
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Reprod. Health , 01 September 2021
Sec. Gynecology
Volume 3 - 2021 | https://doi.org/10.3389/frph.2021.729642
This article is part of the Research Topic Comorbidities in Women with Endometriosis: Risks and Implications View all 6 articles
 Helen C. McNamara1*
Helen C. McNamara1* Helena C. Frawley1,2,3
Helena C. Frawley1,2,3 Jacqueline F. Donoghue1,4
Jacqueline F. Donoghue1,4 Emma Readman3,4Martin Healey1,4Lenore Ellett3,4Charlotte Reddington1,3,4Lauren J. Hicks1Keryn Harlow3Peter A. W. Rogers1,4Claudia Cheng1,4 on behalf of En-DIT (Endometriosis: Diagnosis, Innovation and Treatment) Research Group
Emma Readman3,4Martin Healey1,4Lenore Ellett3,4Charlotte Reddington1,3,4Lauren J. Hicks1Keryn Harlow3Peter A. W. Rogers1,4Claudia Cheng1,4 on behalf of En-DIT (Endometriosis: Diagnosis, Innovation and Treatment) Research GroupEndometriosis-associated pain and the mechanisms responsible for its initiation and persistence are complex and difficult to treat. Endometriosis-associated pain is experienced as dysmenorrhea, cyclical pain related to organ function including dysuria, dyschezia and dyspareunia, and persistent pelvic pain. Pain symptomatology correlates poorly with the extent of macroscopic disease. In addition to the local effects of disease, endometriosis-associated pain develops as a product of peripheral sensitization, central sensitization and cross sensitization. Endometriosis-associated pain is further contributed to by comorbid pain conditions, such as bladder pain syndrome, irritable bowel syndrome, abdomino-pelvic myalgia and vulvodynia. This article will review endometriosis-associated pain, its mechanisms, and its comorbid pain syndromes with a view to aiding the clinician in navigating the literature and terminology of pain and pain syndromes. Limitations of our current understanding of endometriosis-associated pain will be acknowledged. Where possible, commonalities in pain mechanisms between endometriosis-associated pain and comorbid pain syndromes will be highlighted.
Endometriosis is a complex, estrogen dependent disorder with a cumulative prevalence of 11% (1). Endometriosis is characterized by the presence of endometrium-like glands and stroma outside the uterus (2). The pathogenesis of endometriosis remains incompletely defined with genetic and environmental components contributing (3), and can be considered in terms of predisposing factors, initiating factors and propagating factors (4).
Predisposing factors are genetic and anatomical. Genetic factors have been the subject of extensive investigation. Studies have demonstrated that first degree relatives and twins of individuals with endometriosis are at increased risk of disease, and of disease of a more severe stage (5). Genome wide association studies have identified genetic variants linked with severe endometriosis (6). Genetic variants may impact inflammation, cell adhesion, growth factors and hormone receptors (7, 8). Studies using a candidate gene approach have been difficult to replicate. Anatomical factors may also contribute. Individuals with Müllerian abnormalities and/or outflow tract obstruction are at increased risk (9).
Initiating factors likely include retrograde menstruation and coelomic metaplasia. Sampson's hypothesis of retrograde menstruation proposes that endometrial fragments migrate via the fallopian tube to the peritoneal cavity (10). The increased risk of endometriosis seen with outflow tract obstruction, early menarche and short menstrual cycles may be due to an increased volume of retrograde menstruation (11). However, the mechanisms of progression to lesion formation remain unclear and only occur in a subset of women (12). Alternatively, coelomic metaplasia refers to metaplasia of cells into endometrial cells within the visceral and abdominal peritoneum. The presence of endometriosis in males exposed to estrogen, in prepubescent girls, and at extra-pelvic sites including the thoracic cavity give support to this theory (13–16). Other stem cells and progenitor cells might also initiate lesion growth either within or outside the peritoneal cavity (17).
Propagating factors are thought to include an enhanced inflammatory response, alterations in immune response including defective apoptosis, and hormonal changes including progesterone resistance (18). Endometriosis is an inflammatory condition, with increased cytokines and inflammatory mediators found in the peritoneal fluid of affected individuals (Table 1; discussed below). The development of endometriotic lesions may depend on disruption of the innate immune response to menstrual debris and ectopic endometrial cells within the pelvis, with alterations in the concentration and function of peritoneal lymphocytes and macrophages observed (19). Finally, indirect evidence exists to support a theory of progesterone resistance, predominantly related to progesterone receptor alterations within the lesions (20).
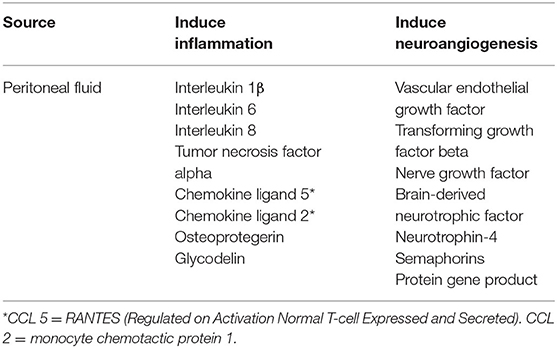
Table 1. Local mediators of inflammation and neuroangiogenesis in endometriosis.
The diagnosis of endometriosis is based on laparoscopic visualization and histology of lesions (21). Ultrasound and MRI act as adjunct methods of diagnosing deep infiltrating endometriosis and endometriomas (22). Evidence to support the use of ultrasound for the diagnosis of superficial endometriosis is emerging, but very limited (23). Clinical history and examination may aid clinicians in suspecting severe disease. However, symptom-based prediction is poor at predicting any-stage endometriosis (24). It is difficult to correlate the level of pain with the macroscopic extent of endometriosis visualized at laparoscopy (25). Some individuals with severe pain have minimal disease (26), and some individuals with severe disease have no pain (27). Laparoscopic surgical removal of endometriotic lesions reduces pain in some, but not all, individuals (28, 29). Current guidelines recommend access to a multidisciplinary pain management service as needed (30–32).
Endometriosis-associated pain (EAP) is experienced as dysmenorrhea, non-cyclical pelvic pain, and cyclical pain related to organ function including dysuria, dyschezia and deep dyspareunia (33, 34). The complexity of EAP is contributed to by the different mechanisms involved. In addition to local factors, EAP may arise and persist as a product of peripheral sensitization, central sensitization and cross sensitization (35). EAP is further contributed to by comorbid persistent pain conditions including bladder pain syndrome, irritable bowel syndrome, abdomino-pelvic myalgia and vulvodynia (36). This article will review EAP, its mechanisms, and its comorbid pain syndromes with a view to aiding the clinician in navigating the terminology of pain and pain syndromes, current knowledge, and its limitations.
Pain refers to an “unpleasant sensory and emotional experience associated with actual or potential tissue damage” (37).
Persistent pelvic pain is defined as pain perceived to be arising from the pelvis that persists >6 months' duration (38). It is acknowledged that while international societies and guidelines refer to “chronic” pelvic pain, the authors, like other groups (39–41), prefer the term “persistent” pelvic pain.
Endometriosis-associated pain has been variably described and defined either as a subset of persistent pelvic pain, or as a discrete condition. Different definitions have arisen from guidelines and classifications to facilitate and aid patient care and research, and have evolved over time. The most recent World Health Organization International Classification of Diseases (ICD-11) defines chronic primary pain syndromes, as distinguished from chronic secondary pain associated with other diagnoses (42). As a subset of chronic secondary pain, chronic secondary visceral pain may be further defined as having a causative condition like endometriosis (42).
Alternatively, the International Association for the Study of Pain (IASP) differentiates between diseases (endometriosis, secondary dysmenorrhea with endometriosis) and chronic pelvic pain syndromes, and specifically defines “endometriosis-associated pain syndrome” (37). Similarly, the European Association of Urology (EAU) separates pain syndromes with no obvious diagnosis from chronic primary pelvic pain syndromes and non-pain syndromes, and follows the IASP in separately defining “endometriosis-associated pain syndrome” (43).
As such, endometriosis-associated pain syndrome is defined as persistent or recurrent pelvic pain in individuals with laparoscopically diagnosed endometriosis, where symptoms persist after adequate treatment, and is associated with “cognitive, behavioral, sexual or emotional consequences” (43). Nevertheless, as outlined by the IASP and EAU, the phenotype of endometriosis may be less relevant. In patients with pain where endometriosis is found, it is not clear whether endometriosis is coexistent or causative (43). In addition to the fact that pain can exceed levels expected based on endometriotic lesions visualized at laparoscopy, individuals often experience symptoms of lower urinary tract, sexual and bowel dysfunction.
Therefore, while definitions are essential, they are restricted by the limitations of our current understanding of endometriosis, EAP, and its mechanisms, and by the presence of comorbid pain syndromes. For the purposes of this review, EAP refers simply to pain where endometriosis has been identified.
Endometriosis-associated pain arises due to initial local inflammatory and nociceptive events. It may persist as a function of peripheral, central, and cross sensitization (44). Psychosocial factors also contribute (45).
The generation and sense of EAP is multifactorial, and confounded by the complexity of endometriotic lesion development, and diversity of lesion placement. Contributing factors include altered distribution of pelvic nerve fibers, inflammation, secreted factors, and neuronal growth (46–49).
Endometriosis-associated pain involves stimulation of nerve fibers of the peritoneal and visceral tissues. The parietal peritoneal tissue is highly innervated with sensory nerve fibers, sympathetic nerve fibers, myelinated and unmyelinated nerve fibers, presynaptic vesicles and neuropeptides that sense pain, pressure, touch, friction, cutting and temperature (50–52). The visceral tissue is innervated by the autonomic nervous system, with unmyelinated sensory and myelinated mechanosensory neurons that sense stretching, tearing, distention and contraction. The sensation of pain may arise from these networks. Thin unmyelinated nerve fibers lie just below the peritoneal surface (51). Myelinated nerve fibers arise from the sub-mesothelial tissue and penetrate the peritoneal cavity with demyelinated nerve endings. These nerve endings may then sense the peritoneal fluid for noxious or nociceptive stimuli (52).
Endometriotic lesions are sources of inflammation, cytokines, angiogenic factors and nerve growth factors. Inflammatory mediators at both lesion sites and within the peritoneal fluid have been investigated as potential activators of nociceptive pathways (39). Inflammatory mediators including interleukin-1β (IL-1β), interleukin-6 (IL-6), interleukin-8 (IL-8), regulated upon activation, normal T cell expressed and secreted [RANTES, or chemokine ligand 5 (CCL5)] and tumor necrosis factor alpha (TNF-α), and chemokines including monocyte chemotactic protein 1 [chemokine ligand 2 (CCL2)] are increased in the peritoneal fluid of women with endometriosis (Table 1) (53–58).
It has been commonly suggested that, consistent with endometrial tissue, endometriotic lesions cycle and bleed in response to changes in estrogen and progesterone. As such, apoptosis, necrosis and shedding would trigger inflammation and pain (35, 59–61). Cyclic changes have been thought to be responsible for hemorrhage at lesion sites visualized at the time of laparoscopy (62). However, more recent data suggest endometriotic lesions rarely cycle in synchrony with the eutopic endometrium (63). Endometriotic lesions are heterogeneous in histological morphology and hormonal responsiveness, with only some lesions demonstrating cyclic changes (64). Hemorrhage within lesions is observed throughout the menstrual cycle and may be caused by local inflammation and angiogenesis (63). Recognizing the heterogeneity of endometriotic lesions is an important step toward understanding the complexity of EAP and its treatment.
Peripheral sensitization refers to “increased responsiveness and reduced threshold of nociceptive neurons in the periphery to the stimulation of their receptive fields” (37, 59). It is proposed that persistence of EAP is associated with sensitization of the peripheral nervous system. The following mechanisms may contribute to peripheral sensitization: altered nerve density at lesion sites, changes in the peritoneal fluid, perineural invasion, and alterations in the sympathetic nervous system.
The structure and function of peripheral nerves are altered in endometriosis. Changes in nerve density have been observed in peritoneal endometriosis, ovarian endometriomas and deep infiltrating endometriosis (DIE). Significantly more nerve fibers are found in endometriotic lesions compared with normal peritoneum (65). Ovarian endometriomas have been found to have more nerve fibers compared with normal ovarian tissue (66). DIE has a higher nerve fiber density compared with endometriosis at other sites; endometriosis in the rectovaginal septum has been demonstrated to have higher nerve fiber density compared with superficial peritoneal endometriosis (55, 67). Moreover, increased density of calcitonin gene-related peptide (CGRP) positive nerve fibers in lesions has been shown to positively correlate with pain severity in individuals with endometriosis (68).
Differences in receptors on peripheral nerve fibers have also been observed. The density of transient receptor potential vanilloid 1 receptor (TRPV1), involved in nociceptive pain pathways, is increased in endometriotic lesions, and its increased density has been associated with increasingly severe dysmenorrhea (69).
Alterations in the peritoneal fluid may cause sensitization of peripheral nociceptors. Changes in peritoneal fluid contribute to neuroangiogenesis in endometriotic lesions and in the adjacent peritoneum. Neurotrophins [nerve growth factor (NGF), brain derived neurotrophic factor (BDNF), neurotrophin-4] and other growth factors [vascular endothelial growth factor (VEGF) and transforming growth factor beta (TGF-β)] are increased in the peritoneal fluid of women with endometriosis (Table 1). Growth factors stimulate new nerve growth in the periphery, potentially contributing to the altered nerve density in endometriotic lesions (70).
Perineural invasion (PNI) may also be associated with pelvic sensitization. PNI, more commonly associated with malignancy, is defined in this context as the migration or integration of endometriotic lesions along nerve fibers (71–73). PNI in patients with deep infiltrative endometriosis has been shown to be associated with higher pain scores, dysmenorrhea, dyspareunia, persistent pelvic pain, sciatica and unilateral leg pain (73, 74). PNI contributes to increased neurogenesis and angiogenesis (75). Increased endometriotic lesion secretion of NGF (76) and TGF-β (77) also correlates with lesional invasion of pelvic nerves (70).
Dysregulation of the autonomic nervous system (ANS) may further amplify peripheral sensitization. Some endometriotic lesions are found to have a lower density of sympathetic nerve fibers while sensory nerve fiber density is unchanged (78). A loss of sympathetic nerve fibers is associated with chronic inflammation, and is seen in other chronic inflammatory diseases (79). However, the mechanisms by which ANS dysregulation contributes to EAP remain unclear.
Central sensitization refers to the heightened excitability of the central nervous system in response to noxious stimuli (37). Central sensitization has been classically described as increased excitability of nociceptive neurons in the dorsal horn of the spinal cord following continued or recurrent exposure to noxious stimuli, tissue injury or nerve damage (80). Changes in dorsal horn neurons are exhibited as a decreased pain threshold and an increased pain response. Subsequent alterations in synaptic efficacy in surrounding nerves gives rise to central facilitation, with pain experienced due to innoxious stimuli. Impaired descending pain modulation at the level of the dorsal horn neurons may also contribute to central sensitization (81).
It has been demonstrated that women with endometriosis and persistent pelvic pain demonstrate hyperalgesia in response to noxious stimuli compared to healthy pain-free controls (82). Evidence is mixed when women with pelvic pain with endometriosis and women with pelvic pain without endometriosis are compared, with studies finding increased hyperalgesia in those with biopsy proven endometriosis (82), or no difference (40).
Central sensitization may also be described as arising due to primary changes in brain activity or structure. Changes in brain structure, function and activity have been evaluated in individuals with persistent pain using functional MRI and PET imaging (83). Women with EAP have been found to have reduced volume in areas of the brain associated with pain processing, including the thalamus, insula and putamen (84). It is suggested that reduced tissue volume occurs due to neuronal atrophy, neurodegeneration or medication effects (44).
Using functional MRI, it has been demonstrated that women with EAP have increased resting-state connectivity between pain processing regions including the anterior insula compared to women with endometriosis and no pain, and healthy controls (85). Women with dysmenorrhea have been found to have increased activation of pain processing regions in response to noxious stimuli both within the pelvis and in the periphery (86).
Finally, central sensitization may occur as a consequence of changes in the hypothalamic-pituitary-adrenal (HPA) axis. Women with persistent pelvic pain display alterations in their HPA axis and HPA axis-mediated pain response. Persistent pain alters the HPA axis and its capacity to mount a stress response to noxious stimuli. Women with dysmenorrhea have been demonstrated to have reduced levels of cortisol compared to women without pain (86). Acute stress leads to activation of the HPA axis but with chronic insult, this response hypo-attenuates (44).
Cross sensitization refers to nociceptive inputs from a diseased tissue impacting the perception of pain arising from normal tissue in close proximity (87). Cross sensitization has been studied between the pelvic organs of the bladder, colon, uterus and vagina. It is suggested that sensitized afferent nerves of the uterus and vagina give rise to sensitization in visceral afferents of other organs. These peripheral afferent nerve pathways overlap, converging on similar areas of the spinal cord. This is referred to as viscero-visceral convergence. Cross sensitization has also been observed between pelvic floor muscles and pelvic viscera. This is referred to as somato-visceral convergence (88).
It is hypothesized that shared innervation pathways have evolved to facilitate the coordination of pelvic organ functions—urination, defecation and sexual function—and that the presence of endometriosis causes maladaptation of converging pain pathways. In endometriosis, neurogenesis within lesions may also play a role, with newly sprouted nerve fibers converging on existing innervation pathways (35).
Viscero-visceral hyperalgesia refers to increased pain experienced by women with endometriosis and an associated pelvic pain syndrome. Viscero-visceral hyperalgesia is thought to contribute to pain severity in women with endometriosis (89).
Pain processing is further influenced by genetics, psychological state and cognitive factors (44). Women with persistent pelvic pain and endometriosis report high levels of mood disorders, with population-based studies demonstrating a bidirectional association of diagnosis with endometriosis and psychiatric disorders (90). The mechanisms underlying these associations are complex (91), and impacted by individuals' perception of social functioning (92). Subsequent alterations in pain perception have been observed (93–95). Depressed mood, anxiety, pain catastrophizing, pain anticipation and increased attention to pain are associated with higher pain intensity (39). Evidence suggests that psychosocial factors impact pain processing at all levels, local, peripheral and central (44).
Endometriosis-associated pain often coexists with, and is further complicated by, other pelvic pain syndromes including bladder pain syndrome, irritable bowel syndrome, vulvodynia and abdomino-pelvic myalgia (92). Comorbid pain syndromes have mechanistic features in common with EAP, including peripheral, central, and cross sensitization.
It is acknowledged that while common comorbid pelvic pain syndromes are reviewed in this article, other “chronic overlapping pain conditions” including migraine, lower back pain and fibromyalgia are beyond the scope of this review (Table 2) (96).
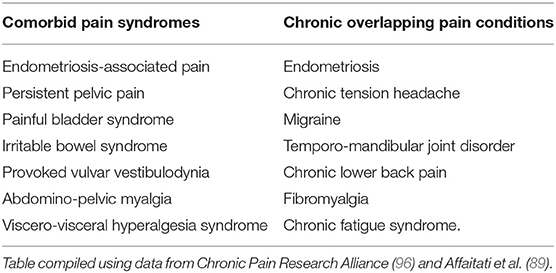
Table 2. Comorbid pain syndromes vs. chronic overlapping pain conditions.
Bladder pain syndrome (BPS) is characterized by pain in the bladder and/or pelvis associated with lower urinary tract symptoms including urinary urgency and frequency (97). In women diagnosed with endometriosis at laparoscopy the rate of co-existing BPS is in the order of 43–60% (98–100). Women with endometriosis have a 4-fold risk of diagnosis with BPS within 3 years of diagnosis with endometriosis (101). Like EAP, pain in BPS is mediated by inflammation. High levels of urothelial inflammatory mediators including IL-6 and TNF-α are observed in individuals with BPS (102). Central pain amplification and altered processing of afferent signals may also contribute (103).
Irritable bowel syndrome (IBS) is a functional gastrointestinal disorder defined by the Rome IV criteria as the presence of abdominal pain related to defecation and/or change in bowel habit, in the absence of other gastrointestinal disease (104). In women diagnosed with endometriosis the rate of IBS is as high as 60% (105). In a cohort of adolescents with endometriosis, 24% self-reported a concurrent diagnosis of IBS, with an increased association between pain severity and diagnosis with IBS (106). The pathogenesis of IBS is thought to relate to alterations in the enteric nervous system and brain-gut interactions. Peripheral sensitization may contribute with similar mechanisms of sensitization observed in IBS as to those seen in EAP, including increased activation of the TRPV1 receptor (107). Altered visceral sensation and pain in IBS may also be a consequence of central sensitization, with changes observed in the activation of brain regions associated with emotional arousal and pain modulation in individuals with IBS (108).
Abdomino-pelvic myalgia refers to pain felt in the abdominal or pelvic muscles and surrounding connective tissue. Myalgia refers to tenderness (allodynia or hyperalgesia) of the muscles on palpation, in the absence of increased tone (109). If increased muscle tone is detected, the condition is termed abdominal or pelvic tension myalgia, and further defined as pelvic floor muscle (PFM) tension myalgia if the location of the tenderness and tone are specific to the PFM (109). Women with EAP are highly likely to be found to have PFM tension (110). PFM tension is more common in those with biopsy proven endometriosis than in women with persistent pelvic pain without endometriosis (82). Individuals with DIE have been found to have PFM tension in 29%, with inappropriate and weak PFM contraction, and inability to completely relax in up to 45% (111). Both peripheral and central nervous system changes have been implicated in the development of myalgia (112). Peripheral nociceptors in pelvic floor muscles may contribute to referred pain through central mechanisms, at the level of the dorsal horn (113).
Vulvodynia refers to vulvar pain of at least 3 months' duration, without clear identifiable cause (114). The most commonly reported subtype is provoked vestibulodynia (PVD) where pain is provoked and localized to the vulvar vestibule. Diagnostic criteria sometimes include positive cotton swab testing. PVD gives rise to superficial dyspareunia and has a negative impact on sexual functioning (114). Vulvodynia and endometriosis are comorbid in ~11% of affected individuals (115, 116). PVD has been diagnosed in individuals with persistent pelvic pain (with or without a diagnosis of endometriosis) in 33% (117). Moreover, PVD is reported in up to 74% of individuals with BPS (118). Central sensitization may contribute. Individuals with PVD exhibit decreased pain thresholds in regions distant to the vulva including the thumb and deltoid (119, 120). Studies related to changes in brain structure in individuals with PVD demonstrate mixed results, with a trend toward increased gray matter in pain modulating regions in younger women and decreased gray matter in older women (121). In pre-menopausal women, increased gray matter volume has been observed in the basal ganglia, hippocampus and sensorimotor cortices (122). PVD is associated with psychological distress including pain related anxiety and depression (123).
Endometriosis-associated pain and the mechanisms responsible for its initiation and persistence are complex. Therefore, EAP is difficult to treat. The frequent presence of comorbid pelvic pain syndromes adds to the difficulty. In this review, the terminology and mechanisms of EAP have been described. Mechanisms that are common between EAP and comorbid pain syndromes have been highlighted. It is clear that peripheral sensitization, central sensitization and cross-sensitization are important future therapeutic targets. It is prudent that clinicians attend to the biological, psychological and social factors contributing to individuals' experience of EAP, and screen for comorbid pelvic pain syndromes.
HF and CC conceived and designed the study. HM wrote the original manuscript. JD, ER, MH, LE, CR, LH, KH, and PR made comments and contributed to subsequent drafts of the manuscript. All authors contributed to the article and approved the submitted version.
PR, MH, JD, HF, and CC hold funding from the Medical Research Future Fund for endometriosis research (MRF1199715) and HF holds funding from the Victorian Cancer Agency.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Rowlands IJ, Abbott JA, Montgomery GW, Hockey R, Rogers P, Mishra GD. Prevalence and incidence of endometriosis in Australian women: a data linkage cohort study. BJOG. (2021) 128:657–65. doi: 10.1111/1471-0528.16447
2. Clement PB. The pathology of endometriosis: a survey of the many faces of a common disease emphasizing diagnostic pitfalls and unusual and newly appreciated aspects. Adv Anat Pathol. (2007) 14:241–60. doi: 10.1097/PAP.0b013e3180ca7d7b
3. Koninckx PR, Ussia A, Adamyan L, Wattiez A, Gomel V, Martin DC. Pathogenesis of endometriosis: the genetic/epigenetic theory. Fertil Steril. (2019) 111:327–40. doi: 10.1016/j.fertnstert.2018.10.013
4. Sourial S, Tempest N, Hapangama DK. Theories on the pathogenesis of endometriosis. Int J Reprod Med. (2014) 2014:179515. doi: 10.1155/2014/179515
5. Kennedy S, Mardon H, Barlow D. Familial endometriosis. J Assist Reprod Genet. (1995) 12:32–4. doi: 10.1007/BF02214126
6. Isidor B, Latypova X, Ploteau S. Familial deep endometriosis: a rare monogenic disease? Eur J Obstet Gynecol Reprod Biol. (2018) 221:190–3. doi: 10.1016/j.ejogrb.2017.11.025
7. Rahmioglu N, Nyholt DR, Morris AP, Missmer SA, Montgomery GW, Zondervan KT. Genetic variants underlying risk of endometriosis: insights from meta-analysis of eight genome-wide association and replication datasets. Hum Reprod Update. (2014) 20:702–16. doi: 10.1093/humupd/dmu015
8. Fung JN, Rogers PAW, Montgomery GW. Identifying the biological basis of GWAS hits for endometriosis. Biol Reprod. (2015) 92:87. doi: 10.1095/biolreprod.114.126458
9. Pitot MA, Bookwalter CA, Dudiak KM. Müllerian duct anomalies coincident with endometriosis: a review. Abdominal Radiol. (2020) 45:1723–40. doi: 10.1007/s00261-020-02465-y
10. Sampson JA. Peritoneal endometriosis due to the menstrual dissemination of endometrial tissue into the peritoneal cavity. Am J Obstet Gynecol. (1927) 14:422–69.
11. Missmer SA, Hankinson SE, Spiegelman D, Barbieri RL, Malspeis S, Willett WC, et al. Reproductive history and endometriosis among premenopausal women. Obstet Gynecol. (2004) 104:965–74. doi: 10.1097/01.AOG.0000142714.54857.f8
12. Sampson JA. The development of the implantation theory for the origin of peritoneal endometriosis. Am J Obstet Gynecol. (1940) 40:549–57.
13. Schrodt GR, Alcorn MO, Ibanez J. Endometriosis of the male urinary system: a case report. J Urol. (1980) 124:722–3. doi: 10.1016/S0022-5347(17)55627-X
14. Pinkert TC, Catlow CE, Straus R. Endometriosis of the urinary bladder in a man with prostatic carcinoma. Cancer. (1979) 43:1562–7. doi: 10.1002/1097-0142(197904)43:4<1562::AID-CNCR2820430451>3.0.CO;2-W
15. Sharma N, Todhe P, Ochieng P, Ramakrishna S. Refractory thoracic endometriosis. BMJ Case Rep. (2020) 13:e235965. doi: 10.1136/bcr-2020-235965
16. Maniglio P, Ricciardi E, Meli F, Vitale SG, Noventa M, Vitagliano A, et al. Catamenial pneumothorax caused by thoracic endometriosis. Radiol Case Rep. (2018) 13:81–5. doi: 10.1016/j.radcr.2017.09.003
17. Sasson IE, Taylor HS. Stem cells and the pathogenesis of endometriosis. Ann N Y Acad Sci. (2008) 1127:106–15. doi: 10.1196/annals.1434.014
18. Taylor HS, Kotlyar AM, Flores VA. Endometriosis is a chronic systemic disease: clinical challenges and novel innovations. Lancet. (2021) 397:839–52. doi: 10.1016/S0140-6736(21)00389-5
19. Braun DP, Muriana A, Gebel H, Rotman C, Rana N, Dmowski WP. Monocyte-mediated enhancement of endometrial cell proliferation in women with endometriosis. Fertil Steril. (1994) 61:78–84. doi: 10.1016/S0015-0282(16)56456-5
20. Patel BG, Rudnicki M, Yu J, Shu Y, Taylor RN. Progesterone resistance in endometriosis: origins, consequences and interventions. Acta Obstet Gynecol Scand. (2017) 96:623–32. doi: 10.1111/aogs.13156
21. Carneiro MM, Filogônio IDDS, Costa LMP, De Ávila I, Ferreira MC. Accuracy of clinical signs and symptoms in the diagnosis of endometriosis. J Endometr. (2010) 2:63–70. doi: 10.1177/228402651000200203
22. Guerriero S, Saba L, Pascual MA, Ajossa S, Rodriguez I, Mais V, et al. Transvaginal ultrasound vs magnetic resonance imaging for diagnosing deep infiltrating endometriosis: systematic review and meta-analysis. Ultrasound Obstetr Gynecol. (2018) 51:586–95. doi: 10.1002/uog.18961
23. Chowdary P, Stone K, Ma T, Readman E, McIlwaine K, Druitt M, et al. Multicentre retrospective study to assess diagnostic accuracy of ultrasound for superficial endometriosis—Are we any closer? Aust N Zeal J Obstetr Gynaecol. (2019) 59:279–84. doi: 10.1111/ajo.12911
24. Nnoaham KE, Hummelshoj L, Kennedy SH, Jenkinson C, Zondervan KT. Developing symptom-based predictive models of endometriosis as a clinical screening tool: results from a multicenter study. Fertil Steril. (2012) 98:692–701.e5. doi: 10.1016/j.fertnstert.2012.04.022
25. Vercellini P, Fedele L, Aimi G, Pietropaolo G, Consonni D, Crosignani PG. Association between endometriosis stage, lesion type, patient characteristics and severity of pelvic pain symptoms: a multivariate analysis of over 1000 patients. Hum Reprod. (2007) 22:266–71. doi: 10.1093/humrep/del339
26. Howard FM. Laparoscopic evaluation and treatment of women with chronic pelvic pain. Am Assoc Gynecol Laparosc. (1994) 1:325–31.
27. Matorras R, Rodríguez F, Pijoan JI, Etxanojauregui A, Neyro JL, Elorriaga MA, et al. Women who are not exposed to spermatozoa and infertile women have similar rates of stage I endometriosis. Fertil Steril. (2001) 76:923–8. doi: 10.1016/S0015-0282(01)02833-3
28. Sutton CJG, Ewen SP, Whitelaw N, Haines P. Prospective, randomized, double-blind, controlled trial of laser laparoscopy in the treatment of pelvic pain associated with minimal, mild, and moderate endometriosis. Fertil Steril. (1994) 62:696–700. doi: 10.1016/S0015-0282(16)56990-8
29. Abbott J, Hawe J, Hunter D, Holmes M, Finn P, Garry R. Laparoscopic excision of endometriosis: a randomized, placebo-controlled trial. Fertil Steril. (2004) 82:878–84. doi: 10.1016/j.fertnstert.2004.03.046
30. Dunselman GA, Vermeulen N, Becker C, Calhaz-Jorge C, D'Hooghe T, De Bie B, et al. ESHRE guideline: management of women with endometriosis. Hum Reprod. (2014) 29:400–12. doi: 10.1093/humrep/det457
31. National Institute for Health and Care Excellence. Endometriosis: diagnosis and management, NICE guideline [NG73]. London, UK: National Institute for Health and Care Excellence (2017). Available online at: https://www.nice.org.uk/guidance/ng73/resources/endometriosis-diagnosis-and-management-pdf-1837632548293.
32. Royal Australian and New Zealand College of Obstetricians and Gynaecologists. Australian Clinical Practice Guideline for the Diagnosis and Management of Endometriosis Melbourne, Australia. (2021). Available online at: https://ranzcog.edu.au/RANZCOG_SITE/media/RANZCOG-MEDIA/Women%27s%20Health/Statement%20and%20guidelines/Clinical%20-%20Gynaecology/Endometriosis-clinical-practice-guideline.pdf?ext=.pdf (accessed August 14, 2021).
33. Bellelis P, Dias JA Jr, Podgaec S, Gonzales M, Baracat EC, Abrão MS. Epidemiological and clinical aspects of pelvic endometriosis - series of cases. Rev Assoc Med Bras. (2010) 56:467–71. doi: 10.1590/s0104-42302010000400022
34. Lukic A, Di Properzio M, De Carlo S, Nobili F, Schimberni M, Bianchi P, et al. Quality of sex life in endometriosis patients with deep dyspareunia before and after laparoscopic treatment. Arch Gynecol Obstet. (2016) 293:583–90. doi: 10.1007/s00404-015-3832-9
35. Maddern J, Grundy L, Castro J, Brierley SM. Pain in endometriosis. Front Cell Neurosci. (2020) 14:590823. doi: 10.3389/fncel.2020.590823
36. Surrey ES, Soliman AM, Johnson SJ, Davis M, Castelli-Haley J, Snabes MC. Risk of developing comorbidities among women with endometriosis: a retrospective matched cohort study. J Womens Health. (2018) 27:1114–23. doi: 10.1089/jwh.2017.6432
37. International Association for the Study of Pain. IASP Terminology: Pain Terms. Washington, D.C., USA: International Association for the Study of Pain (2021). Available online at: https://www.iasp-pain.org/Education/Content.aspx?ItemNumber=1698 (accessed August 14, 2021).
38. International Association for the Study of Pain. Classification of Chronic Pain. 2nd ed. Washington, DC, USA: IASP (2012). Available online at: iasp-pain.org/PublicationsNews/Content.aspx?ItemNumber=1673&nav ItemNumber=677 (accessed August 14, 2021).
39. Allaire C, Aksoy T, Bedaiwy M, Britnell S, Noga HL, Yager H, et al. An interdisciplinary approach to endometriosis-associated persistent pelvic pain. J Endometr Pelvic Pain Disord. (2017) 9:77–86. doi: 10.5301/jeppd.5000284
40. Grundström H, Gerdle B, Alehagen S, Berterö C, Arendt-Nielsen L, Kjølhede P. Reduced pain thresholds and signs of sensitization in women with persistent pelvic pain and suspected endometriosis. Acta Obstet Gynecol Scand. (2019) 98:327–36. doi: 10.1111/aogs.13508
41. Mooney SS, Grover SR. The persistent pelvic pain study: Factors that influence outcomes in women referred to a public hospital with chronic pelvic pain – A study protocol. Aust N Zeal J Obstetr Gynaecol. (2021) 61:E6–11. doi: 10.1111/ajo.13289
42. World Health Organisation. International Classification of Diseases 11th Revision. Geneva: World Health Organisation (2019). Available online at: https://icd.who.int/en (accessed August 14, 2021).
43. Engeler D, Baranowski AP, Berghmans B, Borovicka J, Cottrell A, Dinis-Oliveira P, et al. EAU Guidelines on Chronic Pelvic Pain: European Association of Urology. (2021). Available online at: https://uroweb.org/guideline/chronic-pelvic-pain/ (accessed August 14, 2021).
44. Coxon L, Horne AW, Vincent K. Pathophysiology of endometriosis-associated pain: a review of pelvic and central nervous system mechanisms. Best Pract Res Clin Obstetr Gynaecol. (2018) 51:53–67. doi: 10.1016/j.bpobgyn.2018.01.014
45. Latthe P, Mignini L, Gray R, Hills R, Khan K. Factors predisposing women to chronic pelvic pain: systematic review. BMJ. (2006) 332:749–55. doi: 10.1136/bmj.38748.697465.55
46. Berkley KJ, Rapkin AJ, Papka RE. The pains of endometriosis. Science. (2005) 308:1587–9. doi: 10.1126/science.1111445
47. Stratton P, Berkley KJ. Chronic pelvic pain and endometriosis: translational evidence of the relationship and implications. Hum Reprod Update. (2011) 17:327–46. doi: 10.1093/humupd/dmq050
48. Arnold J, Barcena de Arellano ML, Rüster C, Vercellino GF, Chiantera V, Schneider A, et al. Imbalance between sympathetic and sensory innervation in peritoneal endometriosis. Brain Behav Immun. (2012) 26:132–41. doi: 10.1016/j.bbi.2011.08.004
49. Arnold J, Vercellino GF, Chiantera V, Schneider A, Mechsner S, Barcena De Arellano ML. Neuroimmunomodulatory alterations in non-lesional peritoneum close to peritoneal endometriosis. Neuroimmunomodulation. (2012) 20:9–18. doi: 10.1159/000342163
50. Sulaiman H, Gabella G, Davis C, Mutsaers SE, Boulos P, Laurent GJ, et al. Presence and distribution of sensory nerve fibers in human peritoneal adhesions. Ann Surg. (2001) 234:256–61. doi: 10.1097/00000658-200108000-00016
51. Struller F, Weinreich FJ, Horvath P, Kokkalis MK, Beckert S, Königsrainer A, et al. Peritoneal innervation: embryology and functional anatomy. Pleura Peritoneum. (2017) 2:153–61. doi: 10.1515/pp-2017-0024
52. Tanaka K, Kuwahara-Otani S, Maeda S, Minato Y, Yagi H. Possible role of the myelinated neural network in the parietal peritoneum in rats as a mechanoreceptor. Anatomical Rec. (2017) 300:1662–9. doi: 10.1002/ar.23613
53. Oosterlynck DJ, Meuleman C, Waer M, Koninckx PR. Transforming growth factor-β activity is increased in peritoneal fluid from women with endometriosis. Obstet Gynecol. (1994) 83:287–92.
54. Bersinger NA, von Roten S, Wunder DM, Raio L, Dreher E, Mueller MD. PAPP-A and osteoprotegerin, together with interleukin-8 and RANTES, are elevated in the peritoneal fluid of women with endometriosis. Am J Obstet Gynecol. (2006) 195:103–8. doi: 10.1016/j.ajog.2005.12.010
55. McKinnon B, Bersinger NA, Wotzkow C, Mueller MD. Endometriosis-associated nerve fibers, peritoneal fluid cytokine concentrations, and pain in endometriotic lesions from different locations. Fertil Steril. (2012) 97:373–80. doi: 10.1016/j.fertnstert.2011.11.011
56. Mori H, Sawairi M, Nakagawa M, Itoh N, Wada K, Tamaya T. Peritoneal fluid lnterleukin-1β and tumor necrosis factor in patients with benign gynecologic disease. Am J Reprod Immunol. (1991) 26:62–7. doi: 10.1111/j.1600-0897.1991.tb00972.x
57. Khorram O, Taylor RN, Ryan IP, Schall TJ, Landers DV. Peritoneal fluid concentrations of the cytokine RANTES correlate with the severity of endometriosis. Am J Obstet Gynecol. (1993) 169:1545–9. doi: 10.1016/0002-9378(93)90433-J
58. Arici A, Tazuke SI, Oral E, Olive DL, Attar E. Monocyte chemotactic protein-1 concentration in peritoneal fluid of women with endometriosis and its modulation of expression in mesothelial cells. Fertil Steril. (1997) 67:1065–72. doi: 10.1016/S0015-0282(97)81440-9
59. Morotti M, Vincent K, Becker CM. Mechanisms of pain in endometriosis. Eur J Obstetr Gynecol Reprod Biol. (2017) 209:8–13. doi: 10.1016/j.ejogrb.2016.07.497
60. Patel BG, Lenk EE, Lebovic DI, Shu Y, Yu J, Taylor RN. Pathogenesis of endometriosis: interaction between endocrine and inflammatory pathways. Best Pract Res Clin Obstetr Gynaecol. (2018) 50:50–60. doi: 10.1016/j.bpobgyn.2018.01.006
61. Zheng P, Zhang W, Leng J, Lang J. Research on central sensitization of endometriosis-associated pain: a systematic review of the literature. J Pain Res. (2019) 12:1447–56. doi: 10.2147/JPR.S197667
62. Burney RO, Lathi RB. Menstrual bleeding from an endometriotic lesion. Fertil Steril. (2009) 91:1926–7. doi: 10.1016/j.fertnstert.2008.08.125
63. Colgrave EM, Bittinger S, Healey M, Dior UP, Rogers PAW, Keast JR, et al. Superficial peritoneal endometriotic lesions are histologically diverse and rarely demonstrate menstrual cycle synchronicity with matched eutopic endometrium. Hum Reprod. (2020) 35:2701–14. doi: 10.1093/humrep/deaa249
64. Kamergorodsky G, Ribeiro PAA, Galvão MAL, Abrão MS, Donadio N, de Barros Moreira Lemos NL, et al. Histologic classification of specimens from women affected by superficial endometriosis, deeply infiltrating endometriosis, and ovarian endometriomas. Fertil Steril. (2009) 92:2074–7. doi: 10.1016/j.fertnstert.2009.05.086
65. Tokushige N, Markham R, Russell P, Fraser IS. High density of small nerve fibres in the functional layer of the endometrium in women with endometriosis. Hum Reprod. (2006) 21:782–7. doi: 10.1093/humrep/dei368
66. Tokushige N, Russell P, Black K, Barrera H, Dubinovsky S, Markham R, et al. Nerve fibers in ovarian endometriomas. Fertil Steril. (2010) 94:1944–7. doi: 10.1016/j.fertnstert.2009.12.074
67. Anaf V, El Nakadi I, De Moor V, Chapron C, Pistofidis G, Noel JC. Increased nerve density in deep infiltrating endometriotic nodules. Gynecol Obstet Invest. (2011) 71:112–7. doi: 10.1159/000320750
68. Yan D, Liu X, Guo SW. Neuropeptides substance p and calcitonin gene related peptide accelerate the development and fibrogenesis of endometriosis. Sci Rep. (2019) 9:2698. doi: 10.1038/s41598-019-39170-w
69. Liu J, Liu X, Duan K, Zhang Y, Guo SW. The expression and functionality of transient receptor potential vanilloid 1 in ovarian endometriomas. Reprod Sci. (2012) 19:1110–24. doi: 10.1177/1933719112443876
70. Anaf V, Simon P, El Nakadi I, Fayt I, Simonart T, Buxant F, et al. Hyperalgesia, nerve infiltration and nerve growth factor expression in deep adenomyotic nodules, peritoneal and ovarian endometriosis. Hum Reprod. (2002) 17:1895–900. doi: 10.1093/humrep/17.7.1895
71. Siquara De Sousa AC, Capek S, Amrami KK, Spinner RJ. Neural involvement in endometriosis: review of anatomic distribution and mechanisms. Clin Anat. (2015) 28:1029–38. doi: 10.1002/ca.22617
72. Langebrekke A, Qvigstad E. Endometriosis entrapment of the obturator nerve after previous cervical cancer surgery. Fertil Steril. (2009) 91:622–3. doi: 10.1016/j.fertnstert.2008.03.024
73. Liang Y, Liu D, Yang F, Pan W, Zeng F, Wu J, et al. Perineural invasion in endometriotic lesions contributes to endometriosis-associated pain. J Pain Res. (2018) 11:1999–2009. doi: 10.2147/JPR.S168715
74. Pacchiarotti A, Milazzo GN, Biasiotta A, Truini A, Antonini G, Frati P, et al. Pain in the upper anterior-lateral part of the thigh in women affected by endometriosis: study of sensitive neuropathy. Fertil Steril. (2013) 100:122–6. doi: 10.1016/j.fertnstert.2013.02.045
75. Asante A, Taylor RN. Endometriosis: the role of neuroangiogenesis. Annu Rev Physiol. (2011) 73:163–82. doi: 10.1146/annurev-physiol-012110-142158
76. Kajitani T, Maruyama T, Asada H, Uchida H, Oda H, Uchida S, et al. Possible involvement of nerve growth factor in dysmenorrhea and dyspareunia associated with endometriosis. Endocr J. (2013) 60:1155–64. doi: 10.1507/endocrj.EJ13-0027
77. Tamburro S, Canis M, Albuisson E, Dechelotte P, Darcha C, Mage G. Expression of transforming growth factor β1 in nerve fibers is related to dysmenorrhea and laparoscopic appearance of endometriotic implants. Fertil Steril. (2003) 80:1131–6. doi: 10.1016/S0015-0282(03)01182-8
78. Ferrero S, Haas S, Remorgida V, Camerini G, Fulcheri E, Ragni N, et al. Loss of sympathetic nerve fibers in intestinal endometriosis. Fertil Steril. (2010) 94:2817–9. doi: 10.1016/j.fertnstert.2010.06.069
79. Wei Y, Liang Y, Lin H, Dai Y, Yao S. Autonomic nervous system and inflammation interaction in endometriosis-associated pain. J Neuroinflammation. (2020) 17:80. doi: 10.1186/s12974-020-01752-1
80. Ji RR, Kohno T, Moore KA, Woolf CJ. Central sensitization and LTP: do pain and memory share similar mechanisms? Trends Neurosci. (2003) 26:696–705. doi: 10.1016/j.tins.2003.09.017
81. Arendt-Nielsen L, Morlion B, Perrot S, Dahan A, Dickenson A, Kress HG, et al. Assessment and manifestation of central sensitisation across different chronic pain conditions. Eur J Pain. (2018) 22:216–41. doi: 10.1002/ejp.1140
82. Stratton P, Khachikyan I, Sinaii N, Ortiz R, Shah J. Association of chronic pelvic pain and endometriosis with signs of sensitization and myofascial pain. Obstet Gynecol. (2015) 125:719–28. doi: 10.1097/AOG.0000000000000663
83. May A. Structural brain imaging: a window into chronic pain. Neuroscientist. (2011) 17:209–20. doi: 10.1177/1073858410396220
84. As-Sanie S, Harris RE, Napadow V, Kim J, Neshewat G, Kairys A, et al. Changes in regional gray matter volume in women with chronic pelvic pain: a voxel-based morphometry study. Pain. (2012) 153:1006–14. doi: 10.1016/j.pain.2012.01.032
85. As-Sanie S, Kim J, Schmidt-Wilcke T. Functional connectivity is associated with altered brain chemistry in women with endometriosis-associated chronic pelvic pain. J Pain. 2015:S1526–5900. doi: 10.1016/j.jpain.2015.09.008
86. Vincent K, Warnaby C, Stagg CJ, Moore J, Kennedy S, Tracey I. Dysmenorrhoea is associated with central changes in otherwise healthy women. Pain. (2011) 152:1966–75. doi: 10.1016/j.pain.2011.03.029
87. Malykhina AP. Neural mechanisms of pelvic organ cross-sensitization. Neuroscience. (2007) 149:660–72. doi: 10.1016/j.neuroscience.2007.07.053
88. Hoffman D. Understanding multisymptom presentations in chronic pelvic pain: the inter-relationships between the viscera and myofascial pelvic floor dysfunction. Curr Pain Headache Rep. (2011) 15:343–6. doi: 10.1007/s11916-011-0215-1
89. Affaitati G, Costantini R, Tana C, Cipollone F, Giamberardino MA. Co-occurrence of pain syndromes. J Neural Transm. (2020) 127:625–46. doi: 10.1007/s00702-019-02107-8
90. Gao M, Koupil I, Sjöqvist H, Karlsson H, Lalitkumar S, Dalman C, et al. Psychiatric comorbidity among women with endometriosis: nationwide cohort study in Sweden. Obstetr Gynecol Survey. (2020) 75:744–5. doi: 10.1097/01.ogx.0000723716.77258.ae
91. Galambos A, Szabó E, Nagy Z, Édes AE, Kocsel N, Juhász G, et al. A systematic review of structural and functional MRI studies on pain catastrophizing. J Pain Res. (2019) 12:1155–78. doi: 10.2147/JPR.S192246
92. Surrey ES, Soliman AM, Yang H, Du EX, Su B. Treatment patterns, complications, and health care utilization among endometriosis patients undergoing a laparoscopy or a hysterectomy: a retrospective claims analysis. Adv Ther. (2017) 34:2436–51. doi: 10.1007/s12325-017-0619-3
93. Bryant C, Cockburn R, Plante AF, Chia A. The psychological profile of women presenting to a multidisciplinary clinic for chronic pelvic pain: high levels of psychological dysfunction and implications for practice. J Pain Res. (2016) 9:1049–56. doi: 10.2147/JPR.S115065
94. Sewell M, Churilov L, Mooney S, Ma T, Maher P, Grover SR. Chronic pelvic pain-pain catastrophizing, pelvic pain and quality of life. Scand J Pain. (2018) 18:441–8. doi: 10.1515/sjpain-2017-0181
95. McPeak AE, Allaire C, Williams C, Albert A, Lisonkova S, Yong PJ. Pain catastrophizing and pain health-related quality-of-life in endometriosis. Clin J Pain. (2018) 34:349–56. doi: 10.1097/AJP.0000000000000539
96. Chronic Pain Research Alliance. Impact of Chronic Overlapping Pain Conditions on Public Health and the Urgent Need for Safe and Effective treatment. Milwaukee, WI, USA: Chronic Pain Research Alliance (2015). Available online at: http://www.chronicpainresearch.org/public/CPRA_WhitePaper_2015-FINAL-Digital.pdf (accessed August 14, 2021).
97. van de Merwe JP, Nordling J, Bouchelouche P, Bouchelouche K, Cervigni M, Daha LK, et al. Diagnostic criteria, classification, and nomenclature for painful bladder syndrome/interstitial cystitis: an ESSIC proposal. Eur Urol. (2008) 53:60–7. doi: 10.1016/j.eururo.2007.09.019
98. Tirlapur SA, Kuhrt K, Chaliha C, Ball E, Meads C, Khan KS. The 'evil twin syndrome' in chronic pelvic pain: a systematic review of prevalence studies of bladder pain syndrome and endometriosis. Int J Surg. (2013) 11:233–7. doi: 10.1016/j.ijsu.2013.02.003
99. Cheng C, Rosamilia A, Healey M. Diagnosis of interstitial cystitis/bladder pain syndrome in women with chronic pelvic pain: a prospective observational study. Int Urogynecol J. (2012) 23:1361–6. doi: 10.1007/s00192-012-1711-5
100. Collings R, Healey M, Dior U, Erwin R, Rosamilia A, Cheng C. Effect of investigative laparoscopy on bladder pain syndrome: a prospective cohort trial. Int Urogynecol J. (2020) 31:1583–91. doi: 10.1007/s00192-019-04023-7
101. Wu CC, Chung SD, Lin HC. Endometriosis increased the risk of bladder pain syndrome/interstitial cystitis: a population-based study. Neurourol Urodyn. (2018) 37:1413–8. doi: 10.1002/nau.23462
102. Lotz M, Villiger P, Hugli T, Koziol J, Zuraw BL. Interleukin-6 and interstitial cystitis. J Urol. (1994) 152:869–73. doi: 10.1016/S0022-5347(17)32594-6
103. Birder LA. Pathophysiology of interstitial cystitis. Int J Urol. (2019) 26:12–5. doi: 10.1111/iju.13985
104. Rome Foundation. Rome IV Criteria Raleigh. North Carolina, USA: Rome Foundation (2016). Available online at: https://theromefoundation.org/rome-iv/rome-iv-criteria/ (accessed August 14, 2021).
105. Schomacker ML, Hansen KE, Ramlau-Hansen CH, Forman A. Is endometriosis associated with irritable bowel syndrome? A cross-sectional study. Eur J Obstetr Gynecol Reprod Biol. (2018) 231:65–9. doi: 10.1016/j.ejogrb.2018.10.023
106. DiVasta AD, Zimmerman LA, Vitonis AF, Fadayomi AB, Missmer SA. Overlap between irritable bowel syndrome diagnosis and endometriosis in adolescents. Clin Gastroenterol Hepatol. (2021) 19:528–37.e1. doi: 10.1016/j.cgh.2020.03.014
107. Wouters MM, Balemans D, Van Wanrooy S, Dooley J, Cibert-Goton V, Alpizar YA, et al. Histamine receptor H1-mediated sensitization of TRPV1 mediates visceral hypersensitivity and symptoms in patients with irritable bowel syndrome. Gastroenterology. (2016) 150:875–87.e9. doi: 10.1053/j.gastro.2015.12.034
108. Tillisch K, Mayer EA, Labus JS. Quantitative meta-analysis identifies brain regions activated during rectal distension in irritable bowel syndrome. Gastroenterology. (2011) 140:91–100. doi: 10.1053/j.gastro.2010.07.053
109. Frawley H, Shelly B, Morin M, Bernard S, Bø K, Digesu GA, et al. An International Continence Society (ICS) report on the terminology for pelvic floor muscle assessment. Neurourol Urodyn. (2021) 40:1217–60. doi: 10.1002/nau.24658
110. Phan VT, Stratton P, Tandon HK, Sinaii N, Aredo JV, Karp BI, et al. Widespread myofascial dysfunction and sensitisation in women with endometriosis-associated chronic pelvic pain: a cross-sectional study. Eur J Pain. (2021) 25:831–40. doi: 10.1002/ejp.1713
111. Fraga MV, Oliveira Brito LG, Yela DA, de Mira TA, Benetti-Pinto CL. Pelvic floor muscle dysfunctions in women with deep infiltrative endometriosis: an underestimated association. Int J Clin Pract. (2021) 75:e14350. doi: 10.1111/ijcp.14350
112. Meister MR, Shivakumar N, Sutcliffe S, Spitznagle T, Lowder JL. Physical examination techniques for the assessment of pelvic floor myofascial pain: a systematic review. Am J Obstet Gynecol. (2018) 219:497.e1-e13. doi: 10.1016/j.ajog.2018.06.014
113. Denneny D, Frawley HC, Petersen K, McLoughlin R, Brook S, Hassan S, et al. Trigger point manual therapy for the treatment of chronic noncancer pain in adults: a systematic review and meta-analysis. Arch Phys Med Rehabil. (2019) 100:562–77. doi: 10.1016/j.apmr.2018.06.019
114. Bornstein J, Goldstein AT, Stockdale CK, Bergeron S, Pukall C, Zolnoun D, et al. 2015 ISSVD, ISSWSH, and IPPS consensus terminology and classification of persistent vulvar pain and vulvodynia. J Sex Med. (2016) 13:607–12. doi: 10.1016/j.jsxm.2016.02.167
115. Smorgick N, Marsh CA, As-Sanie S, Smith YR, Quint EH. Prevalence of pain syndromes, mood conditions, and asthma in adolescents and young women with endometriosis. J Pediatr Adolesc Gynecol. (2013) 26:171–5. doi: 10.1016/j.jpag.2012.12.006
116. Graziottin A, Murina F, Gambini D, Taraborrelli S, Gardella B, Campo M. Vulvar pain: the revealing scenario of leading comorbidities in 1183 cases. Eur J Obstetr Gynecol Reprod Biol. (2020) 252:50–5. doi: 10.1016/j.ejogrb.2020.05.052
117. Bao C, Noga H, Allaire C, Williams C, Bedaiwy MA, Sadownik LA, et al. Provoked vestibulodynia in women with pelvic pain. Sex Med. (2019) 7:227–34. doi: 10.1016/j.esxm.2019.03.002
118. Gardella B, Porru D, Nappi RE, Daccò MD, Chiesa A, Spinillo A. Interstitial cystitis is associated with vulvodynia and sexual dysfunction-A case-control study. J Sex Med. (2011) 8:1726–34. doi: 10.1111/j.1743-6109.2011.02251.x
119. Giesecke J, Reed BD, Haefner HK, Giesecke T, Clauw DJ, Gracely RH. Quantitative sensory testing in vulvodynia patients and increased peripheral pressure pain sensitivity. Obstet Gynecol. (2004) 104:126–33. doi: 10.1097/01.AOG.0000129238.49397.4e
120. Pukall CF, Binik YM, Khalifé S, Amsel R, Abbott FV. Vestibular tactile and pain thresholds in women with vulvar vestibulitis syndrome. Pain. (2002) 96:163–75. doi: 10.1016/S0304-3959(01)00442-0
121. Schweinhardt P, Kuchinad A, Pukall CF, Bushnell MC. Increased gray matter density in young women with chronic vulvar pain. Pain. (2008) 140:411–9. doi: 10.1016/j.pain.2008.09.014
122. Bhatt RR, Gupta A, Rapkin A, Kilpatrick LA, Hamadani K, Pazmany E, et al. Altered gray matter volume in sensorimotor and thalamic regions associated with pain in localized provoked vulvodynia: a voxel-based morphometry study. Pain. (2019) 160:1529–40. doi: 10.1097/j.pain.0000000000001532
Keywords: endometriosis, persistent pelvic pain, peripheral sensitization, central sensitization, cross sensitization
Citation: McNamara HC, Frawley HC, Donoghue JF, Readman E, Healey M, Ellett L, Reddington C, Hicks LJ, Harlow K, Rogers PAW and Cheng C (2021) Peripheral, Central, and Cross Sensitization in Endometriosis-Associated Pain and Comorbid Pain Syndromes. Front. Reprod. Health 3:729642. doi: 10.3389/frph.2021.729642
Received: 23 June 2021; Accepted: 06 August 2021;
Published: 01 September 2021.
Edited by:
Cecilia H. M. Ng, Jean Hailes for Women's Health, AustraliaReviewed by:
Donatella Caserta, Sapienza University of Rome, ItalyCopyright © 2021 McNamara, Frawley, Donoghue, Readman, Healey, Ellett, Reddington, Hicks, Harlow, Rogers and Cheng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Helen C. McNamara, aGVsZW4ubWNuYW1hcmFAdGhld29tZW5zLm9yZy5hdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.