
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Reprod. Health , 18 December 2023
Sec. Adolescent Reproductive Health and Well-being
Volume 5 - 2023 | https://doi.org/10.3389/frph.2023.1303218
This article is part of the Research Topic The Impact of Emerging Infections on Adolescent Sexual and Reproductive Health View all 5 articles
 Cory J. Cascalheira1*
Cory J. Cascalheira1* Tyler H. Pugh2Chenglin Hong3Michelle Birkett4,5
Tyler H. Pugh2Chenglin Hong3Michelle Birkett4,5 Kathryn Macapagal4,5Ian W. Holloway3
Kathryn Macapagal4,5Ian W. Holloway3
Compared to their heterosexual and cisgender peers, young sexual and gender minority (YSGM) people are more likely to contract sexually transmitted infections (STIs; e.g., HIV) and to face adverse consequences of emerging infections, such as COVID-19 and mpox. To reduce these sexual health disparities, technology-based interventions (TBIs) for STIs and emerging infections among YSGM adolescents and young adults have been developed. In this Perspective, we discuss ethical issues, ethical principles, and recommendations in the development and implementation of TBIs to address STIs and emerging infections among YSGM. Our discussion covers: (1) confidentiality, privacy, and data security (e.g., if TBI use is revealed, YSGM are at increased risk of discrimination and family rejection); (2) empowerment and autonomy (e.g., designing TBIs that can still function if YSGM users opt-out of multiple features and data collection requests); (3) evidence-based and quality controlled (e.g., going above and beyond minimum FDA effectiveness standards to protect vulnerable YSGM people); (4) cultural sensitivity and tailoring (e.g., using YSGM-specific models of prevention and intervention); (5) balancing inclusivity vs. group specificity (e.g., honoring YSGM heterogeneity); (6) duty to care (e.g., providing avenues to contact affirming healthcare professionals); (7) equitable access (e.g., prioritizing YSGM people living in low-resource, high-stigma areas); and (8) digital temperance (e.g., being careful with gamification because YSGM experience substantial screen time compared to their peers). We conclude that a community-engaged, YSGM-centered approach to TBI development and implementation is paramount to ethically preventing and treating STIs and emerging infections with innovative technology.
Adolescence and young adulthood (12–25 years old) are developmental periods when sexual health disparities in sexually transmitted infections [STIs; e.g., chlamydia, gonorrhea, human immunodeficiency virus (HIV)] emerge between young sexual and gender minority (YSGM) people (1) and their heterosexual and cisgender counterparts (2, 3). Without intervention, STI disparities persist across the life course (4). Evidence also indicates that YSGM people are at greater likelihood of (1) contracting certain emerging infections [e.g., mpox; (5)] and (2) developing more severe health outcomes from emerging infections [e.g., COVID-19; (6, 7)]. As such, there is an urgent need to develop and implement innovative interventions to reduce these sexual health disparities in YSGM people (8).
Technology-based interventions (TBIs), or the use of mobile and internet technologies for health prevention and remediation, are innovative solutions to reducing disparities in STIs and emerging infections among YSGM people. TBIs for STIs typically focus on enhancing STI prevention messaging, increasing STI testing, bolstering pre-exposure prophylaxis (PrEP) uptake, surveilling STI prevalence, improving adherence to medication, and connecting to wraparound services (9). Evidence indicates that TBIs for STIs can significantly improve medication adherence (e.g., pre-exposure prophylaxis) and clinic attendance, significantly reduce transmission risk behaviors, and are perceived as acceptable and feasible (1, 10). Among YSGM people, many of whom have limited knowledge of STIs given their age and reduced access to familial or peer supports, TBIs have the added benefit of accessibility outside of discriminatory medical environments (11). However, substantial gaps in TBIs for STIs and emerging infections remain, such as developing TBIs for subgroups of the YSGM community [e.g., sexual minority female adolescents (1)] and developing TBIs for emerging infections. As momentum builds to develop and implement TBIs to address these gaps, stakeholders must consider pertinent ethical issues and principles in working with YSGM people. In this Perspective, we discuss these ethical issues and principles as well as provide recommendations to navigate them.
Drawing from the ethical frameworks of the Belmont Report (12) and the American Psychological Association code of ethics (13), we identify eight ethical issues and principles that raise important questions during TBI development and implementation for YSGM at risk for STIs and emerging infections. Table 1 summarizes this Perspective's central recommendations as questions.
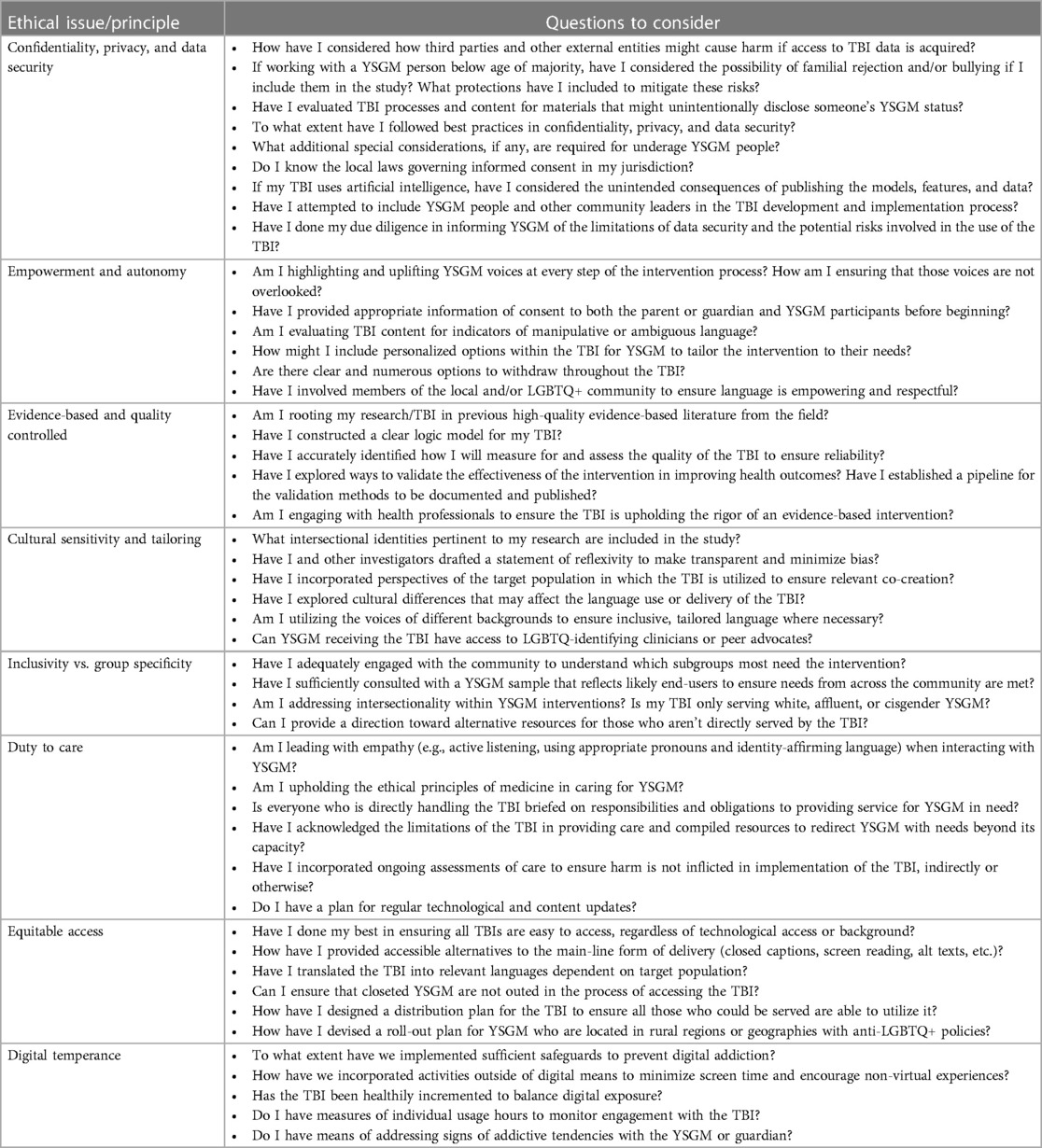
Table 1. A summary of ethical considerations.
Maintaining confidentiality, privacy, and data security is paramount for TBI research, but additional care is required when working with YSGM people because the consequences of data breach can be dire. Adolescence and young adulthood are periods when many YSGM people develop their identities and decide if and how to disclose their YSGM status (14). Identity disclosure during research has important interpersonal implications (15), and thus, researchers and clinicians must consider whether third parties might cause harm if access to TBI data is acquired (16). For example, some families may reject their YSGM teenager upon disclosure of their SGM status, possibly resulting in homelessness (17). Identity disclosure can also increase the risk of bullying and victimization in high-stigma areas (18). Unintentional disclosure might occur during TBI development and validation [e.g., having one YSGM person reach out to a closeted YSGM person via snowball sampling; (19)], content design (e.g., using rainbow images in an app's logo design), content storage [e.g., content stored on the cloud vs. locally on a YSGM person's smartphone; (20, 21)], or implementation (e.g., providing the TBI at a clinic where the YSGM person is out to the provider but not the parent).
In addition to best practices in maximizing confidentiality, privacy, and data security [e.g., anonymity, encryption, data held separately from identifiers; see (22)], we recommend the following.
1. Decide on the age range of the intended end user (23), as some issues related to unintentional identity disclosure can be avoided with older YSGM people.
2. Know the local laws about consent. In the United States, for example, parental or guardian permission may be waived if sufficient safeguards are available to protect children or adolescents, and provided that the waiver does not contradict laws (24).
3. In TBIs that use artificial intelligence, ensure that reverse engineering of features and models is unlikely by restricting the access and use of preprocessed data.
4. Conduct focus groups to understand how YSGM people might want the TBI presented (e.g., what images and language to use) to maximize confidentiality and privacy (25).
5. Involve YSGM at all stages of TBI development and implementation (e.g., advisory boards to provide input on local needs, technology preferences, concept design, recruitment materials, distribution points; stipends for youth to design social media outreach and visualizations of study findings) to ensure the processes are embedded in community norms and prioritize digital rights.
Non-affirming parenting practices (26), peer bullying (27), anti-YSGM language in public spaces (28), and anti-YSGM laws (29) disempower YSGM people. Because disempowering experiences drive YSGM health disparities (30), it is important to center empowerment and autonomy in TBIs. One method is to design TBIs that adequately function if YSGM users opt-out of multiple features and data collection requests. TBI developers could also provide opportunities to promote autonomous decision-making by designing modular TBIs [vs. linear and constrained; (31)], using visually based and easy to comprehend informed consent materials, and eliciting informed consent throughout the TBI (23). Another method might be featuring YSGM people as co-authors or co-developers of the TBI. For instance, if focus groups or advisory boards are used throughout TBI development and implementation as recommended in this perspective, YSGM who participate in such activities could be featured somewhere on the TBI explaining their contributions. This representation could convey a message of “for us by us” which, in turn, could help other YSGM people feel seen and valued.
In the United States, most TBIs are classified as low-to-moderate risk by the Food and Drug Administration (i.e., the nation's regulatory body for healthcare products), so they receive minimal premarket clinical testing (32). In this regulatory environment, venture capitalists are investing heavily in TBIs [$637 million in 2019; (33)]. As a result, TBIs may enter the market without adequate effectiveness evidence, leaving the burden of determining effectiveness on individual providers (16). Furthermore, the regulation of artificial intelligence in healthcare, including TBIs, is a moving target (34). These regulatory realities raise concerns about the extent to which TBIs are based on scientific evidence.
Regulatory limitations also underscore the potential for harm in rapid TBI development and implementation. YSGM people, given their increased vulnerability in healthcare settings relative to heterosexual and cisgender people (35), require extra care to reduce the potential of “technology-facilitated abuse” (36)—that is, the harm that derives from TBIs with poor validity, accuracy, safety, and scientific rigor. Even if a local jurisdiction does not require extensive effectiveness evidence, we charge TBI developers and providers to implement TBIs with YSGM people if and only if: (a) the TBI is technologically stable, has high fidelity, and yields clinically meaningful results (37); (b) implementation stakeholders are educated on the scientific evidence behind the TBI; (c) the TBI has a robust monitoring and evaluation plan (38); and (d) the TBI presents accurate claims of its effectiveness for YSGM people.
Without cultural sensitivity and tailoring, TBI uptake and effectiveness among YSGM people may be suboptimal. Research suggests that culturally tailored interventions tend to be effective among YSGM people (39–41), especially for non-White YSGM (42) and for outcomes like HIV (43, 44). From an implementation perspective, clinical practitioners who lack understanding of YSGM issues and concerns (45) may hinder TBI uptake. Thus, we caution against adapting extant TBIs to YSGM people without adequate consideration of how intervention components are delivered in a YSGM-affirming manner. Instead:
• Involve YSGM people at all stages of TBI development and implementation to reduce the chances that a TBI perpetuates stereotypes, promotes discrimination, or causes unintended harm;
• Co-design TBIs with clinical providers and end users (46–48) to help increase the health literacy of YSGM people and the cultural literacy of clinical providers.
• Use a community-engaged, YSGM-centered approach to TBI development and implementation to create partnerships with local YSGM-affirming clinical providers, local YSGM community organizations, national advocacy organizations, and academic research centers.
Special consideration for TBIs enhanced by artificial intelligence [e.g., a chatbot to increase demand for STI medications; (49)] is warranted because anti-YSGM bias may be integrated into the technological architecture of specific models [e.g., large language models (50)]. In these special cases, we recommend regular algorithmic auditing and validation [for more information, see (51)] as well as the creation of community-tailored algorithms, or artificial intelligence algorithms trained from the ground up using data from YSGM people.
Rates of STIs differ by gender identity and sexual orientation (52), necessitating the development of differentiated interventions for YSGM people. Moreover, majority group researchers, clinical providers, or public health officials may treat YSGM communities as a monolith even though members have intersectional identities (53), unique constellations of stressful experiences (54), and diverse healthcare experiences (55). Because YSGM people are a historically neglected population (56, 57), it can be tempting to overlook the heterogeneity of this group when developing TBIs for STIs and emerging infections. We encourage the careful consideration of whether the mechanisms of the TBI are broadly applicable to YSGM people, the execution of thorough acceptability and feasibility studies with YSGM subgroups, the matching of YSGM people with subgroup-specific interventions (58), and the adaptation of existing TBIs to specific subgroups [e.g., transgender youth; (1)].
TBIs should prioritize the long-term well-being of YSGM people with sustainable plans for TBI maintenance and appropriate connections to other forms of care. Developing, releasing, and forgetting a TBI is unacceptable because YSGM people constitute a vulnerable population. For instance, with an infection like HIV, it could be useful to design TBIs to connect to wraparound services. Furthermore, YSGM people may perceive TBIs for STIs and emergent infections as spaces to seek help for comorbid concerns, especially since YSGM-specific TBIs for mental health conditions are relatively lacking (1). Because suicide is alarmingly high in this population (59), careful attention to how high-risk suicidal behaviors may be disclosed in interactive components (e.g., forums, web chat) is warranted (60, 61). We recommend creating TBIs that have clear pathways to affirming healthcare providers, easy to access crisis lines, and ongoing plans for monitoring risk if interactive components are featured (e.g., passive-sensing suicide risk detection systems that alert clinical team members to perform a suicide assessment). For emergent infections, we encourage TBI developers to design technologies that connect to other forms of care (e.g., another TBI for sexual health) in the event that an infection is rapidly controlled.
We also recommend regular technological and content updates. Technological updates are important to ensure the TBI syncs with operating systems and does not pose a safety risk. Larger technological updates may be required if the TBI technology becomes substantially outdated or no longer meets user expectations. Regular content updates are also crucial. Information on STIs and emerging infections can rapidly develop, so it is important to have content that reflects new recommendations and science.
YSGM people who might most benefit from TBIs for STIs or emergent infections (i.e., YSGM people in high-stigma, low-resource areas) are also least likely to have the TBI developed with them. Many TBIs for YSGM people are developed in urban centers where YSGM people cluster (1, 44). Even in urban areas, facilitators of and barriers to healthcare resources within the YSGM community is not uniform (62). Thus, although it may be practical to roll out a TBI in urban centers with YSGM people that are easier to recruit (e.g., gay men presenting regularly at a sexual health clinic), we recommend that TBI stakeholders have a plan to scale up distribution of the TBI to YSGM people in high-need, underserved areas. Moreover, through the inequity of the technological landscape, access to broadband, Wi-Fi, and other technological pre-requisites to receiving care are inevitably variable. In response, adaptable interventions that can remain versatile to the access barriers of a given region become essential.
While TBIs offer solutions to address the disparities in STIs and emerging infectious disease outbreaks, it is important to acknowledge and minimize the potential harm in their implementation. Many TBIs inevitably increase the screen time among users. Previous research suggests that increased screen time is associated with poorer mental health, increased behavioral problems, worsening sleep quality, and other outcomes including poor academic performance (63, 64). Therefore, TBI development and implementation must consider the potential downside of excessive technology use. Similarly, there is a growing trend of integrating gamification and serious gaming in health and wellbeing promotion in recent years (65, 66). While these approaches could generate positive behavioral changes and cognitive outcomes, excessive use of such elements could lead to addiction-like behaviors, contributing to the already existing mental health inequities among YSGM. These considerations are particularly important given the recent statement from the U.S. Surgeon General on social media use and its impact on adolescents' mental health (67). Therefore, it is crucial for TBI developers and clinicians to strike a balance between optimizing TBI engagement for positive behavior changes and maintaining a moderate amount of technology use.
This Perspective discussed eight ethical issues and principles is designing and deploying TBIs for STIs and emerging infections, focusing on YSGM people as the target population. Ultimately, a community-engaged, YSGM-centered approach to TBI development and implementation is paramount to ethically treating STIs and emerging infections with innovative technology. Although some of the ethical issues, principles, and recommendations in this Perspective cut across populations, attention to how ethical considerations apply to YSGM people is crucial given the ethical infractions of extant computational technologies with this population (68, 69) as well as the health disparities observed between YSGM people and their heterosexual and cisgender peers (2, 3). Ethically robust TBI development and implementation is not only sound science, but is also a way to ensure systems of personal and public health remain spaces of help, healing, and hope at a time when YSGM people face an unprecedented assault on their basic human rights (29).
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
CC: Conceptualization, Funding acquisition, Supervision, Writing – original draft, Writing – review & editing. TP: Writing – original draft, Writing – review & editing. CH: Writing – original draft. MB: Writing – review & editing. KM: Writing – review & editing. IH: Conceptualization, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
CJC is supported as a RISE Fellow by the National Institutes of Health (R25GM061222). KM was supported in part by R01MH129207.
We used ChatGPT (based on the GPT-3.5 architecture; 14 March 2023 version; OpenAI, LLC) and Consensus (Consensus NLP, Inc.) during the brainstorming phase of this manuscript. All suggestions from these artificial intelligence (AI) systems were fact checked. AI was not used to author or edit any text in the present article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Gilbey D, Morgan H, Lin A, Perry Y. Effectiveness, acceptability, and feasibility of digital health interventions for LGBTIQ+ young people: systematic review. J Med Internet Res. (2020) 22(12):e20158. doi: 10.2196/20158
2. Everett BG, Schnarrs PW, Rosario M, Garofalo R, Mustanski B. Sexual orientation disparities in sexually transmitted infection risk behaviors and risk determinants among sexually active adolescent males: results from a school-based sample. Am J Public Health. (2014) 104(6):1107–12. doi: 10.2105/AJPH.2013.301759
3. Stutterheim SE, van Dijk M, Wang H, Jonas KJ. The worldwide burden of HIV in transgender individuals: an updated systematic review and meta-analysis. PLoS One. (2021) 16(12):e0260063. doi: 10.1371/journal.pone.0260063
4. Rice CE, Vasilenko SA, Fish JN, Lanza ST. Sexual minority health disparities: an examination of age-related trends across adulthood in a national cross-sectional sample. Ann Epidemiol. (2019) 31:20–5. doi: 10.1016/j.annepidem.2019.01.001
5. Philpott D, Hughes CM, Alroy KA, Kerins JL, Pavlick J, Asbel L, et al. Epidemiologic and clinical characteristics of monkeypox cases — United States, may 17–July 22, 2022. Morb Mortal Wkly Rep. (2022) 2022(71):1018–22. doi: 10.15585/mmwr.mm7132e3
6. Cascalheira CJ, Morrison C, D’Angelo AB, Garcia Villanueva O, Grov C. The impact of the COVID-19 pandemic on HIV-positive men who have sex with men: (dis)connection to social, sexual, and health networks. Psychol Sex. (2022) 14(1):306–20. doi: 10.1080/19419899.2022.2112745
7. Heslin KC, Hall JE. Sexual orientation disparities in risk factors for adverse COVID-19–related outcomes, by race/ethnicity — behavioral risk factor surveillance system, United States, 2017–2019. MMWR Morb Mortal Wkly Rep. (2021) 70:149–54. doi: 10.15585/mmwr.mm7005a1
8. Mustanski B, Macapagal K. Clinical psychological science must move beyond documenting disparities in LGBTQ health toward eliminating them. J Consult Clin Psychol. (2023) 91:57–9. doi: 10.1037/ccp0000800
9. Cao B, Bao H, Oppong E, Feng S, Smith KM, Tucker JD, et al. Digital health for sexually transmitted infection and HIV services: a global scoping review. Curr Opin Infect Dis. (2020) 33(1):44–50. doi: 10.1097/QCO.0000000000000619
10. Daher J, Vijh R, Linthwaite B, Dave S, Kim J, Dheda K, et al. Do digital innovations for HIV and sexually transmitted infections work? Results from a systematic review (1996–2017). BMJ Open. (2017) 7(11):e017604. doi: 10.1136/bmjopen-2017-017604
11. Cascalheira CJ, Flinn RE, Zhao Y, Klooster D, Laprade D, Hamdi SM, et al. Models of gender dysphoria using social media data for use in technology-delivered interventions: machine learning and natural language processing validation study. JMIR Form Res. (2023) 7:e47256. doi: 10.2196/47256
12. The National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research. The Belmont Report: Ethical principles and guidelines for the protection of human subjects of research. U.S. Department of Health & Human Services. Published 1979. Availbale at: https://www.hhs.gov/ohrp/regulations-and-policy/belmont-report/read-the-belmont-report/index.html (Accessed September 25, 2023).
13. American Psychological Association. Ethical principles of psychologists and code of conduct. Published 2017. Availbale at: https://www.apa.org/ethics/code/index (Accessed September 30, 2019).
14. Son D, Updegraff KA. Sexual minority adolescents’ disclosure of sexual identity to family: a systematic review and conceptual framework. Adolesc Res Rev. (2023) 8(1):75–95. doi: 10.1007/s40894-021-00177-y
15. Fisher CB, Mustanski B. Reducing health disparities and enhancing the responsible conduct of research involving LGBT youth. Hastings Cent Rep. (2014) 44(s4):S28–31. doi: 10.1002/hast.367
16. National Institute of Mental Health. Technology and the future of mental health treatment. National Institutes of Health. Published April 2021. Availbale at: https://www.nimh.nih.gov/health/topics/technology-and-the-future-of-mental-health-treatment (Accessed February 13, 2022).
17. Tierney WG, Ward JD. Coming out and leaving home: a policy and research agenda for lgbt homeless students. Educ Res. (2017) 46(9):498–507. doi: 10.3102/0013189X17733964
18. Collier KL, van Beusekom G, Bos HMW, Sandfort TGM. Sexual orientation and gender identity/expression related peer victimization in adolescence: a systematic review of associated psychosocial and health outcomes. J Sex Res. (2013) 50(3-4):299–317. doi: 10.1080/00224499.2012.750639
19. McInroy LB. Pitfalls, potentials, and ethics of online survey research: LGBTQ and other marginalized and hard-to-access youths. Soc Work Res. (2016) 40(2):83–94. doi: 10.1093/swr/svw005
20. Shafique M, Theocharides T, Bouganis C-S, Hanif MA, Khalid F, Hafiz R, et al. An overview of next-generation architectures for machine learning: roadmap, opportunities and challenges in the IoT era. 2018 Design, automation & test in Europe conference & exhibition (DATE) (2018). p. 827–32. doi: 10.23919/DATE.2018.8342120
21. Wu CJ, Brooks D, Chen K, Chen D, Choudhury S, Dukhan M, et al. Machine learning at Facebook: understanding inference at the edge. 2019 IEEE international symposium on high performance computer architecture (HPCA) (2019). p. 331–44. doi: 10.1109/HPCA.2019.00048
22. Thapa C, Camtepe S. Precision health data: requirements, challenges and existing techniques for data security and privacy. Comput Biol Med. (2021) 129:104130. doi: 10.1016/j.compbiomed.2020.104130
23. World Health Organization. Youth-centred digital health interventions: A framework for planning, developing and implementing solutions with and for young people. World Health Organization. Published July 19, 2021. Availbale at: https://www.who.int/publications/i/item/9789240011717 (Accessed July 31, 2023).
24. U.S. Department of Health & Human Services. Research with children FAQs. Office for Human Research Protections About OHRP Regulatio. Published 2023. Availbale at: https://www.hhs.gov/ohrp/regulations-and-policy/guidance/faq/children-research/index.html (Accessed September 25, 2023).
25. Peiris-John R, Dizon L, Sutcliffe K, Kang K, Fleming T. Co-creating a large-scale adolescent health survey integrated with access to digital health interventions. Digit Health. (2020) 6:2055207620947962. doi: 10.1177/2055207620947962
26. McCurdy AL, Russell ST. Perceived parental social support and psychological control predict depressive symptoms for lesbian, gay, bisexual, transgender, queer, or questioning youth in the United States. Child Dev. (2023) 94(3):691–705. doi: 10.1111/cdev.13894
27. Goldbach JT, Rhoades H, Rusow J, Karys P. The development of proud & empowered: an intervention for promoting LGBTQ adolescent mental health. Child Psychiatry Hum Dev. (2023) 54(2):481–92. doi: 10.1007/s10578-021-01250-2
28. Kosciw JG, Greytak EA, Zongrone AD, Clark CM, Truong NL. The 2017 national school climate survey: The experiences of lesbian, gay, bisexual, transgender, and queer youth in our nation’s schools. New York: GLSEN (2018).
29. Peele C. Roundup of anti-LGBTQ+ legislation advancing in states across the country. Human Rights Campaign. Published May 23, 2023. Availbale at: https://www.hrc.org/press-releases/roundup-of-anti-lgbtq-legislation-advancing-in-states-across-the-country (Accessed July 7, 2023).
30. Meyer IH. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: conceptual issues and research evidence. Psychol Bull. (2003) 129:674–97. doi: 10.1037/0033-2909.129.5.674
31. Smit ES, Zeidler C, Resnicow K, de Vries H. Identifying the most autonomy-supportive message frame in digital health communication: a 2(2 between-subjects experiment. J Med Internet Res. (2019) 21(10):e14074. doi: 10.2196/14074
32. Cortez NG, Cohen IG, Kesselheim AS. FDA regulation of mobile health technologies. N Engl J Med. (2014) 371(4):372–9. doi: 10.1056/NEJMhle1403384
33. Shah RN, Berry OO. The rise of venture capital investing in mental health. JAMA Psychiatry. (2021) 78(4):351–2. doi: 10.1001/jamapsychiatry.2020.2847
34. Gamble A. Artificial intelligence and mobile apps for mental healthcare: a social informatics perspective. Aslib J Inf Manag. (2020) 72(4):509–23. doi: 10.1108/AJIM-11-2019-0316
35. Williams KA, Chapman MV. Comparing health and mental health needs, service use, and barriers to services among sexual minority youths and their peers. Health Soc Work. (2011) 36(3):197–206. doi: 10.1093/hsw/36.3.197
36. Straw I, Tanczer L. Safeguarding patients from technology-facilitated abuse in clinical settings: a narrative review. PLoS Digit Health. (2023) 2(1):e0000089. doi: 10.1371/journal.pdig.0000089
37. Murray E, Hekler EB, Andersson G, Collins LM, Doherty A, Hollis C, et al. Evaluating digital health interventions: key questions and approaches. Am J Prev Med. (2016) 51(5):843–51. doi: 10.1016/j.amepre.2016.06.008
38. World Health Organization. Monitoring and Evaluating Digital Health Interventions: A Practical Guide to Conducting Research and Assessment. World Health Organization. (2016). Available at: https://apps.who.int/iris/bitstream/handle/10665/252183/?sequence=1.
39. Craig SL, Leung VWY, Pascoe R, Pang N, Iacono G, Austin A, et al. AFFIRM online: utilising an affirmative cognitive–behavioural digital intervention to improve mental health, access, and engagement among LGBTQA+ youth and young adults. Int J Environ Res Public Health. (2021) 18(4):1541–47. doi: 10.3390/ijerph18041541
40. Eliason MJ, Dibble SL, Gordon R, Soliz GB. The last drag: an evaluation of an LGBT-specific smoking intervention. J Homosex. (2012) 59(6):864–78. doi: 10.1080/00918369.2012.694770
41. Burton CL, Wang K, Pachankis JE. Psychotherapy for the spectrum of sexual minority stress: application and technique of the ESTEEM treatment model. Cogn Behav Pract. (2019) 26(2):285–99. doi: 10.1016/j.cbpra.2017.05.001
42. Desrosiers A, Levy M, Dright A, Zumer M, Jallah N, Kuo I, et al. A randomized controlled pilot study of a culturally-tailored counseling intervention to increase uptake of HIV pre-exposure prophylaxis among young black men who have sex with men in Washington, DC. AIDS Behav. (2019) 23(1):105–15. doi: 10.1007/s10461-018-2264-5
43. Greene GJ, Madkins K, Andrews K, Dispenza J, Mustanski B. Implementation and evaluation of the keep it up! online HIV prevention intervention in a community-based setting. AIDS Educ Prev. (2016) 28(3):231–45. doi: 10.1521/aeap.2016.28.3.231
44. Mustanski B, Parsons JT, Sullivan PS, Madkins K, Rosenberg E, Swann G. Biomedical and behavioral outcomes of keep it up!: an eHealth HIV prevention program RCT. Am J Prev Med. (2018) 55(2):151–8. doi: 10.1016/j.amepre.2018.04.026
45. Lund EM, Burgess CM. Sexual and gender minority health care disparities: barriers to care and strategies to bridge the gap. Prim Care - Clin Off Pract. (2021) 48(2):179–89. doi: 10.1016/j.pop.2021.02.007
46. Jessup RL, Osborne RH, Buchbinder R, Beauchamp A. Using co-design to develop interventions to address health literacy needs in a hospitalised population. BMC Health Serv Res. (2018) 18(1):989. doi: 10.1186/s12913-018-3801-7
47. O’Brien J, Fossey E, Palmer VJ. A scoping review of the use of co-design methods with culturally and linguistically diverse communities to improve or adapt mental health services. Health Soc Care Community. (2021) 29(1):1–17. doi: 10.1111/hsc.13105
48. Morse B, Soares A, Ytell K, DeSanto K, Allen M, Holliman BD, et al. Co-design of the transgender health information resource: web-based participatory design. J Particip Med. (2023) 15:e38078. doi: 10.2196/38078
49. Massa P, de Souza Ferraz DA, Magno L, Silva AP, Greco M, Dourado I, et al. A transgender chatbot (Amanda selfie) to create pre-exposure prophylaxis demand among adolescents in Brazil: assessment of acceptability, functionality, usability, and results. J Med Internet Res. (2023) 25:e41881. doi: 10.2196/41881
50. Cirillo D, Catuara-Solarz S, Morey C, Guney E, Subirats L, Mellino S, et al. Sex and gender differences and biases in artificial intelligence for biomedicine and healthcare. NPJ Digit Med. (2020) 3(1):81. doi: 10.1038/s41746-020-0288-5
51. Raji ID, Smart A, White RN, Mitchell M, Gebru T, Hutchinson B, et al. Closing the AI accountability gap: defining an end-to-end framework for internal algorithmic auditing. Proceedings of the 2020 conference on fairness, accountability, and transparency (2020). p. 33–44. FAT* ‘20. Association for Computing Machinery; doi: 10.1145/3351095.3372873
52. Shover CL, DeVost MA, Beymer MR, Gorbach PM, Flynn RP, Bolan RK. Using sexual orientation and gender identity to monitor disparities in HIV, sexually transmitted infections, and viral hepatitis. Am J Public Health. (2018) 108(S4):S277–83. doi: 10.2105/AJPH.2018.304751
53. Parent MC, DeBlaere C, Moradi B. Approaches to research on intersectionality: perspectives on gender, LGBT, and racial/ethnic identities. Sex Roles. (2013) 68(11):639–45. doi: 10.1007/s11199-013-0283-2
54. Cyrus K. Multiple minorities as multiply marginalized: applying the minority stress theory to LGBTQ people of color. J Gay Lesbian Ment Health. (2017) 21(3):194–202. doi: 10.1080/19359705.2017.1320739
55. Johns MM, Gordon AR, Andrzejewski J, Harper CR, Michaels S, Hansen C, et al. Differences in health care experiences among transgender and gender diverse youth by gender identity and race/ethnicity. Prev Sci. (2023) 24:1128–41. doi: 10.1007/s11121-023-01521-5
56. Grov C, Bux D, Parsons JT, Morgenstern J. Recruiting hard-to-reach drug-using men who have sex with men into an intervention study: lessons learned and implications for applied research. Subst Use Misuse. (2009) 44(13):1855–71. doi: 10.3109/10826080802501570
57. McDermott E, Roen K, Piela A. Hard-to-reach youth online: methodological advances in self-harm research. Sex Res Social Policy. (2013) 10(2):125–34. doi: 10.1007/s13178-012-0108-z
58. Matsuno E, Goodman JA, Israel T, Choi AY, Lin YJ, Kary KG. L or G or B or T: matching sexual and gender minorities with subpopulation-specific interventions. J Homosex. (2020) 69:1–23. doi: 10.1080/00918369.2020.1819714
59. Ream GL. What’s unique about lesbian, gay, bisexual, and transgender (LGBT) youth and young adult suicides? Findings from the national violent death reporting system. J Adolesc Health. (2019) 64(5):602–7. doi: 10.1016/j.jadohealth.2018.10.303
60. Broer T. Technology for our future? Exploring the duty to report and processes of subjectification relating to digitalized suicide prevention. Information. (2020) 11(3):170–81. doi: 10.3390/info11030170
61. Rassy J, Bardon C, Dargis L, Côté L-P, Corthésy-Blondin L, Mörch C-M, et al. Information and communication technology use in suicide prevention: scoping review. J Med Internet Res. (2021) 23(5):e25288. doi: 10.2196/25288
62. Macapagal K, Bhatia R, Greene GJ. Differences in healthcare access, use, and experiences within a community sample of racially diverse lesbian, gay, bisexual, transgender, and questioning emerging adults. LGBT Health. (2016) 3(6):434–42. doi: 10.1089/lgbt.2015.0124
63. Paulich KN, Ross JM, Lessem JM, Hewitt JK. Screen time and early adolescent mental health, academic, and social outcomes in 9- and 10- year old children: utilizing the adolescent brain cognitive developmentSM (ABCD) study. PLoS One. (2021) 16(9):e0256591. doi: 10.1371/journal.pone.0256591
64. Parent J, Sanders W, Forehand R. Youth screen time and behavioral health problems: the role of sleep duration and disturbances. J Dev Behav Pediatr. (2016) 37(4):277–84. doi: 10.1097/DBP.0000000000000272
65. Johnson D, Deterding S, Kuhn KA, Staneva A, Stoyanov S, Hides L. Gamification for health and wellbeing: a systematic review of the literature. Internet Interv. (2016) 6:89–106. doi: 10.1016/j.invent.2016.10.002
66. Xie H. A scoping review of gamification for mental health in children: uncovering its key features and impact. Arch Psychiatr Nurs. (2022) 41:132–43. doi: 10.1016/j.apnu.2022.07.003
67. Harris E. Surgeon general urges action to improve social media safety for kids. JAMA. (2023) 329(24):2118–2118. doi: 10.1001/jama.2023.9926
68. Eubanks V. Automating inequality: how high-tech tools profile, police, and punish the poor. London: Picador (2018).
Keywords: infectious disease, LGBTQ+, young adults, emerging infections, adolescents, mobile health, technology-delivered interventions, eHealth
Citation: Cascalheira CJ, Pugh TH, Hong C, Birkett M, Macapagal K and Holloway IW (2023) Developing technology-based interventions for infectious diseases: ethical considerations for young sexual and gender minority people. Front. Reprod. Health 5:1303218. doi: 10.3389/frph.2023.1303218
Received: 27 September 2023; Accepted: 20 October 2023;
Published: 18 December 2023.
Edited by:
Jason Zucker, Columbia University, United StatesReviewed by:
Joseph Cherabie, Washington University in St. Louis, United States© 2023 Cascalheira, Pugh, Hong, Birkett, Macapagal and Holloway. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cory J. Cascalheira Y2pjYXNjYWxoZWlyYUBnbWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.