies was assessed by inspection of the forest plot, the confidence intervals of studies, and Chi2 and I2 statistics. The analysis under each intervention category was grouped by study design. It was not possible to separate very low-quality studies from high-quality studies due to a lack of sufficient studies or outcome data.
The publication bias was analyzed by examining funnel plots and cumulative meta-analysis. No publication bias was observed.
GRADE quality of evidence
We assessed the methodological quality of the included studies according to the GRADE system for rating the quality of evidence. We ranked the overall quality of evidence across all studies as very low quality. Please see, the summary of findings (GRADE) for road engineering interventions (Table 4) and the summary of findings (GRADE) for enforcement of traffic laws and regulations (Table 5).
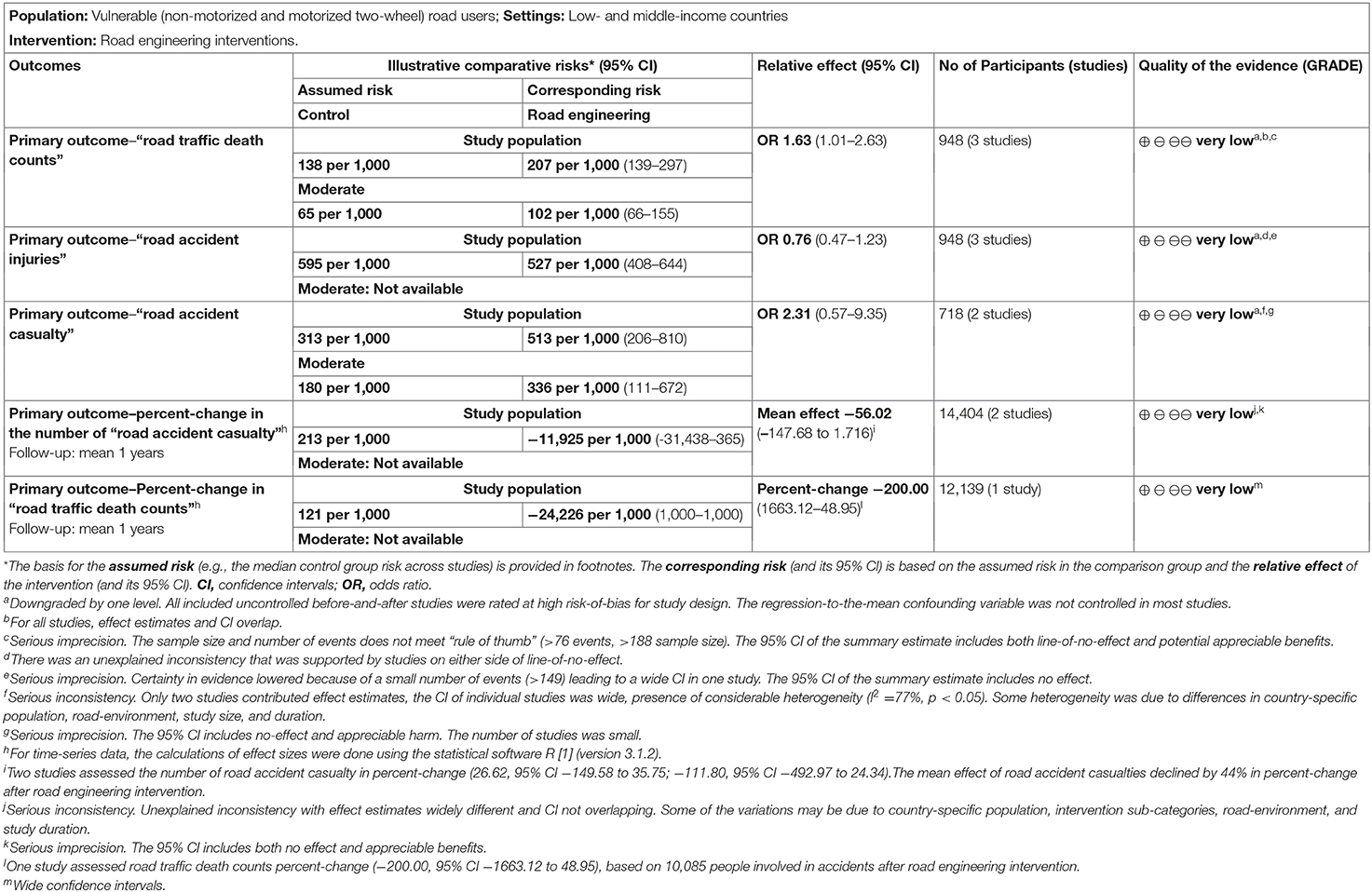
Table 4. Summary of findings (GRADE) for road engineering interventions.
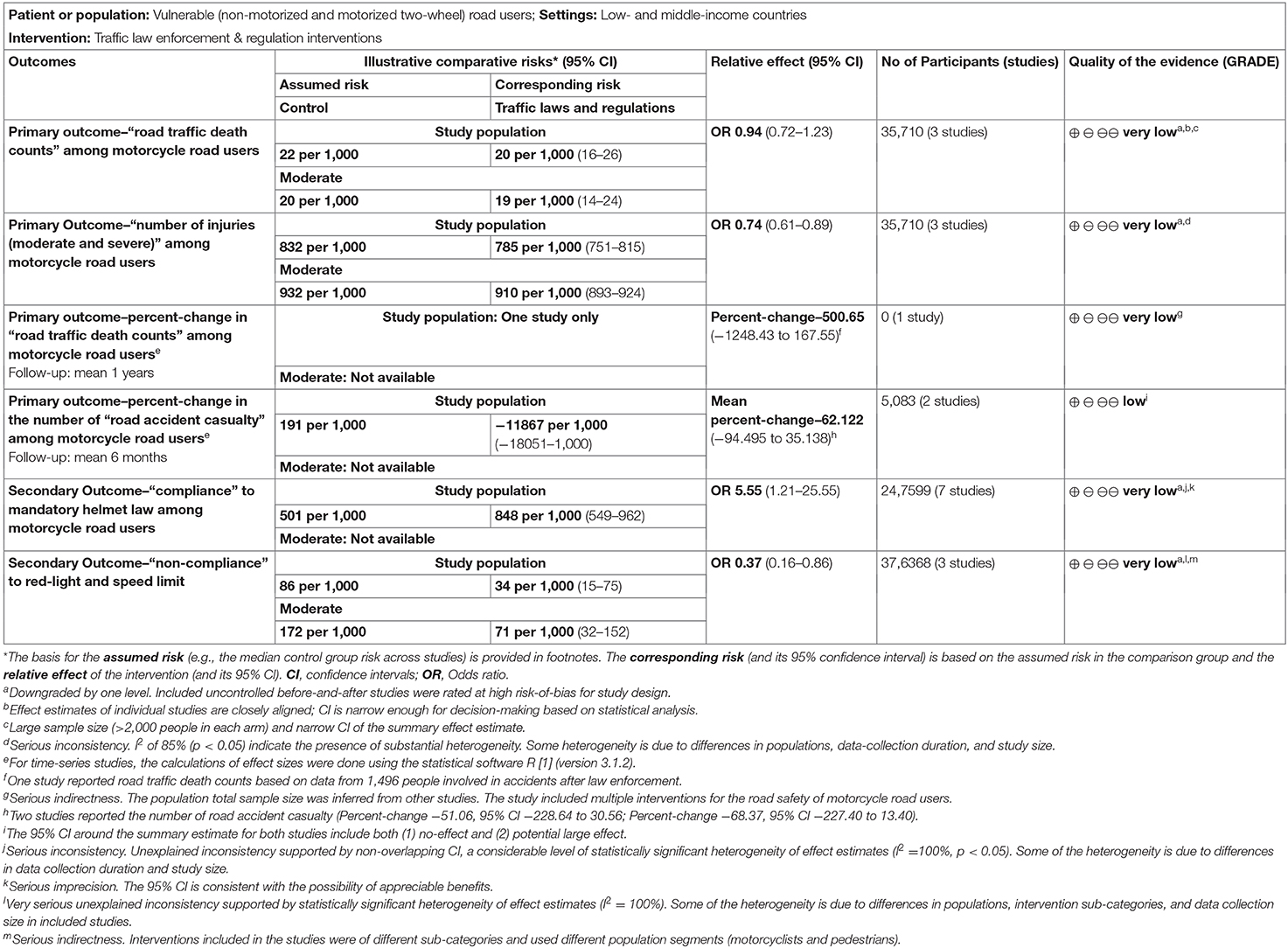
Table 5. Summary of findings (GRADE) for traffic laws and regulation interventions.
Discussion
Road engineering interventions were not effective in reducing road traffic death counts, the number of injuries, and road accident casualty outcomes after road improvements. While the enforcement of mandatory helmet law was ineffective in reducing road traffic death counts, the intervention efforts proved effective in decreasing overall injuries and increasing helmet use compliance. Automated-enforcement-system (camera) and pedestrian signal interventions were effective in increasing road users' compliance to road safety measures. The daytime-running headlight intervention was effective in reducing road accident casualties.
Four studies presented either a unique outcome or a unique study design to measure enforcement of traffic laws and regulations and road engineering intervention outcome effects. In one study (Liu et al., 2011), the use of transverse rumble strips could reduce the incidence of crashes by 25%, on average. Another study (Antic et al., 2013) showed that the use of speed bumps of 5 and 7 cm height significantly contributed to the safety of vulnerable road users, especially the safety of pedestrians because mean-vehicle-speed was reduced by 79%. The findings of one study (Quistberg et al., 2014) showed that the signalization efforts were associated with an increased risk for pedestrian-vehicle collisions. One RCT (Sumner et al., 2014) found that the free distribution of reflective vests led to a statistically significant increase in vest usage among motorcycle riders; however, the absolute increase was modest.
This review included four non-randomized study designs. Because of methodological differences in study designs, the risk of bias in included studies ranged between A and B grade. Overall, all included studies had adequate information to individually meet the study inclusion criteria. The meta-analysis results assessed the presence of substantial heterogeneity for enforcement of traffic laws and regulation intervention studies. We expected some variations in between studies because of differences in sample size, data collection duration, and road environment. The summary effect estimates of studies showed inconsistency and impreciseness, which downsized the quality evidence of included studies as very low quality. The majority of the studies included in this review were uncontrolled before-and-after. It is difficult to perform controlled trials in the transport environment especially those meant for road improvements. In most studies, the post-intervention period started soon after the deployment of the intervention, and all studies included just one period before and one period after, therefore general changes and traffic volume confounders were most likely controlled. In addition, we attempted to minimize bias in the review process by searching a range of databases and not limiting the search by language. We also ensured that study identification and inclusion, data extraction, and risk-of-bias assessment were carried out by two review authors working independently or together.
This review has some limitations, which must be taken into account when interpreting our results. Given our broad approach to study inclusion criteria, we ended up with multiple types of study design, interventions, and outcomes. In addition, there were variations in between studies due to differences in sample size, duration of data collection, road environment, and macro-economic conditions in which the study was conducted. Almost all road engineering studies were found at the risk of regression-to-the-mean confounder given the fact that the selection of treatment sites for road safety intervention is largely influenced by the high frequency of accident rates. For time-series studies, the effect sizes were computed as the percent change. A drawback of this method is that it does not address the problem of autocorrelation and subsequently may result in reduced standard errors. Using ARIMA models may help evade the problem but fitting the ARIMA models requires larger datasets.
The findings of this review mirror the findings of the first systematic review of road traffic injury initiatives' effectiveness in LMICs (Staton et al., 2016). In this review, the first finding was that legislation interventions evaluated with the best outcomes when combined with strong enforcement initiatives or as part of a multifaceted approach. Second, road improvements may increase road traffic injuries. In our review, the evidence showed that enforcement of legislative interventions when combined with increased police surveillance, penalization for non-compliance, advocacy campaigns, and automated-enforcement-systems were more effective in changing drivers' behaviors when compared to stand-alone road engineering interventions. Because of police surveillance, the likelihood of being caught by the police and of being penalized force compliance behavior among road users in LMICs. It is also likely that road users become more aware of traffic safety because legislative enforcements are generally accompanied by awareness campaigns, as seen in some studies (Radin Umar et al., 1995a; Radin Umar, 2005; Bhatti et al., 2011; Nhan et al., 2017). For road engineering interventions, the results were uncertain on reducing the number of road traffic injuries and deaths. In one study (Mutto et al., 2002), because of the construction of an overpass (footbridge), pedestrian injuries increased, although there was a slight decline in fatalities. Since there was no police surveillance or a financial penalization for using roads to cross or any attempts to channel pedestrian traffic to the overpass, most of the pedestrians crossed by creating their own path at “convenient” points through traffic while risking life. Another research (Hijar et al., 2003) also found similar findings. Conversely, the findings of this review did not mirror the findings of reviews conducted in a high-income country setting. For instance, one review (Bunn et al., 2013) suggested that area-wide traffic calming measures may be a promising intervention for reducing the number of road traffic injuries and deaths. In another review (Liu et al., 2008), researchers found that the motorcycle helmet reduced the risks of death and head injury in motorcyclists who crashed.
Conclusion
Further research is needed to examine the effects of road engineering interventions on injury severity outcomes. Even though the evidence was of very low quality, traffic laws, and regulation interventions when combined with enforcement initiatives or with, other approaches proved effective in changing drivers' behaviors.
Future research on road engineering interventions combined with automated-enforcement-system must be explored in an LMIC setting. There is a need for high-quality study designs that use long-term observational periods at the start of the intervention and after the intervention implementation. This review found evidence gaps on the effects of segregation of vulnerable road users from motorized vehicles, bicycle infrastructure interventions, traffic-calming measures on pedestrian accidents.
Data Availability Statement
All datasets generated for this study are included in the article/Supplementary Material.
Author Contributions
MG prepared the review article. SB read and approved the review article.
Funding
This document is an output from a project funded by the UK Aid from the UK Department for International Development (DFID) for the benefit of developing countries. However, the views expressed and information contained in it are not necessarily those of or endorsed by DFID, which can accept no responsibility for such views or information or for any reliance placed on them.
Disclaimer
SB did the work while he was an Assistant Professor at the Indian Institute of Public Health, Hyderabad, India.
Conflict of Interest
SB is employed by the company GlaxoSmithKline Asia Pvt. Ltd.
The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank the Department for International Development (DFID), UK, for funding this review. We thank Prof David Wilson from the Criminology, Law, and Society Department at George Mason University for sharing the methodology for computing effect sizes of time-series studies using the R statistical software. We thank Newton Opiyo from the Cochrane Public Health and Systems Network for an independent assessment of study inclusion criteria and risk-of-bias in included studies. We thank Melissa G. Lewis for her statistical advise. We thank co-authors Dr. Geetha Menon for her contributions to meta-analysis and Dr. Ganesh Devkar for his contribution to data screening and coding of studies. We thank Ms. Poh Chua, Deputy Librarian at the Royal Children's Hospital Library for her assistance with the development of literature search strategies.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frsc.2020.00010/full#supplementary-material
Footnotes
1. ^According to the Oxford dictionary, second definition of the “casualty” noun (hospital): “emergency room, the part of a hospital where people who are hurt in accident or suddenly become ill are taken for treatment.” Included studies have extracted road traffic accident and injury outcome data from police reported road traffic accidents that either required medical assistance or were hospitalized. Thus, the “number or proportion of road accident casualty” defines the number or proportion of road traffic accidents.
2. ^In before-and-after studies with dichotomous outcome data, the individual study findings are displayed as “n/N,” whereby: n = the number of outcome events (e.g., fatality or helmet use compliance count) in the after intervention period (intervention group) or before intervention period (control group), and N = the total number of outcome events in the interventions group or control group.
3. ^In before-and-after studies with continuous outcome data, the individual study findings are given as “N” and “mean (SD),” whereby N = the total number of outcome events (e.g., road accident causality or red-light running count) in the after intervention period (intervention group) or before intervention period (control group) and mean SD = the arithmetic mean and standard deviation (SD) of the outcome measure in either the intervention or control group.
References
Afukaar, F. K. (2003). Speed control in developing countries: issues, challenges, and opportunities in reducing road traffic injuries. Inj. Control Saf. Promot. 10, 77–81. doi: 10.1076/icsp.10.1.77.14113
Allsop, R. (2010). The effectiveness of speed cameras – A review of evidence. London: RAC Foundation, 42. Available online at: https://www.racfoundation.org/assets/rac_foundation/content/downloadables/efficacy_of_speed_cameras_allsop_181110.pdf (assessed May 28, 2019).
Allyana, S., Mohamed, S., and Jamil, H. M. (2014). Impact studies of automated enforcement system implementation. Malaysia Inst. Road Saf. Res. 129, 6–23.
Antic, B., Pesic, D., Vujanic, M., and Lipovac, K. (2013). The influence of speed bumps heights to the decrease of the vehicle speed - Belgrade experience. Saf. Sci. 57, 303–312. doi: 10.1016/j.ssci.2013.03.008
Bartels, D., Bhalla, K., Shahraz, S., Abraham, J., Lozano, R., and Murray, C. J. L. (2010). Incidence of road injuries in Mexico: country report. Int. J. Inj. Control Safety Promot. 17, 169–176. doi: 10.1080/17457300903564553
Bastos, Y. G. L., de Andrade, S. M., Soares, D. A., and Matsuo, T. (2005). Seat belt and helmet use among victims of traffic accidents in a city of Southern Brazil, 1997-2000. Public Health 119, 930–932. doi: 10.1016/j.puhe.2005.01.008
Bhatti, J. A., Ejaz, K., Razzak, J. A., Tunio, I. A., and Sodhar, I. (2011). Influence of an enforcement campaign on seat belt and helmet wearing, Karachi-Hala Highway, Pakistan. Ann. Adv. Automot. Med. 55, 65–70.
Bishai, M., and Hyder, A. (2006). Modeling the cost-effectiveness of injury interventions in lower and middle-income countries: opportunities and challenges. Cost Eff. Resour. Alloc. 4:2. doi: 10.1186/1478-7547-4-2
Blanco, M., Cabrera, J. M., Carozzi, F., and Cid, A. (2017). Effects of Motorcycle Helmet Laws on Prevention of Fatalities: An Impact Evaluation. Department of Economics Working Paper Series, Universidad de Montevideo. MPRA Paper No. 84652. Available online at: https://mpra.ub.uni-muenchen.de/84652/ (assessed Feb 26, 2020).
Bunn, F., Collier, T., Frost, C., Ker, K., Roberts, I., and Wentz, R. (2003). Area-wide traffic calming for preventing traffic related injuries. Cochrane Database Syst. Rev. CD003110.
Chisholm, D. N. (2008). Road Traffic Injury Prevention: An Assessment of Risk Exposure and Intervention Cost-Effectiveness in Different World and Huseyin regions. Geneva: World Health Organization. 59p. Available online at: https://www.who.int/choice/publications/d_2009_road_traffic.pdf (assessed June 5, 2019).
Chiu, W. T., Kuo, C. Y., Hung, C. C., and Chen, M. (2000). The effect of the Taiwan motorcycle helmet use law on head injuries. Am. J. Public Health 90, 793–796. doi: 10.2105/AJPH.90.5.793
Commission for Global Road Safety (2013). Make Roads Safe - A Decade of Action for Road Safety. London: Commission for Global Road Safety, 43 p. Available online at: https://www.fiafoundation.org/media/46106/mrs-time-for-action-lr.pdf (assessed January 2020).
de Vasconcellos, E. A. (2013). Road safety impacts of the motorcycle in Brazil”, In: International Journal of Injury Control and Safety Promotion, Vol. 20, 144–51. doi: 10.1080/17457300.2012.696663
Elvik, R. (2001). Area-wide urban traffic calming schemes: a meta-analysis of safety effects. Accid. Anal. Prev. 33, 327–336. doi: 10.1016/S0001-4575(00)00046-4
Elvik, R. (2002). The importance of confounding in observational before-and-after studies of road safety measures. Accid. Anal. Prev. 34, 631–635. doi: 10.1016/S0001-4575(01)00062-8
Esperato, A., Bishai, D., and Hyder, A. (2012). Projecting the Health and Economic Impact of Road Safety Initiatives: a Case Study of a Multi-Country Project. Available online at: http://dx.doi.org/10.1080/15389588.2011.647138 (assessed 15 June, 2019).
Espitia-Hardeman, V., Velez, L., Munoz, E., Gutierrez-Martinez, M. I., Espinosa-Vallin, R., and Concha-Eastman, A. (2008). Impact of interventions directed toward motorcyclist death prevention in Cali, Colombia: 1993-2001. Salud Publica Mex. 50, 569–577. doi: 10.1590/S0036-36342008000700011
Gupta, M., Menon, G. R., Devkar, G., and Thomson, H. (2015). Regulatory and Road-engineering interventions for preventing road traffic injuries and fatalities among vulnerable (non-motorized and motorized two-wheel) road users in low- and middle-income countries. Cochrane Database Syst. Rev. CD011495, 1–56. doi: 10.1002/14651858.CD011495
Harris, M. A., Reynolds, C. C. O., Winters, M., Cripton, A. P., Shen, H., Chipman, M. L., et al. (2013). Comparing the effects of infrastructure on bicycling injury at intersections and non-intersections using a case-crossover design. Inj Prev. 19, 303–310. doi: 10.1136/injuryprev-2012-040561
Hijar, M., Vazquez-Vela, E., and Arreola-Risa, C. (2003). Pedestrian traffic injuries in Mexico: a country update. Inj. Control Saf. Promot. 10, 37–43. doi: 10.1076/icsp.10.1.37.14108
Hoque, S., Mumiruzzaman, S., and Syed Noor-ud-Deen, A. (2005). Performance evaluation of road safety measures: a case study of the Dhaka-Arich highway in Bangladesh. Transp. Commun. Bull. Asia Pac. 74, 33–56.
Huang, W. S., and Lai, C. H. (2011). Survival risk factors for fatal injured car and motorcycle drivers in single alcohol-related and alcohol-unrelated vehicle crashes. J. Safety Res. 42, 93–99. doi: 10.1016/j.jsr.2011.01.005
Ichikawa, M., Chadbunchachai, W., and Marui, E. (2003). Effect of the helmet act for motorcyclists in Thailand. Accid. Anal. Prev. 35, 183–189. doi: 10.1016/S0001-4575(01)00102-6
International Transport Forum (2015). Improving Safety for Motorcycle, Scooter and Moped Riders, Paris: OECD Publishing.
International Transport Forum (2016). Zero Road Deaths and Serious Injuries: Leading a Paradigm Shift to a Safe System. Paris France: OECD Publishing. 163p. doi: 10.1787/9789282108055-en
ITRAC (2008). Toward Zero: Ambitious Road Safety Targets, and the Safe System Approach. Paris, France: OECD Publishing. Report No.: ISBN 978-92-821-0195
Kim, P., and Dumitrescu, E. (2010). UNEP Transport Unit. Share the Road: Investments in Walking and Cycling Road Infrastructure. Nairobi: Division of Technology, Industry and Economics Transport Unit, UNEP, 51p.
Liberatti, C. L. B., Andrade, S. M., and Soares, D. A. (2001). The new Brazilian traffic code and some characteristics of victims in southern Brazil. Inj. Prev. 7, 190–193. doi: 10.1136/ip.7.3.190
Lipovac, K., Vujanic, M., Maric, B., and Nesic, M. (2013). The influence of a pedestrian countdown display on pedestrian behavior at signalized pedestrian crossings. Transp. Res. F: Traffic Psychol. Behav. 20, 121–134. doi: 10.1016/j.trf.2013.07.002
Liu, B., Ivers, R., Norton, R., Boufous, S., Blows, S., and Lo, S. K. (2008). Helmets for preventing injury in motorcycle riders. Cochrane Database of Systematic Reviews, Issue 1. doi: 10.1002/14651858.CD004333.pub3
Liu, P., Huang, J., Wang, W., and Xu, C. (2011). Effects of transverse rumble strips on safety of pedestrian crosswalks on rural roads in China. Accid. Anal. Prev. 43, 1947–1954. doi: 10.1016/j.aap.2011.05.012
Lusk, A. C., Furth, P. G., Morancy, P., Miranda-Moreno, L. F., Willett, W. C., and Dennerlein, J. C. (2011). Risk of injury for bicycling on cycle tracks versus in the street. Inj. Prev. 17, 20. doi: 10.1136/ip.2010.028696
Mohan, D., Omer, T., Sivek, M., and Flannagan, M. J. (2009). Road safety in India: challenges and opportunities. Ann Arbor (MI): The University of Michigan Transportation Research Institute. Report No. UMTRI-2009–1 2009. Available online at: https://www.irfnet.ch/files-upload/knowledges/UMTRI-2009-1.pdf (assessed June 5, 2019).
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. J., and PRISMA Group. (2009). Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 6:e1000097. doi: 10.1371/journal.pmed.1000097
Mousa, A., Moghadas, N. F., Javad, T., Alireza, N., and Tanzadeh, R. (2014). “Analysis of motor vehicle collision and effect of more safety requirements using police record information for Iran roads in spring holidays,” in Second International Conference on Traffic and Transport Engineering (ICTTE) (Belgrade), 1250–1256.
Mutto, M., Kobusingye, O. C., and Lett, R. R. (2002). The effect of an overpass on pedestrian injuries on a major highway in Kampala - Uganda. Afr. Health Sci. 2, 89–93.
Nadesan-Reddy, N., and Knight, S. (2013). The effect of traffic calming on pedestrian injuries and motor vehicle collisions in two areas of the eThekwini Municipality: a before-and-after study. South Afr. Med. J. 103, 621–625. doi: 10.7196/samj.7024
Nantulya, V. M., and Reich, M. R. (2003). Equity dimensions of road traffic injuries in low- and middle-income countries. Inj. Control Safety Promot. 10, 13–20. doi: 10.1076/icsp.10.1.13.14116
Nguyen Ha, T., Passmore, J., Cuong Pham, V., and Nguyen, N. P. (2013). Measuring compliance with Viet Nam's mandatory motorcycle helmet legislation. Int. J. Inj. Contr. Saf. Promot. 20, 192–196. doi: 10.1080/17457300.2012.706617
Nhan, L. D. T., Parker, L., Son, M. T. H., Parker, E. M., Moore, M. R., Sidik, M., et al. (2017). Evaluation of an integrated multi-sector campaign to increase child helmet use in Vietnam. Inj. Prev. 25, 206-210. doi: 10.1136/injuryprev-2017-042517
Panichaphongse, V., Watanakajorn, T., and Kasantikul, V. (1995). Effects of law promulgation for compulsory use of protective helmets on death following motorcycle accidents. J. Med. Assoc. Thail. 78, 521–525.
Passmore, J., Phuong Nam, N., Lan, N., and Trong Ha, N. (2010). The development and implementation of mandatory motorcycle helmet legislation in Vietnam. Inj. Prev. 16, 2007–2009. doi: 10.1136/ip.2010.029215.776
Perel, P., Ker, K., Ivers, R., and Blackhall, K. (2007). Road safety in low and middle-income countries: a neglected research area. Inj. Prev. 13:227. doi: 10.1136/ip.2007.016527
Popay, J., Roberts, H., Sowden, A., Petticrew, M., Arai, L., Rodgers, M., et al. (2006). Guidance on the Conduct of Narrative Synthesis in Systematic Reviews: a Product of the ESRC Methods Program (Version I). 1st Edn, London, UK: ESRC.
Quistberg, D. A., Koepsell, T. D., Boyle, L. N., Miranda, J. J., Johnston, B. D., Ebel, B. E., et al. (2014). Pedestrian signalization and the risk of pedestrian-motor vehicle collisions in Lima, Peru. Accid. Anal. Prev. 70, 273–281. doi: 10.1016/j.aap.2014.04.012
Radin Umar, R. S. (2005). The value of daytime running headlight initiatives on motorcycle crashes in Malaysia. Transp. Commun. Bull. Asia Pac. 74, 17–31.
Radin Umar, R. S., Mackay, G. M., and Hills, B. L. (1995a). Preliminary analysis of motorcycle accidents: short-term impacts of the running headlights campaign and regulation in Malaysia. J. Traffic Med. 23, 17–28.
Radin Umar, R. S., Mackay, M. G., and Hills, B. L. (1995b). Preliminary analysis of exclusive motorcycle lanes along the federal highway F02, Shah Alam, Malaysia. IATSS Res. 19, 93–98.
Redelmeirier, D. A., Tibshirani, R. J., and Evans, L. (2003). Traffic-law enforcement and risk of death from motor-vehicle crashes: case-crossover study. Lancet 361, 2177–82. doi: 10.1016/S0140-6736(03)13770-1
Reynolds, C. C., Anne Harris, M., Teschke, K., Cripton, P. A., and Winters, M. (2009).The impact of transportation infrastructure on bicycling injuries and crashes: a review of the literature. Environ. Health 8:47. doi: 10.1186/1476-069X-8-47
Staton, C., Vissoci, J., Gong, E., Toomey, N., Wafula, R., Abdelgadir, J., et al. (2016). Road traffic injury prevention initiatives: a systematic review and meta-summary of effectiveness in low and middle-income countries. PLoS ONE 11:e0144971. doi: 10.1371/journal.pone.0144971
Sumner, S. E., Pallangyo, A. J., Reddy, E. A., Maro, V., Pence, B. W., Lynch, C., et al. (2014). Effect of free distribution of safety equipment on usage among motorcycle-taxi drivers in Tanzania-a cluster randomized controlled trial. Inj. Int. J. 45, 1681–1686. doi: 10.1016/j.injury.2014.04.034
Thomas, H. (1998). Quality Assessment Tool for Quantitative Studies. Hamilton: Canada: Effective Public Health Practice Project (EPPH) (Original link no longer works. Available online at: https://merst.ca/wp-content/uploads/2018/02/qualilty-assessment-dictionary_2017.pdf (accessed November 2018)
Van der Horst, A. R. A., Thierry, M. C., Vet, J. M., and Fazlur Rahman, A. K. M. (2016). An evaluation of speed management measures in Bangladesh based upon alternative accident recording, speed measurements, and DOCTOR traffic conflict observations. Transp. Res. F Traffic Psychol. Behav. 46(Pt B), 390–403. doi: 10.1016/j.trf.2016.05.006
Vasconcellos, E. A. (2001). Urban transport, environment, and equity: The case for developing countries. London: Earth-scan, 413p. Available online at: https://www.researchgate.net/publication/293725981_Urban_transport_environment_and_equity_The_case_for_developing_countries (assessed May 29, 2019).
Wegman, F. (2017). The future of road safety: a worldwide perspective. IATSS Res. 40, 66–71. doi: 10.1016/j.iatssr.2016.05.003
Wilson, C., Willis, C., Hendrikz, J. K., Le Brocque, R., and Bellamy, N. (2010). Speed cameras for the prevention of road traffic injuries and deaths. Cochrane Database Syst Rev. doi: 10.1002/14651858.CD004607.pub3
World Bank (1993). Investing in Health: World Development Report. London, UK: Oxford University Press.
World Health Organization (2013). Pedestrian Safety A Road Safety Manual for Decision-Makers and Practitioners. Geneva: World Health Organization, 192p. Available online at: https://www.who.int/roadsafety/projects/manuals/pedestrian/en/ (assessed June 5, 2019).
World Health Organization (2018). Global status report on road safety 2018. Geneva: World Health Organization, 424p. Available online at: https://www.who.int/violence_injury_prevention/road_safety_status/2018/en/ (assessed June 5, 2019).
Wu, J., Hu, H., and Li, J. (2013). “Speed control effect study on optical illusion,” in 16th Road Safety on Four Continents Conference (Beijing: Swedish National Road and Transport Research Institute).
Yuan, A., Changcheng, L. I., and Zhang, G. (2012). “GRSP/MOT speed management pilot project in China,” in Australasian Road Safety Research, Policing, and Education Conference (Wellington), 1–10.
Keywords: enforcement, engineering, road safety, fatality, injury, motorcycle, pedestrian, LMIC
Citation: Gupta M and Bandyopadhyay S (2020) Regulatory and Road Engineering Interventions for Preventing Road Traffic Injuries and Fatalities Among Vulnerable Road Users in Low- and Middle-Income Countries: A Systematic Review. Front. Sustain. Cities 2:10. doi: 10.3389/frsc.2020.00010
Received: 04 February 2020; Accepted: 24 March 2020;
Published: 19 May 2020.
Edited by:
Krzysztof Goniewicz, Military University of Aviation, PolandReviewed by:
Witold Pawłowski, Medical University of Lublin, PolandJames Damsere-Derry, Building and Road Research Institute (CSIR), Ghana
Copyright © 2020 Gupta and Bandyopadhyay. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Manisha Gupta, bWFuaXNjaGEuZ3VwdGFAZ21haWwuY29t