 Idhaliz Flores-Caldera1,2*
Idhaliz Flores-Caldera1,2* Paola M. Ramos-Echevarría1
Paola M. Ramos-Echevarría1 José A. Oliveras-Torres1
José A. Oliveras-Torres1 Natasha Santos-Piñero1Estefanía D. Rivera-Mudafort1Denisse M. Soto-Soto1,3Brian Hernández-Colón1
Natasha Santos-Piñero1Estefanía D. Rivera-Mudafort1Denisse M. Soto-Soto1,3Brian Hernández-Colón1 Luis E. Rivera-Hiraldo3Loraine Mas1
Luis E. Rivera-Hiraldo3Loraine Mas1 Mary Rodríguez-Rabassa4Nabal J. Bracero5
Mary Rodríguez-Rabassa4Nabal J. Bracero5 Edgardo Rolla6,7Ibero-American Endometriosis Association†
Edgardo Rolla6,7Ibero-American Endometriosis Association†- 1Department of Basic Sciences, Ponce Health Sciences University, Ponce, Puerto Rico
- 2Department of Ob-Gyn, Ponce Health Sciences University, Ponce, Puerto Rico
- 3San Lucas Episcopal Medical Center, Ponce, Puerto Rico
- 4School of Behavioral and Brain Sciences, Ponce Health Sciences University, Ponce, Puerto Rico
- 5Department of Ob-Gyn, University of Puerto Rico, San J uan, Puerto Rico
- 6Sociedad Argentina de Endometriosis, Buenos Aires, Argentina
- 7Sociedad Argentina de Cirugía Laparoscópica, Buenos Aires, Argentina
Background: An international collaborative study was conducted to determine the demographic and clinical profiles of Hispanic/Latinx endometriosis patients from Latin America and Spain using the Minimal Clinical Questionnaire developed by the World Endometriosis Research Foundation (WERF) Endometriosis Phenome and Biobanking Harmonization Project (EPHect).
Methods: This is a cross-sectional study to collect self-reported data on demographics, lifestyle, and endometriosis symptoms of Hispanic/Latinx endometriosis patients from April 2019 to February 2020. The EPHect Minimal Clinical Questionnaire (EPQ-M) was translated into Spanish. Comprehension and length of the translated survey were assessed by Spanish-speaking women. An electronic link was distributed via social media of endometriosis patient associations from 11 Latin American countries and Spain. Descriptive statistics (frequency, means and SD, percentages, and proportions) and correlations were conducted using SPSSv26.
Results: The questionnaire was completed by 1,378 participants from 23 countries; 94.6% had self-reported diagnosis of endometriosis. Diagnostic delay was 6.6 years. Most participants had higher education, private health insurance, and were employed. The most common symptoms were back/leg pain (85.4%) and fatigue (80.7%). The mean number of children was 1.5; 34.4% had miscarriages; the mean length of infertility was 3.7 years; 47.2% reported pregnancy complications. The most common hormone treatment was oral contraceptives (47.0%). The most common comorbidities were migraines (24.1%), polycystic ovary syndrome (PCOS) (22.2%), and irritable bowel syndrome (21.1%). Most participants (97.0%) experienced pelvic pain during menses; for 78.7%, pain was severe; 86.4% reported dyspareunia. The mean age of dysmenorrhea onset was 16.2 years (SD ± 6.1). Hormone treatments were underutilized, while impact was substantial. Pain catastrophizing scores were significantly correlated with pain intensity (p < 0.001).
Conclusion: This is the first comprehensive effort to generate a clinical–demographic profile of Hispanic/Latinx endometriosis patients. Differences in clinical presentation compared to other cohorts included higher prevalence and severity of dysmenorrhea and dyspareunia and high levels of pain catastrophizing. Though future studies are needed to dissect the impact of race and ethnicity on pain and impact, this profile is the first step to facilitate the recognition of risk factors and diagnostic features and promote improved clinical management of this patient population. The EPHect questionnaire is an efficient tool to capture data to allow comparisons across ethnicities and geographic regions and tackle disparities in endometriosis research.
Introduction
Endometriosis is a gynecologic condition diagnosed in 6–10% of women of reproductive age, with a prevalence of 20–50% in infertile women and 71–87% of those with chronic pelvic pain (1–3). Hispanic/Latinx persons with endometriosis are underrepresented in research databases and thus unlikely to benefit from research on pathophysiology, biomarkers, and novel treatments (4). The World Endometriosis Research Foundation (WERF) Endometriosis Phenome and Biobanking Harmonization Project (EPHect) provides standardized protocols based on evidence to allow accrual of detailed surgical, clinical, and epidemiologic data from endometriosis patients to support future research. EPHect developed a clinical questionnaire to obtain self-reported demographic and clinical information to allow cross-sectional studies to better understand differences in the endometriosis phenome across populations (5–9).
A PubMed search using the keywords “endometriosis,” “ethnicity,” “Hispanic,” and “Latina” resulted in only three reports on the prevalence of endometriosis symptoms by race/ethnicity. The Nurse's Health Study II's multivariate hazard models concluded that Black [relative risk (RR) 0.6, 95% confidence interval (CI): 0.4–0.9] and Hispanic women (RR 0.6, 95% CI: 0.4–1.0) had a 40% lower rate of endometriosis diagnosis compared with White women (10). A nationwide study by Eggert et al. found rates (cases per 100,000) of endometriosis ranging from 126.2 (Asian countries) to 42.3 (Eritrea/Ethiopia/Somalia), with Latin American countries at 90.9 compared to 101.9 among Sweden-born patients (11). Both studies conclude that non-Hispanic white women have a higher likelihood of a diagnosis of endometriosis compared to other ethnic groups. However, Bougie et al. stated that there is not enough evidence to definitely conclude that the prevalence of endometriosis in Hispanic/Latinx populations is lower. In their recent systematic review and meta-analysis on the ethnic presentation of endometriosis, they identified only five studies that included patients of Hispanic/Latinx background, compared to 16 studies of White vs. Black women, and 10 studies of White vs. Asian women (12, 13). In total, these studies included only 14,951 Hispanic/Latinx patients compared to 65,332 White patients. This meta-analysis showed that endometriosis was more prevalent in Asian women (OR 1.63, 95% CI: 1.03–2.58), less prevalent in Black women (OR 0.49, 95% CI: 0.29–0.83), and less common in Hispanic women (OR 0.46, 95% CI: 0.14–1.50—not statistically significant), compared to White non-Hispanic women.
Lack of data on Hispanic/Latinx patients with endometriosis highlights the need to conduct more epidemiological investigations with diverse populations of patients to evaluate whether there are racial/ethnic differences in disease prevalence, clinical presentation, and response to treatments. More studies are needed to establish if differences in the prevalence of endometriosis and its clinical presentation among ethnic groups are due to socioeconomic factors that impact access to care, to biological/genetic correlates, or to cultural influences on healthcare seeking. To fill this knowledge gap, we aimed to obtain for the first time the clinical profile of endometriosis patients from Latin America and the Caribbean using a Spanish translation of the EPHect's Minimal Clinical Questionnaire (EPQ-M) (9). Here, we report data collected from Spanish-speaking endometriosis patients from 23 countries on demographics, lifestyle, Ob-Gyn, clinical history, pelvic pain symptoms, pain catastrophizing, impact of pain on quality of life, and utilization of pain medications and hormonal treatments.
Materials and Methods
This study was approved by the Institutional Review Board of the Ponce Research Institute of the Ponce Health Sciences University (PHSU) (IRB Approval #1811001620).
EPHect Survey
The EPHect's EPQ-M was designed to collect self-reported, cross-sectional data from endometriosis patients, including personal information/demographics, lifestyle and risk behaviors, obstetrical and gynecological history, fertility, medical and surgical history, pain intensity (using the numerical rating scale—NRS), pain catastrophizing, quality of life, and surgical and medical treatment. It also captures the level of pain, treatment regimen, and medication use. The EPQ-M quantifies many symptoms, including 71 quality-of-life measures and pain-related variables (McGill Pain Short Questionnaire). Confirmation of self-reported diagnosis by medical chart review was high—on average 84% overall when combining the evaluation of clinical, surgical, and pathology records (and up to 95% in some of the cohorts). These data suggest that patients with endometriosis remember with high accuracy if they have been diagnosed by a physician, especially if the diagnosis was done by surgery (14).
Pain Catastrophizing Scale
The Pain Catastrophizing Scale (PCS) was used as a self-reported measure of catastrophic thinking (15). It evaluates three dimensions of catastrophizing: helplessness, rumination, and magnification. The items are scored from 0 (“not at all”) to 4 (“all the time”) for a total score of 52. A score higher than 30 is considered clinically relevant, and it identifies a population with a higher risk of chronicity and disability regarding pain.
Survey Translation and Validation
A group of endometriosis experts from Latin America translated the EPQ-M survey into Spanish. A certified translator conducted a back-translation to the English version to verify its accuracy. Twenty pre-menopausal women, with and without endometriosis, assessed the comprehension, vocabulary, and length of the survey during one-on-one interviews. Anonymous responses were analyzed quantitatively and qualitatively.
Survey Distribution
The validated Spanish EPQ-M was disseminated from April 2019 to February 2020 via a REDCap link (16) posted in social media platforms and email in collaboration with endometriosis patient support associations in Puerto Rico, Argentina, Colombia, Mexico, Panama, Costa Rica, Dominican Republic, Chile, Peru, Venezuela, and Spain. The questionnaire was self-administered, following an introductory page with instructions and IRB-specific language stating that the study was anonymous and voluntary. Data were captured electronically without identifiers.
Data Analysis
The quality of data was evaluated and then imported to SPSSv26 (IBM Corp, Armonk, NY) for descriptive analysis. The analysis included frequencies and percentages and means and standard deviation. Pearson's correlations were calculated between PCS scores and pain intensity (dysmenorrhea, dyspareunia, and general pelvic pain) measured by the NRS. Data were subdivided into the following categories: pain and its impact, pain catastrophizing, and medical and surgical treatments. Graphical representations of data were generated using GraphPad Prism v9 (San Diego, CA). Percentages were calculated based on the number of responses per question.
Results
Survey Validation
Twenty participants (10 women with and 10 women without endometriosis) evaluated the survey on length, complexity, difficulty, sensitivity of questions, and usefulness of the tool for research. The mean age of evaluators was 35.4+/−7.3 years, and the majority (17/20) had at least a bachelor's degree. Most (16/20) indicated that it took them 20 min or less to evaluate the questionnaire.
Quantitative Data Analysis
The majority of the evaluators reported that the questionnaire was “moderately long” (Figure 1). Only four evaluators considered the length of the survey appropriate (all were endometriosis patients). The complexity and difficulty of the survey were well-accepted. Only one evaluator mentioned that survey included uncomfortable questions. All of the evaluators considered it useful for endometriosis-focused research.
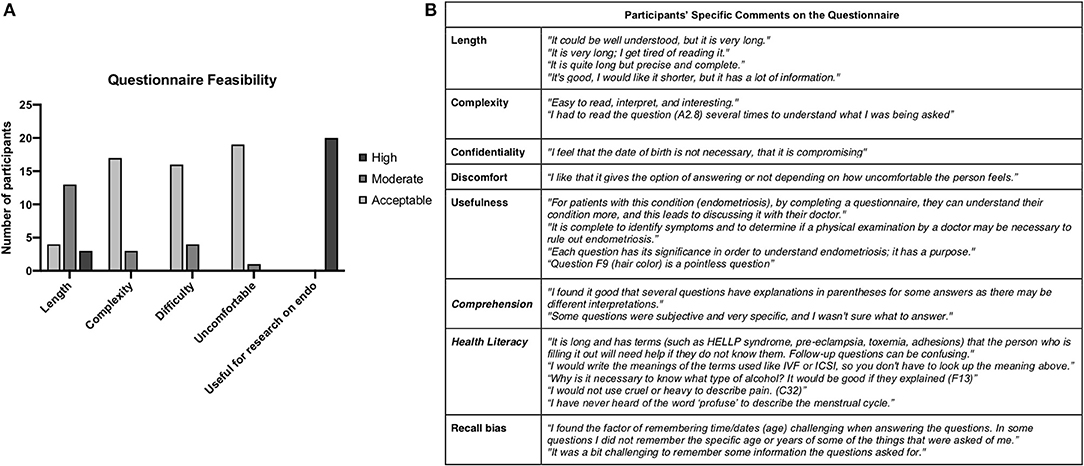
Figure 1. Validation of the Spanish EPhect clinical minimal questionnaire. (A) Quantitative assessment of feasibility. (B) Specific comments made by questionnaire evaluators.
Qualitative Data Analysis
Specific comments on the questionnaire are summarized in Figure 1.
Survey Results
Sociodemographics
The survey linked was accessed a total of 2,352 times, and 1,378 individuals from 23 countries answered the questionnaire. Percentages were calculated based on the number of responses per question. The mean age of the participants was 33.7 (SD ± 7.2) (Table 1). The majority of participants (~80%) were employed full time or part time; 42.7% completed at least a college degree. Six of every 10 patients had private insurance.
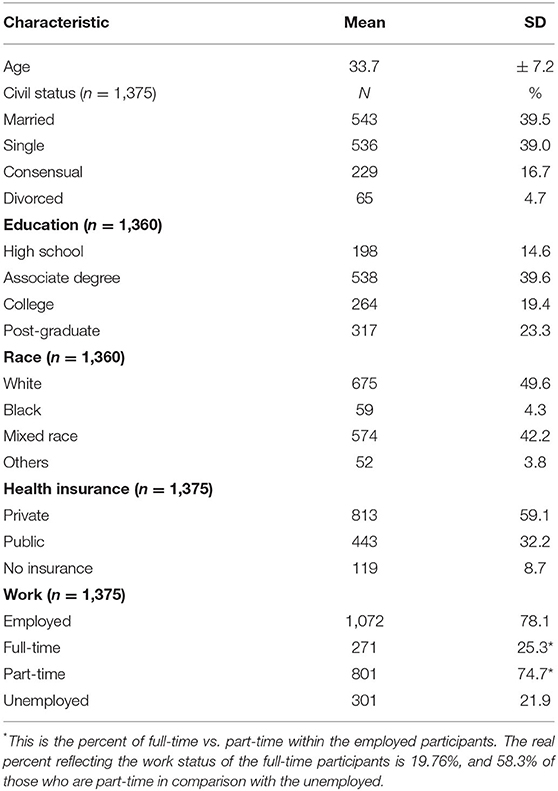
Table 1. Sociodemographic characteristics of the women with endometriosis from Ibero-America.
Almost all (98.3%, n = 1,323/1,346) participants self-identified as Hispanic/Latina; half (49.6%) identified as White, 42.2% as mixed race, and 4.3% as Black (Table 1). Supplementary Table 1 shows the racial distribution of participants. Most participants (15.7%, n = 201/1,277) were from Puerto Rico, Panama (15.0%, n = 191/1,277), Argentina (14.5%, n = 185/1,277) Colombia (11.5%, n = 147/1,277), and Costa Rica (7.5%, n = 96/1,277) (Figure 2). Patients from Chile, Dominican Republic, Mexico, Peru, Venezuela, and Spain, among other countries, also participated.

Figure 2. Countries of birth of study participants. Responses were received from 23 countries in South and Central America, the Caribbean, Spain, and the USA.
Lifestyle Factors
Exercise
Overall, from 9.2% (walking) to 84.4% (swimming) of participants reported not exercising at all. A healthy lifestyle characterized by exercising regularly over 3 h per week was reported by 27% or less. During the previous 12 months, the top three physical activities reported were walking, jogging/running, and aerobic exercises (Figure 3A). The mean BMI was 25.3 (SD ± 5.5).
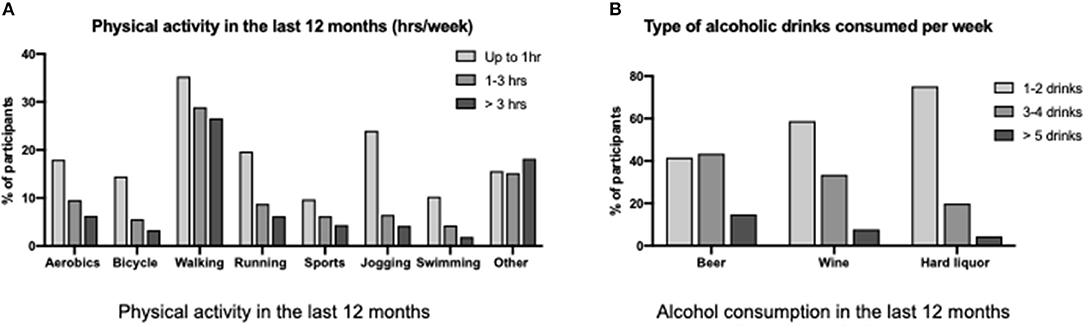
Figure 3. Lifestyle factors reported by participants. (A) Physical activity. (B) Alcohol consumption.
Risk Behaviors
Alcohol consumption was common overall (44.5%, n = 609/1,370) (Figure 3B). However, the risk level of alcohol consumption (over five drinks per week) was reported only by 14.8% for beer (n = 86/575), 7.7% for wine (n = 41/534), and 4.4% for hard liquor (n = 24/492). Regarding cigarette use, 19.7% (n = 271/1,375) reported to have smoked more than 100 cigarettes in their life, and only 9.4% (n = 129/1,371) are currently smokers.
Gynecologic and Obstetrical History
Menstrual Period Characteristics
The mean age at menarche of participants was 11.8 years of age (SD ± 1.61) (Table 2). Most (70.8%, n = 658/930) participants reported a regular cycle, with an average of 21–35 days reported by 63.2% (n = 565/894). Cycles of >35 days were reported by 3.7% (n = 33/894). On average, participants reported 6.5 days (SD ± 6.10) of menstruation. Moderate–heavy menstrual flow was reported by 84.8% (n = 792/934). Menorrhagia, defined as more than 7 days with a profuse menstrual flow, was reported by 11.8% (n = 91/768). During the prior 3 months, 30.9% (n = 424/1,372) reported not having menstrual periods; reasons included hormonal treatment (63.2%, n = 268), hysterectomy (19.1%, n = 81), pregnancy or breastfeeding (4.2%, n = 18), and menopause (4.0%, n = 17).
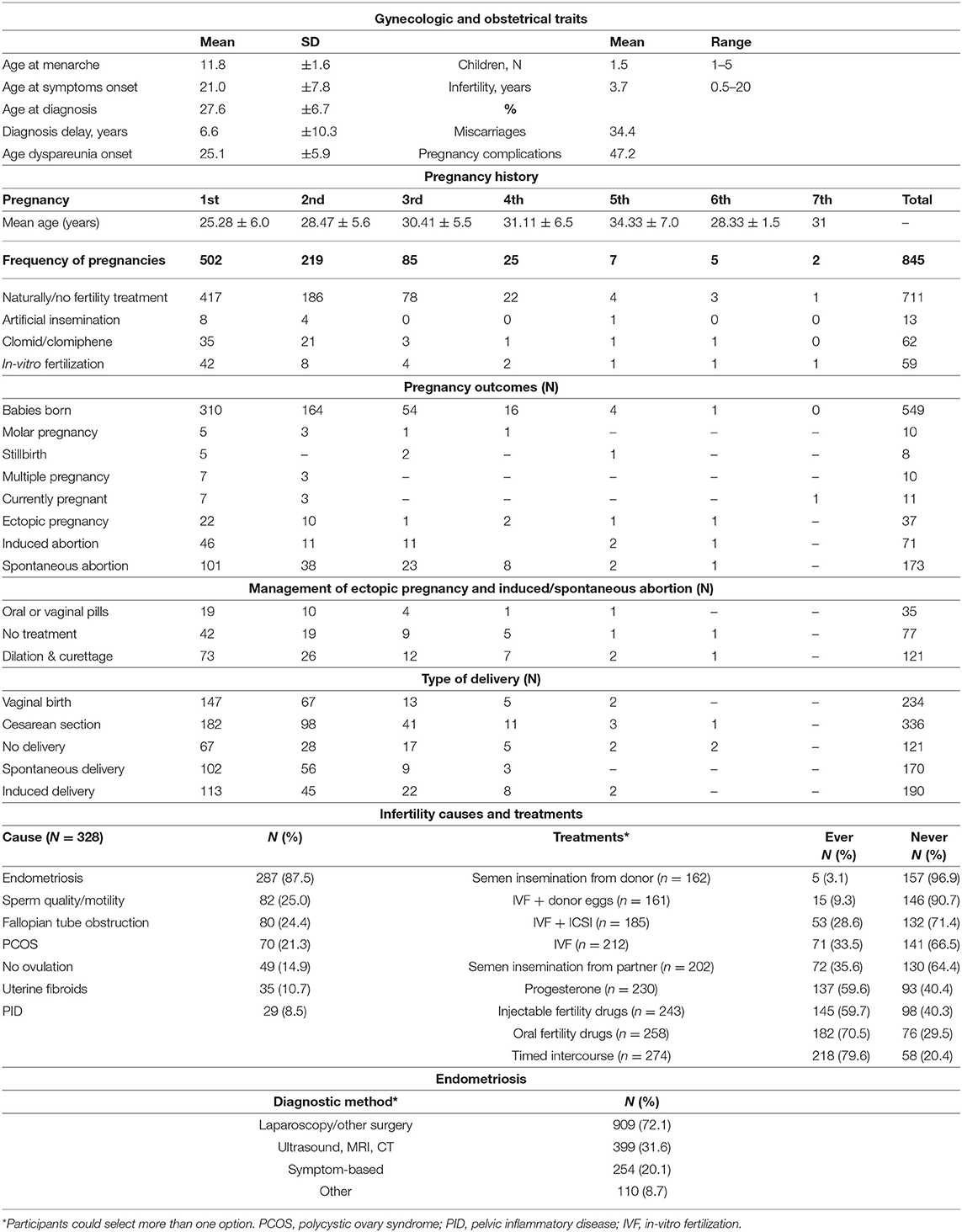
Table 2. Gynecologic and obstetrical traits of endometriosis patients from Ibero-America.
Obstetrical History
Regardless of outcome, 37.7% (n = 502/1,331) of participants reported at least one pregnancy. The mean age at first pregnancy was 25.3 years (SD ± 6.00) (range: 12–41 years old) (Table 2). More than half of all pregnancies reported (59.4%, n = 502/845) were first-time pregnancies; of these, 83.1% (n = 417) were achieved naturally and 61.8% (n = 310) yielded live births (Figure 4A). Only eight stillbirths were reported out of a total of 845 pregnancies (0.9%). Live births were delivered most commonly by C-section (58.7%, n = 182/310), followed by vaginal birth (47.4%, n = 147/310). Of all pregnancies, 20.5% (n = 173/845) resulted in spontaneous abortions. Lactation length ranged from 10 to 26 months, increasing with pregnancy number.
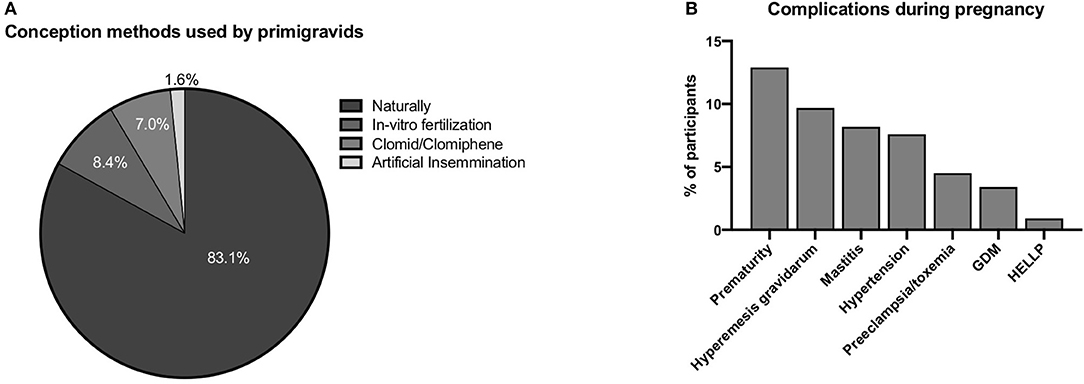
Figure 4. Obstetric characteristics of the study participants. (A) Conception methods. (B) Pregnancy complications.
Few molar (1.2%) or ectopic pregnancies (4.4%) were reported. Dilatation and curettage (D&C) was the treatment most often employed after spontaneous abortions (34.8%, n = 73/210) (Table 2). The most common obstetric complications were prematurity and hyperemesis gravidarum (Figure 4B). Rates of preeclampsia, hypertension, and gestational diabetes were 4.5, 7.6, and 3.4%, respectively.
Infertility History
When asked if they have been trying to conceive for over 6 months, 42.9% (n = 488/1,137) of participants responded yes, with a mean time of 3.7 years (SD ± 3.2) trying (Table 2). Of those, 67.2% (n = 328) underwent infertility workup. Endometriosis was reported in 87.5% (n = 287/328) of the cases, followed by sperm quality and fallopian tube obstruction.
Methods to improve fertility were reported by 27.6% (n = 333/1,206) of participants (Table 2). Timed intercourse (79.6%; n = 218/274) and ovulation induction (70.5%; n = 182/258) were the most used methods. In vitro fertilization (IVF) was reported by 33.5% (n = 71/212).
Endometriosis (Diagnosis, Family History, and Symptoms)
The majority of participants (94.6%; n = 1,261/1,333) reported having an endometriosis diagnosis, mostly by surgery (72.1%) (Table 2). Participants reporting a family history of endometriosis included a total of 461 (108 from mother, 113 from sister(s), 177 from a family member on the maternal side, and 123 from the paternal side, including grandmother, aunts, or cousins). A total of 1,260 participants reported a family history of chronic pelvic pain (381 from mother, 312 from a sister, 373 from a family member on the maternal side, and 194 from the paternal side).
Most of the participants who underwent surgery for an endometriosis diagnosis were prompted by pain symptoms (89.8%, n = 1,132/1,261) and 25.7% (n = 324) for infertility or other symptoms (13.0%, n = 164). The mean age at pelvic pain onset was 21.9 years (SD ± 7.9 years), while the mean age at diagnosis was 27.6 years (SD ± 6.7 years). The calculated diagnostic delay for this cohort is 6.6 years on average (SD ± 10.3 years). The most common symptoms reported were back and leg pain (85.4%), fatigue and low energy (80.7%), and abdominal pain (78.2%) Participants also reported gastrointestinal symptoms, such as abdominal fullness, bloating, and swelling (82.1%), and urinary symptoms such as urgency (54.1%) (Figure 5).
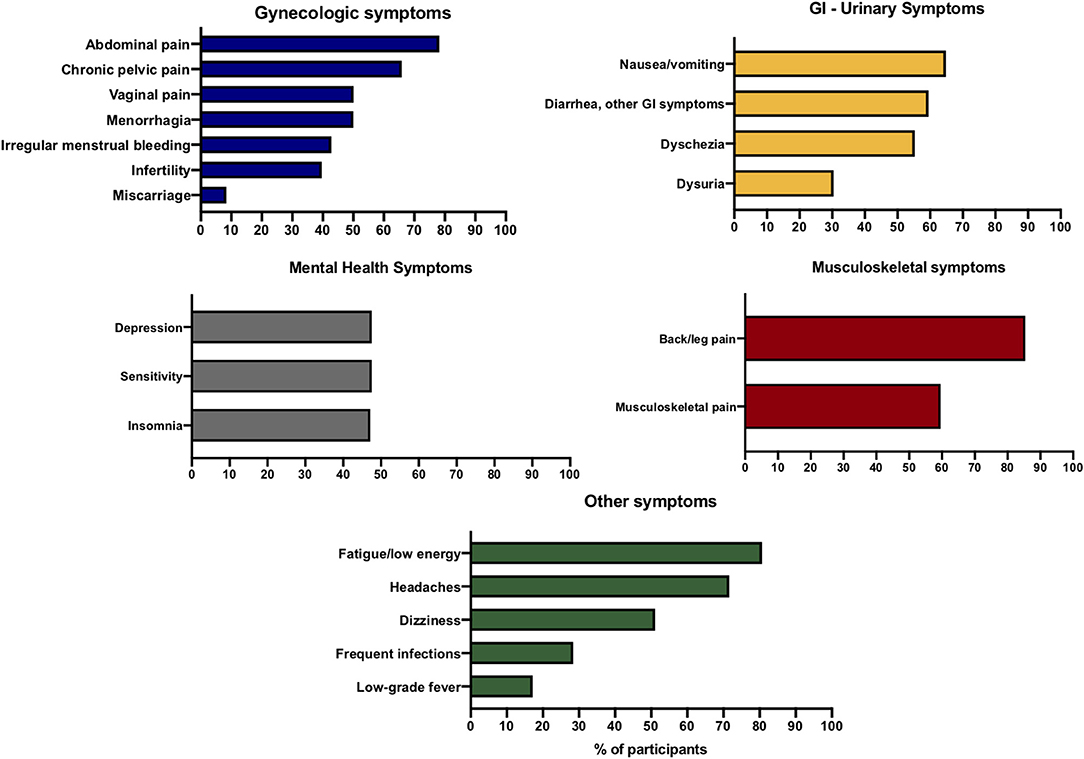
Figure 5. The most common symptoms reported by participants organized by system.
Clinical History
The most common comorbidities reported by participants were migraines, polycystic ovary syndrome (PCOS), and irritable bowel syndrome (IBS) (Table 3). Of interest, 2.3% (n = 31/1,322) reported a cancer diagnosis, at a mean age of 29.7 (SD ± 8.3 years). The most common self-reported malignancies were cervical (n = 11) and endometrial (n = 6) cancers. Anxiety and depression were reported by 19.5 and 17.4%, respectively.
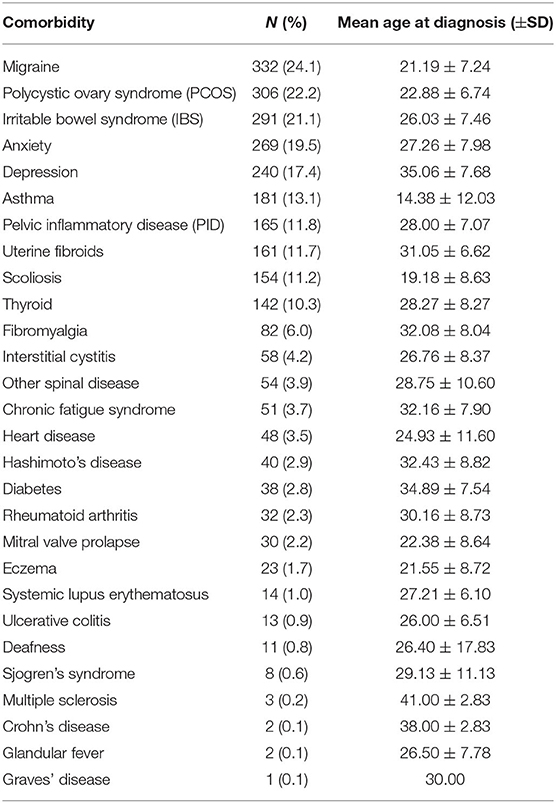
Table 3. Most common comorbidities reported by endometriosis patients from Ibero-America.
Non-Menstrual Pelvic Pain
The majority (94.6%; n = 1,261/1,333) of participants had a self-reported diagnosis of endometriosis. Their mean age at pelvic pain onset was 21.9 (SD ± 7.9 years). The majority (84.7%, n = 993/1,173) reported experiencing generalized pelvic pain at some point during their life; 63.6% (n = 604/949) reported experiencing pelvic pain during the past month. Most participants (87.9%, n = 809/920) stated that the etiology of the pelvic pain was diagnosed by a physician. The most common diagnoses for pain were endometriosis (96.3%, n = 779), IBS (23.5%, n = 190), and PID (15.1%, n = 122) (Figure 6A). Participants often reported these conditions concomitantly.
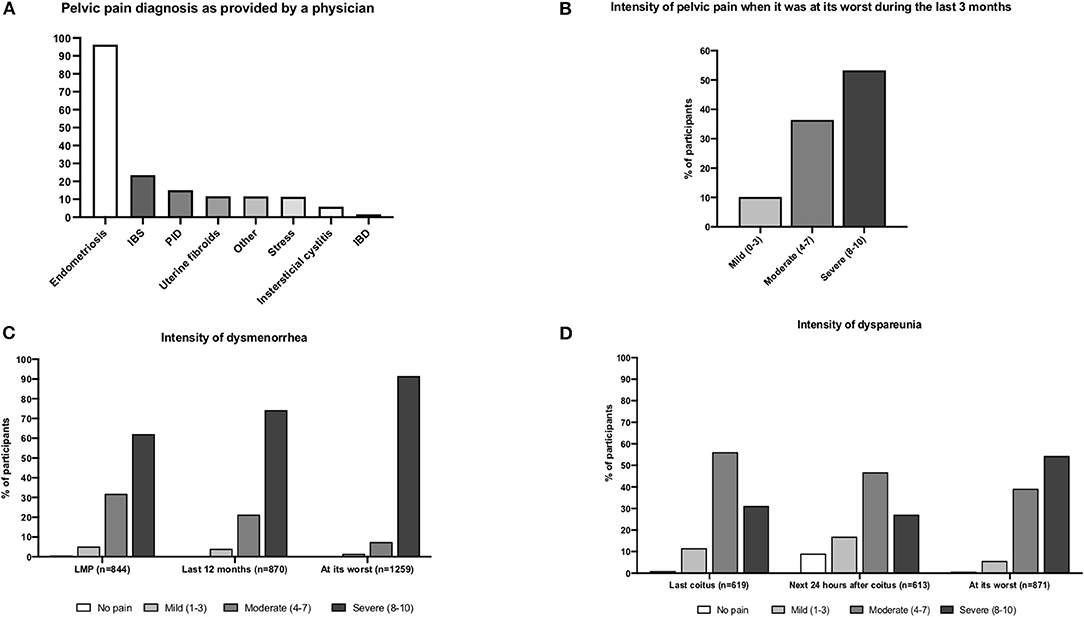
Figure 6. Diagnosis and intensity of pelvic pain. (A) Pelvic pain diagnosis. (B) Intensity level of pelvic pain (last 3 months). (C) Intensity of level of dysmenorrhea. (D) Intensity level of dyspareunia.
Many participants (78.0%) reported feeling pelvic pain within the last 3 months (n = 740/949). This pain was mostly aggravated by stress (58.1%, n = 430), voiding or having a full bladder (58.0%, n = 429), and constipation (55.3%, n = 409). It was mostly relieved by pain medications (79.7%, n = 590) or laying down (72.2%, n = 534). Pain intensity during the last 3 months was reported as severe by 53.3% (n = 391/734) of participants (Figure 6B).
Pelvic Pain During Menses (Dysmenorrhea)
The majority of participants (97.0%, n = 1,320/1,361) reported experiencing “pelvic pain during menses at some point during their life.” The pain was severe for 78.7% (n = 1,039) and moderate for 16.1% (n = 213). The mean age of dysmenorrhea onset was 16.19 ± 6.09 years. Dysmenorrhea was experienced during the last 12 months by 59.7% (n = 522/874) of participants. Severe pain intensity during the last menstrual period was reported by 62.2% (n = 525/844) and moderate by 31.9% (n = 269/844). During the past 12 months, 74.3% (n = 646/870) described their pain intensity as severe and 21.3% (n = 185/870) as moderate. When dysmenorrhea was at its worst, 91.5% (n = 1,152/1,259) reported severe pain, while only 7.5% (n = 94/1,259) reported moderate pain (Figure 6C). The mean pain intensity for dysmenorrhea ranged from 7.7 to 9.2 (Table 4).
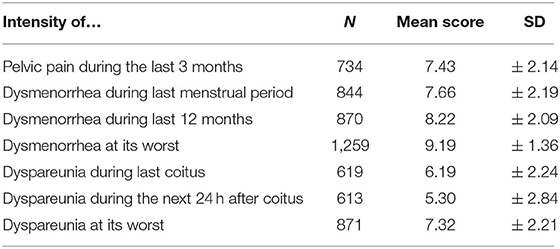
Table 4. Summary of pain intensity measured by NRS.
Pelvic Pain During Sexual Intercourse (Dyspareunia)
Most of the participants (86.4%, n = 907/1,050) had experienced dyspareunia throughout their lives, with a mean age of onset of 25.1 ± 5.85 years of age. Most (77.8%, n = 619/796) reported experiencing dyspareunia during their last sexual encounter. The pain was mostly felt during coitus (40.2%, n = 249), within the first 24 h afterwards (18.6%, n = 115), or both (41.2%, n = 255). Up to 75.9% (n = 44/58) admitted having avoided coitus due to the dyspareunia. The pain was generally experienced during the days following menses (34.9%, n = 97) and was most commonly localized in the pelvis or abdomen (43.9%, n = 457) and the deep vaginal canal (39.2%, n = 408).
Considering dyspareunia during the last year, most (72.4%, n = 440/608) of the participants interrupted coitus due to pain and 82.5% (n = 504/611) reported having avoided coitus overall. In general, 54.4% (n = 474/871) of participants classified dyspareunia as severe when it was at its worst.
Pain intensity (Figure 6D) during the last sexual intercourse (n = 619) was severe for 31.2% (n = 193) and moderate for 56.2% (n = 348). During the 24 h after intercourse (n = 613), pain intensity was severe for 27.1% (n = 166/613) and moderate for 46.8% (n = 287). Dyspareunia at its worst (n = 871) was severe for 54.4% (n = 474) and moderate for 39.2% (n = 341). The mean pain intensity for dyspareunia ranged from 5.3 to 7.3 (Table 4).
Most participants (92.7%, n = 856/923) reported taking medication for pelvic pain control. Approximately half of them used over-the-counter (OTC) medications (52.5%, n = 449/856), while 39.0% (n = 334/856) used prescribed medications. Few participants reported hormone use (8.3%, n = 73/856) as a therapeutic option for the pain, of which only 49.3% (n = 36/73) reported pain relief. A total of 735 participants completed the SF-MPQ. The mean score for this questionnaire was 22.30 (SD ± 11.59). Pelvic discomfort was mostly described as severely painful (46.9%, n = 345), persistent (38.0%, n = 279), and stinging (37.7%, n = 277) (Figure 7A).
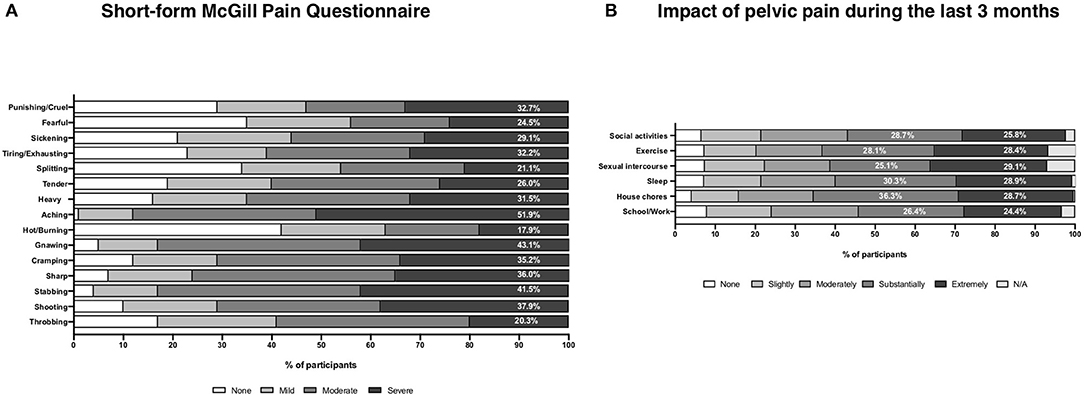
Figure 7. Pain characteristics and impact of pelvic pain on lifestyle. (A) Pain characteristics by the McGill Pain Questionnaire Short Form results. (B) The impact of pelvic pain during the last 3 months.
Impact of Pain in Daily Activities
Participants reported the pain being substantially (25.1–36.3%) or extremely (24.4–29.1%) interfering in daily activities, such as house chores, sleep, exercise, social activities, sexual intercourse, and school/work (Figure 7B).
Pain Catastrophizing Scale (PCS)
Out of all the participants, 1,275 completed all the questions of the PCS. Of those, 45.8% (n = 585) obtained a total score of 30 or higher, and 24.5% (n = 313) had a score between 20 and 29. The mean score for this scale in our population was 27.9 (SD ± 13.66) (Table 5), which is higher than what has been established as the 50th percentile in previous studies on endometriosis patients (17). The median in our cohort was 28.0, comparable to what has been reported in another cohort (18). Within each subscale of the PCS, there was one expression that was scored significantly higher than the others (p < 0.001): helplessness subscale: “I worry all the time about whether the pain will end,” mean score of 2.45 (SD ± 1.26); magnification subscale: “I become afraid that the pain will get worse,” mean score of 2.63 (SD ± 1.32); rumination subscale: “I anxiously want the pain to go away,” mean score of 3.05 (SD ± 1.23). Additionally, there was a positive correlation between the PCS score and pain symptomatology: pain intensity in dysmenorrhea at the last menstrual period (slope = 2.67, Pearson's r = 0.44, p < 0.001), dysmenorrhea at its worst (slope = 2.16, Pearson's r = 0.15, p < 0.001), dyspareunia at its worst (slope = 1.35, Pearson's r = 0.23, p < 0.001), and general pelvic pain at its worst in the last 3 months (slope = 1.54, Pearson's r = 0.30, p < 0.001).
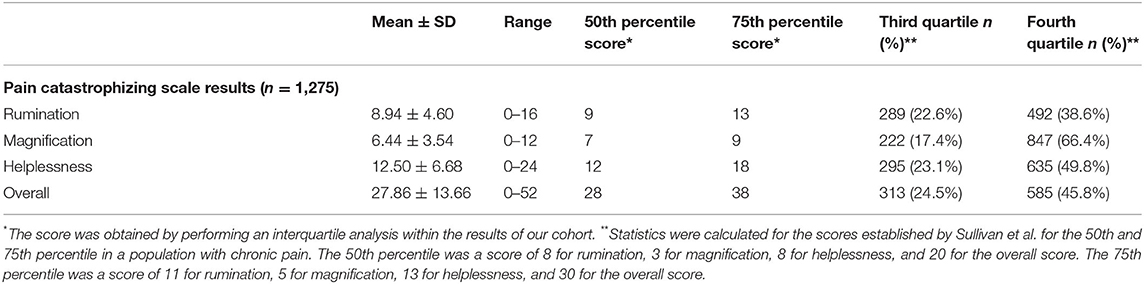
Table 5. Pain catastrophizing scale and subscales results.
Surgical Procedures
At least one abdomino-pelvic diagnostic laparoscopic procedure was reported by 61.6% (n = 849/1,378) of participants, while 14.7% (n = 202) reported having undergone at least two. The mean number of laparoscopies was 1.61 (± 1.01), with a range from 1 to 8. The mean age of laparoscopy was 27.54 ± 6.56 years, and the mean age at hysterectomy was 36.97 ± 6.29 years.
Pain Medications
During the worst pain episodes of dysmenorrhea, the most commonly used medications were OTC (63.0%, n = 831/1,320) and prescribed analgesics (43.5%, n = 574/1,320). Fewer participants (21.6%, n = 285/1,320) reported having used hormone-based medications for the pain, which were beneficial for less than half of them (46.7%, n = 133). Despite the use of analgesics, 42.3% (n = 358/846) of those experiencing dysmenorrhea during their last menses reported that the pain had affected their daily activities.
The most common medications used for pelvic pain were ibuprofen (35.8%, n = 493), acetaminophen (24.5%, n = 337), and other NSAIDs (23.7%, n = 327) (Figure 8A). Similarly, these agents were reported as the most common medications used for other types of pain (n = 1,461) (acetaminophen: 34.4%, n = 474; ibuprofen: 22.0%, n = 303; other NSAIDs: 12.2%, n = 168) (Figure 8B).
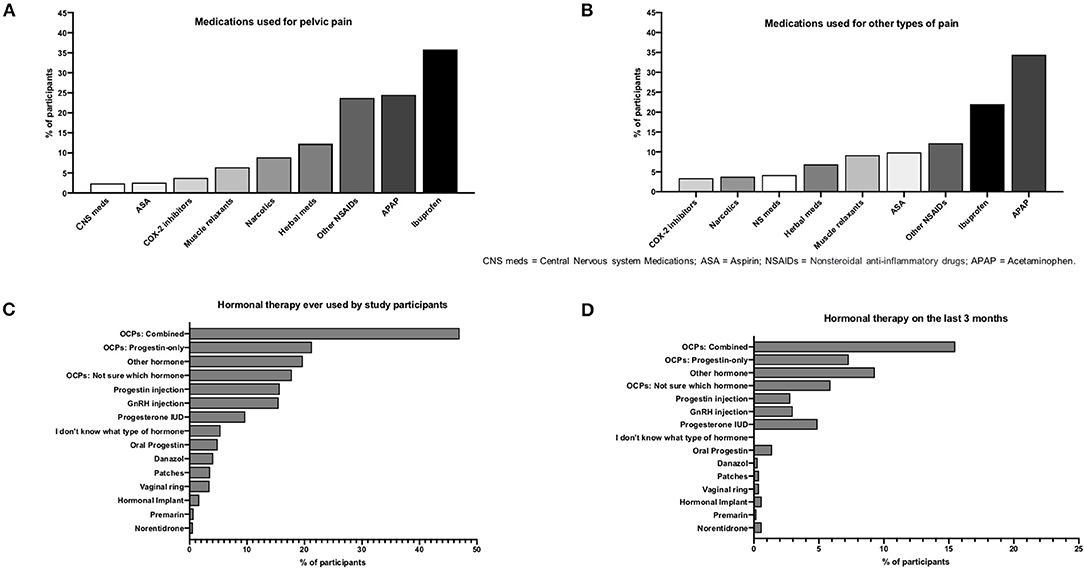
Figure 8. Pain medications and hormonal therapies. (A) Medications used for pelvic pain. (B) Medications used for other types of pain. (C) Hormonal therapies ever used by participants. (D) Hormonal therapies during last 3 months.
Hormonal Medications
Oral contraceptive pills (OCPs) were the hormonal therapy used the most, reported by 47.0% (n = 647) of participants (Figure 8C) and by 15.5% (n = 213) during the last 3 months (Figure 8D). OCPs were used for the longest time (56 ± 65.4 months on average). The main reason for hormone therapy was treatment for pelvic pain (55.4%; n = 764) followed by contraception (28.0%; n = 386). Only 40.7% (n = 309/760) reported some type of improvement of pain after OCP treatment. Half of the participants (50.4%; n = 225/446) changed treatment methods due to failed symptomatic relief of pelvic pain.
Discussion
This study was conducted to determine, for the first time, the demographic and clinical profile of endometriosis patients from Ibero-America using the Spanish translation of the EPhect's Minimal Clinical Questionnaire (EPQ-M) (19). Also, we demonstrate that the EPHect questionnaire is an efficient tool for standardized self-reported data collection to allow comparisons of the endometriosis phenome across ethnicities and geographic regions (5). The scarcity of investigations on the prevalence, disease presentation, level of impact, access to health care, and treatments in endometriosis patients who identify as Hispanic/Latinx adds to the current belief that this disease is less prevalent than in non-Hispanic White or Asian women (20). Collecting comprehensive data from patient populations not well-represented in databases is also critical to understand if there are differences in the clinical presentation of endometriosis based on race, genetics, and environmental or cultural factors and ultimately could help solve disparities in their representation in endometriosis research (4).
The translated EPQ-M survey was well-understood and accepted by Spanish-speaking women. Most evaluators considered it to be too long but a useful tool to conduct research on endometriosis across populations. Cross-sectional data was then collected from 1,378 Hispanic/Latinx endometriosis patients, recruited through collaborations with patient associations from South America, Central America, the Caribbean, and Spain, which represents the largest patient cohort from this ethnic background. Though the study link was disseminated through well-organized patient associations, the sample size could be considered small. Since prevalence data of endometriosis in Latin American and Caribbean populations are lacking (21, 22), it is difficult to estimate the generalizability of our study findings. Based on self-reported race, our cohort was 49.6% White, 4.5% Black, and 42.1% mixed race, vs. the estimated racial distribution of Latin American and Caribbean populations of 11% indigenous, 20% Afro descendants, and 40% White, in average, and these proportions vary from country to country (23). On closer look, the distribution of races per country in our study in general is representative of the respective racial proportions, except for Colombia, Mexico, and Venezuela. For example, Spain, Uruguay, and Argentina had the highest proportions of White participants, while countries with high Amerindian heritage such as Ecuador, Perú, and Mexico had the highest proportions of mixed race (Supplemental Table 1). Also, as expected, Black women had the highest participation in Dominican Republic, Panamá, and Puerto Rico, three countries with rich African heritage. Notably, the study had appropriate representation of non-White women (46.6% overall, and either equal to or higher than expected in most countries), who are not often well-represented in research cohorts. Efforts to recruit more diverse patients are ongoing, and future studies to assess the impact of race and ethnicity on endometriosis symptomatology are warranted.
Our study population had a relatively high economic status, the majority being employed and many having a higher degree of education. The level of education of our cohort is within that reported in other studies, ranging from 45 to 85% of patients reporting a higher than high school education (10, 24–26). It has previously been noted that there is an increased prevalence of endometriosis among well-educated women of higher socio-economic status, which may be due to better access to care or health awareness or possibly other lifestyle factors or habits linked to endometriosis risk (27).
Health risk behaviors were uncommon in this patient cohort; <15% reported high levels of alcohol consumption and <10% were smokers. Correlations between current alcohol intake and smoking and endometriosis risk (in infertile women) have been reported (10). A recent meta-analysis, however, did not find any association between smoking and endometriosis risk (28). Overall, our population did not exercise regularly: only around 30% reported exercising weekly. Moderate-to-high intensity physical activity has been associated with reduced endometriosis risk (29), though randomized studies to establish if an exercise intervention is effective against endometriosis are lacking. Thus, while this cohort did not report high rates of risk behaviors, they also had low rates of protective behaviors against endometriosis development.
The mean age of the participants falls within the age groups with the highest incidence of endometriosis (24–36 years of age) (10). Our cohort reported a lower age at menarche compared to others (11.8 vs. 12.8–12.9 years of age) (28, 30, 31). Menorrhagia prevalence (11.2%) falls within what has been previously reported (2.3–13.2%) (32, 33). We identified known risk factors for endometriosis in this population, including early age at menarche, long and heavy menstrual cycles, and nulliparity (62.3%). The average number of children was 1.5, which is similar to another study (1.7 ± 1.1) (34). The prevalence of spontaneous abortions (20.5%) was within that reported by other endometriosis patient cohorts (14.3–20.8) (24, 34) and that of women without endometriosis (34). The rate of C-sections in our cohort (58.7%) was higher than the US national average (31.9% in 2018) (35) and other patient cohorts of (37.3%) (36, 37). Stillbirth rate (0.9%) was lower than that reported in other endometriosis cohorts (1.9%), while ectopic pregnancy rate was higher (4.4%) compared to another study (1.8%) (34).
Endometriosis has been associated with adverse maternal, fetal, and neonatal outcomes (34, 36, 38). Yet, in our cohort, we observed preeclampsia rates (4.5%) that are within the global rate of 2–8% (39) and lower than the rate reported by other cohorts of endometriosis patients (7.9 and 9.5%) (34, 36). The rate of gestational diabetes (3.4%) was also lower when compared to the average rate in the USA (6%) (39) and to other studies of endometriosis patients (4.3%) (34). Notably, a substantial proportion of our cohort had sought infertility treatment (67.2% of those ever trying to get pregnant), which is higher than that reported in other cohorts (33.7 and 52.8%) (28, 34). We calculated 3.7 years with infertility in average. Endometriosis was reported as the primary cause of infertility by 87.5%, much higher than that in other cohorts (52.8%) (31, 34). The utilization rate of in vitro fertilization (IVF) was 8.4%, similar to other cohorts (7.7%) (36, 37).
In average, the diagnosis of endometriosis was delayed 7 years, in accord with previous estimates (40). The primary reason for diagnostic surgery was for pelvic pain (>90%), higher than other cohorts (63 and 21%) (28, 33). Infertility as the reason for surgery (26%) was within what has been reported in other studies (4–55%) (28, 33). Overall, this study did not identify any major differences in the patient profile compared to other patient cohorts. The most common symptoms reported were back and leg pain, bloating, and fatigue, which were higher than more characteristic symptoms of endometriosis such as pelvic pain (30, 41). GI and urinary symptoms were also very commonly reported as in other cohorts (42).
The most common comorbidities self-reported in our cohort were migraines, PCOS, and IBS. Although endometriosis patients are more likely to suffer migraine headaches (43), the prevalence of migraines in our cohort (24.1%) is close to the upper range for the lifetime prevalence of migraine in women (20.0%; 95% CI: 16.6–23.8%) (44) and lower than in other patient cohorts (35.2 and 38.3%) (45, 46). The PCOS rate (22.2%) was higher than the worldwide incidence (3–10%) (47) and higher than in other cohorts (5%) (48). The IBS prevalence was higher in our study (21%) than what is reported in the US population (14.1%), but similar to other patient cohorts (22.4 and 24.0%) (49, 50). The prevalence of uterine leiomyomas was 12%, which is within what has been reported in other patient cohorts (5–21%) (24, 28, 33, 48) and lower than in the US population (35%) (51). The self-reported prevalence of cancer was relatively high (2.3%) for a young population (mean 33.7 years old); this rate is higher than what has been reported in another cohort (ovarian−0.2%, breast−0.4%, and melanoma−0.7%) (52). Rates of anxiety (19.5%) and depression (17.4%) were significantly lower than those reported in another cohort (45% anxiety and 30% depression) (53).
The majority of patients in this cohort reported feeling generalized pelvic pain early in their lives (in their 20's); endometriosis was the most common cause of this pain, followed by IBS and PID. Dysmenorrhea was reported by almost all participants (97%), and 79% considered the pain severe. This prevalence is higher than that in other studies (69%) (30, 31). Our patient cohort has been extremely affected by pelvic pain as 9 in 10 patients described their pain at its worst as being between intensity 8 and 10 on the NRS. The prevalence of dyspareunia (86.4%) was higher than that in other patient cohorts (38 and 45%) (30, 31), and 8 out of 10 reported severe symptomatology during their last sexual encounter. Many participants (49–65%) reported a substantial-to-extreme interference of daily activities by their pain, adding to the strong evidence that endometriosis impacts all aspects of the life course of those affected (54).
While it identified that there is access to surgical expertise across the region (55), our study was not designed to detect whether this access was determined by socioeconomic status or other variables. In fact, the EPQ-M survey does not capture information on income, urban/rural residence, or other known proxies of economic status when in fact these factors have been shown to influence access to standard of care in endometriosis. A study conducted in Puerto Rico showed that patients of endometriosis who had public health insurance were less likely to receive gynecologic consultation and more likely to seek emergency room services (56). Follow-up studies on factors that affect access to care in each country are needed to better understand and be able to solve any disparities.
This cohort used hormonal treatments (mainly OCP) predominantly for pain management, yet their use was reported by a relatively low number of participants (only half ever used them and 16% during the last 3 months). This indicates that there are opportunities to improve access to hormonal medications that have been shown to provide substantial endometriosis-related pain relief. It will be important to investigate whether cost limits access to hormonal medications or if cultural factors, such as taboos, religion, and stigma, can play a role in the low use of hormones that are also prescribed for contraception. Another important consideration is the high rate of treatment failure to hormonal drugs observed in this study and others that may impact treatment adherence (30).
The average age at diagnosis of our cohort was 22 years old. Patients' age has a profound impact in the management of endometriosis since modern trends avoid surgery and the use of advanced hormonal treatments during early reproductive years. Experts are leaning more toward a presumptive diagnosis of endometriosis trying to avoid multiple laparoscopies and toward combined oral contraceptives that are better tolerated and can be prescribed for a longer, indefinite time. In contrast, most advanced hormonal therapies such as GnRH analogs can only be used for 6–24 months. Furthermore, this young age for self-awareness of endometriosis may reflect a success story regarding patients' self-education and potential providers' detection in timely fashion leading to improved control of the condition.
One of the key symptoms that patients with endometriosis present is pelvic pain, which can become chronic and is often refractory to treatments. This debilitating symptom is cause for substantial detriments to the physical functioning, emotional wellbeing, and quality of life (57–59). We showed here high rates of all pain manifestations surveyed (dysmenorrhea, dyspareunia, and non-menstrual pain) compared to published data. Notably, negative coping responses to painful experience such as pain catastrophizing were common in this patient population. We also observed a positive correlation between reported pain levels and catastrophizing scores, as shown before (18, 60). This maladaptive mechanism has been associated with pain persistence and correlated with poorer quality of life and depression, and it may impact the clinical management of pelvic pain (15, 17, 18). Based on the Pain Catastrophizing Scale score, 46% of our cohort has a high risk of developing persistence of their pain and disability (PSC > 30) (18). This supports the importance of applying a psychosomatic approach for clinical management of chronic pain in endometriosis patients (61). Follow-up studies to assess the impact of race, ethnicity, and socioeconomic factors on the pain catastrophizing scores in this patient population are warranted.
This study may not be representative of all women with endometriosis in this population for various reasons. There may be a bias of recruitment through patient organizations as it is possible that members are more symptomatic. Collection of self-reported data has been previously shown to have relatively high concordance with surgical diagnosis (14). Our study population was highly educated, which may be explained by the fact that the study was conducted using an electronic link requiring of internet access. This finding is in accord to studies showing increased prevalence of endometriosis among well-educated women of higher socio-economic status (27). While, overall, the race distribution in each of the countries included was in accord with each country race proportions, there was a lower-than-expected participation of Black patients. Thus, it could be argued that these results are not representative of all endometriosis patients in this world region. Follow-up studies must be conducted to include a wider racial, ethnic, and socioeconomic representation of persons with endometriosis in these countries, to assess the impact of these factors on pain perception and impact. Our study highlights the need to establish a centralized repository of data collected longitudinally using the EPHect tools that are publicly available for future research, possibly with funding from local institutes of health, patient associations, gynecologic practices, and the WERF.
In conclusion, this study uncovered for the first time the phenome of endometriosis patients of Hispanic/Latinx background, showing substantial severity of symptoms, high pain catastrophizing scores, and overall negative impact on quality of life. As EPHect tools become more widely used, future studies must take into account confounding variables such as socioeconomic status, culture, race, and health systems, as these are known to impact access to care and thus could directly affect the clinical diagnosis of endometriosis. Such studies should also address cultural and religious factors regarding menstruation, contraception, and women's health issues, including normalization of symptoms and paternalistic nature of patient–doctor interactions (62). Importantly, forthcoming studies must recognize that the Hispanic/Latinx population is heterogeneous genetically and culturally and that there are differences in health insurance systems, availability/access to medications or surgical procedures, referral trends for sub-specialists, exposures, diet, and other environmental factors/stressors. Together, all these factors influence clinical care, disease presentation, and outcomes; thus, more research is needed to disentangle their contributions and to provide the best medical care possible to all patients, irrespective of race/ethnicity.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors by request.
Ethics Statement
The studies involving human participants were reviewed and approved by Ponce Research Institute Institutional Review Board (IRB). Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author Contributions
IF-C made substantial contributions in the conception and design of the study, data acquisition, analysis and interpretation of data, drafting the article, critically revising the manuscript for important intellectual content, and giving the final approval. PR-E made substantial contributions in the analysis and interpretation of data, drafting and revising the article, and giving the final approval. JO-T, NS-P, ER-M, BH-C, LR-H, and LM made substantial contributions in the analysis and interpretation of data, revising the article, and giving the final approval. DS-S made substantial contributions in the analysis and interpretation of data, revising the article, and giving the final approval of the version to be published. MR-R made substantial contributions to the conception and design of the survey validation study, revising the manuscript critically for important intellectual content, and giving final approval. NB and ER made substantial contributions in the analysis and interpretation of data, revising the manuscript critically for important intellectual content, and giving the final approval. The Ibero-American Endometriosis Association* made substantial contributions to the acquisition of data, revision of the article critically for important content, and the final approval. All authors contributed to the article and approved the submitted version.
Funding
This study was funded in part by the National Institute of Child Health and Human Development (NICHD), National Institutes of Health (NIH) (R21HD098481-01).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank Nicolle Arroyo, Yadira Lugo, Ariana Cotto, and Paola Ortiz for contributions in aspects of IRB protocol and manuscript review. We acknowledge the role of Dr. Jennifer Mier for verifying the cultural competency of the Spanish translation of the EPQ-M survey. Thanks to Dr. Annelyn Torres-Reverón for substantial contributions to the statistical analysis plan.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frph.2021.667345/full#supplementary-material
References
1. Zondervan KT, Becker CM, Missmer SA. Endometriosis. N Engl J Med. (2020) 382:1244–56. doi: 10.1056/NEJMra1810764
2. Macer ML, Taylor HS. Endometriosis and infertility: a review of the pathogenesis and treatment of endometriosis-associated infertility. Obstet Gynecol Clin North Am. (2012) 39:535–49. doi: 10.1016/j.ogc.2012.10.002
3. Practice bulletin no. 114: management of endometriosis. Obstet Gynecol. (2010) 116:223–36. doi: 10.1097/AOG.0b013e3181e8b073
4. Non-European populations still underrepresented in genomic testing samples: Dearth of African-American, Latino, and other non-European groups contributes to healthcare, research disparities. Am J Med Genet A. (2017) 173:296–7. doi: 10.1002/ajmg.a.38149
5. Miller LM, Johnson NP. EPHect - the endometriosis phenome (and biobanking) harmonisation Project - may be very helpful for clinicians and the women they are treating. F1000Res. (2017) 6:14. doi: 10.12688/f1000research.9850.1
6. Becker CM, Laufer MR, Stratton P, Hummelshoj L, Missmer SA, Zondervan KT, et al. World endometriosis research foundation endometriosis phenome and biobanking harmonisation project: I. Surgical phenotype data collection in endometriosis research. Fertil Steril. (2014) 102:1213–22. doi: 10.1016/j.fertnstert.2014.07.709
7. Fassbender A, Rahmioglu N, Vitonis AF, Vigano P, Giudice LC, D'Hooghe TM, et al. World endometriosis research foundation endometriosis phenome and biobanking harmonisation project: IV. Tissue collection, processing, and storage in endometriosis research. Fertil Steril. (2014) 102:1244–53. doi: 10.1016/j.fertnstert.2014.07.1209
8. Rahmioglu N, Fassbender A, Vitonis AF, Tworoger SS, Hummelshoj L, D'Hooghe TM, et al. World endometriosis research foundation endometriosis phenome and biobanking harmonization project: III. Fluid biospecimen collection, processing, and storage in endometriosis research. Fertil Steril. (2014) 102:1233–43. doi: 10.1016/j.fertnstert.2014.07.1208
9. Vitonis AF, Vincent K, Rahmioglu N, Fassbender A, Buck Louis GM, Hummelshoj L, et al. World endometriosis research foundation endometriosis phenome and biobanking harmonization project: II. Clinical and covariate phenotype data collection in endometriosis research. Fertil Steril. (2014) 102:1223–32. doi: 10.1016/j.fertnstert.2014.07.1244
10. Missmer SA, Hankinson SE, Spiegelman D, Barbieri RL, Marshall LM, Hunter DJ. Incidence of laparoscopically confirmed endometriosis by demographic, anthropometric, and lifestyle factors. Am J Epidemiol. (2004) 160:784–96. doi: 10.1093/aje/kwh275
11. Eggert J, Li X, Sundquist K. Country of birth and hospitalization for pelvic inflammatory disease, ectopic pregnancy, endometriosis, and infertility: a nationwide study of 2 million women in Sweden. Fertil Steril. (2008) 90:1019–25. doi: 10.1016/j.fertnstert.2007.07.1345
12. Bougie O, Healey J, Singh SS. Behind the times: revisiting endometriosis and race. Am J Obstet Gynecol. (2019) 221:35.e1–5. doi: 10.1016/j.ajog.2019.01.238
13. Bougie O, Yap MI, Sikora L, Flaxman T, Singh S. Influence of race/ethnicity on prevalence and presentation of endometriosis: a systematic review and meta-analysis. BJOG. (2019) 126:1104–15. doi: 10.1111/1471-0528.15692
14. Shafrir AL, Wise LA, Palmer JR, Shuaib ZO, Katuska LM, Vinayak P, et al. Validity of self-reported endometriosis: a comparison across four cohorts. Hum Reprod. (2021) 36:1268–78. doi: 10.1093/humrep/deab012
15. Sullivan MJ, D'Eon JL. Relation between catastrophizing and depression in chronic pain patients. J Abnorm Psychol. (1990) 99:260–3. doi: 10.1037/0021-843X.99.3.260
16. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. (2009) 42:377–81. doi: 10.1016/j.jbi.2008.08.010
17. McPeak AE, Allaire C, Williams C, Albert A, Lisonkova S, Yong PJ. Pain catastrophizing and pain health-related quality-of-life in endometriosis. Clin J Pain. (2018) 34:349–56. doi: 10.1097/AJP.0000000000000539
18. Sewell M, Churilov L, Mooney S, Ma T, Maher P, Grover SR. Chronic pelvic pain - pain catastrophizing, pelvic pain and quality of life. Scand J Pain. (2018) 18:441–8. doi: 10.1515/sjpain-2017-0181
19. Rogers PA, Adamson GD, Al-Jefout M, Becker CM, D'Hooghe TM, Dunselman GA, et al. Research priorities for endometriosis. Reprod Sci. (2017) 24:202–26. doi: 10.1177/1933719116654991
20. Farland LV, Horne AW. Disparity in endometriosis diagnoses between racial/ethnic groups. BJOG. (2019) 126:1115–6. doi: 10.1111/1471-0528.15805
21. Flores I, Abreu S, Abac S, Fourquet J, Laboy J, Rios-Bedoya C. Self-reported prevalence of endometriosis and its symptoms among Puerto Rican women. Int J Gynaecol Obstet. (2008) 100:257–61. doi: 10.1016/j.ijgo.2007.08.010
22. Fuentes A, Escalona J, Cespedes P, Espinoza A, Johnson MC. [Prevalence of endometriosis in 287 women undergoing surgical sterilization in Santiago Chile]. Rev Med Chil. (2014) 142:16–9. doi: 10.4067/S0034-98872014000100003
23. Giuffrida A. Racial and ethnic disparities in Latin America and the Caribbean: a literature review. Diversity in Health and Care. (2010) 7:115–28.
24. Fourquet J, Sinaii N, Stratton P, Khayel F, Alvarez-Garriga C, Bayona M, et al. Characteristics of women with endometriosis from the USA and Puerto Rico. J Endometr Pelvic Pain Disord. (2015) 7:129–35. doi: 10.5301/je.5000224
25. Rush G, Misajon R. Examining subjective wellbeing and health-related quality of life in women with endometriosis. Health Care Women Int. (2018) 39:303–21. doi: 10.1080/07399332.2017.1397671
26. Nogueira-Silva C, Costa P, Martins C, Barata S, Alho C, Calhaz-Jorge C, et al. Validation of the Portuguese version of EHP-30 (The Endometriosis Health Profile-30). Acta Med Port. (2015) 28:347–56. doi: 10.20344/amp.5778
27. Parazzini F, Esposito G, Tozzi L, Noli S, Bianchi S. Epidemiology of endometriosis and its comorbidities. Eur J Obstet Gynecol Reprod Biol. (2017) 209:3–7. doi: 10.1016/j.ejogrb.2016.04.021
28. Hemmert R, Schliep KC, Willis S, Peterson CM, Louis GB, Allen-Brady K, et al. Modifiable life style factors and risk for incident endometriosis. Paediatr Perinat Epidemiol. (2019) 33:19–25. doi: 10.1111/ppe.12516
29. Ricci E, Vigano P, Cipriani S, Chiaffarino F, Bianchi S, Rebonato G, et al. Physical activity and endometriosis risk in women with infertility or pain: systematic review and meta-analysis. Medicine. (2016) 95:e4957. doi: 10.1097/MD.0000000000004957
30. Evans SF, Brooks TA, Esterman AJ, Hull ML, Rolan PE. The comorbidities of dysmenorrhea: a clinical survey comparing symptom profile in women with and without endometriosis. J Pain Res. (2018) 11:3181–94. doi: 10.2147/JPR.S179409
31. Warzecha D, Pietrzak B, Szymusik I, Smiech Z, Wielgos M. Should the patients with endometriosis be treated as a risk group of pregnancy complications? Single center experience and literature review and literature review. Ginekol Pol. (2020) 91:383–8. doi: 10.5603/GP.a2020.0084
32. Fong YF, Hon SK, Low LL, Lim Mei Xian K. The clinical profile of young and adolescent women with laparoscopically diagnosed endometriosis in a Singapore tertiary hospital. Taiwan J Obstet Gynecol. (2017) 56:181–3. doi: 10.1016/j.tjog.2016.07.013
33. Hemmings R, Rivard M, Olive DL, Poliquin-Fleury J, Gagne D, Hugo P, et al. Evaluation of risk factors associated with endometriosis. Fertil Steril. (2004) 81:1513–21. doi: 10.1016/j.fertnstert.2003.10.038
34. Farland LV, Prescott J, Sasamoto N, Tobias DK, Gaskins AJ, Stuart JJ, et al. Endometriosis and risk of adverse pregnancy outcomes. Obstet Gynecol. (2019) 134:527–36. doi: 10.1097/AOG.0000000000003410
35. Martin JA, Hamilton BE, Osterman MJK, Driscoll AK. Births: final data for 2018. Natl Vital Stat Rep. (2019) 68:1–47.
36. Chen I, Lalani S, Xie RH, Shen M, Singh SS, Wen SW. Association between surgically diagnosed endometriosis and adverse pregnancy outcomes. Fertil Steril. (2018) 109:142–7. doi: 10.1016/j.fertnstert.2017.09.028
37. Chen I, Thavorn K, Yong PJ, Choudhry AJ, Allaire C. Hospital-associated cost of endometriosis in Canada: a population-based study. J Minim Invasive Gynecol. (2020) 27:1178–87. doi: 10.1016/j.jmig.2019.09.771
38. Lalani S, Choudhry AJ, Firth B, Bacal V, Walker M, Wen SW, et al. Endometriosis and adverse maternal, fetal and neonatal outcomes, a systematic review and meta-analysis. Hum Reprod. (2018) 33:1854–65. doi: 10.1093/humrep/dey269
39. Committee on Practice B-O. ACOG Practice Bulletin No. 190: gestational diabetes mellitus. Obstet Gynecol. (2018) 131:e49–64. doi: 10.1097/AOG.0000000000002501
40. Nnoaham KE, Hummelshoj L, Webster P, d'Hooghe T, de Cicco Nardone F, de Cicco Nardone C, et al. Impact of endometriosis on quality of life and work productivity: a multicenter study across ten countries. Fertil Steril. (2011) 96:366–73.e8. doi: 10.1016/j.fertnstert.2011.05.090
41. Ramin-Wright A, Schwartz ASK, Geraedts K, Rauchfuss M, Wolfler MM, Haeberlin F, et al. Fatigue - a symptom in endometriosis. Hum Reprod. (2018) 33:1459–65. doi: 10.1093/humrep/dey115
42. Ek M, Roth B, Ekstrom P, Valentin L, Bengtsson M, Ohlsson B. Gastrointestinal symptoms among endometriosis patients–a case-cohort study. BMC Womens Health. (2015) 15:59. doi: 10.1186/s12905-015-0213-2
43. Yang MH, Wang PH, Wang SJ, Sun WZ, Oyang YJ, Fuh JL. Women with endometriosis are more likely to suffer from migraines: a population-based study. PLoS ONE. (2012) 7:e33941. doi: 10.1371/journal.pone.0033941
44. Frederick IO, Qiu C, Enquobahrie DA, Aurora SK, Peterlin BL, Gelaye B, et al. Lifetime prevalence and correlates of migraine among women in a pacific northwest pregnancy cohort study. Headache. (2014) 54:675–85. doi: 10.1111/head.12206
45. Maitrot-Mantelet L, Hugon-Rodin J, Vatel M, Marcellin L, Santulli P, Chapron C, et al. Migraine in relation with endometriosis phenotypes: results from a French case-control study. Cephalalgia. (2020) 40:606–13. doi: 10.1177/0333102419893965
46. Ferrero S, Pretta S, Bertoldi S, Anserini P, Remorgida V, Del Sette M, et al. Increased frequency of migraine among women with endometriosis. Hum Reprod. (2004) 19:2927–32. doi: 10.1093/humrep/deh537
47. Wolf WM, Wattick RA, Kinkade ON, Olfert MD. Geographical prevalence of polycystic ovary syndrome as determined by region and race/ethnicity. Int J Environ Res Public Health. (2018) 15:2589. doi: 10.3390/ijerph15112589
48. Deo R, Adami F, Mafra FA, Bianco B, Vilarino FL, Barbosa CP. Causes of endometriosis and prevalent infertility in patients undergoing laparoscopy without achieving pregnancy. Minerva Ginecol. (2016) 68:250–8.
49. Hungin AP, Chang L, Locke GR, Dennis EH, Barghout V. Irritable bowel syndrome in the United States: prevalence, symptom patterns and impact. Aliment Pharmacol Ther. (2005) 21:1365–75. doi: 10.1111/j.1365-2036.2005.02463.x
50. DiVasta AD, Zimmerman LA, Vitonis AF, Fadayomi AB, Missmer SA. Overlap between irritable bowel syndrome diagnosis and endometriosis in adolescents. Clin Gastroenterol Hepatol. (2020) 19:528–37.e1. doi: 10.1016/j.cgh.2020.03.014
51. Baird DD, Dunson DB, Hill MC, Cousins D, Schectman JM. High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidence. Am J Obstet Gynecol. (2003) 188:100–7. doi: 10.1067/mob.2003.99
52. Gemmill JA, Stratton P, Cleary SD, Ballweg ML, Sinaii N. Cancers, infections, and endocrine diseases in women with endometriosis. Fertil Steril. (2010) 94:1627–31. doi: 10.1016/j.fertnstert.2009.07.1698
53. Robert CA, Caraballo-Rivera EJ, Isola S, Oraka K, Akter S, Verma S, et al. Demographics and hospital outcomes in American women with endometriosis and psychiatric comorbidities. Cureus. (2020) 12:e9935. doi: 10.7759/cureus.9935
54. Missmer SA, Tu FF, Agarwal SK, Chapron C, Soliman AM, Chiuve S, et al. Impact of endometriosis on life-course potential: a narrative review. Int J Gen Med. (2021) 14:9–25. doi: 10.2147/IJGM.S261139
55. Hsu AL, Khachikyan I, Stratton P. Invasive and noninvasive methods for the diagnosis of endometriosis. Clin Obstet Gynecol. (2010) 53:413–9. doi: 10.1097/GRF.0b013e3181db7ce8
56. Fourquet J, Zavala DE, Missmer S, Bracero N, Romaguera J, Flores I. Disparities in healthcare services in women with endometriosis with public vs. private health insurance. Am J Obstet Gynecol. (2019) 221:623.e1–11. doi: 10.1016/j.ajog.2019.06.020
57. Fourquet J, Baez L, Figueroa M, Iriarte RI, Flores I. Quantification of the impact of endometriosis symptoms on health-related quality of life and work productivity. Fertil Steril. (2011) 96:107–12. doi: 10.1016/j.fertnstert.2011.04.095
58. Fourquet J, Gao X, Zavala D, Orengo JC, Abac S, Ruiz A, et al. Patients' report on how endometriosis affects health, work, and daily life. Fertil Steril. (2010) 93:2424–8. doi: 10.1016/j.fertnstert.2009.09.017
59. Soliman AM, Coyne KS, Gries KS, Castelli-Haley J, Snabes MC, Surrey ES. The effect of endometriosis symptoms on absenteeism and presenteeism in the workplace and at home. J Manag Care Spec Pharm. (2017) 23:745–54. doi: 10.18553/jmcp.2017.23.7.745
60. Yosef A, Allaire C, Williams C, Ahmed AG, Al-Hussaini T, Abdellah MS, et al. Multifactorial contributors to the severity of chronic pelvic pain in women. Am J Obstet Gynecol. (2016) 215:760.e1–14. doi: 10.1016/j.ajog.2016.07.023
61. Hauser W, Jones G. Psychological therapies for chronic widespread pain and fibromyalgia syndrome. Best Pract Res Clin Rheumatol. (2019) 33:101416. doi: 10.1016/j.berh.2019.05.001
Keywords: endometriosis, hispanic/latinx, epidemiology, symptoms, ethnicity, phenome, dysmenorrhea, dyspareunia
Citation: Flores-Caldera I, Ramos-Echevarría PM, Oliveras-Torres JA, Santos-Piñero N, Rivera-Mudafort ED, Soto-Soto DM, Hernández-Colón B, Rivera-Hiraldo LE, Mas L, Rodríguez-Rabassa M, Bracero NJ, Rolla E and Ibero-American Endometriosis Association (2021) Ibero-American Endometriosis Patient Phenome: Demographics, Obstetric-Gynecologic Traits, and Symptomatology. Front. Reprod. Health 3:667345. doi: 10.3389/frph.2021.667345
Received: 12 February 2021; Accepted: 30 March 2021;
Published: 04 June 2021.
Edited by:
Nilufer Rahmioglu, Wellcome Trust Centre for Human Genetics (WT), United KingdomReviewed by:
Adriana Invitti, Federal University of São Paul, BrazilPaola Vigano', San Raffaele Hospital (IRCCS), Italy
Copyright © 2021 Flores-Caldera, Ramos-Echevarría, Oliveras-Torres, Santos-Piñero, Rivera-Mudafort, Soto-Soto, Hernández-Colón, Rivera-Hiraldo, Mas, Rodríguez-Rabassa, Bracero, Rolla and Ibero-American Endometriosis Association. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Idhaliz Flores-Caldera, aWZsb3Jlc0Bwc20uZWR1
†Eva Alva—Mexico; Luz Marina Araque—Colombia; Marcela Arraya–Chile; Jessica Calvo-Costa Rica; Gabriela Gutierrez—Venezuela; Yuriko Huarcaya—Peru; Paola Paniagua—Dominican Republic; Maria Angeles Poveda—Spain; Viviana Setton—Argentina; Mercedes Valdés—Panama