Abstract
Background:
Despite accumulating evidence of the long-term impacts of childhood sexual abuse (CSA), few studies have investigated the association between CSA and early sexual debut among adolescents. In this study, we examine the relationship between CSA and early initiation of sexual intercourse among Chinese youth, and the role of school-based sex education in this association, based on a nationally representative survey.
Methods:
Data were collected from the Survey of Youth Access to Reproductive Health in China (YARHC) conducted in 2009. Multivariable logistic regression models were used to investigate the association between CSA experience and early sexual debut, and the interaction terms between sexual and reproductive health education and CSA were included to examine the role of education in the association between CSA and early sexual debut.
Results:
Among 4,907 sexually experienced youth, 1,062 (21.6%) made their early sexual debut. After adjusting for sociodemographic characteristics, it was found that CSA experience was significantly associated with early sexual debut, with an adjusted odds ratio of 3.13 (95% CI: 1.67–5.87). Receiving any type of sexuality education (reproductive health, sexually transmitted disease (STD) and HIV prevention, or contraception use) was not associated with a decreased risk of early sexual debut.
Conclusion:
Our results indicate a greater risk of early sexual debut among Chinese adolescents with a history of CSA, and only 46.7% sexually experienced youth had received prior sex education, which suggested an inadequacy of school-based sexuality education. To reduce this risk, targeted intervention with timely and adequate sexuality education for both early starters of sexual intercourse and CSA victims is warranted in China.
Introduction
The development of adolescent sexuality is of great concern to families and society. As a major milestone in life course, the sexual debut of adolescents has been considered as a basis for their subsequent patterns of sexual psychology and behavior. The age of sexual debut among adolescents and youth around the world saw a decline in the past few decades (1, 2). A substantial proportion of adolescents initiated sexual intercourse at an age without reaching a certain level of maturity and cognitive ability to properly handle the circumstance (3). Early sexual debut has been demonstrated to be associated with various sexual risk factors such as multiple sexual partners, reduced use of contraception, and sexual intercourse after alcohol use, which are further linked to subsequent negative outcomes such as sexual transmitted diseases, unintended pregnancy, and even suicide attempts (4–6). Moreover, it has been suggested as an important predictor for undesirable social consequences in later life. Individuals who initiate sexual intercourse in early adolescence are more likely to be in a condition of poor health, compromised economic conditions, and reduced life satisfaction (7).
As one of the major types of adverse childhood experiences, sexual abuse during childhood has been suggested to be associated with multiple adverse health risk behaviors and outcomes such as risky sexual behaviors (8), teenage pregnancy (9), and problems connected with intimacy relationships (10), to name a few. A previous study has indicated that sexual trauma may disrupt the psychosocial development of abused children, operate through cognitive and emotional processes, and further manifest in behaviors (11, 12). Some amount of research seems to suggest that early sexual debut plays a mediating role in the association between childhood sexual abuse (CSA) and risky sexual behaviors in later life (13). However, despite the accumulating evidence of the long-term impacts of sexual trauma, few studies have investigated the association between CSA and early sexual debut among adolescents. Considering the significant influence of sexual debut on individuals’ life-time sexual trajectory, evidence regarding the effect of childhood sexual abuse on the development of sexual activity is absolutely essential for making targeted interventions.
It is widely recognized that sex education is an essential component of healthy physical and psychosocial development of adolescents and young adults (14). A study from the United States has shown that the implementation of sex education can reduce the risk of early initiation of sexual activity among adolescents (15). Comprehensive education of sexual health not only provides the knowledge and skills necessary to help young people make informed choices of sexual and reproductive behaviors and offers useful linkage and resources to clinical services, but also helps adolescents to form healthy relationships and set goals and plans during their transition from adolescence to adulthood (16). Meanwhile, sex education is also recommended as a key component in the treatment of CSA victims (17). An analysis of the CSA intervention programs suggests that sexual and reproductive health education (SRHE) is necessary for reducing negative emotions related to abuse experience and promoting healthy intimate relationships for the victims (17). Thus, the impact of sex education on the timing of sexual debut among CSA victims is essential for the formulation and adjustment of treatment programs. However, little research has been conducted on providing empirical evaluation.
Marked changes have occurred in people's attitudes toward sex and sexual expression in China since the launch of the reform and opening-up policy (18). A study of Chinese university students in 2005 showed that the peak age of sexual debut was 17–19 years, which significantly declined compared with 20–22 years of age a decade ago (19, 20). In the meantime, childhood sexual abuse was not and is not an unusual phenomenon in China. According to an estimation in a systematic review, in the 1988–2013 period, 8.7% of Chinese children under the age of 18 years suffered from sexual abuse (21). Nevertheless, it has been pointed out that the implementation of sex education in China was insufficient in the past and has also failed to keep pace with the physical and social changes that have taken place over the years, leaving the new generation of youth at risk of adverse sexual consequences (22). Formal sexuality education in Chinese schools is widely considered to be inadequate because of its insufficient class hours and a lack of teacher resources (23), which is evident from the fact that 44.4% of Chinese college students reported having never received prior school-based sexuality education (24).
Overall, nearly half of the respondents in this survey reported having never received school-based sexuality education. For the other half, sexuality education was mainly conducted during middle school and college years.
Therefore, in this study, we examined the relationship between CSA and early initiation of sexual intercourse among Chinese youth, and the role of school-based sex education in this association, based on a nationally representative survey.
Methods
Data source and ethical approval
Data were collected from the Survey of Youth Access to Reproductive Health in China (YARHC). This nationally representative and population-based survey was conducted by Peking University in 2009. It aimed to describe the level of knowledge on, and the attitude and behavior toward, sexual and reproductive health among unmarried youth in mainland China and to explore their accessibility to reproductive health services. Experts from related academic fields in China and the United Nations Fund for Population Activities (UNFPA) designed the study protocol and questionnaire of this survey. The Institutional Review Board of Peking University Health Science Center reviewed and approved this study (No. 20090928). Consent to participate was obtained from all respondents, and for those under 18 years, the consent form was signed by their adult guardians.
Participants and samples
In the YARHC survey, the target population was unmarried youth aged 15–24 years living in mainland China. Three subpopulations were included: school youth (in school, either living on campus or in a community), household youth (living with family, either employed or unemployed), and collective household youth (employed, living in a communal house) to cover participants from different environments. All interviewers received rigorous training by a committee of survey experts, who used the standard set, and a pilot study with preliminary interviews was conducted before the formal survey. The privacy of youth was protected during the entire process of the survey, with all participants interviewed face-to-face in independent environments without the presence of a third party. For the section on sensitive topics related to sexual experiences and behaviors, the questionnaire was self-administered and completed by individuals themselves. In addition, the respondents were interviewed by those of the same sex.
This survey applied a four-stage stratified random cluster sampling with probability proportional to size. The four stages for school youth, household youth, and collective household youth were cities-schools-classes-students, cities-counties-communities-household youth, and cities-counties-map pieces-collective household youth, respectively. The final estimated sample size was distributed in 40 cities and counties from 25 provinces/autonomous regions/municipalities in China. When the selected subject could not be contacted, or there was no target youth in the selected household, the interviewers followed the sample substitution principle, in which the neighbor of the nonrespondents would be taken as a replacement, with a swing priority from right to left within five units. Given the refusal rate of 24.9%, 22,465 questionnaires were finally collected, of which 22,288 were valid, achieving a validity rate of 98.9%. Because we focused on the association between CSA and early initiation of sexual intercourse, our study sample was restricted to subjects who were asked whether they have ever had sexual intercourse and never experienced forced sexual intercourse (to avoid a case where the sexual debut was forced sexual intercourse), and a total of 4,907 cases were included in the analysis (Figure 1).
Figure 1
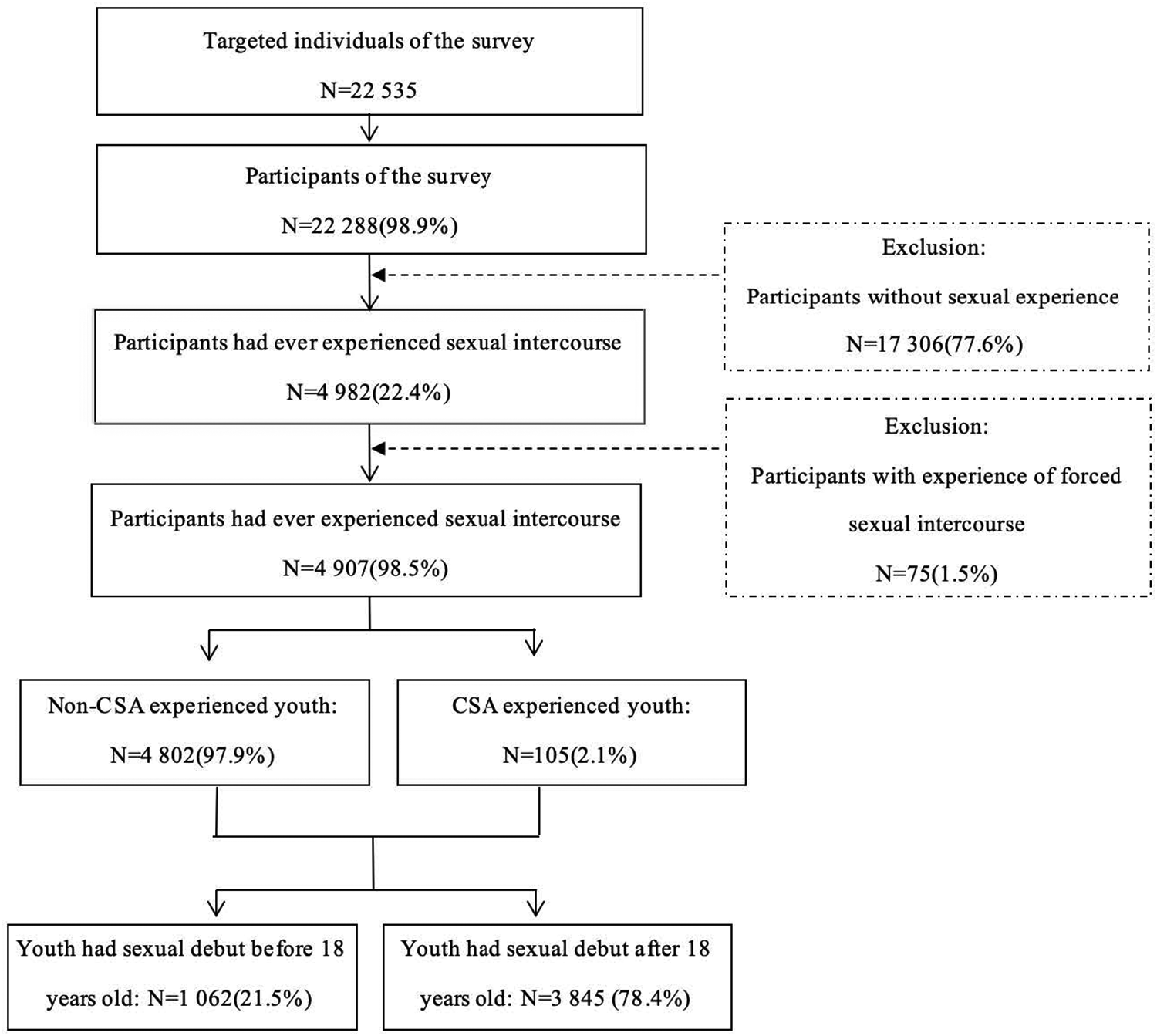
Flowchart of the study sample.
Patient and public involvement
Patients or members of the public were not involved in the design, conduct, reporting, or dissemination plans of our research.
Measures
Related sexual experience
The question “Have you ever had a sexual intercourse (whether it was with your current/latest girlfriend/boyfriend or with any others)?” was employed to determine whether a respondent was sexually experienced; if the answer was “yes,” then the participant was rated as sexually experienced. Also, the question “Some young people are forced to have sexual intercourse with others (non-boy/girlfriends). Have you ever had such an experience?” was employed to determine whether an individual had ever had forced sexual intercourse. The above two variables were used to exclude respondents without sexual experience or respondents who experienced forced sexual intercourse.
Childhood sexual abuse experience (independent variable)
In the YARHC survey, the question “Some young people are forced to touch, or be touched on, the sensitive body parts by others (non-boy/girlfriends). Have you ever had such an experience?” was employed to determine whether an individual had ever been sexually abused. If the answer was “yes,” the age when the first sexual abuse happened was extracted from the question “How old were you when these things first happened?” When the age was younger than 18 years, the respondent was defined as having experienced CSA.
Early sexual debut (dependent variable)
The question “How old were you when you had sexual intercourse for the very first time?” was employed to determine the age of sexual debut. When the age was younger than 18 years, the respondent was defined as having early sexual debut.
Sexual and reproductive health education
Individuals’ experience of SRHE was measured in terms of three aspects: reproductive health education (Have you ever attended the lecture on reproductive health education in school?), STD and HIV prevention education (Have you ever attended the lecture on STD and HIV prevention education in school?), and contraception use education (Have you ever attended the lecture on contraception use education in school?). We also used “any SRHE” to include any of the above three aspects. All four variables were binary (with yes or no answers).
Sociodemographic information (control variables)
Age at the time of survey was set as a continuous variable. Survey youth were categorized by sex (male or female), residence (rural or urban areas), region (east, central, or west), education level (junior high school and below, senior high school, or college and above), employment status (student, unemployed and not at school, or employed), mother's education level (junior high school and below, senior high school, or college and above), and annual family income tertiles (low, middle, or high).
Statistical analysis
Descriptive statistics with chi-square test were applied to present the sample characteristics, population numbers, prevalence, and proportions and to examine the difference between groups where appropriate. Multivariable logistic regression models were used to calculate the adjusted odds ratios (ORs) and 95% confidence intervals (CIs) for determining the association between CSA experience and early sexual debut in Model 1. In Model 2–5, the interaction terms between each type of SRHE and CSA were included in the multivariable logistic regression models to examine the role of education in the association between CSA and early sexual debut. STATA 14 (STATA Corp, College Station, TX, United States) was used to perform all data analyses. A P-value of less than 0.05 was considered statistically significant.
Results
Sample characteristics and CSA experience among Chinese unmarried youth
Among 4,907 sexually experienced youth, 2,835 (57.8%) were male, and the mean age was 20.8 years. There were 2,008 (40.9%) from rural areas and 1,838 (37.5%) youth with a college and above degree. A total of 105 youth (2.1%) experienced CSA, of which 44 (1.5%) were male and 61 (2.9%) were female. Other demographic and socioeconomic characteristics of the study sample in terms of whole samples, male subsamples, and female subsamples are listed in Table 1.
Table 1
| Total N = 4,907 | Male N = 2,835 | Female N = 2,072 | |
|---|---|---|---|
| Age, years, mean (SD) | 20.8 (2.3) | 20.8 (2.3) | 20.9 (2.3) |
| Residence, N (%) | |||
| Rural | 2,008 (40.9) | 1,164 (41.1) | 844 (40.7) |
| Urban | 2,899 (59.1) | 1,671 (58.9) | 1,228 (59.3) |
| Region, N (%) | |||
| East | 2,549 (51.9) | 1,456 (51.4) | 1,093 (52.8) |
| Central | 1,235 (25.2) | 718 (25.3) | 517 (24.9) |
| West | 1,123 (22.9) | 611 (23.3) | 462 (22.3) |
| Education, N (%) | |||
| Junior high school and below | 742 (15.1) | 425 (15.0) | 317 (15.3) |
| Senior high school | 2,327 (47.4) | 1,334 (47.0) | 993 (47.9) |
| College and above | 1,838 (37.5) | 1,076 (38.0) | 762 (36.8) |
| Employment, N (%) | |||
| Student | 1,564 (31.9) | 975 (34.4) | 589 (28.4) |
| Employed | 2,751 (56.1) | 1,541 (54.4) | 1,210 (58.4) |
| Unemployed | 592 (12.0) | 319 (11.2) | 273 (13.2) |
| Family income tertiles, N (%) | |||
| Low | 1,389 (28.3) | 777 (27.4) | 612 (29.5) |
| Middle | 1,863 (38.0) | 1,093 (38.6) | 770 (37.2) |
| High | 1,655 (33.7) | 965 (34.0) | 690 (33.3) |
| Mother's education, N (%) | |||
| Junior high school and below | 3,091 (63.0) | 1,792 (63.2) | 1,299 (62.7) |
| Senior high school | 1,320 (26.9) | 750 (26.9) | 570 (27.5) |
| College and above | 496 (10.1) | 293 (10.3) | 203 (9.8) |
| CSA experience, N (%) | |||
| No | 4,802 (97.9) | 2,791 (98.5) | 2,011 (97.1) |
| Yes | 105 (2.1) | 44 (1.5) | 61 (2.9) |
Characteristics of the study sample by gender.
CSA, childhood sexual abuse.
SRHE of Chinese youth by CSA experience
Among 4,907 sexually experienced youth, only 2,289 (46.7%) received any type of SRHE in school, 2,039 (41.5%) received reproductive health education, 786 (16.0%) received STD and HIV prevention education, and 328 (6.7%) received contraception use education in school.
The proportion of youth who received any type of SRHE, reproductive health education, STD and HIV prevention education, and contraception use education among CSA-experienced youth were 61.9%, 50.5%, 30.5%, and 12.4%, respectively, which were higher than those (46.3%, 41.4%, 15.7%, and 6.6%, respectively) among youth without CSA experience. Except reproductive health education (P = 0.061), chi-square tests showed significant differences in the proportion of any type of SRHE (P = 0.002), STD and HIV prevention (P < 0.001), and contraception use education (P = 0.018) among youth with or without CSA experience (Table 2).
Table 2
| SRHE attainment | Total, N = 4,907 | Non-CSA-experienced youth N = 4,802 | CSA-experienced youth, N = 105 | P-value |
|---|---|---|---|---|
| Any SRHE, N (%) | 0.002 | |||
| No | 2,618 (53.4) | 2,578 (53.7) | 40 (38.1) | |
| Yes | 2,289 (46.7) | 2,224 (46.3) | 65 (61.9) | |
| Reproductive health, N (%) | 0.061 | |||
| No | 2,868 (58.5) | 2,816 (58.6) | 52 (49.5) | |
| Yes | 2,039 (41.5) | 1,986 (41.4) | 53 (50.5) | |
| STD and HIV prevention, N (%) | <0.001 | |||
| No | 4,121 (84.0) | 4,048 (84.3) | 73 (69.5) | |
| Yes | 786 (16.0) | 754 (15.7) | 32 (30.5) | |
| Contraception use, N (%) | 0.018 | |||
| No | 4,579 (93.3) | 4,487 (93.4) | 92 (87.6) | |
| Yes | 328 (6.7) | 315 (6.6) | 13 (12.4) |
SRHE of Chinese youth by CSA experience.
SRHE, sexual and reproductive health education; CSA, childhood sexual abuse.
Prevalence of early sexual debut by CSA experience and SRHE among Chinese youth
Among 4,907 sexually experienced youth, 1,062 (21.6%) made their early sexual debut. Among 105 CSA-experienced youth, 48.6% had early sexual debut, which was significantly higher than that (21.1%) among youth without CSA experience (P < 0.001). The timing of sexual debut tended to be earlier for CSA-experienced youth than for those without CSA experience (Figure 2).
Figure 2
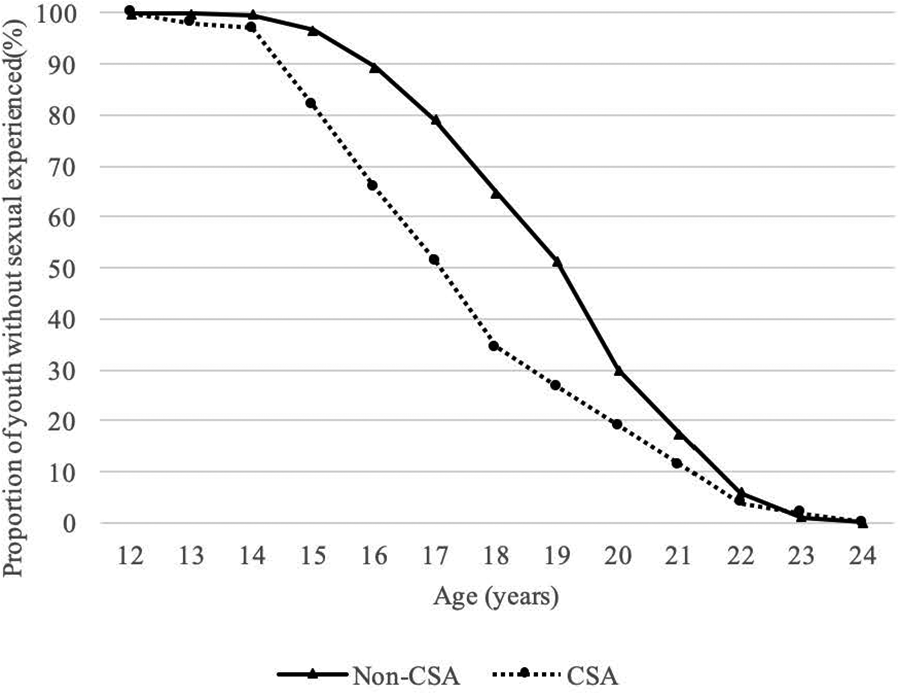
Proportions of Chinese youth who have never had a sexual experience by CSA exposure and age. CSA, childhood sexual abuse.
As displayed in Table 3, the prevalence of early sexual debut was 23.1% among youth who received any type of SRHE in school, which was significantly higher than that (20.3%) among those without any SRHE attainment (P = 0.016). Similar patterns were observed for STD and HIV prevention education and contraception use education.
Table 3
| SRHE attainment | Total | CSA-experienced youth | ||
|---|---|---|---|---|
| Non-early sexual debut, N = 3,845 | Early sexual debut, N = 1,062 | Non-early sexual debut, N = 54 | Early sexual debut, N = 51 | |
| Any SRHE, N (%) | ||||
| No | 2,086 (79.7) | 532 (20.3) | 20 (50.0) | 20 (50.0) |
| Yes | 1,759 (76.9) | 550 (23.1) | 34 (52.3) | 31 (47.7) |
| P-value | 0.016 | 0.818 | ||
| Reproductive health | ||||
| No | 2,260 (78.8) | 608 (21.2) | 23 (44.2) | 29 (55.8) |
| Yes | 1,585 (77.7) | 454 (22.3) | 31 (58.5) | 22 (41.5) |
| P-value | 0.371 | 0.144 | ||
| STD and HIV prevention | ||||
| No | 3,272 (79.4) | 849 (20.6) | 39 (53.4) | 34 (46.6) |
| Yes | 573 (72.9) | 213 (27.1) | 15 (46.9) | 17 (53.1) |
| P-value | <0.001 | 0.537 | ||
| Contraception use | ||||
| No | 3,627 (79.2) | 952 (20.8) | 51 (55.4) | 41 (44.6) |
| Yes | 218 (66.5) | 110 (33.5) | 3 (23.1) | 10 (76.9) |
| P-value | <0.001 | 0.029 | ||
Prevalence of early sexual debut by CSA experience and SRHE.
SRHE, sexual and reproductive health education; CSA, childhood sexual abuse.
For CSA-experienced youth, the prevalence of early sexual debut was 47.7%, 41.5%, 53.1%, and 76.9% among youth who received any type of SRHE, reproductive health education, STD and HIV prevention education, and contraception use education in school, respectively. Also, there was a significant difference in the prevalence of early sexual debut between youth who received contraception use education and those who did not (P = 0.029).
Association between CSA, SRHE, and early sexual debut among Chinese youth
Table 4 presents the results of multivariate regression analysis for determining the association between CSA experience and early initiation of sexual intercourse. In Model 1, after adjusting for sociodemographic characteristics, it was found that CSA experience was significantly associated with early sexual debut, with an adjusted odds ratio of 3.13 (95% CI: 1.67–5.87). The risk of having an early sexual debut was higher among those who received STD and HIV prevention education (aOR: 1.49, 95% CI: 1.08–2.05) and contraception use education (aOR: 1.60, 95% CI: 1.06–2.42) than that among their counterparts without such education attainment. Model 2–Model 5 included the interaction term between CSA and each type of SRHE in the logistic regression. No significant association in the interaction term was observed in all models.
Table 4
| Variables | Age of sexual debut < 18, odds ratio (95% CI) | ||||
|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 4 | Model 5 | |
| CSA experience | |||||
| No | 1 | 1 | 1 | 1 | 1 |
| Yes | 3.13 (1.67–5.87)*** | 5.39 (2.17–13.39)*** | 4.53 (1.95–10.52)*** | 4.50 (2.15–9.45)*** | 3.11 (1.60–6.05)*** |
| Any SRHE | |||||
| No | 1 | 1 | 1 | 1 | 1 |
| Yes | 0.75 (0.45–1.23) | 0.76 (0.46–1.26) | 0.74 (0.45–1.22) | 0.74 (0.45–1.21) | 0.75 (0.45–1.23) |
| Reproductive health | |||||
| No | 1 | 1 | 1 | 1 | 1 |
| Yes | 0.95 (0.60–1.51) | 0.95 (0.60–1.51) | 0.98 (0.62–1.56) | 0.97 (0.61–1.53) | 0.95 (0.60–1.51) |
| STD and HIV prevention | |||||
| No | 1 | 1 | 1 | 1 | 1 |
| Yes | 1.49 (1.08–2.05)*** | 1.50 (1.09–2.07)* | 1.51 (1.09–2.08)* | 1.56 (1.13–2.16)** | 1.49 (1.08–2.05)* |
| Contraception use | |||||
| No | 1 | 1 | 1 | 1 | 1 |
| Yes | 1.60 (1.06–2.42)*** | 1.61 (1.06–2.43)* | 1.59 (1.05–2.40)* | 1.60 (1.06–2.41)* | 1.60 (1.05–2.43)* |
| CSA*: any SRHE | |||||
| Yes* | — | 0.36 (0.10–1.24) | — | — | — |
| CSA*: reproductive health | |||||
| Yes* | — | — | 0.43 (0.12–1.53) | — | — |
| CSA*: STD and HIV prevention | |||||
| Yes* | — | — | — | 0.29 (0.08–1.11) | — |
| CSA*: contraception use | |||||
| Yes* | — | — | — | 1.08 (0.15–7.94) | |
Association between CSA experience, sexual and SRHE, and early sexual debut: adjusted odds ratio and 95% CI.
SRHE, sexual and reproductive health education; CSA, childhood sexual abuse.
All models were adjusted for age, gender, residence, employment, education, mother's education, and family income.
P < 0.001; **P < 0.01; *P < 0.05.
Discussion
Based on a nationally representative survey, this study first investigated the association between CSA experience and early sexual debut among Chinese youth. Our results showed that 21.5% of Chinese unmarried youth had made their sexual debut before 18 years old. One study from Wuhan city suggested that 10.7% of female university students had their first sexual intercourse before 18 years old (4), another study suggested that 5.9% of female university students had their sexual debut also before 18 years old (6), and another study from Ningbo city found that 43.0% of male university students had initiated sexual intercourse before college (25). The national-level data used in our study made the result more representative for the issue in the country. The prevalence of early sexual debut among Chinese youth was lower than that among those in most Western societies (7, 26), but it represents a marked increase compared with that of previous Chinese generations. This may be explained not only by the decline in average age at puberty among Chinese adolescents (27), but also by the context of moderation in societal perceptions of premarital sexual activity, as discussed earlier. This finding justifies the public concern for the potential health risks of early sexual initiation among youth in China.
Consistent with previous studies in the United States (28, 29) and Norway (30), a history of CSA was associated with an elevated risk of early onset of sexual intercourse among Chinese youth. Two separate pathways have been suggested by recent research to explain the influence of sexual abuse, and these are biological and psychological pathways. From the perspective of developmental neurobiology (31), traumatic stress may operate through the biological system, affect the timing of puberty, and place children at risk for sexual precocity (32). Also, the association between sexual abuse and early puberty has been demonstrated by one study on the sexual trajectory of neglected and abused children (13). More empirical evidence has suggested a psychological pathway. Previous research has indicated that CSA victims always have difficulty in forming healthy interpersonal relationships and are more likely to get involved in premature romantic relationships to meet their intimacy needs and heighten their feeling of belonging (33). In addition, due to the cross-sectional design of the data in our study, the association between CSA and early sexual debut can also be explained in an opposite way—youths who initiate sexual intercourse at early adolescence are at a higher risk of sexual exploitation including sexual abuse, which has also been demonstrated by one study from Sweden (34). Our finding highlights the need for making a targeted intervention of subsequent negative outcomes for both early starters of sexual intercourse and CSA victims in China.
It is also worth mentioning that more than half of sexually active youth in this survey never received any type of school-based sexual and reproductive health education, which is consistent with that of a previous study (24). For the other half, the received sexuality education mainly focused on reproductive health knowledge, and only a small proportion of youth received school-based education on STD and HIV prevention and contraception use. This result further indicates the serious lag of sexuality education and the failure to incorporate its guidelines into the curriculum for youth in China’s schools. School-based SRHE has been implemented since 1985, and it has also been reinforced as an obligation by the population and family planning law enacted by the Chinese government in 2002 (35). However, the progress on this score has been quite disappointing—sex has always been and still considered as a sensitive and taboo subject for classroom discussion, and most teachers are reluctant to provide lectures on the subject (22). A survey conducted in Shanghai reported that less than 20% of high school students received sex education from their teachers (22). In addition, knowledge about contraception use and how to reduce risky sexual behaviors are excluded from the curriculum in most Chinese schools, as it is believed that access to such information may prompt early sexual activity among adolescents (35). This finding underlines the urgent need for providing early and timely sexuality education, especially skills and information about contraception and prevention of STD and HIV for the youth.
The multivariate analysis including the interaction terms between CSA and SRHE showed that receiving any type of sexuality education—reproductive health, STD and HIV prevention, or contraception use—was not associated with a decreased risk of early initiation of sexual intercourse among youth with a history of CSA in China. Several reasons should be considered to account for this fact. First, it has been suggested that school-based sexuality education in the country is inadequate and incomprehensive due to insufficient class hours and a lack of professional teaching resources (23), which is proven by the fact that less than 30% of university students have a sound knowledge of HIV transmission (36). Second, most of the school-based education curriculums are designed only for general children and adolescents without considering CSA victims as part of them (17). Evidence shows that abused and nonabused children differ in their responses to materials related to sexual knowledge, which may act as a stimulus and cause emotional distress in abused children, which may further influence their acquisition of sexual health knowledge (37). In addition, there are studies pointing out that sex education is not an effective intervention to delay the timing of sexual debut among adolescents (23, 38). This is also supported by the results in our study that education on STD and HIV prevention and contraception use is associated with an elevated risk of early sexual debut. This finding suggests that current school-based sex education should not be considered as a substitute for the sexual education component of CSA victim treatment. Rather, the coverage of such education for them should be planned appropriately and monitored closely in the treatment setting to address their special needs and process their emotional reactions moderately so that the information would be better retained in their minds (17).
Limitation
The present study has several limitations. First, due to the cross-sectional design of the survey, our results do not provide direct evidence of causality and therefore should be interpreted with caution. Second, the issue of sex remains a sensitive and taboo topic in Chinese society and the data were collected through a self-report; therefore, the responses to CSA experience and the age of sexual debut are subject to error of recall and social-desirability bias. Third, we are unable to obtain more detailed information about sexuality education for more specific analyses such as the age of receiving such education and the course duration, and so on. Despite these limitations, our study provides evidence for determining the association between CSA and early sexual debut among Chinese youth by taking into account the role of sexuality education using a nationally representative survey that could be applicable to other similar cultural and societal contexts.
Conclusion
To sum up, the results of this study indicate a greater risk of early sexual debut among Chinese youth with a history of CSA and to some extent suggest that the current school-based sexuality education is inadequate to act as an effective intervention to delay sexual initiation, either for CSA victims or for the general youth. Targeted intervention with a timely and adequate course of sexuality education for both early starters of sexual intercourse and CSA victims, as well as future research evaluating such intervention programs in China, is warranted.
Statements
Data availability statement
The datasets presented in this article are not readily available because the access to these datasets lies within the purview of the Institute of Population Research, Peking University. Requests to access the datasets should be directed to the corresponding author.
Ethics statement
The Institutional Review Board of Peking University Health Science Center reviewed and approved this study (No. 20090928). Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin. Written informed consent was obtained from the individual(s) and minor(s)’ legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
Author contributions
XW and RD contributed equally to this study. XW initiated the study and participated in writing the article. RD analyzed data and wrote the original article. CG provided suggestions on data analysis and revising the paper. XZ supervised all aspects of its implementation and contributed to writing the article. All authors critically interpreted the findings and edited the article.
Funding
This study was supported by the Beijing Social Science Fund (20SRC029).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1.
FinerLB. Trends in premarital sex in the United States, 1954–2003. Public Health Rep. (2007) 122(1):73–8. 10.1177/003335490712200110
2.
ZhuGBosmaAK. Early sexual initiation in Europe and its relationship with legislative change: a systematic review. Int J Law Crime Justice. (2019) 57:70–82. 10.1016/j.ijlcj.2019.03.001
3.
OshiDCMckenzieJBaxterMRobinsonRNeilSGreeneTet alAssociation between single-parent family structure and age of sexual debut among young persons in Jamaica. J Biosoc Sci. (2019) 51(2):177–87. 10.1017/S0021932018000044
4.
LiJLiSYanHXuDXiaoHCaoYMaoZ. Early sex initiation and subsequent unsafe sexual behaviors and sex-related risks among female undergraduates in Wuhan. China Asia Pac J Public Health. (2015) 27(2_suppl):21S–9S. 10.1177/1010539514549186
5.
KaestleCEHalpernCTMillerWCFordCA. Young age at first sexual intercourse and sexually transmitted infections in adolescents and young adults. Am J Epidemiol. (2005) 161(8):774–80. 10.1093/aje/kwi095
6.
RenJQiXCaoWWangZGuoYGaoshanJet alEarly sexual initiation is associated with suicide attempts among Chinese young people. Int J Environ Res Public Health. (2022) 19(7):3966. 10.3390/ijerph19073966
7.
SandfortTGMOrrMHirschJSSantelliJ. Long-term health correlates of timing of sexual debut: results from a national United States study. Am J Public Health. (2008) 98(1):155–61. 10.2105/AJPH.2006.097444
8.
FriedrichWNUrquizaAJBeilkeRL. Behavior problems in sexually abused young children. J Pediatr Psychol. (1986) 11(1):47–57. 10.1093/jpepsy/11.1.47
9.
FiscellaKKitzmanHJColeRESidoraKJOldsD. Does child abuse predict adolescent pregnancy?Pediatrics. (1998) 101:620–4. 10.1542/peds.101.4.620
10.
MullenPEMartinJLAndersonJCRomansSEHerbisonGP. The effect of child sexual abuse on social, interpersonal and sexual function in adult life. Br J Psychiatry. (1994) 165(1):35–47. 10.1192/bjp.165.1.35
11.
DownsWR. Developmental considerations for the effects of childhood sexual abuse. J Interpers Violence. (1993) 8(3):331–45. 10.1177/088626093008003003
12.
BaidenPPanischLSKimYJLaBrenzCAKimYOnyeakaHK. Association between first sexual intercourse and sexual violence victimization, symptoms of depression, and suicidal behaviors among adolescents in the United States: findings from 2017 to 2019 national youth risk behavior survey. Int J Environ Res Public Health. (2021) 18(15):7922. 10.3390/ijerph18157922
13.
JocelynBPatriciaCHenianCElizabethSJeffreyOG. Sexual trajectories of abused and neglected youths. J Dev Behav Pediatr. (2004) 25(2):77–82. 10.1097/00004703-200404000-00001
14.
ShtarkshallRASantelliJSHirschJS. Sex education and sexual socialization: roles for educators and parents. Perspect Sex Reprod Health. (2007) 39(2):116–9. 10.1363/3911607
15.
ErkutSGrossmanJMFryeAACederICharmaramanLTracyAJ. Can sex education delay early sexual debut?J Early Adolesc. (2013) 33(4):482–97. 10.1177/0272431612449386
16.
CampaMILeffSZTuftsM. Reaching high-need youth populations with evidence-based sexual health education in California. Am J Public Health. (2018) 108(S1):S32–7. 10.2105/AJPH.2017.304127
17.
RubenzahlSAGilbertBO. Providing sexual education to victims of child sexual abuse: what is a clinician to do?J Child Sex Abus. (2002) 11(1):1–25. 10.1300/J070v11n01_01
18.
YuJ. Teenage sexual attitudes and behaviour in China: a literature review. Health Soc Care Community. (2012) 20(6):561–82. 10.1111/j.1365-2524.2011.01054.x
19.
Research Group on Sex Education among University Students. Report on sexual behavior survey among Chinese university students in 2000. Youth Study. (2001) 12:31–9. 10.3969/j.issn.1008-1437.2001.12.007
20.
SongYJiC-yXingYHuP-jChenT-jZhangL. Study on the characteristics of sexual intercourse debut and its influencing factors among college students in 18 provinces in China. Zhonghua Liu Xing Bing Xue Za Zhi. (2011) 32(2):134–7. 10.3760/cma.j.issn.0254-6450.2011.02.007
21.
FangXFryDAJiKFinkelhorDChenJLannenePDunnefMP. The burden of child maltreatment in China: a systematic review. Bull World Health Organ. (2015) 93:176–85C. 10.2471/BLT.14.140970
22.
WattsJ. China sex education lags behind sexual activity. Lancet. (2004) 363(9416):1208. 10.1016/S0140-6736(04)15994-1
23.
BurkiT. Sex education in China leaves young vulnerable to infection. Lancet Infect Dis. (2016) 16(1):26. 10.1016/S1473-3099(15)00494-6
24.
LiCChengZWuTLiangXGaoshanJLiLHongPTangK. The relationships of school-based sexuality education, sexual knowledge and sexual behaviors-a study of 18,000 Chinese college students. Reprod Health. (2017) 14(1):103. 10.1186/s12978-017-0368-4
25.
MaQOno-KiharaMCongLXuGPanXZamaniSet alEarly initiation of sexual activity: a risk factor for sexually transmitted diseases, HIV infection, and unwanted pregnancy among university students in China. BMC Public Health. (2009) 9(1):111. 10.1186/1471-2458-9-111
26.
LaraLAAbdoCH. Age at time of initial sexual intercourse and health of adolescent girls. J Pediatr Adolesc Gynecol. (2016) 29(5):417–23. 10.1016/j.jpag.2015.11.012
27.
ParishWLLaumannEOMojolaSA. Sexual behavior in China: trends and comparisons. Popul Dev Rev. (2007) 33(4):729–56. 10.1111/j.1728-4457.2007.00195.x
28.
HillisSDAndaRFFelittiVJMarchbanksPA. Adverse childhood experiences and sexual risk behaviors in women: a retrospective cohort study. Fam Plann Perspect. (2001) 33(5):206–11. 10.2307/2673783
29.
BrownaMJMashobSWPereracRAMezukbdeBCohenbSA. Sex and sexual orientation disparities in adverse childhood experiences and early age at sexual debut in the United States: results from a nationally representative sample. Child Abuse Negl. (2015) 46:89–102. 10.1016/j.chiabu.2015.02.019
30.
PedersenWSkrondalA. Alcohol and sexual victimization: a longitudinal study of Norwegian girls. Addiction. (1996) 91(4):565–81. 10.1111/j.1360-0443.1996.tb02314.x
31.
PynoosRSSteinbergAMOrnitzEMGoenjianAK. Issues in the developmental neurobiology of traumatic stress. Ann N Y Acad Sci. (1997) 821(1):176–93. 10.1111/j.1749-6632.1997.tb48278.x
32.
De BeilisMDPutnamFW. The psychobiology of childhood maltreatment. Child Adolescent Psychiatr Clin. (1994) 3(4):663–78. 10.1016/S1056-4993(18)30463-2
33.
WolfeDAWekerleCReitzel-JaffeDLefebvreL. Factors associated with abusive relationships among maltreated and nonmaltreated youth. Dev Psychopathol. (1998) 10(1):61–85. 10.1017/S0954579498001345
34.
KastbomÅASydsjöGBladhMPriebeGSvedinC-G. Sexual debut before the age of 14 leads to poorer psychosocial health and risky behaviour in later life. Acta Paediatr. (2015) 104(1):91–100. 10.1111/apa.12803
35.
LeeRNRLTLokeAYHungRNTTMSobelH. A systematic review on identifying risk factors associated with early sexual debut and coerced sex among adolescents and young people in communities. J Clin Nurs. (2018) 27(3–4):478–501. 10.1111/jocn.13933
36.
HuangJBovaCFennieKPRogersAWilliamsAB. Knowledge, attitudes, behaviors, and perceptions of risk related to HIV/AIDS among Chinese university students in Hunan, China. AIDS Patient Care STDs. (2005) 19(11):769–77. 10.1089/apc.2005.19.769
37.
GordonBNSchroederCSAbramsJM. Children's knowledge of sexuality: a comparison of sexually abused and nonabused children. Am J Orthopsychiatry. (1990) 60(2):250–7. 10.1037/h0079177
38.
WangBHertogSMeierALouCGaoE. The potential of comprehensive sex education in China: findings from suburban Shanghai. Int Fam Plan Perspect. (2005) 31(2):63–72. 10.1363/3106305
Summary
Keywords
childhood sexual abuse (CSA), early sexual debut, sexual and reproductive health education, China, nationally representative survey
Citation
Wen X, Ding R, Guo C and Zheng X (2023) Association between childhood sexual abuse and early sexual debut among Chinese adolescents: The role of sexual and reproductive health education. Front. Reprod. Health 4:909128. doi: 10.3389/frph.2022.909128
Received
31 March 2022
Accepted
29 November 2022
Published
23 January 2023
Volume
4 - 2022
Edited by
Fredrick Odhiambo Otieno, Nyanza Reproductive Health Society, Kenya
Reviewed by
Dewi Rokhmah, University of Jember, Indonesia Sandy Wurtele, University of Colorado Colorado Springs, United States Cihad Dundar, Ondokuz Mayıs University, Turkey Marina V. Melkumova, Arabkir Joint Medical Center, Armenia
Updates
Copyright
© 2023 Wen, Ding, Guo and Zheng.
This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaoying Zheng xzheng@pku.edu.cn
These authors have contributed equally to this work
Specialty Section: This article was submitted to Adolescent Reproductive Health and Well-being, a section of the journal Frontiers in Reproductive Health
Disclaimer
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.