 Nebiyu Solomon Tibebu1
Nebiyu Solomon Tibebu1 Melaku Birhanu Alemu2
Melaku Birhanu Alemu2 Bayew Kelkay Rade3
Bayew Kelkay Rade3 Belayneh Ayanaw Kassie4
Belayneh Ayanaw Kassie4 Mequanint Melesse Bicha5
Mequanint Melesse Bicha5 Muhabaw Shumye Mihret1
Muhabaw Shumye Mihret1 Getachew Muluye Gedef3*
Getachew Muluye Gedef3*
- 1Department of Clinical Midwifery, School of Midwifery, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
- 2Department of Health Systems and Policy, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
- 3Department of General Midwifery, School of Midwifery, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
- 4Department of Women’s and Family Health, School of Midwifery, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
- 5Department of Obstetrics and Gynecology, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Background: Abortion complications are the leading causes of maternal death in low and middle-income countries, including Ethiopia. Providing quality and comprehensive abortion care services is crucial for improving the health of women and increased their satisfaction. Evaluating a client's satisfaction with abortion care is clinically relevant since women's satisfaction with health services is one of the key indicators of high-quality healthcare services. Therefore, this study aimed to assess women's satisfaction with comprehensive abortion care services and associated factors.
Methods: An institution-based cross-sectional study was implemented among 333 women in Central Gondar Zone public primary hospitals from October 1, 2022, to April 30, 2023. Eligible participants were selected using a systematic random sampling technique. The data was collected using an interviewer-administered semi-structured, and pretested questionnaire. STATA version 17 and SPSS version 25 software were used for data entry and analysis respectively. Bivariable and multivariable logistic regression models were used to identify factors associated with clients’ satisfaction with comprehensive abortion care services. A P-value of ≤0.05 with a 95% confidence interval was the cutoff point for determining statistical significance.
Results: This study revealed that the level of client satisfaction with comprehensive abortion care services was 60.4% (95% CI: 55.0%, 66.0%). The use of abortion medication (AOR = 4.41, 95% CI: 2.59, 7.48), women's age 20–24 years (AOR = 2.94, 95% CI: 1.02, 8.48), and being a student (AOR = 2.88, 95% CI: 1.10, 7.51) were significantly associated with women's satisfaction with comprehensive abortion care services.
Conclusions: Women's satisfaction with comprehensive abortion care services was relatively low, and it was strongly correlated with the method of abortion, age, and occupation. To improve women's satisfaction requires a comprehensive understanding of women's values and perspectives, providing sexual and reproductive health education, and quality abortion care services are recommended.
Introduction
Abortion is defined by the World Health Organization (WHO) as pregnancy termination prior to fetal viability; however, several nations use different gestational age and/or fetal weight to determine the viability of the fetus (1). Depending on the cause, an abortion can be spontaneous or induced, and the procedure can be carried out using medication or through surgical intervention (2, 3). To further differentiate between abortions, the words “therapeutic abortion” and “voluntary abortion” are employed; therapeutic abortion refers to an abortion performed to save the life of the pregnant woman in cases where continuing the pregnancy poses a serious risk to the mother's life, while voluntary abortion is chosen for personal or social reasons (4).
Ethiopia's 2005 Penal Code and the Ministry of Health's guidance on safe abortion services allow abortions under specific circumstances, such as if the pregnancy is a result of rape or incest; if the continuation of pregnancy endangers the life of the woman, if the fetus has a serious and incurable deformity; or if the pregnant woman is physically and mentally unfit to raise the child due to a physical or mental disability or her minority. Despite this, unsafe abortions remain prevalent in Ethiopia, contributing significantly to maternal morbidity and mortality (5, 6).
Abortion care is a crucial aspect of reproductive health services, and ensuring high-quality and accessible abortion care services is essential for promoting women's health, rights, and satisfaction (7). The WHO has made it very clear in recent years that access to high-quality healthcare, including services related to abortion, is a prerequisite for protecting the right to health as a fundamental human right (8).
Worldwide, nearly 22 million unsafe abortions are carried out annually, and the majority of them occur in low- and middle-income countries (9). Approximately 13% of maternal deaths in developing nations are attributable to unsafe abortion practices (10, 11). In Ethiopia, complications from abortions are the leading cause of maternal morbidity and mortality; about 31% of all maternal mortalities are due to unsafe abortions (12).
Strict national laws, a lack of readily available safe abortion services, and inadequate care following an abortion have caused many women to die too young (13). Maternal death and morbidity associated with abortion are clearly avoidable via comprehensive sexual education, easily accessible family planning services, and safe and legal-induced abortion (14).
Comprehensive abortion care (CAC) is a successful and holistic approach for preventing unintended pregnancy and repeated abortion, managing abortion complications, and eventually increasing client satisfaction (15).
Effective and quality services are essential for improving women's health outcomes and, at the same time, satisfying the healthcare needs and rights of women who have experienced abortion complications (16).
Client service-related satisfaction levels are important for evaluating the quality of healthcare offered by the institution, identifying what factors affect clinical performance and patient retention, and ascertaining whether the services offered meet the needs of the clients, such as having a choice of services, positive interactions with providers, receiving accurate and complete information, and receiving high-quality care (17).
Client satisfaction with abortion services is a relevant and widely used indication of the quality of healthcare provided; it influences women's desire to seek abortion treatment and return for post abortion care and eventually significantly impacts health outcomes (15, 18). Satisfied clients are more likely to adhere to treatment plans, participate actively in their care, continue utilizing services, and recommend others to services. Conversely, low-quality care services may lead women to seek care from unqualified providers or to self-induce abortions, which increases the risk of morbidity and death from abortion (19).
Access to quality abortion care services remains a challenge in low-income nations (17). Continuous service improvement initiatives are necessary to maintain service quality and meet women's healthcare needs. Ethiopia has made progress in providing more access to reproductive healthcare services, including abortion, but there are still gaps in policy objectives and actual implementation, especially in poor and rural areas. Comprehending women's contentment with abortion care services is crucial not only for assessing the quality of services but also shaping policy and practice to better meet women's needs. Therefore, it is reasonable to evaluate client satisfaction with CAC services to identify areas that need attention to improve service quality and obtain better results.
Women's satisfaction with abortion services is influenced by various factors such as the condition of medical facilities and equipment (cleanliness and safety protocols), the skill level and expertise of the healthcare providers; counseling and information provision (clear and comprehensive information about the procedure, risks, and options before the procedure and obtaining informed consent); personal factors (women's prior experiences with healthcare services, level of education and awareness about abortion and reproductive health); cultural and societal factors (cultural sensitivity and personal beliefs towards abortion, support from family and community members); emotional and psychological support, legal environment (restrictions or protections regarding abortion services); timeliness (length of time women have to wait for appointments and procedures) and privacy and confidentiality during the care process (availability of private spaces for consultations and procedures) (7, 13, 15, 16, 20–26).
Previous studies in Ethiopia have primarily focused on the magnitude of abortion services, but little attention has been given to evaluating women's satisfaction with CAC. Therefore this study aims to assess satisfaction levels and to identify associated factors, and to provide actionable insights for healthcare providers and policymakers.
Materials and methods
Study design, setting and period
An institution-based cross-sectional study was carried out in the Central Gondar zone, Amhara Regional State, Ethiopia, from October 1, 2022 to April 30, 2023. The Central Gondar zone is located 748 km from Addis Ababa, Ethiopia, and 182 km from Bahir Dar, the capital town of the Amhara Regional State. It covers thirteen woreda with an estimated total population of 2,896,928. In this zone, there were 14 districts, 9 hospitals and 75 health centers.
Study populations
All women who utilized abortion care in public primary hospitals in the central Gondar Zone during the study period.
Sample size and sampling procedures
Using a single population proportion formula and the following presumptions; prevalence (P) of client satisfaction with abortion care services: 26.9% (27), with a 95% confidence interval (CI) and 5% margin of error; the sample size was calculated as follows:
; by considering a 10% nonresponse rate, a final sample size of 333 was obtained.
where n is the required sample size, z is the standard normal distribution curve at 95% confidence level α = level of significance, p is the proportion of client satisfaction with abortion care services, and d is the margin of error.
Based on the total number of abortions conducted in the preceding month, a proportionate amount of the sample was assigned to each institution. The desired sample sizes from each hospital were then chosen through the application of a systematic random sampling technique.
Data collection procedure
Data were collected using an interviewer-administered, semi-structured questionnaire. The data collection tool was prepared after relevant and related literature was reviewed. Ten midwives collected the data, and five master's-holder midwives supervised the data collection process. Moreover, the principal investigator was available to offer guidance when needed.
Data quality control
The questionnaire was first written in English, then translated into Amharic, the local language, and then back into English. A pretest was carried out on five percent of the sample size before the actual data collection to verify the tool's applicability and linguistic clarity. Half a day training was provided for the data collectors and supervisors to help them better understand the purpose of the study and the overall procedure of the data collection process. Supervisors and the principal investigator conducted daily checks on the questionnaire to ensure its completeness during the actual data collection period.
Data management and analysis
After the data were checked for accuracy, consistency, and missing values, STATA version 17 and SPSS version 25 software were used for data entry and analysis respectively.
Descriptive statistics were computed to characterize the study population in terms of sociodemographic and other pertinent factors. The relationship between each independent variable and outcome variable was initially determined by bivariable logistic regression analysis and variables with a p-value less than 0.2 were subsequently included in the multivariable analysis. Finally, variables with a p-value ≤ 0.05 were considered to be significantly associated factors with women's satisfaction with CAC services. The direction and strength of the associations were determined by the adjusted odds ratio (AOR). Hosmer-Lemeshow goodness of fit test was used to evaluate the fitness of the final model.
Operational definition
Comprehensive abortion care refers to providing safe induced abortion for all legal indications allowed by national law as well as providing elements of post abortion contraceptives (28).
Measurements
Women's satisfaction with CAC was measured using a composite variable with multiple indicators (physical environment, technical quality of provider, information provision, privacy and confidentiality). The satisfaction level of women was measured by 20 five-point Likert scale questions ranging between 0 and 4 (0 = neutral, 1 = strongly disagree, 2 = disagree, 3 = agree & 4 = strongly agree). The scores for each domain were calculated by summing the answers to all items in each domain. The overall and component wise satisfaction scores were categorized into two groups based on the mean score. Women who scored mean and above were categorized as satisfied, whereas those who scored below the mean were categorized as unsatisfied (13, 15, 29).
Ethics approval and informed consent
The study followed the principles outlined in the Declaration of Helsinki. Ethical approval was obtained from the Ethical Review Board (30) of the University of Gondar (Reference number: 189/11/2022). A permission letter for each hospital was obtained from the Amhara Public Health Institute. Before data collection, the study participants were informed about the purpose of the study and their right to decline participation or discontinue the interview at any time. Written informed consent was obtained from each participant and/or their caregivers or legal representatives for underage and illiterate participants on their behalf. Their confidentiality was maintained by omitting personal identifiers from the data collection tool.
Results
Sociodemographic characteristics of the study participants
A total of 333 women were interviewed, yielding a 100% response rate. The mean age of the study participants was 25.3 years (standard deviation ± 4.9). Of the total participants, the majority (82.6%) were Orthodox Christians by religion, 58% lived in urban areas, and 46.5% had no formal education. (Table 1).
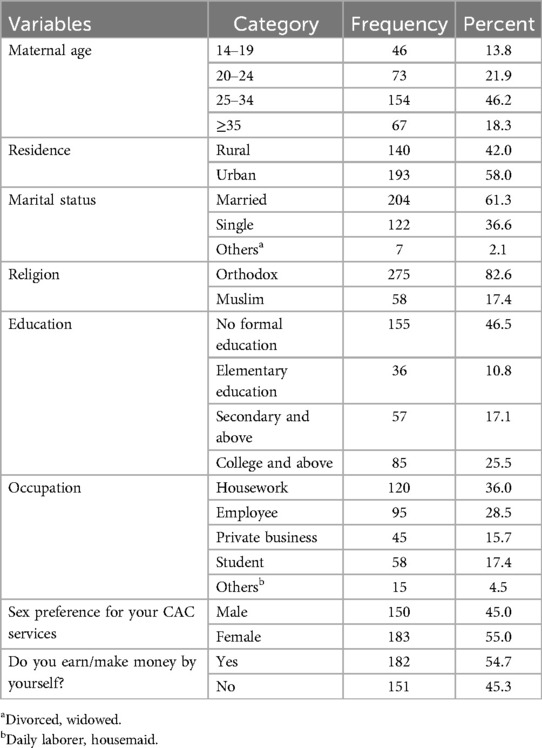
Table 1. Sociodemographic characteristics of the study participants in public primary hospitals of central Gondar zone, Amhara regional state, Ethiopia, 2022/2023 (n = 333).
Abortion care-related characteristics of the study participants
More than half 184(55.3%) of the participants were experienced first trimester abortion by gestational age (GA), and 177(53.2%) of the participants utilized abortion medication as a method of uterine evacuation (Table 2).
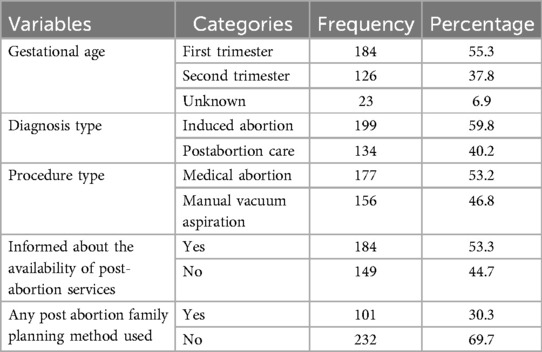
Table 2. Abortion care-related characteristics of the study participants in public primary hospitals of central Gondar zone, Amhara regional state, Ethiopia, 2022/2023 (n = 333).
Level of women's satisfaction with the given abortion care services
Participants were asked to assess their level of satisfaction with the given abortion healthcare services using five item dimensions, such as the physical environment, quality of care, information provision, and privacy and confidentiality. In this analysis, women's satisfaction with privacy and confidentiality accounted for the highest proportion (72.1%). Overall women satisfaction with comprehensive abortion care services was 60.4%, with a 95% CI (55.0, 66.0) (Figure 1).
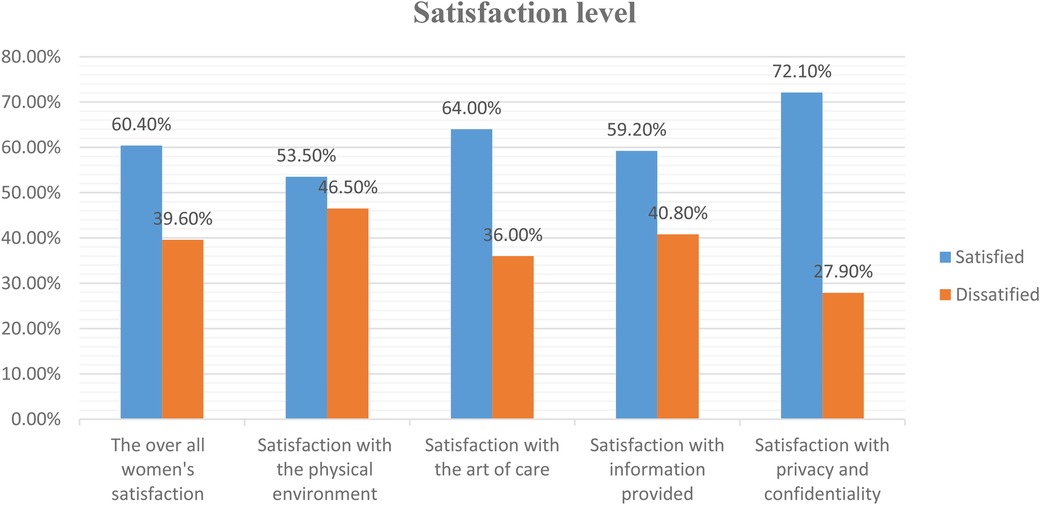
Figure 1. Level of women's satisfaction with each item dimension and overall satisfaction with comprehensive abortion healthcare services in central Gondar zone public primary hospitals, Amhara regional state, Ethiopia, 2022/23.
Factors associated with the level women's satisfaction
To identify the variables related to women's satisfaction, bivariable and multivariable logistic regression analysis were performed. According to the bivariable logistic regression analysis, women's age of 20–24 and 25–34 years, being a rural resident, being a student, and utilizing abortion medication were associated with satisfaction. In the final model women's age of 20–24 years, occupation as a student and use of abortion medication were independently and significantly associated with women's satisfaction.
Compared to women under twenty years of age, women aged twenty to twenty-four years had 2.94 times greater odds of being satisfied with their CAC services (AOR = 2.94, 95% CI: 1.02, 8.48). Similarly, the odds of women's satisfaction with CAC services among women whose occupation was student were 2.88 times higher than those among whose occupation was housework (AOR = 2.88; 95% CI: 1.10, 7.51). Furthermore, respondents who utilized abortion medication as a method of uterine evacuation were 4.41 times more likely to be satisfied with CAC services than that of those who used the surgical method (AOR = 4.41, 95% CI: 2.59, 7.48) (Table 3).
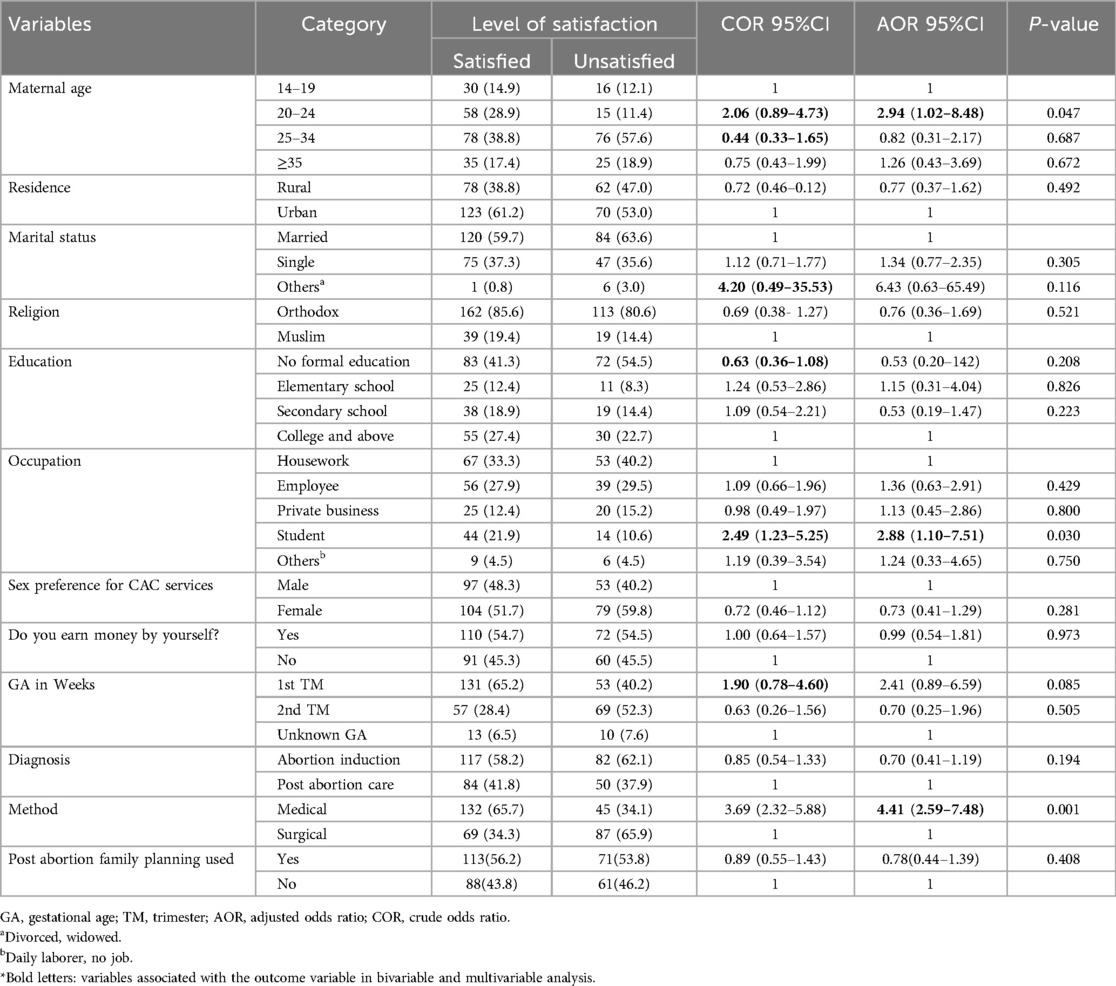
Table 3. Bivariable and multivariable analysis results to identify associated factors with women's satisfaction with CAC services in central Gondar zone public primary hospitals, Amhara regional state, Ethiopia, 2022/2023.
Discussion
Abortion remains a complex and contentious issue globally, shaped by cultural, religious, legal, and healthcare factors. Several scientific studies have examined how satisfied patients are with their healthcare services, highlighting how crucial it is to make sure that the services are of a standard that meets patients’ expectations. Evaluating women's satisfaction with abortion care services in Ethiopia is especially important to make sure services meet women's needs, where access to complete reproductive health treatments is not satisfactory. It provides data for policy insight to improve the accessibility and quality of abortion services and patient-centered care. It also helps to create a healthcare system that upholds the reproductive rights of women, offers high-quality care, and advances their general wellbeing. Patients have specialized knowledge and experience that can be applied to enhance clinical outcomes, quality of care, patient experiences, patient autonomy, research relevance and impact, and public trust in research, it is crucial for them to participate collectively in research (30).
This study assessed the level of women's satisfaction and associated factors with comprehensive abortion care services in Central Gondar Zone public primary hospitals in the Amhara Regional State, Ethiopia. Thus, the prevalence of women's satisfaction with comprehensive abortion care services was 60.4%, with a 95% CI (55.0, 66.0). A woman's age between 20 and 24 years, being a student, and using abortion medication as a method of uterine evacuation were identified as factors associated with women's satisfaction.
The finding of this study are comparable to those of the studies done in Addis Ababa and Mojo town (15, 16). However, this result is lower than those of studies in Jimma (23), the Gambela region (13), and Kenya (31) and higher than those of studies done in northwest Ethiopia (17) and the Tigray region (25).
The variation in the study setting and time, sample size, and sociocultural background of the study subjects could be the cause of the disparity in the level of satisfaction with the services. One explanation for the lower prevalence in the current study might be because some previous studies evaluated the satisfaction levels of women who had only medical abortions. The observed discrepancy may also be explained by variations in the attitudes and abilities of healthcare providers, difficulties in adhering to clinical protocols, and a lack of appropriate equipment at the health institution.
Those respondents who utilized abortion medication for uterine evacuation were 4.41 times more likely to be satisfied with abortion care services than those who utilized surgical methods. This result is consistent with the research finding in Mojo town. One possible explanation is that women may experience pain and discomfort associated with the surgical process. Additionally, a lower level of satisfaction may also result from not receiving counseling or from not using pain management therapy during the procedure. Abortion patients should have access to accurate information and counseling both before and after the procedure. Providers should educate women on the characteristics of abortion methods during counseling sessions and assist them in choosing the best option for them (32).
However, this result contradicts the findings of Addis Abeba, which reported that women who underwent surgical abortion were more satisfied than women who received abortion medication (16). The possible reason might be the expectations and awareness of the respondents about the methods; women in urban residences have adequate information due to better access to various health facilities and more media exposure, which may increase their expectations that surgical methods are associated with pain and discomfort (16). Furthermore, in one randomized trial of women randomized to surgical abortion, 92% stated that they would choose a surgical method for their next abortion, whereas only 63% of women randomized to medical abortion would choose that option in the future (33).
The odds of women's satisfaction with comprehensive abortion care services were 2.94 times greater among women aged is between 20 and 24 years. This is might be because of young women may not have a better understanding of the risks and benefits of abortion in their lives, as they are focused only on ending unwanted pregnancies to avoid social stigma regardless of the standard of treatment.
Women's occupation is also a significant factor for women's satisfaction; being a student was highly likely to be more satisfied with comprehensive abortion care services compared to those whose occupations involved housework. This might be because students might have limited information about the quality of abortion services and low expectations anticipating that they may not be well treated by providers due to interference with their pregnancies, which means that less educated clients may not request for better services (15).
However, this finding differs from those of previous studies conducted in Jimma (23) and Addis Abeba (16), which reported that employed women were more likely to be satisfied with services than those in other occupations. Patients with greater education are able to express their needs and preferences more clearly, which enables medical professionals to give more individualized and fulfilling care. Patients feel more confident and satisfied with their healthcare experiences when they are equipped with the knowledge necessary to make educated decisions regarding their sexual health. Additionally, employed women have better communication with healthcare providers, which may help them understand the scarcity of resources available in health facilities to deliver procedures accordingly (17). Therefore, the possible reason for the discrepancy may be due to the difference in study settings and populations.
Comprehensive sexual and reproductive health (SRH) education plays a crucial role in increasing patient satisfaction and promoting overall health and well-being. It provides information on safe sex practices, contraception, helping to prevent sexually transmitted infections (STIs) and unwanted pregnancies, and enabling early detection of potential health issues. Therefore, healthcare providers can significantly enhance patient satisfaction and promote general health and well-being, which will result in healthier individuals and communities, by incorporating sexual health education into patient treatment.
In summary ensuring high-quality abortion care and improving women's satisfaction involves addressing multiple facets of service delivery, including clinical quality, emotional support, accessibility, and respect for women's autonomy. Comprehensive sexual and reproductive health education is also essential for empowering women to make informed decisions.
The strengths and limitations of the study
The 100% response rate was maintained to investigate the multifactorial nature of women's satisfaction. Furthermore, this study identified contributing factors that grab attention to enhance the quality and increase women's satisfaction with CAC services. Some of the limitations of this study are that, although satisfaction is a process, it was assessed at one point in time, and this might underestimate the level of women's satisfaction. Given that the data were gathered through face-to-face interviews, social desirability bias might have been introduced.
Conclusions
This study revealed that 60.4% of women were satisfied with comprehensive abortion care services. Women's age of 20–24 years, being a student, and utilizing a medical abortion were factors associated with women's satisfaction with CAC services. To improve women's satisfaction with abortion care services, requires a holistic approach to abortion care, including better information provision, enhanced privacy and confidentiality, and quality healthcare services. Thus, all the concerned bodies should focus on advancing these factors to improve the quality of care and increase women's satisfaction with CAC services. In order to fully understand factors that influence comprehensive abortion care services longitudinal study recommended.
Data availability statement
The Datasets are found from the corresponding author upon request.
Ethics statement
Ethical approval was obtained from the Ethical Review Board (30) of the University of Gondar (Reference number: 189/11/2022). A permission letter for each hospital was obtained from the Amhara Public Health Institute. Study participants were informed about the purpose of the study, the importance of their participation, and their rights. Written informed consent was taken before the actual data collection.
Author contributions
NST and GMG involved extensive contributions to conception and design. BAK, GMG, and NST performed the statistical analysis. All authors contributed to the interpretation of data and writing of the manuscript. MBA, BKR, MMB, and MSM also participated in revising the article and offered final approval of the articles to be published.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors would like to thank the University of Gondar for providing them with ethical approval to carry out this research. Authors would also like to acknowledge the health facilities’ staff their support, study participants, data collectors, and supervisors for participation during the data collection process.
Conflict of interest
The authors declare that there are no conflicts of interest regarding the publication of this article.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
AOR, adjusted odds ratio; CAC, comprehensive abortion care; CI, confidence interval; COR, crude odds ratio; GA, gestational age; TM, trimester.
References
1. World Health Organization Abortion definitions. Available online at: https://www.emedicinehealth.com/what_is_abortion_according_to_who/article_em.htm (Accessed March 31, 2022).
2. Ajmal M, Sunder M, Akinbinu R. Abortion. In: StatPearls. Treasure Island, FL: StatPearls Publishing (2023). Available online at: https://www.ncbi.nlm.nih.gov/books/NBK518961/ (Updated July 10, 2023)
3. Agula C, Henry EG, Asuming PO, Agyei-Asabere C, Kushitor M, Canning D, et al. Methods women use for induced abortion and sources of services: insights from poor urban settlements of Accra, Ghana. BMC Womens Health. (2021) 21(1):300. doi: 10.1186/s12905-021-01444-9
4. Shakhatreh HJM, Salih AJ, Aldrou K, Alazzam FAF, Issa MSB. Medico-legal aspects of abortion: updates of the literature. Med Arch. (2022) 76(5):373–6. doi: 10.5455/medarh.2022.76.373-376
5. Feyssa MD, Gebru SK. Liberalizing abortion to reduce maternal mortality: expanding access to all Ethiopians. Reprod Health. (2022) 19(1):151. doi: 10.1186/s12978-022-01457-z
6. Holcombe SJ, Kidanemariam Gebru S. Agenda setting and socially contentious policies: Ethiopia’s 2005 reform of its law on abortion. Reprod Health. (2022) 19(Suppl 1):218. doi: 10.1186/s12978-021-01255-z
7. Baum SE, Wilkins R, Wachira M, Gupta D, Dupte S, Ngugi P, et al. Abortion quality of care from the client perspective: a qualitative study in India and Kenya. Health Policy Plan. (2021) 36(9):1362–70. doi: 10.1093/heapol/czab065
8. Cioffi A, Cecannecchia C, Cipolloni L, Santurro A, Cioffi F. The importance of the international community in protecting the right to abortion: the cases of malta and of the US supreme court. Healthcare. (2023) 11(4):520. doi: 10.3390/healthcare11040520
9. Organization WH. World Health Organization Global and Regional Estimates of the Incidence of Unsafe Abortion 2008. World Health Organization (2011). Available online at: https://www.who.int/publications/i/item/9789241501118#:∼:text=An%20estimated%2021.6%20million%20unsafe,women%20aged%2015%E2%80%9344%20years (Accessed June 16, 2011).
10. World health organization. World Health Organization Fact sheets. Available online at: https://www.who.int/news-room/fact-sheets/detail/abortion (Accessed May 17, 2024).
11. Sayami JT. Trends in comprehensive abortion care (CAC) and characteristics of women receiving abortion care in a tertiary hospital in Nepal. BMC Womens Health. (2019) 19(1):1–7. doi: 10.1186/s12905-019-0739-9
12. Berhan Y, Berhan A. Causes of maternal mortality in Ethiopia: a significant decline in abortion related death. Ethiop J Health Sci. (2014) 24:15–28. doi: 10.4314/ejhs.v24i0.3S
13. Teshome E, Adhena G. Client satisfaction in the quality of post abortion care among women attending in public health facility of Gambella, Ethiopia. J Gynecol Obstet. (2021) 9(3):66–74. doi: 10.11648/j.jgo.20210903.13
14. Dibaba Y, Dijkerman S, Fetters T, Moore A, Gebreselassie H, Gebrehiwot Y, et al. A decade of progress providing safe abortion services in Ethiopia: results of national assessments in 2008 and 2014. BMC Pregnancy Childbirth. (2017) 17(1):1–12. doi: 10.1186/s12884-017-1266-z
15. Oda T, Sento M, Negera A. Women’s satisfaction with abortion care and associated factors in public health facilities of Mojo town, east Ethiopia. Int J Reprod Med. (2023) 2023(1):4726878. doi: 10.1155/2023/4726878
16. Mossie Chekol B, Abera Abdi D, Andualem Adal T. Dimensions of patient satisfaction with comprehensive abortion care in Addis Ababa, Ethiopia. Reprod Health. (2016) 13(1):1–10. doi: 10.1186/s12978-016-0259-0
17. Gashaye KT, Taddese AA, Birhan TY. Prevalence and determinants of women’s satisfaction on the quality of safe abortion service in northwest Ethiopia. Arch Public Health. (2022) 80(1):146. doi: 10.1186/s13690-022-00897-0
18. Ervin NE. Does patient satisfaction contribute to nursing care quality? J Nurs Adm. (2006) 36(3):126–30. doi: 10.1097/00005110-200603000-00005
19. Jewkes RK, Gumede T, Westaway MS, Dickson K, Brown H, Rees H. Why are women still aborting outside designated facilities in metropolitan South Africa? BJOG. (2005) 112(9):1236–42. doi: 10.1111/j.1471-0528.2005.00697.x
20. Gietaneh W, Alle A, Alene M, Assemie MA, Simieneh MM, Birhanu MY. Quality disparity in terms of clients’ satisfaction with selected exempted health care services provided in Ethiopia: meta-analysis. Health Policy Open. (2022) 3:100068. doi: 10.1016/j.hpopen.2022.100068
21. Eboigbe E, Gadama L, Filippi V, Mehrtash H, Adu-Bonsaffoh K, Bello FA, et al. Adolescents’ satisfaction with care for abortion-related complications in 11 sub-Saharan African countries: a cross-sectional facility-based study. Int J Gynaecol Obstet. (2022) 156:63–70. doi: 10.1002/ijgo.13896
22. Asrat W, Mekonnen T, Bedimo M. Assessment of women’s satisfaction with family planning service at public health facilities in northwest region of Ethiopia: a cross sectional study. Contracept Reprod Med. (2018) 3(1):1–8. doi: 10.1186/s40834-018-0079-4
23. Kitila SB, Yadassa F. Client satisfaction with abortion service and associated factors among clients visiting health facilities in Jimma town, Jimma, south west, Ethiopia. Qual Prim Care. (2016) 24(2):67–76.
24. Wu JP, Godfrey EM, Prine L, Andersen KL, MacNaughton H, Gold M. Women’s satisfaction with abortion care in academic family medicine centers. Fam Med. (2015) 47(2):98–106.25646981
25. Demtsu B, Gessessew B, Alemu A. Assessment of quality and determinant factors of post-abortion care in governmental hospitals of Tigray, Ethiopia, 2013. Fam Med Med Sci Res. (2014) 3(4). doi: 10.4172/2327-4972.1000140
26. Taylor D, Postlethwaite D, Desai S, James EA, Calhoun AW, Sheehan K, et al. Multiple determinants of the abortion care experience: from the patient’s perspective. Am J Med Qual. (2013) 28(6):510–8. doi: 10.1177/1062860613484295
27. Obsie GW. Quality of post abortion care and service satisfaction among women who received the Post Abortion Care Service in Dilla University Referral Hospital, SNNPR, Ethiopia. Age. (2020) 15(20):6. doi: 10.13140/RG.2.2.12636.77446
28. Foster AM, Evans DP, Garcia M, Knaster S, Krause S, McGinn T, et al. The 2018 inter-agency field manual on reproductive health in humanitarian settings: revising the global standards. Reprod Health Matters. (2017) 25(51):18–24. doi: 10.1080/09688080.2017.1403277
29. Sheldon W, Blum J, Vogel J, Souza J, Gülmezoglu A, Winikoff B, et al. Postpartum haemorrhage management, risks, and maternal outcomes: findings from the world health organization multicountry survey on maternal and newborn health. BJOG. (2014) 121:5–13. doi: 10.1111/1471-0528.12636
30. Westerink HJ, Oirbans T, Garvelink MM, van Uden-Kraan CF, Zouitni O, Bart HA, et al. Barriers and facilitators of meaningful patient participation at the collective level in healthcare organizations: a systematic review. Health Policy. (2023) 138:104946. doi: 10.1016/j.healthpol.2023.104946
31. Evens E, Otieno-Masaba R, Eichleay M, McCARRAHER D, Hainsworth G, Lane C, et al. Post-abortion care services for youth and adult clients in Kenya: a comparison of services, client satisfaction and provider attitudes. J Biosoc Sci. (2014) 46(1):1–15. doi: 10.1017/S0021932013000230
32. Harvey SM, Beckman LJ, Satre SJ. Choice of and satisfaction with methods of medical and surgical abortion among U.S. clinic patients. Fam Plann Perspect. (2001) 33(5):212–6. doi: 10.2307/2673784
Keywords: abortion care service, Women's satisfaction, sexual and reproductive health, public hospital, Ethiopia
Citation: Tibebu NS, Alemu MB, Rade BK, Kassie BA, Bicha MM, Mihret MS and Gedef GM (2024) Women's satisfaction with comprehensive abortion care services and associated factors in central Gondar zone public primary hospitals, northwest Ethiopia, 2023. Front. Reprod. Health 6:1400359. doi: 10.3389/frph.2024.1400359
Received: 13 March 2024; Accepted: 30 August 2024;
Published: 1 October 2024.
Edited by:
Jessie Ford, Columbia University, United StatesReviewed by:
Babatunde A. Gbolade, BLG ASSIST, United KingdomCamilla Cecannecchia, Sapienza University of Rome, Italy
Copyright: © 2024 Tibebu, Alemu, Rade, Kassie, Bicha, Mihret and Gedef. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Getachew Muluye Gedef, Z2V0YWNoZXcubXVsdXllMjFAZ21haWwuY29t