 Mayra Perez
Mayra Perez Allyson Kelley
Allyson Kelley
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Reprod. Health , 07 May 2024
Sec. Adolescent Reproductive Health and Well-being
Volume 6 - 2024 | https://doi.org/10.3389/frph.2024.1244135
This article is part of the Research Topic Sexual Health Week 2022 View all 7 articles
Introduction: School-based health centers (SBHCs) are an evidence-based model for providing contraceptives to adolescents. SBHCs ability to provide reproductive health services is often limited by school district policies, state laws, and health center policies.
Methods: We used data from the Teens Exploring and Managing Prevention (TEMPO) study to document demographic characteristics and birth control methods among patients at four SBHCs in New Mexico. A total of 264 teens were included in the baseline data collection at SBHCs in New Mexico. A baseline survey was administered via iPad, that specifically focused on questions related to sexual experiences and sexual health topics. Baseline questions included demographic questions, gender identity, sexual orientation, reasons for visits, reproductive practices, and birth control methods. Descriptive statistics were calculated, including means and standard deviations for continuous variables and categorical frequencies.
Results: Our findings present reproductive health behaviors among New Mexican patients attending schools with SBHCs. More than 74% of respondents were Hispanic or Latino. The most common reason teens went to the SBHC was for birth control, and just 62% of teens reported using birth control methods in the past.
Discussion: These behaviors are essential for policymakers to consider as they address policy gaps, the complex landscape of parental permission, reproductive rights, and health as a human right.
School-based health centers (SBHCs) are an evidence-based model for providing contraceptives to adolescents (1). SBHCs play a vital role in providing healthcare services for many underserved populations of children and adolescents in the United States (2). Many SBHC patients lack insurance and may not have regular access to a primary care doctor or health education resources (1). Previous reports indicate that 70% of SBHC patients were racial or ethnic minorities and frequently residents with lower socioeconomic status (3). Offered at elementary, middle, and high schools throughout the country, SBHCs provide a variety of healthcare services on and off school property including sexual health education and reproductive health services (4). While SBHCs are lauded as an effective population-based strategy to support healthy sexual behaviors, their ability to provide reproductive health services is limited by school district policies, state laws, and health center policies (5, 6). A key issue in the provision of services at SBHCs is minors' consent for health care services and the HIPPA Privacy Rule [45 CFR 164.502(g)], which states a parent or guardian has access to their child's medical records. While New Mexico is included as one of the 23 states and the District of Columbia that allow all minors to consent to contraceptive services, the majority of states in the US do not (7).
New Mexico laws allow healthcare providers (and SBHCs) to provide examinations and services for sexually transmitted diseases, pregnancy, contraception, emergency conditions, and mental health/substance use (8). While one would think that these laws would ease access to reproductive health services and improve reproductive health outcomes in New Mexico, the data tell a different story. Teen birth rates have decreased in the US, and other key health indicators have improved; however, New Mexico lags behind. Key health indicators related to reproductive health in New Mexico underscore the need for reproductive health services. Based on 2020 data, the fertility rate is 54.6 per 1,000 women (15–44 years of age), the teen birth rate is 21.9 per 1,000 births (females 15–19 years of age), and the infant mortality rate is 5.1 per 1,000 (deaths per 1,000 live births) infant deaths (9). Teen birth rates are one indicator of reproductive health services, and New Mexico has the 10th highest teen birth rate in the US (Mississippi is the highest with 27.9 per 1,000, and Massachusetts is the lowest with 6.1 per 1,000) (9).
Place, race, and poverty contribute to high teen birth rates. New Mexico is home to more than 2 million people, and 50% are Hispanic or Latino (10). Poverty is common; 18.4% of residents living below the federal poverty level and a median household income of $54,020 (10) do not have health insurance. SBHCs address poverty and the lack of insurance in New Mexico school-aged residents. As of 2022, there were 78 SBHCs in New Mexico and 52 of these SBHCs are contracted with the Department of Health to bill Medicaid (11). Yet, there have been inadequate studies that examined the reproductive health practices of patients enrolled in SBHCs in New Mexico. Documenting the characteristics and reproductive health behaviors of SBHC patients in New Mexico is the first step in designing effective interventions that promote healthy reproductive practices in youth.
We used data from the Teens Exploring and Managing Prevention (TEMPO) study to document demographic characteristics and birth control methods among patients at four SBHCs in New Mexico. Data was collected in November 2016 and supported the purpose of the TEMPO study, which was to evaluate a brief intervention for unintended teenage pregnancy. Teens recruited for the TEMPO study were required to be between the ages of 13 to 19, report unprotected vaginal sex in the past year, and not currently have a Long-Acting Reversible Contraceptive (LARC). Screening questions included these numerous public health-related topics, such as the number of servings of vegetables and fruits eaten per week and questions related to sexual health. The queries related to sexual experiences included asking teens whether or not they have had vaginal intercourse and if so, whether it was protected or unprotected sex. Teens who reported unprotected sex were deemed eligible for the study. Those interested in participating were approved for the study and asked to provide follow-up contact information. Parents provided permission to participate in the TEMPO study. The youth provided assent. After permission and assent was obtained from the teen, a baseline survey was administered via iPad, that specifically focused on questions related to sexual experiences and sexual health topics. Baseline questions included demographic questions, gender identity, sexual orientation, reasons for visits, reproductive practices, and birth control methods. Responses included fixed and scale options. Scales were based on 0–10, where 0 represented the lowest score for example, “Not confident at all,” and 10 represented the highest score, “Extremely confident”. Questions regarding reproductive practices were based on a 0–10 scale where 0 represents “Not important at all,” and 10 represents the highest score, “Extremely important”. After completion of the baseline survey, participants were randomized into one of two groups: intervention or control for the larger study. This paper presents only baseline data from patients at SBHCs enrolled in the TEMPO study. Descriptive statistics were calculated, including means and standard deviations for continuous variables and categorical frequencies. The mean scores presented are based on a scale of 0–10.
Table 1 presents the percentage of responses from patients involved in the TEMPO study and baseline data collection.
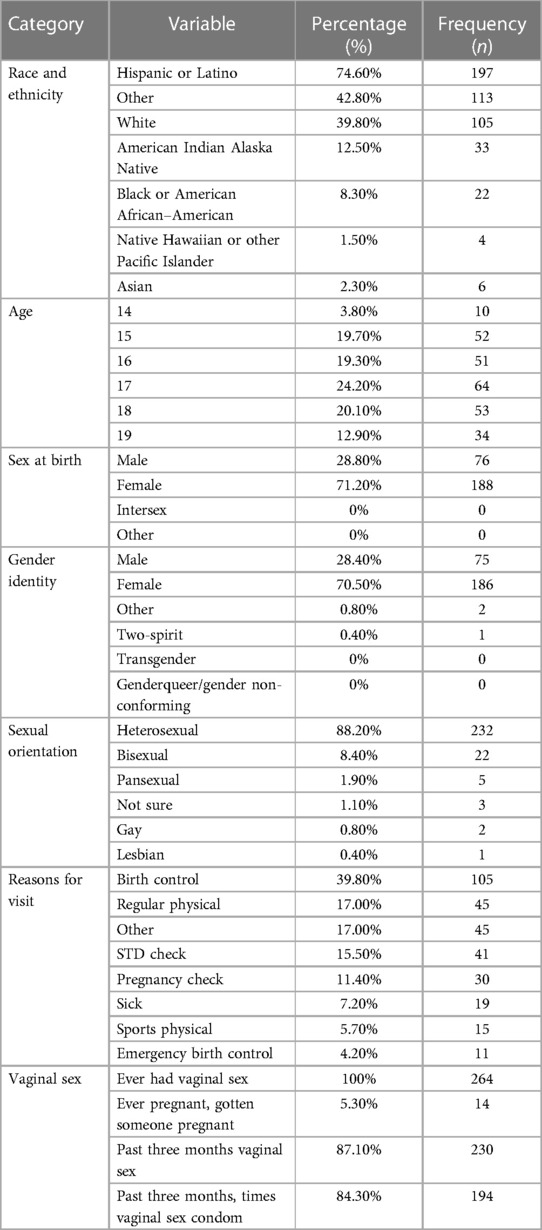
Table 1. Characteristics of New Mexico patients at SBHCs (n = 264).
A total of 264 teens were included in the baseline data collection at SBHCs in New Mexico; five were omitted due to missing data. Most teens were heterosexual females between the ages of 17 and 18. Reasons for visiting the SBHC varied, from regular physicals (39.8%) to emergency birth control (4.2%). Regarding sexual activity, 87.1% reported vaginal sex in the past three months, and 84.3% reported they used a condom during vaginal sex in the past three months.
Table 2 presents reproductive practices, importance of reproductive behaviors, and methods of birth control.
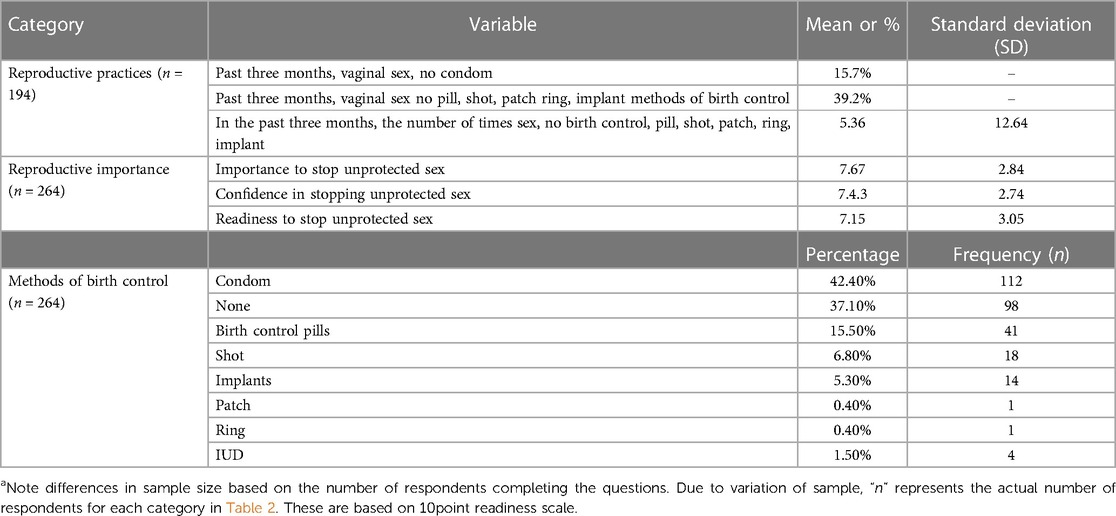
Table 2. Reproductive practices of SBHC patientsa.
Patients report having vaginal sex in the past three months an average of 7.62 times without a condom and 7.36 times with other birth control methods. In contrast, patients reported having vaginal sex 5.36 times with no birth control method. Patients reported a moderate to high level of importance to stop unprotected sex, confidence to stop unprotected sex, and readiness to stop unprotected sex (all mean scores >7.15 based on a 10-point scale). The most frequent method of birth control was condoms (42.4%) and the least was the patch or ring (0.4%).
We explored student reproductive health practices at SBHCs in New Mexico. We found that the majority of eligible patients were females, and their sexual orientation varied from heterosexual, bisexual, pansexual, not sure, gay, and lesbian. While sexual minority groups must be included as a priority population for SBHCs, they represented a relatively small percentage of patients in the baseline data. The majority were Hispanic or Latino. This is consistent with what we would expect since the majority of patients at SBHCs were Hispanic.
Regarding birth control methods, just 62.9% of patients in this study report they used birth control the last time they had sex. In contrast, 86% of teens in the US report they used birth control the last time they had sex and less than 5% of teens in the US on birth control use the most effective types (12). The most common method of birth control among patients in this study was a condom, this is consistent with previous literature on US teens where condoms were reported by 97% of teen females followed by withdrawal and the pill (13).
Patients in this study are ready to improve their reproductive health practices and report high levels of readiness and confidence about using birth control methods in the future. While similar studies are not available for comparison, we feel that this signifies these patients are ready for behavior change and services provided through SBHCs. Previous studies indicate that increased access to reproductive health services addresses barriers and stigma associated with seeking reproductive health resources (6, 14, 15). Researchers have found that school-based sexual and reproductive health education is effective in promoting healthy reproductive practices in youth, including delaying first sexual intercourse, reducing the number of sexual partners, decreasing the frequency of unprotected sex, increasing condom and contractive use, and gains in academic achievement and performance (1, 3).
One indicator of reproductive health service utilization is teen pregnancy rates. While New Mexico still ranks 10th in the US for teen pregnancy, this is an improvement from previous years. Strides may be attributed to increases in education and accessibility to methods of contraception in a SBHC setting (16). New Mexico has also increased low-cost family planning services through public health and primary care sites. However, continued advocacy and support of SBHCs are needed to close the gap and reduce teen pregnancy rates in New Mexico.
Adolescent populations in New Mexico benefit from having SBHCs in their communities. By having access to an SBHC, adolescents not only have access to a wide variety of treatments and resources, but they also have the autonomy to pursue health care anonymously and independently of parents and guardians. NM SBHCs are often able to reach and assist teens with sexual health concerns when others cannot. They do so by providing easy access to free contraception, using teen-friendly communication styles, and being easily accessible during the school day, thereby eliminating real/perceived barriers to reproductive/sexual health care.
Baseline data do not represent all youth seeking reproductive health services at SBHCs in New Mexico. These data provide a snapshot of the characteristics and choices. Moreover, findings from the larger TEMPO study were not analyzed or published due to staffing and leadership changes. Data were collected in November 2016 and since this time, there have been changes in the development of SBHCs, laws, and public health conditions related to the COVID-19 pandemic. Therefore, it is unclear how baseline responses changed as a result of the behavioral intervention. Racial and ethnic classifications are limited because the “other” category did not include specific information about what others represented. Responses are based on self-report data and subject to social desirability bias. For example, participants appear confident and ready to change behaviors, yet 37% use no birth control. Even with these limitations, this study provides the first-ever documentation of SBHC patients' reproductive characteristics in New Mexico.
Findings underscore the need for continued funding, policy, and advocacy around reproductive health and SBHCs. These efforts may be more beneficial in states like New Mexico where teen pregnancy rates are among the highest in the nation, and poverty and lack of medical insurance present gaps in access to services. New Mexico state laws that allow SBHCs to provide reproductive health services without parental permission (8) must be protected and continued.
Our findings present reproductive health behaviors among New Mexican patients attending schools with SBHCs. These behaviors are essential for policymakers and educators to consider as they navigate the complex landscape of consent, parental permission, reproductive rights, and health as a human right (4). Despite the United Nations Declaration that health is a human right (17), not every student or person in New Mexico has full access to services and resources that support and uphold this right. Moreover, continued efforts are necessary in New Mexico and throughout the world to meet the World Health Organization's Sustainable Development Goal Target 3.7 address sexual and reproductive health. This goal aims to ensure universal access to sexual and reproductive health services, and the integration of reproductive health into national strategies (18). SSBHCs in New Mexico and beyond must continue to reach students through innovative, on-site services that fill gaps in the current healthcare system. SBHCs are part of a global solution to lowering teen pregnancy and infant mortality rates and increasing access to care for all.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
MP was part of the TEMPO study and conceptualized this paper. AK assisted with writing the paper, analyzing data, and conducted the literature review. All authors contributed to the article and approved the submitted version.
The TEMPO Study is supported by Grant Number: TP2AH000028 through a cooperative agreement from the U.S. Department of Health and Human Services, Office of Adolescent Health. The contents are solely the responsibility of the authors and do not necessarily represent the official views of the U.S. Department of Health and Human Services or the Office of Adolescent Health.
We appreciate the SBHCs and youth participating in the baseline data collection for the TEMPO study.
AK is the Principal Consultant at Allyson Kelley and Associates PLLC and was contracted by the University of New Mexico.
The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Sullivan EE, Love HL, Fisher RL, Schlitt JJ, Cook EL, Soleimanpour S. Access to contraceptives in school-based health centers: progress and opportunities. Am J Prev Med. (2022) 62(3):350–59. doi: 10.1016/j.amepre.2021.08.030
2. Gustafson EM. History and overview of school-based health centers in the US. Nurs Clin North Am. (2005) 40(4):595–606, vii. doi: 10.1016/j.cnur.2005.08.001
3. The Guide to Community Preventive Services. Social Determinants of Health: Based School-Based Health Centers. (2015). Available online at: https://www.thecommunityguide.org/findings/social-determinants-health-school-based-health-centers.html (Accessed December 1, 2022).
4. Arenson M, Hudson PJ, Lee N, Lai B. The evidence on school-based health centers: a review. Glob Pediatr Health. (2019) 6:2333794X19828745. doi: 10.1177/2333794X19828745
5. Keeton V, Soleimanpour S, Brindis CD. School-based health centers in an era of health care reform: building on history. Curr Probl Pediatr Adolesc Health Care. (2012) 42(6):132–56. doi: 10.1016/j.cppeds.2012.03.002
6. Santelli JS, Nystrom RJ, Brindis C, Juszczak L, Klein JD, Bearss N, et al. Reproductive health in school-based health centers: findings from the 1998–99 census of school-based health centers. J Adolesc Health. (2003) 32(6):443–51. doi: 10.1016/s1054-139x(03)00063-6
7. Guttmacher Institute. “Minors’ Access to Contraceptive Services.” Washington, DC: Guttmacher Institute Minors’ Access to Contraceptive Services: State Laws and Policies. (2016). Available online at: https://www.guttmacher.org/state-policy/explore/minors-access-contraceptive-services (Accessed December 1, 2022).
8. State of New Mexico. Minors Consent for Health Care Services New Mexico. New Mexico Statutes Annotated. (2016). https://www.fnch.org/wp-content/uploads/2021/08/OSAH-SHM-14-MinorsConsentServices-NMSA.pdf (Accessed April 1, 2023).
9. Centers for Disease Control and Prevention. New Mexico. New Mexico Key Health Indicators. (2023). Available online at: https://www.cdc.gov/nchs/pressroom/states/newmexico/nm.htm (Accessed June 1, 2023).
10. U.S. Census. U.S. Census Bureau QuickFacts: New Mexico. (2022). Available online at: https://www.census.gov/quickfacts/fact/table/NM/HEA775221 (Accessed April 1, 2023).
11. State of New Mexico Human Services. School Based Health Centers | New Mexico Human Services Department. (2022). Available online at: https://www.hsd.state.nm.us/lookingforinformation/school-based-health-center-managed-care-organization-project/ (Accessed June 1, 2023).
12. Centers for Disease Control and Prevention. Preventing Teen Pregnancy. (2015). Available online at: https://www.cdc.gov/vitalsigns/pdf/2015-04-vitalsigns.pdf (Accessed June 1, 2023).
13. Abma J, Martinez G. Sexual activity and contraceptive use among teenagers in the United States, 2011–2015. Natl Health Stat Report. (2017) (104):1–23. https://www.cdc.gov/nchs/data/nhsr/nhsr104.pdf28696201
14. Deshmukh DD, Chaniana SS. Knowledge about sexual and reproductive health in adolescent school-going children of 8th, 9th, and 10th standards. J Psychosexual Health. (2020) 2(1):56–62. doi: 10.1177/2631831819898916
15. Minguez M, Santelli JS, Gibson E, Orr M, Samant S. Reproductive health impact of a school health center. J Adolesc Health. (2015) 56(3):338–44. doi: 10.1016/j.jadohealth.2014.10.269
16. Boonstra H. What Is Behind the Declines in Teen Pregnancy Rates? Washington, DC: Guttmacher Institute. (2014). https://www.guttmacher.org/gpr/2014/09/what-behind-declines-teen-pregnancy-rates (Accessed April 1, 2023).
17. United Nations. The Universal Declaration of Human Rights. Geneva: United Nations. (2015). https://www.un.org/en/about-us/universal-declaration-of-human-rights (Accessed April 1, 2023).
18. World Health Organization. Global Health Observatory. SDJ Target 3.7 Sexual and Reproductive Health. (2023). Available online at: https://www.who.int/data/gho/data/themes/topics/indicator-groups/indicator-group-details/GHO/sdg-target-3.7-sexual-and-reproductive-health#:∼:text=Indicator%20Groups-,SDG%20Target%203.7%20%7C%20Sexual%20and%20reproductive%20health%3A%20By%202030%2C,reproductive%20health%20into%20national%20strategies (Accessed June 1, 2023).
Keywords: school-based health center, reproductive health, teen, birth control, New Mexico
Citation: Perez M and Kelley A (2024) Reproductive behaviors among school-based health center clients in New Mexico. Front. Reprod. Health 6:1244135. doi: 10.3389/frph.2024.1244135
Received: 21 June 2023; Accepted: 8 April 2024;
Published: 7 May 2024.
Edited by:
Narges Sheikhansari, University of Exeter, United KingdomReviewed by:
Judith Herrman, University of Delaware, United States© 2024 Perez and Kelley. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mayra Perez bXBlcmV6MDVAc2FsdWQudW5tLmVkdQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.