
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Oral. Health , 28 June 2024
Sec. Preventive Dentistry
Volume 5 - 2024 | https://doi.org/10.3389/froh.2024.1429332
This article is part of the Research Topic Addressing Oral Health Disparities in Maternal and Child Populations View all 7 articles
 Abiola Adeniyi1*
Abiola Adeniyi1* Gladys Akama2
Gladys Akama2 Ochiba Lukandu3
Ochiba Lukandu3 Justus E. Ikemeri4
Justus E. Ikemeri4 Anjellah Jumah4
Anjellah Jumah4 Sheilah Chelagat4
Sheilah Chelagat4 Anusu Kasuya4
Anusu Kasuya4 Laura Ruhl4,5
Laura Ruhl4,5 Julia Songok4,6Astrid Christoffersen-Deb4,7
Julia Songok4,6Astrid Christoffersen-Deb4,7
Oral conditions disproportionately affect mothers and children in Sub-Saharan Africa, due to biological vulnerabilities, a scarcity of oral health workers, deficient preventive strategies, and gender-based barriers to care. The World Health Organization (WHO) recommends integrating oral health into broader health delivery models, to reduce these disparities. We propose integrating preventive oral healthcare into community-based programs to bridge these gaps. We examine integrating preventive oral healthcare into Western Kenya's Chamas for Change (Chamas) community-based program which aims to reduce maternal and child health disparities. Chamas incorporates women's health and microfinance programs best practices to produce a low-cost, community-driven, sustainable, and culturally acceptable health delivery platform. Our strategy is based on the Maternal and Child Oral Health Framework and uses the WHO Basic Package of Oral Care principles. This framework prioritizes community involvement, cultural sensitivity, regular screenings, and seamless integration into general health sessions. We discuss the strengths, weaknesses, opportunities, and threats to enriching Chamas with oral health promotion activities. It is crucial to assess the effectiveness, sustainability, and acceptability of the proposed strategy through implementation and evaluation. Future studies should investigate the long-term impact of integrated oral health models on community health and oral health disparity reduction in Africa.
The World Health Organization (WHO) reports that 3.5 billion people, roughly half of the global population, suffer from oral diseases such as dental caries, periodontal disease, edentulism, and oral cancer (1–3). These conditions share common risk factors and social determinants with many noncommunicable diseases (NCDs) (2–5). They also disproportionately affect vulnerable people, in particular those of low socio-economic status and rural residents (6, 7). Women and children face additional barriers due to gender-based inequalities (8, 9). Oral health has an extremely important role in general well-being and quality of life, particularly for women and children. Moreover, oral diseases despite being largely preventable, still place a considerable financial strain on households (9–12). This situation highlights the need for innovative and cost-effective strategies to address the inequitable impact of oral diseases on mothers and children (2, 3).
In 2019, oral diseases affected over 480 million people —44% of the population -, in Sub-Saharan Africa including Kenya, marking a significant increase over the last three decades (7, 13). This rise is largely due to structural determinants such as financial barriers, lack of oral health policies, inadequate oral health infrastructure and insufficient healthcare providers awareness, which collectively limit access to oral health care (7, 14, 15). These challenges are worse for women and girls, who face additional cultural and economic barriers to health services, including oral health care (16–18). With 25% of the African population suffering from untreated dental caries, there is an urgent need for interventions designed to address these barriers and improve oral health outcomes (6, 13).
Our article aims to bridge the gap in access to oral health care in Sub-Saharan Africa by proposing the incorporation of oral health activities into community-based programs targeting mothers and children in the region. Using the Chamas for Change program (Chamas) in Western Kenya as a prototype, we advocate for the integration of preventive oral health care into community-based interventions. We describe how this can be implemented to address individual and community oral health disparities while aligning with global oral health goals and the Kenyan national oral health strategic plan (19–23). We include a Strengths, Weaknesses, Opportunities, and Threats (SWOT) analysis of this solution to illustrate the rationale and benefits. We posit that our proposal will improve oral health outcomes and overall well-being in underserved populations. Ultimately, we emphasize the essential role of oral health within the broader public health context, and advocate for its recognition as a vital element of comprehensive well-being (22).
The Chamas program was launched in 2012 by the Academic Model Providing Access to Healthcare (AMPATH) in collaboration with the Government of Kenya. This community-based program focuses on addressing the inequities that drive maternal and infant mortality in Kenya by creating a community-based service delivery platform that facilitates access to care, financial empowerment, peer support and sexual and reproductive health (SRH) advocacy (24). Using the longstanding tradition of community-based support structures in East Africa, “Chamas,” which means “groups with purpose” in Swahili, addresses the health, social, and financial needs of pregnant women and mothers in the first 3 years postnatally.
Chamas creates an affordable, community-run, self-sustaining, and culturally acceptable integrated service delivery platform by integrating best practices from microfinance and women's health programs. Chamas' 3-year mentored program improves perinatal outcomes through health, social, and financial literacy (24–26). The program is facilitated by Community Health Promoters (CHPs), that are community nominated part-time government volunteers, under the supervision of Community Health Extension Workers (24). The CHPs undergo comprehensive training, including a 2-week session covering various health topics, with a focus on maternal neonatal and child health (MNCH). These trained individuals conduct routine health visits, collect health information, identify health problems, and refer individuals to health facilities when needed.
The Chamas program engages women in groups of 15–20 participants, meeting twice a month over a 12-month period to attend 24 CHP-facilitated sessions annually. These sessions cover a range of health and social topics, from antenatal care to intimate partner violence, utilizing illustrated flipcharts and participatory discussions. Members commit to practicing key MNCH behaviors and have the option to participate in the “Group Integrated Savings for Health and Empowerment” (GISHE) a table-banking program. This optional program enables members to contribute to a microfinance scheme, fostering financial empowerment. Chamas has been successfully integrated into the primary care delivery framework across counties in Western Kenya. Currently operational in 5 counties (Trans Nzoia, Busia, Bungoma, Uasin-Gishu and Elgeyo Marakwet) and 15 sub-counties, the program has 430 groups with 4,701 participants.
The Chamas program addresses different stages of maternal and child well-being over 3 years. Prenatal and early postnatal care, family planning, exclusive breastfeeding, and financial literacy are covered in year 1 for pregnant women in their first or second trimesters. In year 2, which covers the first year postpartum, the programme emphasises early parenting, childhood immunizations, complementary feeding, and bank account opening. Year 3, for the second-year postpartum, emphasises positive parenting, helps participants apply for government loans, and encourages small businesses. Overall, the program has demonstrated success, with positive effects on key health outcomes, fostering participant's empowerment, and community building (24–26).
Chamas women have demonstrated significantly higher odds of achieving positive MNCH outcomes, including delivering in a healthcare facility under the supervision of a trained healthcare provider, receiving a 48-h postpartum visit from a CHP, exclusively breastfeeding for at least 6 months, and adopting a postpartum contraceptive method (24, 25, 27). Chamas participation was associated with five times the odds of facility delivery and a 5-fold increase in the likelihood of a CHP conducting a post-delivery home visit (24). Moreover, participants reported greater infant immunization completion rates, reduced parental stress, and fewer reports of abuse (24–26). Beyond health impacts, the program promotes community-centered care, builds resilience during pandemics and other health emergencies, fosters increased peer support, enhances women's empowerment, strengthens family and community support, and leads to increased uptake of National Health Insurance.
While the Chamas program effectively addresses various MNCH concerns, its influence on oral health outcomes remains unexamined. Nonetheless, given its demonstrated success in enhancing overall maternal and child health outcomes and promoting community empowerment, integrating preventive oral health activities into the Chamas framework offers a promising avenue for addressing oral health disparities among mothers and children in Kenya. It also holds promise for delivering preventive oral health to people living in rural areas and those who experience limited access to care. Considering the Chamas program's significant impact, the interrelation between oral health and systemic well-being, and the imperative for oral health interventions for mothers and children in Kenya, we propose the integration of preventive oral health activities within the Chamas activities framework.
Our proposed solution aims to integrate oral health education and screening sessions into the 3-year Chamas program. We plan to integrate comprehensive oral health education both as standalone sessions and within selected existing health and social education sessions. Our proposal is to feature 24 oral health promotion topics in the first 2 years of the Chamas program, with a detailed breakdown provided in Table 1. These include four standalone topics and the inclusion of oral health content in nine existing sessions in the first year. This is followed by one standalone topic and the integration of oral health information into ten existing sessions in the second year. Drawing upon the WHO training curriculum, we plan to equip CHPs with the necessary knowledge to impart basic oral health information (28). We intend to train the CHPs via a 3-day workshop facilitated by a trained dental public health specialist. We will supplement the initial training with annual refreshers that align with current MNCH training. This equips CHPs with WHO-guided knowledge to deliver community-based oral health interventions effectively.
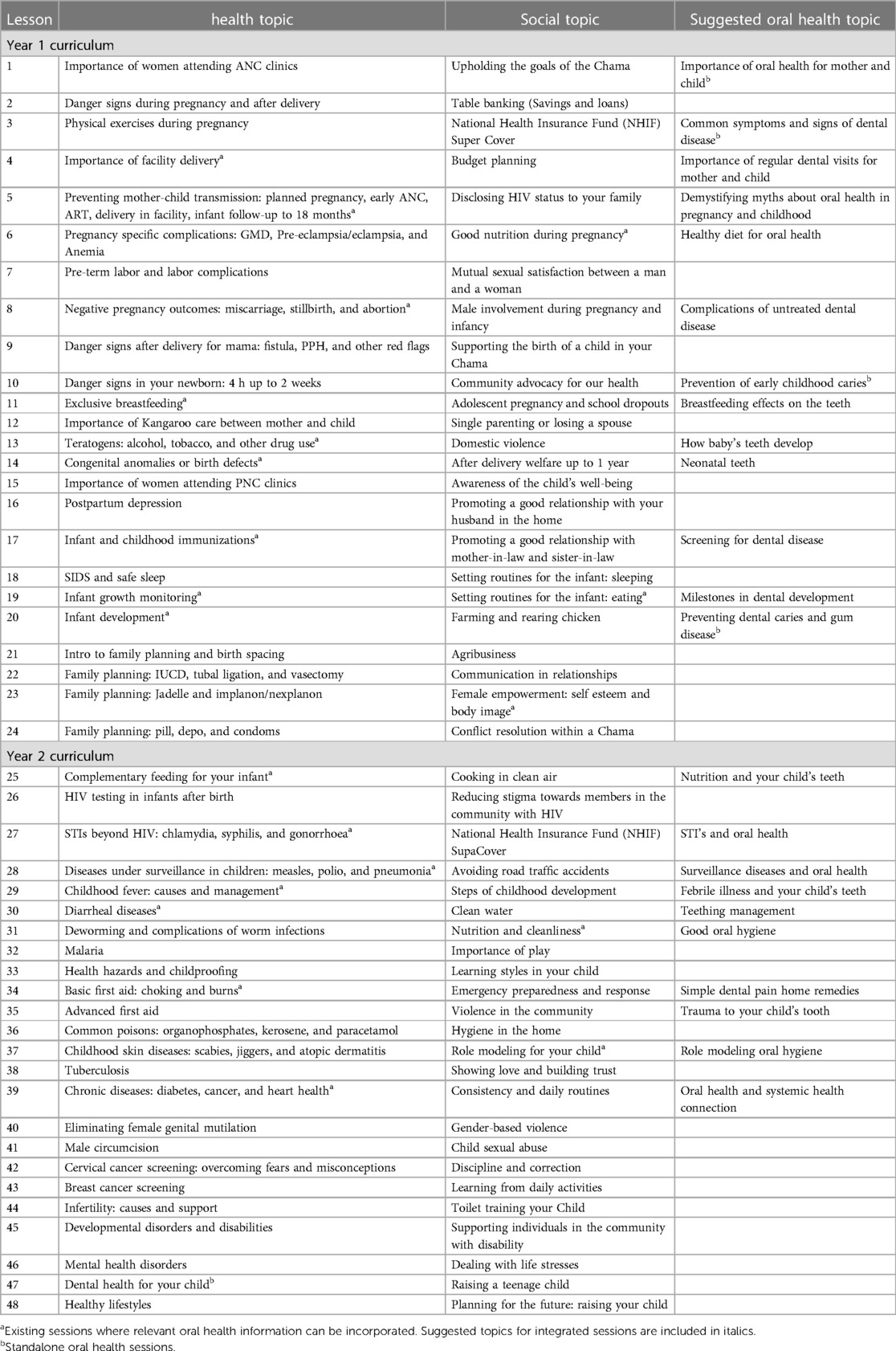
Table 1 Proposed revised Chamas curriculum including oral health education topics.
Our strategy also includes conducting annual oral health screenings in the second and third years, based on the WHO's Basic Package of Oral Care (BPOC) (29). This package includes Oral Urgent Treatment (OUT), the use of Affordable Fluoride Toothpaste (AFT), and Atraumatic Restorative Treatment (ART). Community Oral Health Workers will oversee these screenings, facilitate access to dental care facilities and administer treatments such as AFT and ART where necessary. This approach seeks to enhance the Chamas program by embedding preventive oral healthcare within routine care, to reduce maternal and child oral health disparities.
Our Logic Model (Figure 1) for integrating oral health promotion activities in the Chamas Program outlines a structured approach to improving maternal and child health through enhanced oral health practices. It includes inputs such as funding, trained human resources, necessary materials, and technology for data collection. Key activities involve training CHPs, conducting epidemiological surveys, promoting the use of fluoridated toothpaste, and providing ART procedures. Outputs will measure the reach and effectiveness of these activities, including the number of training sessions, surveys completed, toothpaste distributed, and ART procedures performed. Outcomes are categorized into short-term, intermediate, and long-term effects, highlighting improvements in oral health knowledge, practices, and overall health outcomes. The ultimate impact aims to enhance maternal and child health, increase community awareness, and build the capacity of healthcare providers to address oral health issues effectively.

Figure 1 Logic model depicting the integration of oral health promotion activities within the Chamas program.
The Chamas program is an innovative, integrated health strategy that addresses maternal and child oral health disparities in Sub-Saharan Africa. In this section, we use a SWOT analysis (Table 2) to emphasize the strengths, weaknesses, opportunities, and threats of integrating preventive oral health activities into a community-based program-Chamas— that has enhanced MNCH outcomes in rural Kenya (24–27).
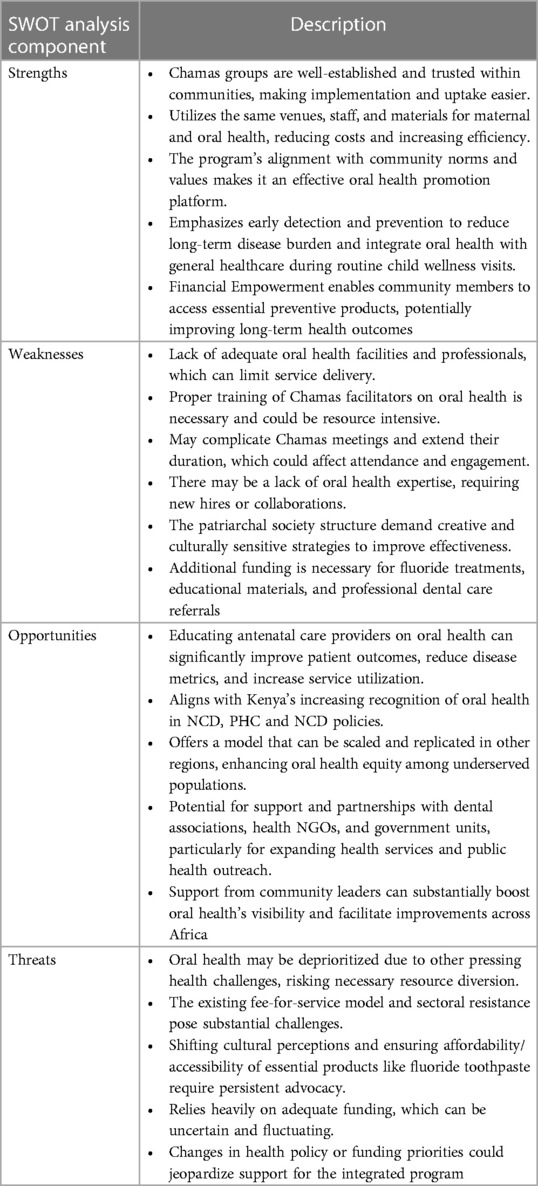
Table 2 A summary of the SWOT analysis for integrating oral health into the Chamas program.
Our planned integration leverages our current infrastructure to expand service delivery. Chamas' established structure within communities and its high level of trust and engagement are therefore key strengths. It will be easy to achieve smooth implementation and higher uptake of the oral health intervention with these attributes. This will help reduce the long-term oral disease burden among vulnerable populations through our intervention, which focuses on prevention and early detection (29). Chamas a viable tool for oral health promotion because it allows the use of the same venues, staff, and materials for oral health making it cost-effective and efficient. The CHPs can deliver oral health education aligning with global and Kenyan policies to optimize resource use and health outreach (1, 3, 5, 15, 19, 22).
We also envisage integrating oral health into routine early child wellness visits and utilizing Chamas' peer-support systems to improve oral health at the individual, familial, and community levels (28, 30–32). This can foster a culture of prevention for oral health, improve access to oral healthcare through annual screenings, and integrate oral health with general healthcare (5, 14). In addition, our program's financial empowerment component can assist members in accessing essential preventive oral health products, such as fluoride toothpastes (33).
We have identified several weaknesses in the proposed integration. The oral health infrastructure in Kenya is insufficient, and there is a lack of awareness about the importance of oral health, including among non-dental health professionals (19, 34, 35). A strong public health system that includes oral health is needed for the oral health component to be effective. Kenya's free maternity services greatly contributed to the improvement of MNCH outcomes for Chamas, indicating a potential model for oral health. Creative solutions to address the cultural and socioeconomic challenges, especially the patriarchal nature of Kenyan society is important. Securing extra funding for fluoride treatments, educational materials, and potential professional oral healthcare referrals could pose a challenge. Training Chamas facilitators in preventive oral health may require significant resources, and potentially complicate Chamas meetings thus extending their duration. Chamas attendance may be impacted, and new skills or collaborations may be required, both of which can create logistical and budgetary challenges.
There are a lot of opportunities to make a positive impact by integrating preventive oral health within Chamas. Our proposal can greatly enhance patient outcomes by training community health providers on oral health. This will empower women to make informed health decisions for themselves and their children. This training can lead to reduce gingival disease metrics, improve plaque control, and increase utilization of oral health services (36, 37). This will significantly decrease oral health issues, improve children's nutrition and overall health, and prevent maternal infections through these clinical improvements.
Our proposed model is scalable, can improve oral health competency among non-dental providers, promote interprofessional collaboration and address the critical oral health workforce gap (12, 38, 39). Our proposal aligns with Kenya's health policies and recognizes the importance of oral health in managing NCDs, enhancing primary healthcare and supporting the achievement of universal health coverage (19, 35). Moreover, we can partner with dental associations, health NGOs, and secure government support to enhance public health outreach. This can enable us to replicate this model in other regions (10, 39).
However, there are a few potential threats that could undermine this integration. The initiative may lose necessary resources due to competing health priorities and the low prioritization of oral health in the health system. There is need for broad-based support from diverse stakeholders to ensure the sustainability of the program, which can be challenging in many African settings. The project can face significant hurdles due to resistance from the healthcare sector and the prevailing fee-for-service delivery model given the high poverty levels in rural communities. Inaccurate information about oral health may greatly impede the acceptance and effectiveness of the intervention. Challenges in educating and engaging the public due to recurring myths and misunderstandings surrounding oral health practices can also occur. Strong advocacy is needed to change cultural perceptions and ensure that essential products, such as fluoride toothpaste, are affordable and accessible.
Our proposal's stability and continuity may be threatened by fluctuations in funding and shifts in health policy or funding priorities. These changes may jeopardize support for the integrated program. Moreover, there is need to coordinate effectively among different health workers and sectors to ensure successful integration. This can be challenging, especially in settings with limited resources. There is also a risk of diluting the quality of maternal and child health services if the program becomes overly diversified or if resources are overly stretched. This dilution could compromise the effectiveness of both the existing services and the new oral health initiative, ultimately impacting the overall health outcomes of the communities served. Each of these threats needs careful consideration and strategic planning to ensure that the potential benefits of the program are not outweighed by these substantial challenges. By addressing these threats, the program can enhance its effectiveness and sustainability, thereby improving maternal and child health outcomes through integrated and comprehensive healthcare services.
Integrating preventive oral health activities into the Chamas program aligns with global and Kenyan health policies, making it essential for achieving global targets for integrated healthcare delivery and improving maternal and child oral health. The proposed integration promises substantial improvements in oral health equity and enhancing overall well-being in Kenyan communities. Despite challenges posed by societal structures and healthcare system constraints, strategic planning and robust advocacy can overcome these obstacles, paving the way for a healthier future for Kenya's rural populations. Through this integrated approach, community-based programs like Chamas can significantly elevate maternal and child health standards by incorporating essential oral health services.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
AA: Conceptualization, Resources, Writing – original draft, Writing – review & editing. GA: Conceptualization, Writing – original draft, Writing – review & editing. OL: Conceptualization, Writing – review & editing. JI: Writing – review & editing. AJ: Writing – review & editing. SC: Writing – review & editing. AK: Writing – review & editing. LR: Writing – review & editing. JS: Writing – review & editing. AC-D: Conceptualization, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Watt RG, Daly B, Allison P, Macpherson LMD, Venturelli R, Listl S, et al. Ending the neglect of global oral health: time for radical action. Lancet. (2019) 394(10194):261–72. doi: 10.1016/S0140-6736(19)31133-X
2. Peres MA, Macpherson LMD, Weyant RJ, Daly B, Venturelli R, Mathur MR, et al. Oral diseases: a global public health challenge. Lancet. (2019) 394(10194):249–60. doi: 10.1016/S0140-6736(19)31146-8
3. Jain N, Dutt U, Radenkov I, Jain S. WHO’s global oral health status report 2022: actions, discussion and implementation. Oral Dis. (2024) 30(2):73–9. doi: 10.1111/odi.14516
4. Dorfer C, Benz C, Aida J, Campard G. The relationship of oral health with general health and NCDs: a brief review. Int Dent J. (2017) 67(Suppl 2):14–8. doi: 10.1111/idj.12360
5. Sheiham A, Alexander D, Cohen L, Marinho V, Moyses S, Petersen PE, et al. Global oral health inequalities: task group–implementation and delivery of oral health strategies. Adv Dent Res. (2011) 23(2):259–67. doi: 10.1177/0022034511402084
6. Abid A, Maatouk F, Berrezouga L, Azodo C, Uti O, El-Shamy H, et al. Prevalence and severity of oral diseases in the Africa and Middle East region. Adv Dent Res. (2015) 27(1):10–7. doi: 10.1177/0022034515582062
7. WHO Regional Office for Africa. Africa Burdened with Largest Global Increase of Oral Diseases. Congo, Brazzaville: World Health Organization (2023). Available online at: https://www.afro.who.int/news/africa-burdened-largest-global-increase-oral-diseases
8. World Health Organization. Breaking Barriers: Towards More Gender-Responsive and Equitable Health Systems. Geneva: World Health Organization (2019).
9. Jahan SS, Hoque Apu E, Sultana ZZ, Islam MI, Siddika N. Oral healthcare during pregnancy: its importance and challenges in lower-middle-income countries (LMICs). Int J Environ Res Public Health. (2022) 19(17):10681. doi: 10.3390/ijerph191710681
10. Abodunrin OR, Olagunju MT, Alade OT, MnO F. Relationships between oral health and the sustainable development goals: a scoping review. BioMed. (2023) 3(4):460–70. doi: 10.3390/biomed3040037
11. Bernabe E, Masood M, Vujicic M. The impact of out-of-pocket payments for dental care on household finances in low and middle income countries. BMC Public Health. (2017) 17(1):109. doi: 10.1186/s12889-017-4042-0
12. Huang YK, Chang YC. Oral health: the first step to sustainable development goal 3. J Formos Med Assoc. (2022) 121(7):1348–50. doi: 10.1016/j.jfma.2021.10.018
13. GBD 2019 Diseases and Injuries Collaborators. Oral disorders—level 3 cause. Lancet. (2020) 396:S180–81.
14. Sheiham A, Williams DM. Reducing inequalities in oral health in the Africa and Middle East region. Adv Dent Res. (2015) 27(1):4–9. doi: 10.1177/0022034515575540
15. Regional Committee for A. Regional Oral Health Strategy 2016–2025: Addressing Oral Diseases as Part of Noncommunicable Diseases: Report of the Secretariat. Brazzaville: World Health Organization (2016).
16. Barros AJ, Ronsmans C, Axelson H, Loaiza E, Bertoldi AD, França GV, et al. Equity in maternal, newborn, and child health interventions in countdown to 2015: a retrospective review of survey data from 54 countries. Lancet. (2012) 379(9822):1225–33. doi: 10.1016/S0140-6736(12)60113-5
17. Bonita R, Beaglehole R. Women and NCDs: overcoming the neglect. Glob Health Action. (2014) 7:23742. doi: 10.3402/gha.v7.23742
18. Langer A, Meleis A, Knaul FM, Atun R, Aran M, Arreola-Ornelas H, et al. Women and health: the key for sustainable development. Lancet. (2015) 386(9999):1165–210. doi: 10.1016/S0140-6736(15)60497-4
19. Kenya Ministry of Health. Kenya National Oral Health Strategic Plan 2022–2026. Nairobi, Kenya: Kenya Ministry of Health (2022).
20. Glick M, Williams DM. FDI vision 2030: delivering optimal oral health for all. Int Dent J. (2021) 71(1):3. doi: 10.1016/j.identj.2020.12.026
21. Nations U. Transforming Our World: The 2030 Agenda for Sustainable Development. New York: United Nations, Department of Economic and Social Affairs (2015) 1:41.
22. Organization WH. Draft global oral health action plan (2023–2030). WHO Discussion Paper; Version Dated 12 August (2022).
23. Petersen PE, Kwan S. The 7th WHO global conference on health promotion-towards integration of oral health (Nairobi, Kenya 2009). Community Dent Health. (2010) 27(Suppl 1):129–36. doi: 10.1922/CDH_2643Petersen08
24. Maldonado LY, Songok JJ, Snelgrove JW, Ochieng CB, Chelagat S, Ikemeri JE, et al. Promoting positive maternal, newborn, and child health behaviors through a group-based health education and microfinance program: a prospective matched cohort study in western Kenya. BMC Pregnancy Childbirth. (2020) 20(1):288. doi: 10.1186/s12884-020-02978-w
25. Maldonado LY, Bone J, Scanlon ML, Anusu G, Chelagat S, Jumah A, et al. Improving maternal, newborn and child health outcomes through a community-based women’s health education program: a cluster randomised controlled trial in western Kenya. BMJ Glob Health. (2020) 5(12):e003370. doi: 10.1136/bmjgh-2020-003370
26. Christoffersen-Deb A, Ruhl L, Elung'at J, Atieno M, Snelgrove J, Songok J. Chamas for change: an integrated community-based strategy of peer support in pregnancy and infancy in Kenya. Lancet Glob Health. (2015) 3:S22. doi: 10.1016/S2214-109X(15)70141-5
27. McHenry MS, Maldonado LY, Yang Z, Anusu G, Kaluhi E, Christoffersen-Deb A, et al. Participation in a community-based women’s health education program and at-risk child development in rural Kenya: developmental screening questionnaire results analysis. Glob Health Sci Pract. (2021) 9(4):818–31. doi: 10.9745/GHSP-D-20-00349
28. Morgan R, Davies SE, Feng H, Gan CCR, Grépin KA, Harman S, et al. Using gender analysis matrixes to integrate a gender lens into infectious diseases outbreaks research. Health Policy Plan. (2022) 37(7):935–41. doi: 10.1093/heapol/czab149
29. Frencken JEFM, Holmgren CJ, Helderman WHP. Basic Package of Oral Care: WHO Collaborating Centre for Oral Health Care Planning and Future Scenarios. Nijmegen, The Netherlands: University of Nijmegen (2002).
30. Thapa P, Bangura AH, Nirola I, Citrin D, Belbase B, Bogati B, et al. The power of peers: an effectiveness evaluation of a cluster-controlled trial of group antenatal care in rural Nepal. Reprod Health. (2019) 16(1):150. doi: 10.1186/s12978-019-0820-8
31. McLeish J, Redshaw M. Peer support during pregnancy and early parenthood: a qualitative study of models and perceptions. BMC Pregnancy Childbirth. (2015) 15(1):257. doi: 10.1186/s12884-015-0685-y
32. Sokol R, Fisher E. Peer support for the hardly reached: a systematic review. Am J Public Health. (2016) 106(7):e1–8. doi: 10.2105/AJPH.2016.303180
33. Nieuwenhuijze M, Leahy-Warren P. Women’s empowerment in pregnancy and childbirth: a concept analysis. Midwifery. (2019) 78:1–7. doi: 10.1016/j.midw.2019.07.015
34. Kenya Ministry of Health. Kenya National Oral Health Survey Report. Nairobi Kenya: Kenya Ministry of Health (2015).
35. Kenya Ministry of Health. Kenya National Oral Health Policy (2022–2030). Nairobi, Kenya: Kenya Ministry of Health (2022).
36. Adams SH, Gregorich SE, Rising SS, Hutchison M, Chung LH. Integrating a nurse-midwife-led oral health intervention into centering pregnancy prenatal care: results of a pilot study. J Midwifery Womens Health. (2017) 62(4):463–9. doi: 10.1111/jmwh.12613
37. Russell SL, Kerpen SJ, Rabin JM, Burakoff RP, Yang C, Huang SS. A successful dental care referral program for low-income pregnant women in New York. Int J Environ Res Public Health. (2021) 18(23):12724. doi: 10.3390/ijerph182312724
38. Gallagher JE, Mattos Savage GC, Crummey SC, Sabbah W, Varenne B, Makino Y. Oral health workforce in Africa: a scarce resource. Int J Environ Res Public Health. (2023) 20(3):2328. doi: 10.3390/ijerph20032328
Keywords: maternal and child health, oral health disparities, community-based strategy, preventive oral healthcare, Sub-Saharan Africa
Citation: Adeniyi A, Akama G, Lukandu O, Ikemeri JE, Jumah A, Chelagat S, Kasuya A, Ruhl L, Songok J and Christoffersen-Deb A (2024) Reducing maternal and child oral health disparities in Sub-Saharan Africa through a community-based strategy. Front. Oral. Health 5:1429332. doi: 10.3389/froh.2024.1429332
Received: 7 May 2024; Accepted: 7 June 2024;
Published: 28 June 2024.
Edited by:
Ollie Yiru Yu, The University of Hong Kong, Hong Kong SAR, ChinaReviewed by:
Maria Cristina Cangussu, Federal University of Bahia (UFBA), Brazil© 2024 Adeniyi, Akama, Lukandu, Ikemeri, Jumah, Chelagat, Kasuya, Ruhl, Songok and Christoffersen-Deb. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Abiola Adeniyi, YS5hZGVuaXlpQGZkdS5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.