
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Reprod. Health , 29 November 2022
Sec. HIV and STIs
Volume 4 - 2022 | https://doi.org/10.3389/frph.2022.953979
This article is part of the Research Topic STI Awareness Day: STI Services and Public Engagement View all 4 articles
 Jennifer Toller Erausquin1,2
Jennifer Toller Erausquin1,2 Joanne Sánchez3
Joanne Sánchez3 Anyi Yu Pon4
Anyi Yu Pon4 Mónica Jhangimal4
Mónica Jhangimal4 Eugenia Millender2Yudith Peña5Winroy Ng4Adelys Reina4
Eugenia Millender2Yudith Peña5Winroy Ng4Adelys Reina4 Candy Nakad6Joselid Quintana5Roberto Herrera Veces5Grace Vistica4,7
Candy Nakad6Joselid Quintana5Roberto Herrera Veces5Grace Vistica4,7 Justo Pinzón-Espinosa2,8,9,10,11Gonzalo Cabezas-Talavero5Jennifer Katz5
Justo Pinzón-Espinosa2,8,9,10,11Gonzalo Cabezas-Talavero5Jennifer Katz5 Juan Miguel Pascale4,12Fátima Rodríguez-Álvarez4
Juan Miguel Pascale4,12Fátima Rodríguez-Álvarez4 Amanda Gabster2,4,13*
Amanda Gabster2,4,13*
Background: The foot transit of migrant peoples originating from the Caribbean, South America, Asia, and Sub-Saharan Africa through the Darién Forest (DF) in Eastern Panamá towards North America has increased in recent years from approximately 30,000 people/year to >133,000 in 2021. In the DF, there is no food/housing provision nor healthcare access. Very little is known of sexual and reproductive health (SRH) among this population. This study used rapid epidemiological methods to describe the SRH situation among migrant peoples in transit through the DF.
Methods: This cross-sectional study randomly selected migrant people in transit (men and women) at a Migrant Reception Station in Darién, Panamá, between January 4–11, 2022. Data collection included a self-applied questionnaire (≥18 years); clinical screening (≥12 years); and HCG, treponemal antibodies, and HIV(I/II) lateral-flow tests with blood samples (≥12 years). Descriptive analyses were used to report findings.
Results: In all, 69 men and 55 women participated in the self-applied questionnaire, 70 men and 51 women in clinical screening; 78 men and 63 women in HCG, treponemal antibody and HIV testing. Overall, 26.1% (18/69) men and 36.4% (20/55) women reported sexual intercourse within the past month. The last sex partner was casual among 43.0% (21/49) of men and 27.8% (10/36) of women; of those, 42.9% (9/21) of men and 80.0% (8/10) of women reported this sex was condomless. Among women, 20.0% (11/55) tested positive for pregnancy; 5 of these pregnancies were planned. Of those screened, a reproductive tract infection symptom was reported by 5.7% (4/70) of men and 58.8% (30/51) of women. A total of 32.7% (18/55) of men and 18.2% (8/44) of women reported no prior HIV testing. Of 78 men, HIV and treponemal antibodies were found among 1.3% (n = 1) and 2.6% (n = 2), and among 63 women, 3.2% (n = 2) and 3.2% (n = 2), respectively.
Conclusions: This rapid epidemiological assessment found high recent sexual activity, low condom use with casual partners, and a need for increased HIV and syphilis testing and treatment. There is a need for increased testing, condom provision, and SRH healthcare access at migrant reception stations that receive migrant peoples in transit through Panamá.
Global migration has greatly increased in the past four decades (1), with a particularly dramatic increase in the number of forcibly displaced people in the past 10 years (2). The current worldwide tally of migrant peoples is over 281 million, and 1 in 95 people worldwide is forcibly displaced, meaning that they had to move away from their home due to conflict, violence, or human rights violations (1). Within forcibly displaced people, the United Nations High Commissioner for Refugees specifically defines four groups as populations of concern: refugees, people in refugee-like situations, asylum-seekers, and Venezuelans displaced abroad.
International migration can be physically difficult, dangerous, and chaotic. During transit, the health needs of migrant peoples, and particularly their sexual and reproductive health needs, grow as they are faced with conditions and vulnerabilities for which they are unprepared (3). The migration process often disrupts supportive and familiar social structures, and may involve precipitous loss of financial means of support and security provided by family and friends, and disintegration of law and order (4). Migration and other humanitarian contexts create circumstances that inhibit migrant peoples' access to sexual and reproductive health (SRH) services and simultaneously increase vulnerability to sexual violence, coercion, and exploitation; transactional or survival sex; sexually transmitted infections; and unintended pregnancies (4, 5). These vulnerabilities are intensified among unauthorized or undocumented migrants and asylum seekers (6). Additionally, humanitarian settings often have very limited access to sexual and reproductive (SRH) healthcare (7).
A rapid escalation in population movement is apparent in the Americas, where migrant peoples from around the world travel through South and Central America headed to North America. Though other portions of the journey may involve traveling via airplane, boat, bus, or train, there is a 106-km gap in the Pan-American Highway near the Colombia-Panamá border. At this point, migrant peoples must cross on foot through the Darién Forest (DF; sometimes called the Darién Gap), a roadless, dense neotropical forest. The journey is dangerous and physically demanding; based on the route taken, food and other supplies carried, and the age and abilities of those traveling, the trek often takes 3–14 days to emerge from the DF in Panamá (8). The International Organization for Migration (UN Migration) and Panamá's National Migration Service estimated that over 133,000 migrant peoples passed through the DF in 2021, more than four times the previous highest annual count [30,000 for the entire year 2016] (9–11). In the first nine months of 2022, more than 150,000 migrant peoples passed through the DF (12).
In Panamá, migrant peoples who emerge from the DF are met by the National Border Police (SENAFRONT) and guided to Migrant Reception Stations (MRS). The MRS are part of a coordinated U.S.-Panamá effort to control the flow of migrant peoples. With the aid of U.S. tools and training, biometric measurements are taken of all migrants at the MRS to identify suspected terrorists and maintain documentation of migrating people (13). As described in our study protocol (14), time spent at the MRS varies based on the individual's nationality, demographic characteristics, and needs. Stays at the MRS can be as short as a few days for citizens of countries with expedited processes (including Cuba and Haiti), to several weeks or months.
To date, much of what is known about the healthcare needs of migrant peoples passing through the Darién Forest and the continued journey north comes from journalistic reports and anecdotes (15, 16). However, there is a dearth of information about the current state of sexual and reproductive health among migrant peoples in transit in this area. Therefore, the current study aims to describe the sexual and reproductive health of migrant peoples in transit and to identify targets for future intervention.
This study was undertaken in a Migrant Reception Station (MRS) in the Darién province of eastern Panamá. The study protocol received ethical approval from the Comité de Bioética de la Investigación del Instituto Conmemorativo Gorgas de Estudios de la Salud (260/CBI/ICGES/21).
Participants were randomly selected at the MRS in Darién. Travel groups (typically 2–8 persons) were introduced to the study; the study objectives and methods were briefly explained. One person from adults in the travel group (≥18 years) and one person from children/youth in the travel group (<18 years) was selected randomly to be invited to participate. Participation was voluntary. Sample size was calculated by , where n is the sample size, Z the confidence statistic, P is expected prevalence and d is the precision, resulting in an intended sample of 120 participants <18 years and 160 participants ≥18 years. We expected the prevalence of pregnancy to be 10% (17); this prevalence was used for sample size calculation.
We obtained approval from the Ministry of Health, and the Ministry of Security (National Migration Service and the National Border Service) to work in the MRS. Participants were selected as described above. Adults of legal age (≥18 years) were taken to a place where the study objectives and procedures could be explained in private so others would not influence participation. Adults were asked to sign their own consent forms. Children (<12 years) were accompanied by an adult guardian when the study was explained; the adult guardian signed a consent form. Adolescents (12–17 years) and their guardians were explained the study in a private location, separately, and were each asked to sign an informed assent or consent form, respectively. The current analysis focused only on data from adolescents and adults. A total of 12 people withdrew from the study, including 4 minors <17 years old; their data were not analyzed here.
After receiving informed consent and assent, participants (≥18 years) self-applied a questionnaire on a tablet computer (14); participants who needed assistance had a trained study volunteer read the questions and record the participant's responses on the tablet computer. Participants then gave blood (2 EDTA tubes) and mid-flow urine (20–50 ml) samples (14), and took part in the sexual and reproductive clinical survey and exam. Additional details about data collection including the self-administered questionnaire are available in our published study protocol and supplementary materials (14).
Blood samples were centrifuged. Lateral flow immunochromatography tests (CTK Biotech, Beijing, China) were performed for HIV (I/II), syphilis (treponemal seroreactivity) and pregnancy (HCG). HIV positive samples were tested again with a second brand (Abbott Diagnostics, Scarborough, United States), as per national guidelines. Samples with two positive results were analyzed for CD4 levels using Vistect Advanced (Omega Diagnostics Scotland, UK), which identifies samples with CD4 below 200 cells/mm3 and thereby meeting the WHO definition of advanced HIV disease (18). Mid-flow urine samples were tested for leukocyte esterase. All female participants were offered a pelvic exam; those who consented and had discharge were offered diagnosis for bacterial vaginosis (Amsel criteria) and yeast (microscopy KOH test).
Participants were offered results of testing and adequate treatment [according to national guidelines (19)] within 3 h of being included in the study. Our guidelines for on-site treatment of conditions identified as part of the study are described in our protocol paper (14). All participants were offered a meeting with a psychologist and psychiatrist.
We conducted descriptive analyses including frequencies and percentages for categorical variables and median and interquartile range for continuous variables. For categorical variables, we also conducted bivariable analyses (Chi square tests comparing men to women) to examine potential gender differences. All analyses were conducted using Stata 17.0 (StataCorp LP, College Station, United States).
Data collection was completed at a Migrant Reception Station in Darién, Panamá, between January 4–11, 2022. During that period, the MRS housed or received 688 migrant peoples 18 years and older and 708 migrant peoples 12 years and older.
Results of descriptive analyses for demographic characteristics are shown in Table 1. In all, 69 men and 55 women were included in the self-applied questionnaire, 70 men and 51 women in the clinical screening and 78 men and 63 women consented/assented to laboratory testing of blood. No participants identified as transgender, nonbinary, or another gender. Participants' region of origin showed statistically significant differences by gender: Caribbean origin for 13.2% (9/68) of men and 52.8% (28/53) of women; North or South America for 51.5% (35/68) of men and 34.0% (18/53) of women; Asia for 5.6% (4/68) of men and 0.0% (0/53) of women; and Sub-Saharan Africa for 29.4% (20/68) of men and 13.2% (7/53) of women.

Table 1. Demographic characteristics (self-reported by adults age ≥18 years).
The median age was 31 years for men and 30 years for women. Educational attainment showed variation by gender, with the majority of women having no formal education (52.8%; 38/53) while the majority of men had attended primary school grades 1–6 (51.5%; 35/68). Nearly one-third of men (29.4%; 20/68) but only 13.2% (7/53) of women reported post-secondary education. A majority of men were single, divorced, widowed, or separated (61.9%) and 38.1% were married/cohabiting; this trend was the reverse for women (30.0% single and 70.0% married/cohabiting). In terms of safety of dwelling, similar proportions of men (36.4%; 24/66) and women (42.6%; 23/54) reported that they did not have a safe place to sleep in the last month. Main reasons for traveling included war or conflict (33.3% among men; 16.4% among women) and other violence (16.7% among men and 20.0% among women). Women also frequently cited work (30.9% among women) as a reason for traveling.
Results of descriptive analyses for sexual behaviors and reported violence are shown in Table 2. A total of 26.1% (18/69) men and 36.4% (20/55) women reported sexual intercourse in the past month. Of those, among men, 50.0% (9/18) reported to have one sex partner and 44.4% (8/18) 3 sex partners; among women, 90.0% (18/20) reported one sex partner and 10.0% (2/20) 3 sex partners. Last sex partner was reported to be casual (a stranger, a friend or travel companion, a person of authority, a sex worker, or another person other than a regular sex partner or husband/wife) among 43.0% (21/49) of men and 27.8% (10/36) of women and formal (a regular sex partner or husband/wife) among 57.1% (28/49) of men and 72.2% (26/36) women; of those, 42.9% (9/21) of men and 80.0% (8/10) of women reported not using a condom with their last casual partner. A total of 32.7% (18/55) of men and 18.2% (8/44) of women reported never having an HIV test prior to this study.
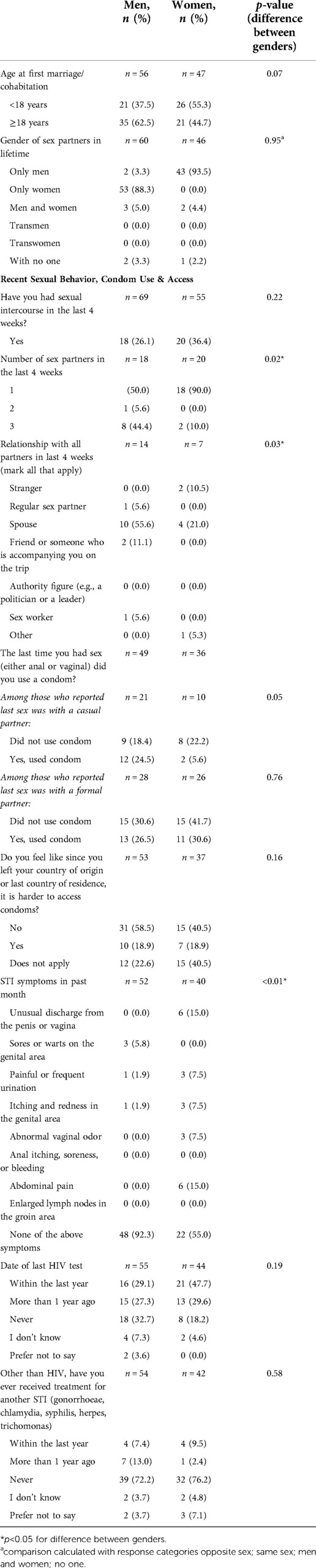
Table 2. Sexual behaviors, access to condoms, STI symptoms, and HIV testing (self-reported by adults age ≥18 years).
Clinical screening (data not shown) revealed that of those screened, 58.8% (30/51) of women and 5.7% (4/70) of men reported a current reproductive tract infection symptom. Among women screened, vaginal discharge was the most common symptom (40.0%; 12/30). Of those reporting vaginal discharge, 25.0% tested positive for leukocyte esterase in urine; 36.4% were positive for Amsel criteria; and 45.4% had hyphae/pseudohyphae evocative of C. albicans upon KOH evaluation using microscopy. Laboratory testing revealed that of 78 men, HIV and syphilis were found among 1.3% (n = 1) and 2.6% (n = 2) respectively. Among 63 women tested, 3.2% (n = 2) were positive for HIV and 3.2% (n = 2) were positive for syphilis. All HIV positive samples were identified as advanced HIV disease, with CD4 counts <200 cells/mm3.
Results of descriptive analyses for transactional sex and concurrent partnerships are shown in Table 3. About thirteen percent (12.7%; 7/55) of men and 8.3% (3/41) of women reported ever receiving money, goods, favors, presents, drugs, or housing in exchange for sex. More than 1 in 4 (26.8%; 15/56) men and 14.7% (5/34) of women reported having sex with someone who was not their formal partner while they were in a partnership; among these, 35.7% of men and 25.0% of women reported not using a condom with the secondary partner. Nearly all of these experiences occurred in the respondent's country of origin or country of residence (men: 92.9%, 13/14; women: 100%, 4/4). In addition, 7.0% (4/57) of men and 16.2% (6/37) of women reported having ever been in a relationship and their partner had another partner at the same time. Among men who reported a non-monogamous partner, this occurred in transit (66.7%; 2/3) or in a country of residence (33.3%; 1/3). Among women who reported a non-monogamous partner, this occurred before leaving country of origin (16.7%; 1/6), in transit (50.0%; 3/6), in country of residence (16.7%; 1/6), or in Panamá (16.7%; 1/6). There were no statistically significant differences in reports of these experiences by gender.
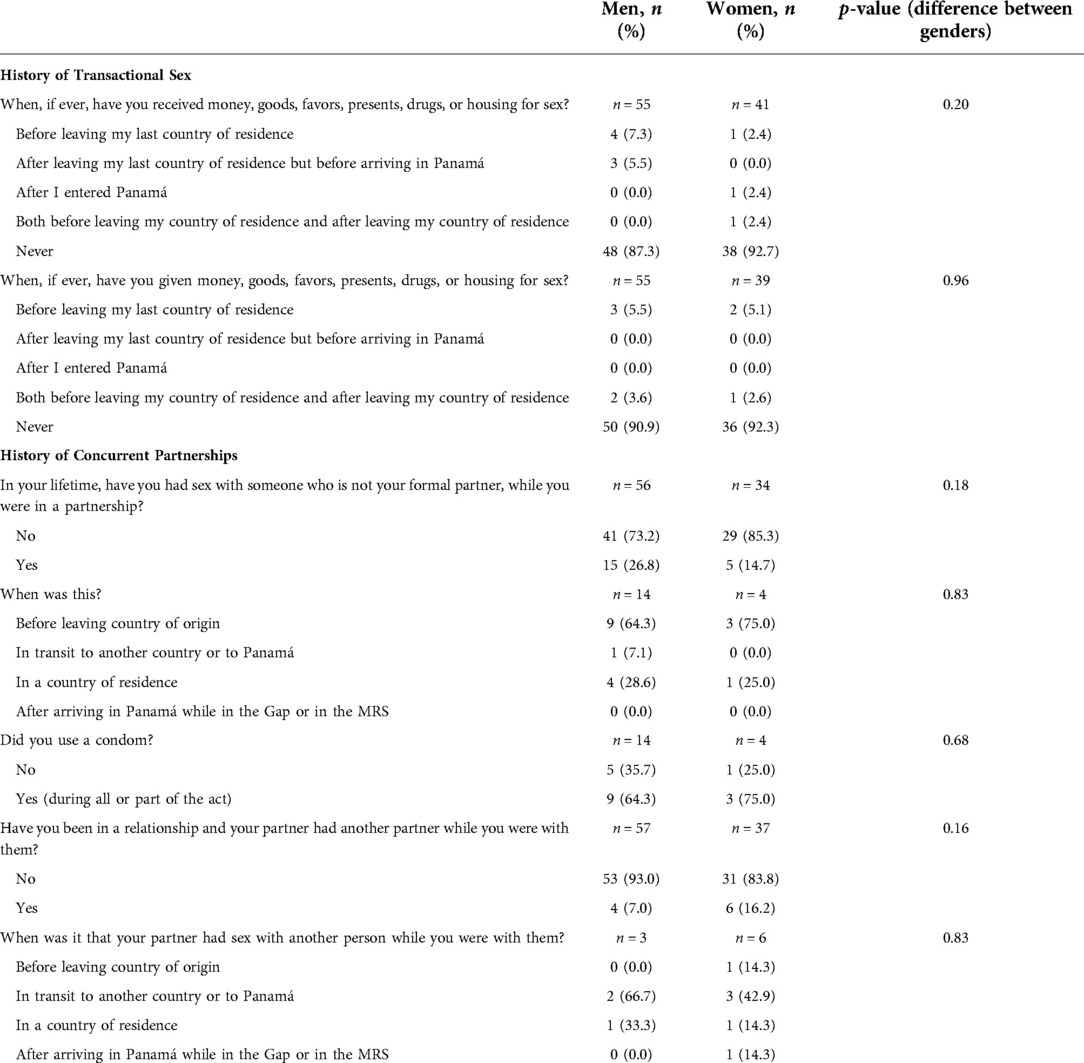
Table 3. Transactional Sex and concurrent partnerships (self-reported by adults age ≥18 years).
Results about sexual assault and perceived safety are presented in Table 4. Of the 52 men and 45 women who responded about perceived safety from sexual assault, 40.4% (n = 21) of men and 44.4% (n = 20) of women felt somewhat or completely unsafe before leaving their last country of residence. Of men, 42.3% (n = 22) and 51.2% (n = 22) of women felt unsafe while traveling from their last country of residence before arriving in Panamá and 40.4% (n = 21) men and 54.8% (n = 23) of women felt unsafe from sexual assault while traveling through the DF.
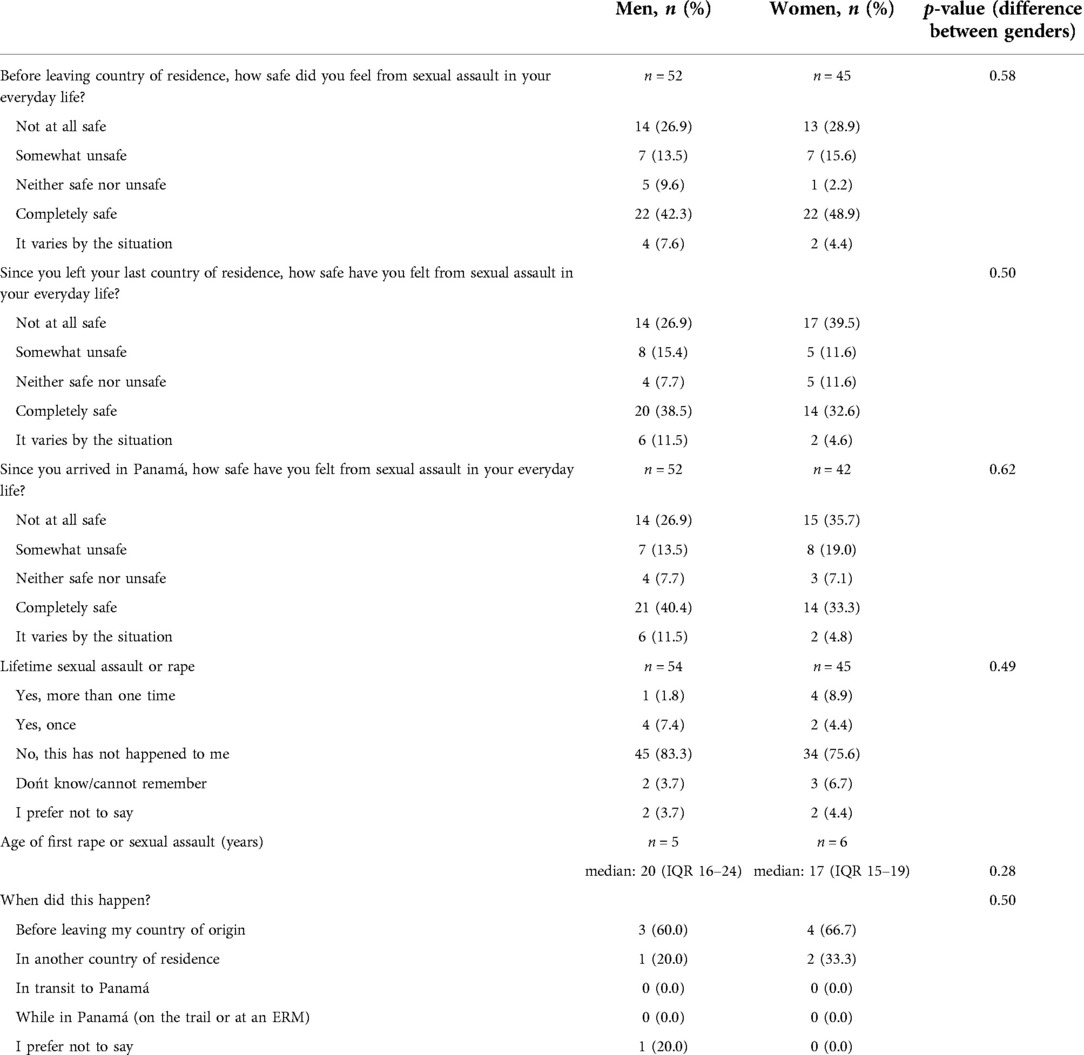
Table 4. Perceived safety from sexual assault and history of sexual assault (self-reported by adults age ≥18 years).
Participants were also asked about sexual assault (being “forced or frightened by another person into doing something sexually that you did not want to do”). Of those who reported lifetime sexual assault, 60.0% (n = 3) of men and 66.7% (n = 4) of women reported that this occurred in their last country of residence; 0.0% of respondents reported sexual assault during migration or during their time in Panamá.
Finally, results of pregnancy testing and questions about pregnancy are shown in Table 5. A total of 20.0% (n = 11) of women tested positive for pregnancy; two women did not know of their pregnancy prior to testing. Five of the 11 pregnancies were planned. Of pregnant women, 72.7% (n = 8) had one sex partner in the past year, and 27.3% (n = 3) had 2 or more partners; the last sexual encounter of pregnant women was within the last 28 days for 36.4% (n = 4) and 54.5% (n = 6) > 28 days. Among women, 39.2% (20/51) were using contraceptives at time of study.
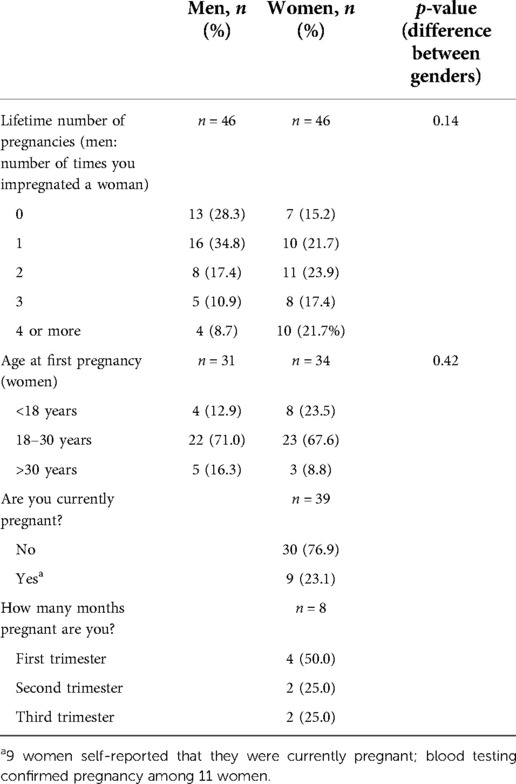
Table 5. Pregnancy (self-reported by adults age ≥18 years).
Our study showed high recent sexual activity, low condom use with casual partners, and a need for increased access HIV and syphilis testing and treatment. In addition, we found high prevalence of reproductive tract symptoms, particularly among women. Taken together, these findings indicate a need for increased testing, condom provision, and SRH healthcare access at Migrant Reception Stations that receive migrant peoples in transit in Panamá.
The findings of this study should be considered in light of several limitations. First, this was a rapid epidemiological assessment conducted over a short period of time in January 2022. There is often a lull in migration flow through Panamá around the December and January holidays. However, COVID-19 slowed migration in 2020, followed by a boom of people passing throughout most of 2021, and a lull again in December 2021. Migrant peoples also anticipated policy changes affecting migrants and immigrants to Mexico and the US in early 2022. As a result, the MRS received between 35 and 250 migrants per day at the time of data collection in January 2022. In addition, this study focused on migrant peoples in transit; there may be different SRH needs at different stages of migration: predeparture, in transit, interception, and arrival at destination (20). Finally, our self-applied questionnaire allowed participants to skip questions that they did not wish to answer, and some items had large proportions of missing data (e.g., only 7/20 women who reported sexual intercourse in the last 4 weeks answered the item on the relationship to that sexual partner). Missing data could bias results if respondents with particular characteristics were less willing to respond.
The UN Committee on Economic, Social, and Cultural Rights and the Convention on the Elimination of All Forms of Discriminations against Women affirm that sexual and reproductive health and access to SRH services are basic human rights (21). Indeed, the 2030 Sustainable Development Goals include the aim to achieve access to universal SRH services (22). However, access to SRH services remains limited in many low and middle income countries and in humanitarian settings (3), often due to scarce resources and inadequate infrastructure (7, 23).
A recent systematic review demonstrated that there are a number of evidence-based interventions to improve HIV and STI prevention knowledge and contraception and condom-use skills for young people in LMIC and humanitarian settings, and that these require adaptation “to the context and realities of humanitarian settings (such as high levels of trauma exposure and loss),” (3). The authors suggest that in such resource-limited and challenging settings, trauma-informed approaches may be considered a priority rather than resource-demanding high intensity interventions. They also suggest that program planners should consider whether SRH services in LMIC and humanitarian settings could be integrated into existing service systems (3).
The Inter-Agency Field Manual on Reproductive Health in Humanitarian Settings provides an outline of minimum reproductive health interventions that should be implemented when a humanitarian crisis emerges (4). Of critical importance is the need for gender-specific care, as women and girls in humanitarian crises have distinct needs when engaging with SRH services (24). In the case of migration through the DF in Panamá, the humanitarian crisis is not new, nor is an end in sight. To address the SRH needs of highly vulnerable migrant peoples who transit the DF en route to North America, a minimum standard of integrated sexual and reproductive health interventions is necessary. Furthermore, the design and delivery of SRH services must take a regional approach, with participation from countries across Latin America and the Caribbean.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Comité de Bioética de la Investigación del Instituto Conmemorativo Gorgas de Estudios de la Salud. Written informed consent to participate in this study was provided by participants age 18 and older. For participants 12–17 years, a parent or legal guardian/next of kin provided written consent and the minor participant provided written assent.
JTE, JS, and AG conceived of the presented idea. JTE and AG conducted the literature review. AG and AYP completed the analyses. JS, MJ, WN, and JP-E provided clinical/laboratory inputs. EM, YP, AR, CN, JQ, RH, GV, GC-T, and FR provided contextual information to integrate findings from clinical, laboratory, and questionnaire components. JTE and AG drafted the manuscript. All authors contributed to the article and approved the submitted version.
This project was supported by funds and donations of supplies from Instituto Conmemorativo Gorgas de Estudios de la Salud, Community Development Network of the Americas, Acino Swiss Farma, Glaxosmithkline Panamá, Ann Knudson, and the Oklahoma University's Physicians Pharmacy, Sagrav SA, and Omega Diagnostics. The National Research System of SENACYT provided funding for some of the rapid tests by means of José Suárez and Amanda Gabster. The funders were not involved in the study design, collection, analysis, interpretation of data, the writing of this article or the decision to submit it for publication.
The authors are immensely grateful to the participants and guardians of underage participants for their involvement in the study. The authors would also like to thank the Center for Research and Diagnosis of Emerging and Infectious Diseases, Metetí, Darién of the Instituto Conmemorativo Gorgas de Estudios de la Salud, Community Development Network of the Americas, UNICEF, Médecins Sans Frontières, Panamás Ministerio de Salud, Servicio Nacional de Fronteras (SENAFRONT), and Servicio Nacional de Migración for their ongoing support, especially the volunteers: Albin Mendoza, Andy Ledezma, Leyner Salinas, Melanio Marin, Roberto Ramos, and Rosendo Fuentes. We also thank the Panamánian Red Cross Darién Chapter, especially the volunteers: Máximo González, Miliza Peralta, Nelson Cabezón, Yudith Peña, Nayelys Miranda, Cynthia Degracia, Orlando Pisario, Lizi Lino, María Sánchez, Yesica Lino, Loyda Berrio, Ludis Mezua, and Caselina Piraza.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. International Organization for Migration. World migration report 2022. Geneva, Switzerland: UN Migration (2021).
2. United Nations High Commissioner for Refugees. Global trends: forced displacement in 2020. Geneva, Switzerland: UNHCR (2021). Available at: https://www.unhcr.org/flagship-reports/globaltrends/ (Accessed May 18, 2022).
3. Desrosiers A, Betancourt T, Kergoat Y, Servilli C, Say L, Kobeissi L. A systematic review of sexual and reproductive health interventions for young people in humanitarian and lower-and-middle-income country settings. BMC Public Health. (2020) 20:666. doi: 10.1186/s12889-020-08818-y
4. Foster AM, Evans DP, Garcia M, Knaster S, Krause S, McGinn T, et al. The 2018 inter-agency field manual on reproductive health in humanitarian settings: revising the global standards. Reprod Health Matters. (2017) 25:18–24. doi: 10.1080/09688080.2017.1403277
5. Meyer K, Abimpaye M, Harerimana JDD, Williams C, Gallagher MC. Understanding the sexual and reproductive health experiences of refugee and host community adolescents and youth in Rwanda during COVID-19: needs, barriers, and opportunities. Front Reprod Health. (2022) 4:1–13. doi: 10.3389/frph.2022.799699
6. Carruth L, Martinez C, Smith L, Donato K, Piñones-Rivera C, Quesada J, Migration and Health in Social Context Working Group. Structural vulnerability: migration and health in social context. BMJ Glob Health. (2021) 6:e005109. doi: 10.1136/bmjgh-2021-005109
7. Ivanova O, Rai M, Kemigisha E. A systematic review of sexual and reproductive health knowledge, experiences and access to services among refugee, migrant and displaced girls and young women in Africa. Int J Environ Res Public Health. (2018) 15:1583. doi: 10.3390/ijerph15081583
8. Agudelo-Higuita NI, Rodriguez-Morales AJ, Henao-Martinez AF, Franco-Paredes C, Gabster A. The treacherous journey of hundreds of migrants from Cameroon to reach the United States. Travel Med Infect Dis. (2021) 44:102172. doi: 10.1016/j.tmaid.2021.102172
9. International Organization for Migration. More than 91,000 migrants have crossed darien gap on way to North America this year. NP: UN Migration (2021). Available at: https://www.iom.int/news/more-91000-migrants-have-crossed-darien-gap-way-north-america-year
10. Moreno E, Moreland S. Panama Says record 150,000 migrants crossed dangerous darien gap this year. Reuters. (2022). Available at: https://www.reuters.com/world/panama-says-record-150000-migrants-crossed-dangerous-darien-gap-this-year-2022-10-11/ (Accessed October 11, 2022).
11. United Nations High Commissioner for Refugees, International Organization for Migration. Number of venezuelans crossing the darien gap soars. Geneva, Switzerland: UN Migration (2022). Available at: https://www.iom.int/news/number-venezuelans-crossing-darien-gap-soars
12. Servicio Nacional de Migración Panamá. Movimiento migratorio 2022. Panama City, Panama: República de Panamá Gobierno Nacional (2022). Available at: https://www.migracion.gob.pa/inicio/estadisticas (Accessed May 25, 2022).
13. Fitzgerald DS. Refuge beyond reach: how rich democracies repel asylum seekers. New York, NY: Oxford University Press (2019).
14. Gabster A, Jhangimal M, Erausquin JT, Suárez JA, Pinzón-Espinosa J, Baird M, et al. Rapid health evaluation in migrant peoples in transit through darien, Panama: protocol for a multimethod qualitative and quantitative study. Therapeutic Advances in Infection. (2021) 8:20499361211066190. doi: 10.1177/20499361211066190
15. Vyas K. Rapes of US-bound migrants make a treacherous route even more dangerous. The Wall Street Journal. (2021). Available at: https://www.wsj.com/articles/rapes-of-u-s-bound-migrants-make-a-treacherous-route-even-more-dangerous-11630956539
16. Taylor L. The growing health crisis on the world’s most perilous migrant crossing. Br Med J. (2022) 376:o419. doi: 10.1136/bmj.o419
17. Dopfer C, Vakilzadeh A, Happle C, Kleinert E, Müller F, Ernst D, et al. Pregnancy related health care needs in refugees—a current three center experience in Europe. Int J Environ Res Public Health. (2018) 15:1934. doi: 10.3390/ijerph15091934
18. World Health Organization. Guidelines for managing advanced HIV disease and rapid initiation of antiretroviral therapy. Geneva, Switzerland: World Health Organization (2017). Available at: https://www.who.int/publications-detail-redirect/9789241550062 (Accessed October 10, 2022).
19. Ministerio de Salud de Panamá, Caja de Seguro Social, & Instituto Conmemorativo Gorgas de Estudios de Salud. Normativa nacional para el abordaje integral de las infecciones de transmisión sexual en Panamá. Panamá City, Panamá: Ministerio de Salud de Panamá (2014).
20. Martinez-Donate AP, Hovell MF, Rangel MG, Zhang X, Sipan CL, Magis-Rodriguez C, et al. Migrants in transit: the importance of monitoring HIV risk among migrant flows at the Mexico–US border. Am J Public Health. (2015) 105:497–509. doi: 10.2105/AJPH.2014.302336
21. United Nations Committee on Economic, Social and Cultural Rights (CESCR). General comment No. 14: the right to the highest attainable standard of health (art. 12 of the covenant). Geneva, Switzerland: United Nations (2000).
22. United Nations. Transforming our world: The 2030 agenda for sustainable development. Geneva, Switzerland: United Nations (2015). Available at: https://sdgs.un.org/publications/transforming-our-world-2030-agenda-sustainable-development-17981
23. Blanchet K, Ramesh A, Frison S, Warren E, Hossain M, Smith J, et al. Evidence on public health interventions in humanitarian crises. Lancet. (2017) 390:2287–96. doi: 10.1016/S0140-6736(16)30768-1
Keywords: sexual and reproductive health (SRH), migrant health care, sexual behavior, sexually transmitted infection (STI), Latin America & Caribbean
Citation: Erausquin JT, Sánchez J, Yu Pon A, Jhangimal M, Millender E, Peña Y, Ng W, Reina A, Nakad C, Quintana J, Herrera Veces R, Vistica G, Pinzón-Espinosa J, Cabezas-Talavero G, Katz J, Pascale JM, Rodríguez-Álvarez F and Gabster A (2022) Sexual and reproductive health and access: Results of a rapid epidemiological assessment among migrant peoples in transit through Darién, Panamá. Front. Reprod. Health 4:953979. doi: 10.3389/frph.2022.953979
Received: 26 May 2022; Accepted: 31 October 2022;
Published: 29 November 2022.
Edited by:
Saiqa Mullick, Wits Reproductive Health and HIV Institute, South AfricaReviewed by:
Maria Pyra, Howard Brown Health Center, United States© 2022 Erausquin, Sánchez, Yu Pon, Jhangimal, Millender, Peña, Ng, Reina, Nakad, Quintana, Herrera Veces, Vistica, Pinzón-Espinosa, Cabezas-Talavero, Katz, Pascale, Rodríguez-Álvarez and Gabster. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Amanda Gabster YWdhYnN0ZXJAZ29yZ2FzLmdvYi5wYQ==
Specialty Section: This article was submitted to HIV and STIs, a section of the journal Frontiers in Reproductive Health
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.